")
Back to Journals » Cancer Management and Research » Volume 11
Progress in immunocytochemical staining for cervical cancer screening
Received 4 December 2018
Accepted for publication 23 January 2019
Published 22 February 2019 Volume 2019:11 Pages 1817—1827
DOI https://doi.org/10.2147/CMAR.S195349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Hengzi Sun, Keng Shen, Dongyan Cao
Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Abstract: Cervical cancer is one of the most common gynecological malignancies. In recent years, the implementation of cervical cancer screening has resulted in the effective control of cervical cancer incidence. However, many deficiencies still exist in the current screening techniques and strategies. With advancements in cervical cancer screening research, immunochemical staining to determine cervical cytology has shown a broader application prospect in the early screening for cervical cancer, especially for triage in cervical cancer screening.
Keywords: HSIL, dual staining, p16, Ki-67, triage strategy, colposcopy referral
Introduction
Cervical cancer has a high mortality rate and is the second most common gynecologic cancer worldwide.1 In recent years, the onset age of cervical cancer has become increasingly younger. Over the past several decades, wide implementation of cervical cancer screening in the USA has contributed to an extraordinary reduction in the mortality rate and the prevalence of cervical cancer by over 50%.2 However, the incidence of cervical cancer in developing countries is approximately four to six times of that in developed countries.1 On the one hand, the increased incidence is associated with imperfect screening systems in developing countries. The medical resources are unevenly allocated, and the poorest regions rarely benefit from cervical cancer screening. On the other hand, the increased incidence is also related to the limited screening techniques and strategies used.3
With advancements in cervical cancer screening, more screening approaches have been applied in the clinic. At present, commonly used screening methods for cervical cancer include cervical cytology tests, human papillomavirus (HPV) detection, acetic acid (VIA) and/or the Lugol’s iodine (VILI) test, p16/Ki67 dual staining, and colposcopy examination. Regular cytological screening tests are dependent on sampling techniques and the opinion of diagnosticians, and some diagnostic test results are ambiguous. The specificity of cytological tests for high-grade lesions, ie, cervical intraepithelial neoplasia 2 and above (CIN 2+), is ~73.4%, but the sensitivity of these tests is only 51.5%, which results in a considerable rate of misdiagnosis.4,5 In comparison, HPV screening yields a sensitivity and specificity of 88.2% and 57.8%, respectively, for detecting CIN 2+; its sensitivity is relatively high, but its specificity is considerably lower than that of cervical cytology, which leads to unnecessary colposcopy and other invasive examinations.6 According to the screening guidelines for cervical cancer issued by the American Society of Colposcopy and Cervical Pathology, the best screening option for women aged 30–65 years is a combined HPV detection and cytology test because co-testing can increase both the sensitivity and the specificity of cervical cancer screening.7 However, although co-testing effectively improves the accuracy of diagnosis, ~60%–80% of patients referred to colposcopy still undergo invasive screening with no benefit.6,8 Therefore, it is imperative to develop new screening strategies and techniques to reduce the misdiagnosis rate and to minimize invasive examinations. Cervical immunocytochemical staining is used to analyze specific molecular markers in liquid-based cytology samples. In the 2014 version of the Bethesda System for Reporting Cervical Cytology, immunocytochemical staining was recommended as an adjuvant test for cytologic diagnosis.9 In recent years, many studies have investigated the clinical application of cervical immunocytochemical staining. The present study reviews the progress in immunocytochemical staining in cervical cytology and its clinical applications.
p16/Ki67 dual staining and its applications
p16/Ki67 dual staining
The cyclin-dependent protein kinase inhibitor p16INK4a is a negative regulator of the cell cycle pathway of cyclinD-CDK4/6-pRb-E2F that regulates the transition from the G1 to the S phase of the cell cycle and normally functions as a cell cycle brake or tumor suppressor.10 The expression of p16 is reduced in many cancers by mutation, deletion of the gene, or hypermethylation of its promoter.11–13 However, in the cases of cervical high-grade squamous intraepithelial lesion (HSIL) and carcinomas induced by persistent infection of high-risk HPV (HR-HPV) that contributes to neoplastic progression through the action of E6 and E7 viral oncoproteins, the product of p16 has been shown to be overexpressed as a result of functional inactivation of retinoblastoma protein (pRb) by the HPV E7 protein, which due to that the loss of pRb function should result in the release of the p16 gene from negative transcriptional feedback control.14 Therefore, p16 was considered as a potential biomarker that can be used in cervical cancer screening.15,16 However, p16 single staining has limited use in screening since p16 is also expressed in normal cervical cells. Ki-67 is a nuclear antigen expressed in all phases of the cell cycle except for G0 phase and is a proliferation marker. Functional inactivation of pRb may lead only to genetic instability in normal cells; however, it will cause malignant transformation in DNA replication-competent cells. Therefore, simultaneous detection of tumor suppressor gene p16 overexpression and expression of the proliferation marker Ki-67 within the same cervical epithelial cell should indicate deregulation of the cell cycle and reveal genuine lesions, which is independent of morphological examination results. Because in normal cells, in which p16 functions as a tumor suppressor gene and the Ki-67 functions as a cellular proliferation marker, they should be mutually exclusive and rarely expressed simultaneously.17–19 Previous studies showed that p16/Ki67 dual staining can effectively detect cervical cancer and precancerous lesions.20 The stain model is shown in Figure 1: A shows the negative staining, B shows the H&E staining, C shows the Ki-67 nuclear positive staining, D shows the p16 cytoplasmic positive staining, and E shows the p16 cytoplasmic and Ki-67 nuclear co-positive staining.
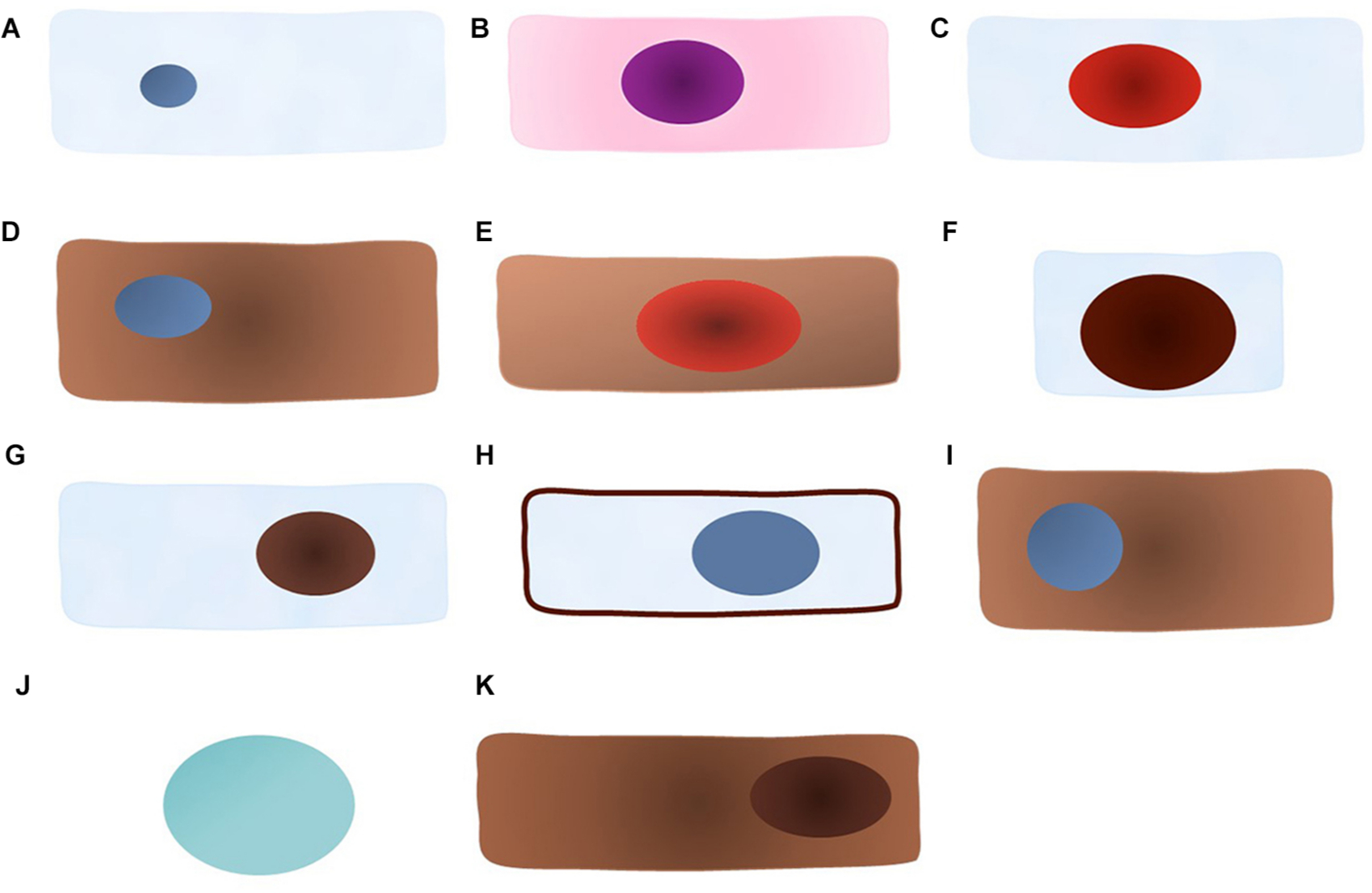 | Figure 1 The cellular model of each marker positive staining. Note: (A) Negative staining; (B) H&E staining; (C) Ki-67 nuclear positive staining; (D) p16 cytoplasmic positive staining; (E) p16 cytoplasmic and Ki-67 nuclear co-positive staining; (F) ProEx™ C nuclear positive staining; (G) HPV L1 capsid protein nuclear positive staining; (H) Claudin 1 membranous positive staining; (I) IMP3 cytoplasmic positive staining; (J) Feulgen-thionin staining for DNA; and (K) RKIP nuclear and cytoplasmic positive staining. Abbreviations: HPV, human papillomavirus; IMP3, insulin-like growth factor-II mRNA-binding protein 3; RKIP, Raf kinase inhibitor protein. |
p16/Ki67 dual staining in primary screening
Primary screening based on cytology or HR-HPV types is associated with an increased misdiagnosis rate and overtreatment. In 2013, the prospective multicenter Primary atypical squamous cells of undetermined significance (ASC-US) low-grade squamous intraepithelial lesion (LSIL) Marker Study (PALMS) screened 27,349 women between the ages of 18 and 65 years in five European countries. The results showed that for all participants, p16/Ki67 dual staining exhibited superior sensitivity (86.7% vs 68.5%, P<0.001) and comparable specificity (95.2% vs 95.4%, P=0.15) compared with cytology for the identification of CIN 2+ by biopsy. For participants >30 years of age, the HPV test exhibited a higher sensitivity (93.3% vs 84.7%, P=0.03) but a lower specificity (93.0% vs 96.2%, P<0.001) than p16/Ki67 dual staining. For participants <30 years of age, p16/Ki67 dual staining exhibited a specificity that was similar to that of cytology (92.6% vs 92.0%, P>0.05) but had a significantly higher sensitivity (89.4% vs 71.9%). Hence, it was proposed that p16/Ki67 dual staining might be a potential screening strategy for cervical lesions, especially for individuals <30 years of age.20
However, another study conducted by Yu et al screened 1,079 women attending ongoing cervical cancer screening and reported an inconsistent outcome.21 The results showed that the sensitivity of p16/Ki-67 for the detection of CIN 2+ in the whole screened population was no different from that of cytology and HR-HPV detection (90.9% vs 93.5% vs 94.4%, P>0.05). However, the specificity was slightly higher than that of cytology (79.5% vs 76.2%, P=0.042). The authors considered that this difference might be due to the different populations and the different methods of cytology or HPV testing between these two studies. Moreover, all the cytological diagnoses were made by experienced cytologists, which may also be an important factor in its comparability with other studies (Table 1).
 | Table 1 Diagnostic performance of the p16/Ki-67 dual staining in primary screening for detecting CIN 2+ Abbreviations: CIN 2+, cervical intraepithelial neoplasia 2 and above; HPV, human papillomavirus; HR-HPV, high-risk HPV. |
p16/Ki67 dual staining in patients referred to colposcopy
According to the current screening guidelines, patients are referred to colposcopy if they are HPV16/18 (+), HR-HPV (–) combined with >atypical squamous cells of undetermined significance (ASCUS) cytology, or HR-HPV (+) with ≥ASCUS cytology. However, both the literature and the data from Peking Union Hospital indicate that among patients referred to colposcopy (except for those with cytologic HSIL), only 10%–40% were CIN 2+ according to biopsy.22,23 Hence, for patients who were referred to colposcopy by co-testing, triage strategies should be implemented to increase the positive detection rate of colposcopy. In 2011, the triage performance of p16/Ki-67 was evaluated by Petry et al in patients with cytology (–) combined HPV (+), and the results showed that the sensitivity and specificity were 91.9% and 82.1%, respectively.24 During the following year, Wentzensen et al examined 625 patients referred to colposcopy and showed that as the cervical lesion severity worsened, the positive rate of p16/Ki67 dual staining increased substantially. For the detection of CIN 2+, dual staining exhibited a sensitivity of 86.4% (81.5%–90.2%) and a specificity of 59.5% (54.2%–64.5%), and the colposcopy referral rate was reduced to 59.55% (55.7–63.3).25 It is also worth noting that for patients with HR-HPV (+) combined with ASCUS/LSIL cytology, p16/Ki67 dual staining exhibited high sensitivity (90.6%, 73.8–97.5) and moderate specificity (48.6%, 43.5–53.9) for the detection of CIN 3+ lesions. A study in Italy also revealed a significant correlation between the positive rate of p16/Ki67 dual staining and the severity of cervical lesions and showed the sensitivity (79.7%) and specificity (73.5%) of dual staining for the detection of CIN 2+.23 In addition, the Dutch study “VUSA-Screen” showed that the sensitivity of p16/Ki67 dual staining for patients with HPV (+) combined with ASCUS cytology was significantly higher than that for patients who were HPV (+) and ThinPrep cytologic test (TCT) (–) (91% vs 68.8%), although the specificity was poor (30.6% vs 72.8%). Afterward, specimens from 1,021 women who were HPV (+) and TCT (–) were subjected to p16/Ki-67 dual staining for subsequent triage. Compared with HPV16/18 genotyping, p16/Ki-67 dual staining exhibited a higher sensitivity (73.3% vs 46.7%) and comparable specificity for detecting CIN 3+.26 Taken together, p16/Ki67 dual staining significantly reduces the referral rate for colposcopy that results from current screening guidelines, but the dual staining approach is accompanied by a noticeable increase in the misdiagnosis rate (Table 2).
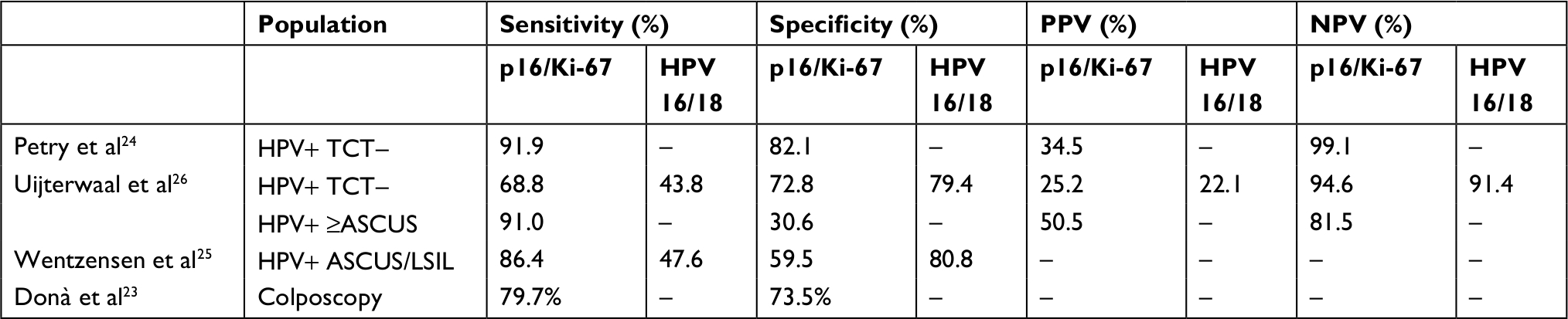 | Table 2 Triage performance of the p16/Ki-67 dual staining in patients referred to colposcopy for detecting CIN 2+ Abbreviations: CIN 2+, cervical intraepithelial neoplasia 2 and above; HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion; NPV, negative predictive value; TCT, ThinPrep cytologic test. |
p16/Ki67 dual staining in patients with ASCUS/LSIL cytology
Patients with ASCUS/LSIL who were screened using primary cytology should be subjected to triage before referral to colposcopy due to several issues associated with cytology, including its low sensitivity, high misdiagnosis rate, poor reproducibility, and reliance on the experience of cytologists.9 Specifically, patients with a low-risk cytology result should then undergo routine screening, whereas those at a higher risk require further examinations or close follow-up. Many studies have examined the triage management for patients with ASCUS/LSIL. In 2010, European Equivocal or Mildly Abnormal Pap Cytology Study, which recruited 810 cytologically diagnosed ASCUS/LSIL patients, showed that p16/Ki67 dual staining exhibited a similar sensitivity for detecting CIN 2+ to that of the HR-HPV test (92.2%–94.2% vs 90.9%–96.4%), and a significantly higher specificity (80.6%–68% vs 36.3%–19.1%).27 In 2015, Bergeron et al conducted the PALMS study, in which over 1,000 patients with ASCUS/LSIL were examined, and reported a similar conclusion. Specifically, the results showed that for detecting CIN 2+ lesions, p16/Ki67 dual staining exhibited a similar sensitivity (94.4% vs 100%, P=0.317) but a significantly higher specificity (78.7% vs 60.4%, P<0.001) compared with the hybrid capture 2 (HC2) test. For detecting CIN 2+ lesions in patients with LSIL, p16/Ki67 dual staining exhibited a slightly lower sensitivity than that of the HC2 test (85.7% vs 98.4%, P=0.005), but its specificity was higher by 37.7% (53.3% vs 15.6%, P<0.001). More importantly, in patients <30 years, the positive predictive value of p16/Ki67 dual staining for CIN 2+ was 86% higher than that of the HC2 test.28 In the same year, however, a prospective multicenter study in China revealed that for patients with ASCUS/LSIL, the sensitivities of the two tests (p16/Ki67 dual staining and the HR-HPV test) were not different and that the specificity of p16/Ki67 dual staining for cervical lesions was increased by only 11% (66.4% vs 55.8%). Nevertheless, its referral rate for colposcopy was reduced by 10% (43.8% vs 53.1%) compared with that of the HR-HPV test.21 Hence, although considerable differences are found in the results from various studies, p16/Ki67 dual staining is superior to the HR-HPV test in the referral rate of patients who are cytologically diagnosed with ASCUS/LSIL (Table 3).
 | Table 3 Triage performance of the p16/Ki-67 dual staining in patients with ASCUS/LSIL for detecting CIN 2+ Abbreviations: ASCUS, atypical squamous cells of undetermined significance CIN 2+, cervical intraepithelial neoplasia 2 and above; HR-HPV, high-risk human papillomavirus; LSIL, low-grade squamous intraepithelial lesion; NPV, negative predictive value. |
p16/Ki67 dual staining in HR-HPV-positive patients
With a deep understanding of persistent HR-HPV infection and the development of cervical cancer, HR-HPV testing has been demonstrated to be a highly sensitive and reproducible screening approach. According to the data based on HR-HPV primary screening, including the publication of the prospective study ATHENA (Addressing The Need for Advanced HPV Diagnostics)29 and the publication of the follow-up data from multiple HPV screening trials, the HR-HPV test was proposed as the primary cervical cancer screening strategy in the 2015 Clinical Guidelines for Cervical Cancer Screening in the USA due to its extremely high sensitivity.7 However, the HR-HPV test showed a poor specificity in that it could not distinguish a transient infection from a persistent infection. Consequently, if all patients with HR-HPV positivity are referred to colposcopy, this inevitably leads to overdiagnosis, overtreatment, and a waste of medical resources. Therefore, tremendous effort has been dedicated to the triage of HR-HPV-positive patients, but the results thus far are controversial. In 2015, Wentzensen et al examined 2,363 HR-HPV-positive patients from the Kaiser Permanente Northern California Health System and showed that for triage of HR-HPV-positive patients, the sensitivity (83.4% vs 76.6%, P=0.1), specificity (58.9% vs 49.6%, P<0.001), positive predictive value (21.0% vs 16.6%, P<0.001), and negative predictive value (96.4% vs 94.2%, P=0.01) of p16/Ki67 dual staining were all better than those of cytology. Moreover, the number of p16/Ki67-positive cells was correlated with a significant increase in specificity.30 In addition, the ATHENA study showed that, compared with cytology, p16/Ki67 dual staining had a higher sensitivity (70.3% vs 51.8%) and a similar specificity (75.6% vs 76.1%) for the triage of HR-HPV-positive patients.31 Ovestad et al also reported that p16/Ki-67 dual staining was more sensitive (88.0% vs 79.0%, P=0.008) but less specific (31.0% vs 35.0%) than cytology for predicting CIN 2+.32 Data from a Chinese study showed that p16/Ki67 dual staining did not exhibit better sensitivity (92.7% vs 94.5%) or specificity (52.7% vs 53.5%) than cytology (Table 4).21
 | Table 4 Triage performance of the p16/Ki-67 dual staining in patients with HPV+ for detecting CIN 2+ Abbreviations: CIN 2+, cervical intraepithelial neoplasia 2 and above; HPV, human papillomavirus; NPV, negative predictive value; PPV, positive predictive value. |
Exploration of other cytological markers
BD ProEx™ C
Topoisomerase II-a (TOP2A) is an enzyme that controls and alters the replication, transcription, and chromosome segregation of DNA during transcription. Mini-chromosome maintenance protein-2 (MCM2) is a member of the highly conserved mini-chromosome maintenance (MCM) protein family, which is involved in the initiation of eukaryotic genome replication in high-grade cervical dysplasia and carcinoma.33,34 Moreover, TOP2A and MCM2 have been identified as overexpressed genes in cervical carcinoma.35,36 The ProEx™ C (TriPath Imaging, Inc., Burlington, NC, USA) test is an immunocytochemical assay that detects TOP2A and MCM2 in liquid-based cervical cytology specimens as a potential diagnostic adjunct for the identification of HSIL.37 Shroyer et al validated the ProEx C test in 330 cervical cytology samples and suggested that the ProEx C could be an adjunct used to improve the diagnostic accuracy of cervical cytology and may be useful in the identification of underlying CIN 2+ lesions by biopsy in patients with LSIL diagnosed by cytology.38 In the same year, another study reported that the sensitivity of ProEx C for biopsy-proven HSIL was significantly greater than that of cytology (85.3% vs 50%) in cases with abnormal cytology.39 Two years later, through an evaluation of 624 cytology samples, Tambouret et al showed that the sensitivity and specificity of ProEx C were 81% and 82%, respectively, for detecting CIN 2+. Additionally, when combined with any level of cytologic atypia, the sensitivity and specificity were increased to 92% and 84%, respectively.40 Moreover, Alaghehbandan et al reported that the sensitivity of ProEx C for detecting CIN 2+ was 71.6% and 67.6% in patients with ASCUS and LSIL, respectively, as detected by cytologic analysis; they also determined that the specificity was 74.6% and 60%, respectively.41 However, another study reported that the combination of p16Ink4a staining and ProEx C did not significantly improve the accuracy of cytology for detecting HSIL by biopsy. In contrast, Walts et al considered that when p16 staining and ProEx C yield discordant results, performing p16 staining and ProEx C followed by Ki-67 staining might provide considerable diagnostic accuracy and a better cost performance ratio.42 Recently, Zheng performed HPV and MCM2 detection on 183 liquid-based Pap smear samples. The result showed that the expression level of MCM2 was positively correlated with the high-risk types of HPV and suggested that MCM2 may serve as a useful marker in cervical lesion screening. The authors also suggested that, due to its superior performance over HPV genotyping, MCM2 detection may improve the diagnosis of ASCUS significance.43 Moreover, the combined detection of TOP2A and Ki-67 may be used in immunocytochemistry assays for cervical cancer screening because the combined immunocytochemistry results were positive in 96.4% of samples that were HPV-DNA+ and that had cytological abnormalities (Table 5).44 The positive staining model is showed in Figure 1F.
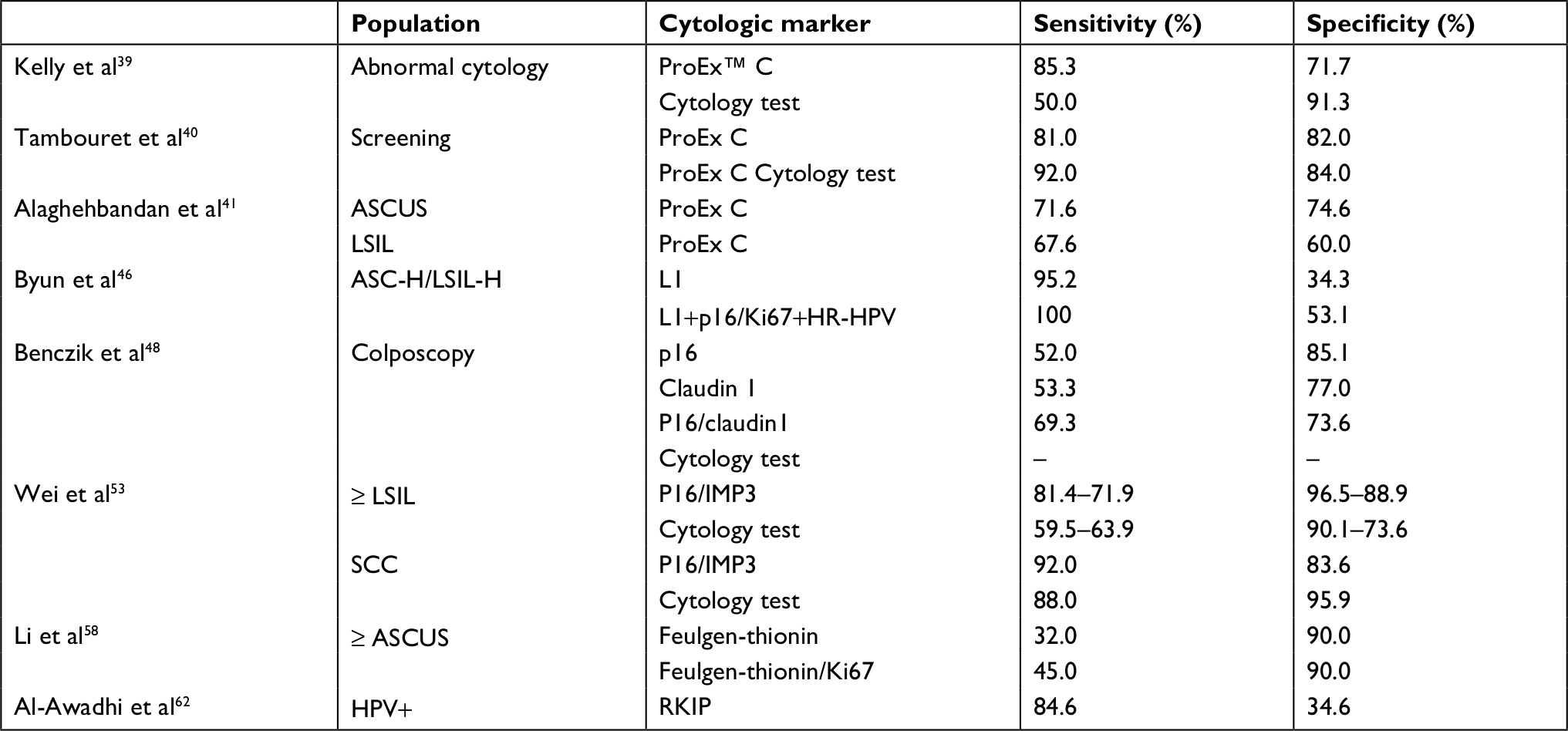 | Table 5 Diagnostic performance of other staining marker for detecting CIN 2+ Abbreviations: CIN 2+, cervical intraepithelial neoplasia 2 and above; HPV, human papillomavirus; HR-HPV, high-risk HPV; IMP3, insulin-like growth factor-II mRNA-binding protein 3; LSIL, low-grade squamous intraepithelial lesion; RKIP, Raf kinase inhibitor protein; SCC, squamous cell carcinoma. |
HPV L1 capsid protein
L1 is a main capsid protein of the HPV virus. During HPV replication, if the virus is not integrated into the host genome, host cells can differentiate normally. The positive expression of L1 allows it to form an immune complex simultaneously with T cells and major histocompatibility class I/II, thereby activating the immune system to produce high, local concentrations of antibodies, which ultimately leads to elimination of the virus. On the contrary, loss of L1 often indicates viral integration into the host DNA, cell cycle dysregulation, and disease progression. As such, the expression of L1 capsid protein may reflect the viral infection state, which is related to the severity of cervical lesions.45 In the study by Byun et al, L1 capsid protein was evaluated for triage of ASC-H/LSIL-H patients, and their data revealed that although L1 capsid protein was highly sensitive (95.2%), its specificity was poor (34.3%). However, by combining the p16/Ki67 staining with the HR-HPV test, the sensitivity reached 100% for detecting CIN 2+ lesions, and the specificity was doubled (Table 5).46 The positive staining model is shown in Figure 1G.
Claudin 1
Claudin protein is the major blocking protein for tight junctions of epithelial cells and is involved in cell signal transduction. The overexpression of claudins is associated with the progression of cervical neoplasms.47 Benczik et al compared the performance of claudin 1, p16, and the combination of claudin 1 and p16 immunocytochemistry in 502 women who were referred to colposcopy according to HPV and cytology test and reported that the sensitivity of claudin 1, p16, and the combination of claudin 1 and p16 immunocytochemistry was 53.3%, 52% and 69.3%, respectively; however, the specificity was 77%, 85.1%, and 73.6%, respectively. The results indicated that sensitivity of claudin1 was slightly higher than the p16, whereas specificity of claudin1 was found to be lower.48 A European study that examined 792 cervical cytology samples indicated that combined p16/Ki67 and claudin1 staining reduced unnecessary invasive examinations and was more cost-effective for clinical use.49 The positive staining model is shown in Figure 1H.
BCL2 associated X/BCL2 antagonist/killer (Bax/Bak)
As an apoptosis-promoting gene, Bax is a member of BCL-2 gene family. Its protein product may interact with HPV E6/E7 to stimulate carcinogenic potential.50 In 2015, an Indian group performed the HPV test, cytology test, and Bax/Bak staining in 120 specimens of cervical liquid-based cytology samples and found that Bax/Bak staining was only weakly correlated with cytological results, although these negative results may be attributable to the small sample size. Moreover, in all cases, the results showed that there is no statistically significant difference in the Bax and Bak scores between any compared groups including the control, low-risk HPV types, and high-risk HPV types group.51 Therefore, the Bax/Bak may not be considered as an accurate immunocytochemistry biomarker for cervical cancer screening according to the existing data. In addition, the connection between the immunocytochemistry expression of Bax/Bak and the development of cervical intraepithelial dysplasia should be developed in a further study to evaluate their potential usefulness as a biomarker for cervical cancer screening.
Insulin-like growth factor-II mRNA-binding protein 3 (IMP3)
IMP3 is a member of the insulin-like growth factor II (IGF-II) mRNA-binding protein (IMP) family, which promotes tumor development by regulating IGF-II and various cell adhesion factors.52 In a Chinese study, IMP3/p16 dual staining was performed on 98 specimens with cytological results ≥LSIL. The data showed that for CIN 1 and CIN 2/3, IMP3/p16 staining was more sensitive (81.4% and 71.9% vs 59.5% and 63.9%) and specific than (96.5% and 88.9% vs 90.1% and 73.6%) cytology. However, for squamous cell carcinoma, IMP3/p16 staining exhibited a higher sensitivity (92.0% vs 88.0%) and a lower specificity than cytology (83.6% vs 95.9%).53 Moreover, studies revealed that the IMP3 is better known to be expressed in endocervical adenocarcinoma in situ but not in benign endocervical glands.54 IMP3 immunocytochemistry staining also showed that IMP3 is consistently positive in glandular neoplasms but not so in squamous-derived lesions, which might due to that IMP3 has been described to be positive in more glandular neoplasms originating from ovarian carcinomas or endometrial carcinomas other than the endocervix sites. Hence, the IMP3 immunocytochemistry staining positive of atypical glandular cells might only favor a neoplastic process rather than the precision origin of the lesion. Furthermore, in the setting of differentiating glandular neoplasms from squamous lesions, the performance of ProEx C appears to be suboptimal for that positivity percent showed no statistically significant difference in both lesion subgroups. Therefore, Ricardo et al used IMP3/ProEx C staining to analyze specimens diagnosed as atypical glandular cells of uncertain significance (AGUS) based on cervical cytology and showed that this method generated a positive predictive value of 100% for adenocarcinoma and a negative predictive value of 83% for lesions not associated with adenocytes.55 Hence, it was suggested that IMP3/ProEx C staining may serve as a potential diagnostic marker for patients with AGUS. The positive staining model is shown in Figure 1I.
Feulgen-thionin staining
“Ploidy” is the genetics term for the number of basic sets of chromosomes in the cell nucleus, which is divided into “euploid” and “aneuploid” for cells with or not an integer multiple of the basic set of chromosomes, respectively. There is abundant evidence that alterations in DNA ploidy, such as aneuploid, is observed in early events of carcinogenesis.56 Feulgen-thionin staining is an intranuclear DNA staining technique that can be used for the quantitative analysis of DNA in the nuclei, which can be used to detect DNA ploidy using computer-assisted image cytometry.
Studies have shown that Feulgen-thionin staining allows for the effective identification of LSIL/HSIL lesions in cervical cytology samples. The number of aneuploid cells is statistically higher in the HSIL biopsy specimens compared with the LSIL specimens (P<0.0005).57 In subsequent studies, Li et al preformed double staining with Feulgen-thionin and anti-Ki-67 immunocytochemistry and found that with the same specificity (90%), the sensitivity of double staining and thionin staining alone was 45% and 32%, respectively (P>0.05).58 Nevertheless, this approach provides a new strategy for the screening of cervical lesions. The positive staining model is shown in Figure 1J.
Mindbomb E3 ubiquitin protein ligase 1 (MIB1)
MIB1 is a nuclear protein that is associated with cell proliferation. More studies have demonstrated that Ki-67/MIB-1 has prognostic value for overall survival in patients with cervical cancer.59 Sahebali et al investigated the positive rate of p16 and MIB1 expressions in cytological samples diagnosed as ASCUS, LSIL, or HSIL. A higher mean number of p16- and MIB-1-immunoreactive cells was observed in HSIL compared with the other cytological categories, which confirms that positive staining for p16 and MIB-1 could be used as an adjunct to increase the sensitivity of cytological screening.60
Raf kinase inhibitor protein (RKIP)
RKIP is a member of the phosphatidylethanolamine-binding family and has a critical role in multiple signaling pathways, including the MAP kinase, NF-kappa B, and glycogen synthase kinase-3 signaling pathways. RKIP showed low expression in cervical carcinomas and differential expression between tumor samples from patients with and without lymph node metastasis.61 Previous studies also demonstrated that RKIP expression, which was mainly associated with normal cervical tissue sections, was lower in CIN tissues and lowest in invasive carcinomas.61 Moreover, RKIP inhibition can induce apoptotic resistance in cervical cancer cells treated with cisplatin.62
To evaluate the ability of RKIP for distinguishing HSIL lesions from cervical samples of HPV infection, Al-Awadhi et al performed RKIP immunocytochemical staining in 316 ThinPrep cervical HPV-positive samples. However, the results showed that RKIP expression increased with the aggravation of cytologic abnormality, which was inconsistent with the results previous research reported. This might be due to that the gold standard was cytology diagnosis rather than colposcopy histology in their study, which may result in different diagnostic results for the same lesion. In addition, the sensitivity and specificity of RKIP were 84.6% and 34.6%, respectively, for the detection of cytology HSIL and above.63 The positive staining model is shown in Figure 1K.
Ezrin and E-cadherin
Ezrin is a cytoplasmic peripheral membrane protein that functions as a protein-tyrosine kinase substrate in microvilli. As a member of the Ezrin/Radixin/Moesin family, Ezrin participates in the regulation of cell surface structure adhesion, migration, and organization, and its overexpression has been reported in various human cancers including cervical cancer and CIN.64,65 The overexpression of Ezrin has also been reported to be associated with poor prognosis and tumor invasiveness, and its expression was higher in invasive cervical cancer and metastatic cancer.66 E-cadherin is a calcium-dependent cell–cell adhesion protein, and its downregulation, which primarily occurs through E6 protein,67 has been demonstrated to be associated with the invasion and metastasis of various cancers.68,69 Recently, Zacapala-Gómez et al performed immunocytochemical staining for Ezrin and E-cadherin in cervical cytological samples from 125 patients. The results showed that high Ezrin and low E-cadherin expressions were observed in 70% and 95% of cervical cancer samples, respectively, in 43% and 87% of samples with multiple HR-HPV infections, respectively, and in 47% and 72% of samples with integrated viral genome, respectively, which demonstrated that the expressions of Ezrin and E-cadherin as detected by immunocytochemistry in cervical cytology samples could be a potential marker for detecting high-risk CIN.70
Conclusion
Cervical cancer is still a major problem for healthy women worldwide despite significant efforts. Although the development of cervical cancer screening has led to a drastic reduction in the incidence of cervical cancer, there are still many challenges. In the past several decades, screening has focused on cytologic analysis rather than on the detection of HPV infection. With our growing understanding of HPV infection and the advent of HPV testing, the sensitivity for detecting CIN 2+ lesions has improved significantly. However, overdiagnosis and treatment of HPV infection has followed because the lifetime risk of having HPV is high (90%), and most HPV infections (80%) will clear within 2 years. Studies have shown that, with co-testing, 60%–80% of patients, except for those who were diagnosed with HSIL by cytology, who underwent colposcopy did not benefit, which reminded us that it should be possible to not only increase sensitivity in order to detect cancers and precancers but also specificity to reduce misdiagnoses and unnecessary invasive examinations in cervical cancer screening. Therefore, there is a need to triage patients with abnormal screening results in order to reduce the number of false positives.
With our understanding of the molecular changes that result from HPV, immunocytochemical staining of cervical cytology samples has exhibited tremendous potential in early cervical cancer screening. On the basis of the existing guidelines for cervical cancer screening, the integration of more sensitive and specific biomarkers can improve the accuracy of cervical cancer screening and reduce unnecessary invasive examinations. This review demonstrated that although many markers were evaluated in cytology samples in various studies, fewer indicators have been used for further clinical application except for ProEx C and p16/Ki-67 dual staining, which might be due to the unsatisfactory sensitivity and specificity. Literature reviews have shown that the sensitivities of ProEx C and p16/Ki-67 dual staining for detecting CIN 2+ ranged from 67.6% to 81% and 68.8% to 94.4%, respectively, and that the specificity ranged from 60% to 82% and 30.6% to 95.2%, respectively. As of now, studies on immunocytochemical staining have primarily focused on p16/Ki67 for triage strategies in populations with cytology-proven ASCUS/LSIL and HR-HPV positivity. However, the sensitivity and specificity differed in various studies, which might be due to differences in the population background (age, race, and categories) and the methods of cytology and HPV testing. The present review showed that p16/Ki-67 dual staining is a more attractive biomarker for screening of cervical lesions and cancer, especially for triage in cervical cancer screening. Because that p16/Ki-67 cytology dual staining has a higher sensitivity and specificity for detecting cervical precancer than any other immunocytochemical staining markers according to the literatures, which could effectively reduce the colposcopy referral. Moreover, a health economic analysis also should be performed in order to assess the cost-effectiveness and economic impact of this triage strategy. Nevertheless, we also anticipate that in the near future, more advantageous molecular markers and staining methods will be discovered, which will lead to cervical cancer screening benefits in a broader population.
Acknowledgment
This study was funded by the CAMS Initiative for Innovative Medicine (CAMS-2017-I2M-1-002 [Keng Shen]).
Disclosure
The authors report no conflicts of interest in this work.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. | ||
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. | ||
Saxena U, Sauvaget C, Sankaranarayanan R. Evidence-based screening, early diagnosis and treatment strategy of cervical cancer for national policy in low-resource countries: example of India. Asian Pac J Cancer Prev. 2012;13(4):1699–1703. | ||
Committee on Practice Bulletins – Gynecology. Practice Bulletin no. 168: cervical cancer screening and prevention. J Gynecol Obstet. 2016;128(4):e111–e130. | ||
Wright TC Jr, Stoler MH, Behrens CM, Sharma A, Sharma K, Apple R. Interlaboratory variation in the performance of liquid-based cytology: insights from the ATHENA trial. Int J Cancer. 2014;134(8):1835–1843. | ||
Murphy J, Kennedy EB, Dunn S, et al. HPV testing in primary cervical screening: a systematic review and meta-analysis. J Obstet Gynaecol Can. 2012;34(5):443–452. | ||
Huh WK, Ault KA, Chelmow D, et al. Use of primary high-risk human papillomavirus testing for cervical cancer screening: interim clinical guidance. Gynecol Oncol. 2015;136(2):178–182. | ||
Graham SV. The human papillomavirus replication cycle, and its links to cancer progression: a comprehensive review. Clin Sci. 2017;131(17):2201–2221. | ||
Nayar R, Wilbur DC. The Bethesda System for Reporting Cervical Cytology: Definitions, Criteria, and Explanatory Notes. New York: Springer; 2015. | ||
Ortega S, Malumbres M, Barbacid M. Cyclin D-dependent kinases, INK4 inhibitors and cancer. Biochim Biophys Acta. 2002;1602(1):73–87. | ||
Piccinin S, Doglioni C, Maestro R, et al. p16/CDKN2 and CDK4 gene mutations in sporadic melanoma development and progression. Int J Cancer. 1997;74(1):26–30. | ||
Zhao P, Hu YC, Talbot IC. Expressing patterns of p16 and CDK4 correlated to prognosis in colorectal carcinoma. World J Gastroenterol. 2003;9(10):2202. | ||
Zhou Y, Gao SS, Li YX, et al. Tumor suppressor gene p16 and Rb expression in gastric cardia precancerous lesions from subjects at a high incidence area in northern China. World J Gastroenterol. 2002;8(3):423. | ||
von Knebel Doeberitz M. Searching for new biomarkers for cervical cancer: molecular accidents and the interplay of papillomavirus oncogenes and epithelial differentiation—Part 1. Papillomavirus Rep. 2002;13(2):35–41. | ||
Darragh TM, Colgan TJ, Cox JT, et al. The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Arch Pathol Lab Med. 2012;136(10):1266–1297. | ||
Murphy N, Ring M, Killalea AG, et al. P16INK4a as a marker for cervical dyskaryosis: CIN and cGIN in cervical biopsies and ThinPrep™ smears. J Clin Pathol. 2003;56(1):56–63. | ||
Waldstrøm M, Christensen RK, Ørnskov D. Evaluation of p16(INK4a)/Ki-67 dual stain in comparison with an mRNA human papillomavirus test on liquid-based cytology samples with low-grade squamous intraepithelial lesion. Cancer Cytopathol. 2013;121(3):136–145. | ||
Atkins K. p16/Ki-67 dual-stain cytology in the triage of ASCUS and LSIL Papanicolaou cytology. Cancer Cytopathol. 2011;119(3):145–147. | ||
Sahasrabuddhe VV, Luhn P, Wentzensen N. Human papillomavirus and cervical cancer: biomarkers for improved prevention efforts. Future Microbiol. 2011;6(9):1083–1098. | ||
Ikenberg H, Bergeron C, Schmidt D, et al. Screening for cervical cancer precursors with p16/Ki-67 dual-stained cytology: results of the palms study. J Natl Cancer Inst. 2013;105(20):1550–1557. | ||
Yu LL, Chen W, Lei XQ, et al. Evaluation of p16/Ki-67 dual staining in detection of cervical precancer and cancers: a multicenter study in China. Oncotarget. 2016;7(16):21181–21189. | ||
Ordi J, Sagasta A, Munmany M, Rodríguez-Carunchio L, Torné A, del Pino M. Usefulness of p16/Ki67 immunostaining in the triage of women referred to colposcopy. Cancer Cytopathol. 2014;122(3):227–235. | ||
Donà MG, Vocaturo A, Giuliani M, et al. p16/Ki-67 dual staining in cervico-vaginal cytology: correlation with histology, Human Papillomavirus detection and genotyping in women undergoing colposcopy. Gynecol Oncol. 2012;126(2):198–202. | ||
Petry KU, Schmidt D, Scherbring S, et al. Triaging Pap cytology negative, HPV positive cervical cancer screening results with p16/Ki-67 dual-stained cytology. Gynecol Oncol. 2011;121(3):505–509. | ||
Wentzensen N, Schwartz L, Zuna RE, et al. Performance of p16/Ki-67 immunostaining to detect cervical cancer precursors in a colposcopy referral population. Clin Cancer Res. 2012;18(15):4154–4162. | ||
Uijterwaal MH, Witte BI, van Kemenade FJ, et al. Triaging borderline/mild dyskaryotic Pap cytology with p16/Ki-67 dual-stained cytology testing: cross-sectional and longitudinal outcome study. Br J Cancer. 2014;110(6):1579–1586. | ||
Schmidt D, Bergeron C, Denton KJ, Ridder R, European CINtec Cytology Study Group. p16/ki-67 dual-stain cytology in the triage of ASCUS and LSIL Papanicolaou cytology: results from the European equivocal or mildly abnormal Papanicolaou cytology study. Cancer Cytopathol. 2011;119(3):158–166. | ||
Bergeron C, Ikenberg H, Sideri M, et al. Prospective evaluation of p16/Ki-67 dual-stained cytology for managing women with abnormal Papanicolaou cytology: PALMS study results. Cancer Cytopathol. 2015;123(6):373–381. | ||
Wright TC, Stoler MH, Behrens CM, Sharma A, Zhang G, Wright TL. Primary cervical cancer screening with human papillomavirus: end of study results from the ATHENA study using HPV as the first-line screening test. Gynecol Oncol. 2015;136(2):189–197. | ||
Wentzensen N, Fetterman B, Castle PE, et al. p16/Ki-67 dual stain cytology for detection of cervical precancer in HPV-positive women. J Natl Cancer Inst. 2015;107(12):djv257. | ||
Wright TC, Behrens CM, Ranger-Moore J, et al. Triaging HPV-positive women with p16/Ki-67 dual-stained cytology: results from a sub-study nested into the ATHENA trial. Gynecol Oncol. 2017;144(1):51–56. | ||
Ovestad IT, Dalen I, Hansen E, et al. Clinical value of fully automated p16/Ki-67 dual staining in the triage of HPV-positive women in the Norwegian Cervical Cancer Screening Program. Cancer Cytopathol. 2017;125(4):283–291. | ||
Chen Y, Miller C, Mosher R, et al. Identification of cervical cancer markers by cDNA and tissue microarrays. Cancer Res. 2003;63(8):1927–1935. | ||
Burden DA, Osheroff N. Mechanism of action of eukaryotic topoisomerase II and drugs targeted to the enzyme. Biochim Biophys Acta. 1998;1400(1–3):139–154. | ||
Santin AD, Zhan F, Bignotti E, et al. Gene expression profiles of primary HPV16- and HPV18-infected early stage cervical cancers and normal cervical epithelium: identification of novel candidate molecular markers for cervical cancer diagnosis and therapy. Virology. 2005;331(2):269–291. | ||
Murphy N, Ring M, Heffron CC, et al. P16INK4a, Cdc6, and MCM5: predictive biomarkers in cervical preinvasive neoplasia and cervical cancer. J Clin Pathol. 2005;58(5):525–534. | ||
Malinowski DP. Molecular diagnostic assays for cervical neoplasia: emerging markers for the detection of high-grade cervical disease. BioTechniques. 2005;38(4S):S17–S23. | ||
Shroyer KR, Homer P, Heinz D, Singh M. Validation of a novel immunocytochemical assay for topoisomerase II-alpha and minichromosome maintenance protein 2 expression in cervical cytology. Cancer. 2006;108(5):324–330. | ||
Kelly D, Kincaid E, Fansler Z, Rosenthal DL, Clark DP. Detection of cervical high-grade squamous intraepithelial lesions from cytologic samples using a novel immunocytochemical assay (ProEx C). Cancer. 2006;108(6):494–500. | ||
Tambouret RH, Misdraji J, Wilbur DC. Longitudinal clinical evaluation of a novel antibody cocktail for detection of high-grade squamous intraepithelial lesions on cervical cytology specimens. Arch Pathol Lab Med. 2008;132(6):918–925. | ||
Alaghehbandan R, Fontaine D, Bentley J, et al. Performance of ProEx C and PreTect HPV-Proofer E6/E7 mRNA tests in comparison with the hybrid capture 2 HPV DNA test for triaging ASCUS and LSIL cytology. Diagn Cytopathol. 2013;41(9):767–775. | ||
Walts AE, Bose S. P16, Ki-67, and BD ProExC immunostaining: a practical approach for diagnosis of cervical intraepithelial neoplasia. Hum Pathol. 2009;40(7):957–964. | ||
Zheng J. Diagnostic value of Mcm2 immunocytochemical staining in cervical lesions and its relationship with HPV infection. Int J Clin Exp Pathol. 2015;8(1):875–880. | ||
Peres AL, E Silva KM, de Araújo RF, et al. Immunocytochemical study of TOP2A and Ki-67 in cervical smears from women under routine gynecological care. J Biomed Sci. 2016;23(1):42. | ||
Guido R, Schiffman M, Solomon D, Burke L, ASCUS LSIL Triage Study (ALTS) Group. Postcolposcopy management strategies for women referred with low-grade squamous intraepithelial lesions or human papillomavirus DNA-positive atypical squamous cells of undetermined significance: a two-year prospective study. Am J Obstet Gynecol. 2003;188(6):1401–1405. | ||
Byun SW, Lee A, Kim S, Choi YJ, Lee YS, Park JS. Immunostaining of p16(INK4a)/Ki-67 and L1 capsid protein on liquid-based cytology specimens obtained from ASC-H and LSIL-H cases. Int J Med Sci. 2013;10(12):1602–1607. | ||
Sobel G, Páska C, Szabó I, Kiss A, Kádár A, Schaff Z. Increased expression of claudins in cervical squamous intraepithelial neoplasia and invasive carcinoma. Hum Pathol. 2005;36(2):162–169. | ||
Benczik M, Galamb Á, Koiss R, et al. Claudin-1 as a biomarker of cervical cytology and histology. Pathol Oncol Res. 2016;22(1):179–188. | ||
Attila M, Gábor S, Nándor Ács, Zsuzsanna S, Tímea S. A study about the efficiency of cervical cancer screening using biomarkers p16/Ki67 and claudin 1. Eur J Obstet Gynecol Reprod Biol. 2016;206:e73. | ||
Croker BA, O’Donnell JA, Nowell CJ, et al. Fas-mediated neutrophil apoptosis is accelerated by bid, Bak, and Bax and inhibited by Bcl-2 and Mcl-1. Proc Natl Acad Sci USA. 2011;108(32):13135–13140. | ||
Klapsinou E, Argyri E, Panotopoulou E, et al. Bax and Bak expression in cervical smears of women with low-and high-risk HPV types: a study of 120 cases. J Cytol. 2015;32(4):223–229. | ||
Prince SN, Foulstone EJ, Zaccheo OJ, Williams C, Hassan AB. Functional evaluation of novel soluble insulin-like growth factor (IGF)-II-specific ligand traps based on modified domain 11 of the human IGF2 receptor. Mol Cancer Ther. 2007;6(2):607–617. | ||
Wei Q, Fu B, Liu J, Xu J, Zhao T. Combined detection of p16(INK4a) and IMP3 increase the concordance rate between cervical cytologic and histologic diagnosis. Int J Clin Exp Pathol. 2013;6(8):1549–1557. | ||
Li C, Rock KL, Woda BA, Jiang Z, Fraire AE, Dresser K. IMP3 is a novel biomarker for adenocarcinoma in situ of the uterine cervix: an immunohistochemical study in comparison with p16(INK4a) expression. Mod Pathol. 2007;20(2):242–247. | ||
Lastra RR, Ou JJ, Reilly ME, et al. Utility of ProExC and IMP3 immunocytochemical staining in atypical glandular cells of undetermined significance in liquid-based cervical cytology. Diagn Cytopathol. 2014;42(5):375–379. | ||
Garner D. Clinical application of DNA ploidy to cervical cancer screening: a review. World J Clin Oncol. 2014;5(5):931. | ||
Mellin W. Cytophotometry in tumor pathology. A critical review of methods and applications, and some results of DNA analysis. Pathol Res Pract. 1990;186(1):37–62. | ||
Li G, Guillaud M, Follen M, MacAulay C. Double staining cytologic samples with quantitative Feulgen-thionin and anti-Ki-67 immunocytochemistry as a method of distinguishing cells with abnormal DNA content from normal cycling cells. Anal Quant Cytol Histol. 2012;34(5):273–284. | ||
Piri R, Ghaffari A, Azami-Aghdash S, Ali-Akbar YP, Saleh P, Naghavi-Behzad M. Ki-67/MIB-1 as a prognostic marker in cervical cancer: a systematic review with meta-analysis. Asian Pac J Cancer Prev. 2015;16(16):6997–7002. | ||
Sahebali S, Depuydt CE, Boulet GA, et al. Immunocytochemistry in liquid-based cervical cytology: analysis of clinical use following a cross-sectional study. Int J Cancer. 2006;118(5):1254–1260. | ||
Hu CJ, Zhou L, Zhang J, Huang C, Zhang GM. Immunohistochemical detection of Raf kinase inhibitor protein in normal cervical tissue and cervical cancer tissue. J Int Med Res. 2011;39(1):229–237. | ||
Martinho O, Pinto F, Granja S, et al. RKIP inhibition in cervical cancer is associated with higher tumor aggressive behavior and resistance to cisplatin therapy. PLoS One. 2013;8(3):e59104. | ||
Al-Awadhi R, Husain S, Chehadeh W, Al-Jassar W, Kapila K, Al-Mulla F. Immunocytochemical detection of Raf kinase inhibitor protein and human papillomavirus profiling of normal and abnormal cervical ThinPrep samples. Acta Cytol. 2013;57(3):259–265. | ||
Auvinen E, Carpen O, Korpela T, Ronty M, Vaheri A, Tarkkanen J. Altered expression of Ezrin, E-cadherin and β-catenin in cervical neoplasia. Neoplasma. 2012;60(01):56–61. | ||
Kong J, Li Y, Liu S, et al. High expression of ezrin predicts poor prognosis in uterine cervical cancer. BMC Cancer. 2013;13(1):520. | ||
Li M, Feng YM, Fang SQ. Overexpression of ezrin and galectin-3 as predictors of poor prognosis of cervical cancer. Braz J Med Biol Res. 2017;50(4):e5356. | ||
Faghihloo E, Sadeghizadeh M, Shahmahmoodi S, Mokhtari-Azad T. Cdc6 expression is induced by HPV16 E6 and E7 oncogenes and represses E-cadherin expression. Cancer Gene Ther. Epub 2016 Nov 11. | ||
Higashi K, Ueda Y, Shimasaki M, et al. High FDG uptake on PET is associated with negative cell-to-cell adhesion molecule E-cadherin expression in lung adenocarcinoma. Ann Nucl Med. 2017;31(8):590–595. | ||
Zhang Z, Bu X, Chen H, Wang Q, Sha W. Bmi-1 promotes the invasion and migration of colon cancer stem cells through the downregulation of E-cadherin. Int J Mol Med. 2016;38(4):1199–1207. | ||
Zacapala-Gómez AE, Navarro-Tito N, Alarcón-Romero LDC, et al. Ezrin and E-cadherin expression profile in cervical cytology: a prognostic marker for tumor progression in cervical cancer. BMC Cancer. 2018;18(1):349. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.