")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Prognostic Value of the Leuko-Glycemic Index in Acute Myocardial Infarction Patients with or without Diabetes
Authors Qi LY, Liu HX, Cheng LC, Luo Y, Yang SQ, Chen X, Cai L
Received 12 January 2022
Accepted for publication 12 May 2022
Published 9 June 2022 Volume 2022:15 Pages 1725—1736
DOI https://doi.org/10.2147/DMSO.S356461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Ling-Yao Qi, Han-Xiong Liu, Lian-Chao Cheng, Yan Luo, Si-Qi Yang, Xu Chen, Lin Cai
Department of Cardiology, The Third People’s Hospital of Chengdu Affiliated Hospital of Southwest Jiaotong University, Chengdu, People’s Republic of China
Correspondence: Lin Cai, Department of Cardiology, The Third People’s Hospital of Chengdu Affiliated Hospital of Southwest Jiaotong University, 82 Qinglong St, Chengdu, Sichuan, People’s Republic of China, Tel/Fax +86 28-67575956, Email [email protected]
Purpose: The leuko-glycaemic index (LGI) is an index that combines white blood cell count and blood glucose and could be a marker of systemic inflammatory response syndrome. The prognostic value of the LGI in acute myocardial infarction (AMI) is still unclear. We aimed to investigate the prognostic value of the LGI for short- and long-term prognosis in AMI patients with different diabetic status.
Patients and Methods: This was an observational, multicenter study involving 1256 AMI patients admitted in 11 hospitals between March 2014 and June 2019 in Chengdu. White blood cell count and blood glucose were measured on admission. The LGI was calculated by multiplying both values and dividing them by a thousand. Logistic regression was used to explore the predictive value of LGI in in-hospital mortality. Receiver operating characteristic curve was used to determine the optimal cut-off values of the LGI to predict in-hospital mortality. The patients were classified into diabetic and non-diabetic groups and further divided into higher and lower LGI subgroups according to the optimal cut-off values. The endpoints were all-cause mortality during the hospitalization and major adverse cardiovascular and cerebrovascular events (MACCE) during follow-up, including all-cause mortality, non-fatal myocardial infarction, vessel revascularization and non-fatal stroke.
Results: LGI was an independent predictor of all-cause mortality during the hospitalization in non-diabetics, but not in diabetics. The optimal cut-off values of diabetics and non-diabetics were 3593 mg/dl. mm3 and 1402 mg/dl. mm3, respectively. Whether diabetics or not, in-hospital mortality was higher in the higher LGI subgroup (p-value < 0.001). And in the follow-up of 15 months (9 months, 22 months), we observed 99 (8.6%), 6 (0.5%), 54 (4.7%) and 29 (2.5%) cases of death, non-fatal MI, revascularization and non-fatal stroke, respectively. The cumulative incidence of MACCE during follow-up was higher in the higher LGI subgroup, both in the diabetics and non-diabetics (p-value < 0.05). In non-diabetics, higher LGI was an independent predictor of MACCE.
Conclusion: LGI was an independent predictor for short- and long-term prognosis in AMI patients without diabetes, but had no prognostic value for short- and long-term prognosis of AMI patients with diabetes.
Keywords: acute myocardial infarction, prediction, leuko-glycemic index, in-hospital mortality, long-term prognosis
Introduction
Cardiovascular diseases have been the leading cause of death worldwide. Acute myocardial infarction (AMI) is one of the most serious and harmful cardiovascular diseases with acute onset, rapid development, multiple complications, high mortality rate, and poor prognosis. Although the incidence of AMI in developed countries has decreased, it remains high in developing countries.1 Using scoring systems, risk stratification is beneficial for rapid identification of high-risk patients, strengthening treatment strategies and prognostication, which are essential for improving patient outcomes. Examples of scoring systems include the Thrombolysis in Myocardial Infarction (TIMI) score and Global Registry of Acute Cardiac Events (GRACE) score. However, the current myocardial infarction (MI) risk scoring system is unable to detect the state of human inflammatory response.2
Inflammation is a major trigger for the development of atherosclerosis. It has been proven that various inflammatory cells and factors are involved in the overall pathogenesis of AMI.3 With the activation and accelerated rate of inflammation, inflammatory markers of AMI can reflect the pathophysiological state of the body.4,5 However, most inflammatory markers are expensive and not readily available, limiting their use in clinical practice and making them unsuitable for risk stratification on admission. The leuko-glycemic index (LGI) was first proposed in 2010 by Quiroga Castro et al, who suggested that LGI could be a useful tool for risk stratification in ST-elevation myocardial infarction (STEMI) patients on admission.6 The LGI contains two readily accessible indicators: leukocyte count and blood glucose level on admission. White blood cell counts are part routine analysis of all hospitalized patients and are readily available but receive little attention. Blood glucose level on admission is an important prognostic factor for patients with AMI.7,8 Studies have shown that LGI may be a marker of systemic inflammatory response and a good predictor of adverse outcomes in various situations in critical care medicine, such as MI and stroke.6,9–13
Previous studies have pointed out that LGI has a good prognostic value in predicting the outcomes of AMI patients. However, there are no relevant studies including the Asian population, and the ideal cut-off value of LGI for the prognostication of AMI patients has not been determined. Previous studies used different grouping methods but did not distinguish between diabetic and non-diabetic patients; therefore, the prognostic value of LGI for AMI patients with different blood glucose levels is still unclear. This study was the first to be conducted in patients with AMI in Asia, and different thresholds for diabetic and non-diabetic patients were used to discuss the prognostic value of LGI in patients with AMI.
Patients and Methods
Study Design and Population
This was an observational, multicenter cohort study. We observed 1256 AMI patients admitted in 11 general hospitals between March 2014 and June 2019 in the city of Chengdu, China. AMI was diagnosed according to current guidelines,14 including STEMI and non-ST-elevation myocardial infarction (NSTEMI). Patients with the following baseline characteristics were excluded: (1) age < 18 years; (2) no available data on leukocytes and plasma glucose on admission; (3) lost to follow-up; (4) severe valvular heart disease; (5) severe congenital heart disease; (6) decompensated heart failure; or (7) malignancies.
The present study complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Third People’s Hospital of Chengdu. The study was registered in the Chinese Clinical Trials Registry in China (http://www.medresman.org, ChiCTR1900025138).
The patients were divided into two groups: diabetic and non-diabetic, according to their discharge diagnosis. Diabetic patients included those with a history of diabetes or who were newly diagnosed with diabetes using the oral glucose tolerance test, fasting glucose test, or Glycated hemoglobin (HbA1c) ≥ 6.5% during hospitalization.15
Both white blood cell count and blood glucose levels were measured in the peripheral blood samples taken at admission. White blood cell count was expressed in cells per mm3 and blood glucose level in mg/dl. The LGI was calculated by multiplying both values and dividing them by one thousand and was expressed in mg/dl mm3.6 Receiver operating characteristic (ROC) curves showed that the optimal critical values of LGI for predicting in-hospital mortality in patients with or without diabetes were 3593 mg/dl. mm3 (area under the ROC curve 0.679; sensitivity, 53.6%; specificity, 85.9%; P-value = 0.002; Figure 1A) and 1402 mg/dl. mm3 (area under the ROC curve 0.730; sensitivity, 66.2%; specificity, 69.5%; P-value < 0.001; Figure 1B), respectively. Both groups were further divided into the higher LGI and lower LGI subgroups.
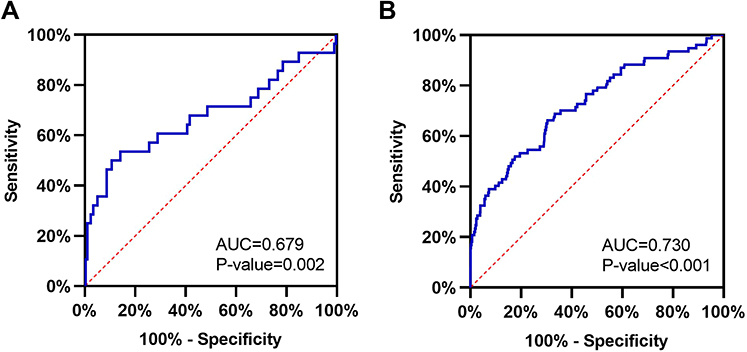 |
Figure 1 (A) The receiver operating characteristic (ROC) curve of leuko-glycemic index (LGI) to predict in-hospital mortality for AMI patients with diabetes. (B) The receiver operating characteristic (ROC) curve of leuko-glycemic index (LGI) to predict in-hospital mortality for AMI patients without diabetes. |
Endpoint and Follow-Up
The endpoints were all-cause mortality during the hospitalization and major adverse cardiovascular and cerebrovascular events (MACCE) during follow-up, including all-cause mortality, non-fatal myocardial infarction (MI), vessel revascularization and non-fatal stroke. MI was defined as newly developed Q wave, raised CK-MB, Tn-I or T above the normal ranges, typical ischemic symptom with accompanied ST elevation. Revascularization was defined as the revascularization of any lesion, including percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). And stroke was defined as a new cerebral infarction or cerebral hemorrhage diagnosed by neurologists.
Follow-up was done as outpatient, rehospitalization, or telephone follow-up 1 month after discharge, then at 6, and 12 months, and annually thereafter. In-hospital mortalities were obtained from the hospital records, and MACCEs during follow-up were obtained from the hospital records or via contact with the patients’ guardians. Trained physicians collected the baseline and follow-up data.
Statistical Analysis
SPSS software version 26.0 was used in the statistical analysis. All the continuous variables were tested for normality. Continuous variables were compared using the Mann–Whitney U-test and expressed as median (interquartile range [IQR]). Categorical variables were compared using the chi-squared test and were presented as counts and percentages. The associations between the LGI and the in-hospital mortality were evaluated using univariate and multivariate logistic regression analysis. The optimal cut-off value for LGI to predict in-hospital mortality was determined using the Youden index in the ROC curve. The Youden index is equal to the sum of sensitivity and specificity minus 1. Then, the optimal cut-off point for LGI is the LGI value that corresponds to the maximum Youden index. The cumulative incidence of MACCE during follow-up was calculated using the Kaplan–Meier curve method, and comparisons between the subgroups were performed using the Log rank test. The associations between the LGI and MACCE were evaluated using univariate and multivariate Cox regression analysis. Variables with statistical significance in univariate analysis (P<0.05) and variables of known prognostic importance were included in multivariate regression analysis. A two-sided p-value <0.05 was considered statistically significant in all analyses.
Results
Baseline Characteristics
A total of 1256 AMI patients (873 STEMI and 383 NSTEMI) were included in the study, among which 74.0% (930/1256) were males and 26.0% (383/1256) were females. The baseline characteristics and angiographic findings are listed in Table 1. In the diabetics, patients were older, included more females, with a higher prevalence of CAD, history of PCI, hypertension and multiple coronary arteries lesion, and had higher serum creatinine and triglyceride (p-value <0.05). However, the proportions of current smoker and STEMI were lower than that of non-diabetics (p-value <0.05).
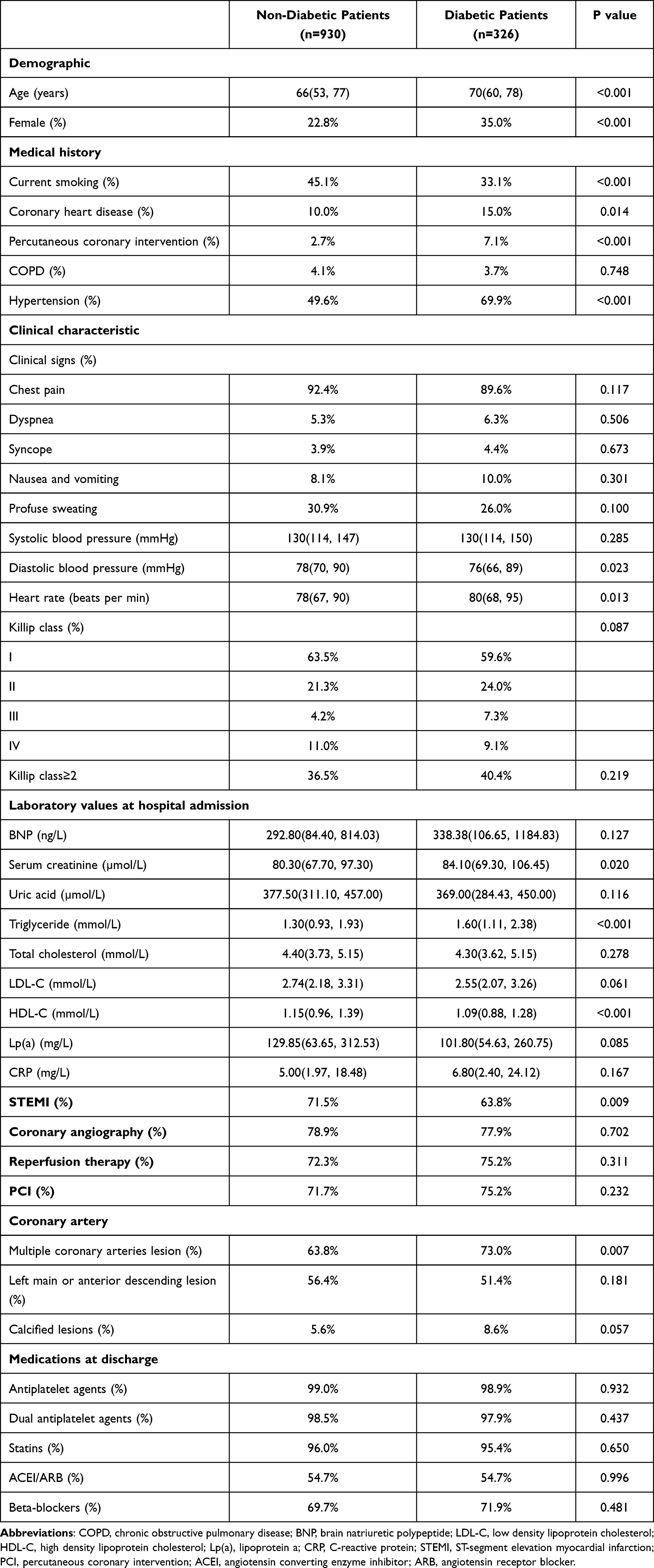 |
Table 1 Baseline Characteristics |
For the diabetic group, the higher LGI subgroup had an LGI ≥ 3593 mg/dl. mm3 (n = 57), and the lower LGI subgroup had an LGI < 3593 mg/dl. mm3 (n = 269). For the non-diabetic patients, the higher LGI subgroup had an LGI ≥ 1402 mg/dl. mm3 (n = 311), and lower LGI subgroup with LGI < 1402 mg/dl. mm3 (n = 619). The details are shown in Table 2. In the diabetic group, the higher LGI subgroup had more females, a higher Killip grade, higher serum creatinine levels, higher uric acid levels, higher total cholesterol levels, and higher low-density lipoprotein cholesterol (LDL-C) levels than those in the lower LGI subgroup (p-value < 0.05). In the non-diabetic group, the higher LGI subgroup had a higher incidence of nausea and vomiting and profuse sweating, lower blood pressure, faster heart rate, higher Killip grade, higher total cholesterol levels, higher LDL-C levels, higher C-reactive protein (CRP) levels, more coronary calcifications, and more STEMI than the lower LGI subgroup (p-value < 0.05).
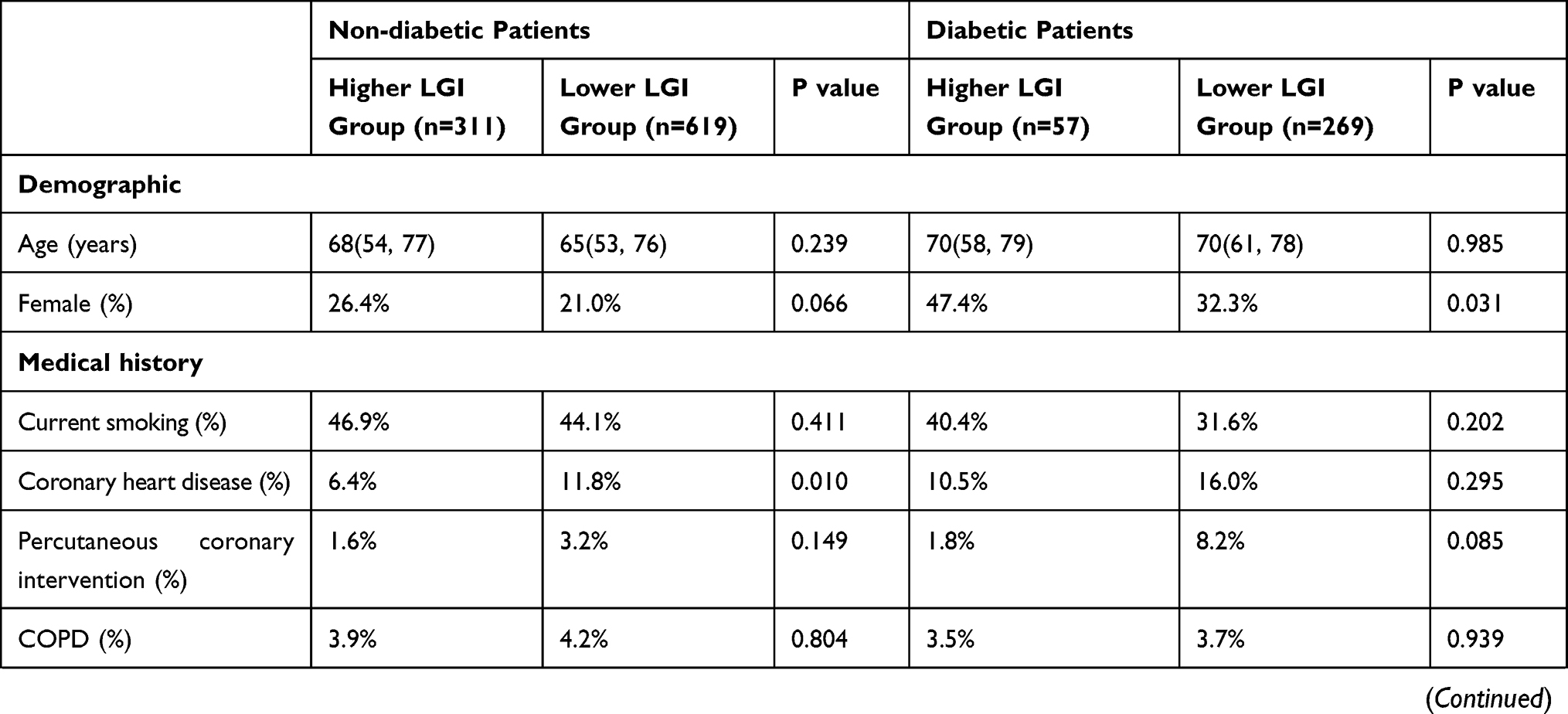 | 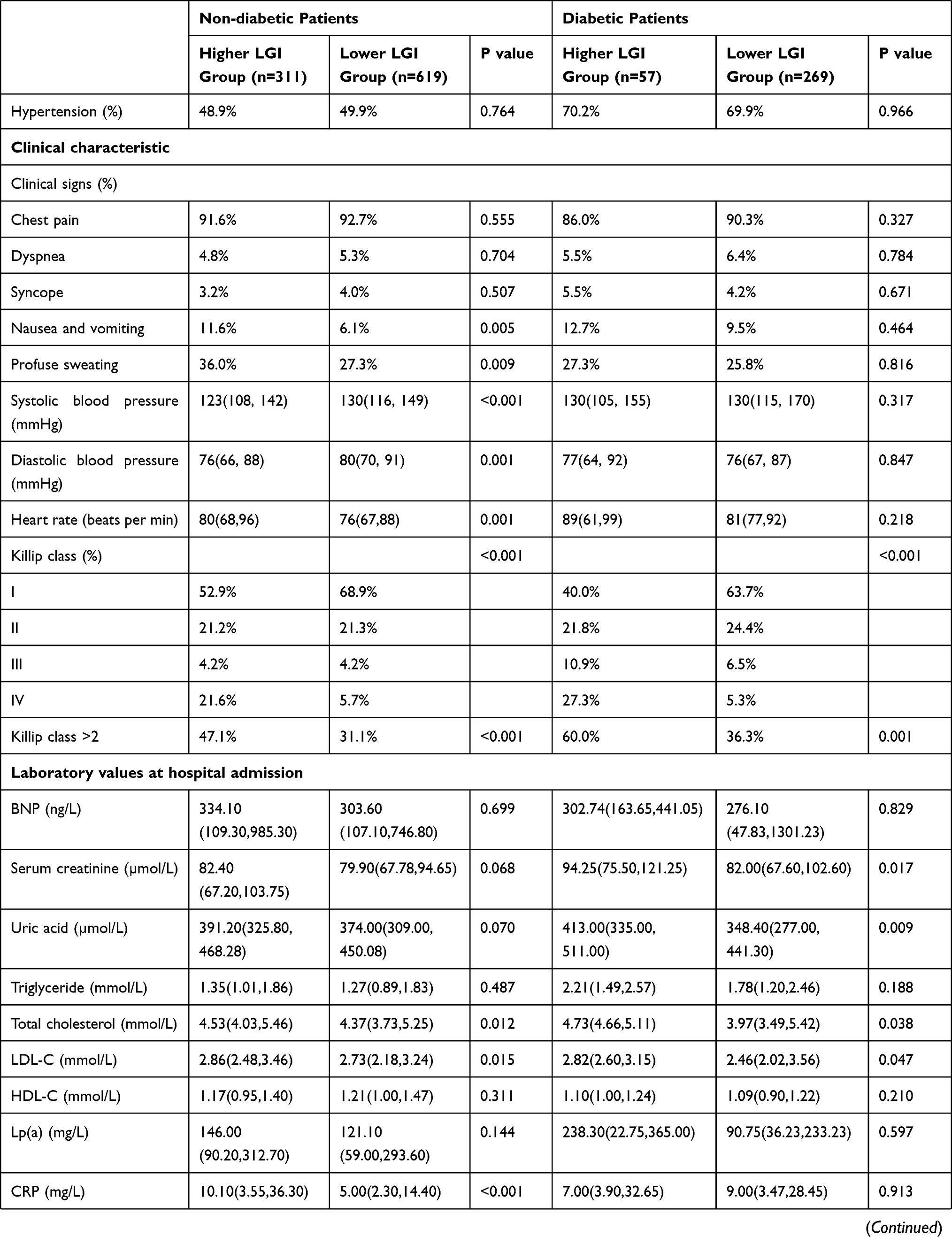 | 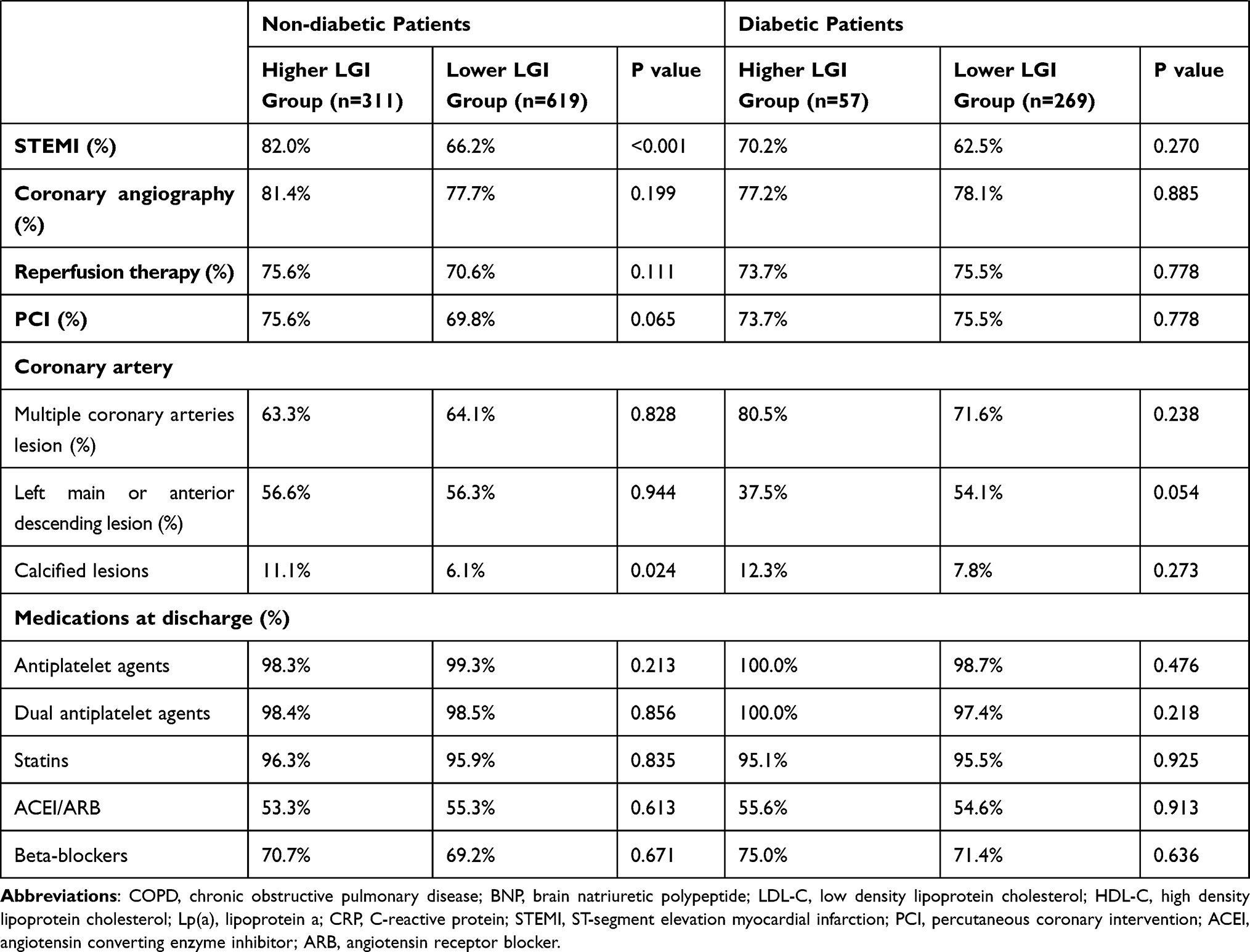 |
Table 2 Baseline Characteristics of Patients with Different LGI Levels |
Clinical Outcomes During Hospitalization
A total of 105 patients died in hospital. Multivariate logistic regression analysis showed that LGI was an independent predictor of all-cause mortality during the hospitalization in non-diabetic patients (p-value < 0.05; Table 3), but not an independent predictor in diabetic patients (p-value > 0.05; Table 3).
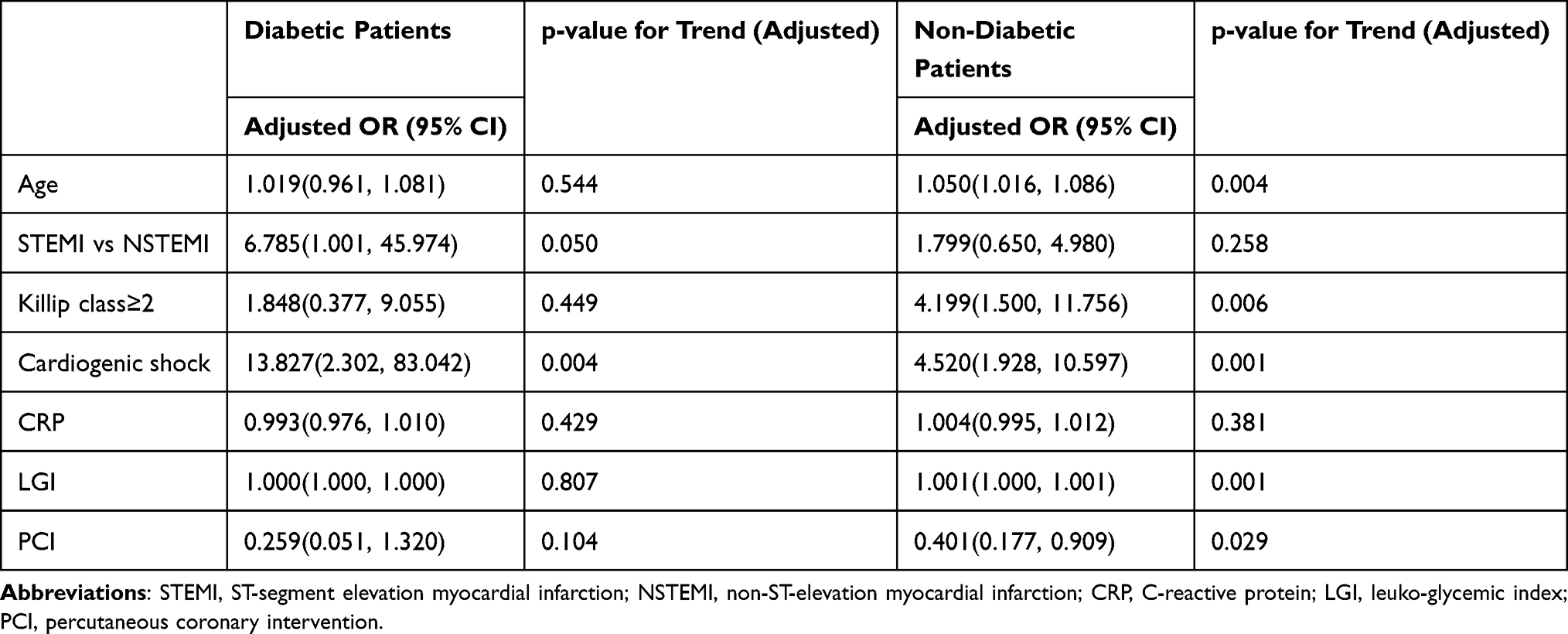 |
Table 3 Logistic Regression Analysis Results for in-Hospital Mortality |
The ROC curves are shown in Figure 1. The AUC of the LGI to predict in-hospital mortality in AMI patients with diabetes was 0.679 (95% CI: 0.551–0.807, p-value =0.002), and the optimal critical value of LGI was 3593 mg/dl. mm3 (sensitivity, 53.6%; specificity, 85.9%) (Figure 1A). The AUC of the LGI to predict in-hospital mortality in AMI patients without diabetes was 0.730 (95% CI: 0.666–0.794, p-value< 0.001), and the optimal critical value of LGI was 1402 mg/dl. mm3 (sensitivity, 66.2%; specificity, 69.5%) (Figure 1B).
In the diabetic group, the in-hospital mortality rate was significantly higher in the higher LGI subgroup (26.3% vs 4.8%, p-value < 0.001; Figure 2). And in the non-diabetic group, the in-hospital mortality rate was significantly higher in the higher LGI subgroup (16.4% vs 4.2%, p-value < 0.001; Figure 2).
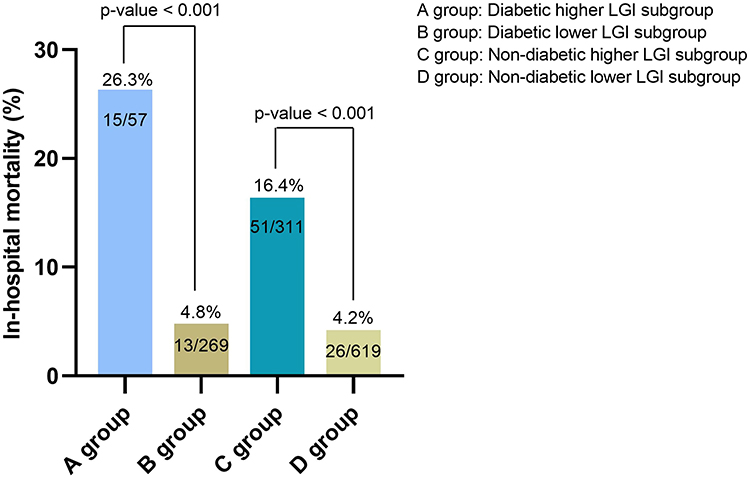 |
Figure 2 Comparison of in-hospital mortality between higher LGI subgroup and lower LGI subgroup. |
Clinical Outcomes at Follow-Up
At the 15 months (9 months, 22 months) follow-up, 99 (8.6%), 6 (0.5%), 54 (4.7%) and 29 (2.5%) cases of death, non-fatal MI, revascularization and non-fatal stroke occurred, respectively. The Kaplan-Meier survival curves showed that the cumulative incidence of MACCE was higher in the higher LGI subgroup, both in the diabetic patients and non-diabetic patients (p-value < 0.05) (Figure 3A and B).
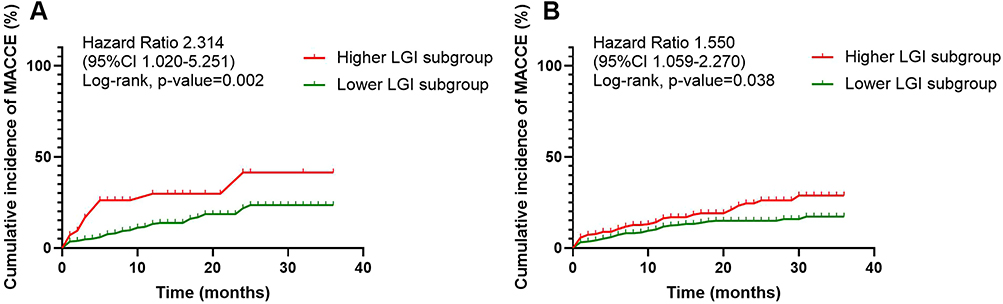 |
Figure 3 (A) The cumulative rate of MACCE on follow-up in AMI patients with diabetes. (B) The cumulative rate of MACCE on follow-up in AMI patients without diabetes. |
In the Multivariate Cox regression analysis of non-diabetic patients, the following factors were included: gender, age, STEMI, Killip classification, heart rate, C-reactive protein (CRP), brain natriuretic polypeptide (BNP), serum creatinine, uric acid, PCI and LGI (as categorical variable). The Cox regression analysis showed that the independent predictors of MACCE on follow-up were age, higher LGI and PCI (Table 4). And the above factors except CRP and BNP were included in the Multivariate Cox regression analysis of diabetic patients. The Cox regression analysis showed that the independent predictors of MACCE in diabetic patients were age and PCI (Table 4).
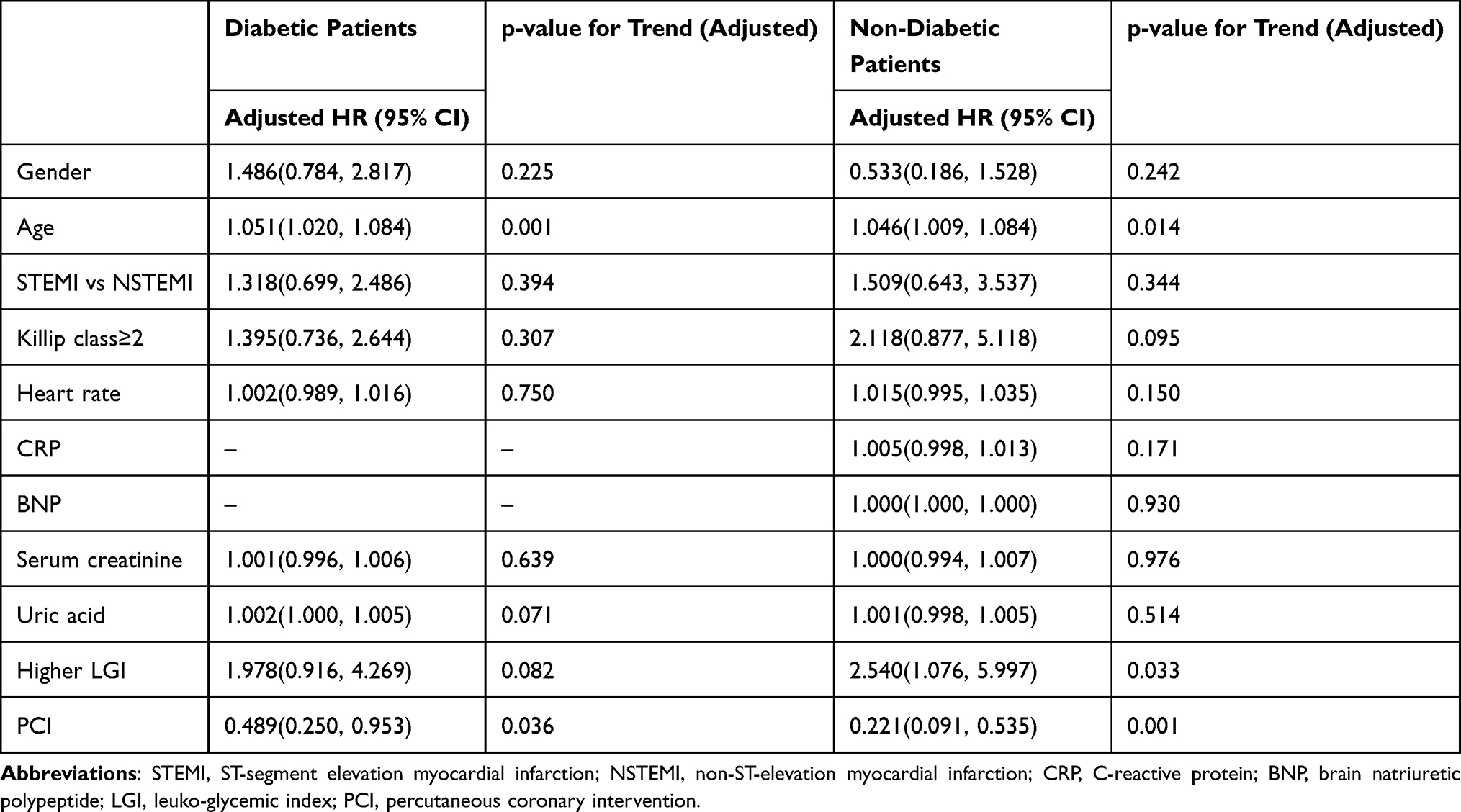 |
Table 4 Cox Regression Analysis Results for MACCE on Follow-Up |
Discussion
The purpose of this study was to analyze the prognostic value of LGI on the short- and long-term outcomes of AMI patients with and without diabetes. We found that LGI was not an independent predictor of all-cause mortality during the hospitalization or MACCE at follow up in patients with diabetes. For non-diabetic patients, LGI was an independent predictor of all-cause mortality during the hospitalization and MACCE at follow-up.
The LGI contains two accessible indicators: leukocyte count and blood glucose level on admission. Leukocytes are the main mediators of inflammation. An increase in leukocyte count reflects the inflammatory state of the body. The peripheral leukocyte count in patients with AMI is closely related to heart failure, cardiogenic shock, and death. Studies have shown that the leukocyte count is a predictor of mortality in patients with AMI, and a higher leukocyte count is associated with increased in-hospital or short-term mortality in AMI patients.16 The release of inflammatory mediators during a state of stress also affects glucose metabolism and promotes a hyperglycemic state.17 AMI patients often experience hyperglycemia, regardless of diabetes history.18 Acute hyperglycemia can enhance the inflammatory response.19 A previous study showed that there was a significant correlation between hyperglycemia and high leukocyte count on admission in patients with AMI.20 The risk of adverse outcomes in STEMI patients increased, suggesting that the outcomes caused by hyperglycemia on admission in AMI patients may be related to systemic inflammatory responses. The above studies show that it is reasonable and feasible to combine leukocyte and blood glucose levels as a new parameter in the prognostication of patients with AMI.
In the study by Quiroga Castro et al, the optimal cut-off value of LGI for predicting in-hospital compound outcome (cardiogenic death, heart failure, and angina after infarction) was 1600; thus, they divided 101 STEMI patients into 4 groups according to LGI: 0–800, 800–1600, 1600–2400 and >1600.6 Another study used the quartile of LGI in 405 STEMI patients.9 Others conducted a retrospective study of 128 patients with STEMI and observed a cut-off point of 1158.10 However, the above studies did not distinguish between diabetic and non-diabetic patients, and the number of patients included was relatively few.
The same threshold value should not be used for diabetic and non-diabetic patients, because diabetics have higher average glycemia, and the range of blood glucose change is different between diabetic and non-diabetic patients under stringent conditions.21,22 Therefore, the study population was divided into diabetic and non-diabetic groups according to discharge diagnosis of the patients, and then further divided into two subgroups according to different cut-off values of LGI, then the method of this study was more scientific and reasonable.
Quiroga Castro et al reported that LGI > 1600 was strongly correlated with in-hospital complications (cardiac death, heart failure, and post-infarction angina pectoris) in STEMI patients.6 Hirschson Prado et al found that LGI was an independent predictor of adverse outcomes (in-hospital death or Killip Kimball 3–4) in patients with STEMI.9 Others reported that LGI was associated with an increased occurrence of hospital complications, failed thrombolysis and death, and was an independent predictor of these complications.10 Rodriguez Jimenez et al11 also proved that a high LGI in the course of an AMI could be associated with a higher in-hospital mortality rate. Recently, it was found that LGI was a good predictor of one-year all-cause mortality in patients with STEMI.23
However, our study found that LGI was a predictor of all-cause mortality in hospital and MACCE at follow-up in patients without diabetics, but not for those with diabetics. Our findings differ from the previous studies. The reasons for these differences may be the following: 1) The study population included AMI patients, which was not completely the same as the study population in previous studies; 2) In this study, a more reasonable grouping method was used. Previous studies did not distinguish blood glucose levels. The final result represented the overall population, most of whom were non-diabetic patients generally; 3) This study found that LGI had no prognostic value for adverse outcomes during follow-up in diabetic patients, possibly because the follow-up time of this study was longer than that of a previous study,23 and there would be more confounding factors.
Regardless of glycemic status, patients with high LGI had a higher Killip class, indicating that patients with higher LGI had worse cardiac function and more severe heart failure. The higher LGI subgroup also had higher total cholesterol and LDL-C levels, suggesting that patients with dyslipidemia may be more prone to elevated LGI. In the diabetic group, the proportion of females, the serum creatinine level and the uric acid level in the higher LGI subgroup were higher. This is possibly due to women being more prone to hyperglycemia after menopause, which may be related to a decrease in sex hormone levels.24 In addition, diabetes can affect renal function, which worsens with the aggravation of diabetes.25 Therefore, high LGI is more likely associated with abnormal serum creatinine levels. On the other hand, in non-diabetic patients, the higher LGI subgroup had a higher percentage of STEMI, a significantly higher CRP level, more vomiting and sweating, lower blood pressure, and faster heart rate. This indicated that non-diabetic patients with high LGI had more severe disease, stronger inflammatory response, and more obvious symptoms. However, there was no difference in the proportion of STEMI and CRP levels among patients with diabetes, possibly due to the small sample size of the diabetic group or the diabetes itself.
This study had some limitations. First, this was a retrospective study and there were more confounding factors than prospective studies. The sample size was relatively small, which may have caused data bias. Second, cardiac ultrasound data were not recorded in this study. And the predictive value of LGI was not compared with other prognostic scores. Third, there was no data on the duration, type, and treatment of diabetes. Moreover, leukocytes and blood glucose may be checked differently in each hospital.
Conclusion
A higher LGI was an independent predictor of all-cause mortality during the hospitalization and MACCE at follow-up in AMI patients without diabetes. Aggressive treatment strategies should be adopted for these patients with higher LGI upon admission.
Data Sharing Statement
The datasets used are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the ethics committee of The Third People’s Hospital of Chengdu. This study was an observational study and was a collection and research of previously archived data and documents, which were public resources. Through the data collected in this study, the subjects could not be sought out, and the research project did not involve personal privacy and commercial interests, which complied with the regulations of “Measures for ethical review of biomedical research involving human beings” issued by China in 2016 and the Declaration of Helsinki, therefore the Ethics Committee of the Third People’s Hospital of Chengdu approved the waiver for informed consent. Statement of patient data confidentiality: After completion of the data collection in our study, the personal information of identifiable subjects related to the data was deleted, and anonymous numbers were used to replace it.
Acknowledgments
This study was supported by the Science and Technology Department of Sichuan, China [Grant number 2020YJ0483 and 2021YJ0215] and Chengdu High-level Key Clinical Specialty Construction Project. The authors would like to express their gratitude to Editage for its help improving the language of the manuscript during preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rosamond WD, Chambless LE, Heiss G, et al. Twenty-two-year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987–2008. Circulation. 2012;125(15):1848–1857. doi:10.1161/CIRCULATIONAHA.111.047480
2. Chen X, Meng Y, Shao M, et al. Prognostic value of pre-infarction angina combined with mean platelet volume to lymphocyte count ratio for no-reflow and short-term mortality in patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention. Med Sci Monit. 2020;7(26):e919300.
3. Granger CB, Kochar A. Understanding and targeting inflammation in acute myocardial infarction: an elusive goal. J Am Coll Cardiol. 2018;72(2):199–201. doi:10.1016/j.jacc.2018.05.006
4. Geovanini GR, Libby P. Atherosclerosis and inflammation: overview and updates. Clin Sci. 2018;132(12):1243–1252. doi:10.1042/CS20180306
5. Frangogiannis NG. The inflammatory response in myocardial injury, repair, and remodelling. Nat Rev Cardiol. 2014;11(5):255–265. doi:10.1038/nrcardio.2014.28
6. Quiroga Castro W, Conci E, Zelaya F, et al. Estratificación del riesgo en el infarto agudo de miocardio según el índice leucoglucémico. ¿El “Killip-Kimball” de laboratorio? Rev Fed Arg Cardiol. 2010;39(1):29–34.
7. Cui CY, Zhou MG, Cheng LC, et al. Admission hyperglycemia as an independent predictor of long-term prognosis in acute myocardial infarction patients without diabetes: a retrospective study. J Diabetes Investig. 2021;12(7):1244–1251. doi:10.1111/jdi.13468
8. Ferreira JA, Baptista RM, Monteiro SR, et al. Admission hyperglycemia and all-cause mortality in diabetic and non-diabetic patients with acute myocardial infarction: a tertiary center analysis. Intern Emerg Med. 2021;16(8):2109–2119. doi:10.1007/s11739-021-02693-0
9. Hirschson Prado A, Higa C, Merlo P, et al. Prognostic value of the leuko-glycemic index in acute myocardial infarction. Results from the SCAR multicenter registry. Rev Argent Cardiol. 2014;82(6):500–505. doi:10.7775/rac.es.v82.i6.3375
10. León-Aliz E, Moreno-Martínez FL, Pérez-Fernández GA, Vega-Fleites LF, Rabassa-López-Calleja MA. Leuko-glycemic index as an in-hospital prognostic marker in patients with ST-segment elevation myocardial infarction. Clin Investig Arterioscler. 2014;26(4):168–175. doi:10.1016/j.arteri.2014.01.002
11. Rodriguez-Jiménez A, Fardales-Rodríguez R, Toledo-Rodríguez E, Quintana C. Índice leuco-glucémico como factor pronóstico tras un infarto agudo de miocardio con elevación del segmento ST. Revista Finlay. 2019;9(2):97–107.
12. Caldas FA, Iaconis Campbell JD. Valor pronóstico del índice leucoglucémico en el stroke isquémico agudo. [Prognostic value of the leukoglycaemic index in cardiac surgery postoperative period]. Buenos Aires (AR): Asociación Médica Argentina; 2012 [cited April 19, 2021]. Available from: http://repositorio.barcelo.edu.ar/greenstone/collect/investig/index/assoc/HASH0183.dir/AMA%20Caldas%20Federico%252C%20Iaconis%20Campbell%20Juan.pdf.
13. García Alvarez PJ, García Albero AP, Santana Alvarez CJ. Índice leuco glucémico como predictor a corto plazo de mortalidad en el ictus isquémico. [Leukoglycaemic index as a predictor in short term of mortality in stroke]. Rev Arc Med Camaguey. 2018;22(2):163–170. Spanish.
14. Thygesen K. ‘Ten commandments’ for the fourth universal definition of myocardial infarction 2018. Eur Heart J. 2019;40(3):226. doi:10.1093/eurheartj/ehy856
15. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36(Suppl1):S67–74. doi:10.2337/dc13-S067
16. Dragu R, Huri S, Zukermann R, et al. Predictive value of white blood cell subtypes for long-term outcome following myocardial infarction. Atherosclerosis. 2008;196(1):405–412. doi:10.1016/j.atherosclerosis.2006.11.022
17. Deedwania P, Kosiborod M, Barrett E, et al. Hyperglycemia and acute coronary syndrome: a scientific statement from the American Heart Association Diabetes Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2008;117(12):1610–1619. doi:10.1161/CIRCULATIONAHA.107.188629
18. Deckers JW, van Domburg RT, Akkerhuis M, Nauta ST. Relation of admission glucose levels, short- and long-term (20-year) mortality after acute myocardial infarction. Am J Cardiol. 2013;112(9):1306–1310. doi:10.1016/j.amjcard.2013.06.007
19. Esposito K, Nappo F, Marfella R, et al. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation. 2002;106(16):2067–2072. doi:10.1161/01.CIR.0000034509.14906.AE
20. Terlecki M, Bednarek A, Kawecka-Jaszcz K, Czarnecka D, Bryniarski L. Acute hyperglycaemia and inflammation in patients with ST segment elevation myocardial infarction. Kardiol Pol. 2013;71(3):260–267. doi:10.5603/KP.2013.0038
21. Chen G, Li M, Wen X, et al. Association between stress hyperglycemia ratio and in-hospital outcomes in elderly patients with acute myocardial infarction. Front Cardiovasc Med. 2021;20(8):698725. doi:10.3389/fcvm.2021.698725
22. Planer D, Witzenbichler B, Guagliumi G, et al. Impact of hyperglycemia in patients with ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: the HORIZONS-AMI trial. Int J Cardiol. 2013;167(6):2572–2579. doi:10.1016/j.ijcard.2012.06.054
23. Padilla-Cueto D, Hernández-Negrín H, Ramírez-Gómez JI. The leucoglycaemic index is a predictor of one-year all-cause mortality in Cuban patients with ST-segment elevation acute myocardial infarction. CorSalud. 2019;11(1):21–29.
24. Kim C. Does menopause increase diabetes risk? Strategies for diabetes prevention in midlife women. Womens Health. 2012;8(2):155–167. doi:10.2217/WHE.11.95
25. Nadkarni GN, Yacoub R, Coca SG. Update on glycemic control for the treatment of diabetic kidney disease. Curr Diab Rep. 2015;15(7):42. doi:10.1007/s11892-015-0612-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.