")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Prosthodontic Rehabilitation and Follow-Up Using Maxillary Complete Conventional Immediate Denture
Authors Yeung C , Leung KCM , Yu OY , Lam WYH , Wong AWY , Chu CH
Received 8 July 2020
Accepted for publication 27 August 2020
Published 23 October 2020 Volume 2020:12 Pages 437—445
DOI https://doi.org/10.2147/CCIDE.S271304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Conson Yeung, Katherine Chiu Man Leung, Ollie Yiru Yu, Walter Yu Hang Lam, Amy Wai Yee Wong, Chun Hung Chu
Faculty of Dentistry, The University of Hong Kong, Hong Kong
Correspondence: Chun Hung Chu
Faculty of Dentistry, The University of Hong Kong, 3B26, Prince Philip Dental Hospital, 34 Hospital Road, Sai Ying Pun, Hong Kong
Tel +852 2859 0287
Email [email protected]
Abstract: Despite global efforts to improve individuals’ oral health, a considerable proportion of patients still progress to the stage in which the extractions of all teeth in one arch or both are indicated. An immediate complete denture remains a relatively accessible treatment option, particularly for those patients who cannot afford or do not need implant treatment. It is often one of the best solutions when the complete extraction of the remaining teeth is unavoidable. The denture is fitted immediately after the surgical clearance of teeth. It acts as a splint for helping with haemostasis, preventing trauma, and promoting wound healing. More importantly, an immediate denture can copy the characteristics of the existing dentition and establishes the vertical dimension of occlusion. It offers immediate replacement of the missing teeth, thereby avoiding a period of edentulism and social embarrassment. These treatments help relieve patient anxiety and bring about patient satisfaction. This study used a case report to illustrate the clinical procedures required for the construction of an immediate complete maxillary denture with good retention, support, stability, and aesthetics.
Keywords: prosthodontics, rehabilitation, immediate complete denture, case report
Introduction
Despite global efforts to improve individuals’ oral health, a considerable proportion of patients still progress to the stage in which the extraction of all teeth in one arch or both is indicated.1 Among the treatment options, complete dentures remain a relatively accessible treatment option.2 An immediate complete denture is delivered immediately following the removal of the remaining teeth to replace the lost dentition and associated structures. Patients who have blood disorders, prolonged wound healing, extensive bone loss, emotional disturbances, or mental incapacity may not be suitable for immediate complete dentures. Immediate maxillary complete dentures often perform well particularly for those patients with well-formed ridges.3 An immediate complete denture copies the characteristics of the existing dentition and establishes the vertical dimension of occlusion. It acts as a surgical splint to control haemorrhage and promote healing. It also prevents trauma that arouses from food, the tongue, and the opposing teeth. An immediate complete denture enables the patient to maintain function as well as aesthetics to avoid a period of complete edentulism and social embarrassment. However, this denture treatment is time consuming. It also requires the patient’s frequent attendance. This study used a case report to illustrate the clinical procedures required for the construction of an immediate complete maxillary denture with good retention, support, stability, and aesthetics.
Case Report
A 65-year-old man presented with the complaint of difficulty with chewing, recurrent pain from various regions of the mouth, and poor aesthetics of the teeth. The man’s medical history was clear. Clinical and radiographic examinations yielded the following findings: only the anterior teeth were in occlusion, and the occlusal vertical dimension was reduced (Figure 1). The mandibular anterior teeth had severe tooth wear and were non-vital (Figure 2). Multiple carious teeth, retained roots, over-contoured and splinted metal-ceramic crowns, and multiple missing teeth were found on the maxillary arch (Figure 3), whereas multiple missing teeth and teeth with severe wear were found on the mandibular arch (Figure 4). The radiographic examination showed caries on the teeth of both arches, as well as periodontal disease with generalized moderate to severe horizontal bone loss (Figure 5). Periapical radiolucencies were observed on the retained roots of the maxillary arch and on the anterior teeth of the mandibular arch. The treatment plan was developed with the objective of restoring his oral health by controlling his periodontal disease, eradicating caries, and restoring his chewing function and aesthetics with removable dentures.4
 |
Figure 1 Frontal view, habitual occlusion. |
 |
Figure 2 Severe wear of the lower incisors. |
 |
Figure 3 Upper occlusal view (flipped mirror image). |
 |
Figure 4 Lower occlusal view (flipped mirror image). |
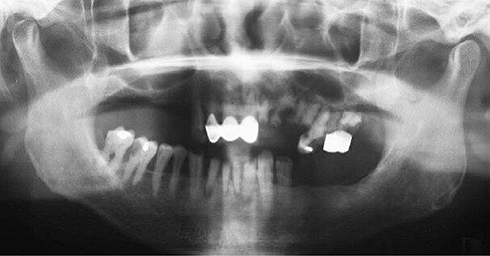 |
Figure 5 Pretreatment orthopantogram. |
Preparation Phase
The patient was informed of the findings, and a treatment plan was formulated following a thorough discussion. The treatment began with oral hygiene instructions and scaling. Caries on the right mandibular first molar and the right mandibular second premolar was restored. In addition, the splinted maxillary anterior crowns were sectioned and replaced with temporary resin crowns. Furthermore, the teeth from the left maxillary lateral incisor to the second molar were extracted due to considerable periodontal attachment loss or severe caries. Clearance of the maxillary arch followed by a maxillary complete denture was planned as well. In view of the patient’s desire to avoid a period of complete maxillary edentulism without replacement, an immediate maxillary complete denture was determined to be the best approach. Further treatment to the mandibular arch included the extractions of mandibular incisors, root canal treatment of the right mandibular first molar, and crowning of the right mandibular first molar and the left mandibular first premolar, as well as the provision of a mandibular partial denture.
Working Impressions
Rapid alveolar bone resorption occurs in the first three months after tooth extraction. Immediate complete maxillary denture construction therefore began about four months after the left maxillary lateral incisor to the second molar were extracted, when the bone resorption in this region had slowed down. Delaying the commencement of denture construction also allowed the posterior sockets to heal without functional loading. Maxillary and mandibular study impressions were then taken. In addition, spaced and perforated maxillary (Figure 6) and mandibular (Figure 7) custom trays for irreversible hydrocolloid impressions were constructed. A space of about 3 mm should be allowed for an irreversible hydrocolloid; otherwise, the material could be torn when an undercut is present. Next, the trays were perforated to improve the tray’s retention of the material. The maxillary working impression recorded the entire denture-bearing area, which the buccal sulcus bordered anteriorly and laterally, and the vibrating line posteriorly (Figure 8). An accurate impression of the remaining teeth was essential for future model trimming and for copying their position and desirable characteristics to the immediate denture. A mandibular study impression was also taken (Figure 9).
 |
Figure 6 Spaced and perforated maxillary custom tray. |
 |
Figure 7 Spaced and perforated mandibular custom tray. |
 |
Figure 8 Maxillary irreversible hydrocolloid impression. |
 |
Figure 9 Mandibular irreversible hydrocolloid impression. |
Jaw Relation and Facebow Record
Self-cured acrylic temporary base was fabricated with a wax occlusal rim for its minimal distortion (Figure 10). Stainless steel clasps were incorporated into the mandibular base for retention (Figure 11). The fit and retention of the base was verified clinically. Standard clinical procedures for adjusting the wax occlusal rims, establishing and recording the jaw relations and facebow records were followed.5 The shade and mould of the denture teeth to be used were also selected.
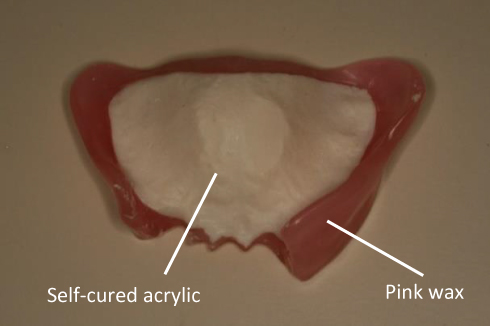 |
Figure 10 Maxillary occlusal rim. |
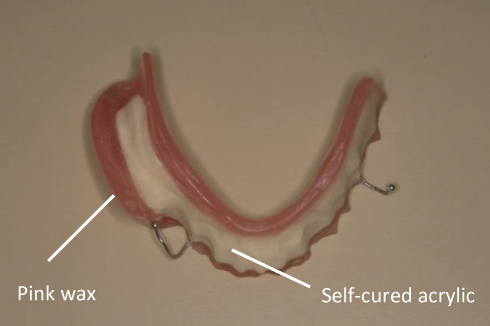 |
Figure 11 Mandibular occlusal rim. |
Wax Try-in
The waxed-up denture was tried in the mouth. The vertical and horizontal jaw relations, and appearance were verified and approved by the patient. (Figure 12).
 |
Figure 12 The wax-up denture try-in. |
Trimming of the Model
The maxillary teeth on the model were removed, and the surrounding area was trimmed (Figure 13). The artificial teeth replacing the teeth to be extracted were set, and the labial flange was added. The denture was then processed. The aim of the trimming was to produce a good approximation of the fitting surface of the denture base to the shape of the ridge immediately after extraction. The situation involving the presence of undercut to prevent the extension of the labial flange to the functional sulcus reflection point will be further discussed. The dentist, not the technician, should trim the cast in this situation because the experience of cast trimming can assist the dentist in performing surgery.
 |
Figure 13 The trimmed maxillary cast. |
Surgery and Denture Delivery
Local anaesthesia was administrated to the remaining maxillary teeth via buccal and palatal infiltration. The replacement of the splinted metal-ceramic crowns with the splinted temporary resin crowns (cemented with temporary cement) allowed for the easy removal of the crowns. The teeth were then extracted. Finger pressure was applied to the labial and palatal plates to help haemostasis. After it was confirmed that the denture could be fitted, sutures were placed in the interdental areas so that they laid over interdental bone instead of the sockets. In this situation, the sutures should not be under tension (Figure 14). Pressure-indicating paste was then applied to the fitting surface and border to identify the area with excessive pressure (Figure 15), and the denture was adjusted accordingly. The extension of the denture border was also checked. After the necessary adjustments had been made, the denture was delivered to the patient (Figure 16).
 |
Figure 14 Sutures to assist haemostasis. |
 |
Figure 15 Area with excessive pressure disclosed with pressure indicating paste. |
 |
Figure 16 Maxillary immediate denture in situ. |
Post Insertion Care
Following the delivery of the immediate complete denture, detailed post-operative instructions were given to the patient. In addition to receiving instructions regarding post-extraction management, the patient was asked to return for a review appointment the following day. Prior to that, the denture should not be removed. At the 24-hour appointment, the patient was asked whether he had any complaint regarding the extraction sites and the denture. Sign of soft tissue trauma stemming from the denture was checked. Special attention was paid to the region corresponding to the trimmed area of the working model because remodelling of the alveolar ridge was unpredictable after teeth extractions. The region would be under excessive pressure if it had been over-trimmed. The denture had to be adjusted accordingly. Instructions regarding the insertion and removal of the denture, as well as instructions regarding denture hygiene was given. The patient was reviewed one week post-extraction to have the sutures removed. Thereafter, the patient was reviewed weekly for a few more times until no new problem was detected. The patient was reminded to visit the dentist promptly if any problem arose.
Treatment for the Mandibular Arch
Further treatment items include the extractions of the mandibular incisors, the root canal treatment of the right mandibular first molar, and the crowning of the right mandibular first molar and the left mandibular first premolar, as well as the provision of a mandibular partial denture (Figure 17). These procedures were completed uneventfully. The patient was satisfied with the treatment and had no problem with the maxillary complete denture and the mandibular partial denture (Figure 18).
 |
Figure 17 Mandibular denture in situ (flipped mirror image). |
 |
Figure 18 Post treatment frontal view. |
Long-Term Follow-Up
During the 10-year follow-up period, the fit and occlusion of both the maxillary complete conventional immediate denture (Figure 19) and the mandibular removable partial denture (Figure 20) as well as the oral hygiene were maintained as needed. His oral hygiene was satisfactory, and no caries was found (Figure 21). This ensured patient's satisfaction in terms of aesthetics, function and comfort (Figure 22).
 |
Figure 19 Maxillary denture 10 years after delivery (flipped mirror image). |
 |
Figure 20 Mandibular denture 10 years after delivery (flipped mirror image). |
 |
Figure 21 Orthopantogram 10 years after treatment. |
 |
Figure 22 The frontal view 10 years after the delivery of the dentures. |
Discussion
Although implant treatment can often achieve good results, there are still situations in which implant are contraindicated.6 In these situations, we need to adopt other treatment options. In addition to the avoidance of a period of complete edentulism without replacement, immediate complete dentures possess other advantages compared with the conventional complete dentures constructed a few months after clearance. The denture base can help with protecting the extraction sockets. Chloe and Marie-Violaine reported an impression technique to avoid discomfort of taking the impression, which can be otherwise difficult and painful, even resulting in extracting the mobile teeth.7 They suggested to coat the mobile teeth and fill the undercuts with light-bodied silicone before taking the complete-arch impression with irreversible hydrocolloid. In addition, immediate complete dentures can copy the shade, shape, position of the natural teeth and the occlusal vertical dimension. Bedrossian et al reported a clinical protocol to develop the occlusal vertical dimension and anterior-posterior tooth set-up of a maxillary immediate complete denture.8 The protocol allows the dentist to adjust the occlusal vertical dimension and deliver a satisfactory complete denture immediately after extraction of teeth.
The disadvantages of immediate dentures include the fact that at least two stages of extraction are needed: one to extract the posterior teeth and the other to extract the anterior teeth. For some patients, such as those with bleeding disorders, it may be preferable to have all the teeth extracted during the same visit under strict medical supervision. These patients may be less suitable for immediate denture treatment. The need for frequent dental office attendance, which results in increased treatment time and cost, may also be a problem. Also, immediate dentures are contra-indicated if an existing infection of the anterior teeth requires urgent treatment. Prosthodontic treatment of this complexity can be challenging. Dentists should understand well the details of the clinical procedures required for denture construction. Good communication with the patient is also essential.
As rapid resorption usually occurs in the first few months after extractions, close mucosal contact in the anterior region may be lost following a short period of time. This may affect retention, support, and stability. When the patient bites with the anterior teeth, the anterior part of the denture may rotate anteroposteriorly. If this occurs, localized relining of the anterior region of the denture should be performed. Michael and Barsoum9 conducted a study to investigate the time required for the residual ridge to become stable following extraction for immediate dentures. They revealed that if the teeth are extracted without subsequent alveoplasty or intraseptal alveoplasty, the rate of bone resorption becomes negligibly low after six months. From this, they concluded that any time after six months would be suitable for relining. However, this does not appear to be a rational recommendation: the denture should be relined once sufficient resorption has taken place to jeopardize its fit, retention, support, or stability. Perhaps it may be interpreted that relining procedures that are performed six months or longer after extractions would likely remain adequate for considerable periods of time.
Although it is relatively uncommon, no denture reline or rebase was necessary in this case after ten years of service because the denture fitted well with patient comfort. Regular review showed the retention, support and stability of the denture remained satisfactory. For this patient, the well-formed ridge in the tuberosity region of both sides helped to develop good retention of the denture in these regions (Figure 23). Secondly, the left maxillary lateral incisor and canine were extracted three months prior to the fabrication of the maxillary denture. Rapid bone resorption would therefore not occur in this region after denture delivery. As a result, the residual ridge in this area could continue to offer good support. The good retention offered by the well-formed ridge in the tuberosity region, and the support offered by the residual ridge in the region corresponding to the extracted left maxillary lateral incisor and canine would help to prevent the denture from rotating anteroposteriorly and therefore eliminated the need for denture reline. This once again illustrates the fact that it is not compulsory to recommend denture reline after six months. Instead, each patient should be monitored according to his/her clinical situation.
 |
Figure 23 Upper occlusal view 10 years after treatment (flipped mirror image). |
St George et al10 suggested the preservation of as much bone as possible even if this results in undercut areas. These authors suggested the construction of a gum-fitted denture and the gradual extension of the labial flange with autopolymerizing or light-cured acrylic resin as bony resorption occurs. Jogezai et al11 also advocated the preservation of an undercut and recommended St George et al’s method of handling an undercut. Jogezai et al12 suggested a partial flange design in which the labial flange border extends about 1 mm beyond the maximum bulbosity of the ridge when an undercut of the alveolar ridge is present, but aesthetics dictate a flange. Jogezai et al12 did not appear to take into consideration the problem of the lack of a border seal. Also, depending on the gradient of the undercut area, as well as the quality of the mucosa, extending the labial flange 1 mm apical to the survey line to provide retention may result in traumatizing the mucosa.
In cases in which undercuts prevent the extension of labial flanges to full sulcular depth, the undercuts can either be left or removed. The removal of an undercut can be achieved either by an alveoloplasty or by an intraseptal alveoloplasty.13 A clinical study compared the effects of postoperative bone resorption after simple extractions, extractions followed by the alveoloplasty of the labial plate, and extractions followed by an intraseptal alveoloplasty.9 It was found that simple extractions resulted in the least amount of long-term bone resorption. Also, it was found that the intraseptal alveoloplasty resulted in less bone resorption compared with the alveoloplasty of the labial plate. The advantage of not performing any alveoloplasty is that it results in the least long-term bone loss. Long-term bone loss is a concern because the patient may consider implant treatment at a later time. Excessive bone loss will make the placement of an implant impossible without any grafting procedure. Also, excessive bone loss with fibrous replacement of the ridge may result in a flabby ridge that provides poor support for any removable dentures.
Without a reliable scientific way of predicting exactly how much the surgical approach will accelerate bone loss, a hard and fast guideline cannot be formulated. The point is that the advocation of preserving as much bone as possible, including the undercut, may not be the most sensible approach. The benefits of preserving undercut areas have to be weighed against the problem that this causes: the failure to achieve an adequate border seal. It is not logical to ask the patient to tolerate an unretentive denture to prevent excessive bone loss when the major objective of bone preservation in denture patients is to enable a retentive denture to be constructed.
A more sensible approach needs to be sought. Another finding of the study by Michael and Barsoum9 is that if teeth are extracted without a subsequent alveoloplasty or intraseptal alveoloplasty, the rate of bone resorption becomes negligibly low after six months. It appears wise to wait for a period of around six months to see if natural bone resorption results in the disappearing of the undercut. If the undercut persists, for those patients who would not consider implants, it appears to be justified to perform an alveoloplasty to remove the undercut. Within these six months, the extension of the labial flange to the full sulcular depth is made possible with a soft denture liner. The liner can either be added chairside14 or in the laboratory.15 In view of the problems associated with extending the border of the labial flange using a soft liner to the functional sulcus reflection point at chairside immediately after extractions, it is better to have the soft liner added in the laboratory before the denture is returned to the clinic for delivery.
After the undercut has been removed, either naturally or surgically, the soft liner should be replaced with a rigid denture base material. The soft liner approach is also applicable to those awaiting implant treatment. However, none of the soft liner materials is completely satisfactory for long-term application. The problems include color stability, long-term resiliency, abrasion resistance, bond strength and porosity.16 If the waiting time for implant treatment is prolonged, replacement with a new liner may be required. This protocol is a pragmatic and more rational approach to managing patients with undercuts than either constructing a gum-fitted denture10 or a denture of which the labial flange extends 1 mm apical to the survey line,12 then waiting indefinitely for the undercut to be resorbed naturally.
Conclusion
Immediate complete dentures can satisfy patients who require the extractions of all teeth in one arch because it prevents a patient from having a period of edentulism and social embarrassment. A good immediate complete denture offers good retention, support, stability, and aesthetics. However, it can be challenging because this type of denture treatment is time consuming. Dentists should understand well the details of the clinical procedures used for denture construction.
Consent for Publication
Written informed consent was obtained for the publication of the details of the patient, which also included the images. No institutional approval was required to publish the case details.
Ethics Approval Informed Consent
Written informed consent for joining the study was obtained prior to the commencement of the treatment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the current journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tyrovolas S, Koyanagi A, Panagiotakos DB, et al. Population prevalence of edentulism and its association with depression and self-rated health. Sci Rep. 2016;6(1):37083. doi:10.1038/srep37083
2. Viola AP, Takamiya AS, Monteiro DR, Barbosa DB. Oral health-related quality of life and satisfaction before and after treatment with complete dentures in a Dental School in Brazil. J Prosthodont Res. 2013;57(1):36–41. doi:10.1016/j.jpor.2012.08.003
3. Thalji G, McGraw K, Cooper LF. Maxillary complete denture outcomes: a systematic review of patient-based outcomes. Int J Oral Maxillofac Implants. 2016;31(Suppl):s169–s181. doi:10.11607/jomi.16suppl.g5.1
4. Chu CH, Chow TW. Esthetic designs of removable partial dentures. Gen Dent. 2003;51(4):322–324.
5. Clark R. An Introduction to Clinical Prosthodontics. Hong Kong: Hong Kong University Press; 1988:
6. Yeung C, Yu OY, Lam WH, Leung KC, Wong AWY, Chu CH. Improving esthetics of removable partial dentures using palatal retentive arms. Clin Cosmet Investig Dent. 2020;12:391–397. doi:10.2147/ccide.s266145
7. Chloë M, Marie-Violaine B. Impression for an immediate denture with mobile teeth: a clinical approach. J Prosthet Dent. 2019;122(5):498–499. doi:10.1016/j.prosdent.2019.06.015
8. Bedrossian EA, Putra A, Chung K-H. A technique to correct anterior-posterior tooth discrepancy for a maxillary immediate complete denture. J Prosthodont. 2019;28(6):719–723. doi:10.1111/jopr.12713
9. Michael CG, Barsoum WM. Comparing ridge resorption with various surgical techniques in immediate dentures. J Prosthet Dent. 1976;35(2):142–155. doi:10.1016/0022-3913(76)90273-0
10. St George G, Hussain S, Welfare R. Immediate dentures: 1 treatment planing. Dent Update. 2010;37(2):
11. Jogezai U, Laverty D, Walmsley AD. Immediate denture part 2: denture construction. Dent Update. 2018;45(8):720–726. doi:10.12968/denu.2018.45.8.720
12. Jogezai U, Laverty D, Walmsley AD. Immediate dentures part 1: assessment and treatment planning. Dent Update. 2018;45(7):617–624. doi:10.12968/denu.2018.45.7.617
13. Tucker MR, Bauer RE. Preprosthetic surgery. In: Hupp JR, Tucker MR, Ellis E, editors. Contemporary Oral and Maxillofacial Surgery.
14. Ramasamy C, Abraham A. Prosthodontic management of undercut tuberosities: a clinical report. J Clin Diagn Res. 2011;5(8):1692–1694.
15. Lowe LG. Flexible denture flanges for patients exhibiting undercut tuberosities and reduced width of the buccal vestibule: a clinical report. J Prosthet Dent. 2004;92(2):128–131. doi:10.1016/j.prosdent.2004.04.026
16. Hashem MI. Advances in soft denture liners: an update. J Contemp Dent Pract. 2015;16(4):314–318. doi:10.5005/jp-journals-10024-1682
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.