")
Back to Journals » Infection and Drug Resistance » Volume 11
Pseudomonas aeruginosa bacteremia among liver transplant recipients
Authors Liu TH, Zhang YZ , Wan QQ
Received 15 July 2018
Accepted for publication 5 October 2018
Published 16 November 2018 Volume 2018:11 Pages 2345—2356
DOI https://doi.org/10.2147/IDR.S180283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Joachim Wink
Taohua Liu,1 Yuezhong Zhang,1 Qiquan Wan2
1Xiangya School of Medicine, Central South University, Changsha 410083, China; 2Department of Transplant Surgery, The Third Xiangya Hospital, Central South University, Changsha 410013, China
Abstract: Pseudomonas aeruginosa bacteremia remains as a life-threatening complication after liver transplantation (LT) and is intractable because of the high rate of drug resistance to commonly used antibiotics. To better understand the characteristics of this postoperative complication, PubMed and Embase searches as well as reference mining was done for relevant literature from the start of the databases through August 2018. Among LT recipients, the incidence of P. aeruginosa bacteremia ranged from 0.5% to 14.4% and mortality rates were up to 40%. Approximately 35% of all episodes of bloodstream infections (BSIs) were P. aeruginosa bacteremia, of which 47% were multidrug resistant and 63% were extensively drug resistant. Several factors are known to affect the mortality of LT recipients with P. aeruginosa bacteremia, including hypotension, mechanical ventilation, and increasing severity of illness. In LT recipients with P. aeruginosa bacteremia, alteration in DNA gyrase A genes and overexpression of proteins involved in efflux systems, namely the expression of KPC-2-type carbapenemase, NDM-1, and VIM-2-type MBL, contribute to the high resistance of P. aeruginosa to a wide variety of antibiotics. Because of complicated mechanisms of drug resistance, P. aeruginosa causes high morbidity and mortality in bacteremic LT patients. Consequently, early detection and treatment with adequate early targeted coverage for P. aeruginosa BSI are of paramount importance in the early posttransplantation period to obtain a better prognosis for LT patients.
Keywords: antimicrobial resistance, morbidity and mortality, risk factor, solid organ transplantation, liver transplantation
Introduction
Pseudomonas aeruginosa, one of the most lethal causative organisms of bacteremia, is classified as non-lactose-fermenting Gram-negative bacilli.1 Beyond the striking virulence, it is intrinsically resistant to some commonly used antibiotics, and it is capable of acquiring resistance to multiple classes of antibiotics.2–5 Consequently, it causes a wide array of life-threatening acute and chronic infections, particularly in immunocompromised patients.
P. aeruginosa bacteremia is a common condition that has a considerable impact on liver transplantation (LT), leading to significant morbidity and mortality. A large body of published studies showed that 0.5%–11.4% of LT recipients develop P. aeruginosa bacteremia, while the incidence of bacteremia caused by Pseudomonas spp. ranged from 0.9% to 11.8% in LT recipients.6–29 Approximately 30% mortality was observed in LT recipients with multidrug resistance (MDR) P. aeruginosa according to three studies over the span of 20 years.25,26,30
To date, a number of literature reviews have been published regarding the topic of P. aeruginosa bacteremia. However, much of them have been descriptive in the context of cystic fibrosis, respiratory disease, or AIDS. There has been no detailed investigation of P. aeruginosa bacteremia and its current impact in LT recipients. The present article will help to address this gap.
The remaining part of this review will discuss the epidemiology, mortality, microbiologic features, risk factors for bacteremia and mortality, mechanisms of drug resistance, prevention, and treatment for P. aeruginosa bacteremia in LT recipients.
Methods
To better understand the characteristics of bacteremia due to P. aeruginosa in LT recipients, PubMed and Embase databases were searched independently by two authors for relevant literature published from the start of these databases up to August 2018 by using the search terms “bloodstream infections (BSIs)”, “bacteremia”, “septicemia”, “infection”, “epidemiology”, “microbiology”, “non-fermenters”, “nonfermenting”, “P. aeruginosa”, “therapy”, “multidrug resistance”, “extensively drug resistant (XDR)”, “risk factor”, “predictor”, “morbidity”, “mortality”, “liver transplantation”, and “solid organ transplantation (SOT)”. We also screened relevant reviews and references available to identify potentially relevant studies. No restriction was applied during the literature search.
Morbidity of bacteremia caused by P. aeruginosa was defined using criteria proposed by Centers for Disease Control and Prevention (CDC): the isolation of P. aeruginosa in one culture with signs of infection or the isolation of P. aeruginosa from at least two consecutive cultures correlated with signs of infection. Mortality was defined as death occurring during the hospitalization of an LT recipient with P. aeruginosa bacteremia.31
In the present review, MDR was defined as acquired non-susceptibility to at least one agent in three or more antimicrobial categories (except for reference 35, which defined MDR as resistance to all of the agents in two or more antimicrobial categories), and XDR was defined as non-susceptibility to at least one agent in all but two or fewer antipseudomonal antimicrobial categories (ie, bacterial isolates remain susceptible to only one or two categories) according to the criteria introduced by Magiorakos et al.32 Given that it is not only resistant to all β-lactam antimicrobials but also frequently to other classes of antimicrobials, such as aminoglycosides and fluoroquinolones, P. aeruginosa producing carbapenem-hydrolyzing β-lactamase is considered to be an MDR isolate.33,34
Morbidity and mortality of P. aeruginosa bacteremia in LT recipients
P. aeruginosa or Pseudomonas spp. bacteremia has not been reported to be problematic in early studies in LT recipients, with only 0–9 episodes documented in four series.21,28,35,36 However, P. aeruginosa bacteremia has become an emerging problem over the last three decades.
Among LT recipients, the morbidity caused by P. aeruginosa bacteremia was reported to be 0.5%–14.4%, while Pseudomonas spp. bacteremia was reported to be 0.9%, 1.0%, and 11.8%.6–29
As shown in Table 1, previous studies on LT recipients with BSIs reported that 2.5%–22.2% of their research subjects had P. aeruginosa bacteremia and 3.4%–6.9% carried Pseudomonas spp.6–13,15–19,21–23,26–30,36–39 In studies on Gram-negative bacteremia after LT, P. aeruginosa was responsible for 8.5%–9.4% of all cases of Gram-negative bacteremia.20,24 We found two other studies that investigated bacteremic LT recipients with focus on drug resistance; one of them reported that carbapenem- and quinolone-resistant P. aeruginosa bacteremia accounted for 5.2%–12.7% of all BSIs, while the second one reported that 9.3% of all episodes of BSIs was XDR P. aeruginosa bacteremia.40,41
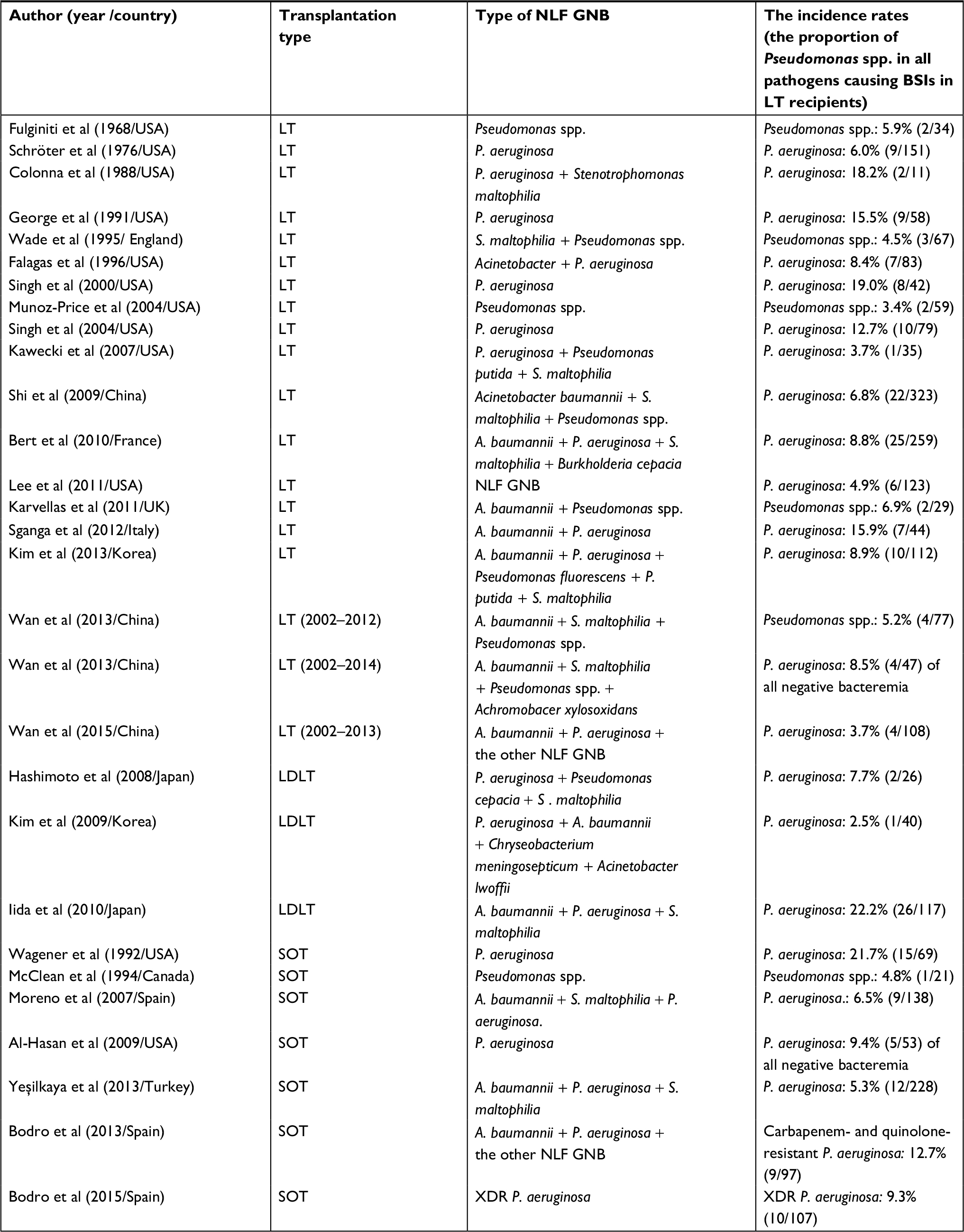 | Table 1 The incidence rates of Pseudomonas spp. in all pathogens causing BSIs in LT recipients Abbreviations: BSIs, bloodstream infections; GNB, non-lactose fermenting Gram-negative bacilli; LDLT, living donor liver transplantation; LT, liver transplantation; NLF, non-lactose fermenting; SOT, solid organ transplantation; XDR, extensively drug-resistant. |
P. aeruginosa is one of the most lethal causative organisms of bacteremia in LT populations. As shown in Table 2, the mortality rates varied in different studies, ranging from 0% to 40% in transplant recipients with P. aeruginosa bacteremia, and more than one-third of patients who developed XDR P. aeruginosa bacteremia after LT (38%) failed to survive.6,14,25,26,30,41–43
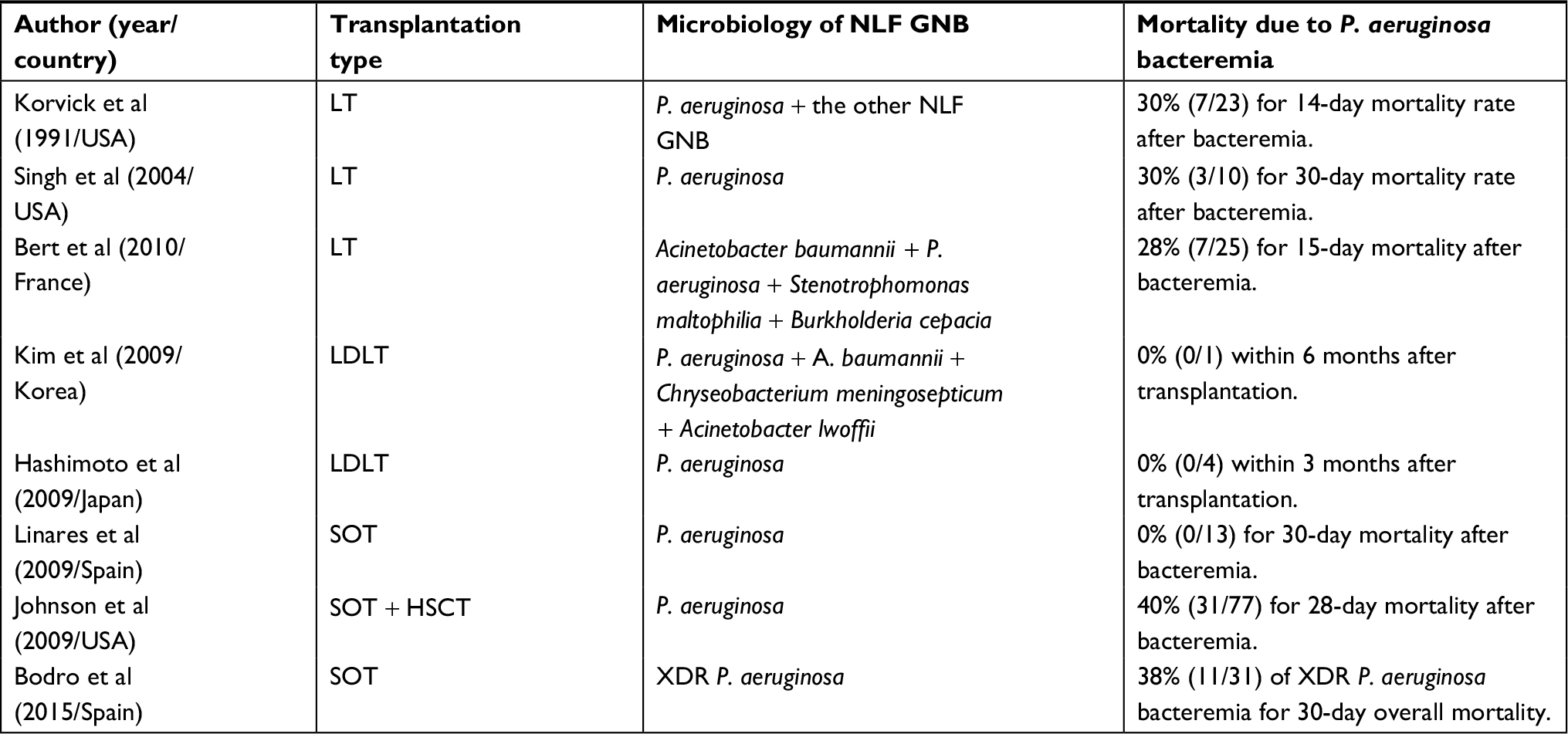 | Table 2 The mortality rates of Pseudomonas aeruginosa bacteremia in LT recipients Abbreviations: GNB, non-lactose fermenting Gram-negative bacilli; HSCT, hematopoietic stem cell transplant recipients; LDLT, living donor liver transplantation; LT, liver transplantation; NLF, non-lactose fermenting; SOT, solid organ transplantation; XDR, extensively drug-resistant. |
Antimicrobial resistance of P. aeruginosa causing bacteremia
Among all P. aeruginosa isolates causing bacteremia in LT recipients, MDR P. aeruginosa accounted for 47% and XDR for 63.2%.41,43 Sganga et al conducted a retrospective cohort study in a single center and reported that 12.5% of non-lactose-fermenting Gram-negative bacilli (largely consisting of P. aeruginosa, 87.5%) were MDR and 62.5% were XDR.9 Another single-center study conducted by Shi et al found 51.5% of Pseudomonas spp. to be MDR, defined by non-susceptibility to two or more antimicrobial categories; resistance rates of Pseudomonas spp. to ceftazidime, ciprofloxacin, and imipenem were 18%, 33%, and 32%, respectively.38
In previous studies on drug resistance, 16% of P. aeruginosa were carbapenem-resistant and 25% were carbapenem- and quinolone-resistant in LT recipients with bacteremia.18,30 The antibiotic resistance of P. aeruginosa causing bacteremia in LT recipients is shown in Table 3.
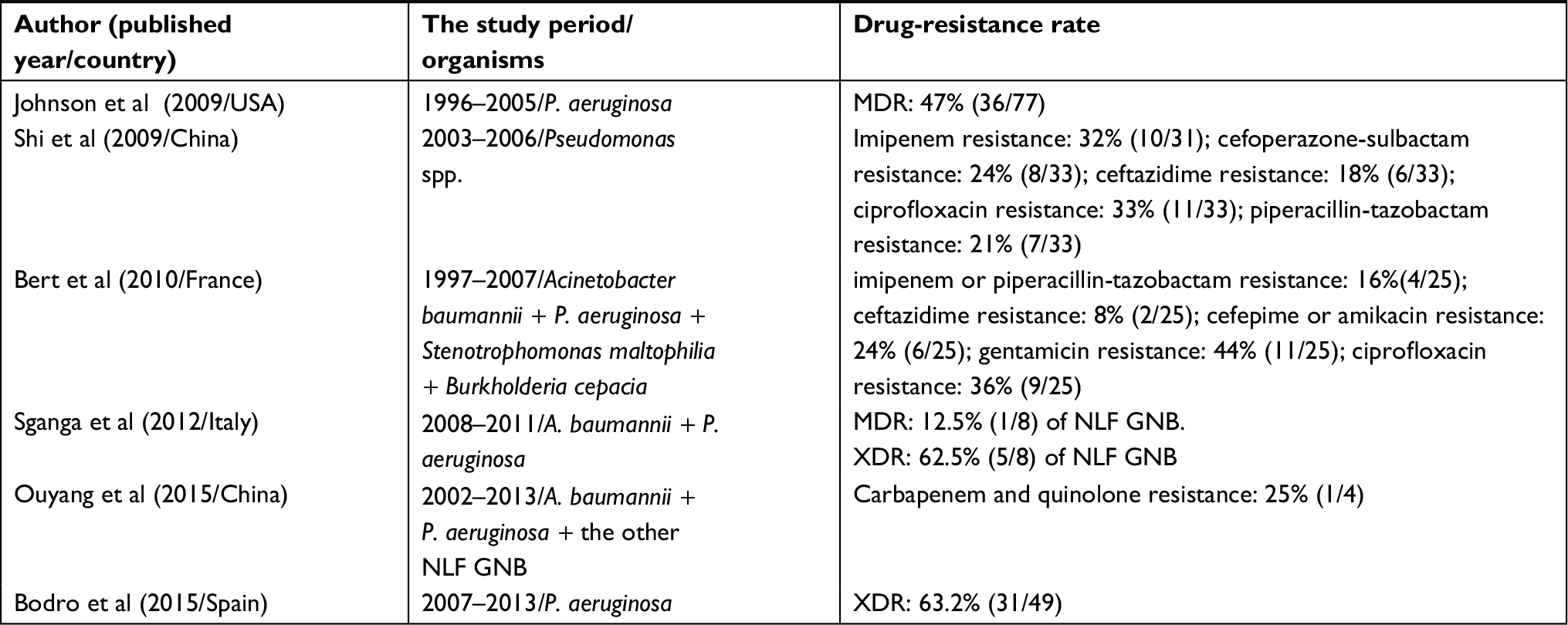 | Table 3 The proportion of MDR Pseudomonas aeruginosa to all P. aeruginosa isolates causing bacteremia in LT recipients Abbreviations: GNB, non-lactose-fermenting Gram-negative bacilli; LT, liver transplantation; MDR, multidrug resistance; NLF, non-lactose fermenting; XDR, extensive drug-resistant. |
Interestingly, there were significant differences in the ratios of MDR P. aeruginosa in that 43% of transplant isolates and only 18% of non-transplant isolates were MDR in a study conducted in the USA.40 A reasonable explanation could be that transplant recipients usually have higher exposure to invasive devices.
The most common portals of P. aeruginosa identified was the abdominal/biliary tract or intravascular catheters in bacteremic LT recipients.8,10,17,22,25,26 Intra-abdominal infections and the urinary tract were also reported as the most common source of P. aeruginosa bacteremia.14,30 Kim et al in a retrospective study of 222 consecutive LT recipients found that the main focus of Pseudomonas spp. bacteremia was the biliary tract.8 Table 4 shows the most common primary sources of P. aeruginosa or Pseudomonas spp. bacteremia in LT recipients.
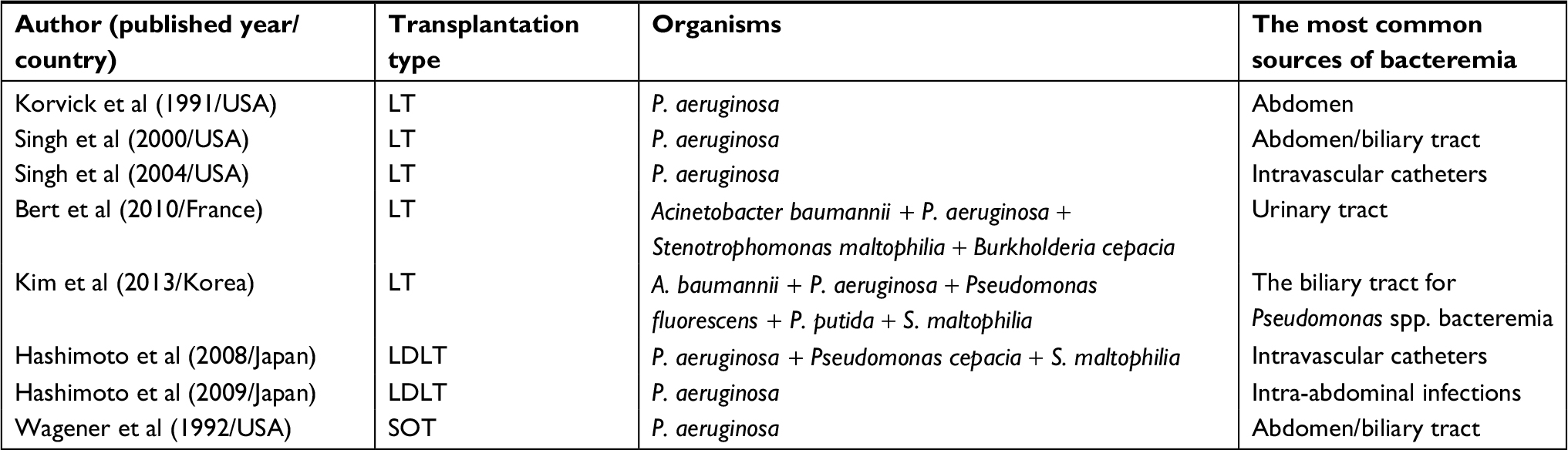 | Table 4 Primary sources of Pseudomonas aeruginosa bacteremia in LT recipients Abbreviations: LDLT, living donor liver transplantation; LT, liver transplantation; SOT, solid organ transplantation. |
The risk factors for the morbidity and mortality of P. aeruginosa bacteremia
Despite high rates of morbidity and mortality, predictors of P. aeruginosa bacteremia and its related mortality remain ill-defined in LT recipients. Recently, a prospective observational study from Spain claimed that in SOT recipients (mainly comprising renal and liver recipients), factors independently associated with XDR P. aeruginosa bacteremia were prior transplantation, nosocomial acquisition, and septic shock at onset.41 Korvick et al demonstrated that in LT recipients with P. aeruginosa bacteremia, survival rates were significantly lower for patients with hypotension, mechanical ventilation, or increasing severity of illness.25 In a large retrospective cohort study on P. aeruginosa BSI, Johnson et al focused on MDR in P. aeruginosa bacteremic transplant recipients, which included 52% of LT recipients. They found previous transplantation, hospital-acquired BSI, and prior intensive care unit admission to be independent risk factors for developing infection with MDR P. aeruginosa isolates. Their study also showed that onset of BSI during stay in the intensive care unit was the only independent predictor for 28-day in-hospital mortality.43 To date, no other study of LT recipients has assessed the association of clinical or laboratory parameters and the risk for P. aeruginosa bacteremia and its related mortality.
Diagnosis of P. aeruginosa bacteremia
Generally, to identify P. aeruginosa bacteremia in liver recipients, blood samples were cultured using the BacT/Alert automated instrument. The diagnosis of P. aeruginosa bacteremia was made by its isolation from one or more sets of blood culture bottles collected using standard sterile techniques, with the presence of clinical features consistent with signs of systemic infection, including fever, chills, or hypotension. Specific selective media and identification procedures such as using selective media with MacConkey agar and cetrimide were also recommended for the isolation of P. aeruginosa. The presence of MBLs was evaluated in imipenem- or meropenem-resistant P. aeruginosa by using both an EDTA screen test and the MBL E-test.44 Analysis by pulsed-field gel electrophoresis was the “gold standard” for confirming relatedness among P. aeruginosa.45 In addition to classic methods described above, new technologies have emerged.
Two FDA and CE marking (Conformité Européenne) approved commercial systems based on the concept of matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry (MS) are available in the market, including the Bruker Microflex Biotyper and the bioMérieux VITEK MS, which can rapidly identify clinical P. aeruginosa. However, ambiguities exist when using protein profiling to differentiate closely related bacterial species or strains because of similarity of proteins as well as the lack of representative spectra in the manufacturer’s database.46
Lipid A signature platforms using MS has been established to detect the chemical structure of lipid A and mechanisms of antibiotic resistance of P. aeruginosa. Using MALDI-TOF MS, the chemical structure of lipid A, especially the fatty acid number, location, and distribution of lipid A moiety extracted from P. aeruginosa were elucidated.47,48 With regard to antibiotic resistance of P. aeruginosa, Moskowitz et al confirmed that mutations in the pmrA/pmrB regulatory system resulted in the addition of epotaminoarabinose to lipid A, which led to polymyxin resistance.49 Liu et al found that lipid A is modified by the addition of phosphoethanolamine in polymyxin-resistant P. aeruginosa strains.50 However, as we stated above, MALDI-TOF analysis is not quantitative and very little structural information can be gained from the simple mass spectrum obtained; this limitation can be overcome by coupling it with tandem mass spectrometry.
Peptide nucleic acid fluorescence in situ hybridization assays is recently introduced as an alternative to other molecular methods to shorten the turnaround time of detection of P. aeruginosa from positive blood culture to 1.5–3 hours, but the information regarding antibiotic susceptibility profile is deficient.51
The mechanisms of drug resistance of P. aeruginosa
P. aeruginosa is intrinsically in vitro resistant to some commonly used antibiotics, such as trimethoprim/sulfamethoxazole and doxycycline. The high resistance of P. aeruginosa to a wide variety of antibiotics is due to its constitutive expression of β-lactamases as well as overexpression of AmpC and carbapenemases. Other likely causes of resistance include modification of penicillin-binding profiles, and the multidrug efflux pumps, such as MexAB-OprM, combined with the low permeability of its outer membrane and a high ability to generate acquired antibiotic resistance.52–58
The β-lactamase enzymes are divided into four functional groups A to D, where B or C β-lactamases are much more common enzymatic causes of resistance in P. aeruginosa. Oxacillinases are common in P. aeruginosa, and only oxacillinases 40 and 198 have been described in isolated reports to express carbapenemase activity.59,60
The clones carrying enzymatic resistance, particularly VIM-2, are of global concern. MBLs are the predominant group of carbapenemases, conferring resistance to all the β-lactams except aztreonam. IMP and VIM types are the most common MBLs found in P. aeruginosa.61 Other types of MBLs include SPM-1, GIM-1, AIM-1, NDM-1, and FIM-1.62–65 The study by Edelstein et al provided longitudinal data showing evidence of cross-transmission of a few successful clones such as ST111, ST175, or ST235, all of which belong to the majority of P. aeruginosa isolates, thereby contributing to the spread of resistance.66
Some studies showed that P. aeruginosa had higher level susceptibility to meropenem than to imipenem, a phenomenon representing reduced production of OprD porin, which is the preferential entry channel for imipenem.67
There are five superfamilies of efflux pumps that can reduce drug accumulation in the bacteria. Efflux pump upregulation can be a potential cause of MDR in a P. aeruginosa isolate. When the MexAB-OprM system is upregulated, it consequently reduces susceptibility to fluoroquinolone, penicillin, cephalosporin, and meropenem. Upregulation of MexCD-OprJ and MexEF-OprN confers P. aeruginosa resistance to fluoroquinolones and some β-lactams, whereas upregulation of MexXY-OprM may lead to reduction in susceptibility to aminoglycosides and fluoroquinolones.4,68
In addition to blaNDM, the blaVIM gene was also found in a carbapenem-resistant P. aeruginosa isolated from an institute of surgical gastroenterology and LT.69 Liu et al reported that a total of 812 strains of P. aeruginosa were isolated from patients including LT recipients from January to September 2012 and 24 carbapenem-resistant P. aeruginosa strains were identified. The resistance mechanism of P. aeruginosa to carbapenems was mainly mediated by the VIM-2-type MBL in their hospital, followed by KPC-2. Among these 24 carbapenem-resistant P. aeruginosa strains, two strains were isolated from LT recipients; one harbored blaKPC-2 and carried the mobile genetic element gene insertion sequence common region 1, while the other harbored ISEcp1.70 Genotype analysis showed that in liver and other solid organ transplant recipients, the selected XDR P. aeruginosa strains belonged to a single clone ST-175.41 Niga et al demonstrated that in a liver recipient, high fluoroquinolone resistance in P. aeruginosa resulted from cooperation between alteration in DNA gyrase A genes and overexpression of proteins involved in efflux systems.71
Treatment measures for P. aeruginosa bacteremia
With limited susceptibility to antimicrobial agents, frequent emergence of antibiotic-resistant mutants during therapy, and limited armamentarium of new antimicrobial agents in the pipeline, P. aeruginosa bacteremia has been an increasing problem in LT recipients in the modern era.72
P. aeruginosa accounts for the most common Gram-negative organism causing early posttransplant bacteremia in LT recipients. Early detection and treatment with adequate early targeted coverage for P. aeruginosa BSI are of paramount importance in the early posttransplantation period to obtain a better prognosis for LT patients.24,73 Surveys such as that conducted by Korvick et al have shown that before transplant or biliary tract manipulation, prophylactic agents should have in vitro activity against P. aeruginosa.25 SOT recipients with bacteremia due to XDR P. aeruginosa more often received inadequate empirical antibiotic therapy and had high case-fatality rates compared to other etiologies.41 Therefore, adequate empirical antibacterial coverage is essential. Detailed knowledge of the local epidemiology of P. aeruginosa bacteremia in LT recipients is also essential to help physicians prescribe adequate empirical antibiotics.
Management of infections caused by MDR P. aeruginosa is a major therapeutic challenge. Several previous studies of lung recipients have established that combination antibiotic therapies, including β-lactam, aminoglycoside, and/or fluoroquinolone, are preferred to monotherapy for infection due to MDR P. aeruginosa.74–76 However, comparable resistance rates of P. aeruginosa to both aminoglycosides and fluoroquinolones were found and should be considered when devising an empiric combination regimen in SOT recipients.24 Given the fact that nephrotoxicity risk due to aminoglycosides is a major concern among SOT recipients, combination therapy with β-lactam and fluoroquinolone antibiotics is a more reasonable option.77 Although colistin in combination with rifampin showed promise, rifampin can hardly be used in SOT patients because of significant drug-drug interactions with immunosuppressive agents.78 Meropenem with colistin showed synergy against P. aeruginosa; the combination of colistin and carbapenems is, therefore, a potential alternative.79 However, further data are required to determine exactly how this combination works for MDR P. aeruginosa.
For XDR P. aeruginosa, few antibiotic options are currently available: examples are colistin or certain aminoglycosides, which are frequently associated with a higher risk of nephrotoxicity owing to decreased glomerular filtration rate, the need for renal replacement therapies, hypotension associated with medical and surgical procedures, or the use of concomitant nephrotoxic medications such as anticalcineurins.27,73 Colistin alone or in combination with amikacin, β-lactam antibiotics in continuous or expanded perfusion, and high-dose carbapenem were recommended for treating XDR P. aeruginosa bacteremia.41 According to a previous study, high doses of colistimethate sodium (6–9 MU daily) without a loading dose may also be effective.41 Sun et al reported a case of a liver transplant recipient who developed intractable MDR P. aeruginosa bacteremia, which was finally controlled by a novel combination regimen of colistimethate, doripenem, and tobramycin.80
Usually, combination therapy is mandatory for treating MDR or XDR P. aeruginosa bacteremia, but little evidence of synergistic effects exists as the data available are based mostly on in vitro studies.79–81 Several recent studies assessing nontransplant patients failed to find a benefit of combination therapy over monotherapy.82–84 Of these studies, Bowers et al in an international multicenter retrospective cohort study failed to find through multivariate analysis that combination therapy was significantly different from monotherapy.82
Some promising new antimicrobial agents are now available for P. aeruginosa infection. For example, ceftolozane, a novel antipseudomonal cephalosporin, has demonstrated activity against carbapenem-resistant P. aeruginosa when used in combination with tazobactam.85,86 In May 2016, ceftolozane/tazobactam was approved by the Pharmacy and Therapeutics Committee of Balearic Public Health System to treat infections caused by MDR P. aeruginosa in the absence of appropriate therapeutic alternatives according to the patient’s characteristics.87 Ceftazidime-avibactam (CZA) may also be a valuable option for serious infections due to resistant P. aeruginosa, as a 17-month retrospective descriptive study found that half of their patients with MDR or XDR P. aeruginosa infection who received CZA as initial or continuation therapy were clinical cured.88 Furthermore, a new study published this year suggest a beneficial role of combination therapy with intravenous CZA and inhaled amikacin when treating pneumonia caused by P. aeruginosa, which indicate that inhaled antimicrobial therapy could be a good auxiliary method.89 Pivmecillinam is a pro-drug of mecillinam which is a β-lactam with specific activity against non-lactose-fermenting Gram-negative bacilli including P. aeruginosa.73
P. aeruginosa bacteremic donor should not be used if not appropriately treated. In case of unknown donor with P. aeruginosa bacteremia, recipients should receive a longer (2–4 weeks) antibiotic course.90
Because the most frequent source was the abdomen/biliary duct or intravascular catheters in LT recipients with P. aeruginosa bacteremia, source control through central venous catheter removal, wound debridement, drainage of abscess, the biliary tree, and body fluid are crucial factors associated with better outcomes of LT recipients.10,17,22,25,26
Control and Prevention of P. aeruginosa bacteremia
As a significant nosocomial pathogen, P. aeruginosa colonization and infections occur as a result of multiple or prolonged hospital admission, excessive exposure to antibiotics, and breaches in infection control, with the capacity of the organism to adhere to various materials used frequently in clinical settings.91,92 For P. aeruginosa, patient-to-patient transmission occurs mainly through the direct or indirect contact or droplet routes.93 Nurse understaffing, reduced isolation barriers, and absence of universal measures are pivotal in the spread of infection in the ICU or in wards. The measures to prevent P. aeruginosa bacteremia in LT recipients are the same as those for nonimmunosuppressed hospitalized patients. Generally, these measures include taking effective isolation measures, appropriate hand washing, restriction of the use of invasive devices, removing unnecessary catheter at the earliest possible time, and minimizing postoperative length of stay in intensive care unit. Strict adherence to the principles of intravascular catheter management recommended by CDC can sharply reduce the incidence of catheter-related bacteremia.94,95 Surveillance using blood culture data can also facilitate choosing appropriate therapy and provide hospital antibiograms that can be used for empiric therapy of critically ill patients.96
Colonization with P. aeruginosa frequently precedes overt P. aeruginosa infection.97 Rigorous infection control precautions aimed at preventing colonization with P. aeruginosa may be important steps against bacteremia caused by MDR or XDR P. aeruginosa. Specifically, recent guidelines recommend educational programs and environmental cleaning to limit the spread of MDR P. aeruginosa.98
No other factor might be more important in the development of antimicrobial resistance of P. aeruginosa than antimicrobial use in hospitals.99 In light of recent events in antibiotic abuse, it is becoming extremely difficult to ignore the cornerstone role of antimicrobial stewardship programs, which have been shown to reduce inappropriate antimicrobial use and its consequences. The implementation of antibiotic management programs is an important strategy to reduce the dissemination of MDR or XDR P. aeruginosa.100
If serious P. aeruginosa infections occur, some measures can still be taken to prevent the occurrence of P. aeruginosa bacteremia, such as reduction of immunosuppression under close monitoring of graft function, and reduction or removal of steroids as soon as possible.
Hospital outbreaks of P. aeruginosa have been described in transplant units.101–103 Contaminated water fittings, including drinking water, tap water, faucets, showers, water outlet, sinks, and waste water system, have been reported as the sources of many outbreaks of P. aeruginosa infection.102–110 Soap, contaminated mouth swabs, or a contaminated graft can also act as a reservoir of P. aeruginosa.101,107,108
The outbreak of P. aeruginosa infection is generally considered to be the product of insufficient hand hygiene practices and contact precautions.115 The measures of terminating the outbreak of P. aeruginosa infection consist of environmental investigation, intensification of hand hygiene and isolation measures, replacing or installing contaminated reservoirs, water network hyperchlorination, excreta management, use of gloves, and the decontamination of medical utilities.101,104,105,110–113
For environmental investigation, the use of a molecular tool such as gene-based methods, for example pulsed-field gel electrophoresis or protein-based typing method involving surface-enhanced lasers desorption/ionization-time-of-flight MS, has been proposed to provide knowledge of the clonal origin of the outbreak and to find the accurate sources and transmission pathways, which are crucial for designing optimal infection control and prevention strategies and thus reduce the apparent scale of an outbreak.101,114,115 Enhancing general infection control measures including hand hygiene and isolation measures led to a reduction in clinical cases in most studies but often did not completely terminate outbreaks.116 Replacing reservoirs; point-of-use filtration; and decontaminating using bleach, hydrogen peroxide vapor, acetic acid, hot water, UV light, ozonation, and aldehyde-based disinfectants, were effective to end the outbreak.103,117 Each method has advantages and disadvantages related to ease of implementation, cost, maintenance issues, and short- and long-term effectiveness. Point-of-use filtration and replacing reservoirs were thought to be a very effective method over the long term.118,119 Acetic acid is highly effective against P. aeruginosa biofilms and may be used as a simple method to decontaminate sink drains and to prevent nosocomial transmission without evidence of indicated complete and persistent eradication of P. aeruginosa from drains.104,105,120 Bundled approaches involving enhanced general infection control measures, disinfection, and replacing seem to be most successful.105
Future research
Despite the considerable mortality and morbidity, the quest for more intensive prophylactic measures and effective treatments for P. aeruginosa bacteremia is warranted for LT recipients. However, very little was found in the literature regarding the risk factors for the development of P. aeruginosa bacteremia and the predictors of poor outcome after LT transplantation, including mortality. Furthermore, most studies provided a general comment about preventive and therapeutic measures against P. aeruginosa bacteremia, which were not centered specifically for LT recipients. Additional research is therefore needed to better identify these predictors specifically for preventive and therapeutic strategies for LT population with P. aeruginosa bacteremia.
Because inadequate empirical therapy has been shown to be an independent risk factor for mortality in SOT recipients with P. aeruginosa bacteremia, multicenter studies providing more robust and generalizable data regarding knowledge of local microbiology are urgently needed.
Given that colonization with P. aeruginosa is a precursor to overt P. aeruginosa infection, strict infection control precautions aimed at preventing colonization in high-risk LT recipients are required. However, data on the effectiveness of such strategies are lacking in LT population.43 Future management should focus on the implementation of effective preventative strategies to limit the colonization with P. aeruginosa.
Studies examining treatment measures specific to LT recipients with bacteremia caused by P. aeruginosa are also deficient, with most studies being limited by small sample size. Although LT recipients with P. aeruginosa bacteremia may be benefit from combination therapy, it is also notable that not all combinations are created equal. In vitro combination synergy studies should be performed in future clinical practices to choose the most suitable agents for the combination regimen. Further studies regarding how we can better use our existing antibiotic armamentarium are required, and the exploration of new antibiotics needs to be fully supported.
Research studies have emerged that offer new strategies against P. aeruginosa infections, including new antibiotics, β-lactamase and efflux pump inhibitors, quorum quenching molecules, and nanoparticles with antibacterial activity. Methods to prevent P. aeruginosa infection through vaccines, therapeutic antibodies, and development of antimicrobial peptides are considered to support the human immunological system. Moreover, the development of alternative/supportive therapies such as phage therapy and photodynamic therapy, in which the mechanism of action is completely different from that of the current antibiotic therapy, is of great interest.121 More funding and clinical trials are urgently needed to explore therapeutic options for MDR and XDR P. aeruginosa.
Acknowledgment
This work was supported by grant 20170311 from the New Xiangya Talent Project of the Third Xiangya Hospital of Central South University.
Disclosure
The authors report no conflicts of interest in this work.
References
McGowan JE. Resistance in nonfermenting Gram-negative bacteria: multidrug resistance to the maximum. Am J Med. 2006;119(6 Suppl 1):S29–S36. | ||
Steinberg JP, del Rio C. Other Gram-negative bacilli. In: Mandell GL, Bennet JE, Dolin R, editors. Mandell’s Principles and Practice of Infectious Diseases. Philadelphia: Elsevier; 2000:e2459–e2474. | ||
Quinn JP. Clinical problems posed by multiresistant nonfermenting Gram-negative pathogens. Clin Infect Dis. 1998;27(Suppl 1):S117–S124. | ||
Livermore DM. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: our worst nightmare? Clin Infect Dis. 2002;34(5):634–640. | ||
Bonomo RA, Szabo D. Mechanisms of multidrug resistance in Acinetobacter species and Pseudomonas aeruginosa. Clin Infect Dis. 2006;43(Suppl 2):S49–S56. | ||
Kim SI, Kim YJ, Jun YH, et al. Epidemiology and risk factors for bacteremia in 144 consecutive living-donor liver transplant recipients. Yonsei Med J. 2009;50(1):112–121. | ||
Wade JJ, Rolando N, Hayllar K, Philpott-Howard J, Casewell MW, Williams R. Bacterial and fungal infections after liver transplantation: an analysis of 284 patients. Hepatology. 1995;21(5):1328–1336. | ||
Kim HK, Park YK, Wang HJ, et al. Epidemiology and clinical features of post-transplant bloodstream infection: an analysis of 222 consecutive liver transplant recipients. Infect Chemother. 2013;45(3):315–324. | ||
Sganga G, Spanu T, Bianco G, et al. Bacterial bloodstream infections in liver transplantation: etiologic agents and antimicrobial susceptibility profiles. Transplant Proc. 2012;44(7):1973–1976. | ||
Hashimoto M, Sugawara Y, Tamura S, et al. Bloodstream infection after living donor liver transplantation. Scand J Infect Dis. 2008;40(6-7):509–516. | ||
Yes¸ilkaya A, Azap OK, Demirkaya MH, Ok MA, Arslan H, Akdur A. Bloodstream infections among solid organ transplant recipients: eight years’ experience from a Turkish University Hospital. Balkan Med J. 2013;30(3):282–286. | ||
Falagas ME, Snydman DR, Griffith J, Werner BG; The Boston Center for Liver Transplantation CMVIG Study Group. Exposure to cytomegalovirus from the donated organ is a risk factor for bacteremia in orthotopic liver transplant recipients. Clin Infect Dis. 1996;23:468–474. | ||
Kawecki D, Chmura A, Pacholczyk M, et al. Etiological agents of bacteremia in the early period after liver transplantation. Transplant Proc. 2007;39(9):2816–2821. | ||
Hashimoto M, Sugawara Y, Tamura S, et al. Pseudomonas aeruginosa infection after living-donor liver transplantation in adults. Transpl Infect Dis. 2009;11(1):11–19. | ||
George DL, Arnow PM, Fox AS, et al. Bacterial infection as a complication of liver transplantation: epidemiology and risk factors. Clin Infect Dis. 1991;13(3):387–396. | ||
McClean K, Kneteman N, Taylor G. Comparative risk of bloodstream infection in organ transplant recipients. Infect Control Hosp Epidemiol. 1994;15(9):582–584. | ||
Singh N, Paterson DL, Gayowski T, Wagener MM, Marino IR. Predicting bacteremia and bacteremic mortality in liver transplant recipients. Liver Transpl. 2000;6(1):54–61. | ||
Ouyang W, Li X, Wan Q, Ye Q. The risk factors for mortality and septic shock in liver transplant recipients with ESKAPE bacteremia. Hepatogastroenterology. 2015;62(138):346–349. | ||
Iida T, Kaido T, Yagi S, et al. Posttransplant bacteremia in adult living donor liver transplant recipients. Liver Transpl. 2010;16(12):1379–1385. | ||
Wan Q, Ye Q, Su T, Zhou J. The epidemiology and distribution of pathogens and risk factors for mortality in liver transplant recipients with Gram negative bacteremia. Hepatogastroenterology. 2014;61(134):1730–1733. | ||
Colonna JO, Winston DJ, Brill JE, et al. Infectious complications in liver transplantation. Arch Surg. 1988;123(3):360–364. | ||
Wagener MM, Yu VL. Bacteremia in transplant recipients: a prospective study of demographics, etiologic agents, risk factors, and outcomes. Am J Infect Control. 1992;20(5):239–247. | ||
Wan QQ, Ye QF, Ming YZ, et al. The risk factors for mortality in deceased donor liver transplant recipients with bloodstream infections. Transplant Proc. 2013;45(1):305–307. | ||
Al-Hasan MN, Razonable RR, Eckel-Passow JE, Baddour LM. Incidence rate and outcome of Gram-negative bloodstream infection in solid organ transplant recipients. Am J Transplant. 2009;9(4):835–843. | ||
Korvick JA, Marsh JW, Starzl TE. et a1. Pseudomonas aeruginosa bacteremia in patients undergoing liver transplantation: an emerging problem. Surgery. 1991;109:62–68. | ||
Singh N, Wagener MM, Obman A, Cacciarelli TV, de vera ME, Gayowski T. Bacteremias in liver transplant recipients: shift toward Gram-negative bacteria as predominant pathogens. Liver Transpl. 2004;10(7):844–849. | ||
Moreno A, Cervera C, Gavaldá J, et al. Bloodstream infections among transplant recipients: results of a nationwide surveillance in Spain. Am J Transplant. 2007;7(11):2579–2586. | ||
Fulginiti VA, Scribner R, Groth CG, et al. Infections in recipients of liver homografts. N Engl J Med. 1968;279(12):619–626. | ||
Munoz-Price LS, Slifkin M, Ruthazer R, et al. The clinical impact of ganciclovir prophylaxis on the occurrence of bacteremia in orthotopic liver transplant recipients. Clin Infect Dis. 2004;39(9):1293–1299. | ||
Bert F, Larroque B, Paugam-Burtz C, et al. Microbial epidemiology and outcome of bloodstream infections in liver transplant recipients: an analysis of 259 episodes. Liver Transpl. 2010;16:393–401. | ||
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16(3):128–140. | ||
Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–281. | ||
Dorotkiewicz-Jach A, Augustyniak D, Olszak T, et al. Modern therapeutic approaches against Pseudomonas aeruginosa infections. Curr Med Chem. 2015;22(14):1642–1664. | ||
Bratu S, Mooty M, Nichani S, et al. Emergence of KPC-possessing Klebsiella pneumoniae in Brooklyn, New York: epidemiology and recommendations for detection. Antimicrob Agents Chemother. 2005;49(7):3018–3020. | ||
Cuervas-Mons V, Julio Martinez A, Dekker A, Starzl TE, van Thiel DH. Adult liver transplantation: an analysis of the early causes of death in 40 consecutive cases. Hepatology. 1986;6(3):495–501. | ||
Schröter GPJ. Infections complicating orthotopic liver transplantation. Arch Surg. 1976;111(12):1337–1347. | ||
Lee SO, Kang SH, Abdel-Massih RC, Brown RA, Razonable RR. Spectrum of early-onset and late-onset bacteremias after liver transplantation: implications for management. Liver Transpl. 2011;17(6):733–741. | ||
Shi SH, Kong HS, Xu J, et al. Multidrug resistant Gram-negative bacilli as predominant bacteremic pathogens in liver transplant recipients. Transpl Infect Dis. 2009;11(5):405–412. | ||
Karvellas CJ, McPhail M, Pink F, et al. Bloodstream infection after elective liver transplantation is associated with increased mortality in patients with cirrhosis. J Crit Care. 2011;26(5):468–474. | ||
Bodro M, Sabé N, Tubau F, et al. Risk factors and outcomes of bacteremia caused by drug-resistant ESKAPE pathogens in solid-organ transplant recipients. Transplantation. 2013;96(9):843–849. | ||
Bodro M, Sabé N, Tubau F, et al. Extensively drug-resistant Pseudomonas aeruginosa bacteremia in solid organ transplant recipients. Transplantation. 2015;99(3):616–622. | ||
Linares L, García-Goez JF, Cervera C, et al. Early bacteremia after solid organ transplantation. Transplant Proc. 2009;41(6):2262–2264. | ||
Johnson LE, D’Agata EM, Paterson DL, et al. Pseudomonas aeruginosa bacteremia over a 10-year period: multidrug resistance and outcomes in transplant recipients. Transpl Infect Dis. 2009;11(3):227–234. | ||
Parkins MD, Gregson DB, Pitout JD, Ross T, Laupland KB. Population-based study of the epidemiology and the risk factors for Pseudomonas aeruginosa bloodstream infection. Infection. 2010;38(1):25–32. | ||
Yetkin G, Otlu B, Cicek A, et al. Clinical, microbiologic, and epidemiologic characteristics of Pseudomonas aeruginosa infections in a University Hospital, Malatya, Turkey. Am J Infect Control. 2006;34(4):188–192. | ||
Cox CR, Jensen KR, Saichek NR, Voorhees KJ. Strain-level bacterial identification by CeO2-catalyzed MALDI-TOF MS fatty acid analysis and comparison to commercial protein-based methods. Sci Rep. 2015;5(1):10470. | ||
Korneev KV, Arbatsky NP, Molinaro A, et al. Structural relationship of the lipid a acyl groups to activation of murine toll-like receptor 4 by lipopolysaccharides from pathogenic strains of Burkholderia mallei, Acinetobacter baumannii, and Pseudomonas aeruginosa. Front Immunol. 2015;6(3):595. | ||
di Lorenzo F, Silipo A, Bianconi I, et al. Persistent cystic fibrosis isolate Pseudomonas aeruginosa strain RP73 exhibits an under-acylated LPS structure responsible of its low inflammatory activity. Mol Immunol. 2015;63(2):166–175. | ||
Moskowitz SM, Ernst RK, Miller SI. PmrAB, a two-component regulatory system of Pseudomonas aeruginosa that modulates resistance to cationic antimicrobial peptides and addition of aminoarabinose to lipid A. J Bacteriol. 2004;186(2):575–579. | ||
Liu YY, Chandler CE, Leung LM, et al. Structural modification of lipopolysaccharide conferred by mcr-1 in Gram-negative ESKAPE pathogens. Antimicrob Agents Chemother. 2017;61(6). | ||
Florio W, Morici P, Ghelardi E, et al. Recent advances in the microbiological diagnosis of bloodstream infections. Crit Rev Microbiol. 2018;44(3):351–370. | ||
Mesaros N, Nordmann P, Plésiat P, et al. Pseudomonas aeruginosa: resistance and therapeutic options at the turn of the new millennium. Clin Microbiol Infect. 2007;13(6):560–578. | ||
Yoshihara E, Eda S. Diversity in the oligomeric channel structure of the multidrug efflux pumps in Pseudomonas aeruginosa. Microbiol Immunol. 2007;51(1):47–52. | ||
Shahcheraghi F, Nikbin VS, Feizabadi MM. Identification and genetic characterization of metallo-beta-lactamase-producing isolates of Pseudomonas aeruginosa in Tehran, Iran. New Microbiol. 2010;33:243e8. | ||
Walsh TR, Toleman MA, Poirel L, Nordmann P. Metallo-beta-lactamases: the quiet before the storm? Clin Microbiol Rev. 2005;18(2):306–325. | ||
Moyá B, Beceiro A, Cabot G, et al. Pan-β-lactam resistance development in Pseudomonas aeruginosa clinical strains: molecular mechanisms, penicillin-binding protein profiles, and binding affinities. Antimicrob Agents Chemother. 2012;56(9):4771–4778. | ||
Riera E, Cabot G, Mulet X, et al. Pseudomonas aeruginosa carbapenem resistance mechanisms in Spain: impact on the activity of imipenem, meropenem and doripenem. J Antimicrob Chemother. 2011;66(9):2022–2027. | ||
Moradali MF, Ghods S, Rehm BH. Pseudomonas aeruginosa lifestyle: a paradigm for adaptation, survival, and persistence. Front Cell Infect Microbiol. 2017;7(Pt 4):39. | ||
Sevillano E, Gallego L, García-Lobo JM. First detection of the OXA-40 carbapenemase in P. aeruginosa isolates, located on a plasmid also found in A. baumannii. Pathol Biol. 2009;57(6):493–495. | ||
El Garch F, Bogaerts P, Bebrone C, Galleni M, Glupczynski Y. OXA-198, an acquired carbapenem-hydrolyzing class D beta-lactamase from Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2011;55(10):4828–4833. | ||
McCarthy K. Pseudomonas aeruginosa: evolution of antimicrobial resistance and implications for therapy. Semin Respir Crit Care Med. 2015;36(1):44–55. | ||
Castanheira M, Toleman MA, Jones RN, Schmidt FJ, Walsh TR. Molecular characterization of a beta-lactamase gene, blaGIM-1, encoding a new subclass of metallo-beta-lactamase. Antimicrob Agents Chemother. 2004;48(12):4654–4661. | ||
Yong D, Toleman MA, Bell J, et al. Genetic and biochemical characterization of an acquired subgroup B3 metallo-β-lactamase gene, blaAIM-1, and its unique genetic context in Pseudomonas aeruginosa from Australia. Antimicrob Agents Chemother. 2012;56(12):6154–6159. | ||
Pollini S, Maradei S, Pecile P, et al. FIM-1, a new acquired metallo-β-lactamase from a Pseudomonas aeruginosa clinical isolate from Italy. Antimicrob Agents Chemother. 2013;57(1):410–416. | ||
Yong D, Toleman MA, Giske CG, et al. Characterization of a new metallo-beta-lactamase gene, bla(NDM-1), and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae sequence type 14 from India. Antimicrob Agents Chemother. 2009;53(12):5046–5054. | ||
Edelstein MV, Skleenova EN, Shevchenko OV, et al. Spread of extensively resistant VIM-2-positive ST235 Pseudomonas aeruginosa in Belarus, Kazakhstan, and Russia: a longitudinal epidemiological and clinical study. Lancet Infect Dis. 2013;13(10):867–876. | ||
Livermore DM. Of Pseudomonas, porins, pumps and carbapenems. J Antimicrob Chemother. 2001;47(3):247–250. | ||
Lister PD, Wolter DJ, Hanson ND. Antibacterial-resistant Pseudomonas aeruginosa: clinical impact and complex regulation of chromosomally encoded resistance mechanisms. Clin Microbiol Rev. 2009;22(4):582–610. | ||
Krishnaraju M, Kamatchi C, Jha AK, et al. Complete sequencing of an IncX3 plasmid carrying blaNDM-5 allele reveals an early stage in the dissemination of the blaNDM gene. Indian J Med Microbiol. 2015;33(1):30–38. | ||
Liu Y, Deng Q, Yu Y, Cao X, Xu Q, Wan L. Analysis of the resistance mechanism and homology of carbapenems-resistant Pseudomonas aeruginosa. Zhonghua Shao Shang Za Zhi. 2014;30(1):15–20. | ||
Niga T, Ito H, Oyamada Y, et al. Cooperation between alteration of DNA gyrase genes and over-expression of MexB and MexX confers high-level fluoroquinolone resistance in Pseudomonas aeruginosa strains isolated from a patient who received a liver transplant followed by treatment with fluoroquinolones. Microbiol Immunol. 2005;49(5):443–446. | ||
Tam VH, Rogers CA, Chang KT, Weston JS, Caeiro JP, Garey KW. Impact of multidrug-resistant Pseudomonas aeruginosa bacteremia on patient outcomes. Antimicrob Agents Chemother. 2010;54(9):3717–3722. | ||
Cervera C, van Delden C, Gavaldà J, et al. Multidrug-resistant bacteria in solid organ transplant recipients. Clin Microbiol Infect. 2014;20(Suppl 7):49–73. | ||
Meachery G, de Soyza A, Nicholson A, et al. Outcomes of lung transplantation for cystic fibrosis in a large UK cohort. Thorax. 2008;63(8):725–731. | ||
Boussaud V, Guillemain R, Grenet D, et al. Clinical outcome following lung transplantation in patients with cystic fibrosis colonised with Burkholderia cepacia complex: results from two French centres. Thorax. 2008;63(8):732–737. | ||
Alexander BD, Petzold EW, Reller LB, et al. Survival after lung transplantation of cystic fibrosis patients infected with Burkholderia cepacia complex. Am J Transplant. 2008;8(5):1025–1030. | ||
Al-Hasan MN, Wilson JW, Lahr BD, et al. The role of beta-lactam and fluoroquinolone combination antibiotic therapy in Gram-negative bacteremia. Antimicrob Agents Chemother. 2009;53:1386–1394. | ||
Aoki N, Tateda K, Kikuchi Y, et al. Efficacy of colistin combination therapy in a mouse model of pneumonia caused by multidrug-resistant Pseudomonas aeruginosa. J Antimicrob Chemother. 2009;63(3):534–542. | ||
Pankuch GA, Lin G, Seifert H, Appelbaum PC. Activity of meropenem with and without ciprofloxacin and colistin against Pseudomonas aeruginosa and Acinetobacter baumannii. Antimicrob Agents Chemother. 2008;52(1):333–336. | ||
Sun HY, Shields RK, Cacciarelli TV, Muder RR, Singh N. A novel combination regimen for the treatment of refractory bacteremia due to multidrug-resistant Pseudomonas aeruginosa in a liver transplant recipient. Transpl Infect Dis. 2010;12(6):555–560. | ||
Averbuch D, Cordonnier C, Livermore DM, et al. Targeted therapy against multi-resistant bacteria in leukemic and hematopoietic stem cell transplant recipients: guidelines of the 4th European Conference on Infections in Leukemia (ECIL-4, 2011). Haematologica. 2013;98(12):1836–1847. | ||
Bowers DR, Liew YX, Lye DC, Kwa AL, Hsu LY, Tam VH. Outcomes of appropriate empiric combination versus monotherapy for Pseudomonas aeruginosa bacteremia. Antimicrob Agents Chemother. 2013;57(3):1270–1274. | ||
Peña C, Suarez C, Ocampo-Sosa A, et al. Effect of adequate single-drug vs combination antimicrobial therapy on mortality in Pseudomonas aeruginosa bloodstream infections: a post hoc analysis of a prospective cohort. Clin Infect Dis. 2013;57(2):208–216. | ||
Hu Y, Li L, Li W, et al. Combination antibiotic therapy versus monotherapy for Pseudomonas aeruginosa bacteraemia: a meta-analysis of retrospective and prospective studies. Int J Antimicrob Agents. 2013;42(6):492–496. | ||
Juan C, Zamorano L, Perez JL, et al. Activity of a new antipseudomonal cephalosporin, CXA-101 (FR264205), against carbapenem-resistant and multidrug-resistant Pseudomonas aeruginosa clinical strains. Antimicrob Agents Chemother. 2010;54(2):846–851. | ||
Sader HS, Rhomberg PR, Farrell DJ, et al. Antimicrobial activity of CXA-101, a novel cephalosporin tested in combination with tazobactam against Enterobacteriaceae, Pseudomonas aeruginosa, and Bacteroides fragilis strains having various resistance phenotypes. Antimicrob Agents Chemother. 2011;55(5):2390–2394. | ||
Díaz-Cañestro M, Periañez L, Mulet X, et al. Ceftolozane/tazobactam for the treatment of multidrug resistant Pseudomonas aeruginosa: experience from the Balearic Islands. Eur J Clin Microbiol Infect Dis. 2018;37(11):2191–2200. | ||
Rodríguez-Núñez O, Ripa M, Morata L, et al. Evaluation of ceftazidime-avibactam for serious infections due to multidrug and extensive drug resistant Pseudomonas aeruginosa. J Glob Antimicrob Resist. 2018;15:136–139. | ||
Almarzoky Abuhussain SS, Kuti JL, Nicolau DP. Antibacterial activity of human simulated epithelial lining fluid concentrations of ceftazidime-avibactam alone or in combination with amikacin inhale (BAY41-6551) against carbapenem-resistant Pseudomonas aeruginosa and Klebsiella pneumoniae. Antimicrob Agents Chemother. 2018;62(7). | ||
Fischer SA, Avery RK; AST Infectious Disease Community of Practice. Screening of donor and recipient prior to solid organ transplantation. Am J Transplant. 2009;9(Suppl 1):S7–S18. | ||
Agodi A, Barchitta M, Cipresso R, Giaquinta L, Romeo MA, Denaro C. Pseudomonas aeruginosa carriage, colonization, and infection in ICU patients. Intensive Care Med. 2007;33(7):1155–1161. | ||
Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med. 2000;132(5):391–402. | ||
Saiman L, Siegel J; Cystic Fibrosis Foundation. Infection control recommendations for patients with cystic fibrosis: microbiology, important pathogens, and infection control practices to prevent patient to patient transmission. Infect Control Hosp Epidemiol. 2003;24: S6–S52. | ||
Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16(3):128–140. | ||
Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–2732. | ||
Kajumbula H, Fujita AW, Mbabazi O, et al. Antimicrobial drug resistance in blood culture isolates at a tertiary hospital, Uganda. Emerg Infect Dis. 2018;24(1):174–175. | ||
Pollack M. Pseudomonas aeruginosa. Principles and Practice of Infectious Diseases. 4th ed. NewYork, NY: Churchill Livingstone Inc; 2000:2310–2334. | ||
Tacconelli E, Cataldo MA, Dancer SJ, et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin Microbiol Infect. 2014;20(Suppl 1):1–55. | ||
Gaynes R. The impact of antimicrobial use on the emergence of antimicrobial-resistant bacteria in hospitals. Infect Dis Clin North Am. 1997;11(4):757–765. | ||
Kritikos A, Manuel O. Bloodstream infections after solid-organ transplantation. Virulence. 2016;7(3):329–340. | ||
Fanci R, Bartolozzi B, Sergi S, et al. Molecular epidemiological investigation of an outbreak of Pseudomonas aeruginosa infection in an SCT unit. Bone Marrow Transplant. 2009;43(4):335–338. | ||
Wong V, Levi K, Baddal B, Turton J, Boswell TC. Spread of Pseudomonas fluorescens due to contaminated drinking water in a bone marrow transplant unit. J Clin Microbiol. 2011;49(6):2093–2096. | ||
Ambrogi V, Cavalié L, Mantion B, et al. Transmission of metallo-β-lactamase-producing Pseudomonas aeruginosa in a nephrology-transplant intensive care unit with potential link to the environment. J Hosp Infect. 2016;92(1):27–29. | ||
Stjärne Aspelund A, Sjöström K, Olsson Liljequist B, Mörgelin M, Melander E, Påhlman LI. Acetic acid as a decontamination method for sink drains in a nosocomial outbreak of metallo-β-lactamase-producing Pseudomonas aeruginosa. J Hosp Infect. 2016;94(1):13–20. | ||
Gbaguidi-Haore H, Varin A, Cholley P, et al. A bundle of measures to control an outbreak of Pseudomonas aeruginosa associated with P-trap contamination. Infect Control Hosp Epidemiol. 2018;39(2):164–169. | ||
Kanamori H, Weber DJ, Rutala WA. Healthcare outbreaks associated with a water reservoir and infection prevention strategies. Clin Infect Dis. 2016;62(11):1423–1435. | ||
Iversen BG. Contaminated mouth swabs caused a multi-hospital outbreak of Pseudomonas aeruginosa infection. J Oral Microbiol. 2010;2:5123. | ||
Kumar D, Cattral MS, Robicsek A, Gaudreau C, Humar A. Outbreak of Pseudomonas aeruginosa by multiple organ transplantation from a common donor. Transplantation. 2003;75(7):1053–1055. | ||
Sato A, Kaido T, Iida T, et al. Bundled strategies against infection after liver transplantation: lessons from multidrug-resistant Pseudomonas aeruginosa. Liver Transpl. 2016;22(4):436–445. | ||
Decraene V, Ghebrehewet S, Dardamissis E, et al. An outbreak of multidrug-resistant Pseudomonas aeruginosa in a burns service in the North of England: challenges of infection prevention and control in a complex setting. J Hosp Infect. 2018. pii: S0195–6701(18)30376–1. | ||
Breathnach AS, Cubbon MD, Karunaharan RN, Pope CF, Planche TD. Multidrug-resistant Pseudomonas aeruginosa outbreaks in two hospitals: association with contaminated hospital waste-water systems. J Hosp Infect. 2012;82(1):19–24. | ||
Tran-Dinh A, Neulier C, Amara M, et al. Impact of the relocation of an ICU and role of tap water on an outbreak of Pseudomonas aeruginosa expressing OprD-mediated resistance to imipenem. J Hosp Infect. 2018. | ||
Vianelli N, Giannini MB, Quarti C, et al. Resolution of a Pseudomonas aeruginosa outbreak in a hematology unit with the use of disposable sterile water filters. Haematologica. 2006;91(7):983–985. | ||
Yun HC, Tully CC, Mende K, Castillo M, Murray CK. A single-center, six-year evaluation of the role of pulsed-field gel electrophoresis in suspected burn center outbreaks. Burns. 2016;42(6):1323–1330. | ||
Song M, Tang M, Ding Y, et al. Application of protein typing in molecular epidemiological investigation of nosocomial infection outbreak of aminoglycoside-resistant Pseudomonas aeruginosa. Environ Sci Pollut Res Int. 2018;25(23):22437–22445. | ||
Kizny Gordon AE, Mathers AJ, Cheong EYL, et al. The hospital water environment as a reservoir for carbapenem-resistant organisms causing hospital-acquired infections-a systematic review of the literature. Clin Infect Dis. 2017;64(10):1435–1444. | ||
Seara N, Oteo J, Carrillo R, et al. Interhospital spread of NDM-7-producing Klebsiella pneumoniae belonging to ST437 in Spain. Int J Antimicrob Agents. 2015;46(2):169–173. | ||
Ortolano GA, McAlister MB, Angelbeck JA, et al. Hospital water point-of-use filtration: a complementary strategy to reduce the risk of nosocomial infection. Am J Infect Control. 2005;33(5 Suppl 1):S1–S19. | ||
Cervia JS, Ortolano GA, Canonica FP. Hospital tap water: a reservoir of risk for healthcare-associated infection. Infect Dis Clin Pract. 2008;16(6):349–353. | ||
Bjarnsholt T, Alhede M, Jensen PØ, et al. Antibiofilm properties of acetic acid. Adv Wound Care. 2015;4(7):363–372. | ||
Dorotkiewicz-Jach A, Augustyniak D, Olszak T, Drulis-Kawa Z. Modern therapeutic approaches against Pseudomonas aeruginosa infections. Curr Med Chem. 2015;22(14):1642–1664. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.