")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Psychological status of nursing survivors in China and its associated factors: 6 years after the 2008 Sichuan earthquake
Authors Liao J, Ma X, Gao B, Zhang M, Zhang Y, Liu M, Li X
Received 2 February 2019
Accepted for publication 3 July 2019
Published 14 August 2019 Volume 2019:15 Pages 2301—2311
DOI https://doi.org/10.2147/NDT.S203909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Jingping Liao,1,2 Xiaofang Ma,1,3 Bin Gao,4 Mingfeng Zhang,5 Yuanfang Zhang,6 Maoqun Liu,7 Xiaolin Li1
1Department of Nursing, West China Hospital, West China School of Medicine, Sichuan University, Chengdu 610041, People’s Republic of China; 2School of Nursing, Peking University, Beijing 100191, People’s Republic of China; 3Department of Emergency, West China Hospital, Sichuan University, Chengdu 610041, People’s Republic of China; 4Department of Nursing, Dujiangyan Medical Center, Dujiangyan 611830, People’s Republic of China; 5Department of Nursing, People’s Hospital of Mianzhu City, Deyang 618200, People’s Republic of China; 6Department of Nursing, Wenchuan People’s Hospital, Aba Tibetan and Qiang Autonomous Prefecture 623000, People’s Republic of China; 7Department of Nursing, Dujiangyan Second People’s Hospital, Dujiangyan 611830, People’s Republic of China
Purpose: Nursing survivors are often not only the victims but also the rescuers in a disaster. Severe natural disasters can cause them long-term psychological impact. This study aimed to investigate the psychological status of nursing survivors and its associated factors 6 years after the severe earthquake that occurred in Wenchuan, Sichuan, on May 12, 2008.
Methods: The study used a cross-sectional design. A total of 597 nurses who survived the earthquake and took care of victims were recruited about 6 years after the disaster. They completed a self-report questionnaire assessing information about demographics, earthquake-related characteristics, psychological status, posttraumatic stress disorder, and posttraumatic growth and resilience.
Results: The mean score on the Symptom Checklist-90-Revised (SCL-90-R) was (123.56±41.26). Of symptoms indicated by the SCL-90-R, obsessive-compulsive dimension had the highest score (1.62±0.62). The psychological status of nursing survivors differed with the title, monthly per capita household income, financial loss, health status, residential satisfaction, and satisfaction with leaders and colleagues. Severe financial loss and poor health status were significant factors of psychological distress. In addition, psychological status was negatively related to posttraumatic stress disorder and posttraumatic growth, and positively related to resilience.
Conclusion: Nursing survivors had a relatively normal level of psychological status 6 years after the 2008 Sichuan earthquake. However, psychological symptoms such as obsessive-compulsive patterns still remained. Interventions focusing on the improvement of financial subsidies and physical health may be particularly useful in reducing psychological problems after the disaster.
Keywords: natural disaster, posttraumatic growth, resilience, rescue, mental health, disaster response
Introduction
The Sichuan earthquake, which occurred on May 12, 2008, struck Wenchuan, Beichuan, and Qingchuan counties, located in the northwestern part of the Sichuan Province of China.1 It was one of the most severe natural disasters in China, registering 8.0 on the Richter Scale, with damaged regions exceeding 100,000 km.1 It was estimated that at least 69,229 people lost their lives, 374,643 were injured, 17,923 were missing, 4.8 million were homeless, and 46 million were affected in this disaster.1
Severe natural disasters could cause the survivors both short-2,3 and long-term3,4 psychological impact. In the short term, disasters have been found to be associated with increased prevalence of psychiatric disorders5 such as posttraumatic stress disorder (PTSD),6,7 anxiety,7 depression,7 somatic complaints,8 and sleep disorder.9 With regard to the long-term sequelae, previous reports suggested that: 1) the general rule was that symptoms declined with time;10 2) post-disaster psychological recovery might be related to positive factors, such as posttraumatic growth (PTG) and resilience;11–13 3) there might be a latency period or delayed onset of some symptoms;14 and 4) significant psychiatric symptomatology might persist for as long as 14 years.14,15 However, previous studies have focused mainly on single and specific psychiatric disorders among survivors rather than their general psychological status. Besides, PTSD, the frequently reported pathological response to disasters, and its relationship with positive responses (ie, PTG and resilience) has been demonstrated in previous studies.11–13,16 Unfortunately, to our best knowledge, there were limited data on the relationship of overall psychological status with PTSD, PTG, and resilience after an earthquake. In other words, the impact of PTSD, PTG, and resilience on overall psychological status of survivors remains unknown.
There are many variables associated with post-earthquake psychological problems. Some demographic variables are reported as risk factors for earthquake-related psychopathology including being women;2 having low educational level,4 health complaints,2 and financial strain;2,17 and being from developing countries.10 Other commonly reported risk factors for earthquake-related psychopathology include the level of exposure to earthquake, such as exposure to actual or threatened injury during the earthquake,18 proximity to the epicenter,19 death of or severe injury to family members,20 serious destruction of property/home,6,21 material and psychological support,6 and social support.17
As a special group of survivors, nurses were not only the victims but also the rescuers in the disaster. As victims, they suffered from the loss of their families/friends and destruction of property/home.22 As rescuers, they played critical roles in disaster relief after the earthquake,23 often working in the front line of care. While rescuing victims, they were frequently exposed to terrifying scenes of deceased or severely wounded people, mass destruction, and frequent aftershocks. These stresses might place them at a risk for psychological distress. For instance, a study showed that 11% of rescuers exhibited general psychiatric morbidity and 21.4% exhibited posttraumatic morbidity after an earthquake in Taiwan.24 Another study reported that of rescuers who responded to the terrorist attack of September 11, 2001, in New York, 16.7% exhibited PTSD and 21.7% exhibited depression at 13 months.25 As both victims and rescuers, prevalence rates of psychological disturbances of the nurses who survived the 2008 Sichuan Earthquake might be much higher than those of the other groups. Besides, these nurses had other characteristics, including most of them being female, with relatively low educational levels compared to doctors, from a developing country and its impoverished areas (Western China).22,26 As mentioned, previous studies have indicated that having low educational level and being from developing countries might be significantly associated with psychological problems.2,10 Thus, the post-disaster psychological status of nursing survivors should be explored further.
In addition, exploration of long-term perspectives on psychological status of nursing survivors remains limited. Therefore, using a cross-sectional survey, this study aimed to investigate the psychological status of nursing survivors 6 year after the 2008 Sichuan earthquake, and the associated factors of the psychological status, and analyze the relationship between psychological status, PTSD, PTG, and resilience.
Materials and methods
Design and participants
A cross-sectional study was conducted in Southwest China. Seven hospitals (Dujiangyan Medical Center, Dujiangyan Second People’s Hospital, People’s Hospital of Mianzhu city, Wenchuan People’s Hospital, Wenchuan Traditional Chinese Medicine hospital, Yingxiu Community Hospital, Shuimo Community Hospital) in three cities (Dujiangyan, Mianzu, and Wenchuan county) were selected from the areas that were affected the most in the 2008 Sichuan earthquake.27 All assessments were completed 6 years after the earthquake (between December 2014 and March 2015). All participants were enrolled through convenience sampling. The inclusion criteria were: (1) the nurses with registered nurse licenses; (2) the nurses who personally experienced the 2008 Sichuan earthquake; (3) being involved in the rescue work of the 2008 Sichuan earthquake. Participants were excluded if they did not want to participate in the study. Ultimately, 694 eligible nurses were invited to participate and 597 of them agreed.
Data collection
The data for the research were collected by 14 graduate students from the department of nursing at Sichuan University. These students were divided into seven teams, each of which was responsible for data collection in one hospital. They participated in a five-day training program offered by psychologists, statisticians, and psychiatrists from the West China School of Medicine, Sichuan University. Prior to the formal survey, preliminary pilot evaluations were conducted in two hospitals to test the original questionnaire, and then adjustments were made to adapt to the local conditions.
From December 2014 to March 2015, the trained teams were assigned to the hospitals according to a previously arranged schedule. Nurses who met the inclusion criteria were selected through face-to-face interviews. First, the investigators explained the purpose and main content of the survey. After obtaining informed consent from eligible participants, the investigators explained to the respondents how to complete the questionnaires. Then the respondents were asked to complete the questionnaires independently and according to their actual conditions and feelings. No respondent was found to have an extremely low level of education or literacy problem, but the investigators still assisted them in completing the survey if necessary. Finally, the investigators collected the questionnaires immediately after their completion to check the integrity of the data.
Ethical considerations
The study received approval from the Ethics Committee of West China Hospital of Sichuan University. The investigation complied with the principle of voluntariness, and written informed consent was obtained from all participants. The consent forms and the completed questionnaires were separated, and data were treated confidentially.
Measures
Basic information
Basic information was obtained through a questionnaire consisting of demographic and earthquake-related characteristics. Demographic variables included age, sex, title, marital status, ethnicity, religious belief, educational level, and monthly per capita household income (MPCHI). Earthquake-related characteristics included physical injury, death of family member(s), financial loss, duration of rescue of victims, health status, residential satisfaction, psychological support, satisfaction with social support systems, and satisfaction with support from family members, leaders and colleagues, and friends and relatives.
Symptom checklist-90-revised
The Symptom Checklist-90-Revised (SCL-90-R)28 is a self-report symptom inventory used to measure psychological distress and psychological symptoms. It consists of 90 items across nine primary symptom domains: (a) somatization, (b) obsessive-compulsive, (c) interpersonal sensitivity, (d) depression, (e) anxiety, (f) hostility, (g) phobic anxiety, (h) paranoid ideation, and (i) psychoticism. Participants respond to it on a five-point scale ranging from 0 (“asymptomatic”) to 4 (“very severe”). Scores higher than two indicate psychopathology. A total score of over 160 is a possible indication of mental health problems.29 The Chinese version of the SCL-90-R has high reliability and validity and can be used to measure psychological distress and psychological symptoms in the Chinese population.29,30 The Cronbach’s alpha in the current study was 0.984. The internal reliabilities for the nine subscales were 0.923, 0.895, 0.876, 0.908, 0.874, 0.847, 0.848, 0.829, and 0.886, respectively.
PTSD check list-civilian version
PTSD symptoms were assessed using the PTSD Check List-Civilian Version (PCL-C),31 with 17 items corresponding to the symptoms discussed in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), PTSD criteria B, C, and D. The response options for each item on the PCL-C were recorded on a five-point Likert scale ranging from 1 (not at all) to 5 (extremely). Higher scores indicate severer PTSD symptoms. A score of 50 or higher was considered indicate PTSD symptoms. The scale has been widely used to assess PTSD symptoms among college students,32 survivors of road traffic accidents,33 and adolescents who survived an earthquake,6,34,35 with excellent reliability and validity in China. In this study, the Cronbach’s alpha value for this scale was 0.945.
PTG inventory
PTG was assessed using the PTG Inventory (PTGI).36 The PTGI comprises 21 items in five major domains: (a) relating to others; (b) new possibilities; (c) personal strength; (d) spiritual change; and (e) appreciation of life. Participants responded on a five-point Likert scale ranging from 0 (no change) to 4 (complete change). Higher scores indicate greater PTG. According to Yu Xiaonan,37 total scores above the 60th percentile were considered to have probable PTG. The Chinese version of the PTGI has high reliability and validity and can be used to measure PTG in the Chinese population.38 In this study, the Cronbach’s alpha value for this scale was 0.965.
Connor-davidson resilience scale
Resilience was assessed using the Connor-Davidson Resilience Scale (CD-RISC).39 This inventory consists of 25 items across five resilience domains: (a) personal competence, high standards, and tenacity; (b) trust in one’s instincts, tolerance of negative affect, and strengthening effects of stress; (c) positive acceptance of change and secure relationships; (d) control; and (e) spiritual influences. Each item is rated on a five-point Likert-type scale ranging from 0 (not true at all) to 4 (true nearly all of the time).39 Total scores on the CD-RISC range from 0 to 100, with higher scores corresponding to greater resilience.39 Previous studies have demonstrated that this scale has good reliability and validity for use with Chinese adults.40 In this study, the Cronbach’s alpha value for this scale was 0.969.
Statistical analysis
Continuous variables were described using means and standard deviations, and categorical variables were described using frequencies and percentages. In univariate analysis, independent sample t-test and one-way analysis of variance were used to analyze the relationship between demographic, earthquake-related variables, and psychological status in nursing survivors. Multivariate analysis was conducted using multiple linear regression analysis to explore the factors associated with psychological status. Pearson’s correlation analysis was used to examine the relationships between PTSD, PTG, resilience, and psychological status. A two-tailed P-value <0.05 was considered statistically significant. Analyses were performed using SPSS Inc., Chicago, IL, USA version 21.0.
Results
Participant characteristics
Of the 597 respondents in the study, 1.0% were male and 99.0% were female participants. Their age ranged from 26 to 55 years with an average of 37.95 years (SD=8.46).
The majority of the respondents were married (87.9%). The Han ethnic group accounted for the majority (90.8%), and the Qiang ethnic group were somewhat fewer in number than the Han (5.5%), but higher than other ethnic minorities in the survey. Overall, 72.6% respondents had a relatively low educational level, and 83.2% had a monthly income of $150–800. These demographic characteristics are presented in Table 1.
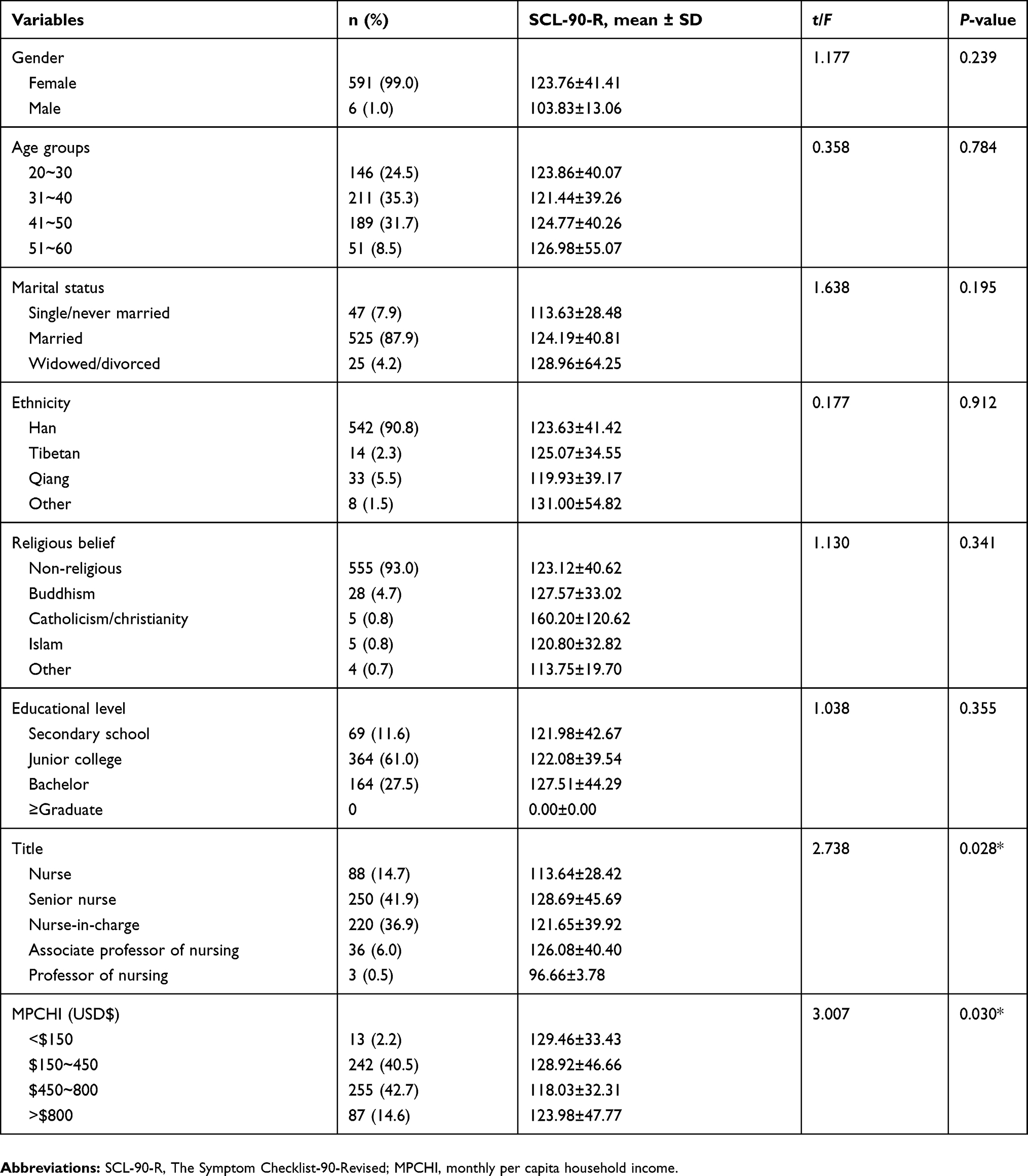 |
Table 1 The demographic characteristics of the participants(n=597) |
Concerning the earthquake, 110 nurses (18.4%) were injured in the disaster. Thirty-eight nurses (6.4%) lost their family member(s). Five hundred and thirty-six respondents (89.8%) experienced financial loss in the earthquake. After the earthquake, all of them participated in the relief work and most (80.7%) rescued victims for over 3 weeks. Four hundred and three nurses (32.5%) received some kind of psychological support. Most nurses were satisfied with social support systems (60.8%), family members (86.6%), leaders and colleagues (59.1%), and friends and relatives (74.2%). Earthquake-related characteristics are described in Table 2.
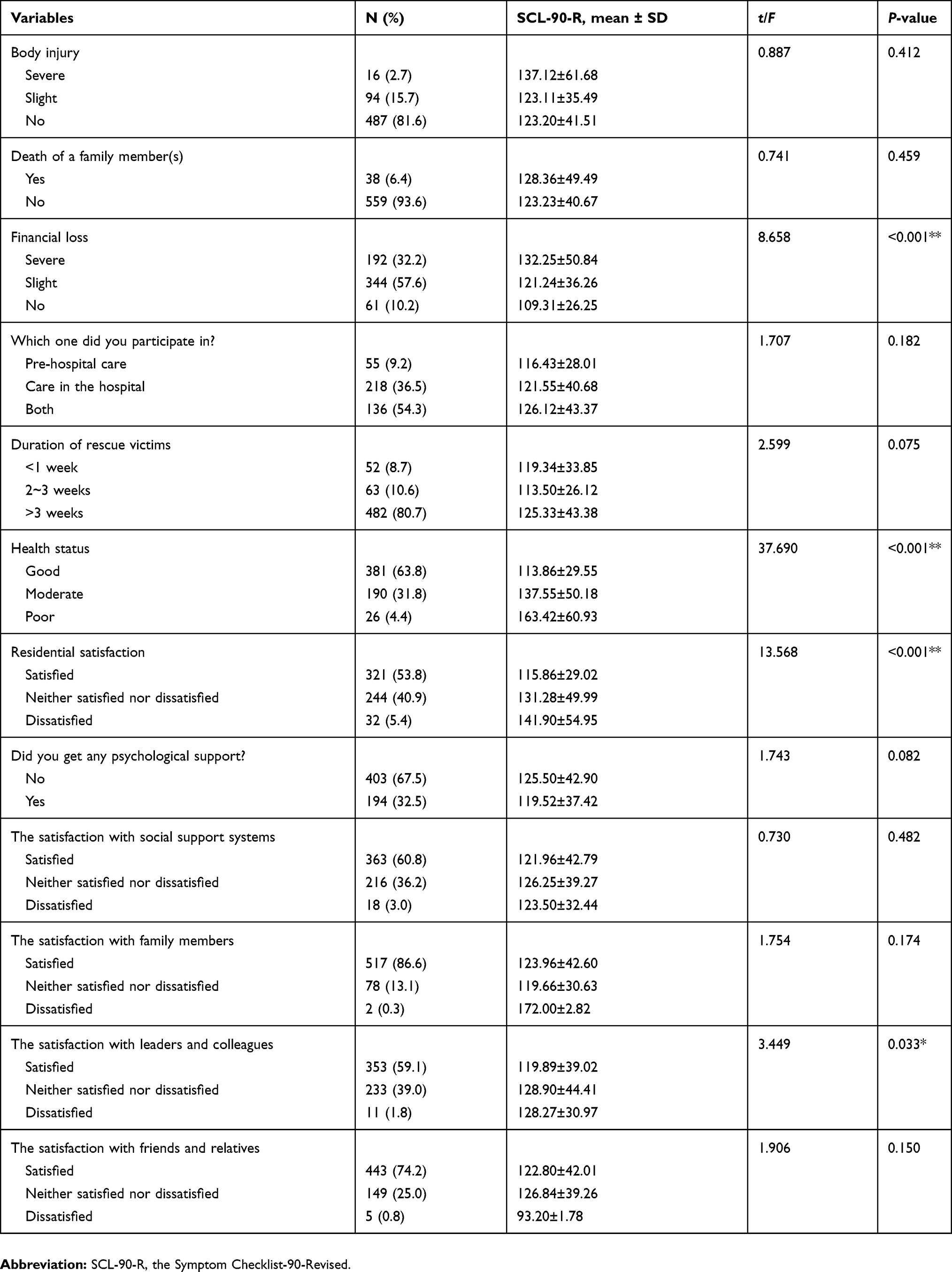 |
Table 2 The basic characteristics of the participants about the earthquake (n=597) |
Psychological status, PTSD, PTG, and resilience in nursing survivors
The mean scores on psychological status (SCL-90-R), PTSD (PCL-C), PTG (PTGI), and resilience (CD-RISC) were 123.56 (SD=41.26), 24.76 (SD=9.46), 43.71 (SD=23.81), and 57.57 (SD=21.13), respectively. For the entire sample, the mean scores on SCL-90-R, PCL-C, and PTGI were relatively low compared to the cutoff point, while the mean score on CD-RISC was higher than the moderate level. These scores indicated that the nurses had a relatively low level of psychological stress, mild PTSD, low PTG, and good resilience. Concerning SCL-90-R, the highest score among the dimensions was on obsessive-compulsive, and the lowest on psychoticism. Five items with the highest scores were trouble remembering things (obsessive-compulsive), feeling easily annoyed and irritated (hostility), feeling low in energy or slowed down (depression), trouble falling sleep (additional scales), and having to check and double check what you do (obsessive-compulsive). Five items with the lowest scores were feelings of guilt (additional scales), hearing voices that other people do not hear (paranoid ideation), thoughts of ending your life (depression), trembling (anxiety), hearing voices that other people do not hear (psychoticism). Further details are described in Tables 3 and 4.
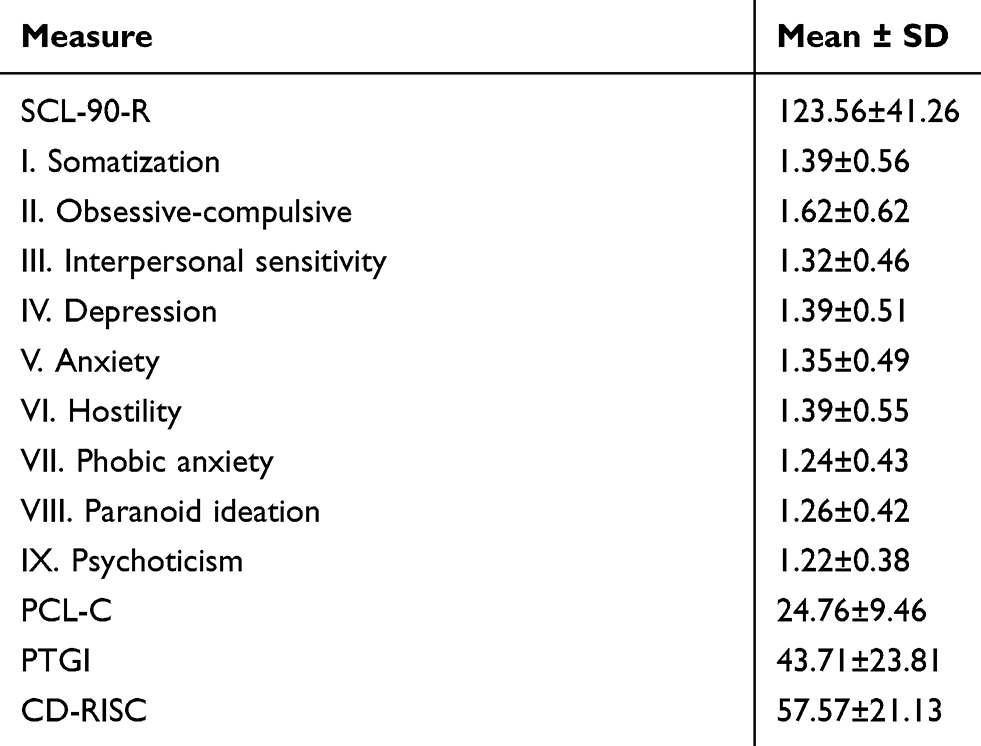 |
Table 3 Scores on psychological status, PTSD, PTG and resilience among nursing survivors 6 years after 2008 Sichuan Earthquake in south-west China (n=597) |
 |
Table 4 Five items with the highest and the lowest scores on the SCL-90-R (n=597) |
The relationships of demographic characteristics with earthquake-related variables and psychological status
In the univariate analysis, the results showed that the psychological status of nursing survivors differed with regard to title (P=0.028), MPCHI (P=0.030), financial loss (P<0.001), health status (P<0.001), residential satisfaction (P<0.001), and satisfaction with leaders and colleagues (P=0.033) (Tables 1 and 2).
As shown in Table 5, the results of multivariate regression analyses showed that relatively less financial loss and better health status after the earthquake were significantly related to better psychological status (b=−0.116, P<0.001; b =0.285, P<0.001). These variables could explain 13.7% of the variance. However, there was no significant association between psychological status and the other variables, including title, MPCHI, residential satisfaction, and satisfaction with leaders and colleagues.
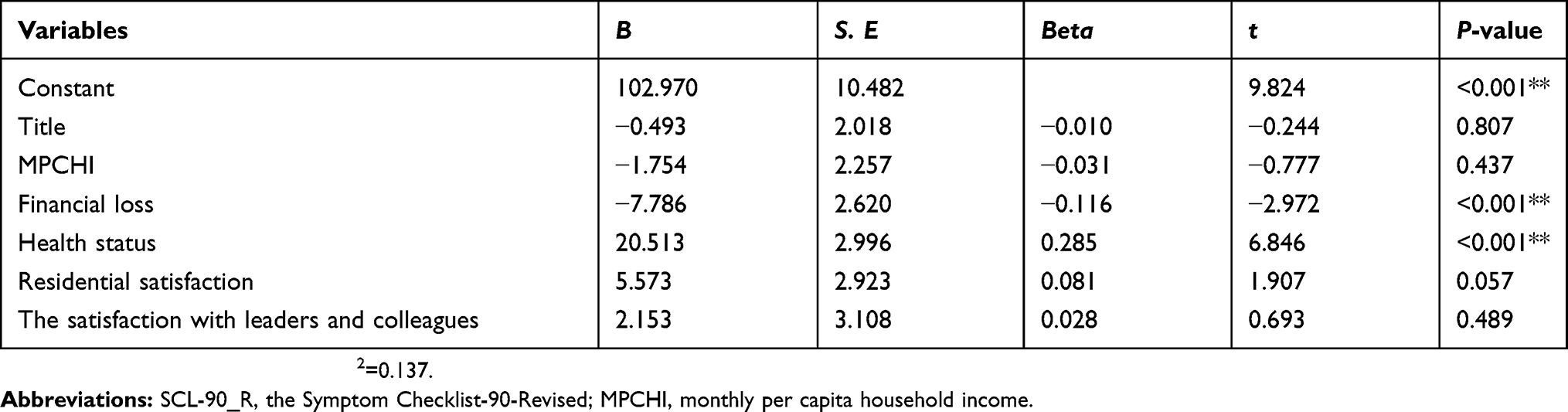 |
Table 5 A multiple regression analysis in SCL-90-R (N=597) |
Analysis of correlation between psychological status, PTSD, PTG, and resilience
As shown in Table 6, better psychological status was significantly related to mild PTSD (r=0.765, P<0.001), less PTG (r=0.092, P=0.025), and more resilience (r=−0.171, P<0.001).
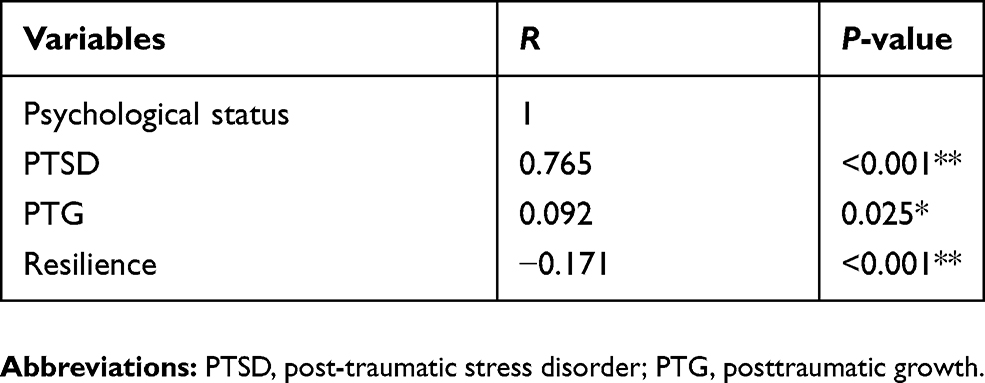 |
Table 6 The analysis of correlation between psychological status, post-traumatic stress disorder, posttraumatic growth and resilience |
Discussion
The findings of this six-year follow-up study of the 2008 Sichuan earthquake highlight the long-term impact of a major disaster on the nursing survivors. In our study, the mean score of SCL-90-R was 123.56±41.26, which demonstrated that our nurses had a relative normal psychological status. This finding was similar to an online survey41 among Dutch survivors of the 2004 Asian tsunami, which concluded that there was a trend towards recovery over 4 years. Our finding was also consistent with those previous studies10 that showed that psychological symptoms would decline consistently over time. The reason might be explained by the relatively low levels of PTSD and PTG and high level of resilience among our nursing survivors. Resilience is associated with the ability and competence of an individual to rebound after a disruption.42 It refers to the “bouncing back” or positive adaptation of individuals following an experience of trauma or stress.43,44 High level of resilience could help nursing survivors reduce their PTSD and enhance PTG,11 and help their psychological status recover to a relatively normal level. As a result, most of survivors would recover in the long run.10
However, our participants still showed several psychological symptoms even 6 years after the earthquake. Of symptoms indicated by the SCL-90-R, the highest score was found on the obsessive-compulsive dimension (1.62±0.62), indicating that it was the most prominent symptom in these survivors. This is in line with a previous study45 conducted with female middle-school students from post-earthquake Wenchuan, which showed that obsessive-compulsive traits were the most prevalent. More specifically, obsessive-compulsive symptoms mainly manifested in trouble remembering things and having to check and double check. Besides, being easily annoyed, having low energy, and insomnia were also prominent problems among nursing survivors. There were several possible reasons to explain why these symptoms still existed. The first one might be that the earthquake still impacted victims. Some symptoms including obsessive-compulsive and insomnia were reported among disaster survivors in previous studies.9,45 The second reason might be that nursing staff, as rescuers in the disaster, suffered from vicarious trauma. When rescuers, owing to professional duty, took care of traumatized victims or those who were in physical or psychological distress, they could develop the same emotive experiences, therefore indirectly becoming victims.46 Symptoms of vicarious trauma included insomnia, being easily annoyed, having low energy, and memory problems.47 These were consistent with the symptoms reported by our participants. The third reason might be explained by the nature of nursing work. Symptoms prevalent among our nurses were also commonly reported among other Chinese nurses.48 Due to shift work and heavy workload, nurses easily reported mental health problems such as insomnia, having low energy, being easily annoyed, and trouble remembering things.48–50 Additionally, because of the high requirements of nursing work, some nurses developed the habit of checking and rechecking, which annoyed them very much.48 It was hard to distinguish whether these symptoms were caused by the earthquake, nature of nursing work, or both. Therefore, this question needs to be further clarified in the future.
Our analysis showed that, for nursing survivors, less financial loss was associated with better psychological status. Previous studies17,51 have suggested that financial strain was a strong risk factor for survivors’ mental health post-disaster. However, in our study, we stressed more on the impact of financial loss in the earthquake. As far as we know, a severe earthquake can destroy almost all the survivors’ properties, including their houses. Moreover, the areas affected the worst in the 2008 Sichuan earthquake were located in the northwest of Sichuan Province, China. They were among the most underdeveloped in China. The residents were very poor. In this survey, most participants’ MPCHI ranged from $150–800. Severe financial loss and low income might result in inability to recover from the financial problems within a short time. Extreme and widespread damage to property would cause a long-term financial strain after the earthquake. It could affect survivors’ psychological status even 6 years after the big disaster. This indicates that ample financial support from the government and society should be provided to nursing survivors not just in the short term but also in the long run.
In addition, we observed that better physical health status was associated with better psychological health status. It was reported that, 5 months after the 2004 Japan earthquake, survivors with physical illnesses were more likely to experience psychological distress than those without, which is consistent with the results of our study.52 Because of the nature of nursing work, physical health problems prevail among nurses.53 Current physical health could impact their psychological status. Our study showed that 4.4% participants reported very poor physical health status. It would be a long-term stressor for them. Actions such as periodic physical examinations and timely treatment should be undertaken to improve nursing survivors’ physical health.
In our study, we also investigated the relationships between psychological status, PTSD, PTG, and resilience among nursing survivors after a severe earthquake. Previous studies have demonstrated the relationships between PTSD, PTG, and resilience among refugees,16 students,11 survivors of motor vehicle accident,12 ex-prisoners of war, and combat veterans.13 However, our study was the first to use the SCL-90-R as the measure to demonstrate the relationship of overall psychological status with PTSD, PTG, and resilience among nursing survivors. Our study showed that psychological status was negatively (and strongly) related to PTSD, negatively (but weakly) related to PTG, and positively (but weakly) related to resilience. In other words, better psychological status might be significantly related to low level of PTSD (strongly), low PTG (weakly), and high resilience (weakly). This is consistent with the findings of studies that demonstrated that PTSD was positively related to PTG,54 negatively to resilience,11 and that their correlations are not strong.11,54 However, this is inconsistent with the results of the studies that showed that PTSD was negatively,13 or curvilinearly55 related to PTG. Our findings support the notion11 that growth may be integral to trauma by helping the individual cope effectively with trauma exposure. Namely, growth may stem from trauma. However, it should be noted that the degree of correlation of psychological status with PTG and resilience is very weak. Given the uncertainty in previous studies, such relationships in this population should be further clarified in the future.
Our study had several limitations. First, it was a cross-sectional survey. With such a design, the limitation is that it is difficult to achieve a longitudinal understanding of the situation before and immediately after the earthquake. It allowed only for an examination of the correlation, not the causation. Second, we do not know the effect of other factors such as life events on the current symptoms. Third, the data were collected using a self-report and not a clinical interview, which might not reflect the true psychological status. Finally, psychological problems are considered to be unacceptable by the Chinese society. Though we promised the confidentiality of the results repeatedly to the participants, it might have been hard for them to disclose their symptoms. This might have resulted in underestimation of the positive rates.
Conclusion
Despite its limitations, this study showed the long-term impact of an earthquake on the nursing survivors. In general, nursing survivors had a relatively normal psychological status 6 years after the 2008 Sichuan earthquake. However, several psychological symptoms such as obsessive-compulsive persisted even 6 years after the earthquake. Besides, severe financial loss and poor health status after the earthquake were found to be associated factors of psychological symptoms. Furthermore, better psychological status was significantly related to mild PTSD, less PTG, and more resilience. There is an urgent need to develop strategies to decrease nursing survivors’ psychological symptoms and help them improve their psychological status after an earthquake. It is highly recommended that governments and social institutions pay more attention to the improvement of financial subsidies to and physical health of the nurses exposed to major disasters.
Abbreviations
PTG, posttraumatic growth; PTSD, posttraumatic stress disorder; SCL-90-R, symptom checklist-90-revised; PCL-C, PTSD check list-civilian version; PTGI, posttraumatic growth inventory; CD-RISC, Connor-Davidson resilience scale; MPCHI, monthly per capita household income.
Data availability
The data used to support the findings of this study are included within the article.
Acknowledgment
The authors wish to thank all those who kindly volunteered to participate in the study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Central People’s Government of the People’s Republic of China. Up to June 9,there were 69,142 individuals dead in Wenchuan earthquake. 2008. Available from: http://www.gov.cn/jrzg/2008-06/09/content_1010832.htm.
2. Yokoyama Y, Otsuka K, Kawakami N, et al. Mental health and related factors after the Great East Japan earthquake and tsunami. PLoS One. 2014;9(7):e102497. doi:10.1371/journal.pone.0102497
3. Peek LA, Mileti DS. The history and future of disaster research. In: Churchman RBBA, editor. Handbook of Environmental Psychology. Hoboken (NJ): John Wiley & Sons Inc; 2002:511–524.
4. Chen CH, Tan HK, Liao LR, et al. Long-term psychological outcome of 1999 Taiwan earthquake survivors: a survey of a high-risk sample with property damage. Compr Psychiatry. 2007;48(3):269–275. doi:10.1016/j.comppsych.2006.12.003
5. Maj M, Starace F, Crepet P, et al. Prevalence of psychiatric disorders among subjects exposed to a natural disaster. Acta Psychiatr Scand. 1989;79(6):544–549.
6. Zhang W, Jiang X, Ho KW, Wu D. The presence of post-traumatic stress disorder symptoms in adolescents three months after an 8.0 magnitude earthquake in southwest China. J Clin Nurs. 2011;20(21–22):3057–3069. doi:10.1111/j.1365-2702.2011.03825.x
7. Fan F, Zhang Y, Yang Y, Mo L, Liu X. Symptoms of posttraumatic stress disorder, depression, and anxiety among adolescents following the 2008 Wenchuan earthquake in China. J Trauma Stress. 2011;24(1):44–53. doi:10.1002/jts.20599
8. Escobar JI, Canino G, Rubio-Stipec M, Bravo M. Somatic symptoms after a natural disaster: a prospective study. Am J Psychiatry. 1992;149(7):965–967. doi:10.1176/ajp.149.7.965
9. Wood JM, Bootzin RR, Rosenhan D, Nolen-Hoeksema S, Jourden F. Effects of the 1989 San Francisco earthquake on frequency and content of nightmares. J Abnorm Psychol. 1992;101(2):219–224.
10. Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: part I. An empirical review of the empirical literature, 1981–2001. Psychiatry. 2002;65(3):207–239.
11. Bensimon M. Elaboration on the association between trauma, PTSD and posttraumatic growth: the role of trait resilience. Pers Individ Dif. 2012;52(7):782–787. doi:10.1016/j.paid.2012.01.011
12. Nishi D, Matsuoka Y, Kim Y. Posttraumatic growth, posttraumatic stress disorder and resilience of motor vehicle accident survivors. Biopsychosoc Med. 2010;4:7. doi:10.1186/1751-0759-4-7
13. Zerach G, Solomon Z, Cohen A, Ein-Dor T. PTSD, resilience and posttraumatic growth among ex-prisoners of war and combat veterans. Isr J Psychiatry Relat Sci. 2013;50(2):91–99.
14. Green BL, Lindy JD, Grace MC, et al. Buffalo Creek survivors in the second decade: stability of stress symptoms. Am J Orthopsychiatry. 1990;60(1):43–54.
15. Priebe S, Marchi F, Bini L, Flego M, Costa A, Galeazzi G. Mental disorders, psychological symptoms and quality of life 8 years after an earthquake: findings from a community sample in Italy. Soc Psychiatry Psychiatr Epidemiol. 2011;46(7):615–621. doi:10.1007/s00127-010-0227-x
16. Ssenyonga J, Owens V, Olema DK. Posttraumatic Growth, Resilience, and Posttraumatic Stress Disorder (PTSD) among Refugees. Procedia Soc Behav Sci. 2013;82:144–148. doi:10.1016/j.sbspro.2013.06.238
17. Chen AC, Keith VM, Leong KJ, et al. Hurricane Katrina_ prior trauma, poverty and health among Vietnamese-American survivors. Int Nurs Rev. 2007;4(54):324–331. doi:10.1111/j.1466-7657.2007.00597.x
18. Carr VJ, Lewin TJ, Webster RA, Kenardy JA, Hazell PL, Carter GL. Psychosocial sequelae of the 1989 Newcastle earthquake: II. Exposure and morbidity profiles during the first 2 years post-disaster. Psychol Med. 1997;27(1):167–178.
19. Goenjian AK, Najarian LM, Pynoos RS, et al. Posttraumatic stress disorder in elderly and younger adults after the 1988 earthquake in Armenia. Am J Psychiatry. 1994;151(6):895–901. doi:10.1176/ajp.151.6.895
20. Dell OL, Carmassi C, Massimetti G, et al. Impact of traumatic loss on post-traumatic spectrum symptoms in high school students after the L’Aquila 2009 earthquake in Italy. J Affect Disord. 2011;134(1–3):59–64. doi:10.1016/j.jad.2011.06.025
21. Bland SH, O’Leary ES, Farinaro E, Jossa F, Trevisan M. Long-term psychological effects of natural disasters. Psychosom Med. 1996;58(1):18–24.
22. Zhen Y, Huang ZQ, Jin J, Deng XY, Zhang LP, Wang JG. Posttraumatic stress disorder of Red Cross nurses in the aftermath of the 2008 Wenchuan China Earthquake. Arch Psychiatr Nurs. 2012;26(1):63–70. doi:10.1016/j.apnu.2011.02.004
23. Fung OW, Loke AY, Lai CK. Disaster preparedness among Hong Kong nurses. J Adv Nurs. 2008;62(6):698–703. doi:10.1111/j.1365-2648.2008.04655.x
24. Chang CM, Lee LC, Connor KM, Davidson JR, Jeffries K, Lai TJ. Posttraumatic distress and coping strategies among rescue workers after an earthquake. J Nerv Ment Dis. 2003;191(6):391–398. doi:10.1097/01.NMD.0000071588.73571.3D
25. Fullerton CS, Ursano RJ, Wang L. Acute stress disorder, posttraumatic stress disorder, and depression in disaster or rescue workers. Am J Psychiatry. 2004;161(8):1370–1376. doi:10.1176/appi.ajp.161.8.1370
26. National Bureau of Statistics of China. China Statistical Yearbook 2015; 2015. http://www.stats.gov.cn/.
27. Ministry of Civil Affairs of the People’s Republic of China. Ten severely affected sub-districts are defined in Sichuan province. 2008. http://www.gov.cn/jrzg/2008-07/22/content_1053017.htm.
28. Derogatis LR. The SCL-90 Manual I: Scoring, Administration and Procedures for the SCL-90. Baltimore (MD): Clinical Psychometric Research; 1977.
29. Ni C, Liu X, Hua Q, Lv A, Wang B, Yan Y. Relationship between coping, self-esteem, individual factors and mental health among Chinese nursing students: a matched case-control study. Nurse Educ Today. 2010;30(4):338–343. doi:10.1016/j.nedt.2009.09.003
30. Zhang ZJ. Behavioral Medicine Scale Manual. Chinese Medical Audio-Video Organization; 2005. Peking.
31. Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility. Annual Convention of the International Society for Traumatic Stress Studies. San Antonio: International Society for Traumatic Stress Studies; 1993.
32. Yang X, Yang H, Liu Q. The research on the reliability and validity of PCL-C and influence factors. China J Health Psychol. 2007;15(1):6–9.
33. Wu K, Chan S, Yiu V. Psychometric properties and confirmatory factor analysis of the posttraumatic stress disorder checklist for Chinese survivors of road traffic accidents. Hong Kong Psychiatry. 2008;18(4):144–151.
34. Dongling L, Hui C, Ling M, Wenqian B, Zailiang L, Changying C. Post-traumatic stress disorder and its predictors among bereaved Tibetan adolescents 4 years after the Yushu earthquake: a cross-sectional survey in China. J Clin Nurs. 2017;26(7–8):1095–1105. doi:10.1111/jocn.13481.
35. Zhang W, Liu H, Jiang X, Wu D, Tian Y. A longitudinal study of posttraumatic stress disorder symptoms and its relationship with coping skill and locus of control in adolescents after an earthquake in China. PLoS One. 2014;9(2):e88263. doi:10.1371/journal.pone.0088263
36. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress. 1996;9(3):455–471.
37. Yu XN, Lau JTF, Zhang J, et al. Posttraumatic growth and reduced suicidal ideation among adolescents at month 1 after the Sichuan Earthquake. J Affect Disord. 2010;123(1–3):327–331. doi:10.1016/j.jad.2009.09.019
38. Wang J, Chen Y, Wang Y, Liu X. Revision of the Posttraumatic Growth Inventory and testing its reliability and validity. J Nurs Sci. 2011;22(5):5–15.
39. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
40. Yu X, Zhang J. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) in Chinese people. Soc Behav Pers Int J. 2007;35(1):19–30. doi:10.2224/sbp.2007.35.1.19
41. Marres GM, Leenen LP, de Vries J, Mulder PG, Vermetten E. Disaster-related injury and predictors of health complaints after exposure to a natural disaster: an online survey. BMJ Open. 2011;1(2):e000248. doi:10.1136/bmjopen-2011-000248
42. Bhamra R, Dani S, Burnard K. Resilience: the concept, a literature review and future directions. Int J Prod Res. 2011;49(18):5375–5393. doi:10.1080/00207543.2011.563826
43. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–562. doi:10.1111/cdev.2000.71.issue-3
44. Tugade MM, Fredrickson BL. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J Pers Soc Psychol. 2004;86(2):320–333. doi:10.1037/0022-3514.86.2.320
45. Liu X, Yang Y, Yuan P, et al. A study of the relationship between mental health and menstrual abnormalities in female middle school students from postearthquake Wenchuan. Biosci Trends. 2010;4(1):4–8.
46. Figley CR. Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized. New York (NY): Routledge; 2013.
47. Argentero P, Setti I. Engagement and Vicarious Traumatization in rescue workers. Int Arch Occup Environ Health. 2011;84(1):67–75. doi:10.1007/s00420-010-0601-8
48. Wang ZH, Ye Y, Shen Z, et al. An analysis of the evaluation results of symptom checklist 90 for female medical workers. Chin J Ind Hyg Occup Dis. 2018;36(10):745–748.
49. Lin SH, Liao WC, Chen MY, Fan JY. The impact of shift work on nurses’ job stress, sleep quality and self-perceived health status. J Nurs Manag. 2014;22(5):604–612. doi:10.1111/jonm.12020
50. Samaha E, Lal S, Samaha N, Wyndham J. Psychological, lifestyle and coping contributors to chronic fatigue in shift-worker nurses. J Adv Nurs. 2007;59(3):221–232. doi:10.1111/j.1365-2648.2007.04338.x
51. Yuan KC, Ruo Yao Z, Zhen Yu S, et al. Prevalence and predictors of stress disorders following two earthquakes. Int J Soc Psychiatry. 2013;59(6):525–530. doi:10.1177/0020764012453233
52. Kuwabara H, Shioiri T, Toyabe S, et al. Factors impacting on psychological distress and recovery after the 2004 Niigata-Chuetsu earthquake, Japan: community-based study. Psychiatry Clin Neurosci. 2008;62(5):503–507. doi:10.1111/j.1440-1819.2008.01842.x
53. Fronteira I, Ferrinho P. Do nurses have a different physical health profile? A systematic review of experimental and observational studies on nurses’ physical health. J Clin Nurs. 2011;20(17–18):2404–2424. doi:10.1111/j.1365-2702.2011.03721.x
54. Xu J, Liao Q. Prevalence and predictors of posttraumatic growth among adult survivors one year following 2008 Sichuan earthquake. J Affect Disord. 2011;133(1–2):274–280. doi:10.1016/j.jad.2011.03.034
55. Kleim B, Ehlers A. Evidence for a curvilinear relationship between posttraumatic growth and posttrauma depression and PTSD in assault survivors. J Trauma Stress. 2009;22(1):45–52. doi:10.1002/jts.20378
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.