")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Psychological Status and Correlated Factors of Primary Medical Staff During the COVID-19 Outbreak in Hefei City, China
Authors Wang S, Gao RC, Li R, Wu GC
Received 4 January 2021
Accepted for publication 11 March 2021
Published 31 March 2021 Volume 2021:14 Pages 751—756
DOI https://doi.org/10.2147/JMDH.S289336
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Song Wang, 1,* Rui-Chen Gao, 2,* Rui Li, 3,* Guo-Cui Wu 1
1Lianhua Community Health Service Center, The Second Affiliated Hospital, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2School of Nursing, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 3Department of Hospital Infection Management, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guo-Cui Wu
School of Nursing, Anhui Medical University, 15 Feicui Road, Hefei, 230601, Anhui, People’s Republic of China
Email [email protected]
Objective: To investigate the mental illness and correlated factors of primary medical staff during the COVID-19 outbreak in Hefei city, China.
Methods: A total of 180 primary medical staff were randomly selected from seven community hospitals in Hefei Economic and Technological Development Zone as a study group. One hundred and eighty-two health people were recruited as the control group. The self-rating Anxiety Scale (SAS), self-rating Depression Scale (SDS) and Psychological questionnaire of public health emergencies were distributed to them for evaluation.
Results: The score of SAS, SDS in study group was higher than that in control group [(35.57± 10.39) vs (31.31± 7.98); (44.16± 8.46) vs (41.47± 9.47)] (t=4.371, P< 0.001; t=2.849, P=0.005). The fear subscale and total score in the psychological questionnaire of sudden public health events were negatively correlated with age (r=− 0.216, P=0.004; r=− 0.154, P=0.039). Marriage was negatively correlated with depression subscales in psychological questionnaires of SAS, SDS and sudden public health events (r=− 0.184, P=0.013; r=− 0.298, P< 0.001; r=− 0.161, P=0.031; r=− 0.147, P=0.049). Education level was positively correlated with the total score of a psychological questionnaire for sudden public health events (r=0.151, P=0.043); Logistic regression analysis showed that marital status was a protective factor of psychological abnormality.
Conclusion: It is necessary to pay attention to the psychological status of primary medical staff, especially the young unmarried medical staff.
Keywords: novel coronavirus pneumonia, doctor, nurse, anxiety, depressed
A Letter to the Editor has been published for this article.
Introduction
The new coronavirus is a new strain of coronavirus found in humans in addition to the six coronaviruses currently known to infect humans. It is named “COVID-19” by the World Health Organization (WHO), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The virus strain spreads rapidly in a short time,1,2 and the doubling time is relatively shorter than severe acute respiratory syndrome (SARS). Currently, the disease has spread to other regions of China and around the world.3 The COVID-19 epidemic spreads very quickly and affects a large number of people. By February 15, 2020, a total of 26 countries had been affected by the epidemic, resulting in 51,857 laboratory-confirmed infections and 1669 deaths. In response to this serious situation, the WHO declared the COVID-19 epidemic a public health emergency of international concern on January 30, 2020 and called for collaborative efforts of all countries to prevent and control its rapid spread.4 However, the investigation from the early notification of the outbreak showed that many important information about the source of the virus and the ability to spread between the population, various clinical manifestations, treatment and epidemic characteristics is still unknown,2 and thus the prevention and control of COVID-19 and the implementation of effective measures has great uncertainty.
Currently, COVID-19 spread has become a major national public health event, threatening people’s physical and mental health and even life safety, seriously affecting people’s daily life and work, endangering social and economic development.5 Since the outbreak, response efforts by the China government have been swift, and three weeks into the epidemic, in an unprecedented move to retard the spread of the SARS-CoV-2 virus, a lockdown was imposed on Wuhan on 23 January, 2020, with travel restrictions. Within days, the quarantine was extended to additional provinces and cities, affecting more than 50 million people in total.6 However, COVID-19 patients were found in almost all provinces across China in the short term. There was no doubt that the medical workforce played an indispensable role in this major public health emergency.7 As of February 22, 2020, Anhui Province had a total of 989 confirmed cases, ranking in the top 10 in China. The primary medical staffs who are on the front line of prevention and control are under heavy work pressure and also suffer from huge psychological pressure. They feel lonely, isolated from the outside world, and unable to communicate face-to-face with their families. The pressure from all aspects cannot be effectively alleviated, making them feel more afraid and worried.8 In the present study, we selected primary medical staff during the first-level prevention and control period in Anhui Province as the study group to evaluate the mental health status and compared them with healthy people in Hefei city, China in the same period. In addition, we also compared the mental health differences between doctors and nurses groups.
Materials and Methods
Study Subjects
A total of 180 primary medical staff consisting of doctors, nurses and medical technicians from 7 community health service centers in the Economic Development Zone of Hefei City were selected as a study group. The average age was 37.96±9.81 years. Ninety two of 180 participants were male, and 88 were female. For marital status, 29 were unmarried, 139 were married, 10 were divorced, and 2 were widowed. For educational level, there were 85 cases with a bachelor degree or above, 38 cases with a junior college degree, 30 cases with higher vocational education and 27 cases with technical secondary school. The inclusion criteria of study subjects were as follows: (1) participated in first-line epidemic prevention; (2) voluntarily participated in this study; exclusion criteria: (1) complicated with physical and mental diseases; (2) those who have not completed all scale measurements. One hundred and eighty-two healthy citizens of Hefei City in the same period were selected as control group, and the inclusion criteria were as follows: (1) healthy people who did not suffer from COVID-19; (2) volunteered to participate in this study; (3) junior high school education level or above; exclusion criteria: (1) combined with other physical and mental diseases; (2) those who did not complete all scale measurements. There were no significant differences in age, gender, marriage, and education level (all P>0.05) between the two groups (Table 1).
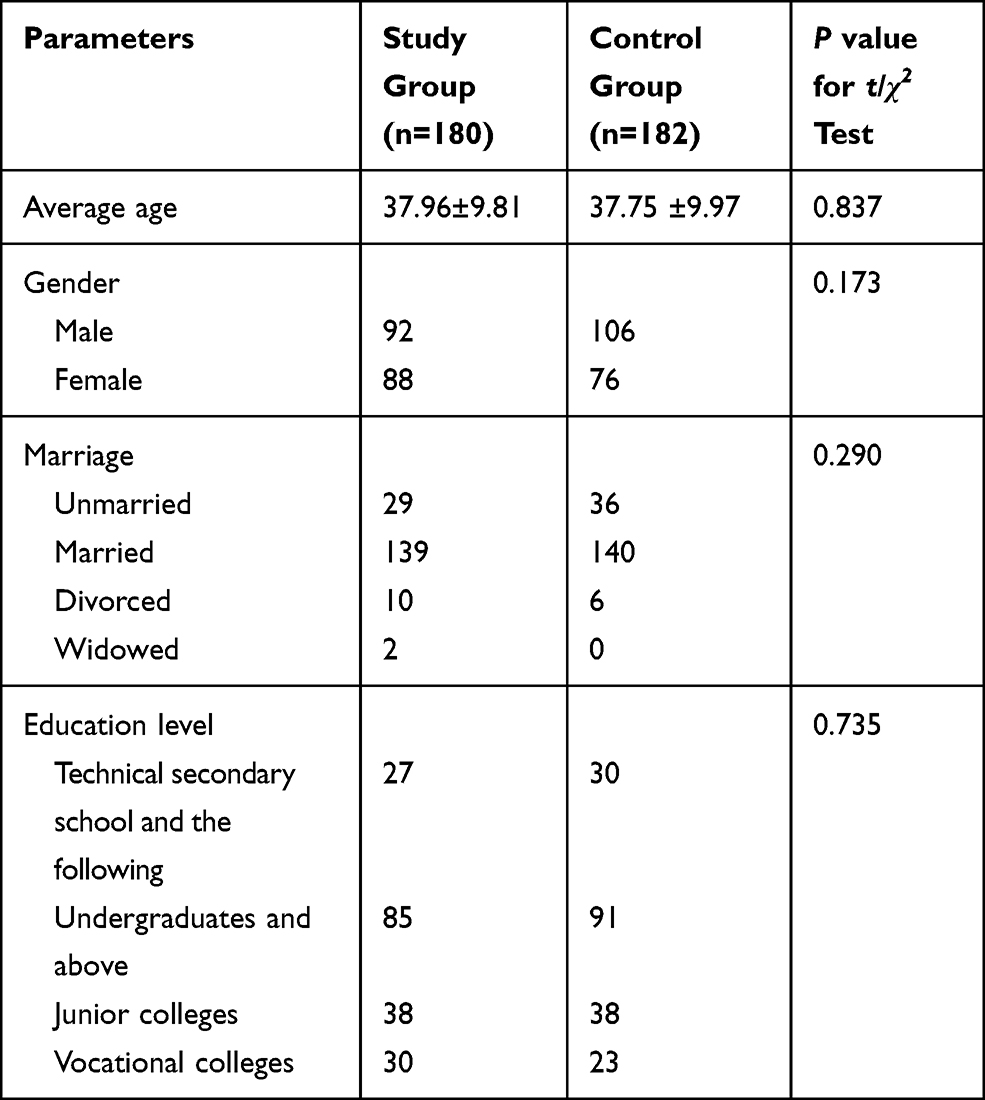 |
Table 1 Baseline Characteristics of Study Subjects |
Ethics statement: The study protocol was approved by the Committee on Medical Ethics of the Second Affiliated Hospital of Anhui Medical University (approval number: YX2020-093), informed consent were received from the study participants and that the guidelines outlined in the Declaration of Helsinki were followed.
Research Tools
Wenjuanxing, an online crowdsourcing platform, was used for questionnaire survey (www.wjx.cn/). The scales used in this online survey included: (1) Self-rating Anxiety Scale (SAS):9 This scale contains a total of 20 items, using a 4-point scale of 1 to 4 points; there is anxiety in Chinese norm of depression of less than 50 points;9 (2) Self-rating Depression Scale (SDS):9 The scale has a total of 20 questions, all of which have a score of 1 to 4 points, and Chinese norm for depression is<50 points, there is depressive;9 (3) Impact of Event Scale-Revised (IES-R), a Psychological Questionnaire for Sudden Public Health Events:9 This scale was surveyed by residents in 2003 to be affected by SARS. After evaluation of reliability and validity, a total of 25 items were established, using 0 to 3 four-level scores, the higher the total score, the greater the psychological impact of public health emergencies.9
Statistical Analysis
SPSS 23.0 was used for statistical processing, measurement data was expressed as (mean ± sd), comparison of means between two groups was performed by two-sample t test, and comparison of category variables was performed by chi-square test. Correlation analysis was conducted by Pearson correlation coefficient, and risk factors wer analyzed by logistic regression analysis; P <0.05 means the difference is statistically significant.
Results
Comparison of SAS, SDS and Psychological Questionnaires for Public Health Emergencies Between the Two Groups
The SAS and SDS scale scores of the study group were higher than those of the control group [(35.57±10.39) vs (31.31±7.98); (44.16±8.46) vs (41.47±9.47)] (t=4.371, P< 0.001; t=2.849, P=0.005) (Table 2).
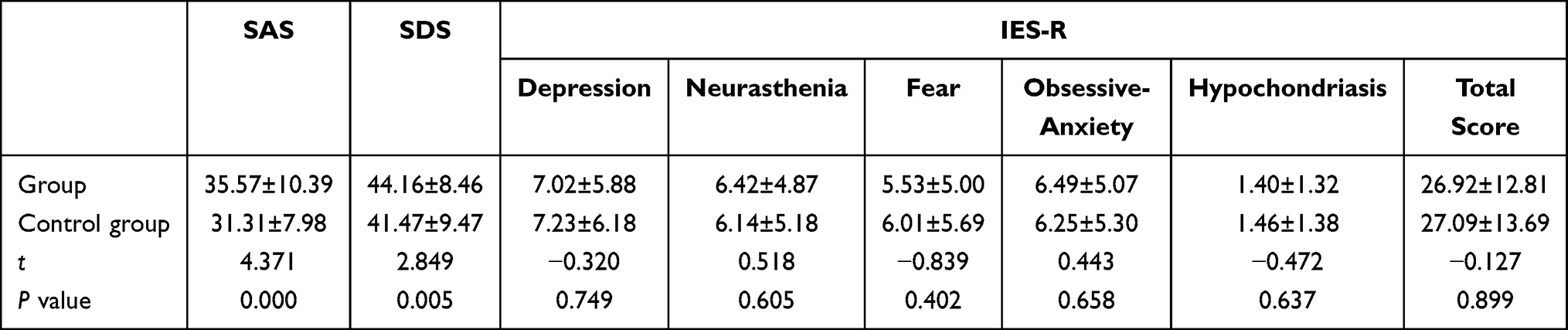 |
Table 2 Comparison of SAS, SDS and IES-R Scores Between Two Groups |
Comparison of Abnormal SAS and SDS Between the Two Groups
In the study group, there were 11 cases with abnormal scores on the SAS scale, 46 cases with abnormal scores on the SDS scale, and 52 persons with abnormal scores on the SAS and SDS scales. In the control group, there were 4 cases with abnormal scores on the SAS scale and 23 cases with abnormal scores on the SDS scale; the total number of abnormal scores on the SAS and SDS scale was 27. There was no significant difference in the proportion of the number of abnormal SAS scores between the study group and the control group (χ2 = 3.489, P = 0.062); the study group had a greater proportion of SDS population than the control group (χ2= 9.789, P = 0.002; χ2 = 10.477, P = 0.001).
Analysis of Related Factors of Mental Health Status of the Study Group
Age was negatively correlated with the fear subscale and total score in the psychological questionnaire of sudden public health events (r=−0.216, P=0.004; r=−0.154, P=0.039). Marriage was negatively correlated with SAS, SDS, depression scale in Psychological Questionnaire of Sudden Public Health Events, and total score of the psychological questionnaire of sudden public health events (r=−0.184, P=0.013; r=−0.298, P<0.001; r=−0.161, P=0.031; r=−0.147, P=0.049). The educational level was positively correlated with the total score of the psychological questionnaire of sudden public health events (r=0.151, P=0.043) (Table 3).
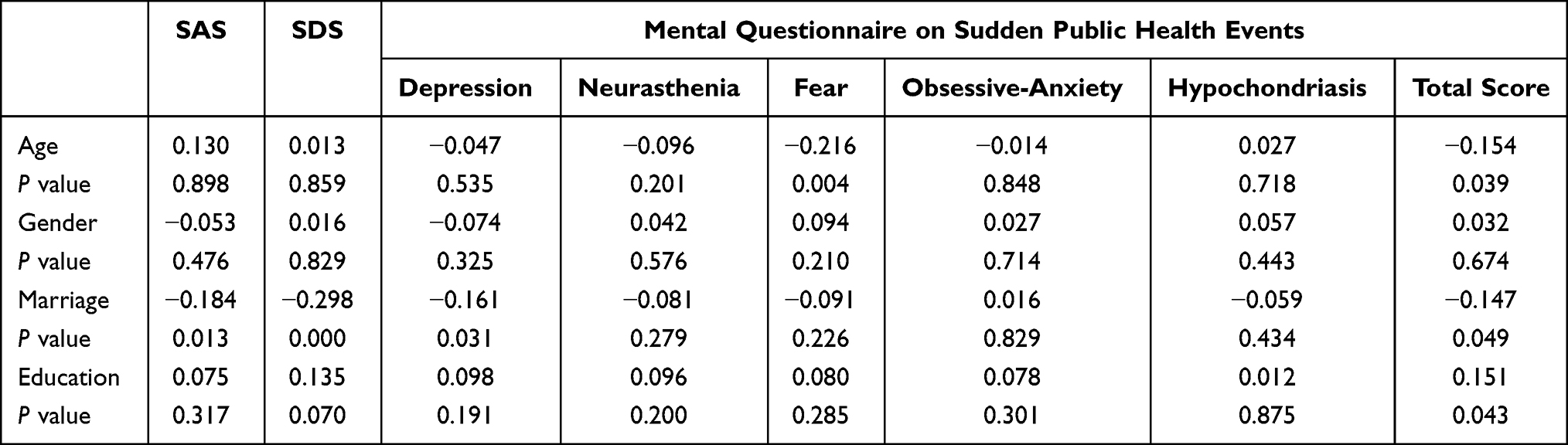 |
Table 3 Analysis of the Relevant Factors of Mental Health Status (r Values) |
Logistic Regression Analysis of Related Factors Affecting the Mental Health of Primary Medical Staff
Mental state was taken as the dependent variable (Y = 1 means “mental abnormality” and 0 means “title mental status”), the above four factors were regarded as independent variables, and the forward LR method was adopted to incorporate the above factors into the logistic regression model. The analysis showed that marriage was a protective factor for psychological abnormalities (OR = 0.015, 95% CI 0.003–0.070) (Table 4).
 |
Table 4 Logistic Regression Analysis of Influencing Factors of Mental State Among Primary Medical Staff |
Discussion
It has been reported that during the epidemic of influenza A (H1N1) in 2009 high-risk medical staff had a certain degree of psychological disorders, mainly manifested as emotional and sleep disorders, among which the medical staff in fever clinic were the most severe, especially at the early stage and the outbreak stage of H1N1.10 Liu et al11 found that there were problems with the mental health status of medical staff in military hospitals during the SARS outbreak. The scores of somatization, depression, anxiety and obsession were all increased in the psychological questionnaire evaluation, and the scores of somatization and depression were significantly increased. During the outbreak of the Ebola virus outbreak, an analysis of the psychological status of medical staff in Africa found that front-line medical staff had more prominent psychological problems in terms of compulsive behavior, interpersonal sensitivity, depressive symptoms and partial execution behaviors.8 A study from Arab countries showed that during the outbreak of Middle East respiratory syndrome (MERS), medical staff’s anxiety scores were relatively high.12 During the outbreak of influenza A in Japan, a survey of the psychological status of 1625 medical staff showed that medical staff in high-risk departments showed varying degrees of anxiety and mental fatigue13. Chan et al14 conducted a survey on the psychological status of medical staff in Singapore two months after the SARS outbreak, their results showed that approximately 20% of medical staff had stress disorders. At the same time, this psychological disorder was related to health, family relations, friends or colleagues. There is a correlation between the relationship, work, and mental appearance of the medical staff, and the emotions of medical staff after the SARS outbreak were affected and hurt to varying degrees. Not only during the epidemic outbreak, medical staff suffered severely from the stress of the epidemic, the anxiety symptoms, depression symptoms and post-traumatic stress of high-risk medical staff remained at a relatively high level for 1–2 years or more after the SARS outbreak.15,16
Previous studies were mostly concentrated in general hospitals and were mostly limited to cross-sectional investigations.8,11 The present study suggested that the mental health status of primary medical staff was lower than that of the healthy control group. Age was negatively correlated with the fear subscale and total score in the psychological questionnaire for public health emergencies; Marriage was negatively correlated with the subscale and total score of depression in the psychological questionnaire of SAS, SDS and sudden public health events. Educational level was positively correlated with the total scores of psychological questionnaires for public health emergencies; these findings indicated that young and unmarried medical care groups had higher scores on the scale and worse mental health status; logistic regression analysis showed that marriage was a risk factor for psychological abnormalities. This study suggests that during the epidemic period, attention should be paid to the psychological status of primary care workers, especially young unmarried health care workers. Studies on the psychological status of and its influencing factors in health care workers (HCWs) during the coronavirus disease 2019 (COVID-19) outbreak indicated that married people were 1.639 times than single (OR = 1.639, 95% CI 1.355–1.922). The main reason for married people’s stress might be that their work increased the risk of infection among family members.17
At present, there are relatively fewer researches on the mental state of medical staff during the outbreak of COVID-19, and most of the related studies were in Wuhan18,19 or the tertiary hospitals.20 There are few researches on the psychological changes among primary medical staff under long-term stress. As the first line of epidemic prevention and control, primary-level medical institutions need to participate in pre-examination and triage, key personnel investigation, and follow-up work of people returned from epidemic areas, fever residents and close contacts.21 Because there is a certain gap between the medical knowledge, skills and protective equipment of the primary medical staff and the general hospital above the second level, the psychological problems may be more prominent. However, due to the COVID-19 epidemic, the questionnaire survey could only be conducted through an online platform, and the sample size is limited. In the future, further studies with a large sample size are still needed to provide a more precise reference for the psychological health interventions among primary medical staff in public health emergencies.
Acknowledgment
Song Wang, Rui-Chen Gao and Rui Li should be considered co-first authors.
Funding
Humanities Research Center Project of Anhui Medical University (No. YJSK202017). Doctoral Research Project of the First Affiliated Hospital of Anhui Medical University (No.BSKY2019037).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Munster VJ, Koopmans M, van Doremalen N, et al. A novel coronavirus emerging in china – key questions for impact assessment. N Engl J Med. 2020;382(8):692–694. doi:10.1056/NEJMp2000929
2. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
3. Hong KH, Lee SW, Kim TS, et al. Guidelines for Laboratory Diagnosis of Coronavirus Disease 2019 (COVID-19) in Korea. Ann Lab Med. 2020;40(5):351–360. doi:10.3343/alm.2020.40.5.351
4. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
5. Chen Y, Jin YL, Zhu LJ, et al. The network investigation on knowledge, attitude and practice about Novel coronavirus pneumonia of the residents in Anhui Province. Chin J Prevent Med. 2020;54(4):367–373. doi:10.3760/cma.j.cn112150-20200205-00069
6. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health. 2020;17:5.
7. Lu W, Wang H, Lin Y, et al. Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. 2020;288:112936. doi:10.1016/j.psychres.2020.112936
8. Chan-Yeung M. Severe acute respiratory syndrome (SARS) and healthcare workers. Int J Occup Environ Health. 2004;10(4):421–427. doi:10.1179/oeh.2004.10.4.421
9. Zhang ZJ. Behavioral Medicine Scale Manual [M/CD]. China Med Electronic Audiovisual Press. 2005;
10. Wu JS, Yan T, Peng S. A retrospective analysis of the cognition and psychological state of medical staff during A-flow. Chine J Health Psychol. 2011;19(11):1324–1327.
11. Liu JH, Wang W, Gao WB, et al. The effect of SARS on the mental health of medical staff in the hot hospitals of military hospitals. Southern J Nurs. 2004;11(4):9–10.
12. Alsubaie S, Temsah MH, Al-Eyadhy AA, et al. Middle East Respiratory Syndrome Coronavirus epidemic impact on healthcare workers’ risk perceptions, work and personal lives. Infect Dev Countr. 2019;13(10):920–926. doi:10.3855/jidc.11753
13. Matsuishi K, Kawazoe A, Imai H, et al. Psychological impact of the pandemic (H1N1) 2009 on general hospital workers in Kobe. PSYCHIAT CLIN NEUROS. 2012;66(4):353–360. doi:10.1111/j.1440-1819.2012.02336.x
14. Chan AOM, Huak CY. Psychological impact of the 2003 severe acute respiratory syndrome outbreak on health care workers in a medium size regional general hospital in Singapore. Occup Med (Chic Ill). 2004;54(3):190–196. doi:10.1093/occmed/kqh027
15. McAlonan GM, Lee AM, Cheung V, et al. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can J Psychiatry. 2007;52(4):241–247. doi:10.1177/070674370705200406
16. Su TP, Lien TC, Yang CY, et al. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: a prospective and periodic assessment study in Taiwan. J Psychiatr Res. 2007;41(1–2):119–130. doi:10.1016/j.jpsychires.2005.12.006
17. Yao Y, Tian Y, Zhou J, et al. Psychological status and influencing factors of hospital medical staff during the COVID-19 Outbreak. Front Psychol. 2020;11.
18. Shen W, Qin Y, Tao MY, et al. Investigation on mental health level of first-line medical personnel in prevention and control of new coronavirus pneumonia in Hunan province. General Care. 2020;18(8):957–962.
19. Wang F, Shu C. Psychological stress response and intervention measures of first-line medical staff in the new coronavirus pneumonia epidemic. Gen Nurs. 2020;18(7):837–838.
20. Wu JJ, Rong X, Chen F, et al. Sleep quality investigation and influencing factors of clinical first-line nurses in the fight against the new coronavirus pneumonia epidemic. Nurs Res. 2020;34(4):558–562.
21. Chi CH, Wu H, Yang T, et al. Do a good job in the primary prevention and control of new coronavirus infection. Chine J Gen Pract. 2020;19. doi:10.3760/cma.j.issn.1671-7368.2020.0002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.