")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Proportion of Depression and Its Associated Factors Among Youth HIV/AIDS Clients Attending ART Clinic in Dessie Town Government Health Facilities, Northeast Ethiopia
Authors Getaye A, Cherie N , Bazie GW , Gebremeskel Aragie T
Received 10 December 2020
Accepted for publication 13 January 2021
Published 29 January 2021 Volume 2021:14 Pages 197—205
DOI https://doi.org/10.2147/JMDH.S296849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Amare Getaye,1 Niguss Cherie,1 Getaw Walle Bazie,1 Teshome Gebremeskel Aragie2
1Wollo University, College of Medicine and Health Sciences, School of Public Health, Dessie, Ethiopia; 2Woldia University, College of Health Sciences, Department of Anatomy, Woldia, Ethiopia
Correspondence: Amare Getaye
Wollo University, College of Medicine and Health Sciences, School of Public Health, Dessie, Ethiopia
Email [email protected]
Background: Depression is the most prevalent among people living with HIV/AIDS than people without HIV/AIDS. Depression is associated with an increase in morbidity and mortality in people living with HIV/AIDS and adversely affects the adherence to antiretroviral therapy, quality of life, and health-related parameters.
Objective: The aim of this study was to assess the proportion of depression and its associated factors among youth HIV/AIDS patients attending ART clinics in Dessie town Government health facilities, Northeast Ethiopia.
Methods: Institutional-based cross-sectional study design was employed on 431 youth HIV/AIDS patients attending ART clinics at Dessie town Public health facilities. Data were collected by face-to-face interview using a structured questionnaire. EPI-Data software version 3.1 was used to enter the data and analysis was done using SPSS version 23. Binary logistic regression was used to identify factors associated with depression. Statistical significance was declared at a p-value of less than 0.05 in the final model.
Results: The proportion of depression among youth HIV/AIDS patients was 26.2%. The age range between 20 and 24 years (AOR = 2.019, 95% CI: 1.143– 3.566), poor medication adherence (AOR = 9.007, 95% CI: 3.061– 26.500), stigma (AOR = 4.14, 95% CI: 2.08– 8.26), and low social support (AOR = 1.854, 95% CI: 1.034– 3.324) were associated with depression.
Conclusion: The proportion of depression among youth HIV patients in the current study was found to be lower compared to previous studies. Age, HIV-related stigma, social support, lost job, and poor medication adherence were found to be independent predictors of depression. Therefore, scaling up the pediatric psychosocial support program to youth psychosocial support for all ART site health facilities, strengthening health education about the medication adherence and complication of HIV/AIDS are needed.
Keywords: depression, Ethiopia, HIV/AIDS, youth
Introduction
Globally, depression has become a substantial public health problem both at the social and economic levels as well as at the clinical level. More than 264 million people of all ages suffer from depression. It is the leading cause of disability worldwide and is a major contributor to the overall global burden of disease.1–3 Depression is associated with an increase in morbidity and mortality in people living with HIV/AIDS and adversely affects the adherence to antiretroviral therapy, quality of life including health-related parameters.4,5
Globally, it is estimated that 38 million people are living with HIV/AIDS; of whom, 36.2 million are aged greater than 15 years. About 1.7 million people became newly infected with HIV and 690,000 people died from AIDS-related illnesses worldwide in 2019.6 In sub-Saharan Africa, four in five new infections among age 15–19 years in girls, and women age 15–24 years are twice likely to be living with HIV than men. In Ethiopia, it is estimated that 690,000 people were living with HIV; among those 23,000 are people became newly infected with HIV in 2018. In the same year, 11,000 people died due to HIV/AIDS.6 Depression is the most prevalent among people living with HIV/AIDS than people without HIV/AIDS. The burden of depression and HIV/AIDS would result in poor health outcomes due to obstacles to treatment and deterioration of medical outcomes, including treatment resistance, high viral load, and increase morbidity and mortality of people living with HIV.7,8
People living with HIV/AIDS are at risk for co-morbid diseases including depression and neuropsychiatric comorbidities are highly dominant among HIV-positive youth.9 Ethiopia adopted strategies designed to eliminate HIV/AIDS epidemics by 2030. Therefore, to achieve these goals, health systems need to adopt innovations to tackle barriers that have hitherto been under-recognized or unaddressed.10
HIV-infected patients become vulnerable to a set of disease-specific conditions or factors such as medical, psychological, and social factors, as well as the general threat of death; which often leads to depression.4 In this group of the population, even accessing to care and antiretroviral medications, depressive symptoms were associated with poor medication adherence,11,12 risky behaviors including substance use and high-risk sexual practices,12,13 poor virological response to treatment,14 and increased risk of mortality.15
Adequate assessment and treatment of depression are critical to improving the overall health outcomes in PLWHIV. Routine screening for depression and the integration of mental health interventions into HIV/AIDS programs and produced training materials for its assessment and management in these populations have been recommended for nearly a decade. However, whether assessed by screening or self-report, depression was undertreated, with approximately one-third or less receiving treatment.12,16
Treating depression can help to manage HIV/AIDS and improve overall health outcomes.17 However, majority of healthcare professionals are often not skilled in detecting psychological symptoms. In addition, those skilled healthcare professionals do not also take the necessary action for further assessment, management, and referral.16 Little was known about the proportion of depression and its associated factors among youth HIV/AIDS patients in Ethiopia, particularly in the study area. Therefore, this study would serve as a foundation for future public health and mental health research and intervention in this area.
Methods
Study Area and Period
The study was conducted in Dessie town government health facilities. Dessie town is located 401 km away from Addis Ababa the capital city of Ethiopia. Administratively the town is divided into five sub-cities that consist of 18 Kebeles. The estimated population size of the town was 218,471; of whom, 102,378 (46.86%) were men and 116,093 (53.14%) were women. Dessie town has eight Health centers, two governmental hospitals, and five general private hospitals. Currently, three health centers, two governmental hospitals, and two private hospitals provide ART services. Among these health facilities, a total of 10,510 HIV patients and 896 youths were on ART. The study was conducted from February 2 to March 20, 2020.
Study Design
Facility-based cross-sectional study was conducted to assess the proportion of depression and its associated factors among youth on RVI.
Source Population
All RVI youth clients who attend ART care service in Dessie town governmental health facilities of ART clinics.
Study Population
HIV infected youth on ARV drug and who were on follow-up in Dessie town Government health facilities during the study period.
Inclusion Criteria
All youth HIV/AIDS clients who attend ART chronic care service in Dessie town Government health facilities.
Exclusion Criteria
Youth HIV/AIDS clients who were seriously ill and unable to communicate were excluded from the study.
Sample Size Determination
The sample size was determined by using a single population proportion formula considering the following assumptions: confidence level at 95% with its standard normal curve value of 1.96 (Zα/2 = ±1.96), a margin of error (d = 0.05), the proportion of depression among youth HIV/AIDS clients attending ART clinic in Addis Ababa, Ethiopia, 35.5% and 10% for non-response rate.9 The final sample size became 440.
Sampling Procedures
The calculated sample size was proportionately allocated based on the average number of client flow per month to each health facility providing ART service. The sampling method employed to select study participants for this study was a systematic random sampling technique. After listing them by their medical record, the sampling frame was used containing the list of youth on ART in Dessie town government health facilities. A systematic random sampling technique was used to select the participants by calculating the Kth value. Then, every two clients were interviewed and the first client was selected by the lottery method (Figure 1).
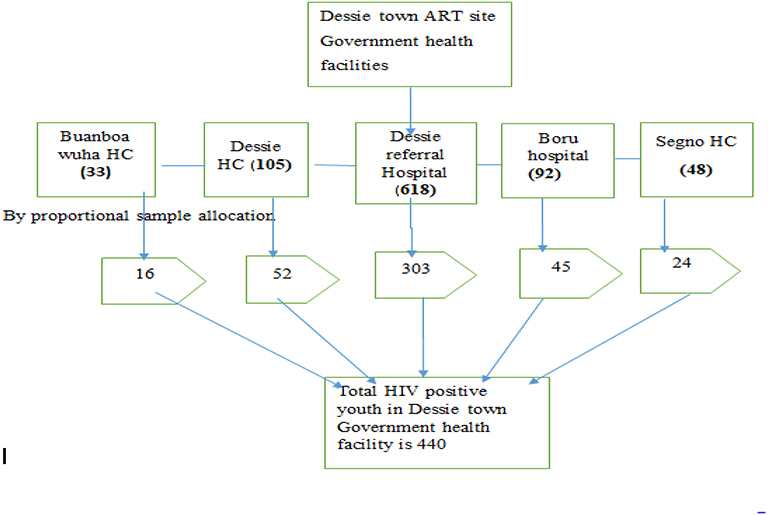 |
Figure 1 Sampling procedures for youth RVI clients attending the ART clinic at Dessie town governmental health facilities, Northeast Ethiopia, 2020. |
Data Collection Tools and Procedures
Data were collected by pre-tested and structured questionnaire through face-to-face interview. The questionnaire was prepared in its English version by reviewing relevant literature and it was translated to local language followed by back translation to English to check its consistency. The Beck Depression Inventory (BDI-II) scale was used to measure depression. The questionnaire includes seven group of questions. These questions were categorized as sadness, pessimism, past failure, loss of pleasure, guilty feelings, punishment feelings, and self-dislike. Each question has a four-point scale ranging from 0 (symptom not present) to 3 (symptom very intense). The maximum point scored will be 21 if they answer all the questions 3 and the minimum point scored will be 0 if they answer all the questions 0. A cut-off point of 14 and more was used to identify people with depression. In the current study, the internal consistency of the depression questions was checked by the Cronbach’s alpha value and it was found to be 0.85.9
The internalized stigma scale and social support questionnaire were developed by reviewing similar studies. The internalized stigma scale consisted of 10 items rated on a 5-point response format ranging from “strongly disagree” (1) to “strongly agree” (5) based on the extent to which a respondent felt about him/herself since being diagnosed with HIV. A total score (possible range = 10–50) was obtained by summing responses to all items.18
Social support is assessed by (SSQ-6). It included six (6) items scale that assessed the number of available social support. The number of persons available to provide the type of support described in each item was coded as either “no one” (0) or “one or more” (1). The total score is obtained by summing all 6 items with a possible range of 0 to 5.18
Data Quality Control
The questionnaire was pretested on 22 participants of the total sample size in Kombolcha health center and based on feedback obtained from the pretest, the necessary modification was done accordingly. The training was given to four data collector nurses and one public health officer supervisor for two days. The training was targeted on the objective of study, the content of questionnaire through question by question, data collection procedure, how to help study participants, and different ethical issues. The data collection process was supervised by the supervisor. During the data collection period, the collected data were checked continuously on a daily basis for completeness by the principal investigator and supervisor in the respective health facilities. The filled questionnaire was given its own code.
Data Processing and Analysis
The data were entered using the EPI Data version 3.1 statistical package and exported to SPSS version 23 for analysis. Data cleaning was performed by running frequencies of each variable to check for outliers and missed values. Descriptive statistics such as frequency, proportion, and summary measures (mean, standard deviation, median, and inter-quartile) were calculated. A binary logistic regression model was applied to identify the association between independent variables and dependent variables. The bi-variable analysis was done for each explanatory variable and variables having a p-value less than 0.2 were passed for the final multivariable logistic regression analysis. The significance of association was assessed using p-value and a 95% confidence interval. If the p-value is less than 0.05, the variable is considered as statistically significant in the final model. In addition, the odds ratio with its 95% confidence interval was used to measure the strength of the study.
Ethical Considerations
The study was conducted following the Declaration of Helsinki. Verbal informed consent was obtained from participants after they were informed about objectives and procedures of the study and verbal informed assent was taken from minors (participants under the age of 18 years) and permission was obtained from their parents and/or guardians. Verbal informed consent was approved by the Institutional Review board of the College of Medicine and Health Sciences, Wollo University. Permission letter to conduct the study was obtained from South Wollo Zone Health Office. Their rights to refuse participation any time they want were assured. For this purpose, a one-page consent letter was attached as a cover page of each questionnaire stating the general objective of the study and issues of confidentiality that was discussed by the data collectors before proceeding to the data collection. After getting informed consent from the selected participants, the data collection was taken place in a silent place separately from others to avoid an influence on each other.
Results
Socio-Demographic Characteristics of Study Participants
In this study, the data were collected from 431 respondents through face-to-face interviews with a response rate of 97.9%. Among those, 222 (51.5%) were in the age group of 20–24 and the mean age of the participants’ was 19.6 years with a range from 15 to 24. Of the study participants, 257 (59.6%) were females, from the study participants, 363 (84.2%) were Amhara in ethnicity, 248 (57.5) were Muslim in religion, 388 (90%) were single, 185 (42.9%) were primary education. The monthly income of family respondents involved in the study was 1000–1999, 140 (32.5%) clients (Table 1).
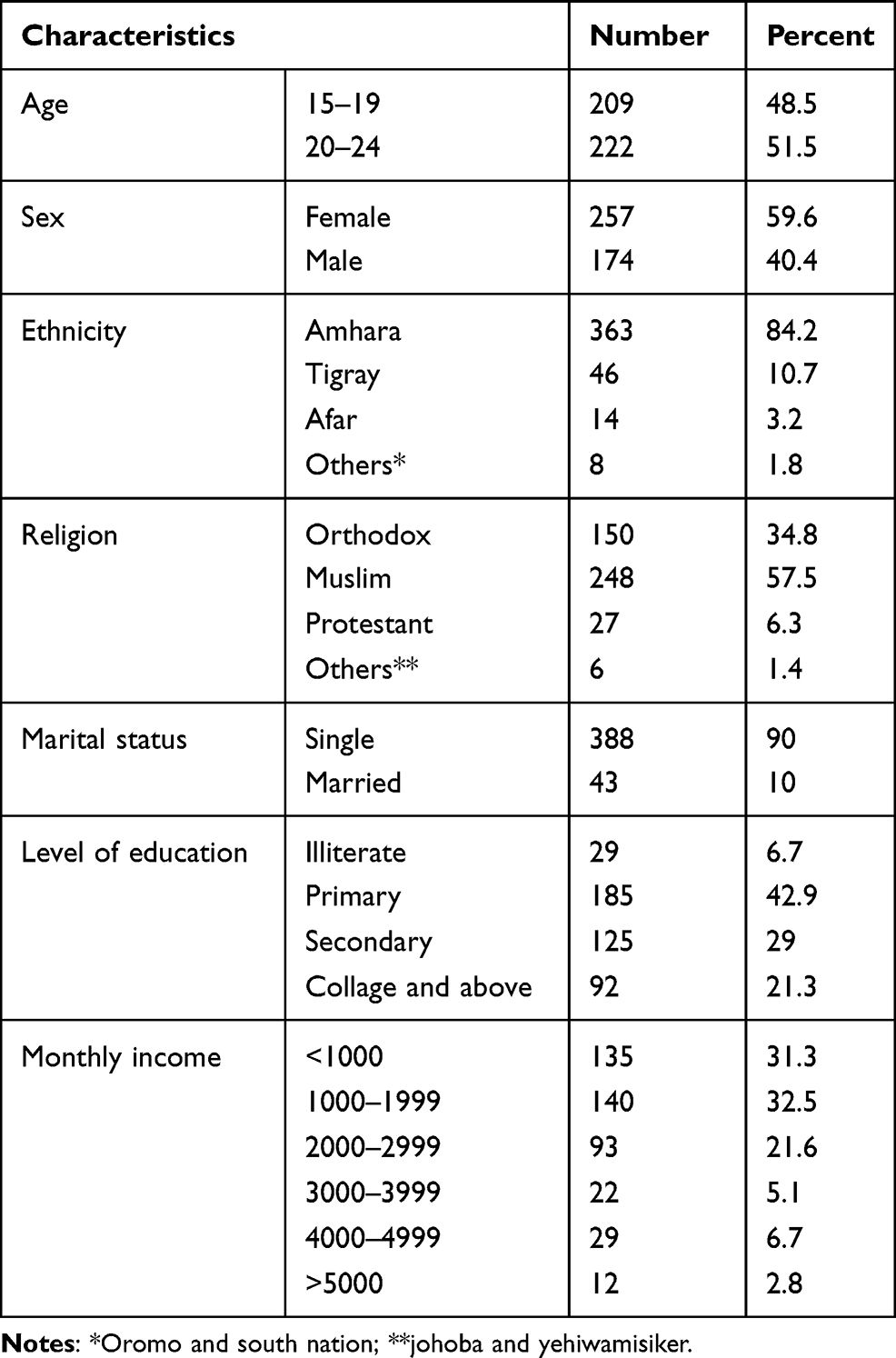 |
Table 1 Socio-Demographic Characteristics of Youth RVI Patients Attending Dessie Town Government Health Facilities, Northeast, Ethiopia, 2020 (n=431) |
Psychosocial Characteristics
Among the study participants, 361 (83.8%) were living with their family members. Of 276 (64%) respondents were internally stigmatized and two-third 287 (66.6%) had low social support from their families or other supportive bodies. Concerning their job status, 272 (63.1%) did not lose their jobs due to HIV/AIDS-related illness (Table 2).
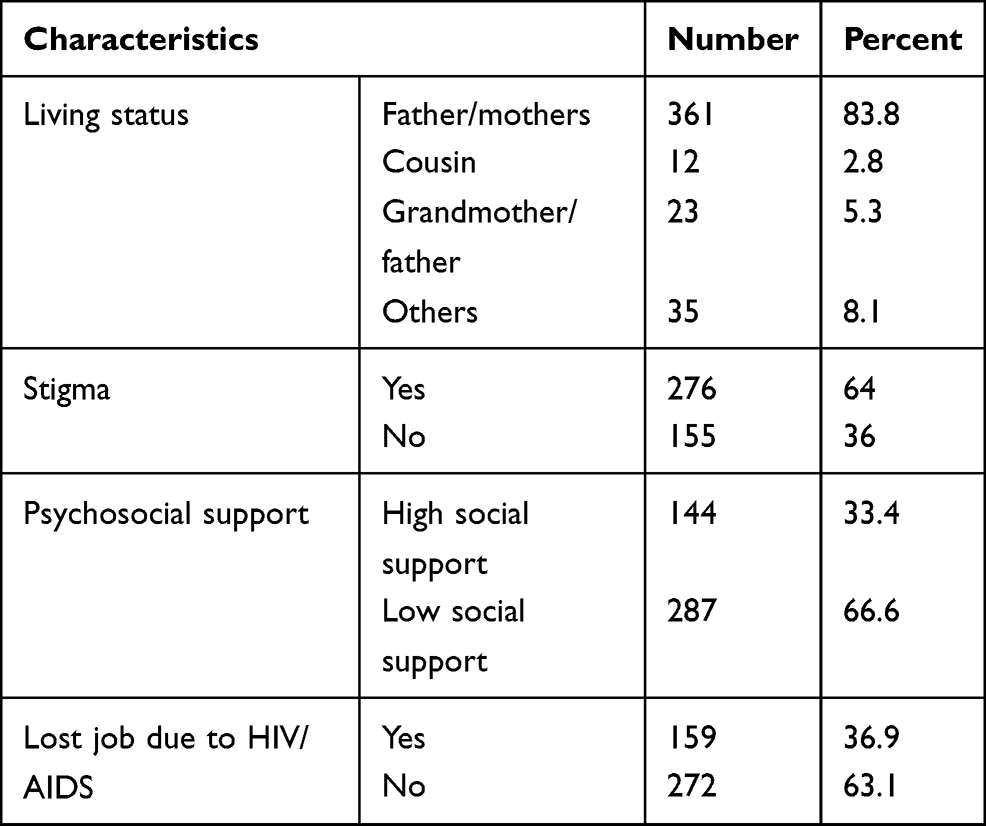 |
Table 2 Psychosocial Characteristics of Youth RVI Patients Attending Dessie Town Government Health Facilities, Northeast Ethiopia, 2020 (n=431) |
Clinical-Related Characteristics
About 236 (54.8%) study participants were under WHO clinical stage I, 217 (50.3%) had CD4 counts greater than 350, 375 (87%) were under first-line ART drug regimen and 347 (80.5%) took their medication for more than 6 months. Almost three-fourths of study participants 316 (73.3%) had good drug adherence and 247(57.5%) had an opportunistic infections (Table 3).
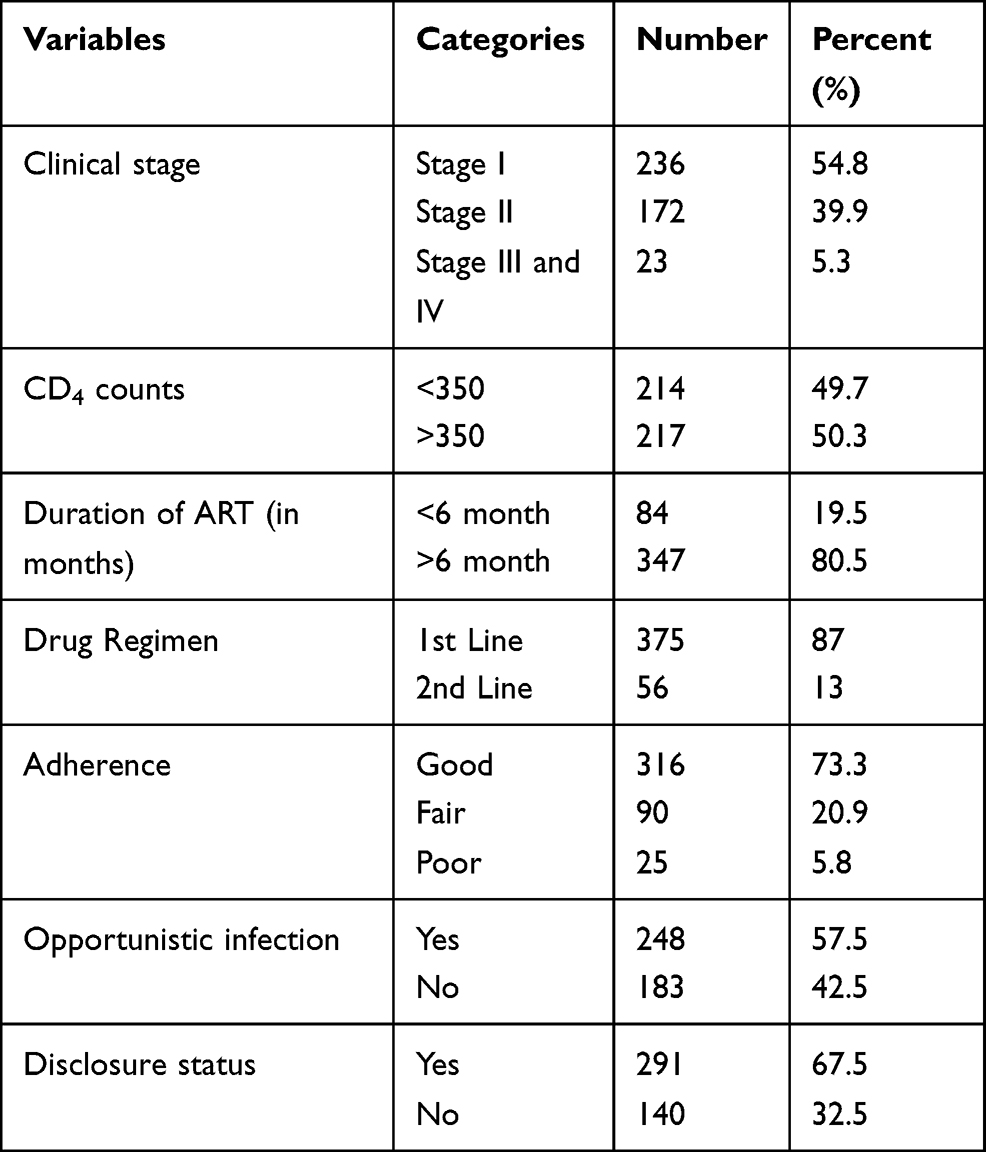 |
Table 3 Clinical-Related Characteristics of Youth RVI Patients Attending Dessie Town Government Health Facilities, Northeast Ethiopia, 2020 (n=431) |
Factor Associated with Depression Among Youth HIV/AIDS Patients
In the bi-variable analysis, age, marital status, lost jobs, internalized stigma, living condition, social support, CD4 count, duration of HAART, adherence, OI, disclosure status, alcohol drinking, and chat chewing were associated with depression among youth RVI patients. In the final multivariable logistic regression analysis, age, medication adherence, internalized stigma, lost jobs, and social support were statistically significantly associated with the proportion of depression among youth RVI patients.
Study participants aged from 20 to 24 were 2.019 times more likely to develop depression than participants aged 15 to 19 [AOR=2.019; 95% CI (1.143–3.566)]. Patients who had poor adherence were 9.007 times more likely to develop depression than patients who had good adherence [AOR= 9.007; 95% CI (3.061–26.500)]. The odds of depression were 4.14 times higher among patients who were internally stigmatized compared to patients who were not internally stigmatized [AOR=4.14; 95% CI (2.08–8.26)]. Patients who had low social support were 1.85 times more likely to develop depression than patients who had high social support [AOR=1.85; 95% CI (1.03–3.32)] and patients who had lost the job due to HIV/AIDS were 2.088 times more likely to develop depression than patients who had not lost the job [AOR=2.08; 95% CI (1.23–3.54)] (Table 4).
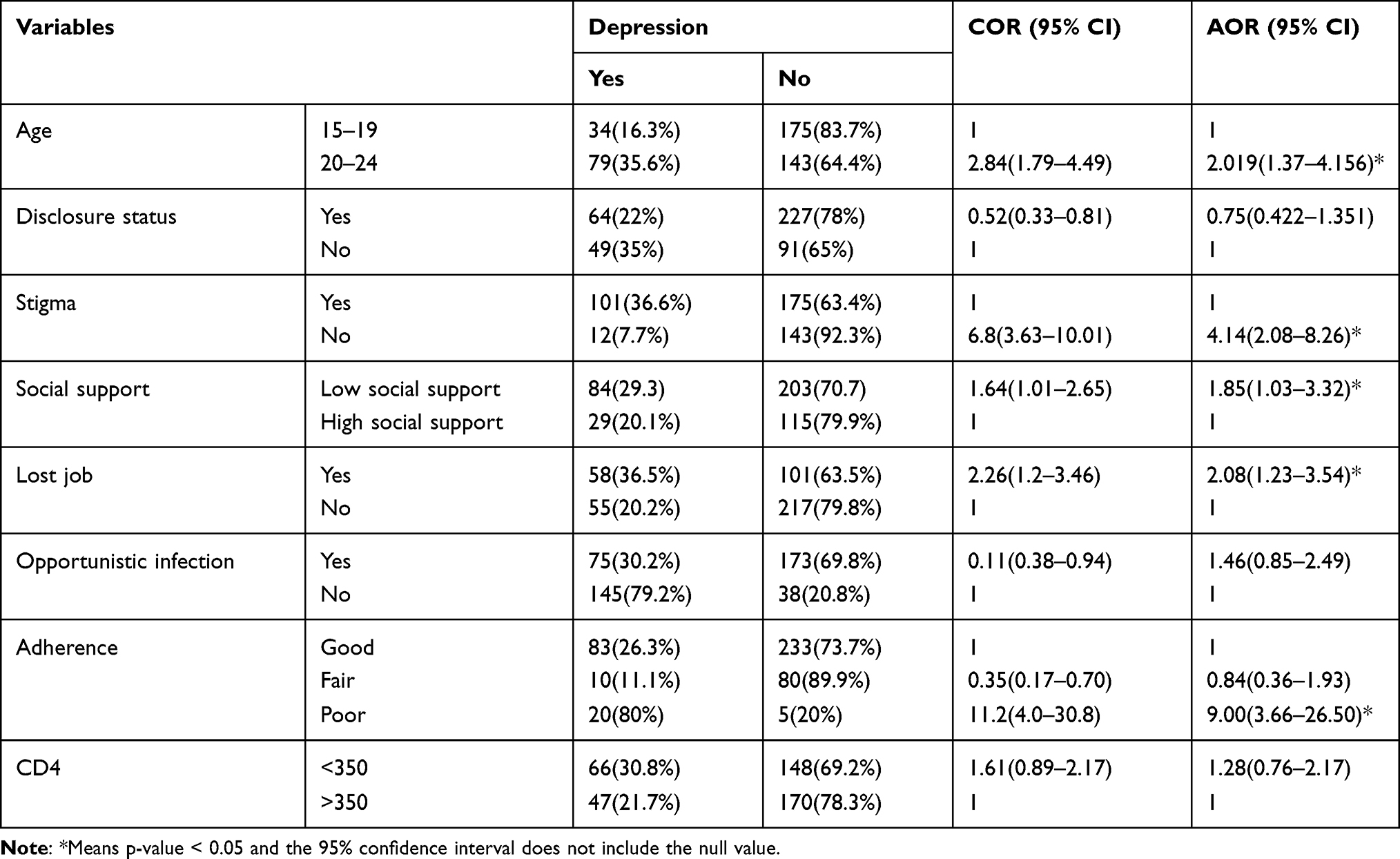 |
Table 4 Bi-Variable and Multi-Variable Logistic Regression Analysis of Factors Associated with Depression Among Youth RVI Patients Attending Dessie Town Government Health Facility, Northeast, Ethiopia, 2020 |
Discussion
This study was designed to identify the proportion of depression and factors associated with youth RVI status among Dessie town governmental health facilities. The proportion of depression among youth RVI patients was found to be 26.2%. Based on the Beck depression inventory (BDI-II) scale; this finding was lower than the reported rates in Zimbabwe 63%,19 USA 52%,20 Kenya 48%,21 and Addis Ababa 35.5%.9 The possible reason for this variation might be occurred due to differences in the study period, the new initiative, cultural factors, test, and treatment start. It might also be related to substance use and age, which increases the risk of HIV infection and interfere with their treatment, and conversely, some mental disorders occur as a direct result of HIV infection. But this study result is higher than the study conducted in Malawi 18.9%,22 and Malaysia 18.5%.23 The possible reason for this discrepancy might be due to the study design, and socioeconomic characteristics. It might also be due to poor medication adherence and the presence of stigma in our study.
Regarding the factors, age, medication adherence and internalized stigma, lost jobs and social support were statistically significantly associated with the proportion of depression among youth RVI patients. Study participants aged 20 to 24 were 2.019 times more likely to develop depression than participants aged 15 to 19. Similarly, a study done in Addis Ababa, Ethiopia reported as increased age of participants was positively associated with depression.24 The possible explanation might be due to the youth’s stage of realization of economic and psychosocial self-reliance roles.
Patients who had poor adherence were 9.007 times more likely to develop depression than patients who had good adherence. In the same way, a study conducted in Ethiopia showed that the odds of depression among youth HIV patients were higher among respondents who had poor adherence to medication. The possible explanation might be due to poor medication adherence has been implicated the increment of disease progression, probability of occurrence of opportunistic infections and stigma which results in a decrease in viral load suppression. The finding is in line with the studies in Addis Ababa,9 Zimbabwe19, Kano, and North Western Nigeria.25
The odds of depression were 4.14 times higher among patients who were internally stigmatized compared to patients who were not internally stigmatized. This study is in agreement with a study conducted in Addis Ababa, Ethiopia that HIV-related stigma increases the individual’s vulnerability to develop depression.9 This finding was also consistent with studies done in different developed and developing countries.26,27 The possible reason might be related to the fact that youth people with HIV status develop an increased sense of isolation, poor self-worth, and rekindle hopelessness that might lead to psychological distress.
Patients who had low social support were 1.85 times more likely to develop depression than patients who had high social support. Youths with no close family to disclose their problem are unable to get the care and may have increased depressive symptoms.20 This might also be due to factors such as educational disability, food insecurity, isolation, and debilitation. Low social support could result in poor adherence to medication and as a result, poor adherence leads to immune suppression which finally leads to depression.15
Patients who had lost the job due to HIV/AIDS were 2.088 times more likely to develop depression than patients who had not lost a job. An institutional study conducted in Addis Ababa, Malawi, and Kenya showed that there was no association between lost job and depression.9,21,22 The possible explanation for this might be PLWHA who have low income can not easily fulfill their needs, have difficulty to get a balanced diet and to cover health expense. In addition to their disease status, financial hardship leading to psychological distress and frustration, so they might easily develop depression.
The cross-sectional nature of the study did not enable us to establish strong causal relationships between the independent variables and depression and many of the variables were self-reported and therefore, the respondents might be influenced by social desirability bias. Hence, we recommend other researchers to conduct the study using study designs that will establish strong causal relationships between the independent variables and depression such as cohort study.
Conclusions
The proportion of depression among youth HIV patients in the current study was found to be lower compared to previous studies. Age, HIV-related stigma, social support, poor medication adherence, and lost job were found to be independent predictors of depression. Therefore, scaling up the pediatric psychosocial support program to youth psychosocial support for all ART site health facilities, strengthening health education about the medication adherence and complication of HIV/AIDS, recruiting adherence supporter for all high load ART site health facilities and developing guidelines for psychosocial support for youth with HIV/AIDS are needed.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study was conducted following the Declaration of Helsinki. Verbal informed consent was obtained from participants after they were informed about objectives and procedures of the study and verbal informed assent was taken from minors (participants under the age of 18 years) and permission was obtained from their parents and/or guardians. Verbal informed consent was approved by the Institutional Review board of the College of Medicine and Health Sciences, Wollo University. Permission letter to conduct the study was obtained from South Wollo Zone Health Office. Their rights to refuse participation any time they want were assured. For this purpose, a one-page consent letter was attached as a cover page of each questionnaire stating the general objective of the study and issues of confidentiality that was discussed by the data collectors before proceeding to the data collection. After getting informed consent from the selected participants, the data collection was taken place in a silent place separately from others to avoid an influence on each other.
Acknowledgments
We thank data collectors and supervisors who heartfully participated during data collection and we are grateful to the participants for their voluntary participation in our study. Lastly, we would like to thank all health institutions for their cooperation from the beginning until the end of this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, took part in drafting the article and revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding
The research did not receive specific funding.
Disclosure
The authors declare that they have no conflicts of interest for this work or regarding the publication of this paper.
References
1. Beyene Gebrezgiabher B, Huluf Abraha T, Hailu E. et al. Depression among adult HIV/AIDS patients attending ART clinics at Aksum Town, Aksum, Ethiopia: a Cross-Sectional Study. Depress Res Treat. 2019:2019. doi:10.1155/2019/3250431
2. Benjamin JS; VAKSs. Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. Lippincott Williams & Wilkins; 2007:529.
3. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858.
4. Shittu R, Issa B, Olanrewaju G, et al. Prevalence and correlates of depressive disorders among people living with HIV/AIDS. North Central Nigeria J AIDS Clin Res. 2013;4(11):251.
5. Ntshakala TT, Mavundla TR, Dolamo BL. Quality of life of people living with HIV and AIDS who are on antiretroviral therapy in Swaziland. Afr J Nurs Midwifery. 2015;17(1):17–32.
6. UNAIDS. Global, HIV/AIDS Statistics–2019 Fact Sheet. Vol. 2019. 2020.
7. Kibret GD, Salilih SZ. Prevalence and associated factors of depression among HIV infected patients in Debre Markos town Northwest Ethiopia. Int J Emerg Ment Health Hum Resilience. 2015;17:714–716.
8. Tesfaw G, Ayano G, Awoke T, et al. Prevalence and correlates of depression and anxiety among patients with HIV on-follow up at Alert Hospital, Addis Ababa, Ethiopia. BMC Psychiatry. 2016;16(1):368. doi:10.1186/s12888-016-1037-9
9. Abebe H, Shumet S, Nassir Z, Agidew M, Abebaw D. Prevalence of depressive symptoms and associated factors among HIV-positive youth attending ART follow-up in Addis Ababa, Ethiopia. AIDS Res Treat. 2019;2019:2019. doi:10.1155/2019/4610458
10. Girum T, Wasie A, Worku A. Trend of HIV/AIDS for the last 26 years and predicting achievement of the 90-90-90 HIV prevention targets by 2020 in Ethiopia: a time series analysis. BMC Infect Dis. 2018;18(1):320. doi:10.1186/s12879-018-3214-6
11. Ammassari A, Antinori A, Aloisi MS, et al. Depressive symptoms, neurocognitive impairment, and adherence to highly active antiretroviral therapy among HIV-infected persons. Psychosomatics. 2004;45(5):394–402. doi:10.1176/appi.psy.45.5.394
12. Eller LS, Kirksey KM, Nicholas PK, et al. A randomized controlled trial of an HIV/AIDS symptom management manual for depressive symptoms. AIDS Care. 2013;25(4):391–399. doi:10.1080/09540121.2012.712662
13. Ryan K, Forehand R, Solomon S, Miller C. Depressive symptoms as a link between barriers to care and sexual risk behavior of HIV-infected individuals living in non-urban areas. AIDS Care. 2008;20(3):331–336. doi:10.1080/09540120701660338
14. Hartzell JD, Spooner K, Howard R, Wegner S, Wortmann G. Race and mental health diagnosis are risk factors for highly active antiretroviral therapy failure in a military cohort despite equal access to care. J Acquir Immune Defic Syndr. 2007;44(4):411–416. doi:10.1097/QAI.0b013e31802f83a6
15. Anastos K, Schneider MF, Gange SJ, et al. The association of race, sociodemographic, and behavioral characteristics with response to highly active antiretroviral therapy in women. J Acquir Immune Defic Syndr. 2005;39(5):537–544.
16. Health R, Services A; Control CfD, Prevention, America HMAotIDSo. Incorporating HIV prevention into the medical care of persons living with HIV. Recommendations of CDC, the health resources and services administration, the National Institutes of Health, and the HIV medicine association of the Infectious Diseases Society of America. MMWR Morb Mortal Wkly Rep. 2003;52(RR–12):1.
17. Teachman BA, McKay D, Barch DM, Prinstein MJ, Hollon SD, Chambless DL. How psychosocial research can help the National Institute of Mental Health achieve its grand challenge to reduce the burden of mental illnesses and psychological disorders. Am Psychol. 2019;74(4):415. doi:10.1037/amp0000361
18. Dorsisa B, Ahimed G, Anand S, Bekela T. Prevalence and factors associated with depression among HIV/AIDS-infected patients attending ART clinic at Jimma University Medical Center, Jimma, Southwest Ethiopia. Psychiatry J. 2020;2020:1–9. doi:10.1155/2020/5414072
19. Mavhu W, Berwick J, Chirawu P, et al. Enhancing psychosocial support for HIV positive adolescents in Harare, Zimbabwe. PLoS One. 2013;8(7):e70254. doi:10.1371/journal.pone.0070254
20. Mellins CA, Malee KM. Understanding the mental health of youth living with perinatal HIV infection: lessons learned and current challenges. J Int AIDS Soc. 2013;16(1):18593. doi:10.7448/IAS.16.1.18593
21. Kamau JW, Kuria W, Mathai M, Atwoli L, Kangethe R. Psychiatric morbidity among HIV-infected children and adolescents in a resource-poor Kenyan urban community. AIDS Care. 2012;24(7):836–842. doi:10.1080/09540121.2011.644234
22. Mukangabire P, Katende G, Rugema J, Moreland P, Nkurunziza A. Factors associated with depression among adolescents living with HIV at health facilities in Rwanda. 2019.
23. Ng S-Y, Chan H-K, Almehmadi A, et al. A clinical pharmacist-based screening for depression in children with transfusion-dependent thalassemia in Malaysia. Arch Pharm Pract. 2018;9:1.
24. Getalem A, Emnet A. Prevalence and associated factors of depression among HIV patients taking antiretroviral therapy at Zewditu Memorial Hospital, Addis Ababa, Ethopia. J Sci Res Stud. 2016;3(4):81–86.
25. Lawan UM, Abubakar S, Gambo MD. HIV risk behaviors and knowledge of HIV/AIDS and its prevention among unmarried adolescents in Kano Metropolis, Northwestern Nigeria. J Behav Health. 2012;1(4):252–259. doi:10.5455/jbh.20120720042617
26. Martinez J, Harper G, Carleton RA, et al. The impact of stigma on medication adherence among HIV-positive adolescent and young adult females and the moderating effects of coping and satisfaction with health care. AIDS Patient Care STDS. 2012;26(2):108–115. doi:10.1089/apc.2011.0178
27. Hill LM, Maman S, Groves AK, Moodley D. Social support among HIV-positive and HIV-negative adolescents in Umlazi, South Africa: changes in family and partner relationships during pregnancy and the postpartum period. BMC Pregnancy Childbirth. 2015;15(1):1–9. doi:10.1186/s12884-015-0542-z
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.