")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 11
Protective Effects of Parental Education Against Youth Cigarette Smoking: Diminished Returns of Blacks and Hispanics
Authors Assari S , Mistry R, Caldwell CH, Bazargan M
Received 13 November 2019
Accepted for publication 8 February 2020
Published 22 May 2020 Volume 2020:11 Pages 63—71
DOI https://doi.org/10.2147/AHMT.S238441
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Alastair Sutcliffe
Shervin Assari,1 Ritesh Mistry,2 Cleopatra H Caldwell,2 Mohsen Bazargan1,3
1College of Medicine, Charles R Drew University of Medicine and Science, Los Angeles, CA 90059, USA; 2Department of Health Behavior and Health Education, University of Michigan School of Public Health, Ann Arbor, MI, 48109, USA; 3Department of Family Medicine, University of California, Los Angeles (UCLA), Los Angeles, CA, 90095, USA
Correspondence: Shervin Assari
Department of Family Medicine, Charles R. Drew University of Medicine and Science, 1731 E. 120th St., Los Angeles, CA 90059, USA
Email [email protected]
Background: High parental educational attainment is protective against youth health risk behaviors such as tobacco use. According to the Marginalization-related Diminished Returns (MDRs) theory, however, higher parental education is less protective for marginalized groups relative to non-Hispanic Whites.
Objective: To explore race/ethnic differences in the effects of parental educational attainment on cigarette smoking in a national sample of American adolescents.
Methods: In a cross-sectional study, we used baseline data of 10,878 American youth who had participated in the Population Assessment of Tobacco and Health (PATH 2013). The independent variable was parental educational attainment. The dependent variables were lifetime cigarette smoking, current (past 30-day) cigarette moking, and daily cigarette smoking. Youth age, youth gender, and parental marital status were the covariates. Race/ethnicity was the moderating variable. Logistic regression model was used for data analysis.
Results: Overall, a higher parental educational attainment was associated with a lower lifetime cigarette smoking, current (past 30-day) cigarette smoking, and daily cigarette smoking. Parental educational attainment showed significant interaction with race/ethnicity suggesting smaller protective effects of parental educational attainment on youth tobacco outcomes for Black and Hispanic than for non-Hispanic White youth.
Conclusion: For American youth, race/ethnicity limits the health gains that are expected to follow parental educational attainment. While high parental educational attainment is protective against smoking overall, non-Hispanic Whites (the most socially privileged group) gain most and Blacks and Hispanics (the least socially privileged groups) gain least from such resource. In addition to addressing low SES, researchers and policymakers should identify and address mechanisms by which high SES minority youth remain at risk of tobacco use.
Keywords: education, smoking, tobacco use, population groups, ethnicity, socioeconomic position, socioeconomic status, youth, adolescents
Background
Tobacco is still among the leading preventable causes of disease in the US.1–3 About 480,000 Americans die from tobacco-related illnesses annually. In addition, more than 16 million Americans are impacted by diseases caused by smoking.4 These tobacco-related illnesses cost the US more than $300 billion each year. Unfortunately, there is an unequal health burden from tobacco use in the US.4 Despite the progress in reducing overall morbidity and mortality attributed to smoking, tobacco use has shifted from a mainstream behavior to a one that is largely concentrated among marginalized populations defined by SES and race/ethnicity.5
Pervasive disparities in the health burden of tobacco use by race/ethnicity6–10 and socioeconomic status (SES)11–13 exist in the US. In addition, despite the overall decline in tobacco use rates, disparities across SES groups have increased.13–15 Between 1966 and 2015, smoking declined by 83% in individuals with a college degree, while the decline for individuals without a high school diploma was almost half (40%). A large proportion of such disparities may not be due to individuals making poor choices but to predatory marketing.16–18 Low SES individuals and ethnic minorities are at an increased risk for point-of-sale advertising, retail display, coupons, and discounts.19 The result is their increasing vulnerability20 which is exacerbated by low access to smoking cessation programs.8,21,22
Marginalization-related Diminished Returns (MDRs) refer to “less than expected” health effects of SES resources particularly educational attainment for socially marginalized compared the socially privileged population.23,24 These patterns are persistent and suggest that: (a) not all race/ethnic disparities are caused by SES gaps but also by differential health gains from social and economic resources for Black and Hispanic compared to White populations, and (b) race/ethnic gaps in a wide range of outcomes increase as SES increases. These unexpected patterns suggest the need to address disparities across all SES spectrum.23,24
Research has suggested that MDRs may also apply to understand racial/ethnic differences in tobacco25,26 and alcohol27 use in adults.25,26,28 In a study using a national random sample of White and Black older adults, educational attainment showed a stronger association with alcohol use among Whites than among Blacks.27 In a study using the National Survey of American Life (NSAL), educational attainment showed a smaller protective effect on smoking among Black adults than among White adults.25 In another study that used a representative sample Los Angeles residents, employment had a larger protective effect against smoking for non-Hispanic than for Hispanic adults.26 Several studies have also shown that parental educational attainment also generates less tangible health outcomes for Black and Hispanic youth than for non-Hispanic white youth.29–35
Using data from a nationally representative sample of US adolescents, we performed this study to explore whether adolescents’ race/ethnicity alters the effects of parental educational attainment (family SES) on tobacco use. We hypothesized that the protective effect of family SES on youth tobacco use would be smaller in Black and Hispanic than in Non-Hispanic White youth.
Methods
Design and Settings
This is a secondary analysis of wave 1 data from the Population Assessment of Tobacco and Health (PATH). Funded by the NIH and the FDA, PATH is the state-of-the-art study on tobacco use in the US. PATH has enrolled about 49,000 people 12 years or older. Wave 1 data were collected in 2013–2014.
Sample and Sampling
The PATH study’s adolescent sample in Wave 1 was the civilian, non-institutionalized, US population 12–17 years old in the US. The PATH study used a four-stage stratified area probability sample design to recruit participants. At the 1st stage, a stratified sample of geographical primary sampling units (PSUs, n = 156) was selected. The PATH PSUs were counties or a group of counties. The 2nd stage was formed from sampled smaller geographical segments in each PSU. The 3rd stage sampled residential addresses. The fourth stage was the selection of one adolescent and adult participant within households. Participants completed a questionnaire using an Audio Computer-Assisted Self-Interview system. This study only includes data on adolescents (n=10,878).
Study Variables
The study variables included adolescent age, gender, race/ethnicity and tobacco use. Parental educational attainment (indicator of SES) and marital status were also included.
Independent Variable
Parental educational attainment. Parental educational attainment was measured as a continuous variable ranging from 1 to 5: (1) “less than high school”, (2) “GED or high school graduate”, (3) “some college (no degree) or associates degree”, (4) “Bachelor’s degree”, and (5) “advanced degree”. Separate questions were asked for mother’s and father’s educational attainment. We created a parental educational attainment variable by using the higher of the two reported educational levels.
Moderator Variables
Race/ethnicity. Adolescent race/ethnicity was used as moderator variable and was operationalized as a three-level categorical variable: Black, Hispanic, and Non-Hispanic White.
Demographic Confounders
Age, gender, and family structure. Age was measured as a dichotomous variable: 1) 12 to 15 years old, 2) 16 to 17 years old. Gender was a dichotomous variable. Parental family structure was a dichotomous variable; 1= married, 0 = otherwise. Cohabiting parents were not collapsed with married parents because cohabiting parents are still unmarried.
Dependent Variables
Cigarette Use. Dependent variables were ever, current (past 30-day) and daily cigarette smoking. Ever use was measured using the following question: “Did you ever try cigarette smoking, even one or two puffs?”(1=Yes, 0=No). Current cigarette smoking was measured by asking participants the number of cigarettes they smoked in the past 30 days (1=smoked 1 or more days, 0=did not smoke). Those who said they said they use tobacco were asked about number of days they smoked during the past 30 days question. So, we could identify individuals who smoked everyday over the past 30 days. “Every day” was coded as 1 if the person had smoked all the 30 days and 0 if the person had not smoked or had smoked less than 30 days. (1 smoked every day in the last month, 0 did not smoke all days in the last month).
Conceptual Model
Figure 1 shows the conceptual model of the study. Building on the concept of MDRs, our study focused on interactions between adolescent race/ethnicity and parental educational attainment on cigarette use. The predictor of interest was parental educational attainment and we were predominantly interested in the differential effects of parental educational attainment on adolescent tobacco use outcomes based on adolescent race/ethnicity. We expected high parental education (family SES) to reduce the risk of adolescent tobacco use, but the reduction in risk would be smaller in Black and Hispanic compared to White adolescents. We expect results for Blacks and Hispanics to have similar patterns, because many social processes such as discrimination operate similarly across various marginalized groups.36
 |
Figure 1 Conceptual model of Marginalization-related Diminished Returns (MDRs) for youth tobacco use. |
Data Analytical Plan
As we were interested in the cross-sectional association between family SES (parental educational attainment) and tobacco use outcomes, we limited the analysis to wave 1 (baseline) data. We analyzed the data using SPSS 23.0 (IBM Corporation, Armonk, NY, USA). Since the PATH study uses a complex multi-stage sampling design and provides survey weights to makes results generalizable to the US population, we applied the weights and used Taylor series linearization for variance estimation. We first explored the distribution of our categorical and continuous variables. We then ruled out collinearity between race/ethnicity, parental educational attainment, and parental marital status. For univariate analysis, we used a frequency table. Next, we used multivariable logistic regression analysis with lifetime, current, and daily cigarette smoking as outcomes. First, we ran models in the pooled samples. The first model always had no interaction terms. To assess moderation, Model 2 included two interaction terms between race/ethnicity and parental educational attainment. Finally, we further assessed moderation by stratifying the regression models by race/ethnicity.
Ethics
All adolescent participants in the PATH study provided written assent. Their parents or guardians also provided permission and consent to be interviewed. Westat’s institutional review board approved the PATH’s study protocol. We, however, used the PATH public data set which is fully deidentified. As a result, the current analysis was non-human research and was exempt from an IRB review. PATH data are publicly available at the ICPSR website.
Results
Descriptive Statistics
This study included 10,878 American youth. Table 1 shows the descriptive data in the total sample.
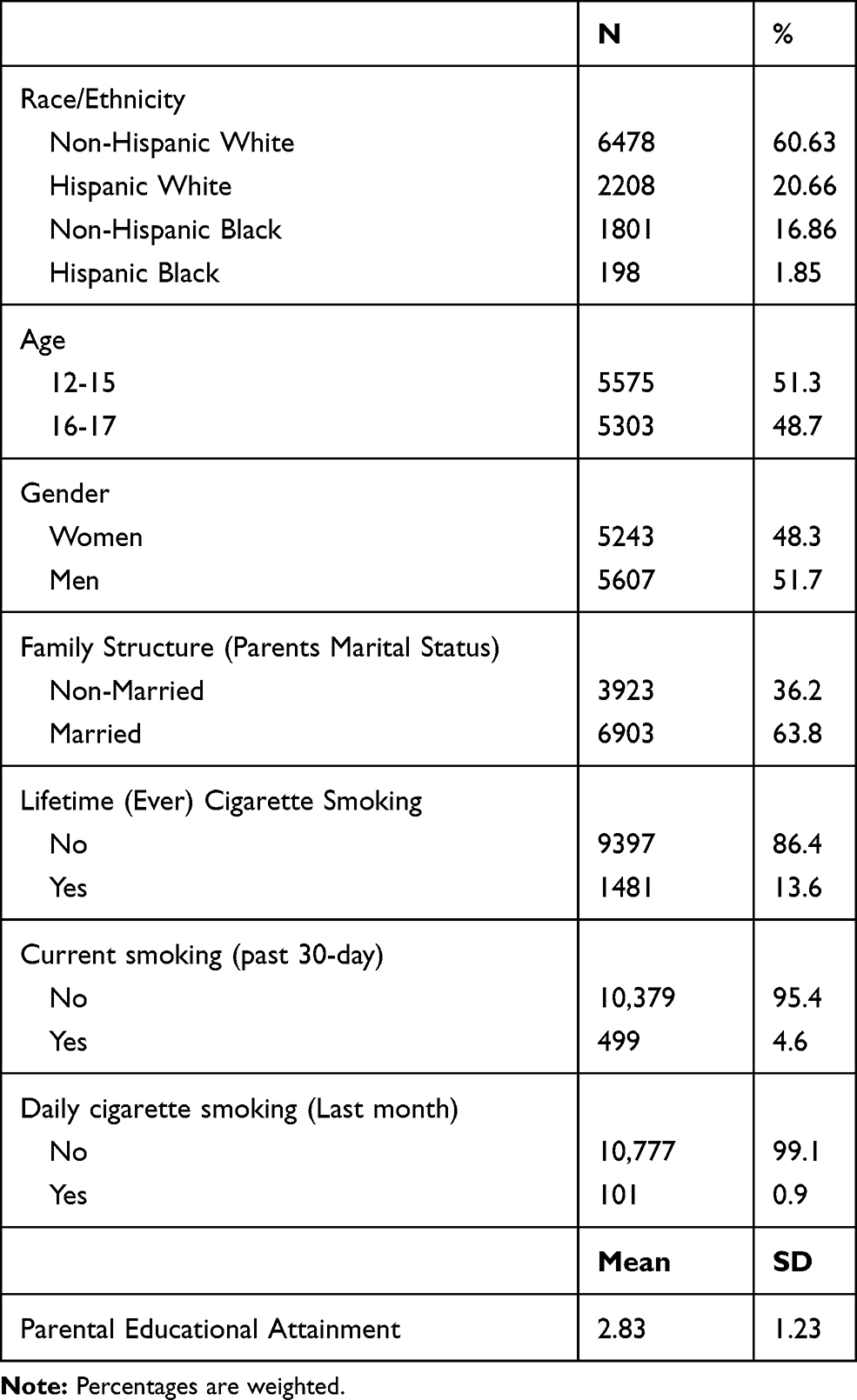 |
Table 1 Descriptive Statistics (n = 10,878) |
Multivariable Models
Table 2 presents the summary of the results of two nested logistic regression models with parental educational attainment as the independent variable and tobacco use outcomes as the dependent variables. Both models were estimated in the pooled sample. While Model 1 only entered the main effects of parental educational attainment, race, ethnicity, and covariates, Model 2 also included two interaction terms between race and ethnicity with parental educational attainment. These models are shown for (a) lifetime cigarette smoking (Ever), (b) last month cigarette smoking (30 Days), and (c) daily cigarette smoking (30 Days).
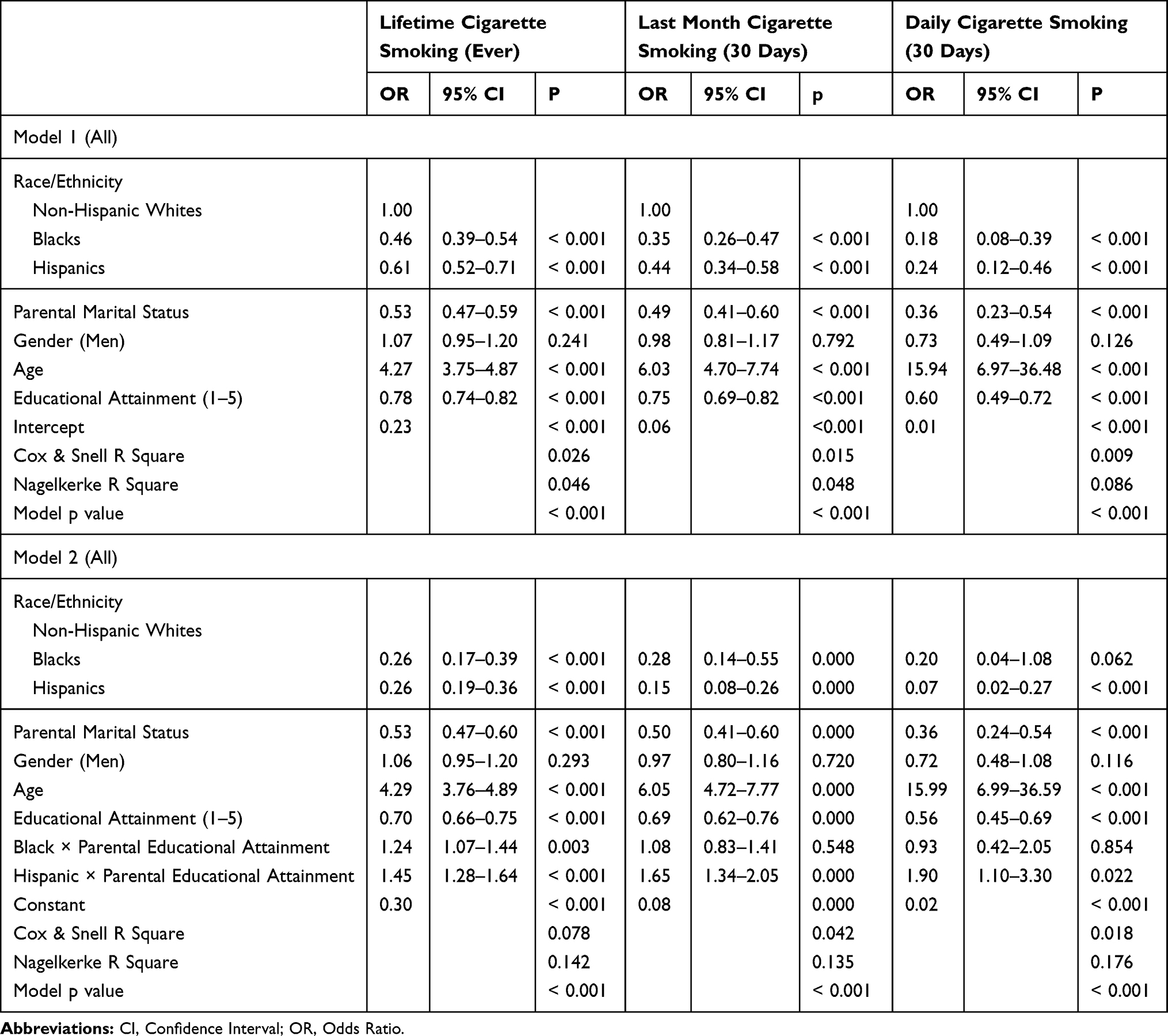 |
Table 2 Logistic Regressions on Ever, Current and Daily Cigarette Smoking in the Pooled Sample |
Based on Model 1, high parental educational attainment was associated with lower odds of tobacco use (all outcomes). Although there were some inconsistencies, Model 2 showed statistically significant interactions between both race and ethnicity with parental educational attainment on youth tobacco use indicators, that suggests a higher parental educational attainment has a smaller protective effect on youth tobacco use outcomes for Black and Hispanic than non-Hispanic White families (Table 2).
Table 3 presents the results of race/ethnicity-stratified logistic regression models with Lifetime cigarette smoking (Ever), last month cigarette smoking (30 Days), and daily cigarette smoking (30 Days) as the dependent variable and parental educational attainment as the independent variable. Model 1, Model 2, Model 3, and Model 4 were performed in non-Hispanics, Hispanics, Whites, and Blacks. Based on Model 1 and Model 3, high parental education was associated with less tobacco use in non-Hispanics and Whites. Model 2 and Model 4 did not show any statistically significant association between parental educational attainment and youth tobacco use in Hispanics and Blacks (Table 3).
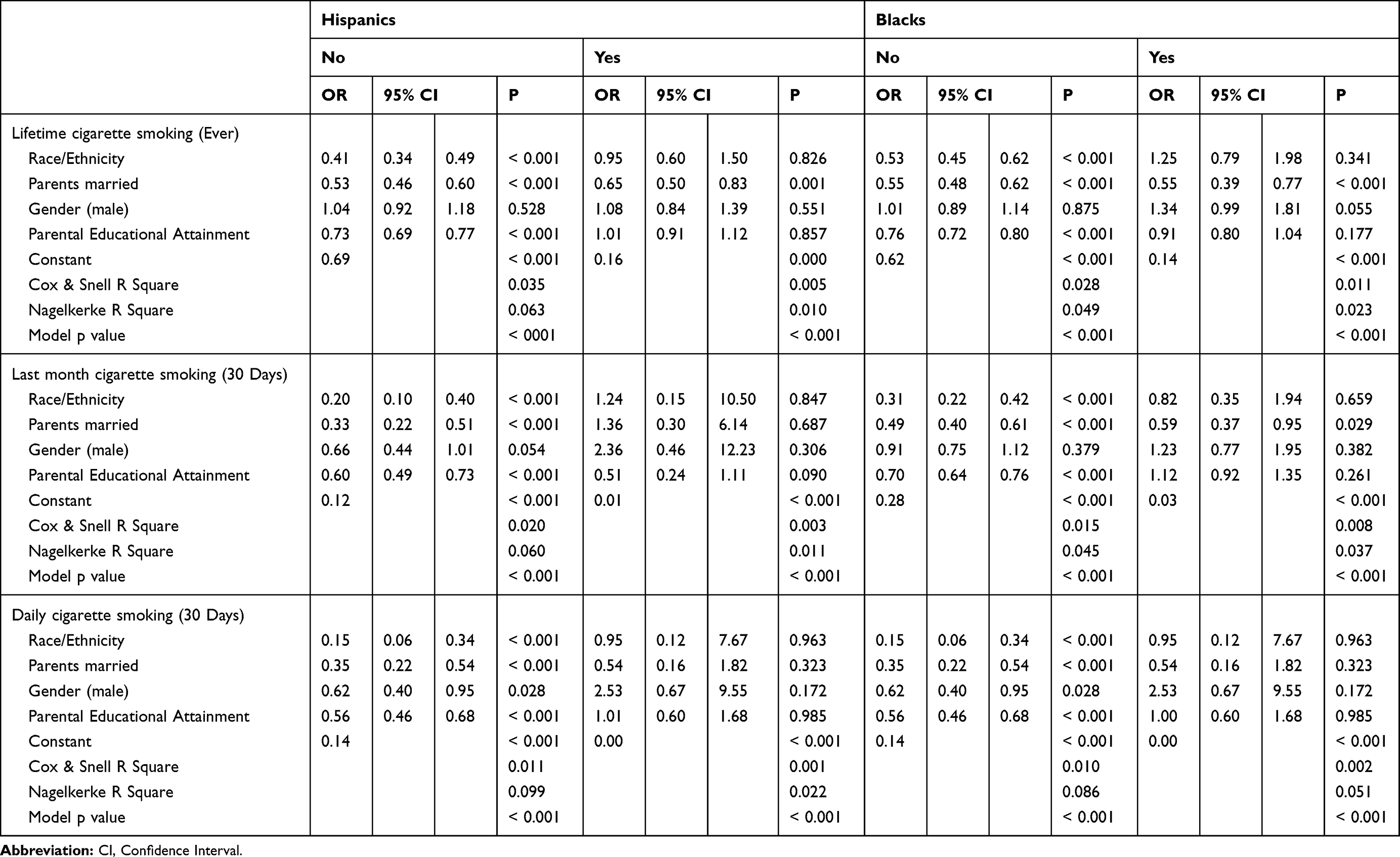 |
Table 3 Logistic Regressions on Tobacco Use by Race/Ethnicity |
Discussion
The current study produced two findings. First, in the overall sample, parental educational attainment was inversely associated with youth tobacco use, across outcomes. Second, race/ethnicity showed statistical interactions with parental education: parental education level showed weaker protective effects on reducing youth tobacco use for Black and Hispanic families than for non-Hispanic White families. Race/ethnicity stratified logistic regressions showed similar results.
Our findings are in line with our previous work showing that high SES (e.g., educational attainment, income, marital status, and employment) Blacks and Hispanics remain at a disproportionately high risk of substance use, a level which is not expected given their SES.25,27,28,37 These patterns are consistent with what we know about the impact of SES on other health outcomes. The effects of educational attainment,30 income,38 employment,39 and marital status40 on diet,41 obesity,34 substance use,28 depression,38 happiness,42 affect,42 anxiety,40 self-rated health,43 chronic disease,44 oral health,31 hospitalization,45 disability,46 and mortality39 are all smaller for Blacks and Hispanics than for non-Hispanic Whites.
In a recent study, higher parental education reduced a wide range of behavioral risks for non- Hispanic White adolescents more than for Black and Hispanic adolescents.47 In one study, high education and income had weaker protective effect on reducing the risk of tobacco use for Hispanics than their White counterparts.48 In other studies, highly educated Blacks remained at higher risk of smoking and vaping, however education was reducing the risk of smoking and vaping for Whites.25,49 Another study showed similar findings for Native Americans for whom education showed weaker than expected protective effect against tobacco use.50 Furthermore, high SES LGBT were at higher risk of tobacco use than high SES heterosexuals, due to a weaker than expected effects of education on their smoking.51 The universal nature of MDRs suggests that marginalized people experience fewer protective effects of access to SES resources such as education. As a result, these patterns of MDRs can be attributed to social stratification, contextual factors, and unequal treatment rather than the behavioral choice of specific racial, ethnic or sexual minority groups.51
There is a need to conduct more studies that help us understand the role of predatory marketing practices on racial/ethnic and SES disparities in tobacco use. We argue that structural factors such as predatory marketing may generate MDRs on tobacco use of non-White youth. That is, predatory marketing and advertising may impose additional risk of tobacco use to high SES Black and Hispanic individuals through reducing the effects of SES. SES is shown to have smaller effects for Blacks and Hispanics to bring them out of poor urban areas.52 High SES Black and Hispanic youth may be exposed to a high density of tobacco retails and advertisements. Introducing more restrictive tobacco marketing regulations may be particularly beneficial to Black and Hispanic populations. Example policies include banning point-of-sale advertisement, flavoring, coupons and discounts. However, all these hypotheses need additional research.
Implications
The results may have some policy and public health implications. The results help increase “understanding [of] why people become susceptible to using tobacco products”.53 The results may contribute to the development of public policies designed to address tobacco-related disparities such as more restrictive national and local marketing and other policies.54 Fortunately, the literature shows that currently Americans tend to positively evaluate tobacco control regulations and do not view them as against their autonomy.54
There is a need for both national and local policies that may successfully reduce the effect of MDRs on tobacco use and other health outcomes.24,25,28,31,32,34,37,40,55,56 We need to study the roles of discounts, coupons, flavoring, density of tobacco retails in shaping MDRs-related disparities in tobacco use.25,28 Similarly, we need to study the role of tobacco control policies and regulations that may minimize MDRs-related tobacco disparities. It is essential to explore how these marketing strategies target low SES Black and Hispanic communities.25,27,28,37 To undo race/ethnic disparities in tobacco use, there is a need to stop predatory tobacco marketing in low-income areas. We argue that understanding MDRs helps with developing such strategies.
Limitations
This study had some methodological limitations. The cross-sectional design of our study limits any causal inferences. Sample size was imbalanced across race/ethnic groups and tobacco use outcomes. Income, employment, marital status, as well as area-level SES factors were not included in this study. This study did not measure tobacco control policies that vary based on the geographic location of the participants. Despite these limitations, this study still contributes to the existing literature on adolescent tobacco use. For Daily cigarette smoking (Last month), less than 1% were positive. So, this outcome was very skewed. Our sample size was large, sampling was random, the results were generalizable to the US, and multiple tobacco use outcomes were studied. Still, more research is needed on the mechanisms of MDRs of parental educational attainment on youth tobacco use.
Conclusion
In the United States, minority youth are at a relative disadvantage compared to White youth in gaining tobacco use prevention benefits from their family SES (parental educational attainment). While higher parental educational attainment helped adolescents have lower tobacco use, this pattern is more pronounced in the most privileged group (whites) compared to marginalized groups (Blacks and Hispanics). As a result, we should expect a higher than expected risk of tobacco use in Black and Hispanic youth from high SES families. Race/ethnic disparities in tobacco use may be generated by factors beyond SES families. Research should explore structural factors that contribute to the reduced protective effects of parental education on tobacco use of middle-class Black and Hispanic youth.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health (NIH) and FDA Center for Tobacco Products (CTP) under Award Number U54CA229974. Shervin Assari is also funded by the NIH (NIMHD) under Award S21MD000103. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration.
Disclosure
The authors declare no conflict of interest.
References
1. McCarthy M. Smoking remains leading cause of premature death in US. BMJ. 2014;348:g396. doi:10.1136/bmj.g396
2. Samet JM. Tobacco smoking: the leading cause of preventable disease worldwide. Thorac Surg Clin. 2013;23(2):103–112. doi:10.1016/j.thorsurg.2013.01.009
3. Novick LF. Smoking is the leading preventable cause of death and disability in the United States. J Public Health Manag Pract. 2000;6(3):vi. doi:10.1097/00124784-200006030-00001
4. CDC. Smoking & Tobacco Use. Fast Facts; 2019.
5. Yang T, Jiang S, Barnett R, et al. Who smokes in smoke-free public places in China? Findings from a 21 city survey. Health Educ Res. 2016;31(1):36–47. doi:10.1093/her/cyv054
6. Ellickson PL, Orlando M, Tucker JS, Klein DJ. From adolescence to young adulthood: racial/ethnic disparities in smoking. Am J Public Health. 2004;94(2):293–299. doi:10.2105/AJPH.94.2.293
7. Centers for Disease C, Prevention. Racial disparities in smoking-attributable mortality and years of potential life lost — Missouri, 2003-2007. MMWR Morb Mortal Wkly Rep. 2010;59(46):1518–1522.
8. Trinidad DR, Perez-stable EJ, White MM, Emery SL, Messer K. A nationwide analysis of US racial/ethnic disparities in smoking behaviors, smoking cessation, and cessation-related factors. Am J Public Health. 2011;101(4):699–706. doi:10.2105/AJPH.2010.191668
9. Soulakova JN, Huang H, Crockett LJ. Racial/ethnic disparities in consistent reporting of smoking-related behaviors. J Addict Behav Ther Rehabil. 2015;4(4). doi:10.4172/2324-9005.1000147
10. Blumenthal DS. Racial and ethnic disparities in smoking prevalence in Israel and the United States: progress to date and prospects for the future. Isr J Health Policy Res. 2017;6(1):51. doi:10.1186/s13584-017-0177-9
11. Laveist TA, Thorpe RJ
12. Reid JL, Hammond D, Driezen P. Socio-economic status and smoking in Canada, 1999-2006: has there been any progress on disparities in tobacco use? Can J Public Health. 2010;101(1):73–78. doi:10.1007/BF03405567
13. Zhang X, Martinez-donate AP, Jones NR. Educational disparities in home smoking bans among households with underage children in the United States: can tobacco control policies help to narrow the gap? Nicotine Tob Res. 2013;15(12):1978–1987. doi:10.1093/ntr/ntt090
14. Reimer RA, Gerrard M, Gibbons FX. Racial disparities in smoking knowledge among current smokers: data from the health information national trends surveys. Psychol Health. 2010;25(8):943–959. doi:10.1080/08870440902935913
15. Rock VJ, Davis SP, Thorne SL, Asman KJ, Caraballo RS. Menthol cigarette use among racial and ethnic groups in the United States, 2004-2008. Nicotine Tob Res. 2010;12(Suppl 2):S117–S124. doi:10.1093/ntr/ntq204
16. Terry-mcelrath YM, Wakefield MA, Emery S, et al. State anti-tobacco advertising and smoking outcomes by gender and race/ethnicity. Ethn Health. 2007;12(4):339–362. doi:10.1080/13557850701300723
17. Keeler C, Max W, Yerger V, Yao T, Ong MK, Sung HY. The association of menthol cigarette use with quit attempts, successful cessation, and intention to quit across racial/ethnic groups in the United States. Nicotine Tob Res. 2017;19(12):1450–1464. doi:10.1093/ntr/ntw215
18. Giovenco DP, Spillane TE, Merizier JM. Neighborhood differences in alternative tobacco product availability and advertising in New York City: implications for health disparities. Nicotine Tob Res. 2018;21:896–902.
19. Anderson SJ. Marketing of menthol cigarettes and consumer perceptions: a review of tobacco industry documents. Tob Control. 2011;20(Suppl 2):ii20–ii28. doi:10.1136/tc.2010.041939
20. Greaves L, Hemsing N. Women and tobacco control policies: social-structural and psychosocial contributions to vulnerability to tobacco use and exposure. Drug Alcohol Depend. 2009;104(Suppl 1):S121–S130. doi:10.1016/j.drugalcdep.2009.05.001
21. Cokkinides VE, Halpern MT, Barbeau EM, Ward E, Thun MJ. Racial and ethnic disparities in smoking-cessation interventions: analysis of the 2005 National Health Interview Survey. Am J Prev Med. 2008;34(5):404–412. doi:10.1016/j.amepre.2008.02.003
22. Tran ST, Rosenberg KD, Carlson NE. Racial/ethnic disparities in the receipt of smoking cessation interventions during prenatal care. Matern Child Health J. 2010;14(6):901–909. doi:10.1007/s10995-009-0522-x
23. Assari S. Health disparities due to diminished return among black Americans: public policy solutions. Soc Issues Policy Rev. 2018;12(1):112–145. doi:10.1111/sipr.12042
24. Assari S. Unequal gain of equal resources across racial groups. Int J Health Policy Manag. 2017;7(1):1–9. doi:10.15171/ijhpm.2017.90
25. Assari S, Mistry R. Educational attainment and smoking status in a national sample of american adults; evidence for the blacks’ diminished return. Int J Environ Res Public Health. 2018;15(4):763. doi:10.3390/ijerph15040763
26. Shervin A, Ritesh M. Diminished return of employment on ever smoking among hispanic whites in Los Angeles. Health Equity. 2019;3(1):138–144. doi:10.1089/heq.2018.0070
27. Assari S, Lankarani MM. Education and alcohol consumption among older americans; black-white differences. Front Public Health. 2016;4:67. doi:10.3389/fpubh.2016.00067
28. Assari S, Farokhnia M, Mistry R. Education attainment and alcohol binge drinking: diminished returns of hispanics in Los Angeles. Behav Sci (Basel). 2019;9(1):9.
29. Assari S. Parental education attainment and educational upward mobility; role of race and gender. Behav Sci (Basel). 2018;8(11):107.
30. Assari S. Parental educational attainment and mental well-being of college students; diminished returns of blacks. Brain Sci. 2018;8(11). doi:10.3390/brainsci8110193
31. Assari S, Hani N. Household income and children’s unmet dental care need; blacks’ diminished return. Dent J (Basel). 2018;6(2):17.
32. Assari S, Caldwell CH, Mincy R. Family socioeconomic status at birth and youth impulsivity at age 15; blacks’ diminished return. Children (Basel). 2018;5(5):58.
33. Assari S, Caldwell CH, Mincy RB. Maternal educational attainment at birth promotes future self-rated health of white but not black youth: a 15-year cohort of a national sample. J Clin Med. 2018;7(5):93. doi:10.3390/jcm7050093
34. Assari S, Thomas A, Caldwell CH, Mincy RB. Blacks’ diminished health return of family structure and socioeconomic status; 15 years of follow-up of a national urban sample of Youth. J Urban Health. 2018;95(1):21–35. doi:10.1007/s11524-017-0217-3
35. Assari SBM, Caldwell CH. Parental educational attainment and youth outcomes: hispanics’ diminished returns. JAMA Netw Open. 2020;1:21.
36. Chaloupka FJ, Pacula RL. Sex and race differences in young people’s responsiveness to price and tobacco control policies. Tob Control. 1999;8(4):373–377. doi:10.1136/tc.8.4.373
37. Assari S, Mistry R. Educational attainment and smoking status in a national sample of american adults; evidence for the blacks’ diminished return. Int J Environ Res Public Health. 2018;15:763. doi:10.3390/ijerph15040763
38. Assari S. High income protects whites but not African Americans against risk of depression. Healthcare (Basel). 2018;6(2):37.
39. Assari S. Life expectancy gain due to employment status depends on race, gender, education, and their intersections. J Racial Ethn Health Disparities. 2018;5(2):375–386. doi:10.1007/s40615-017-0381-x
40. Assari S, Caldwell CH, Zimmerman MA. Family structure and subsequent anxiety symptoms; minorities’ diminished return. Brain Sci. 2018;8(6):97. doi:10.3390/brainsci8060097
41. Assari S, Lankarani M. Educational attainment promotes fruit and vegetable intake for whites but not blacks. J (Basel). 2018;1(1):5.
42. Assari S, Preiser B, Kelly M. Education and income predict future emotional well-being of whites but not blacks: a ten-year cohort. Brain Sci. 2018;8(7):122. doi:10.3390/brainsci8070122
43. Assari S, Lapeyrouse LM, Neighbors HW. Income and self-rated mental health: diminished returns for high income black Americans. Behav Sci (Basel). 2018;8(5):50.
44. Assari S, Caldwell CH. Family income at birth and risk of attention deficit hyperactivity disorder at age 15: racial differences. Children (Basel). 2019;6(1):10.
45. Assari S, Bazargan M. Minorities’ diminished returns of educational attainment on hospitalization risk: National Health Interview Survey (NHIS). Hosp Pract Res. 2019;4:86–91. doi:10.15171/hpr.2019.17
46. Assari S, Bazargan M. Educational attainment better reduces disability for non-hispanic than hispanic Americans. Eur J Invest Health Psychol Educ. 2019;10(1):10–17. doi:10.3390/ejihpe10010002
47. Assari S, Caldwell CH, Bazargan M. Association between parental educational attainment and youth outcomes and role of race/ethnicity. JAMA Netw Open. 2019;2(11):e1916018. doi:10.1001/jamanetworkopen.2019.16018
48. Assari S, Mistry R. Diminished return of employment on ever smoking among hispanic whites in Los Angeles. Health Equity. 2019;3(1):138–144. doi:10.1089/heq.2018.0070
49. Assari S, Mistry R, Bazargan M. Race, educational attainment, and E-cigarette use. J Med Res Innovation. 2020;4(1):e000185–e000185. doi:10.32892/jmri.185
50. Assari S, Bazargan M. Protective effects of educational attainment against cigarette smoking; diminished returns of American Indians and Alaska natives in the National Health Interview Survey. Int J Travel Med Global Health. 2019;7:105–110. doi:10.15171/ijtmgh.2019.22
51. Assari S, Bazargan M. Education level and cigarette smoking: diminished returns of lesbian, gay and bisexual individuals. Behav Sci (Basel). 2019;9(10):103.
52. Assari S. Parental education better helps white than black families escape poverty: National Survey of Children’s Health. Economies. 2018;6(2):30. doi:10.3390/economies6020030
53. FDA. FaDA. Research Priorities. Accessed February 5, 2019.
54. Feliu A, Filippidis FT, Joossens L, et al. Impact of tobacco control policies on smoking prevalence and quit ratios in 27 European Union countries from 2006 to 2014. Tob Control. 2019;28(1):101–109. doi:10.1136/tobaccocontrol-2017-054119
55. Assari S. Blacks’ diminished return of education attainment on subjective health; mediating effect of income. Brain Sci. 2018;8(9):176. doi:10.3390/brainsci8090176
56. Assari S. Socioeconomic status and self-rated oral health; diminished return among hispanic whites. Dent J (Basel). 2018;6(2):11.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.