")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Psychometric Evaluation of a Korean Version of the Sexual Risk Behavior Beliefs and Self-Efficacy Scale Among Female College Students: A Secondary Analysis
Authors Lee J , Montegrico JJC
Received 23 August 2022
Accepted for publication 24 October 2022
Published 1 November 2022 Volume 2022:15 Pages 3205—3215
DOI https://doi.org/10.2147/PRBM.S387296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Jungmin Lee,1 Jhordin James C Montegrico2
1School of Nursing, Hallym University, Chuncheon, Gangwon-do, 24252, South Korea; 2School of Nursing, University of North Carolina at Charlotte, Charlotte, NC, 28223, USA
Correspondence: Jungmin Lee, School of Nursing, Hallym University, 1 Hallymdaehak-gil, Chuncheon, Gangwon-do, 24252, South Korea, Tel +82-33-248-2728, Email [email protected]
Background and Purpose: Currently, no instrument exists to measure condom use behavior among Korean college students. This study aims to create a cross-cultural adaptation of the English version of the sexual risk behavior beliefs and self-efficacy (SRBBS) instrument into Korean and examine the psychological properties of the translated version.
Methods: Participants included 169 female college students recruited using convenience sampling techniques. Validity and reliability were examined using item and factor analyses and Cronbach’s alpha. Seventeen items were ultimately selected for analysis.
Results: Four factors were extracted through factor analysis, representing 63.80% of the variance. Following two modifications, it showed a good model fit in the KR-SRBBS.
Conclusion: The KR-SRBBS may be suitable for evaluating sexual behavior and self-efficacy among female college students.
Keywords: factor analysis, psychometrics, self-efficacy, sexual behavior, women
Introduction
During early adulthood, sex-related value systems are not generally fully established. As a result, young adults can be vulnerable to subjective judgment or choices regarding sexual behavior.1 Young adults are at high risk of engaging in risky sexual activities. These include sexual intercourse with multiple partners, unprotected sex, and sexual intercourse under the influence of drugs or alcohol.2 Unsafe or risky behaviors include engaging in sexual intercourse or other sexual activities without the use of protection. This considerably increases the risk of sexually transmitted diseases (STDs), including human immunodeficiency virus (HIV).3
A study found that poor sexual knowledge and higher acceptance of risky sexual behavior were correlated with earlier initial sexual experiences.4,5 Youths may risk negative health outcomes to satisfy their curiosity and explore sexual behaviors. According to previous studies, people under the age of 25 are more vulnerable to STDs as they often engage in risky sexual activities. These include having more than one sexual partner and a more frequent sex partner change rate than the general population. These activities increase the risk of STD/HIV transmission.6,7
Condom use is critical in preventing STD incidence,8 and increasing condom use among the youth has become a national health promotion and infection control priority.9 Regrettably, the level of condom use among young adults remains inconsistent or low.10,11 Between 2011 and 2015, 47.3% of men and 59.9% of women aged 15–44 in the US did not use condoms while engaging in sexual intercourse.12 In South Korea, a study by Lee13 showed similar results, indicating only 25%‒38.2% of young people used proper contraception such as condoms in the past year. Among them, 17.1% of Korean youths reported contracting STDs.14
In South Korea, there has been a higher prevalence of STDs (particularly gonorrhea and chlamydia) and HIV among females between the ages of 19 and 34 compared to males and other age groups.15 This might substantially impact their future sex life and marriage. Inadequate contraception use may increase their risk of exposure to various sexual health problems, including unwanted or unplanned pregnancies, single parenthood, abortions, and STDs, making women more vulnerable.16 Here, gender and power dynamics related to Confucian patriarchy may make contraceptive use more difficult for women than men.17 This can be conceptualized as a woman’s lack of control or power to avoid unhealthy or risky sexual behavior. Condom use behavior may vary by gender, age, sexual orientation, and marital status; hence, we limited this study’s target population to heterosexual, unmarried female emerging adults.
To our knowledge, there is currently no instrument to measure the intent to use condoms among Korean college students. Only a few studies focused on youths’ intention to use condoms to prevent STD/HIV transmission in South Korea. Therefore, this study adapted an instrument for examining condom use intent among Korean students. This instrument could play a significant role in explaining risky sexual behavior among female youths. Furthermore, this study aims to cross-culturally adapt the English version of the sexual risk behavior beliefs and self-efficacy (SRBBS) instrument by translating it into Korean before investigating the psychological properties of the translated version. The SRBBS instrument was selected because it highlights specific aspects of risky sexual behavior associated with the concepts presented in this study.
Background and Conceptual Framework
Theory of Planned Behavior
The concepts associated with the SRBBS instrument were derived from the theory of reasoned action, social learning theory, and the health belief model.18 The theory of planned behavior (TPB) plays a significant role in explaining the reasons for unsafe and risky sexual behaviors among young Korean adults. Most studies on this subject have demonstrated that young adults do not use condoms because of subjective norms (eg, cultural or social norms) or they are unaware of the potential risks (eg, misconceptions or misunderstandings). Previous studies also indicate that risky sexual behavior among the youth is significantly associated with their attitudes and beliefs regarding condom use.19
According to the TPB, four concepts could affect sexual behaviors among young adults: attitude, subjective norms, perceived behavioral control (PBC), and intention. As we cannot examine sexual behavior among the youth directly, the intention to use condoms will be used as a proxy for actual condom use behavior using three concepts based on the TPB. The TPB assumes that certain behaviors are predicted by the individual’s intention to engage in a specific behavior.20 Furthermore, predictors of the intention to engage in specific behaviors include attitudes, subjective norms, and PBC. First, attitudes toward specific behaviors indicate how actions seem desirable to each individual. This attribute is determined based on an individual’s mindset or beliefs, particularly the perceived outcomes of the behavior and the value placed on such outcomes. Second, subjective norms indicate how others perceive behaviors and how significant referents’ perceptions or beliefs could influence an individual’s behavior. Third, PBC can indicate an individual’s ability to engage in a specific behavior. This concept refers to perceived facilitators or barriers to enacting a specific behavior. Finally, intention indicates an individual’s decision to engage in specific behaviors, such as risky or unprotected sexual intercourse. In this study, the intention to use condoms is considered a proxy for sexual behavior.
Methods
Design
This study is methodological in that it evaluated the reliability and validity of the Korean version of the sexual risk behavior beliefs and self-efficacy (KR-SRBBS) instrument.
Participants
A total of 169 female college students aged 18‒25 were included in this study. The sample size was calculated using G*Power 3.1.9.2.21 The results indicated that 160 students were required to obtain reliable factors for the exploratory factor analysis. A 40% drop-off was accounted for due to incomplete or rushed surveys (completed in less than five minutes); hence 224 participants were recruited, and 169 samples were ultimately included in the analysis.
Measurement
Sexual Risk Behavior Beliefs and Self-Efficacy (SRBBS)
The initial study conducted by Basen-Engquist et al22 involved 6213 high school students in Texas and California. The SRBBS comprises 22 items rated on a 3- or 4-point Likert scale. Higher values for seven of the eight scales (except barriers to condom use) reflect greater intent not to engage in risky sexual behavior.23 The internal consistency reliability of the sub-categories, as indicated by Cronbach’s alpha, ranged from 0.70 to 0.78 in the initial study.
Translation Procedures
The guidelines for the cross-cultural adaptation process follow the recommendations outlined by the World Health Organization (WHO).24 The first step is forward translation, involving linguistic, conceptual, and cultural translation. This step was performed independently by two translators whose first language was Korean. In the second step, an expert panel reviewed the first forward-translated versions to identify and resolve inadequate expressions. They also identified discrepancies between the forward translation and the original English version. The panel comprised four experts, including the two in the forward translation phase. After debriefing and considering socio-cultural aspects, we changed some words to help the target population understand the content. After expert-panel approval, the third step involved back-translating the translated version into English. Back-translation was performed using the same method applied in the first step for consistency but using different translators. After back-translation, approval was obtained from the original author before instrument pre-testing. The fourth step involved an expert committee review. This committee comprised six experts from the forward translation, expert panel, and back-translation phases. In this step, the experts assessed the meaning of the translated questions and laid out the pre-final version. We discussed the clarity and appropriateness of the translated instrument in detail to ensure semantic and idiomatic equivalence. Furthermore, we confirmed experiential and conceptual equivalence between the two versions. Excluding the first author, five experts used the item relevance ratings to compute and verify the content validity of the KR-SRBBS. The fifth step involved pre-testing the translated instrument. We recruited 10 Korean undergraduate college students and tested their ability to read and comprehend the questions. Through this process, we determined whether the target population could predictably answer the questionnaire. After gathering the students’ data, one question was slightly revised. Ultimately, 22 questions were generated in the final version of the KR-SRBBS (Figure 1).
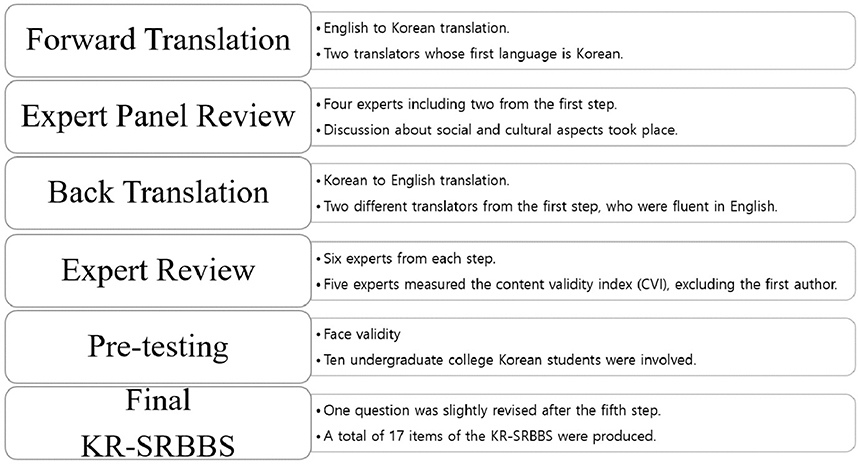 |
Figure 1 The KR-SRBBS Validation Process. |
The KR-SRBBS Validation Process
Content Validity
Content validity was assessed by five experts using the item-level content validity index (I-CVI). The final version of the KR-SRBBS was completed after considering socio-cultural aspects.
Construct and Convergent Validity
Exploratory Factor Analysis (EFA): First, varimax rotation was performed for EFA using the principal axis factoring method. Second, the Kaiser–Meyer–Olkin (KMO) and Bartlett’s test of sphericity were used to evaluate data factorability. Third, the screen test of eigenvalues was plotted. Fourth, the cumulative proportion (%) of variance was used to measure the proportion of variance accounted for by a factor. Finally, the pattern matrix was confirmed, which included the factor loadings for each key factor of interest.
Confirmatory Factor Analysis (CFA): CFA was performed using the factors extracted from the EFA. Chi-square, df and its p-value, RMSEA (90% CI), and CFI were tested to establish whether the findings showed a suitable model fit. The average variance extracted (AVE) was calculated using the CFA results. AVE is often considered one of the measures to check the convergent validity, indicating the size of variance that the indicator can explain for the latent concept. This value should be 0.5 or higher.
Internal Consistency Reliability
The item-total correlation and Cronbach’s alpha were measured to verify the internal consistency reliability of the KR-SRBBS. In addition, CR was used to measure the internal consistency of the indicator. The evaluation of the confidence level should be 0.7 or higher to guarantee internal consistency.
Procedures
Before the study, we received approval from the University of North Carolina at Greensboro Institutional Review Board. Convenience sampling was used, and participants were recruited using social networking services.
Data Analysis
The SPSS statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA) and AMOS statistics for Windows, version 26.0 (SPSS Inc., Chicago, IL. USA) were used for data analysis.
Ethics Consideration
This study was performed in line with the principles of the Declaration of Helsinki.25 Before this study was conducted, the Institutional Review Board of the University of North Carolina at Greensboro approved it. The questionnaire was distributed to the participants through an online survey (Qualtrics survey software). Informed consent was obtained on the first page before the students proceeded with the survey. After perusing the information sheet, students were asked to click yes if they agreed to participate in the study. The consent form contained the researcher’s introduction, the study’s purpose and method, the benefits of the study, confidentiality, and the procedure for withdrawing participation.
Results
Validity Test for KR-SRBBS
Content Validity
Five experts on maternity, women’s health nursing, and child and adolescent nursing computed the I-CVI. The mean I-CVI was 1.0.
Face Validity
We recruited 10 Korean undergraduate college students to verify face validity, and a post-position-related change was made to one question to increase readability and comprehensibility.
Construct Validity 1: Item Analysis for Internal Consistency
The item-to-total correlations of the KR-SRBBS were reasonable (Table 1). If we deleted items #14, #15, #16, and #17, Cronbach’s alpha increased slightly. Regardless, the items were retained because the change was negligible.
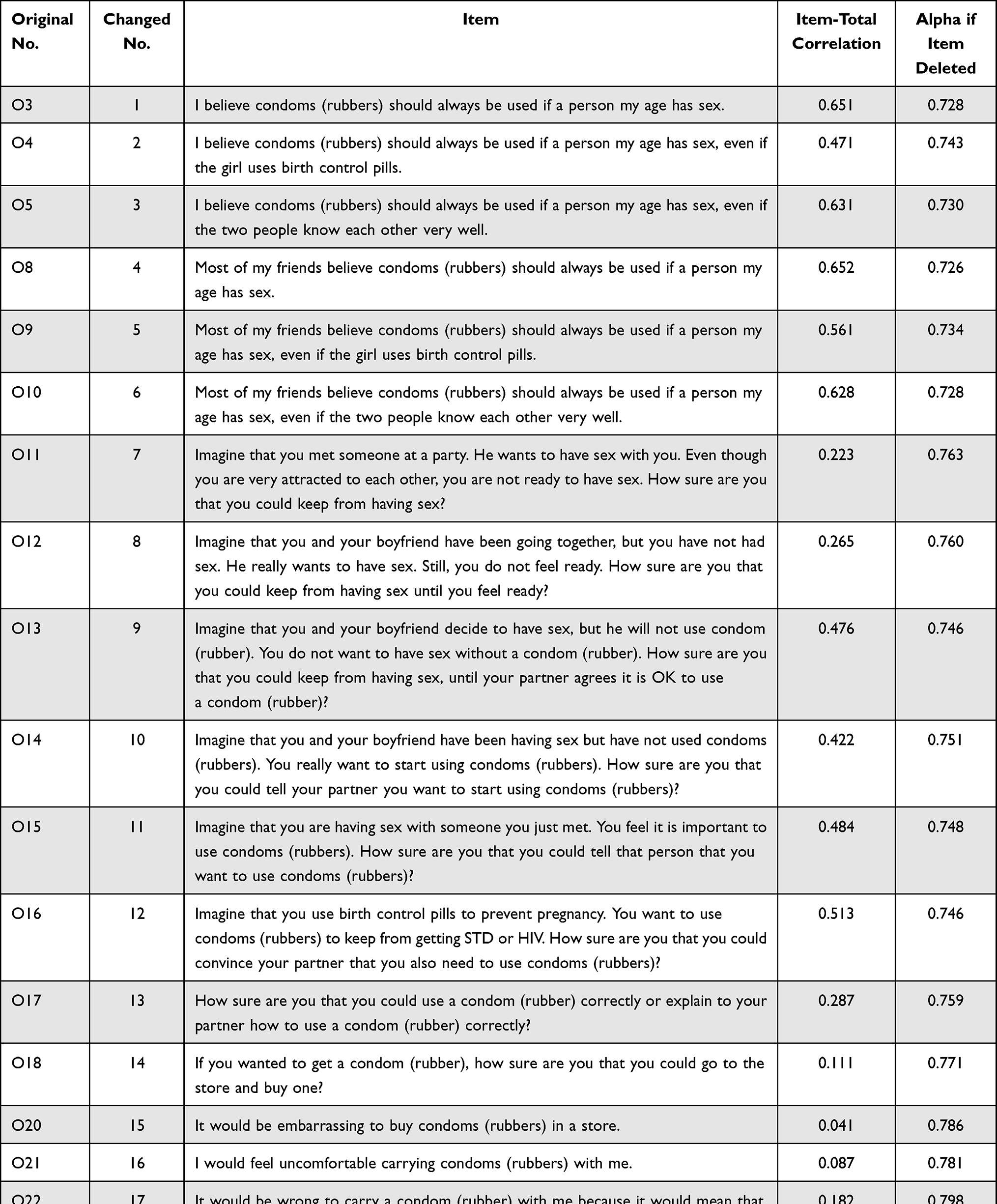 |
Table 1 Internal Consistency |
Construct Validity 2: EFA to Identify Hypothesized Components
EFA with Promax rotation was performed on the KR-SRBBS, and four factors were extracted, accounting for 63.797% of the variance of 17 items. The initial tool comprised 22 items, all of which were loaded onto at least one derived factor. We removed the items with factor loadings of < 0.30 (#O2, #O7, and #O19) and factors with only two items (#O1 and #O6). Subsequently, 17 items were included in the EFA. The KMO test result was 0.807, which was reasonably acceptable for factor analysis (the closer the value was to 1, the better the prospects for factor analysis, as values of 0.80 or higher were considered satisfactory). In addition, Bartlett’s test of sphericity was found to be statistically significant (χ2 = 1335.466, df = 136, p <0.001). This supports the factorability of the data. A sharp decline in the slope was observed in the screen plot. The final version of the KR-SRBBS produced four factors with a loading range of 0.374–0.870 (Table 2).
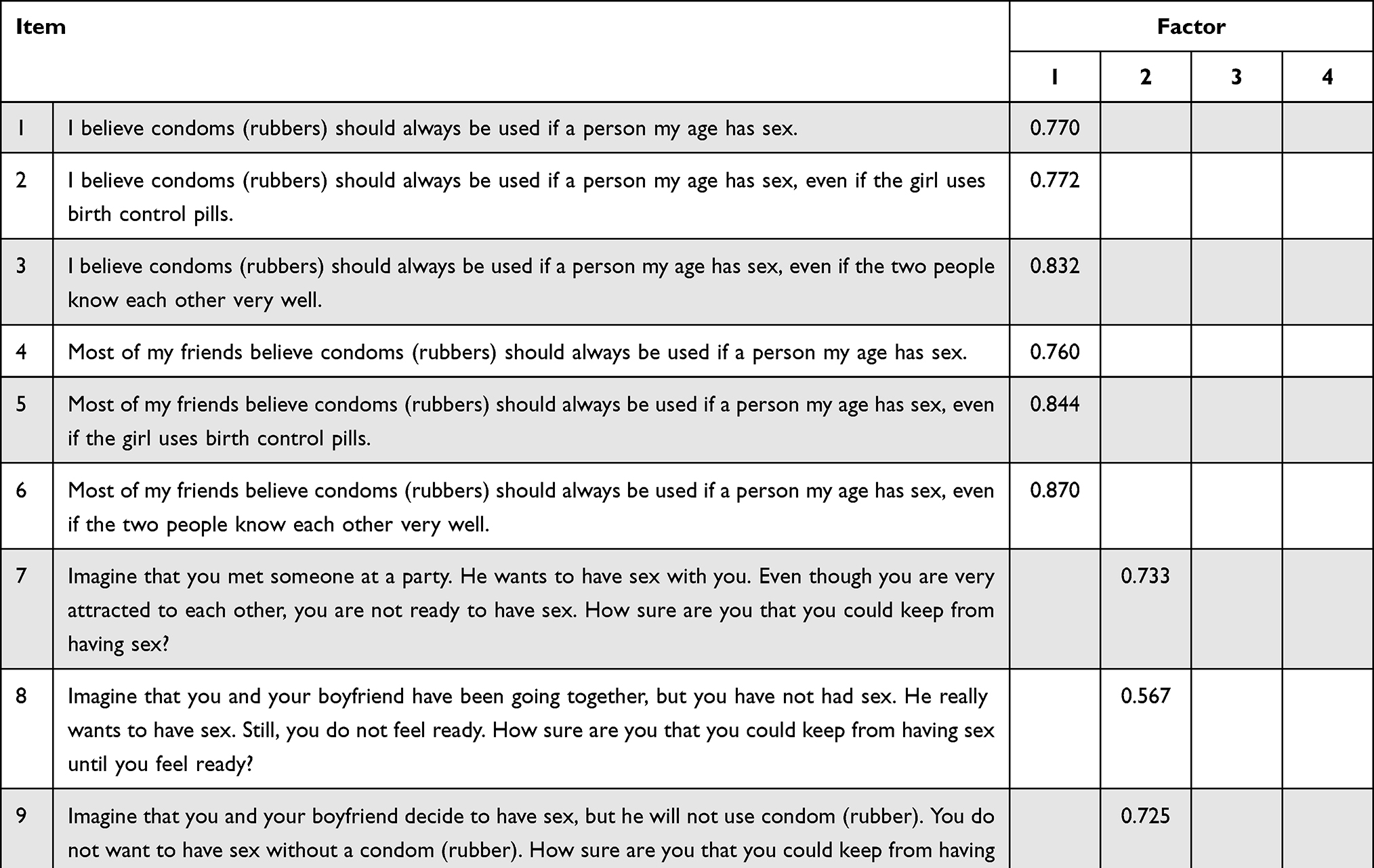 |
Table 2 Result of Exploratory Factor Analysis |
The first factor contained six items and was titled “behavioral and normative beliefs” (eigenvalue = 5.161; variance explained = 30.356%). The second factor, containing four items, was titled “control beliefs for refusing to have sexual relationships” (eigenvalue = 2.702; variance explained = 46.248%). The third factor, comprising four items, was labeled “control beliefs for communication and condom use” (eigenvalue = 1.856; variance explained = 57.166%). Finally, the fourth factor comprised three items and was titled “access difficulty” (eigenvalue = 1.127, variance explained = 63.797%) (Table 2).
Construct Validity 3: Appropriateness of CFA
The CFA model fit indices for the KR-SRBBS were χ2 = 325.162 (df = 113, p <0.001), CMIN/DF = 2.878, RMSEA = 0.106 (90% CI: 0.092–0.119), and CFI = 0.831 (Table 3). The goodness-of-fit test indicated that the model fits the data well. However, some indices were unsatisfactory (RMSEA and CFI), indicating that the current model requires some modification. Therefore, we reviewed the modification indices and reset the model to increase fit.
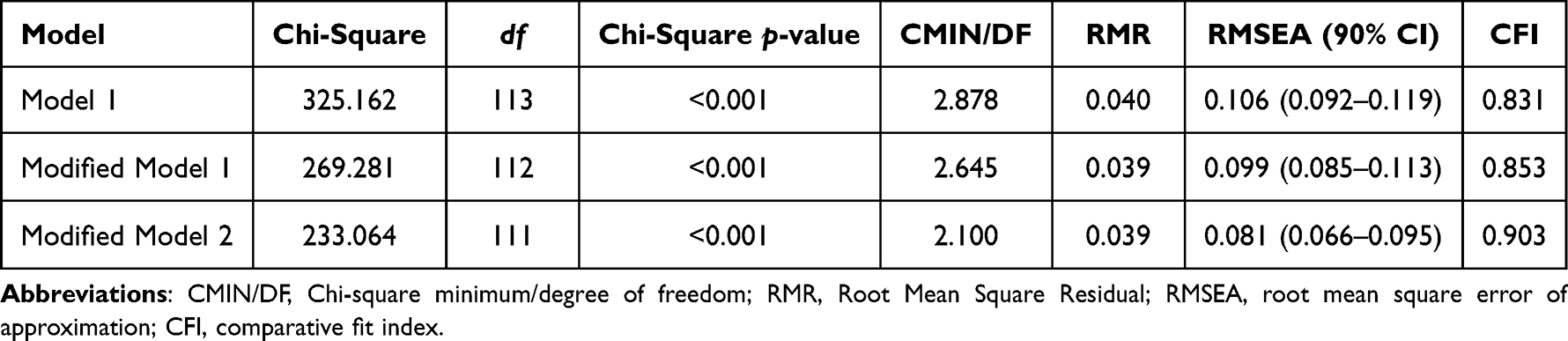 |
Table 3 Model’s Goodness of Fit |
We found that the best way to improve the fit was to define a correlation between error terms e2 and e5.26 After the modification, the statistics were analyzed again. The result showed that the model fit was slightly improved by dropping the RMSEA to <0.010. Moreover, the CFI should ideally be > 0.90 to be acceptable (Modified Model 1; Table 3), but it was 0.853. Therefore, another route was added (correlation between the error terms e1 and e3) to improve the model (Modified Model 2; Table 3) (Figure 2). This final modification yielded acceptable results,27 showing good model fit. The model indicated χ2 = 233.064 (df = 111, p <0.001), CMIN/DF = 2.100, RMSEA = 0.081 (90% CI: 0.066–0.095), and CFI = 0.903 (Table 3).
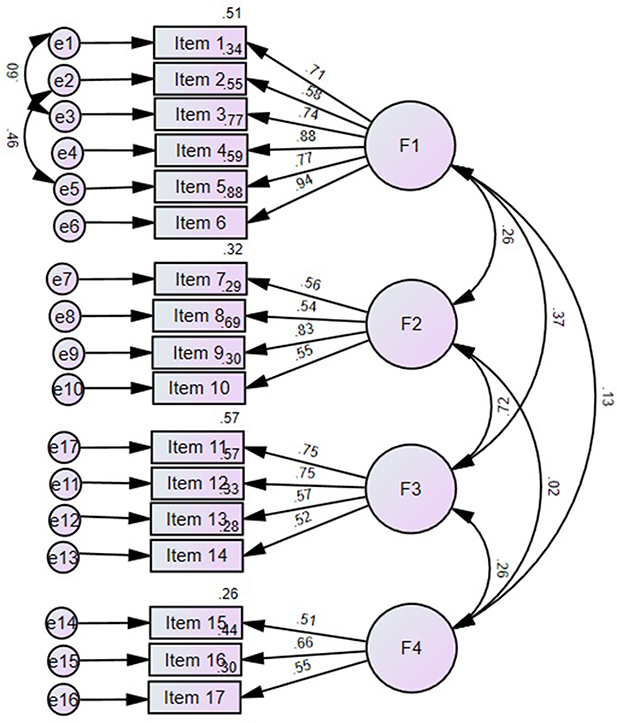 |
Figure 2 Reliability for KR-SRBBS. |
Convergent Validity
An AVE value ≥0.5 confirms the convergent validity. In this study, the AVE value of factors 1, 2, and 3 ranged from 0.67–0.76 (Table 4). Although the AVE value of factor 4 was 0.40, the CR value was higher than 0.6, indicating the convergent validity of the construct is still acceptable.28
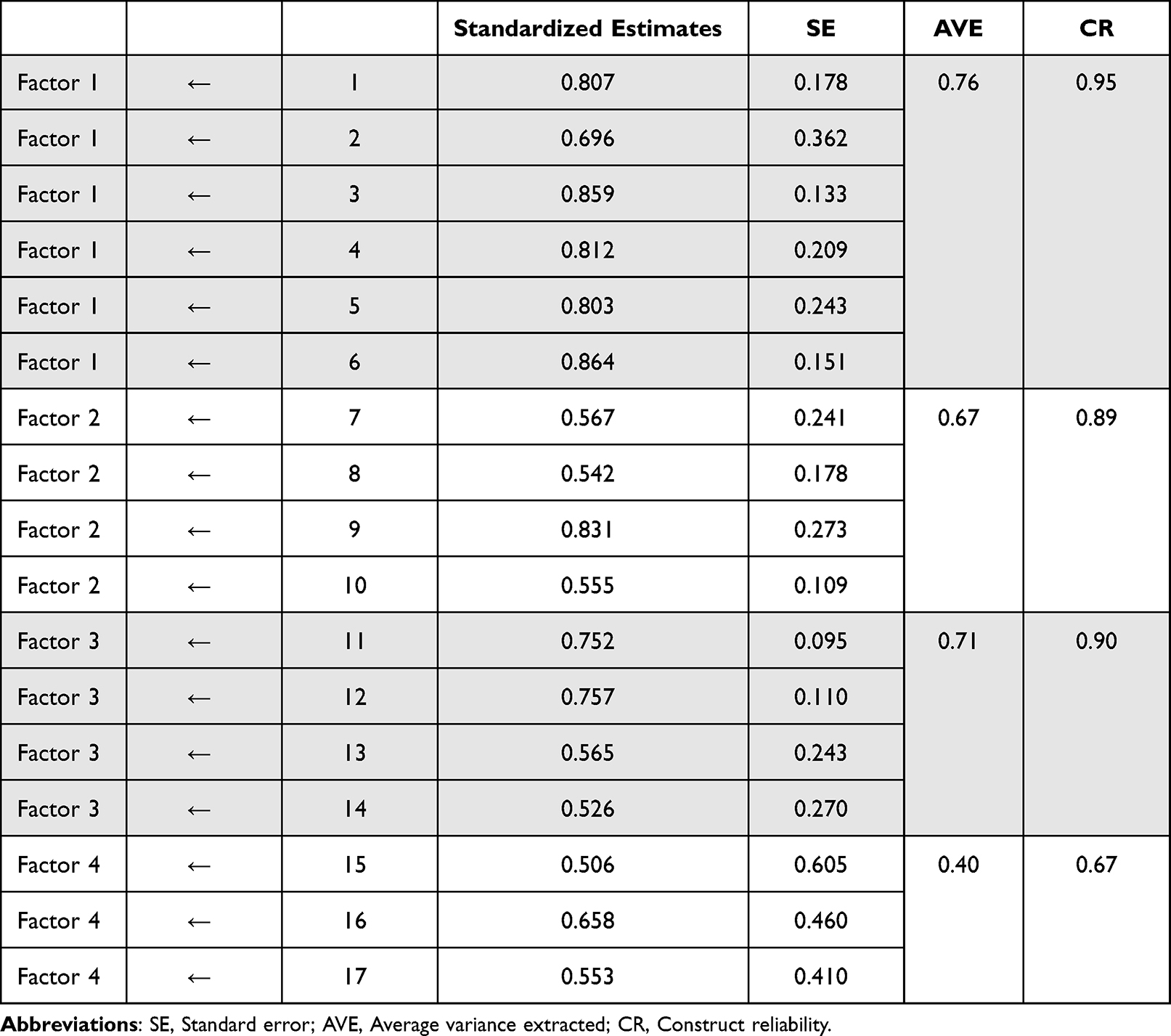 |
Table 4 AVE and CR Using CFA |
Reliability of the KR-SRBBS
Cronbach’s alpha was 0.77 for all 17 KR-SRBBS items. The reliability values were 0.91 for “behavioral and normative beliefs” (Factor 1), 0.71 for “control beliefs for refusing to have a sexual relationship” (Factor 2), 0.74 for “control beliefs for communication and condom use” (Factor 3), and 0.59 for “access difficulty” (Factor 4). These results have high to moderate reliability.29 Furthermore, CR was measured as an indicator of the shared variance among observed variables and latent constructs.28 Values more than 0.6 are considered to be adequate. In the present study, the CR values for all factors ranged from 0.67 to 0.95, within the acceptable range.
Discussion
This study determined the validity and reliability of the KR-SRBBS by assessing its content validity, construct validity, and reliability coefficients for the scale and its subscales.30 The content validity was established by conducting face validity using subject matter experts and determining the I-CVI. Construct validity was assessed through EFA and CFA. The overall reliability of the KR-SRBBS was evaluated using Cronbach’s alpha for the subscales and total scale.
Content validity is critical in determining whether the tool’s items adequately represent the domains the instrument measures.30 Ten Korean college students assessed the face validity of the KR-SRBBS. Face validity is not a true measure of validity, but it is crucial to ascertain how a potential participant understands the tool. The five subject matter experts are essential for judging the relevance and adequacy of the tool’s items. The I-CVI quantifies the extent of agreement of the five subject matter experts. It indicated that they unanimously agreed on the relevance of all items in the tool.
Construct validity evaluates the extent to which the items and domains are consistent with theoretical constructs defined in the tool.30 Using EFA and CFA enabled us to assess the construct validity of the KR-SRBBS.30,31 EFA is a data-driven statistical tool to determine the association of items and constructs in a tool. EFA enables hypotheses generation during the early phase of instrument development.32 On the other hand, CFA is a theory-driven, complex statistical approach for establishing construct validity.30
EFA resulted in a four-factor solution with 17 items. EFA simple structure guidelines were followed in determining the four KR-SRBBS factors. Each factor generated at least three items. Except for three items with a factor loading of <0.30, all other items have a factor loading of at least 0.40, satisfying the assumptions of using EFA. The KMO test and Bartlett’s test of sphericity were done31 to establish correlations and item sampling adequacy. Determining item correlations provides information about the factorability of the items. Items with low correlations indicate non-factorability. The item-to-total correlations, KMO, and Bartlett’s test demonstrated sufficient item factorability in the KR-SRBBS.
Furthermore, various model fit indices, such as Chi-square, CMIN/DF, RMSEA, and CFI, were used to determine whether CFA provided evidence of theoretical appropriateness of the tool. The initial model resulted in unsatisfactory fit indices (ie, RMSEA and CFI). This prompted two subsequent modifications to ensure model fit indices showed satisfactory acceptability.
The reliability of KR-SRBBS was established by determining Cronbach’s alpha of the four factors and subscales. This approach is suitable for establishing any instrument’s reliability because it assesses the tools’ multidimensionality.30 Ultimately, the reliability of each factor was ascertained. The reliability coefficient of Factor 4 was higher than the other factors. Despite this, it is a good start in measuring the reliability of KR-SRBBS since reliability testing does not involve a single measurement but continuous testing.30
Conclusions
The findings establish the KR-SRBBS as an assessment tool for measuring the intention to use condoms. The KR-SRBBS might then be used as an outcome measure to evaluate the impact of future interventions to reduce the spread of STDs and HIV. The KR-SRBBS has significant implications for nursing practice and research. In the absence of a Korean version to measure college students’ self-efficacy and intention to engage in high-risk sexual behaviors, the KR-SRBBS can be used to address this issue and reduce the spread of STDs and HIV. The tool can be used for youths in clinics, schools, or community settings to reduce their sexually risky behaviors. Establishing the psychometric properties of KR-SRBBS helps ensure the adaptability and relevance of the tool to the Korean adolescent population. This study is the first to adapt a tool of this nature from its original English version. We believe this psychometric research adds to the methodological studies that determined the appropriateness of an instrument for a target population. Further studies are required to assess the psychometric properties in terms of validity, reliability, and sensitivity for condom use intention among Korean college students.
Data Sharing Statement
The data that support the findings of this study are available from the first author on special request.
Acknowledgments
This study was conducted after additional research based on the doctoral thesis of the first author, Jungmin Lee.
Funding
This research was supported by Hallym University Research Fund, 2022 (HRF-202209-003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choi SH. Factors influencing sexual assertiveness of women university students in nursing. J Korean Acad Psychiatr Ment Health Nurs. 2016;25(4):367–374. doi:10.12934/jkpmhn.2016.25.4.367
2. Ritchwood TD, Ford H, DeCoster J, Sutton M, Lochman JE. Risky sexual behavior and substance use among adolescents: a meta-analysis. Child Youth Serv Rev. 2015;52:74–88. doi:10.1016/j.childyouth.2015.03.005
3. AVERT. Unprotected sex and HIV; 2013. Available from https://www.avert.org/hiv-transmission-prevention/unprotected-sex.
4. Khurana A, Cooksey EC. Examining the effect of maternal sexual communication and adolescents’ perceptions of maternal disapproval on adolescent risky sexual involvement. J Adolesc Health. 2012;51(6):557–565. doi:10.1016/j.jadohealth.2012.03.007
5. Kim NH, Park YJ, Jung HS. Relationships among sexual knowledge, attitude and sexual behavior that university students perceived. J Psychol Behav. 2015;7(2):17–42.
6. Idele P, Gillespie A, Porth T, et al. Epidemiology of HIV and AIDS among adolescents: current status, inequities, and data gaps. J Acquir Immune Defic Syndr. 2014;66(Supplement 2):s144–s153. doi:10.1097/QAI.0000000000000176
7. Vasilenko SA, Lanza ST. Predictors of multiple sexual partners from adolescence through young adulthood. J Adolesc Health. 2014;55(4):491–497. doi:10.1016/j.jadohealth.2013.12.025
8. Centers for Disease Control and Prevention. Prevention; January 21, 2016. Available from https://www.cdc.gov/std/prevention/default.htm.
9. Centers for Disease Control and Prevention. Reported cases of STDs on the rise in the U.S; November, 17, 2015. Available from https://www.cdc.gov/nchhstp/newsroom/2015/std-surveillance-report-press-release.html.
10. Kanda L, Mash R. Reasons for inconsistent condom use by young adults in Mahalapye, Botswana. Afr J Prim Health Care Fam Med. 2018;10(1):1–17. doi:10.4102/phcfm.v10i1.1492
11. Zhao Y, Wong CKH, Miu HYH, et al. Translation and validation of a Condom Self-Efficacy Scale (CSES) Chinese version. AIDS Educ Prevent. 2016;28(6):499–510. doi:10.1521/aeap.2016.28.6.499
12. Copen CE. Condom use during sexual intercourse among women and men aged 15–44 in the United States: 2011–2015 National Survey of Family Growth. National Health Statistics Reports; 2017. Available from: https://www.cdc.gov/nchs/data/nhsr/nhsr105.pdf.
13. Lee JY. Factors affecting contraceptive use among adolescent girls in South Korea. Child Health Nurs Res. 2017;23(3):259–267. doi:10.4094/chnr.2017.23.3.259
14. Park JJ, Seo YB, Jeong SK, Lee J. Prevalence of and risk factors for sexually transmitted infections among Korean adolescents under probation. J Korean Med Sci. 2017;32(11):1771–1778. doi:10.3346/jkms.2017.32.11.1771
15. Kim MJ, Lim ES, Park SS, Choi NK. Factors associated with Human Papillomavirus non-vaccination: the national health and nutrition survey. J Health Inf Stat. 2021;46(1):72–81. doi:10.21032/jhis.2021.46.1.72
16. Shin HW, Lee JM, Min HY. An integrative literature review on sex education programs for Korean college students. J Korean Acad Soc Nurs Educ. 2020;26(1):78–96. doi:10.5977/jkasne.2020.26.1.78
17. Lee JM, Kim YJ. Translation and psychometric evaluation of the female sexual resourcefulness scale in South Korea. Psychol Res Behav Manag. 2022;15:2357–2368. doi:10.2147/PRBM.S378841
18. Fisher TD, Davis CM, Yarber WL. Handbook of Sexuality-Related Measures. Routledge; 2013:588.
19. Ramiro L, Reis M, de Matos MG, Diniz JA. Trends in adolescent sexual behavior, impact of information, and attitudes about HIV/AIDS in Portugal. Psychol Health Med. 2014;19(5):614–624. doi:10.1080/13548506.2013.845299
20. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
21. Faul F, Erdfelder E, Buchner A. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
22. Basen-Engquist K, Masse LC, Coyle K, et al. Validity of scales measuring the psychosocial determinants of HIV/STD-related risk behavior in adolescents. Health Educ Res. 1999;14(1):25–38. doi:10.1093/her/14.1.25
23. Unis B, Johansson I, Sällström C. Rural high school students’ sexual behavior and self-esteem. Open J Nurs. 2015;05(01):24–35. doi:10.4236/ojn.2015.51004
24. World Health Organization Process of translation and adaptation of instruments; n.d.. Available from: http://www.who.int/substance_abuse/research_tools/translation/en/index.html.
25. World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053.
26. Smolkowski K. Correlated errors in CFA and SEM models. Unpublished manuscript; 2007. Available from http://www.ori.org/~keiths/Files/Tips/Stats_SEMErrorCorrs.html.
27. Hooper D, Coughlan J, Mullen MR. Structural equation modelling: guidelines for determining model fit. Electron J Bus Res Methods. 2008;6(1):53–60.
28. Shrestha N. Factor analysis as a tool for survey analysis. Am J Appl Math Stat. 2021;9(1):4–11. doi:10.12691/ajams-9-1-2
29. Nunnally JC, Bernstein IR. Psychometric Theory.
30. Waltz CF, Strickland OL, Lenz ER, Eds. Measurement in Nursing and Health Research.
31. Polit DF. Statistics and Data Analysis for Nursing Research.
32. Tabachnick BG, Fidell LS. Using Multivariate Statistics.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.