")
Back to Journals » Infection and Drug Resistance » Volume 13
Protective Effects of Cytomegalovirus DNA Copies ≧1000/mL for AML Patients in Complete Remission After Single Cord Blood Transplantation
Authors Dong MY, Tang BL, Zhu XY, Cheng SQ, Fang XC, Tong J , Wan X, Zheng CC, Liu HL, Sun ZM
Received 31 July 2019
Accepted for publication 17 December 2019
Published 7 February 2020 Volume 2020:13 Pages 373—383
DOI https://doi.org/10.2147/IDR.S225465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sahil Khanna
Man-Yu Dong, Bao-Lin Tang, Xiao-Yu Zhu, Si-Qi Cheng, Xin-Chen Fang, Juan Tong, Xiang Wan, Chang-Cheng Zheng, Hui-Lan Liu, Zi-Min Sun
Department of Hematology, The First Affiliated Hospital of University of Science and Technology of China, Hefei, Anhui, People’s Republic of China
Correspondence: Zi-Min Sun
Department of Hematology, The First Affiliated Hospital of University of Science and Technology of China, No. 17, Lujiang Road, Hefei, Anhui 230001, People’s Republic of China
Tel +86 551 6228 2992
Fax +86 551 6228 2121
Email [email protected]
Introduction: Current consensus recommends a protective effect of cytomegalovirus (CMV) infection on relapse after peripheral blood or bone marrow hematopoietic stem cell transplantation. However, in cord blood transplantation (CBT), studies of CMV infection, especially CMV viral load, on relapse are limited.
Patients and Methods: We retrospectively analyzed the effect of CMV infection on 3-year outcomes in 249 AML patients according to CMV DNA load (DNA copies < 1000/mL and DNA copies ≧1000/mL) within 100 days after CBT. Furthermore, eight-colour flow cytometry was used to detect peripheral blood lymphocyte subsets in 38 patients who received CBT in the last year, and 10 healthy volunteers were included as controls.
Results: The results showed that CMV DNA load did not affect the cumulative incidence of relapse in the whole study population. However, in patients with complete remission status before transplantation, the high CMV DNA load group showed a significantly reduction of relapse than the low CMV DNA load group (3.9% vs 14.6%, p=0.012, respectively), which was confirmed by multivariate analysis (HR 0.23; 95% CI, 0.07– 0.73, p = 0.012). Surprisingly, high or low CMV DNA load did not significantly affect non-relapse mortality or overall survival (18.0% vs 17.0%, p=0.777 and 79.0% vs 74.6%, p=0.781, respectively). Besides, the absolute number of CD8+ T cells were increased in the high CMV DNA load group compared with the low DNA load group 1 month after CBT (0.20× 10 9/L vs 0.10× 10 9/L, p=0.021, respectively).
Conclusion: DNA copies ≧1000/mL for AML patients in complete remission was associated with a lower incidence of relapse after CBT, which might partly result from the expansion of CMV-related CD8+ T cells.
Keywords: cord blood transplantation, cytomegalovirus, DNA load, relapse, acute myeloid leukemia, complete remission
Introduction
Hematopoietic stem cell transplantation (HSCT) is a curative approach for hematologic malignancies. In general, cord blood transplantation (CBT) is a safe and effective alternative for patients lacking an HLA-matched related or unrelated donor.1–3 In recent years, with the improvement of transplantation procedures, the use of unrelated cord blood (CB) has dramatically increased,4 whereas immunodeficiency during the transplantation procedures can provide opportunities for cytomegalovirus (CMV) infection.
CMV infection is a major cause of morbidity and mortality related to CMV disease and non-relapse mortality (NRM) in HSCT.5,6 With the improvement of CMV management, severe CMV infection and death has significantly reduced.7,8 However, recent studies reported that CMV infection was associated with reduced relapse in AML recipients receiving peripheral blood (PB) or bone marrow (BM) HSCT but not CBT.9–14 And the protective effects appeared to be related to myeloablative conditioning (MAC) HSCT12 and whether or not to use ATG.14 Additionally, Michael Koldehoff et al suggested that CMV might initiate viral anti-leukemia functions to promote apoptosis in AML or BCR-ABL-positive ALL cells.15 However, more studies have theorized that CMV exerted anti-leukemia effects through indirect modulation of innate and adaptive immune responses.16–19
All of the above has provoked a reassessment of CMV infection on relapse after CBT. In this paper we attempt to defend the view that the degree of CMV infection might be related to the strength of the anti-leukemia effect. Thus, we retrospectively analyzed the relationship between CMV infection and 3-year outcomes according to CMV DNA load. In order to identify the mechanisms of CMV on outcomes, a group of patients were asked to analyze the immunological responses caused by CMV.
Patients and Methods
Study Design and Patients
This study was performed at the Anhui Provincial Hospital in Hefei, China. All patients who received a single unrelated CB graft between August 2008 and October 2018 were invited to participate in the study. The enrolment criteria were as follows: 1) Patients diagnosed with AML; 2) Patients with no vital organs seriously injured before transplantation, such as the brain, heart, lungs and abdominal organs et al; 3) Patients who had neutrophil engraftments; and 4) Patients who received MAC without depleted-T cells. We captured data for CMV infection before day 100 post transplantation.20 The 3-years outcomes of the high CMV DNA load group (DNA copies ≧1000/mL) and the low CMV DNA load group (DNA copies <1000/mL) were comparatively analyzed after CBT. The negative CMV DNA copy group was merged into the CMV DNA copies <1000/mL group due to the high incidence of CMV infection (85%) in the analysis of survival.
Meanwhile, PB samples from 38 patients of the above populations, receiving a CB graft between January 2017 and February 2018, were collected 1 month after CBT. Correspondingly, 10 healthy physical examination populations were recruited as controls. Our protocol complied with the Declaration of Helsinki and was approved by the Anhui Medical University Institutional Review Board, and all individuals included in the study provided written informed consent.
Study Endpoints and Definitions
The primary endpoint was the cumulative incidence (CI) of relapse that was stratified by CMV DNA load. The secondary endpoints included NRM, disease-free survival (DFS), overall survival (OS), GVHD-free relapse-free survival (GRFS),21 CMV disease,22 acute and chronic GVHD status.23,24 Neutrophil engraftment was defined as the achievement of an ANC ≧ 0.5×109/L for 3 consecutive days. The MAC regimen referred to an intravenous busulfan-based regime (Bu, total 12.8 mg/kg, 0.8mg/kg every 6 h, day-7 to day-4) or a total body irradiation-based regime (TBI, total 12 Gy in 4 fractions, day-7 to day-6).25,26 The NCCN-2018 guideline definitions of disease risk stratification were used.27 Complete remission (CR) was defined as less than 5% blasts in the bone marrow, the absence of extra-medullary leukemia, and normal values for absolute neutrophil count (>1×109/L) and platelet count (>100×109/L), and independence from red cell transfusion.28 Any other disease status was categorized as non-complete remission (NR). Pre-engraftment syndrome (PES) was characterized by a noninfectious fever and various other clinical findings before neutrophil engraftment, including skin rash, pulmonary infiltrates, and weight gain.29
CMV Monitoring and Pre-Emptive Therapy
CMV infection was defined as virus isolation or the detection of viral proteins (antigens) or nucleic acids in any body fluid or tissue specimen. In this study, CMV infection referred to CMV viremia, which was defined as the detection of CMV DNA in samples of plasma, serum, whole blood, peripheral blood leukocytes, bronchoalveolar lavage fluid, or tissue.30 And CMV disease referred to symptomatic CMV infectious disease, which was defined as the quantitation of CMV DNA in bronchoalveolar lavage fluid or tissue combined with attributable symptoms.22 The CMV nucleic acid testing was performed using the quantitative real-time PCR (RT-PCR) method as we previously reported.31 CMV monitoring was examined twice per week for at least 100 days and once a week for at least half a year after transplantation.
Recently, letermovir was approved for CMV prophylaxis in allogeneic HSCT recipients32 but was not yet available in China. Therefore, the enrolled patients did not receive prophylaxis of CMV. The pre-emptive antiviral therapy (5 mg/kg intravenous ganciclovir every 12 h) was initiated when CMV DNA copies ≧1000/mL of whole blood for at least 7 days, followed by an intravenous or oral maintenance therapy until two consecutive negative CMV DNA copies were obtained. Foscarnet (90 mg/kg every 12 h), with or without intravenous gammaglobulin administration (0.4 g/kg daily, for 3–5 d), was used as an alternative drug for the treatment of ganciclovir intolerance or for resistant and refractory CMV. The same treatment regimen was also adapted to the treatment of CMV disease.
Flow Cytometry Analysis of Peripheral Blood Cells
T cells (CD3+, CD3+CD4+, CD3+CD8+), regulatory T (Treg) cells (CD3+CD4+CD25+CD127low), B cells (CD19+), regulatory B (Breg) cells (CD3−CD19+CD24highCD38highCD27−CD5dim) and NK cells (CD3−CD16+CD56+) were assessed via flow cytometry to monitor the recovery of immune reconstruction 1 month after transplantation.
The same specimen was divided into three tubes for detection: 1) TBNK: a multitest six- colour TBNK reagent panel (from Tongsheng Times, Beijing, China) of monoclonal antibodies as used for CD3 (FITC), CD16CD56 (PE), CD45 (PerCP-cy5.5), CD4 (PE-Cy7), CD19 (APC) and CD8 (APC-Cy7); 2) Treg: fluorescein-labelled monoclonal antibodies were used for CD45 (PerCP-cy5.5), CD4 (FITC), CD25 (PE) and CD127 (APC); and 3) Breg: fluorescein-labelled monoclonal antibodies were used for CD45 (PerCP-cy5.5), CD19 (PE-Cy7), CD27 (FITC), CD24 (PE), CD5 (APC) and CD38 (V450). Two hundred microliters of fresh PB from EDTA tubes were added to the above fluorescein-labeled monoclonal antibodies for 30 mins (4°C and protected from light). Then, red blood cell lysates (Beckman Coulter, Miami, FL, USA) were added for 5 mins and then washed three times. And appropriate isotype controls were performed simultaneously. All of the fluorescein-labelled monoclonal antibodies were obtained from BD Biosciences (San Jose, CA, USA), except for CD19, which was obtained from Biolegend (San Diego, CA, USA), and CD25, which was obtained from Beckman Coulter (Miami, FL, USA). Flow cytometry was performed on a FACS Canto II (BD Bioscience) and analyzed using Flowjo V10 software.
Statistical Analysis
The patients and transplantation characteristics of different CMV DNA load groups were compared using the chi-square test or Fisher exact test for categorical variables and the Mann–Whitney Nonparametric test for continuous variables. The probabilities of OS, DFS, and GRFS were analyzed by the Kaplan–Meier method. For the CI analyses of relapse, acute GVHD (aGVHD) and chronic GVHD (cGVHD), death was a competing event, whereas relapse was the competing event for the CI of NRM. Time-to-event analyses were performed using the Gray test for competing events. In multivariate analysis of acute and chronic GVHD, the proportional hazard assumption was examined. If violated, it was compared using the time-dependent cox regression model. A stepwise selection procedure was used. In univariate analysis, the main aim was to investigate the relationship between the outcomes and the CMV DNA load, and a series of other independent variables like recipient’s age/gender/weight, donor-recipient ABO/HLA compatibility, disease stage/risk stratification, total number of nucleated cells (TNC), total number of CD34+ cells, conditioning regimes, PES,26 and acute/chronic GVHD were also taken into consideration. In multivariate analysis, borderline significance (p < 0.1) in univariate analysis or more related to the outcomes was analyzed simultaneously. Statistical analyses were performed using SPSS software, version 24.0, and Easy R software, Version 3.3.2. A p-value <0.05 was considered to indicate statistical significance.
Results
Patient Characteristics and CMV Infection
For the entire population, a total of 249 patients participated in the study, among whom 199 (80%) patients achieved CR while 50 (20%) patients in NR before transplantation. With a median follow-up period of 1148 (349–4075) days, CMV infection occurred in 211 (85%) patients at a median time of 31 (15–90) days after CBT. Specifically, 130 (52%) patients had a high CMV DNA load and 119 (48%) patients had low CMV DNA load. Additionally, a total of 202 patients underwent pre-transplantation CMV antibody tests (IgG), most of which were transplanted after 2015. We found that the CMV-IgG positive rate in this group of patients was as high as 98%. The baseline characteristics for the entire population are shown in Table 1.
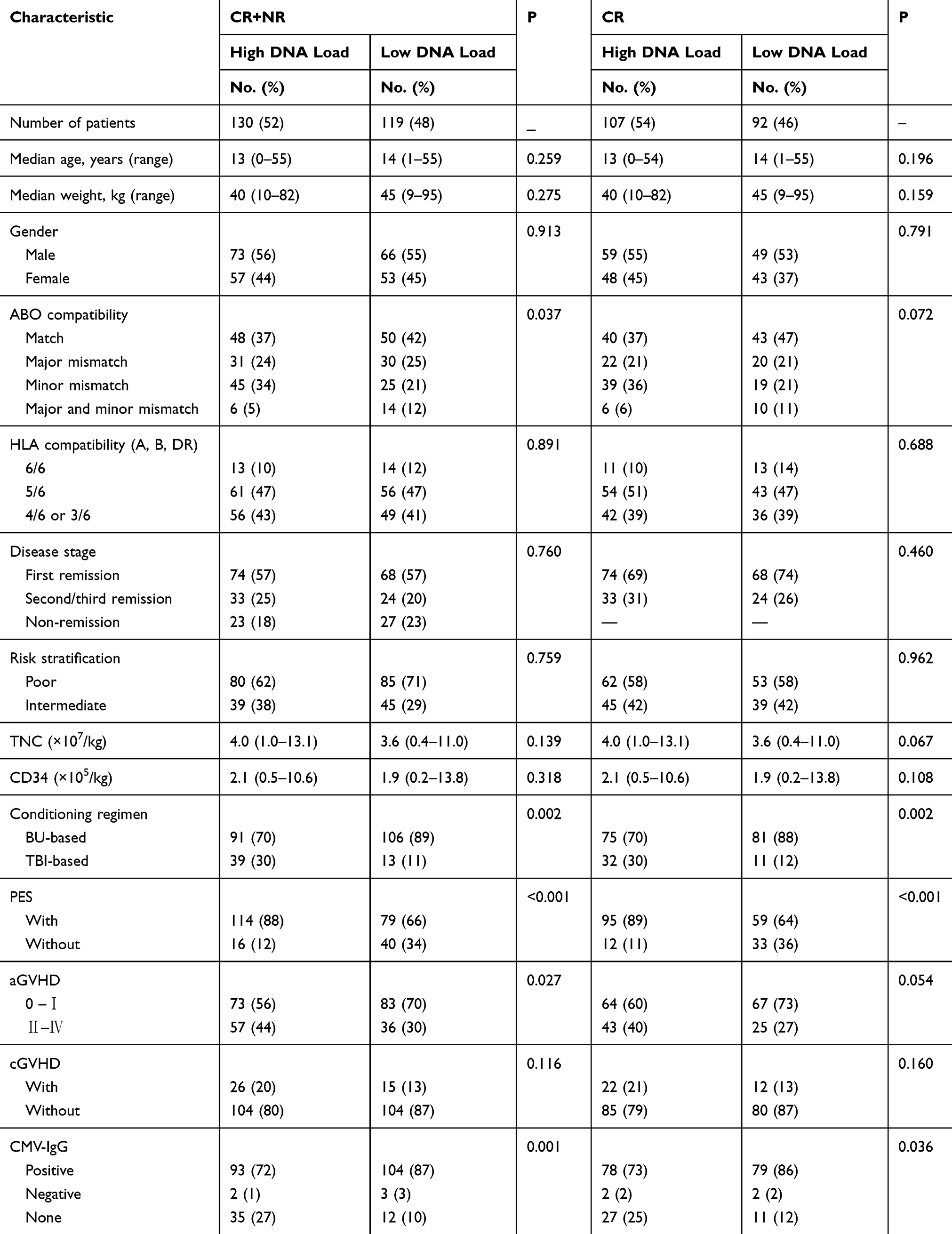 |
Table 1 Patients’ Characteristics for the Groups According to CMV DNA Load |
The baseline characteristics in CR patients are also shown in Table 1, and the patients’ ages, gender, weights, disease statuses, HLA compatibility, ABO blood compatibility, TNC cell doses, CD34+ cell doses, aGVHD and cGVHD statuses exhibited no significant differences between the high and low CMV DNA load groups. However, the Conditioning regimens and incidence of PES were imbalance between the two groups, and all of them were included in the univariate analysis of the outcomes.
CBT Outcomes
For the entire population, there were no statistically significant differences in the CI of relapse, NRM, and the probability of survival between the two different CMV DNA load groups (Table 2), which were confirmed by multivariate analysis (Supporting Information, Table S1). A total of 26 patients in the entire cohort suffered relapse (10 cases in high DNA load group and 16 cases in low DNA load group), and 16 (62%) of them relapsed within 1 year after CBT (data not shown). Besides, in 199 patients with CR status before transplantation, we have seen the following differences.
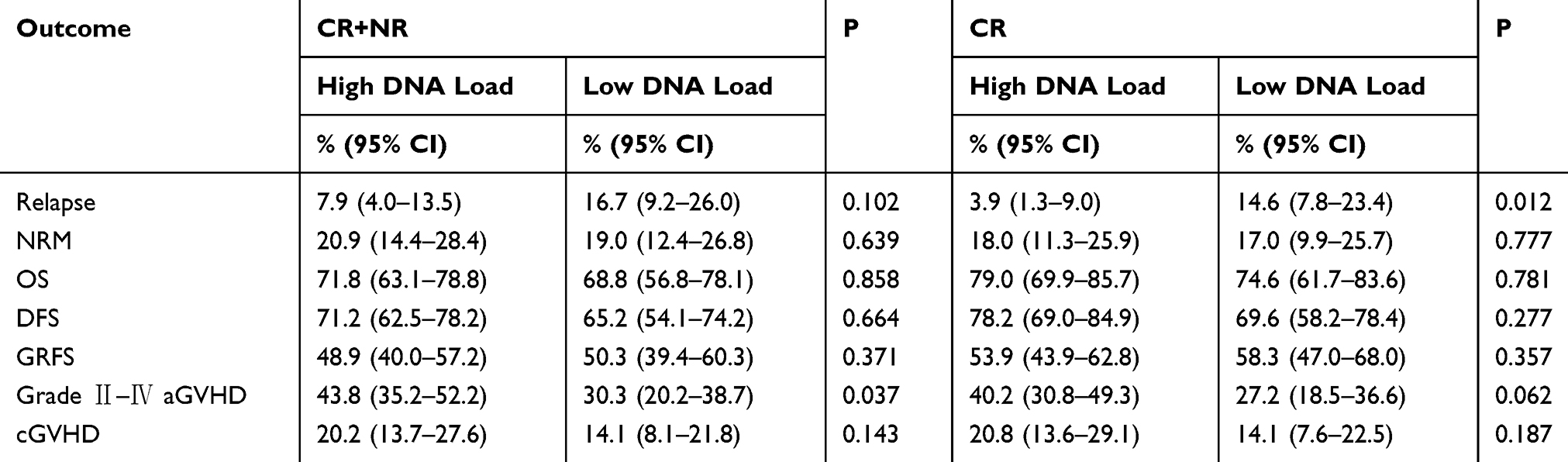 |
Table 2 Univariate Analysis of 3-Year Outcomes for the Groups According to CMV DNA Load |
Relapse and Non-Relapse Mortality
For CR recipients, the high CMV DNA load group had a lower 3-year CI of relapse than the low CMV DNA load group (Figure 1A; 3.9% vs 14.6%, p=0.012, respectively). In detail, a total of 16 patients suffered relapse (4 cases in high DNA load group and 12 cases in low DNA load group). In multivariate analysis, a high CMV DNA load was confirmed to have a protective effect on relapse (Table 3; HR 0.23; 95% CI, 0.07–0.73, p = 0.012). Besides, man recipient had a higher CI of relapse (Table 3; HR: 4.39; 95% CI: 1.24–15.54; p=0.022) in multivariate analysis.
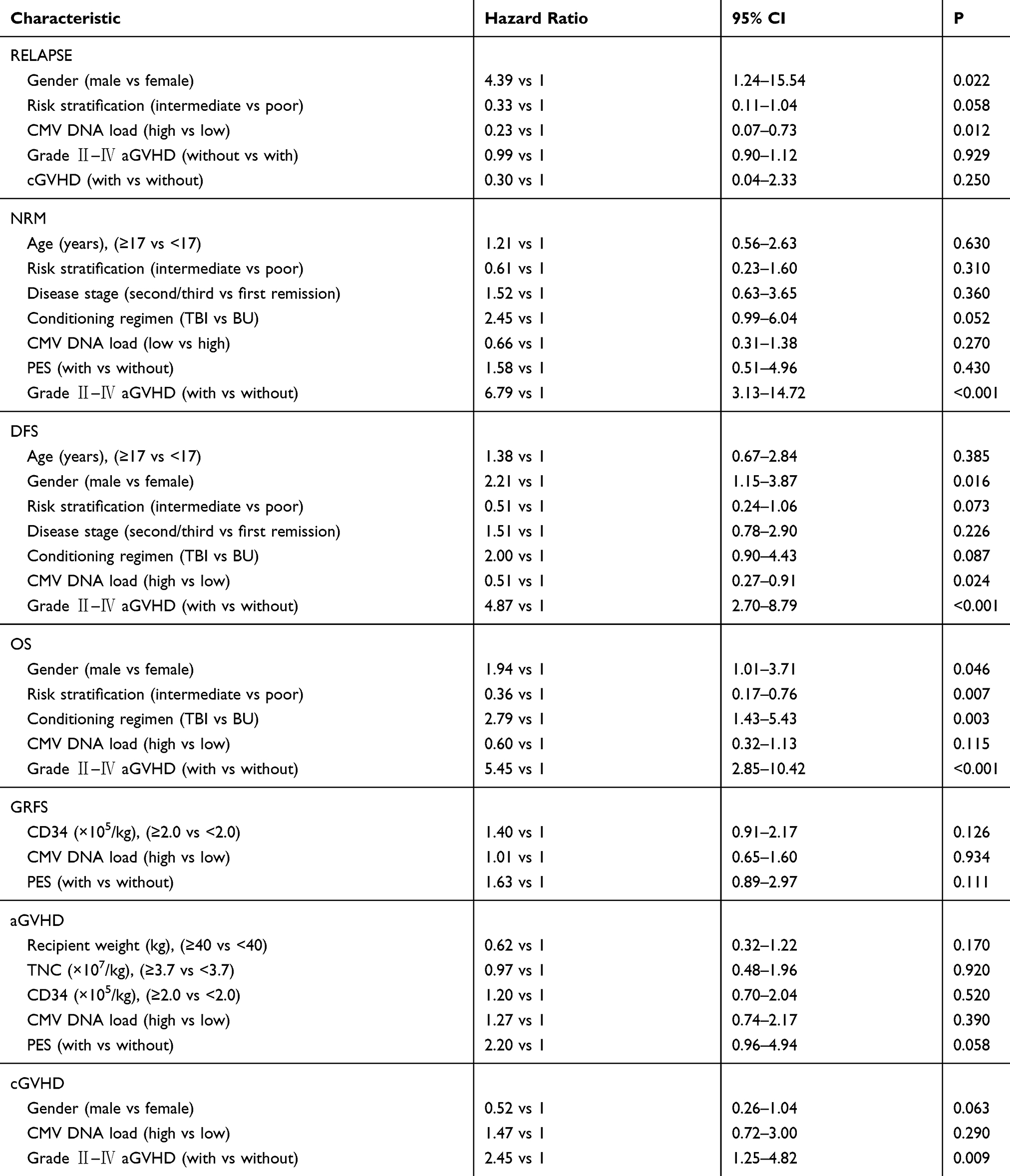 |
Table 3 Multivariate Analysis of 3-Year Outcomes in CR Patients |
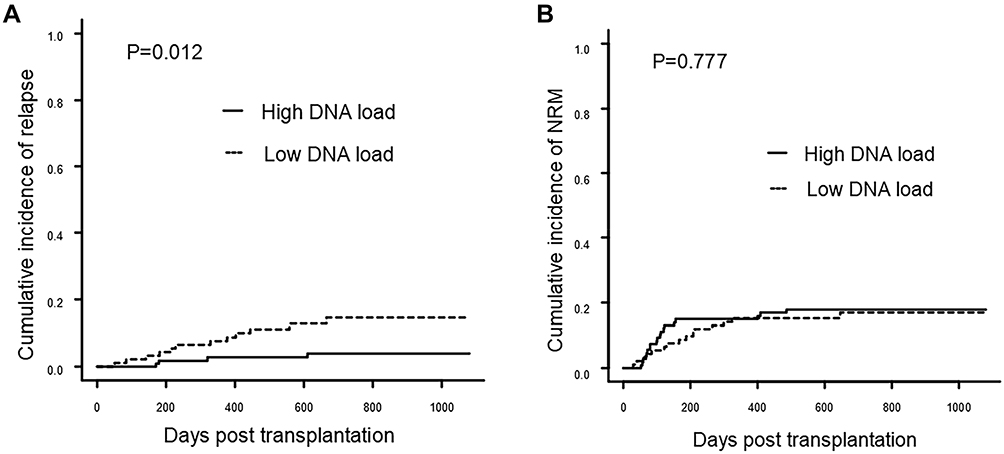 |
Figure 1 Cumulative incidence of relapse and NRM according to CMV DNA load in CR patients. (A) Relapse; (B) Non-relapse mortality. |
The 3-year NRM showed no significant difference between the high and low CMV DNA load groups (Figure 1B; 18.0% vs 17.0%, p=0.777, respectively). In multivariate analysis, grade Ⅱ–Ⅳ aGVHD was an important risk factor for increasing NRM (Table 3; HR: 6.79; 95% CI: 3.13–14.72; p < 0.001). In detail, 15 (16%) patients in the low DNA load group and 19 (18%) patients in the high DNA load group died without relapse. Pulmonary infection and grade Ⅱ–Ⅳ aGVHD were the leading causes of death.
Survival and GVHD
For CR recipients, 3-years DFS was non-significant between the high and low DNA load groups in univariate analysis (Figure 2A; 78.2% vs 69.6%, p=0.277, respectively). However, in multivariate analysis including variables with borderline significance (p < 0.1), high CMV DNA load was associated with the improvement of DFS (HR 0.51, 95% CI, 0.27–0.91, p=0.024). Besides, OS and GRFS showed non-significant between the high and low CMV DNA load groups (Figure 2B and C; 79.0% vs 69.6%, p=0.781 and 53.9% vs 58.3%, p=0.357, respectively). When comparing the aGVHD and cGVHD, there were no significant differences between the two CMV DNA load groups (Table 2).
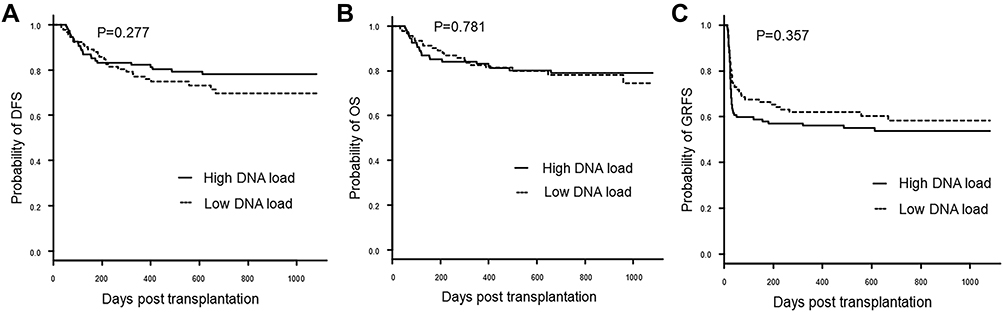 |
Figure 2 Probability of survival according to CMV DNA load in CR patients. (A) Disease-free survival; (B) Overall survival; (C) GVHD-free, relapse-free survival. |
It was worth noting that grade Ⅱ–Ⅳ aGVHD was a remarkable risk factor for reducing OS, and DFS (Table 3; HR, 5.45, 95% CI, 2.85–10.42, p<0.001 and HR, 4.87, 95% CI, 2.70–8.79, p<0.001, respectively) in multivariate analysis. Also, man recipients showed significantly reduced probability of OS and DFS than female recipients (Table 3; HR, 1.94, 95% CI, 1.01–3.71, p=0.046 and HR, 2.21, 95% CI, 1.15–3.87, p=0.016, respectively). In addition, BU-based conditioning regimen presented a better OS than TBI-based conditioning regimen and poor risk stratification was associated with the reduction of OS in multivariate analysis (Table 3; HR, 2.79, 95% CI, 1.43–5.43, p=0.003 and HR, 0.36, 95% CI, 0.17–0.76, p=0.007, respectively).
CMV Disease
In the entire group of patients, precise CMV monitoring and pre-emptive treatments were performed for CMV management. Since the launch of the CMV disease-related examination in 2016, only six (2.4%) cases of CMV disease were diagnosed (one case of CMV pneumonia and three cases of CMV enteritis in low CMV DNA load group while two cases of CMV enteritis in high CMV DNA load group) (data not shown). Fortunately, all of them cured and survived from CMV disease at the end of follow-up.
Immune Reconstruction
High CMV DNA Load Alters Peripheral CD8+ T Cells Distribution
A total of 38 patients were included in the immune reconstruction analysis. Among them, 11 (29%) patients were high CMV DNA loads, 27 (71%) patients were low CMV DNA loads. There were no significant differences in baseline characteristics between the two groups (Supporting Information, Table S2). We analyzed the number of T cells, B cells, NK cells, Treg cells and Breg cells according to CMV DNA load.
The data showed that CD3+ T cells were significantly increased in the high CMV DNA load group (Figure 3A; 0.40×109/L vs 0.27×109/L, p=0.010). And NK cells presented no statistical difference between the high and low CMV DNA groups (Figure 3B; 0.20×109/L vs 0.21×109/L, p=0.657, respectively). However, donor-derived B cells, along with Breg cells, were not reconstituted 1 month after transplantation.
 |
Figure 3 Lymphocytes reconstitution according to CMV DNA load in CR patients. (A) Absolute number of T cells; (B) Absolute number of NK cells; Notes: All of the statistical graphs show median±interquartile range. *P ≦ 0.05. |
Upon further analyses of T cell subsets found that CD8+ T cells in the high CMV DNA load group were significantly expanded (Figure 4A; 0.20×109/L vs 0.10×109/L, p=0.021). Nevertheless, no significant differences were found in CD4+ T cells and Treg cells between the high and low CMV DNA load groups (Figure 4B and C; 0.20×109/L vs 0.10×109/L and 0.20×107/L vs 0.32×107/L; p=0.159 and p =0.612, respectively).
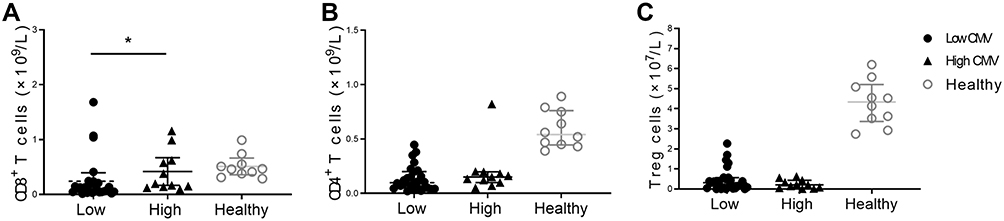 |
Figure 4 T cell subsets reconstitution according to CMV DNA load in CR patients. (A) Absolute number of CD8+ T cells; (B) Absolute number of CD4+ T cells; (C) Absolute number of Treg cells. Notes: All of the statistical graphs show median±interquartile range. *P ≦ 0.05. |
Discussion
Studies have shown that CMV infection for AML patients after PB or BM HSCT has a protective effect on relapse.11–13 However, in the CB setting, CMV infection was not associated with relapse.9 Indeed, our previous study has also shown that only infection with CMV for AML patients could not reduce relapse after CBT (data not shown). The results of this study indicated that the CMV DNA copies ≥1000/mL (high CMV DNA load) might be a valuable parameter to that protective purpose.
In our center, up to 98% of the patients receiving pre-transplant antibody testing were positive for CMV-IgG (data not shown). Similarly, previous research has reported that CMV seroprevalence (IgG) tended to be highest in South America, Africa and Asia (>90%).33 Antiviral prophylaxis has not been a first-line option for CMV prevention in allogeneic HSCT recipients because myelosuppression, particularly leukopenia and neutropenia, is commonly observed when using intravenous ganciclovir and valganciclovir.32 In this study, the CMV infection rate was as high as 88% after CBT (data not shown). Considering the reasons, the high serological positive rate before transplantation and the absence of CMV prevention after transplantation might contribute to this result.
Further in-depth analysis found that high CMV DNA load was associated with a significant reduction of relapse after CBT in CR recipients (p=0.012). The protective effect was confirmed and independent of acute/chronic GVHD in multivariate analyses (Table 3). However, patients who did not achieve disease remission before transplantation could not benefit from the high CMV DNA load (Table 2). Through the above, we could summarize the following two points. Firstly, this meant that the effect of CMV on relapse was related to the level of DNA replication of CMV, and the high CMV DNA load group had a lower CI of relapse than the low CMV DNA load group. Secondly, the high CMV DNA load played apositive role in relapse for patients who achieved CR before transplantation, but was not strong enough to reduce relapse in NR patients. For patients who did not achieve CR before HSCT, relapse was the predominant cause of treatment failure.34,35 So, the intensity of CMV on relapse might be so limited that high CMV DNA load failed to reverse the natural characteristics of high risk of relapse in NR recipients after transplantation. Considering the other factors, male gender was an independent risk predictor for relapse in multivariate analysis (p=0.022). This negative effect of male gender on relapse has been reported in studies of diffuse large B-cell lymphoma, but has not been reported in HSCT.36
In the study, pre-emptive therapy was initiated at the CMV level threshold of DNA copies ≧1000/mL.5 Under the CMV management, the results suggested an improvement of DFS in the high DNA load group (Table 3). And the NRM, OS, or GRFS showed non-significant between the two groups (Table 3). Considering the other risk factors, grade Ⅱ–Ⅳ aGVHD was an independent risk factor in increasing NRM and reducing OS and DFS.37 Besides, the high DNA load group contained more patients with Ⅱ–Ⅳ aGVHD in baseline data, which might explain why a high CMV viral load reduced relapse but did not translate into OS benefits in the study.
As mentioned above, through the analysis of CMV DNA load and disease remission status, we first reported this protective effect of CMV DNA copies ≧1000/mL on relapse after CBT, while not affected NRM or OS. The finding was similar to previous studies demonstrating a protective effect of CMV infection on relapse after PB and BM transplantation.11,38 However, another study reported that under the era of pre-emptive therapy, a CMV DNA load of ≧250 IU/mL (four DNA copies=1 IU) was associated with increased risk of NRM and overall mortality within one-year post HSCT.5 Considering the reasons for different results, only 11% of them received CBT without indicating single or double CBT, and 40% of them received reduced intensity conditioning, which were different from us. In the study, all patients received MAC without depleted-T cells treatment. In general, MAC was correlated with a lower incidence of relapse39,40 and depleted-T cells treatment indicated a better outcome due to the faster and more complete T cells recovery. Overall, the high CMV DNA load in our transplant central indicated a better outcome, probably due to the strong clearance of leukemia cells by MAC and immune protection without T-cell depletion.
Amplification of T cells and NK cells stimulated by CMV was considered to play a role in the protection of relapse after HSCT.16–18 Studies in both humans and animal models have indicated the protective effect of CD8+ T cell expansion on tumor regression.41,42 In HSCT, it has also been reported that CMV-related or CMV-specific CD8+ T-cells were associated with a lower CI of relapse.43,44 To understand the immunological basis of high CMV DNA on relapse, a study involving seven lymphocyte subsets according to CMV DNA load had been conducted. The results showed that the high CMV DNA load group presented a significant CD8+ T cells expansion 1 month after CBT, which was similar to the previous report.44 Moreover, the infusion of CMV-specific T cells indicated that T cells are required for CMV to exert anti-tumour effects after transplantation.45 Consequently, all of the above data demonstrated the expansion of CD8+ T cells induced by high CMV DNA load was partly associated with the reduction of relapse.
In conclusion, in CB setting, this study indicated the correlation of a significant reduction of relapse with CMV DNA copies ≧1000/mL in patients with CR. What’s more, the high CMV DNA load promoted peripheral CD8+ T cells expansion 1 month after CBT. Therefore, patients with AML, achieving CR status before transplantation can benefit from CMV DNA copies ≧1000/mL after CBT, and partly from CMV-related CD8+ T cells expansion. However, we failed to further define whether the populations of CD8+ T cells were specific for CMV. Further serological status of CMV analysis was limited because of the imbalance sample side between the negative and positive CMV-IgG groups in the study. Meanwhile, the number of relapse events could not reach 10 times the number of variables in the multivariate analysis. Previous studies have reported that the probability of relapse was lower in the CBT than other unrelated PB or BM stem cell transplantation, which might account for the low probability of relapse in the study.46 The causative conclusions were also limited by the limited involved cases and the inherent defects of retrospective clinical studies. It is recommended that further larger sample size of studies be undertaken.
Acknowledgments
We would like to extend our sincere gratitude to American Journal Experts for their assistance in editing this manuscript. This work was supported by grants from the National Natural Science Foundation of China (No. 81470350) and the Fundamental Research Funds for the Central Universities (No. WK9110000001).
Disclosure
The authors declare no competing financial interests in this work.
References
1. Gragert L, Eapen M, Williams E, et al. HLA match likelihoods for hematopoietic stem-cell grafts in the U.S. N Engl J Med. 2014;371(4):339–348. doi:10.1056/NEJMsa1311707
2. Baron F, Labopin M, Ruggeri A, et al. Unrelated cord blood transplantation for adult patients with acute myeloid leukemia: higher incidence of acute graft-versus-host disease and lower survival in male patients transplanted with female unrelated cord blood–a report from Eurocord, the Acute Leukemia Working Party, and the Cord Blood Committee of the Cellular Therapy and Immunobiology Working Party of the European Group for Blood and Marrow Transplantation. J Hematol Oncol. 2015;8:107–117.
3. Ballen KK, Gluckman E, Broxmeyer HE. Umbilical cord blood transplantation: the first 25 years and beyond. Blood. 2013;122(4):491–498. doi:10.1182/blood-2013-02-453175
4. Brunstein CG. Umbilical cord blood transplantation for the treatment of hematologic malignancies. Cancer Control. 2011;18(4):222–236. doi:10.1177/107327481101800403
5. Green ML, Leisenring W, Xie H, et al. Cytomegalovirus viral load and mortality after haemopoietic stem cell transplantation in the era of pre-emptive therapy: a retrospective cohort study. Lancet Haematol. 2016;3(3):e119–e27. doi:10.1016/S2352-3026(15)00289-6
6. Ljungman P, Perez-Bercoff L, Jonsson J, et al. Risk factors for the development of cytomegalovirus disease after allogeneic stem cell transplantation. Haematologica. 2006;91(1):78–83.
7. Broers AEC, Holt R, Esser J, et al. Increased transplant-related morbidity and mortality in CMV-seropositive patients despite highly effective prevention of CMV disease after allogeneic T-cell–depleted stem cell transplantation. Blood. 2000;95(7):2240–2245. doi:10.1182/blood.V95.7.2240
8. Boeckh M, Ljungman P. How we treat cytomegalovirus in hematopoietic cell transplant recipients. Blood. 2009;113(23):5711–5719. doi:10.1182/blood-2008-10-143560
9. Ramanathan M, Teira P, Battiwalla M, et al. Impact of early CMV reactivation in cord blood stem cell recipients in the current era. Bone Marrow Transplant. 2016;51(8):1113–1120. doi:10.1038/bmt.2016.89
10. Peric Z, Wilson J, Durakovic N, et al. Early human cytomegalovirus reactivation is associated with lower incidence of relapse of myeloproliferative disorders after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018;53(6):1450–1456. doi:10.1038/s41409-018-0172-y
11. Green ML, Leisenring WM, Xie H, et al. CMV reactivation after allogeneic HCT and relapse risk: evidence for early protection in acute myeloid leukemia. Blood. 2013;122(7):1316–1324. doi:10.1182/blood-2013-02-487074
12. Manjappa S, Bhamidipati PK, Stokerl-Goldstein KE, et al. Protective effect of cytomegalovirus reactivation on relapse after allogeneic hematopoietic cell transplantation in acute myeloid leukemia patients is influenced by conditioning regimen. Biol Blood Marrow Transplant. 2014;20(1):46–52. doi:10.1016/j.bbmt.2013.10.003
13. Takenaka K, Nishida T, Asano-Mori Y, et al. Cytomegalovirus reactivation after allogeneic hematopoietic stem cell transplantation is associated with a reduced risk of relapse in patients with acute myeloid leukemia who survived to day 100 after transplantation: the Japan Society for hematopoietic cell transplantation transplantation-related complication working group. Biol Blood Marrow Transplant. 2015;21(11):2008–2016. doi:10.1016/j.bbmt.2015.07.019
14. Xiebing Bao QZ, Shengli X, Xiaohui H, et al. Cytomegalovirus induces strong antileukemic effect in acute myeloid leukemia patients following sibling HSCT without ATG-containing regimen. Am J Transl Res. 2016;8:653–661.
15. Koldehoff M, Lindemann M, Opalka B, Bauer S, Ross RS, Elmaagacli AH. Cytomegalovirus induces apoptosis in acute leukemia cells as a virus-versus-leukemia function. Leuk Lymphoma. 2015;56(11):3189–3197. doi:10.3109/10428194.2015.1032968
16. Cichocki F, Cooley S, Davis Z, et al. CD56dimCD57+NKG2C+ NK cell expansion is associated with reduced leukemia relapse after reduced intensity HCT. Leukemia. 2016;30(2):456–463. doi:10.1038/leu.2015.260
17. Foley B, Cooley S, Verneris MR, et al. Cytomegalovirus reactivation after allogeneic transplantation promotes a lasting increase in educated NKG2C+ natural killer cells with potent function. Blood. 2012;119(11):2665–2674. doi:10.1182/blood-2011-10-386995
18. Scheper W, van Dorp S, Kersting S, et al. GammadeltaT cells elicited by CMV reactivation after allo-SCT cross-recognize CMV and leukemia. Leukemia. 2013;27(6):1328–1338. doi:10.1038/leu.2012.374
19. Knight A, Madrigal AJ, Grace S, et al. The role of Vδ2-negative γδ T cells during cytomegalovirus reactivation in recipients of allogeneic stem cell transplantation. Blood. 2010;116(12):2164–2172. doi:10.1182/blood-2010-01-255166
20. Teira P, Battiwalla M, Ramanathan M, et al. Early cytomegalovirus reactivation remains associated with increased transplant-related mortality in the current era: a CIBMTR analysis. Blood. 2016;127(20):2427–2438. doi:10.1182/blood-2015-11-679639
21. Holtan SG, DeFor TE, Lazaryan A, et al. Composite end point of graft-versus-host disease-free, relapse-free survival after allogeneic hematopoietic cell transplantation. Blood. 2015;125(8):1333–1338. doi:10.1182/blood-2014-10-609032
22. Humar A, Michaels M, Monitoring A. American society of transplantation recommendations for screening, monitoring and reporting of infectious complications in immunosuppression trials in recipients of organ transplantation. Am J Transplant. 2006;6(2):262–274. doi:10.1111/j.1600-6143.2005.01207.x
23. Przepiorka D, Weisdorf D, Martin P, Klingemann H-G, Beatty P, Hows J. Consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995;15:825–828.
24. Filipovich AH, Weisdorf D, Pavletic S, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–956. doi:10.1016/j.bbmt.2005.09.004
25. Sun Z, Liu H, Luo C, et al. Better outcomes of modified myeloablative conditioning without antithymocyte globulin versus myeloablative conditioning in cord blood transplantation for hematological malignancies: A retrospective (development) and a prospective (validation) study. Int J Cancer. 2018;143(3):699–708. doi:10.1002/ijc.v143.3
26. Bacigalupo A, Ballen K, Rizzo D, et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transplant. 2009;15(12):1628–1633. doi:10.1016/j.bbmt.2009.07.004
27. Network NCC. Acute myeloid leukemia, version 1.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw.
28. BD C, PA C, DR H, Head DR. Report of the National Cancer Institute-sponsored workshop on definitions of diagnosis and response in acute myeloid leukemia. J Clin Oncol. 1990;8(5):813–819. doi:10.1200/JCO.1990.8.5.813
29. Lee Y-H, Lim Y-J, Kim J-Y, Kim Y-D, Lee S-W. Pre-engraftment syndrome in hematopoietic stem cell transplantation. J Korean Med Sci. 2008;23(1):98–103. doi:10.3346/jkms.2008.23.1.98
30. Ljungman P, Boeckh M, Hirsch HH, et al. Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials. Clin Infect Dis. 2017;64(1):87–91. doi:10.1093/cid/ciw668
31. Tong J, Sun Z, Liu H, et al. Risk factors of CMV infection in patients after umbilical cord blood transplantation: a multicenter study in China. Chin J Cancer Res. 2013;25(6):695–703. doi:10.3978/j.issn.1000-9604.2013.11.08
32. Meesing A, Razonable RR. New developments in the management of cytomegalovirus infection after transplantation. Drugs. 2018;78(11):1085–1103.
33. Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol. 2010;20(4):202–213. doi:10.1002/rmv.v20:4
34. Duval M, Klein JP, He W, et al. Hematopoietic stem-cell transplantation for acute leukemia in relapse or primary induction failure. J Clin Oncol. 2010;28(23):3730–3738. doi:10.1200/JCO.2010.28.8852
35. Hemmati PG, Terwey TH, Na IK, et al. Allogeneic stem cell transplantation for refractory acute myeloid leukemia: a single center analysis of long-term outcome. Eur J Haematol. 2015;95(6):498–506. doi:10.1111/ejh.12522
36. Eyre TA, Martinez-Calle N, Hildyard C, Eyre DW, Plaschkes H, Griffith J. Male gender is an independent predictor for worse survival and relapse in a large, consecutive cohort of elderly DLBCL patients treated with R-CHOP. Br J Haematol. 2019;186:e65–e115. doi:10.1111/bjh.15927
37. Storb R, Gyurkocza B, Storer BE, et al. Graft-versus-host disease and graft-versus-tumor effects after allogeneic hematopoietic cell transplantation. J Clin Oncol. 2013;31(12):1530–1538. doi:10.1200/JCO.2012.45.0247
38. Elmaagacli AH, Steckel NK, Koldehoff M, et al. Early human cytomegalovirus replication after transplantation is associated with a decreased relapse risk: evidence for a putative virus-versus-leukemia effect in acute myeloid leukemia patients. Blood. 2011;118(5):1402–1412. doi:10.1182/blood-2010-08-304121
39. Horwitz ME. Reduced intensity versus myeloablative allogeneic stem cell transplantation for the treatment of acute myeloid leukemia, myelodysplastic syndrome and acute lymphoid leukemia. Curr Opin Oncol. 2011;23(2):197–202. doi:10.1097/CCO.0b013e328342b82a
40. Weisdorf DJ. Reduced-intensity versus myeloablative allogeneic transplantation. Hematol Oncol Stem Cell Ther. 2017;10(4):321–326. doi:10.1016/j.hemonc.2017.05.002
41. Qiu Z, Huang H, Grenier JM, et al. Cytomegalovirus-based vaccine expressing a modified tumor antigen induces potent tumor-specific CD8(+) T-cell response and protects mice from melanoma. Cancer Immunol Res. 2015;3(5):536–546. doi:10.1158/2326-6066.CIR-14-0044
42. Kawai O, Ishii G, Kubota K, et al. Predominant infiltration of macrophages and CD8(+) T Cells in cancer nests is a significant predictor of survival in stage IV nonsmall cell lung cancer. Cancer. 2008;113(6):1387–1395. doi:10.1002/cncr.23712
43. Zhang J, Chen X, Rong G, et al. Peripheral blood lymphocyte responses to cytomegalovirus seropositivity after allogeneic-hematopoietic stem cell transplantation. Onco Targets Ther. 2018;11(2):5143–5150. doi:10.2147/OTT
44. Perez-Martinez A, Varanasi PR, Ogonek J, et al. Cytomegalovirus-specific CD8+ T-cells are associated with a reduced incidence of early relapse after allogeneic stem cell transplantation. PLoS One. 2019;14(3):e0213739. doi:10.1371/journal.pone.0213739
45. Elmaagacli AH, Koldehoff M, Lindemann M, et al. Response: T cells are required for the CMV-induced antileukemia effect after transplant. Blood. 2012;119:1090–1091. doi:10.1182/blood-2011-11-386821
46. Milano F, Gooley T, Wood B, et al. Cord-blood transplantation in patients with minimal residual disease. N Engl J Med. 2016;375(10):944–953. doi:10.1056/NEJMoa1602074
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.