")
Back to Journals » Journal of Pain Research » Volume 15
Protective and Risk Factors at the Intersection of Chronic Pain, Depression, Anxiety, and Somatic Amplification: A Latent Profile Approach
Received 29 September 2021
Accepted for publication 25 November 2021
Published 15 April 2022 Volume 2022:15 Pages 1107—1121
DOI https://doi.org/10.2147/JPR.S340382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
ShinYe Kim,1 Jaehoon Lee,2 Dianna Boone3
1Department of Psychological Sciences, Texas Tech University, Lubbock, TX, USA; 2Department of Educational Psychology, Leadership, and Counseling, Texas Tech University, Lubbock, TX, USA; 3Center for Behavioral Health, Johns Hopkins All Children’s Hospital, St. Petersburg, FL, USA
Correspondence: ShinYe Kim Email [email protected]
Objective: Research indicates a complex nexus between chronic pain, depression, anxiety, and somatic amplification (PDAS) symptoms, marked by high rates of co-morbidity and mutually maintaining mechanisms. Although recent frameworks have attempted to explain co-occurrence rates of pain and other comorbid disorders, the interrelations between PDAS and their impacts on pain outcomes have not been adequately examined with a person-centered approach. Using nationally representative data, this study assessed the heterogeneity in PDAS symptomatology and examined links among risk and protective factors in different profiles.
Methods: Data were derived from 1027 participants in the National Survey of Midlife Development in the United States (MIDUS) who completed telephone interviews or self-report measures that assessed PDAS, various sources of social supports (family, friends, spouses/partners, religion, coworkers, and supervisors), and the number of healthcare visits.
Results: We found heterogeneity in symptom severity rather than symptom type across classes over time. Regardless of comorbidity severity, people reported similar levels of somatic symptoms, which may help clinicians more effectively diagnose comorbidity issues among chronic pain patients. As PDAS symptomatology increased by group, the perceived levels of social support decreased. Membership in a higher symptom severity class was associated with being female, younger age, and an increase in medical, but not mental health visits.
Limitations: Limitations included the use of a cross-sectional design, reliance on self-report measures, and a sample largely comprised of Whites.
Conclusion: PDAS co-occurs across classes, which may relate to shared risk and protective factors. This study lays the foundation to investigate similar questions for overlapping symptoms that occur during the same period, which would shed light on whether—among middle to older age adults—these disorders are attributable to a common mechanism and if they may inform transdiagnostic treatments.
Keywords: chronic pain, depression, anxiety, somatic amplification, comorbidity, transdiagnostic
Introduction
Chronic pain, depression, anxiety, and somatic amplification (PDAS) co-occur frequently,1–5 and people who suffer from chronic pain are more likely to have psychological disorders than those who do not.2,3 National epidemiological surveys estimate that among those with chronic pain, comorbidity rates between chronic pain and depression range from 5% to 85%1,6 and approximately 25% of people with chronic pain qualify for a Somatic Symptom Disorder diagnosis.5 Studies have found that approximately 6%7 to 35%8 of those with chronic pain also have a comorbid anxiety disorder, and up to 50% of patients with chronic pain exhibit symptoms of anxiety and depression, although the comorbidity rate exceeds 75% in some studies.9
Despite robust evidence for co-occurrence between chronic pain and other psychological disorders, exact mechanisms of development and maintenance of such comorbidity remain ill-defined and controversial in the literature. Recent conceptual models illustrating chronic pain and co-occurring disorders in adolescence have highlighted the dynamic interplay between biological, behavioral, cognitive-affective, and social factors that unfold throughout development.10 Such factors may interact, potentially predisposing individuals to developing co-occurring pain and depression or maintaining the course of each disorder. For example, due to the lack of positive social interactions, social withdrawal may precipitate depression and exacerbate one’s chronic pain. Alternatively, anhedonia or fatigue due to chronic pain or depression could lead to social withdrawal and other forms of behavioral avoidance.10 Another recent review11 highlights shared neural pathways and physiological mechanisms that put individuals at risk for developing chronic pain or depression. Specifically, inflammatory processes, dysfunction of stress systems, and shared brain processes associated with pain or depression may influence the onset or exacerbation of the other.11 Neurobiological mechanisms underlying pain and co-morbid disorders may interact with other psychological or social factors, increasing one’s vulnerability to greater or more severe PDAS symptoms.
The diathesis-stress biopsychosocial model of chronic pain12 depicts that social support from multiple domains, as well as coping strategies, mutually interact with other biopsychosocial factors (eg, genetic disposition, social vulnerabilities and psychiatric conditions) to predict health and pain-related outcomes. PDAS shares multiple protective factors including levels of social support,13 as well as risk factors, such as being female14,15 or a racial minority.16 Notably, people who report co-occurring chronic pain and affective disorders generally experience greater impairment attributable to distress than do those with chronic pain, depression, or anxiety alone.17 Furthermore, heterogeneity exists among people with PDAS, such that two people with a similar diagnosis may have different symptoms and presentations. As a construct, chronic pain is also highly heterogeneous.18,19 Identifying subgroups of people is critical to developing individualized preventive strategies and treatment plans. Large comorbidity studies recommend a person-centered approach to discern such subgroups.20 We assessed not only the degree to which chronic pain and affective disorders co-occur but we also investigated how these associations related to types of social support, sociodemographic variables, and the number of medical vs mental health visits.
Several theories help explain PDAS comorbidity. The shared vulnerability and maintenance model17 depicts various factors that underlie the development and maintenance of chronic pain and other affective disorders. Cognitive, affective, and neuro-biological mechanisms interact, increasing one’s risk of developing both comorbid chronic pain and DAS. For example, one’s predisposition to catastrophize (a common presentation of anxiety), may induce fear around activity or exercise, inhibiting one’s recovery from injury.21–23 The model also states that common features of depression-anxiety-somatic amplification may be driving (via meditation/underlying mechanisms) both psychiatric and pain comorbidities. Recent research has highlighted shared neural mechanisms and inflammatory processes, contributing to high rates of comorbidities between pain, depression, and anxiety.11 As such, chronic pain and DAS share risk and maintenance features, likely interacting in a bidirectional nature, which unfold over time. Similarly, Soltani et al10 proposed a recent theoretical framework describing links among psycho-social outcomes, neurobiological pathways, and chronic pain. Specifically, this model posits that person-specific factors are related to the bidirectional relation between depression and chronic pain. Soltani et al10 also emphasized how family social support is related to these person-specific factors.
Another possible theory, the diathesis-stress biopsychosocial model of chronic pain,12 posits the potential diathesis and psychosocial factors—depression, anxiety, pain sensory catastrophizing or amplification—that contribute to the course and prognosis of chronic pain. A hypothesis of emotion regulation also indicates that chronic pain may result in someone using unhealthy coping skills that fail to improve outcomes and may lead to experiencing more DAS.4 Finally, the Communal Coping Model of Pain Catastrophizing shifts the focus from the individual to the social level.24 Specifically, the expression of pain may result in other people’s altered expectations, extra assistance, or empathetic responses. Conversely, it is also possible that an exaggerated expression of pain may result in negative responses from others, which may lead to social rejection and concomitant anxiety and depression.24
Assuming homogeneity in the population, several cross-sectional studies that assessed chronic pain and affective disorder comorbidity have relied on factor analyses to determine the relationships among these variables,25,26 but such variable-oriented approaches are problematic. If, and when, there is heterogeneity in the population, then aggregated results may not apply to individual-based relations, posing the risk of an ecological fallacy.27 Furthermore, variable-oriented approaches that tailor individual treatments often examine moderators of treatment effects, such as age or problem severity,28 but have limited ability to simultaneously examine multiple moderators.29 In contrast, a person-centered approach “… uses multiple indicator variables simultaneously to define subgroups, allowing for more precise matching of subgroups with appropriate treatments”.29 Therefore, person-centered approaches that account for population heterogeneity are recommended.30,31 One such approach involves Latent Profile Analysis (LPA), which groups individuals into latent homogeneous classes based on similar response patterns across continuous indicators that assess symptom severity.32 LPA is better suited to examine comorbidity because it will identify whether a proportion of the sample reports chronic pain, depression, or anxiety by themselves or in a combination of all three.
This person-centered approach has been used to examine heterogeneity separately in major depressive disorders,33 anxiety disorders,34 non-chronic pain,35 and chronic pain.36,37 To our knowledge, only three studies—all of which have some limitations—have conducted LPA on chronic pain and mental health comorbidities.36–38 First, none examined somatic-related symptoms. Second, the chronic pain subgroups most frequently examined were derived based on pain severity, so it is unclear in what ways mental health issues were related to pain interference. Third, chronic lower back pain was examined most often with less information provided about other chronic pain diagnoses. Fourth, because they frequently focused on risk factors, studies that examined heterogeneity in chronic pain and psychological comorbidities rarely investigated the role of protective factors, such as social support or meditation. Lastly, our understanding is further limited because none of these studies included depression and anxiety items based on clinical interviews.
Consequently, we extended the research to assess heterogeneity in chronic pain-depression-anxiety-somatic amplification symptomatology using nationally representative data. Our study had two goals: 1) examine the best-fitting latent class solution that categorizes participants based on their responses to chronic pain, anxiety, depression, and somatic amplification items; and 2) examine associations among the relevant sociodemographic risk factors, as well as protective factors, frequently associated with group membership. We also examined links between healthcare visits (both medical and mental health) and PDAS in differentiating comorbidity profiles. Research has indicated a link between female gender and higher levels of comorbidity between chronic pain and depression/anxiety.6,39 There is also a relationship between racial minority status and worse comorbidity patterns,15 as well as between low social support and higher levels of comorbidity.40,41 There have been mixed results with respect to age: both younger16 and older groups6 have exhibited higher levels of comorbidity.
Methods
Participants and Procedure
We analyzed data from 1,027 participants in the third wave of the National Survey of Midlife Development in the United States (MIDUS), a 2013 national survey of non-institutionalized, English-speaking adults residing in the U.S.42,43 The study received Institutional Review Board (IRB) approval from the University of Wisconsin–Madison. The MIDUS study, from which the data used in the present study were drawn, performed all procedures involving human protections in accordance with the ethical standards of the University of Wisconsin IRB.
Most sociodemographic variables (except income) were obtained from the baseline phone interviews, whereas most health questions (except subjective health, smoking, and drinking behaviors) were obtained from the self-administered questionnaires.43 The survey was multimodal, employing an initial 30-minute phone interview followed by a set (two) of questionnaires, which were mailed to individuals after completing the phone interview.43 Most of the scales that measured psychosocial and health-related outcomes were from the self-administered surveys while demographic information was obtained from the phone interviews. Detailed information regarding data sampling, estimate of sampling, response and selection bias can be found from previous reports in Radler & Ryff43 and Radler.44 Participants ranged in age from 25 to 74 (M = 65.2 years, SD = 11.2) with 41.9% identifying as male and 58.1% as female. Approximately 89.2% identified as White, 3.3% as Black and/or African American, 1.2% as Native American or Alaskan Islander, 0.2% as Asian, 0.1% as Native Hawaiian or Pacific Islander, and 5.0% identified as other races/ethnicities. To enable us to assess employer/colleague support, all study participants were employed and experienced some form of chronic pain. Subjects participated in telephone interviews or completed self-administered questionnaires (IRB approval by the University of Wisconsin), both of which measured behavioral, psychological, and social factors, as well as those related to health and well-being.
Measures
Chronic Pain
To assess for the presence and severity of chronic pain, we first asked the MIDUS screening question: “Do you have chronic pain, that is do you have pain that persists beyond the time of normal healing and has lasted anywhere from a few months to many years?” Those who responded “Yes” were then asked, Brief Pain Inventory (BPI) [“During the past week, how much did your pain interfere with your enjoyment of life”] on a scale of 0 (not at all) to 10 (completely) to assess their pain severity and their score on the BPI interference scale was then calculated.45 The BPI is an instrument possessing good reliability that assesses the degree to which chronic pain interferes with general activity, walking, work, mood, relationships with others, sleep, and enjoyment of life.46 Shortened interference scales are frequently used as some items may not apply to all patients.47 The shortened version was given to all of those in the dataset with chronic pain. Responses were measured on a 10-point scale (0 = not at all, 10 = completely) and based on our sample, the Cronbach’s alpha was calculated to be 0.91.
Depression
We assessed depression using a structured clinical interview created by the World Health Organization’s Composite International Diagnostic Interview (CIDI).48 A trained telephone interviewer conducted each structured interview. Although this version of the CIDI is based on the Diagnostic and Statistical Manual of Mental Disorders-3rd edition (DSM-III-R),49 the criteria for Major Depressive Disorder are identical to those specified in the DSM-V.50 Participants responded to two yes/no questions that asked, 1) if they experienced depression or sadness for two weeks or greater, and 2) if they have experienced anhedonia for two weeks or greater. Participants who endorsed “Yes” to either question were subsequently asked if they experienced at least five of the following symptoms during the past year: depressed mood or anhedonia (most of the day, nearly every day); decreased or increased appetite; insomnia, fatigue or loss of energy; feelings of worthlessness; concentration problems, and recurrent thoughts of death. The final variable ranged from 0 to 7. Scores between 1 and 7 indicated the range of symptom severity and 0 represented participants who did not have a major depression diagnosis.51 This scale possesses acceptable validity and reliability,48 and the interrater reliability was reported to be 0.95. Regarding validity, good diagnostic concordance overall was found between a clinical checklist and CIDI diagnoses (K = 0.84 for depressive disorders).48
Anxiety
To assess anxiety, participants also participated in structured interviews based on the WHO CIDI Generalized Anxiety Disorder (GAD) determinations, which were based on definitions and criteria specified in the DSM-III-R.49 The telephone interview assessed GAD symptoms over the prior 12 months. Participants were asked how often they experienced any of the following symptoms attributable to worry: restlessness, feeling keyed up or on edge, or having considerable nervous energy; irritability; trouble falling or staying asleep; difficulty keeping their mind on what they were doing; trouble remembering things; low energy; tiring easily, or sore/aching muscles. The final variable ranged from 0 to 10 with scores between 1 and 10 representing the range of symptom severity and 0, which represented a negative diagnosis for GAD. Participants rated the frequency of their symptoms using a 4-point numerical rating scale (1 = most days, 2 = about half the days, 3 = less than half the days, 4 = never). The scale’s interrater reliability was reported to be 0.96 with strong diagnostic concordance between a clinical checklist and CITI diagnoses (K = 0.76 for anxiety disorders).48
Somatic Amplification
The original 5-item somatic amplification scale was used to assess the degree to which somatic symptoms are experienced as intense or uncomfortable.52 Example items included: “I hate to be too hot or too cold” and “Sudden loud noises really bother me”.52 Participants responded on a 4-point Likert scale, ranging from 1 (not at all true) to 4 (extremely true). Total scores were calculated by averaging responses across items with higher scores indicating greater somatic symptom amplification. As shown in prior studies, the scale has good construct validity and strong positive correlations with psychopathological symptoms, including depression, anxiety, hostility, and somatic symptoms.52 According to Barsky et al.,52 the scale displayed adequate internal consistency (Cronbach’s α = 72) in a sample of hospitalized patients. Based on our sample, Cronbach’s alpha was calculated at 0.54.
Doctor and Mental Health Professional Visits
Both the frequency of medical doctor and mental health professional visits were assessed by a single item. Participants were asked, “How many times during the last 12 months did you see a medical doctor?” and “How many times during the last 12 months did you see a mental health professional?”
Meditation/Relaxation Frequency
The use of meditation/relaxation was assessed by asking respondents,
In the past 12 months, either to treat a physical health problem, to treat an emotional or personal problem, to maintain or enhance your wellness, or to prevent the onset of illness, how often did you use relaxation or meditation techniques?
Participants answered on a 5-point numerical scale (1 = a lot, 2 = often, 3 = sometimes, 4 = rarely, to 5 = never).
Social Support
Social support was examined for the following relationships: family members (other than spouse or partner), spouses/partners, friends, coworkers, supervisors, and religious congregations. All items were answered on a 4-point Likert scale (1 = a lot, 2 = some, 3 = a little, to 4 = not at all). Higher scores represented higher levels of perceived support.
Family and Friends’ Support
Family and friends’ support were assessed using four questions: 1) How much do they understand the way you feel about things? 2) How much do they really care about you? 3) How much can you rely on them for help if you have a serious problem? and 4) How much can you open up to them if you need to talk about your worries? According to Walen & Lachman,53 Cronbach’s α reliability coefficients for perceived family support were as follows: non-spouse family = 0.82, friends = 0.88, and spouse = 0.86. Evidence for validity was provided through significant small-to-moderate positive correlations with the life satisfaction and self-reported health.53 Based on our current sample, the Cronbach’s alphas for both the family social and friends social support scales were calculated to be 0.87.
Spouse/Partner Support
Spouse/partner’s support was assessed using six items: 1) How much does your spouse really care about you? 2) How much does he or she understand the way you feel about things? 3) How much does he or she appreciate you? 4) How much do you rely on him or her for help if you have a serious problem? 5) How much can you open up to them if you need to talk about your worries? and 6) How much can you relax and be yourself around them? Correlations with family strain, positive/negative mood, and life satisfaction is supportive of construct validity.53 In a previous study, the Cronbach’s α was reported to be 0.92,54 while based on our current sample, it was calculated to be 0.93.
Supervisor/Coworkers’ Support
Coworker support was assessed using two questions: 1) How often do you get help and support from coworkers? and 2) How often are your coworkers willing to listen to your work-related problems? Three questions were asked to measure supervisor support: 1) How often do you get the information you need from your supervisor(s)? 2) How often do you get help and support from your immediate supervisor? and 3) How often is your immediate supervisor willing to listen to your work-related problems? Evidence for validity was provided through significant small-to-moderate correlations with negative affectivity, work-to-family and family-to-work conflict.55 McDonald’s omega56 for this measure was ω = 0.72.
Religious Support
Religious support was assessed using four questions from the Fetzer Multidimensional Measure of Religiosity for Health Research:57 1) If you were ill, how much would people in your congregation help you? 2) If you had a problem or were faced with a difficult situation, how much comfort would people in your congregation be willing to give you? 3) How often do people in your congregation or spiritual community make too many demands on you? and 4) How often do people in your congregation or spiritual community criticize you and the things you do? Correlation with self-rated health is supportive of construct validity.58 McDonald’s omega56 based on our current sample was ω = 0.72.
Data Analysis
This study performed a secondary analysis of the MIDUS 3 data. Specifically, we utilized latent profile analysis (LPA) to uncover unobserved heterogeneity among adults with chronic pain.59 LPA, a person-centered approach, provides several statistical advantages in addition to the theoretical supports described earlier. Unlike variable-centered analyses like regression and factor analysis that group similar variables and items, LPA groups individuals based on shared characteristics that differentiate members of one group from those of other group(s). If these shared characteristics represent a range of well-defined pathological constructs, then the resulting symptoms and risks could characterize adults with chronic pain by the nature and complexity of their clinical presentations. LPA also allows for deeper investigations because it merges continuous dimensionality and categorical subgroups into a single model.60 Thus, complex interactions among the physical and psychological components of comorbidity can be accounted for simultaneously.
In this study, data analysis proceeded in two stages. In the first, LPA was conducted to identify distinct groups/classes of adults with chronic pain that have similar comorbidity profiles—pain (5 domains: pain interfered with general activity, mood, relations with others, sleep, and enjoyment of life), depression, anxiety, and somatic amplification (“class indicators”). We fitted 1- to 4-class models to determine the number of comorbidity classes. In addition to the class profiles’ substantive meaningfulness and theoretical conformity,61 we considered various diagnostic tests and model fit indices62 including: 1) entropy,63,64 the larger the value and closer to 1, the less classification error; 2) Vuong-Lo-Mendell-Rubin65 likelihood-ratio test (LRT); and 3) adjusted Lo-Mendell-Rubin (aLMR)66 LRT—a significant p value suggests that the k–1-class model should be rejected in favor of the k-class (current) model; and 4) Akaike Information Criteria (AIC)67 and 5) sample-size adjusted Bayesian Information Criterion (aBIC)68—a lower value suggests a better fitting model. For each model, we used robust (full information) maximum likelihood (MLR) estimation implemented in Mplus 8.069 to address missing data (ie, making use of all data points available) and obtain the parameter estimates and sandwich standard errors that are robust to data’s non-normality and non-independence.
Once we identified the optimal number of comorbidity classes, the second stage examined the associations between class membership and theoretically meaningful variables related to comorbidity frequency. Those variables included age, gender, number of times a medical doctor or a mental health professional were seen in the prior 12 months, frequency of using relaxation/meditation techniques during the prior 12 months, as well as support from family, friends, spouses/partners, coworkers, supervisor, and their religious congregation. Specifically, we conducted a t-test or analysis of variance (ANOVA, with post-hoc pairwise comparisons when class difference was significant overall), depending on the number of classes identified, to compare the classes for continuous variables, and Chi-squared or Fisher’s exact test for categorical variables. The class comparisons were performed using SAS 9.4.70
Results
Study Variables’ Descriptive Statistics
Tables 1 and 2 provide the descriptive statistics of the variables analyzed. On average, participants were 65.15 (SD = 11.23) years old, and the majority were female (58.1%) and White (89.2%). Typically, participants experienced mild-to-moderate levels of interference with general activity, mood, relations with others, sleep, and enjoyment of life attributable to their chronic pain. They also reported moderate levels of somatic amplification, but low levels of depression and anxiety. The participants had visited a medical doctor approximately five times and a mental health specialist at least once during the prior 12 months. The majority (70.1%) had never used relaxation or meditation techniques during the prior 12 months, but reported good support from family, friends, spouses/partners, coworkers, supervisors, and their congregations.
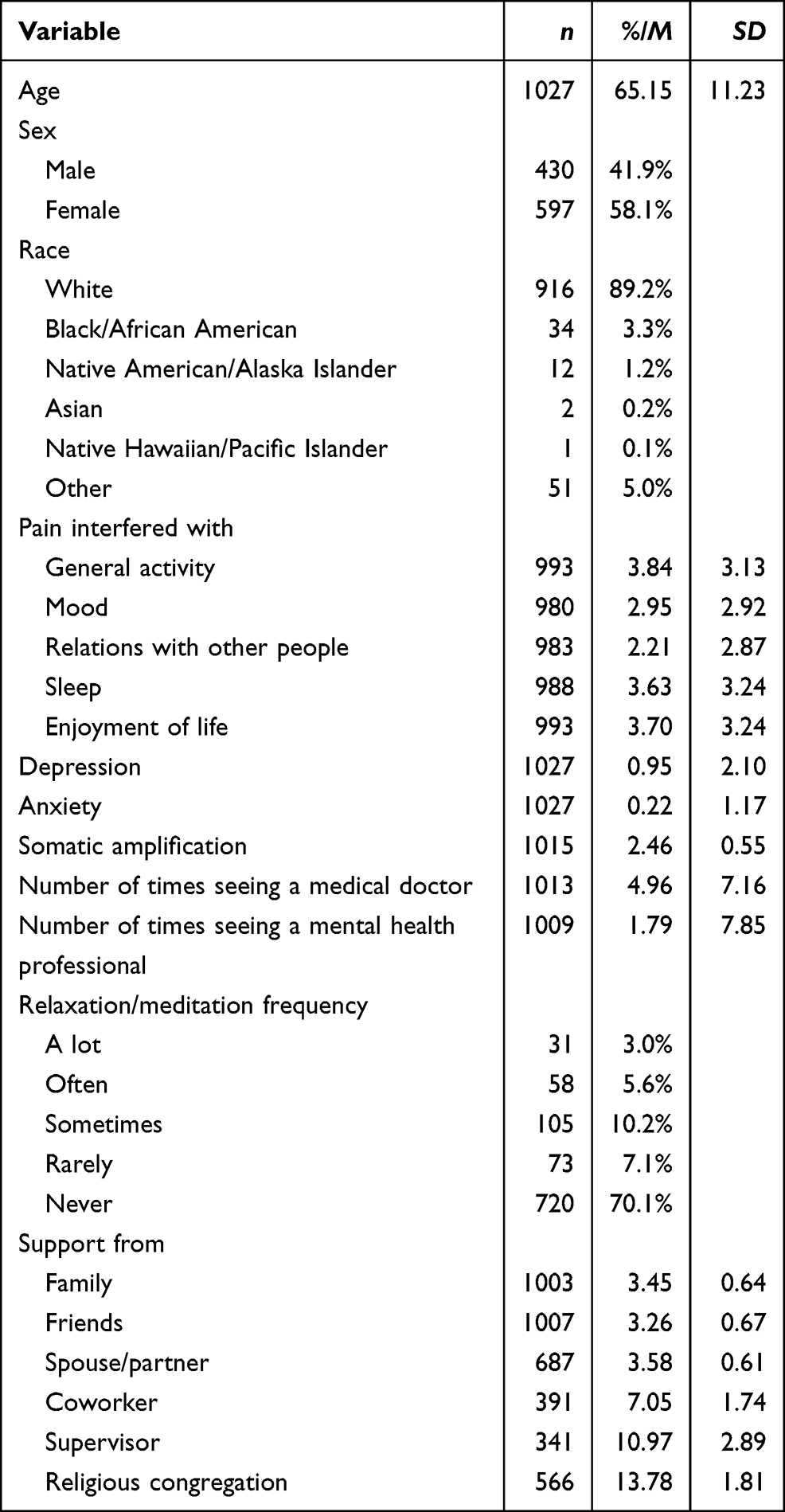 |
Table 1 Descriptive Statistics of Study Variables (N = 1027) |
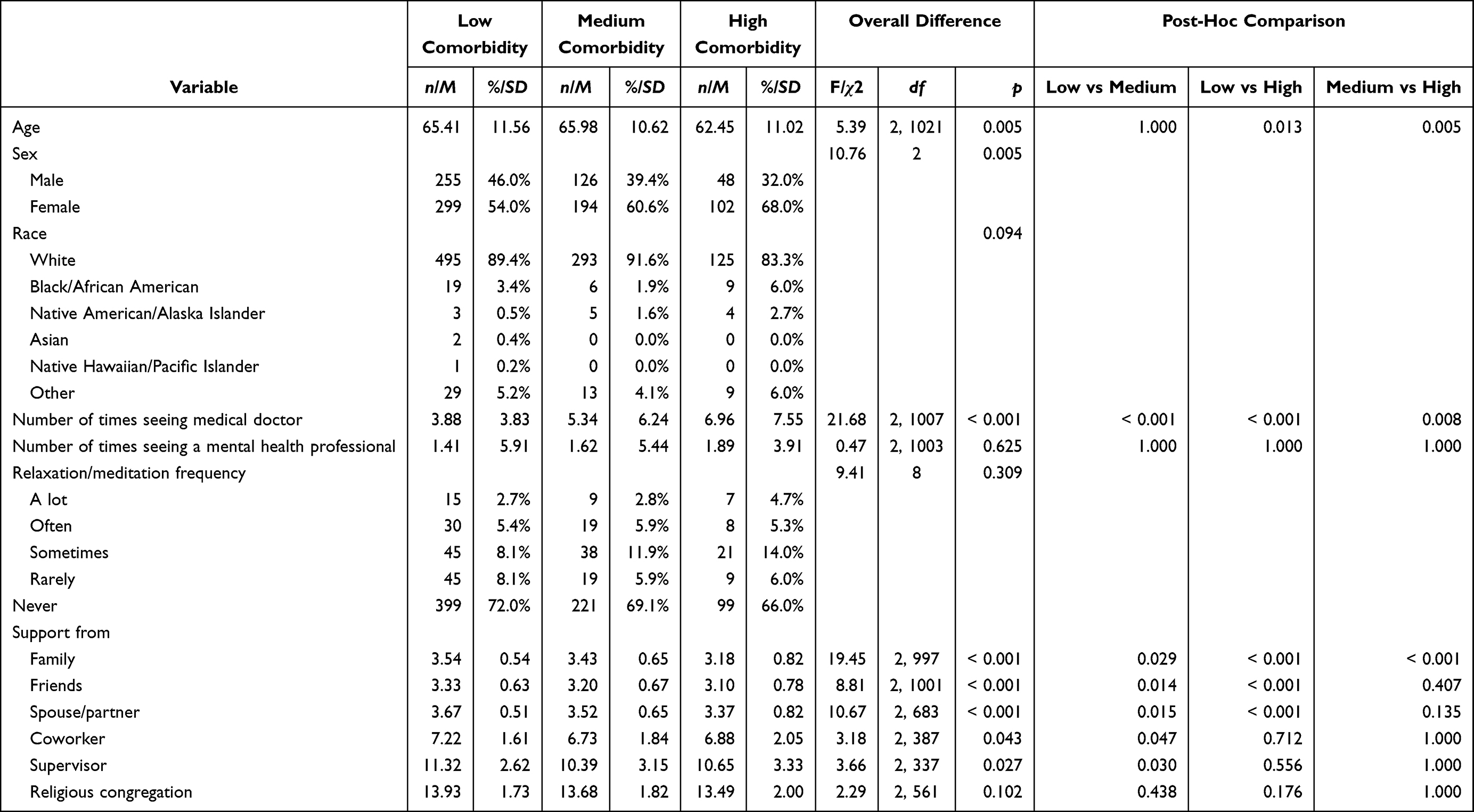 |
Table 2 Class Comparisons |
Comorbidity Classes
Three classes were identified that best represented the profiles of pain, depression, anxiety, and somatic amplification in 1027 adults with chronic pain. Table 3 presents the diagnostic test results and fit values of the latent mixture models that hypothesize one to four classes. Entropy and LRTs are not available for the case of a single class so that comparisons against the 1-class model could not be made using these statistics. The entropy values greater than 0.80 indicated a good separation of the classes in each model.63 The results of both VLMR and LMR LRTs suggested that three classes best represented the data (i.e., significant p values for the 2- and 3-class models and non-significant p-values for the 4-class model). The AIC and aBIC values decreased as the number of classes increased. However, it is known well that both AIC and aBIC tend to overestimate the number of classes.71–74 Therefore, caution should be used when interpreting any AIC or aBIC value. Considering the superiority of the 3-class model indicated by the entropy and LRTs, we concluded that three classes optimally explained the correlations among the participants’ pain, depression, anxiety, and somatic amplification.
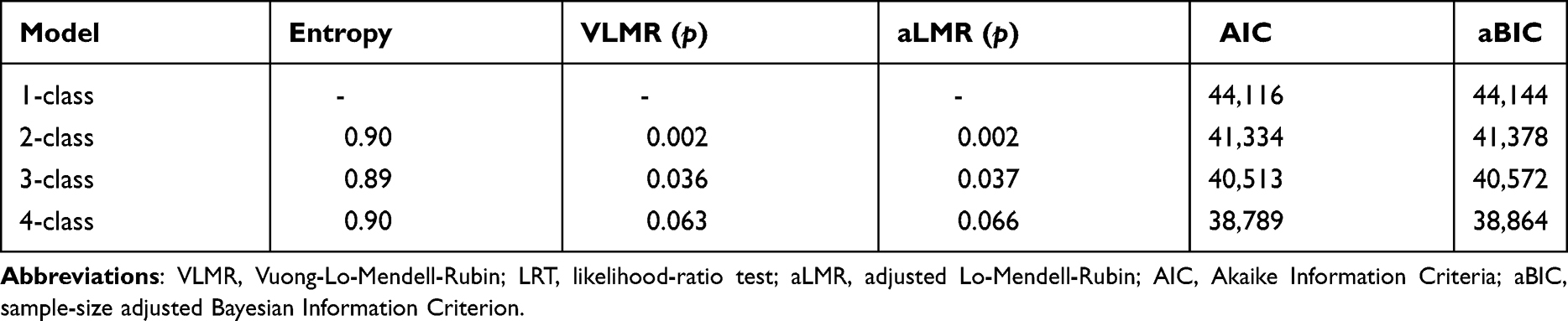 |
Table 3 Diagnostic Test Results and Fit Values of Latent Mixture Models |
The three classes were substantively interpretable and could classify those participants who shared highly distinct comorbidity profiles. As depicted in Figure 1, more than half of the participants (n = 554, 54.1%) were included in the first class and showed low levels of pain, depression, anxiety, and somatic amplification. This class was referred to as Low Comorbidity. The second class (n = 320, 31.3%) was characterized by moderate levels of comorbidity and was referred to as Medium Comorbidity. The last class, referred to as High Comorbidity, accounted for the smallest proportion of the sample (n = 150, 14.6%) and showed high levels of comorbidity.
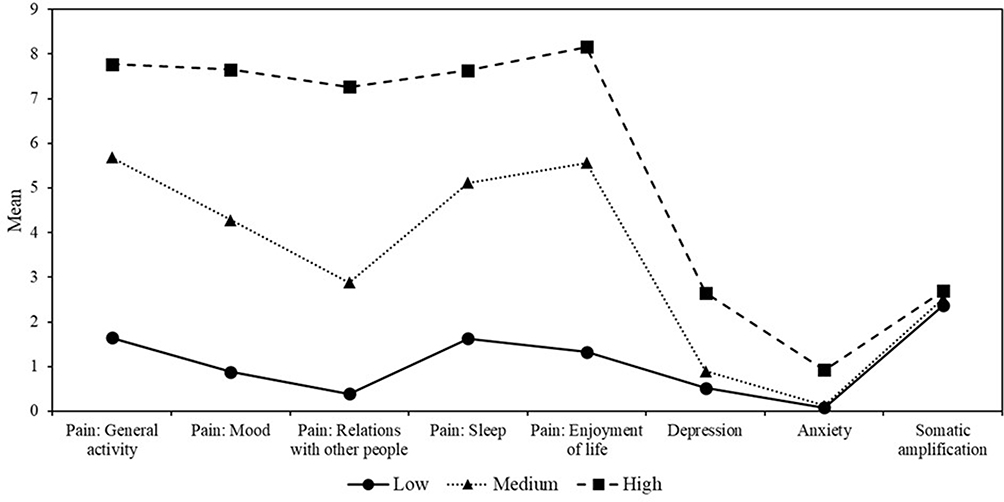 |
Figure 1 Profiles of three comorbidity classes. |
Class Comparisons
Table 2 provides the results of class comparisons of the theoretically meaningful and comorbidity-related variables. The participants in the High Comorbidity class were significantly younger than were those in the Medium and Low Comorbidity classes (both Bonferroni-corrected p < 0.05). The High comorbidity class also included significantly more females compared to the other two classes (p < 0.01). However, the three classes did not differ with respect to the members’ races (p = 0.09). During the prior 12 months, the participants in the High Comorbidity class had seen a medical doctor most often, followed by those in the Medium Comorbidity class and then those in the Low Comorbidity class (all three Bonferroni-corrected p < 0.01). However, there was no difference in the number of visits to a mental health professional (p = 0.63) or the frequency of using relaxation or meditation techniques (p = 0.31).
The degree of comorbidity was significantly associated with the level of support from others. Support from the family was the lowest in the High Comorbidity class followed by the Medium Comorbidity class and then the Low Comorbidity class (all three Bonferroni-corrected p < 0.05). Participants in the High Comorbidity class also reported significantly less support from friends than did those in the Medium and Low Comorbidity classes (both Bonferroni-corrected p < 0.05). Similar results were found for spouse/partner support (both Bonferroni-corrected p < 0.05). Support from coworkers and supervisors was significantly greater for the Low Comorbidity class than for the Medium Comorbidity class (both Bonferroni-corrected p < 0.05), while the three classes did not differ with respect to support from their religious congregation (p = 0.10).
Discussion
The study assessed discrete patterns of chronic pain, depression, anxiety, and somatic amplification symptoms using LPA. Our results determined that a three-class solution that differed only in symptom severity (low comorbidity-class 1, medium comorbidity-class 2, and high comorbidity-class 3) among middle age and older adults fit best. Furthermore, age, sex, number of times a medical doctor was consulted, and social support were significantly associated with the comorbidity classes.
We found that the best-fitting three-class solution was consistent with prior research on chronic pain, depression, and anxiety,36–38 although only one of these studies included pain interference as a class indicator38 and none examined somatic symptoms. Two of the studies included chronic pain patients, but did not include chronic pain level as a class indicator. Our study also differed in its focus on depression and anxiety comorbidity. We extended prior studies’ findings by assessing intra- and interclass heterogeneity in chronic pain-depression-anxiety symptom severity rates that were based on clinical interviews (CIDI and DSM). Interestingly, our findings indicated differences across classes only in chronic pain-depression-anxiety-somatic amplification symptom severity rather than the types of symptoms comprising each homogeneous class. Thus, this comorbidity symptomatology presented together regardless of severity, and classes were distinguished only by the severity of chronic pain, depression, anxiety, and somatic symptoms, rather than the presence or absence of specific symptoms. This pattern reflected a high degree of similarity in symptom severity response patterns across these distress disorders. These results are consistent with the shared vulnerability and maintenance model,17 which asserts cognitive, affective, and neurobiological mechanisms interact, increasing one’s risk of developing both comorbid chronic pain and DAS.
Studies using person-centered approaches to assess symptom heterogeneity, particularly for mood disorders with comorbid chronic pain symptoms, are more limited than variable-centered approaches. Most comorbidity studies to date examined chronic pain and one or two mental health variables. Although there are a few studies (eg)75–77 that examined PDAS concurrently, all studies on this topic were published around or before 2000 and all of them used a variable-centered approach. To the best of our knowledge, our study is the first person-centered study that examined PDAS comorbidity.
Unlike variable-centered analyses like regression and factor analysis that group similar variables and items, LPA groups individuals based on shared characteristics that differentiate members of one group from those of other group(s). If these shared characteristics represent a range of well-defined pathological constructs, then resulting symptoms and risks could characterize adults with chronic pain by the nature and complexity of their clinical presentation. Also, the use of LPA allows for a deeper investigation because it merges continuous dimensionality and categorical sub-groups into a single model.60 Thus, complex interactions among the physical and psychological components of comorbidity can be simultaneously taken into account. The use of LPA with symptoms of multiple conditions highlighted important symptom differences (severity and/or type) among sub-classes of people. This finding may inform more individualized clinical assessments and treatments and help us better anticipate that people with severe chronic pain may present with greater levels of depression and anxiety symptoms, either overlapping with chronic pain symptoms or at different times, longitudinally. Therefore, LPA approaches allow for a more refined categorization of individuals.31
Our second objective was to ascertain whether differential associations were apparent between chronic pain, depression, anxiety, and somatic amplification groupings and levels of different types of social support. Overall, as the chronic pain-depression-anxiety-somatic symptomatology increased by group, the perceived levels of social support decreased. Specifically, support from family was the lowest in the high comorbidity class, followed by the medium, and then the low. Participants in the high comorbidity class reported significantly less support from friends, as well as from their spouses/partners, than did those in the medium and low comorbidity classes. In particular, coworker and supervisor support was significantly greater for the low comorbidity class compared to the medium class. The three classes did not differ in the religious support they received.
Our findings are consistent with the limited literature that has assessed social support as it relates to co-occurring chronic pain-depression-anxiety symptomatology:41 an increase in social support was associated with lower levels of comorbidity. At least two explanations can help us understand this. A common explanation is the buffering hypothesis,78 wherein social support systems help buffer people from adverse effects of stressful events, in this case, chronic pain and psychological comorbidity. Therefore, people who perceive better social support are likely to have lower comorbidity. The Communal Coping Model of Pain Catastrophizing is another framework that can explain the associations between social support and pain comorbidities. Exaggerated expressions of pain may repel people and those with severe comorbidities may be less likely to receive social support. Future longitudinal or experimental studies may help clarify the directional links among social support, chronic pain, and psychological comorbidities.
There are three additional points regarding the symptom patterns. First, people in the low comorbidity class presented with few anxiety symptoms. They did, however, report probable chronic pain and depression diagnoses. This trend is consistent with research that found a greater prevalence of depression than anxiety in chronic pain patients.2,4,9 Findings from studies that examined chronic pain and psychological comorbidities also shared similar patterns, in which more depressive symptoms (vs anxiety) were associated with chronic pain in comorbidity profiles.36,37 Second, the level of somatic amplification in the three comorbidity profiles did not differ significantly, indicating that regardless of comorbidity severity, people may report similar levels of somatic symptoms. This information can help clinicians more effectively diagnose comorbidity issues among chronic pain patients along with adding to the literature in which few studies have examined comorbidity among chronic pain, depression, anxiety, and somatic symptoms. Third, chronic pain’s comorbidity with anxiety, depression, and somatic amplification increased with class symptom severity. This is consistent with research that has found that, as the severity of chronic pain increases, comorbidity with conditions such as mood disorders also increases.36,37 People with less severe chronic pain symptoms may also have comorbid depression, psychosomatic issues, and anxiety disorders. They could still benefit from clinical interventions. Therefore, rather than assume that only those people with more severe chronic pain have mood disorders, those with what appears to be little chronic pain still have psychological comorbidities. Because few studies to date have examined people with less severe comorbidities, further research is needed.
Among sociodemographic risk factors, only sex and age predicted class membership. Being female and younger were associated with membership in a higher symptom severity class. These results are consistent with the existing literature that has reported that being female is a risk factor in chronic pain and psychological comorbidities.6,39 Our results indicated a significant relationship between younger age and membership in the more symptomatic comorbidity class, a pattern also found in another chronic pain-psychological comorbidity study.16 While being older is typically associated with greater chronic pain symptoms, older age has also been associated with comorbid chronic pain and depression.3,15 However, limited research has been conducted to examine the associations among age, chronic pain, and anxiety. Only one study16 examined the relationship between age and chronic pain-depression-anxiety comorbidities, which found that younger patients were more likely to report pain complaints, depression, and anxiety. The relationships among these variables require further research. Our study contributes to this body of research by providing evidence and explanations of the associations between age and chronic pain-depression-anxiety comorbidities. These results demonstrate that clinicians should consider the importance of certain sociodemographic factors, such as sex and age, and the way they may affect their patients’ symptoms relating to comorbid pain and mood disorders.
Racial minority status as a risk factor, along with meditation/relaxation frequency and religious support as protective factors, was not associated with class membership. Similarly, the number of mental health professional visits did not differentiate between classes, although more severe levels of comorbidity symptomatology were associated with an increased number of medical doctor visits. Some studies have examined the number of medical care visits in relation to chronic pain, finding that more severe chronic pain conditions significantly increased the likelihood of frequent healthcare visits.79 Greater mental health care needs among chronic pain patients were also associated with more frequent healthcare visits.79 To date, our study is the only one that has examined the associations between the frequency of medical vs mental healthcare visits and chronic pain-depression-anxiety-somatic symptomatology. Our results call for increased attention to the associations between medical/mental healthcare visits and chronic pain comorbidities to optimize healthcare services by focusing on patients with comorbidities who have differing needs.
Limitations and Future Research
Although this study has implications that may contribute to our understanding of, and ability to treat, chronic pain and psychological comorbidity symptoms, it is not without limitations. First, the use of cross-sectional data precludes any conclusions about the direction of effects. For example, among those in the highest comorbidity group, we were unable to determine if low social support leads to greater symptoms or vice versa. Future studies should investigate longitudinal associations among chronic pain, depression, anxiety, and somatic amplification over time. Although using archival data restricted our ability to choose measurements, we believe that the benefit of our data outweighs that weakness because we were able to provide generalizable findings from a nationally representative sample of adults with chronic pain in the United States. In addition, the comorbidity associations between pain interference, depression, anxiety and somatic amplification, as well as how they relate to various types of social support, have not been examined to date, so the present study adds to pain comorbidity research as it relates to psychosocial factors. Additionally, using a nationally representative sample did enable us to generalize our findings to less symptomatic groups. Second, due to using secondary data, we were unable to use well-established measures (eg, somatic amplification and social support), and two of our measures had Cronbach’s alpha of 0.54 and 0.57, which are below the 0.70 traditional standard. Future studies should utilize well-validated self-report measures to assess somatic amplification and social support. Third, our sample was primarily older White adults, limiting our ability to generalize the results in other age/racial groups. Fourth, while we used the Brief Pain Inventory to assess pain interference, a single retrospective question was used to discern chronic pain conditions. Due to the subjectivity in chronic pain interpretations, it is possible participants may have under-reported or over-reported their pain symptoms without additional criteria and clinical judgments from healthcare providers. Thus, it will be important for future researchers to conduct follow-up studies with a well-validated clinical interview to reduce the disparities in what constitutes chronic pain. Lastly, because LPA is primarily an exploratory and data reduction technique, correct class assignments rely on model factors, including covariate effects and sample size,80,81 making model misspecification possible.
Implications
This study has important clinical and theoretical implications. First, when looking at symptoms of typical comorbid disorders, there seems to be heterogeneity in symptom severity rather than in symptom type across classes over time. Based on the biopsychosocial framework and the body of research in integrative and holistic treatment, assessing risks that may contribute to the development of both pain and psychiatric disorders (based on either demographic or psychosocial factors) significantly enhances provider ability to determine urgency and inform treatment plans and recommendations, especially during triage when not all resources and services are simultaneously available to patients.12,82,83 Thus, the study findings facilitate practitioners’ efficiency to differentiate patients between mild and severe risks for pain and psychiatric comorbidities. For instance, a person who lacks social support, identifies as a younger female, and demonstrates higher levels of DAS is at higher risk, which may warrant more immediate and comprehensive help as compared to others who indicate mild or moderate risk levels. Studies have shown that pretreatment risk assessment to identify who may benefit from a primary care or an interdisciplinary approach is clinically pivotal to treatment outcomes.12 Patients who received a pretreatment clinical risk assessment reported greater improvements in quality of life and satisfaction compared to those who did not.84 Clinicians’ routine assessment of specific psychosocial outcomes (eg, depression, anxiety, somatic amplification) in addition to pain symptoms will assist clinicians in providing patients with appropriate outpatient mental health referrals. Second, the similarity of types of response patterns across classes supports the idea that chronic pain and mood disorders may share certain risk and protective factors. Third, finding distinct classes of people who differed consistently in symptom severity across symptoms further supports the usefulness of person-centered approaches. Lastly, younger adults, female adults, and adults with less perceived social support may demonstrate more severe comorbidity symptomatology. These variables may be important to address in preventive efforts and should be highlighted in clinical assessments so more tailored treatments can be provided. Encouraging people to build and maintain better social supports may serve as a protective factor for chronic pain, depression, anxiety, and somatic symptom severity.
This study lays the foundation for addressing similar questions about overlapping symptoms during the same period. This will shed light on whether these disorders are attributable to a common mechanism among middle to older age adults and may inform transdiagnostic treatments.85 In conclusion, the study suggests that chronic pain, depression, anxiety, and somatic amplification co-occur, possibly related to shared risk and protective factors. Given this co-occurrence, this study highlighted the need for continual assessment and targeted treatment of co-occurring chronic pain and psychological comorbidities.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding authors on request.
Ethical Approval
The MIDUS study, from which the data used in the present study were drawn, was approved by the University of Wisconsin–Madison IRB and performed all procedures involving human protections in accordance with its ethical standards, as well as the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all MIDUS participants. Since the study uses publicly available de-identified data, Texas Tech University IRB office waived the need for additional approval of the study.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
The authors did not receive any funding for this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Bair M, Robinson R, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Int Med. 2003;163(20):2433–2445. doi:10.1001/archinte.163.20.2433
2. De Heer E, Gerrits M, Beekman A, et al. The association of depression and anxiety with pain: a study from NESDA. PLoS One. 2014;9(10):1–11. doi:10.1371/journal.pone.0106907
3. Gadermann A, Alonso J, Vilagut G, Zaslavsky A, Kessler R. Comorbidity and disease burden in the National Comorbidity Survey Replication (NCS-R). Depress Anxiety. 2012;29(9):797–806. doi:10.1002/da.21924
4. Gerrits M, Van Oppen P, Leone S, Van Marwijk H, Van Der Horst H, Penninx B. Pain, not chronic disease, is associated with the recurrence of depressive and anxiety disorders. BMC Psychiat. 2014;14(1):1–9. doi:10.1186/1471-244X-14-187
5. Katz J, Rosenbloom B, Fashler S. Chronic pain, psychopathology, and DSM-5 somatic symptom disorder. Can J Psychiatry. 2015;60(4):160–167. doi:10.1177/070674371506000402
6. Tsang A, Von Korff M, Lee S, et al. Common chronic pain conditions in developed and developing countries: gender and age differences and comorbidity with depression-anxiety disorders. J Pain. 2008;9(10):883–891. doi:10.1016/j.jpain.2008.05.005
7. Von Korff M, Crane P, Lane M, et al. Chronic spinal pain and physical–mental comorbidity in the United States: results from the national comorbidity survey replication. Pain. 2005;113(3):331–339. doi:10.1016/j.pain.2004.11.010
8. McWilliams L, Cox B, Enns M. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample. Pain. 2004;106(1):127–133. doi:10.1016/S0304-3959(03)00301-4
9. Dahan A, Van Velzen M, Niesters M. Comorbidities and the complexities of chronic pain. Anesthesiology. 2014;121(4):675–677. doi:10.1097/ALN.0000000000000402
10. Soltani S, Kopala-Sibley DC, Noel M. The co-occurrence of pediatric chronic pain and depression: a narrative review and conceptualization of mutual maintenance. Clin J Pain. 2019;35(7):633–643. doi:10.1097/AJP.0000000000000723
11. Ishak WW, Wen RY, Naghdechi L, et al. Pain and depression: a systematic review. Harv Rev Psychiatry. 2018;26(6):352–363. doi:10.1097/HRP.0000000000000198
12. Bevers K, Watts L, Kishino ND, Gatchel RJ. The biopsychosocial model of the assessment, prevention, and treatment of chronic pain. US Neurol. 2016;12(2):98–104. doi:10.17925/USN.2016.12.02.98
13. Jang Y, Haley W, Small B, Mortimer J. The role of mastery and social resources in the associations between disability and depression in later life. Gerontologist. 2002;42(6):807–813. doi:10.1093/geront/42.6.807
14. Demyttenaere K, Bruffaerts R, Lee S, et al. Mental disorders among persons with chronic back or neck pain: results from the world mental health surveys. Pain. 2007;129(3):332–342. doi:10.1016/j.pain.2007.01.022
15. Miller L, Cano A. Comorbid chronic pain and depression: who is at risk? J Pain. 2009;10(6):619–627. doi:10.1016/j.jpain.2008.12.007
16. Husain M, Rush A, Trivedi M, et al. Pain in depression: STAR*D study findings. J Psychol Res. 2007;63(2):113–122. doi:10.1016/j.jpsychores.2007.02.009
17. Asmundson G, Coons M, Taylor S, Katz J. PTSD and the experience of pain: research and clinical implications of shared vulnerability and mutual maintenance models. Can J Psychiatry. 2002;47(10):930–937. doi:10.1177/070674370204701004
18. Cipher D, Clifford P, Schumacker R. The heterogeneous pain personality: diverse coping styles among sufferers of chronic pain. Altern Ther Health Med. 2002;8:60–69.
19. Vellucci R. Heterogeneity of chronic pain. Clinic Drug Investig. 2012;32:3–10. doi:10.2165/11630030-000000000-00000
20. Vaidyanathan U, Patrick C, Iacono W. Patterns of comorbidity among mental disorders: a person-centered approach. Comp Psychiat. 2011;52(5):527–535. doi:10.1016/j.comppsych.2010.10.006
21. Han C, Pae C. Pain and depression: a neurobiological perspective of their relationship. Psychiat Investig. 2015;12(1):1–8. doi:10.4306/pi.2015.12.1.1
22. Ribeiro S, Kennedy S, Smith Y, Stohler C, Zubieta J. Interface of physical and emotional stress regulation through the endogenous opioid system and opioid receptors. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(8):1264–1280. doi:10.1016/j.pnpbp.2005.08.011
23. Vlaeyen J, Linton S. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
24. Sullivan M, Tripp D, Santor D. Gender differences in pain and pain behavior: the role of catastrophizing. Cognit Ther Res. 2000;24(1):121–134. doi:10.1023/A:1005459110063
25. Lerman S, Rudich Z, Shahar G. Distinguishing affective and somatic dimensions of pain and depression: a confirmatory factor analytic study. J Clin Psychol. 2010;66:456–465.
26. McCracken L, Vowles K, Eccleston C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain. 2004;107(1):159–166. doi:10.1016/j.pain.2003.10.012
27. Von Eye A, Bogat G. Person-oriented and variable-oriented research: concepts, results, and development. Merrill Palmer Q. 2006;53:390–420.
28. Curry J, Rohde P, Simons A, et al. Predictors and moderators of acute outcome in the Treatment for Adolescents with Depression Study (TADS). J Am Academy Child Adol Psychiat. 2006;45(12):1427–1439. doi:10.1097/01.chi.0000240838.78984.e2
29. Bonadio F, Dynes M, Lackey J, Tompsett C, Amrhein K. Grouping youth with similar symptoms: a person-centered approach to transdiagnostic subgroups. J Clin Psychol. 2016;72(7):676–688. doi:10.1002/jclp.22274
30. Muthen B, Muthen L. Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcohol Clin Exp Res. 2000;24(6):882–891. doi:10.1111/j.1530-0277.2000.tb02070.x
31. Nugent N, Koenen K, Bradley B. Heterogeneity of posttraumatic stress symptoms in a highly traumatized low income, urban, African American sample. J Psychiat Res. 2012;46(12):1576–1583. doi:10.1016/j.jpsychires.2012.07.012
32. McCutcheon A. Latent Class Analysis (No. 64). Thousand Oaks, CA: SAGE; 1987.
33. Barton Y, Barkin S, Miller L. Deconstructing depression: a latent profile analysis of potential depressive subtypes in emerging adults. Spirit Clin Pract. 2017;4(1):1–21. doi:10.1037/scp0000126
34. Mammarella I, Donolato E, Caviola S, Giofre D. Anxiety profiles and protective factors: a latent profile analysis in children. Personality Individ Diff. 2018;124:201–208. doi:10.1016/j.paid.2017.12.017
35. Holden S, Rathleff M, Roos E, Jensen M, Pourbordbari N, Granven-Nielsen T. Pain patterns during adolescence can be grouped into four pain classes with distinct profiles: a study on a population-based cohort of 2953 adolescents. Euro J Pain. 2018;22(4):793–799. doi:10.1002/ejp.1165
36. Rabey M, Beales D, Slater H, O’Sullivan P. Multidimensional pain profiles in four cases of chronic non-specific axial low back pain: an examination of the limitations of contemporary classification systems. Man Ther. 2015;20(1):138–147. doi:10.1016/j.math.2014.07.015
37. Rabey M, Smith A, Beales D, Slater H, O’Sullivan P. Differing psychologically derived clusters in people with chronic low back pain are associated with different multidimensional profiles. Clin J Pain. 2016;32(12):1015–1027. doi:10.1097/AJP.0000000000000363
38. Banta-Green C, Merrill J, Doyle S, Boudreau D, Calsyn D. Opioid use behaviors, mental health and pain–development of a typology of chronic pain patients. Drug Alcohol Depend. 2009;104(1–2):34–42. doi:10.1016/j.drugalcdep.2009.03.021
39. Kivrak Y, Kose-Ozlece H, Ustundag M, Asoglu M. Pain perception: predictive value of sex, depression, anxiety, somatosensory amplification, obesity, and age. Neuropsychiatr Dis Treat. 2016;12:1913–1918. doi:10.2147/NDT.S106974
40. Smite D, Rudzite I, Ancane G. Sense of social support in chronic pain patients. SHS Web Conf. 2012;2:1–6.
41. Zyrianova Y, Kelly B, Gallagher C, et al. Depression and anxiety in rheumatoid arthritis: the role of perceived social support. Irish J Med Sci. 2006;175(2):32–36. doi:10.1007/BF03167946
42. Brim O, Ryff C, Kessler R. How Healthy are We? A National Study of Wellbeing at Midlife. University of Chicago Press; 2004.
43. Radler BT, Ryff CD. Who participates? Accounting for longitudinal retention in the MIDUS national study of health and wellbeing. J Aging Health. 2010;22(3):307–331. doi:10.1177/0898264309358617
44. Radler BT. The midlife in the United States (MIDUS) series: a national longitudinal study of health and well-being. Open Health Data. 2014;2(1):e3. doi:10.5334/ohd.ai
45. Raichle K, Osborne T, Jensen M, Cardenas D. The reliability and validity of pain interference measures in persons with spinal cord injury. J Pain. 2006;7(3):179–186. doi:10.1016/j.jpain.2005.10.007
46. Brown T, Partanen J, Chuong L, Villaverde V, Chantal Griffin A, Mendelson A. Discrimination hurts: the effect of discrimination on the development of chronic pain. Soc Sci Med. 2018;204:1–8. doi:10.1016/j.socscimed.2018.03.015
47. Harding G, Schein J, Nelson W, et al. Development and validation of a new instrument to evaluate the ease of use of patient-controlled analgesic modalities for postoperative patients. J Med Econ. 2010;13(1):42–54. doi:10.3111/13696990903484637
48. Wittchen H. Reliability and validity studies of the WHO-Composite International Diagnostic Interview (CIDI): a critical review. J Psychiat Res. 1994;28:57–84.
49. American Psychiatric Association. Committee on Nomenclature and Statistics. In: Diagnostic and Statistical Manual of Mental Disorders. Revised
50. American Psychiatric Association. Committee on Nomenclature and Statistics. In: Diagnostic and Statistical Manual of Mental Disorders.
51. Wang P, Berglund P, Kessler R. Recent care of common mental disorders in the United States. J Gen Internal Med. 2000;15(5):284–292. doi:10.1046/j.1525-1497.2000.9908044.x
52. Barsky A, Goodson J, Lane R, Cleary P. The amplification of somatic symptoms. J Psychosom Med. 1988;50:510–519.
53. Walen HR, Lachman ME. Social support and strain from partner, family, and friends: costs and benefits for men and women in adulthood. J Soc Pers Relat. 2000;17(1):5–30.
54. Grzywacz J, Marks N. Family solidarity and health behaviors: evidence from the National Survey of Midlife Development in the United States. J Fam Issues. 1999;20(2):243–268. doi:10.1177/019251399020002004
55. Selvarajan TT, Singh B, Cloninger PA. Role of personality and affect on the social support and work family conflict relationship. J Vocat Behav. 2016;94:39–56. doi:10.1016/j.jvb.2016.02.004
56. McDonald RP. Test Theory: A Unified Treatment. Lawrence Erlbaum Associates Publishers; 1999.
57. Fetzer Institute/National Institute on Aging Working Group. Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research. John E. Fetzer Institute; 1999.
58. Homan KJ, Hollenberger JC. Religious support moderates the long reach of adverse childhood events on physical health in middle to late adulthood. J Relig Health. 2021;60(6):4186–4208. doi:10.1007/s10943-021-01259-w
59. Lazarsfeld P, Henry N. Latent Structure Analysis. Boston, Massachusetts; 1968.
60. Roh S, Lee Y, Lee J, Martin J. Typology of religiosity/spirituality in relation to perceived health, depression, and life satisfaction among older Korean immigrants. Aging Ment Health. 2014;18(4):444–453. doi:10.1080/13607863.2013.848837
61. Marsh H, Lüdtke O, Trautwein U, Morin A. Latent profile analysis of academic self-concept dimensions: synergy of person- and variable-centered approaches to the internal/external frame of reference model. Struct Equ Modeling. 2009;16(2):1–35. doi:10.1080/10705510902751010
62. McLachlan G, Peel D. Mixtures of factor analyzers. In: Finite Mix Models. John Wiley & Sons; 2000:238–256.
63. Celeux G, Soromenho G. An entropy criterion for assessing the number of clusters in a mixture model. J Classif. 1996;13(2):195–212. doi:10.1007/BF01246098
64. Ramaswamy V, DeSarbo W, Reibstein D, Robinson W. An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Mark Sci. 1993;12(1):103–124. doi:10.1287/mksc.12.1.103
65. Vuong Q. Likelihood ratio tests for model selection and nonnested hypotheses. Econometrica. 1989;57(2):307–333. doi:10.2307/1912557
66. Lo Y, Mendell N, Rubin D. Testing the number of components in a normal mixture. Biometrika. 2001;88(3):767–778. doi:10.1093/biomet/88.3.767
67. Akaike H. Factor analysis and AIC. Psychometrika. 1987;52(3):317–332. doi:10.1007/BF02294359
68. Sclove L. Application of model-selection criteria to some problems in multivariate analysis. Psychometrika. 1987;52(3):333–343. doi:10.1007/BF02294360
69. Muthén L, Muthén BO. Mplus User’s Guide.
70. Institute SAS. SAS/STAT 9.4 User’s Guide. Cary, North Carolina; 2002–2012.
71. Henson J, Reise S, Kim K. Detecting mixtures from structural model differences using latent variable mixture modeling: a comparison of relative model fit statistics. Struct Equ Modeling. 2007;14(2):202–226. doi:10.1080/10705510709336744
72. Nylund K, Asparouhov T, Muthén B. Deciding on the number of classes in latent class analysis and growth mixture modeling. A Monte Carlo simulation study. Struct Equ Modeling. 2007;14(4):535–569. doi:10.1080/10705510701575396
73. Tofighi D, Enders C. Identifying the correct number of classes in growth mixture models. In: Hancock G, Samuelsen K, editors. Advances in Latent Variable Mixture Models. Charlotte, North Carolina: Information Age Publishing; 2008:317–341.
74. Yang C. Evaluating latent class analysis models in qualitative phenotype identification. Comput Stat Data Anal. 2006;50(4):
75. Gregory RJ, Manring J, Berry SL. Pain location and psychological characteristics of patients with chronic pain. Psychosomatics. 2000;41(3):216–220. doi:10.1176/appi.psy.41.3.216
76. Yavuz BG, Aydinlar EI, Dikmen PY, Incesu C. Association between somatic amplification, anxiety, depression, stress and migraine. J Headache Pain. 2013;14(1):53. doi:10.1186/1129-2377-14-53
77. McCracken LM, Faber SD, Janeck AS. Pain-related anxiety predicts non-specific physical complaints in persons with chronic pain. Behaviour Research and Therapy. 1998;36(6):191–225. doi:10.1016/S0005-7967(97)10039-0
78. Cohen S, Wills T. Stress, social support and the buffering hypothesis. Psychol Bullet. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
79. Von Korff M, Lin E, Fenton J, Saunders K. Frequency and priority of pain patients’ health care use. ClinJ Pain. 2007;23(5):400–408. doi:10.1097/AJP.0b013e31804ac020
80. Lee C, Ryff CD. Pathways linking combinations of early-life adversities to adult mortality Tales that vary by gender. Soc Sci Med. 2019;240:112566. doi:10.1016/j.socscimed.2019.112566
81. Lubke G, Muthén BO. Performance of factor mixture models as a function of model size, covariate effects, and class-specific parameters. Struct Equ Modeling. 2007;149(1):26–47. doi:10.1080/10705510709336735
82. Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical approach for primary care. Med J Aust. 2017;206(6):268–273. doi:10.5694/mja16.00828
83. Gatchel RJ, Maddrey AM. The biopsychosocial perspective of pain. In: Handbook of Clinical Health Psychology: Volume 2. Disorders of Behavior and Health. American Psychological Association; 2004:357–378.
84. Rothman MG, Ortendahl M, Rosenblad A, Johansson AC. Improved quality of life, working ability, and patient satisfaction after a pretreatment multimodal assessment method in patients with mixed chronic muscular pain: a randomized-controlled study. Clin J Pain. 2013;29(3):195–204. doi:10.1097/AJP.0b013e318250e544
85. McEvoy P, Nathan P, Norton P. Efficacy of transdiagnostic treatments: a review of published outcome studies and future research directions. J Cognit Psycho. 2009;23(1):20–33. doi:10.1891/0889-8391.23.1.20
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.