")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Progranulin and Breast Cancer Mortality: 13-Year Follow-Up of a Cohort Study
Authors Koo DH , Lee KS, Sim SH, Chae H, Lee EG, Han JH, Jung SY , Lee S, Kang HS, Lee ES , Park CY , Oh SW
Received 1 February 2023
Accepted for publication 12 April 2023
Published 14 April 2023 Volume 2023:15 Pages 251—261
DOI https://doi.org/10.2147/BCTT.S406685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Dong-Hoe Koo,1,* Keun Seok Lee,2,* Sung Hoon Sim,2 Heejung Chae,2 Eun-Gyeong Lee,2 Jai Hong Han,2 So-Youn Jung,2 Seeyoun Lee,2 Han-Sung Kang,2 Eun Sook Lee,2 Cheol-Young Park,1,* Sang Woo Oh3,*
1Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea; 2Center for Breast Cancer, Research Institute and Hospital, National Cancer Center, Goyang-si, Gyeonggi-do, Republic of Korea; 3Department of Family Medicine, Center for Obesity, Metabolism, and Nutrition, Dongguk University Ilsan Hospital, Goyang-si, Gyeonggi-do, Republic of Korea
*These authors contributed equally to this work
Correspondence: Cheol-Young Park, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 29 Saemunan-ro, Jongno-gu, Seoul, 03181, Republic of Korea, Tel +82-2-2001-1869, Fax +82-2-2001-1588, Email [email protected] Sang Woo Oh, Center for Obesity, Nutrition, and Metabolism, Department of Family Medicine, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, 27 Donggung-ro, Ilsandong-gu, Goyang-si, Gyeonggi-do, 10326, Republic of Korea, Tel +82-31-961-7000, Email [email protected]
Background: We have reported that serum progranulin (PGRN) levels are clinically significant in predicting recurrence in patients with HR-positive breast cancer. The aim of the present study was to examine whether PGRN levels might be associated with breast cancer mortality.
Methods: This was a cohort study of 695 newly diagnosed breast cancer patients who underwent curative surgery between 2001 and 2004. The relationship between breast cancer mortality and pre-operative serum PGRN levels in these patients with a median follow-up of 12.7 years was evaluated until May 2020.
Results: A total of 118 (17%) deaths were identified in the cohort. According to the HR status, (10, 15, and 20)-year overall survival (OS) rates were (91.4, 81.1, and 75.9) % for HR-positive patients, and (76.5, 74.2, and 69.8) % for HR-negative patients, respectively (p = 0.003). Higher levels of PGRN were significantly associated with poor OS in the HR-positive group (p for trend = 0.001). In particular, hazard ratios for PGRN quartiles suggested a dose–response relationship, with the highest quartile having the worst OS in the HR-positive group (highest vs lowest: 15-year OS, (68.3 vs 90.0) %; 20-year OS, (62.3 vs 84.8) %, even after adjusting for age, tumor stage, and metabolic confounders.
Conclusion: Pre-operative serum PGRN levels had clinical significance for predicting cancer mortality in breast cancer patients independent of tumor stage and metabolic parameters, especially in HR-positive tumors.
Keywords: breast cancer, progranulin, mortality, long-term follow-up
Introduction
Breast cancer is the most common cancer in women in Korea and worldwide.1,2 Hormone-receptor (HR)–positive breast cancer accounts for approximately three-quarters of all cases of breast cancer.3 It has better prognosis than other HR-negative tumors, because adjuvant endocrine therapy for 5-year is available in addition to adjuvant chemotherapy.4 A recent study has reported that adjuvant chemotherapy is not beneficial for some subgroups of patients with HR-positive breast tumor.5 According to 21-gene expression, adjuvant endocrine therapy is not inferior to adjuvant chemotherapy followed by endocrine therapy, since both can lead to excellent prognosis.5
However, HR-positive breast cancers have a risk of late recurrence. Recurrence rates of HR-positive tumors are relatively constant over many years. In addition, these tumors may recur over a long time. Recurrence events beyond 10 years are not uncommon.6 From a long-term perspective, the prognosis of patients with HR-positive breast cancers seems to be not much different from that of patients with HR-negative tumors.7 Such well-known long-term risk of recurrence has led to several trials investigating the benefits of extended endocrine therapy for up to 10 years or more.8,9 Therefore, from a long-term management perspective, it is necessary to predict patients with poor prognosis.
Progranulin (PGRN) is a secreted glycoprotein recognized as an adipokine involved in diet-induced obesity, insulin resistance, or tumor progression cascade, including proliferation, migration, and angiogenesis.10,11 PGRN can enhance proliferation and promote the growth of several cancer cells, such as breast, gastrointestinal, hepatic, lung, and genitourinary cancers.12 Previously, we have reported that preoperative serum PGRN levels have clinical significance for predicting recurrence in patients with HR-positive breast cancer during adjuvant tamoxifen therapy.13 At a median follow-up of 5.2 years, the mortality rate was only 7%. Since the data was immature, we could not compare breast cancer mortality rates according to PGRN levels.
Recent updates after nearly 13 years of cumulative follow-up have shown that the mortality rate of patients with breast cancer is 17%. The aim of the present study was to examine whether PGRN levels might be associated with breast cancer mortality.
Methods
Data Source and Study Cohort
Participants of this study were a cohort of newly diagnosed breast cancer patients who underwent surgery and consented to provide blood samples at the National Cancer Center, Korea, between April 2001 and December 2004. From a total of 856 patients considered for the initial recruitment, 695 patients were analyzed, after excluding 161 patients for the following reasons: unavailable pre-operative PGRN (n = 6), previous history of breast cancer (n = 6), ductal carcinoma in situ (n = 17), cancer with unreported estrogen receptor (ER) or progesterone receptor (PR) status (n = 83), or non-epithelial origin of cancer (n = 49). All diagnoses were verified by reviewing hospital records. All patients with HR-positive tumors received adjuvant tamoxifen therapy, and adjuvant chemotherapy was administered according to postoperative stage, regardless of HR status.13 Written informed consent was obtained from all patients. This study protocol was approved by the Institutional Review Board of the National Cancer Center, Korea (IRB Protocol No. NCCNCS-09-220) and complied with the tenets of the Declaration of Helsinki. Mortality follow-up until May of 2020 was based on nationwide death certificate data from the Korea National Statistical Office (KNSO). The cause of death was listed on each death certificate. It was classified according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). Concordance rate between the cause of death on the death certificate and patient diagnosis in the medical utilization data was 72.2% for all-cause deaths, and 94.9% for cancer deaths.14 Breast cancer mortality was defined as death due to malignant neoplasms of the breast (ICD-10, C50).
Laboratory Assessments
Venous blood samples were taken on the morning following an overnight fast before surgery. After centrifugation, sera were collected, and frozen at −70 °C until analysis. To determine PGRN expression levels in human plasma samples, a human Progranulin ELISA kit (Adipogen Inc., Seoul, Korea) was used with a 1:100 dilution of the plasma sample in 1× diluent, following the manufacturer’s instructions.13,15 The wash solution was aspirated after each third wash, to ensure that all residual wash solution was removed.
Immunohistochemical Staining
To assess ER and PR expression status, immunohistochemical staining was performed using tissue sections cut from formalin-fixed, paraffin-embedded representative breast tumors. Staining was performed using an I–View DAB detection kit and a Ventana ES autostainer (Ventana Medical Systems, Tucson, AZ, USA), using primary antibodies against ER and PR (both from Ventana Medical Systems). Specimens were defined as ER- or PR-positive when nuclear staining was observed in at least 10% of tumor cells tested.16 The ER/PR status was classified into two categories: 1) HR-negative group, patients with ER-negative and PR-negative tumors; and 2) HR-positive group, patients with ER-positive or PR-positive tumors.
Statistical Analysis
Patient characteristics are summarized as median with range, mean with standard deviation, or percentage. They were compared using an unpaired t-test or Chi-square statistic, as appropriate. Owing to skewed distributions and the lack of consensus on cut-off points for discriminating abnormalities, PGRN levels were categorized in quartiles. Overall survival (OS) was measured from the date of surgery to the day of confirmed death from breast cancer, or was censored at the last follow-up. Patients who died of other causes were censored at the date of death. For the purpose of illustration, estimates of time to death stratified by quartiles of the PGRN were displayed using Kaplan–Meier curves. These estimates were analyzed using the Log rank test for trends. To adjust for possible confounding effects of prognostic factors, we constructed a Cox proportional hazards regression model, and estimated adjusted hazard ratios with 95% confidence intervals (CI). All statistical analyses were performed using the SPSS 25.0 software package (IBM SPSS Statistics, USA). A two-sided p-value < 0.05 was considered statistically significant.
Results
Patient Characteristics
Baseline participant characteristics have been previously described.13 A total of 695 patients were analyzed in this long-term follow-up study. Their mean age ± standard deviation (SD) at surgery was 45 ± 10 years. There were 210 (30%) postmenopausal women (Table 1). There were no significant differences in age, tumor size, positive lymph nodes, or BMI between HR-positive and HR-negative groups. All patients with HR-positive tumors received adjuvant tamoxifen therapy.
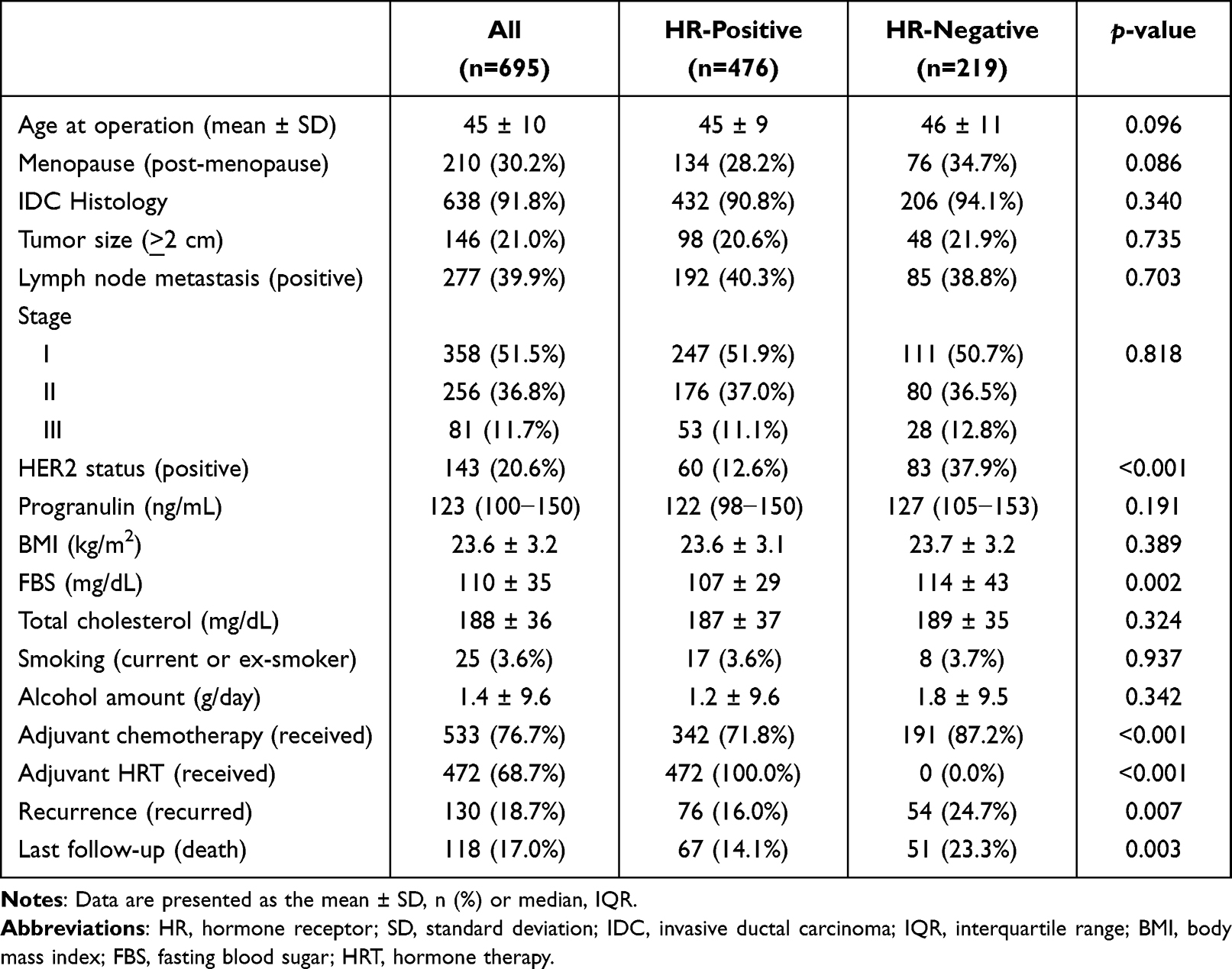 |
Table 1 Baseline Characteristics of Participants According to Their Hormone Receptor Status |
Survival Outcomes According to Hormonal Status and Stage
The median follow-up duration of 577 surviving patients was 12.7 years (interquartile range [IQR]: 8.8 − 15.7) years; maximum: 19.0 years). During 94,444 person-years of follow-up, 118 breast cancer-specific deaths occurred, with a mortality rate of 12.6 (95% CI: 10.1 − 15.1) per 104 person-years. In all cohort, (10, 15, and 20)-year OS rates were 87.9% (95% CI: 85.5 − 90.3), 79.1% (95% CI: 76.1 − 82.1), and 74.0% (95% CI: 70.7 − 77.3), respectively (Figure 1A). According to the HR status, (10, 15, and 20)-year OS rates were 91.4% (95% CI: 88.9 − 93.9), 81.1% (95% CI: 77.6 − 84.6), and 75.9% (95% CI: 72.1 − 79.7) in HR-positive patients, and 76.5% (95% CI: 70.9 − 82.1), 74.2% (95% CI: 68.4 − 80.0), and 69.8% (95% CI: 63.7 − 75.9) in HR-negative patients, respectively (p = 0.003; Figure 1B; Supplemental Table 1). There were significant differences in OS according to breast cancer stage, regardless of HR-positive or negative (Figure 2; all p < 0.001). In the HR-negative group, almost all mortality events occurred up to 10 years after surgery, then the OS curve was stagnant. However, in the HR-positive group, death events were rarely observed until 5-years after surgery; then they steadily increased until 20 years after surgery.
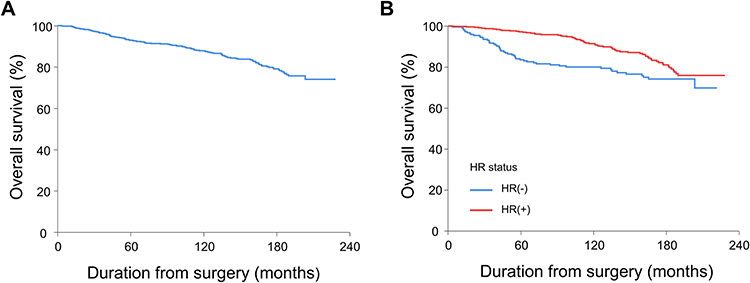 |
Figure 1 Overall survival of (A) all patients, and (B) according to hormone receptor status. |
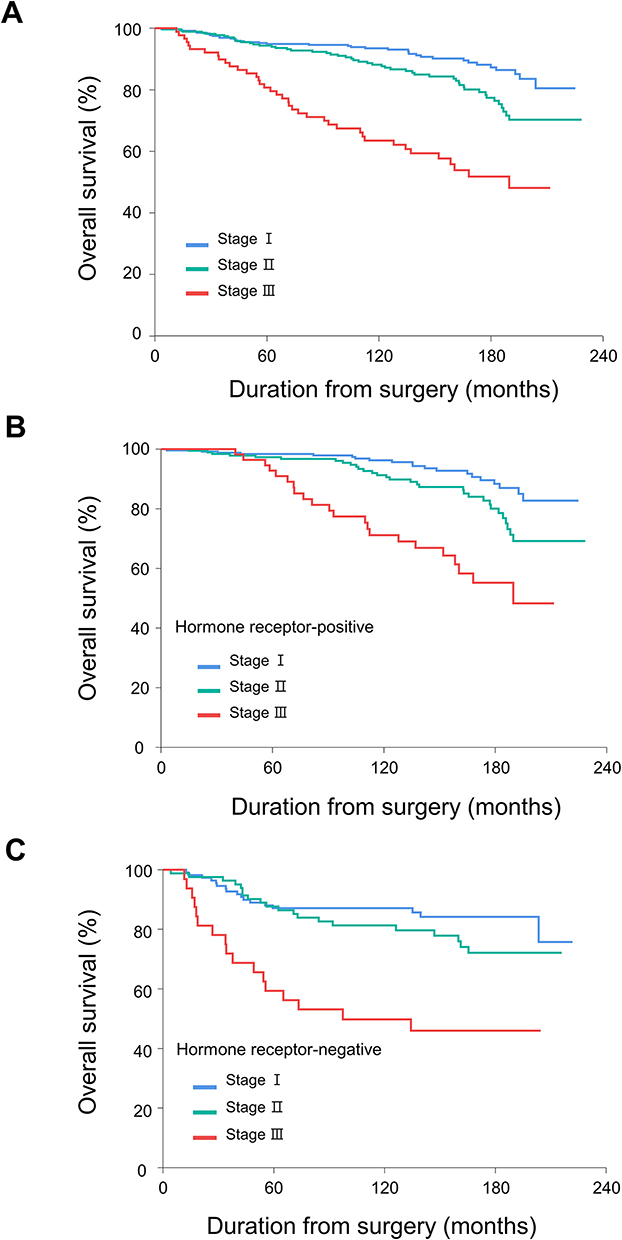 |
Figure 2 Overall survival according to cancer stage in (A) all, (B) hormone receptor-positive, and (C) hormone receptor-negative patients. |
Progranulin Levels are Significantly Associated with Mortality
The median level of pre-operative PGRN was 121 ng/mL (IQR: (98−147) ng/mL). A higher level of PGRN was associated with an increased risk of breast cancer mortality. The statistical significance of PGRN was observed in all cohorts and in the HR-positive group (Table 2 and Figure 3; Supplemental Table 2). However, it was not observed in the HR-negative group. After adjusting for age, histology, tumor size, lymph node metastasis, and adjuvant chemotherapy, higher PGRN had a significant association with an increased risk of death in the HR-positive group (model 2; p for trend = 0.005). After further adjusting for metabolic confounders including body mass index, fasting blood sugar, diastolic blood pressure, total cholesterol, smoking, and alcohol amount in model 2, higher PGRN still showed a significant association with an increased risk of death in the HR-positive group (model 3; p for trend = 0.003).
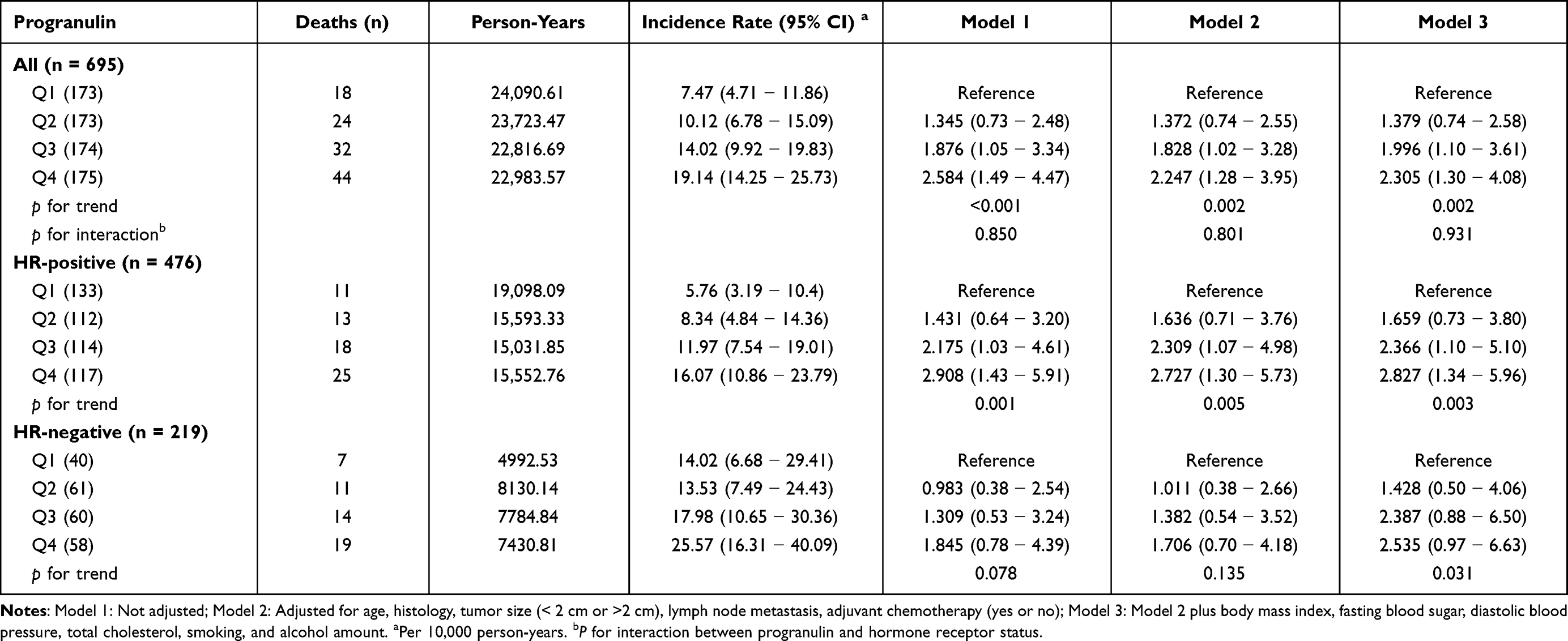 |
Table 2 Hazard Ratios and 95% Confidence Intervals for Breast Cancer Mortality According to Progranulin Levels in Quartiles |
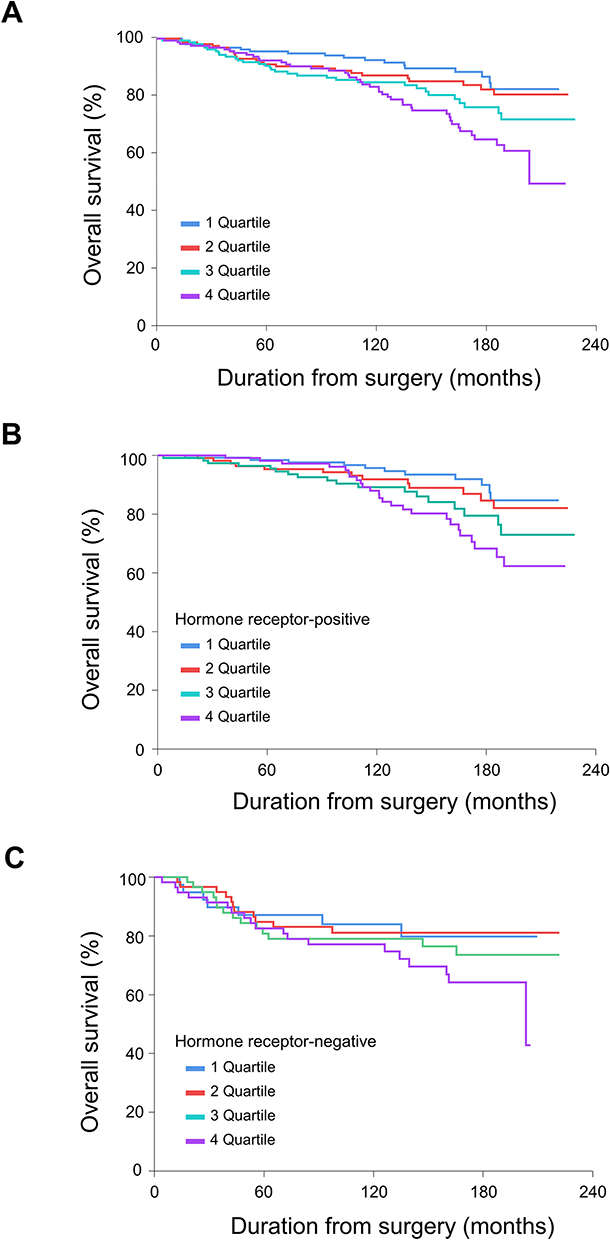 |
Figure 3 Overall survival according to progranulin levels in quartiles in (A) all, (B) hormone receptor-positive, and (C) hormone receptor-negative patients. |
In the HR-positive group, adjusted hazard ratios (95% CI) for deaths in the second-quartile (Q2), third-quartile (Q3), and fourth-quartile (Q4), compared to the first-quartile (Q1), were 1.66 (0.73 − 3.80), 2.37 (1.10 − 5.10), and 2.83 (1.34 − 5.96), respectively (model 3). Hazard ratios for PGRN quartiles suggest a dose–response relationship, with the highest quartile having the highest hazard ratio for OS in the HR-positive group in all models (4Q vs 1Q: 10-year OS, (88.0 vs 95.7) %; 15-year OS, (68.3 vs 90.0) %; 20-year OS, (62.3 vs 84.8) %; hazard ratio: (2.73 − 2.91). The highest quartile of PGRN in the HR-negative group also had the worst OS rate in the long-term follow-up data, although there was no statistical significance in the entire quartile. It was noteworthy that after adjusting for various confounders in model 3 (p for trend = 0.031; Table 2), higher PGRN showed a significant association with an increased risk of death in the HR-negative group.
Furthermore, receiver operating characteristics (ROC) curve analysis was conducted to determine the best cut-off value of progranulin to separate HR-positive breast cancer patients into death and survival groups. The results of ROC curve analysis revealed that the optimal cut-off value of serum progranulin was 130 ng/mL for dead patients, with a sensitivity of 61.2% and a specificity of 60.6% (area under the curve: 0.595; 95% CI: 0.52 − 0.67; p = 0.013). The HR-positive group was then categorized by combining PGRN level and breast cancer stage (Figure 4; Supplemental Table 3). For patients with stage II/III, those with higher PGRN levels had significantly worse OS than those with lower PGRN levels (10-year OS: (81.7 vs 89.5) %; 15-year OS: (63.1 vs 81.4) %; 20-year OS: (48.0 vs 77.0) %; hazard ratio: 2.33 [95% CI, 1.31 − 4.17]; p = 0.003).
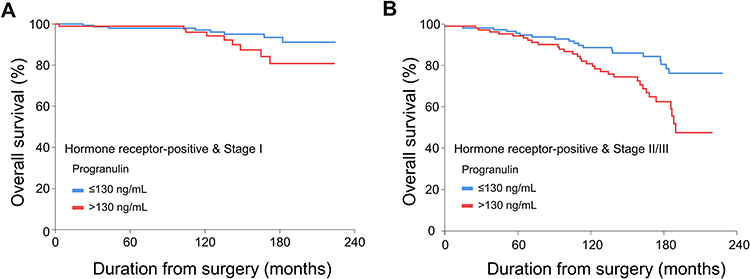 |
Figure 4 Overall survival of hormone receptor-positive patients according to the optimal cut-off value of serum progranulin at 130 ng/mL in (A) stage I, and (B) stage II/III. |
Discussion
With a long-term follow-up for a cohort of patients with early breast cancer, the mortality of HR-positive breast cancers was not much different from that of HR-negative tumors over 15−20 years. Preoperative serum PGRN was significantly associated with the risk of breast cancer mortality, especially for those with HR-positive tumors, even after adjusting for possible clinical prognostic factors that included tumor and metabolic confounders. This association between PGRN and breast cancer mortality showed a dose–response relationship.
A representative biomarker associated with breast cancer prognosis is a molecular-based subtype, mainly a tissue-based classification.17 Biomarkers currently play an essential role in managing patients with invasive breast cancer, especially in deciding the type of systemic therapy to be administered. For predicting response to endocrine treatment, both ER and PR are measured to define HR-positive tumors. On the other hand, HER2 expression or gene copy number should be determined to select patients to receive anti-HER2 therapy.18 However, few serum biomarkers for breast cancer prognosis have been suggested.
PGRN can stimulate the proliferation of mesenchymal and epithelial cells by activating different kinase pathways, such as mitogen-activated protein (MAP) kinase, phosphatidylinositol 3′-kinase (PI3K), and focal adhesion kinase pathways.10,19 PGRN overexpression is associated with several drug resistance mechanisms in breast cancer cells, especially ER-signaling pathways, such as letrozole resistance to aromatase overexpressing cells, and tamoxifen resistance in MCF7 cells.20,21 A recent study using prospectively collected serum PGRN has shown that PGRN levels are significantly associated with treatment response, disease progression, and survival in metastatic breast cancer.22 In addition, in vitro and in vivo studies have reported that anti-progranulin antibodies can inhibit the proliferation and migration of breast cancer cells, and PGRN is a therapeutic target of breast cancer.23
After 5 years of adjuvant endocrine therapy, breast-cancer recurrences continued to occur steadily throughout the study period from 5 to 20 years.6 Sequential endocrine therapy with tamoxifen for 2−3 years, followed by letrozole for 5 years, should be considered as one of the optimal standard endocrine treatments for postmenopausal patients with hormone receptor-positive breast cancer.24 However, extending hormone therapy by 5-years in addition to 5 years of adjuvant endocrine therapy provided no benefit over a 2-year extension, but was associated with a greater risk of bone fracture.25 Therefore, decisions regarding extended aromatase-inhibitor therapy will continue to be individualized, with a combined assessment of recurrence risk, treatment tolerance, and patient preference.26
Recent guidelines recommend that adjuvant treatment (either endocrine therapy alone, or chemoendocrine therapy) for patients with HR-positive breast cancer should be determined using biomarkers, such as Oncotype DX scores.27 This Oncotype DX is required for patient selection to avoid unnecessary cytotoxic chemotherapy for patients with good prognosis. However, the Oncotype DX is not available in all institutions or countries. Thus, biomarkers that are easily accessible and cost-effective need to be developed.
Meanwhile, it is necessary to find a subgroup of patients with HR-positive tumors who have poor prognosis, and require long-term adjuvant endocrine therapy for up to 10 years.28 If serum biomarkers could be combined with clinicopathological prognostic factors, it would help predict high-risk groups. When PGRN level and stage were combined, stage II/III patients with high PGRN levels had significantly poorer OS than those with low PGRN levels. Furthermore, patients with high PGRN/stage I and those with low PGRN/stage II/III had similar long-term survival outcomes (15-year OS: (80.8 vs 81.4) %). These results suggest that higher PGRN level was significantly associated with poor long-term OS in patients with HR-positive breast cancer. It would be better to consider extended adjuvant endocrine therapy up to 15 years or more for stage II/III patients with high PGRN levels.
Our results confirmed that PGRN levels were significantly correlated with both the recurrence rate, and the mortality rate of HR-positive breast cancer patients after long-term follow-up. Such association between PGRN and mortality was still significant, even after adjusting for well-known prognostic factors, such as age, histology, tumor size, lymph node metastasis, adjuvant chemotherapy, and representative metabolic parameters. Anti-PGRN antibody is under development. It has recently been reported that blocking PGRN with antibody therapy could inhibit tumor growth of some types of breast cancer cells in vivo.23 Therefore, PGRN might provide novel-targeted solutions for treating breast cancer.
This study has several limitations. HER2 status, another important prognostic factor, was not considered, because HER2 was not routinely evaluated at the time of recruitment. Cancer recurrence was not evaluated either, since the national reimbursement program was only provided for up to 5 years after surgery, without implementing surveillance. In addition, the statistical significance of PGRN level in all breast cancers was probably because HR-positive tumors accounted for the majority. The insignificance of PGRN level in HR-negative tumors might be due to our small sample size. Thus, further studies enrolling more patients are needed.
However, this study also has several strengths. First, our cohort comprised a considerable number of patients with homogeneous characteristics in terms of Asian ethnicity, invasive ductal carcinoma histology, and administration of adjuvant tamoxifen treatment to all HR-positive patients. Second, several factors related to both the tumor, and metabolic syndrome, were investigated and adjusted. Finally, the prognostic role of a serum biomarker was evaluated using data after long-term follow-up of about 13 years.
Conclusion
This study showed that preoperative serum PGRN levels had clinical significance for predicting cancer mortality in patients with HR-positive breast cancer. Further studies are needed to validate the prognostic value of PGRN level and potential treatment strategies for breast cancer patients.
Data Sharing Statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available, due to the issue of patient privacy.
Ethics Approval and Consent to Participate
This study protocol was approved by the Institutional Review Board of the National Cancer Center, Republic of Korea (IRB Protocol No. NCCNCS-09-220) and complied with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Acknowledgments
The authors thank the participants and their families, and all investigators and site personnel. D.-H. K. and K. S. L. contributed equally to this work as co-first authors. C.-Y. P. and S. W. O. contributed equally to this work as co-corresponding authors.
Funding
There is no funding to report.
Disclosure
Dr. Keun Seok Lee has consulting or advisory role for AstraZeneca, Eisai, Lilly, Merck, Novartis, Pfizer, Everest Medicine, Bixink, Daiichi Sankyo, and Roche; has received research funding from Novartis; has received research drug supply from Dong-A ST. The authors declare that they have no other competing interests.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Jung KW, Won YJ, Hong S, Kong HJ, Lee ES. Prediction of cancer incidence and mortality in Korea, 2020. Cancer Res Treat. 2020;52(2):351–358. doi:10.4143/crt.2020.203
3. DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA. 2019;69(6):438–451. doi:10.3322/caac.21583
4. Coates AS, Winer EP, Goldhirsch A, et al. Tailoring therapies--improving the management of early breast cancer: st Gallen International expert consensus on the primary therapy of early breast cancer 2015. Ann Oncol. 2015;26(8):1533–1546. doi:10.1093/annonc/mdv221
5. Sparano JA, Gray RJ, Makower DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. 2018;379(2):111–121. doi:10.1056/NEJMoa1804710
6. Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377(19):1836–1846. doi:10.1056/NEJMoa1701830
7. Bae SY, Kim S, Lee JH, et al. Poor prognosis of single hormone receptor- positive breast cancer: similar outcome as triple-negative breast cancer. BMC Cancer. 2015;15(1):138. doi:10.1186/s12885-015-1121-4
8. Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381(9869):805–816. doi:10.1016/S0140-6736(12)61963-1
9. Goss PE, Ingle JN, Pritchard KI, et al. Extending aromatase-inhibitor adjuvant therapy to 10 years. N Engl J Med. 2016;375(3):209–219. doi:10.1056/NEJMoa1604700
10. Serrero G. Autocrine growth factor revisited: PC-cell-derived growth factor (progranulin), a critical player in breast cancer tumorigenesis. Biochem Biophys Res Commun. 2003;308(3):409–413. doi:10.1016/S0006-291X(03)01452-9
11. Nguyen AD, Nguyen TA, Martens LH, Mitic LL, Farese RV
12. Arechavaleta-Velasco F, Perez-Juarez CE, Gerton GL, Diaz-Cueto L. Progranulin and its biological effects in cancer. Med Oncol. 2017;34(12):194. doi:10.1007/s12032-017-1054-7
13. Koo DH, Park CY, Lee ES, Ro J, Oh SW. Progranulin as a prognostic biomarker for breast cancer recurrence in patients who had hormone receptor-positive tumors: a cohort study. PLoS One. 2012;7(6):e39880. doi:10.1371/journal.pone.0039880
14. Song YM, Sung J. Body mass index and mortality: a twelve-year prospective study in Korea. Epidemiology. 2001;12(2):173–179. doi:10.1097/00001648-200103000-00008
15. Youn BS, Bang SI, Kloting N, et al. Serum progranulin concentrations may be associated with macrophage infiltration into omental adipose tissue. Diabetes. 2009;58(3):627–636. doi:10.2337/db08-1147
16. Wells CA, Sloane JP, Coleman D, et al. Consistency of staining and reporting of oestrogen receptor immunocytochemistry within the European Union--an inter-laboratory study. Virchows Arch. 2004;445(2):119–128. doi:10.1007/s00428-004-1063-8
17. Perou CM, Sorlie T, Eisen MB, et al. Molecular portraits of human breast tumours. Nature. 2000;406(6797):747–752. doi:10.1038/35021093
18. Duffy MJ, Harbeck N, Nap M, et al. Clinical use of biomarkers in breast cancer: updated guidelines from the European Group on Tumor Markers (EGTM). Eur J Cancer. 2017;75:284–298. doi:10.1016/j.ejca.2017.01.017
19. Bateman A, Bennett HP. The granulin gene family: from cancer to dementia. BioEssays. 2009;31(11):1245–1254. doi:10.1002/bies.200900086
20. Abrhale T, Brodie A, Sabnis G, et al. GP88 (PC-cell derived growth factor, progranulin) stimulates proliferation and confers letrozole resistance to aromatase overexpressing breast cancer cells. BMC Cancer. 2011;11:231. doi:10.1186/1471-2407-11-231
21. Tangkeangsirisin W, Hayashi J, Serrero G. PC cell-derived growth factor mediates tamoxifen resistance and promotes tumor growth of human breast cancer cells. Cancer Res. 2004;64(5):1737–1743. doi:10.1158/0008-5472.CAN-03-2364
22. Tkaczuk KHR, Hawkins D, Yue B, Hicks D, Tait N, Serrero G. Association of serum progranulin levels with disease progression, therapy response and survival in patients with metastatic breast cancer. Clin Breast Cancer. 2020;20(3):220–227. doi:10.1016/j.clbc.2019.11.010
23. Guha R, Yue B, Dong J, Banerjee A, Serrero G. Anti-progranulin/GP88 antibody AG01 inhibits triple negative breast cancer cell proliferation and migration. Breast Cancer Res Treat. 2021;186(3):637–653. doi:10.1007/s10549-021-06120-y
24. Del Mastro L, Mansutti M, Bisagni G, et al. Extended therapy with letrozole as adjuvant treatment of postmenopausal patients with early-stage breast cancer: a multicentre, open-label, randomised, Phase 3 trial. Lancet Oncol. 2021;22(10):1458–1467. doi:10.1016/S1470-2045(21)00352-1
25. Gnant M, Fitzal F, Rinnerthaler G, et al. Duration of adjuvant aromatase-inhibitor therapy in postmenopausal breast cancer. N Engl J Med. 2021;385(5):395–405. doi:10.1056/NEJMoa2104162
26. Goodwin PJ. Extended aromatase inhibitors in hormone-receptor-positive breast cancer. N Engl J Med. 2021;385(5):462–463. doi:10.1056/NEJMe2109356
27. Andre F, Ismaila N, Henry NL, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: ASCO clinical practice guideline update-integration of results from TAILORx. J Clin Oncol. 2019;37(22):1956–1964. doi:10.1200/JCO.19.00945
28. Burstein HJ, Lacchetti C, Anderson H, et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J Clin Oncol. 2019;37(5):423–438. doi:10.1200/JCO.18.01160
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.