")
Back to Journals » Clinical Interventions in Aging » Volume 16
Prognostic Significance of Uric Acid in Patients with Obstructive and Nonobstructive Coronary Artery Disease Undergoing D-SPECT
Authors Xu S, Liu L, Yin G, Mohammed AQ, Lv X, Feng C, Shi T , Abdu FA, Che W
Received 16 September 2021
Accepted for publication 6 November 2021
Published 16 November 2021 Volume 2021:16 Pages 1955—1965
DOI https://doi.org/10.2147/CIA.S339600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Siling Xu,1 Lu Liu,1 Guoqing Yin,1 Abdul-Quddus Mohammed,1 Xian Lv,1 Cailing Feng,1 Tingting Shi,1 Fuad A Abdu,1 Wenliang Che1,2
1Department of Cardiology, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2Department of Cardiology, Shanghai Tenth People’s Hospital Chongming Branch, Shanghai, People’s Republic of China
Correspondence: Wenliang Che; Fuad A Abdu
Department of Cardiology, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, 301 Yanchang Road, Jingan District, Shanghai, 200072, People’s Republic of China
Tel +86-21-66307259
Fax +86-21-66301051
Email [email protected]; [email protected]
Purpose: The association of serum uric acid (SUA) levels with cardiovascular outcomes in patients with coronary artery disease (CAD) has been extensively studied and yielded conflicting results. We aimed to investigate whether the severity of coronary stenosis and ischemia influences the prognostic impact of SUA levels in patients with CAD undergoing D-SPECT.
Patients and Methods: This study consecutively included patients who were admitted for CAD in Shanghai Tenth People’s Hospital between June 2014 and August 2018, had complete SUA data and underwent both coronary angiography and D-SPECT within 3 months. Hyperuricemia was defined as an SUA level of > 7 mg/dL in men and > 6 mg/dL in women. The primary outcome was major adverse cardiovascular events (MACE), defined as a composite of cardiac death, unplanned coronary revascularization, nonfatal myocardial infarction, ischemic stroke, heart failure, and angina-related hospitalization.
Results: A total of 695 patients were included, of whom 432 (62.2%) presented with obstructive CAD and 117 (16.8%) had hyperuricemia. During a median follow-up of 26 months, the incidence rates of MACE in patients with hyperuricemia and normouricemia were 15.2% and 21.1%, respectively. After a multivariable adjustment, hyperuricemia was significantly associated with an increased risk of MACE (HR: 1.39, 95% CI: 1.03– 1.87, p = 0.033) when compared with normouricemia. When repeating the primary analysis in patients with and without obstructive CAD, we showed that hyperuricemia was independently associated with an 80% increased risk of MACE among patients with nonobstructive CAD (HR: 1.80, 95% CI: 1.04– 3.11, p = 0.035), while such a significant association was not found among those with obstructive CAD (HR: 1.18, 95% CI: 0.82– 1.72, p = 0.373). Moreover, we uncovered a U-shaped and linear trajectory of SUA levels with MACE in the obstructive and nonobstructive CAD, respectively. The sex-specific analysis showed that the adverse impact of hyperuricemia was only pronounced in males (HR: 1.73, 95% CI: 1.18– 2.53, p = 0.005) but not in females (HR: 0.98, 95% CI: 0.57– 1.66, p = 0.933).
Conclusion: Hyperuricemia is significantly associated with increased risk of MACE in the nonobstructive CAD rather than in the obstructive CAD.
Keywords: coronary artery disease, serum uric acid, D-SPECT, nonobstructive, outcomes
Introduction
Coronary artery disease (CAD) remains one of the leading causes of cardiovascular morbidity and mortality worldwide. Despite the identification of modifiable risk factors and the development of risk prediction models that enable recognition of individuals at greater risk of future events, CAD risk evaluation still lacks accuracy in daily clinical practice.1,2 In this regard, investigating novel risk factors is of great clinical importance in improving CAD risk prediction, thus leading to better patient care.
Uric acid is the metabolic end product of purine metabolism in humans, which is under the control of the enzyme xanthine oxidase.3 Although a wealth of research has reported that greater serum uric acid (SUA) levels are associated with poorer survival in patients with CAD,4–7 several recent studies have failed to establish such an association.8,9 Apart from the differences in study design, clinical backgrounds, adjustment of confounders, length of follow-up, etc., the severity of CAD itself may also be responsible for these conflicting results. However, so far, data regarding the interaction effects of SUA levels with CAD severity are still limited.
Invasive coronary angiography is an important imaging examination for the assessment of coronary stenosis severity. Due to the lack of pathophysiological data on myocardial ischemia, its usefulness in the functional assessment of stenosis is hampered. As the technological advancement in noninvasive myocardial perfusion imaging (MPI) with single-photon emission computed tomography (SPECT), current guidelines have recommended its application in the suspected CAD population for ischemia evaluation.10 More recently, a cardiac SPECT system equipped with cadmium-zinc-telluride (CZT) detectors (D-SPECT), which provides a higher speed and resolution than the traditional NaI scintillation detectors, has been introduced into clinical practice.11 Our previous study has validated that the impaired myocardial ischemia detected by D-SPECT MPI was significantly associated with adverse cardiovascular events.12 Additionally, D-SPECT MPI also offers a novel opportunity to explore the prognostic impacts of SUA in patients with CAD stratified by the severity of ischemia. Accordingly, in the present analysis, we aimed to investigate the clinical implications of SUA in a cohort of CAD subjects stratified by stenosis severity who had undergone both coronary angiography and D-SPECT MPI.
Patients and Methods
Study Population
The electronic medical records of all consecutive patients who were admitted for suspected CAD at Shanghai Tenth People’s Hospital between June 2014 and August 2018 were screened for eligibility. We only included individuals who were over 18 years old and underwent both invasive coronary angiography and stress-rest MPI within 3 months. Patients with missing data on SUA were excluded (as shown in Online Figure 1). The suspected CAD was considered according to symptoms and/or signs of myocardial ischemia, ECG presentation, and clinical risk profiles. Our study was performed following the Declaration of Helsinki, and the protocol had been approved by the ethics committee of the Shanghai Tenth People’s Hospital. Informed consent was waived as patients’ information was retrieved anonymously.
D-SPECT Examination
Details with respect to the acquisition and analysis of D-SPECT had been previously described.12 In brief, the MPI was acquired using a D-SPECT cardiac scanner (Spectrum Dynamics, Biosensors, Israel), and a single-day rest/stress protocol with the use of 99mTc-sestamibi (99mTc-MIBI) was applied. The rest of the testing was performed approximately 1 hour after the administration of 99mTc-MIBI (3 MBq·kg−1), and the stress testing was performed using intravenous injection of ATP (140μg·kg−1·min−1). The stress and rest D-SPECT images were evaluated visually using the 17-segment model of the left ventricle and a five-point scale.13 Hence, myocardial ischemic and functional parameters, such as summed stress score (SSS), summed rest score (SRS), summed difference score (SDS), stress total perfusion defects (TPD), stress and rest LVEF, as well as transient ischemic dilation (TID), could be adequately calculated (Definitions are shown in Online Table 1). Myocardial ischemia was considered as with an SDS of ≥2.14 All D-SPECT images were independently reviewed and analyzed by two experienced nuclear cardiologists.
Data Collection
The main exposure was the baseline SUA collected after a 12-h fast. Hyperuricemia was defined as an SUA level of >7 mg/dL in men and > 6 mg/dL in women.15 Each epicardial coronary artery with a > 2.0 mm diameter examined by coronary angiography was analyzed for the presence of coronary stenosis and was quantified into 2 groups: nonobstructive (0~50% stenosis) and obstructive (≥50% stenosis). A detailed review of medical records was performed to collect information on demographics, medical history, admission presentation, laboratory indices, D-SPECT characteristics, and medication usage. Detailed definitions of baseline characteristics are presented in Online Table 1.
Outcomes and Follow-Up
The primary outcome was a major adverse cardiovascular event (MACE) that was defined as a composite of cardiac death, unplanned coronary revascularization, nonfatal myocardial infarction, ischemic stroke, heart failure, and angina-related hospitalization. All deaths without a definite non-cardiac cause would be treated as cardiac deaths. Ischemic stroke was defined as the presence of a new focal neurologic deficit considered to be ischemic in origin, with symptoms or signs lasting over 24 hours. Myocardial infarction cases were confirmed if they had: (1) elevated troponin level higher than twice the upper limit of normal and (2) either ischemia-related symptoms and/or typical ECG changes. Heart failure was diagnosed according to symptoms including dyspnea and fatigue, and signs of pulmonary or peripheral edema that required intravenous diuretic treatment. Patients were followed from the date of index D-SPECT examination to the date of the presence of an outcome of interest, death, or last follow-up (July 2020), whichever occurred first. Follow-up information was collected either by a comprehensive review of individuals’ medical records or by telephone interview.
Statistical Analysis
Categorical variables were presented as n (%) and were compared using the chi-square test or Fisher’s exact test. Continuous variables were presented as median (interquartile [IQR]) or mean±SD and were compared using the Student’s t-test or the Mann−Whitney U-test, as appropriate. All p values were two-sided, and the significance level was set at 0.05. All analyses were performed using Stata 14.0 (StataCorp, College Station, TX, USA).
In the long-term survival analysis, the incidence rate was estimated as the number of patients occurring in an outcome of interest divided by person-years at risk. Crude cumulative event curves were illustrated using the Kaplan–Meier method and compared with Log rank tests. Cox proportional hazards regression models were constructed to explore the impact of SUA levels on subsequent outcomes, in which we adjusted for: (i) the HEART score, a well-validated and calibrated algorithm for the total cardiovascular risk estimate;16 (ii) age, gender, current smoker, hypertension, diabetes, dyslipidemia, stroke, congestive heart failure, creatinine, left ventricular ejection fraction (LVEF), and medication at discharge (aspirin, statin, ACEI/ARB, β-blocker, and diuretic) as a fully adjusted model. The proportional hazards assumption was validated by examining graphs of estimated log(-log) curves. Given only 4 (0.6%) and 27 (3.9%) missing values in the creatinine and LVEF, respectively; we used the median value of each variable to impute the aforementioned missing data. To further investigate the nonlinear association between SUA levels and MACE, restricted cubic spline models were fitted for SUA with 3 knots fixed at 10th, 50th, and 90th percentage of SUA levels. The median value of SUA (5.6 mg/dL) was used as the reference. Moreover, we conducted a propensity score-matching (PSM) analysis to evaluate the impact of hyperuricemia on the primary outcome based on the propensity scores calculated from baseline covariates (details were presented in Online Methods).
We also performed several subgroup analyses according to the D-SPECT MPI characteristics including SSS (<4 vs ≥4) SDS (<2 vs ≥2), TPD (<2 vs ≥2), and abnormal TID (Yes vs No). In our sensitivity analyses, we repeated the main analyses in a non-missing dataset (N=664) and patients without the use of urate-lowering agents (N=684), accounting for its influence on the SUA concentration. To explore the sex differences in the prognostic impact of SUA among patients with CAD, we further performed a sex-specific analysis by repeating the main analysis in men and women, separately.
Results
Baseline Characteristics
Overall, a total of 695 patients were included in the present study, the mean age was 63.3±9.8 years, 56.4% were men, and 117 (16.8%) patients presented with hyperuricemia. Patients with hyperuricemia were younger, with a higher BMI, serum creatinine, and lipid profiles, more likely to have a history of hypertension and atrial fibrillation and to be prescribed urate-lowering agents when compared with those with normouricemia. MPI characteristics were similar between the 2 groups (Table 1). Of the 695 patients, 411 were diagnosed with myocardial ischemia derived from D-SPECT. Baseline clinical characteristics of patients presenting with myocardial ischemia are shown in Online Table 2.
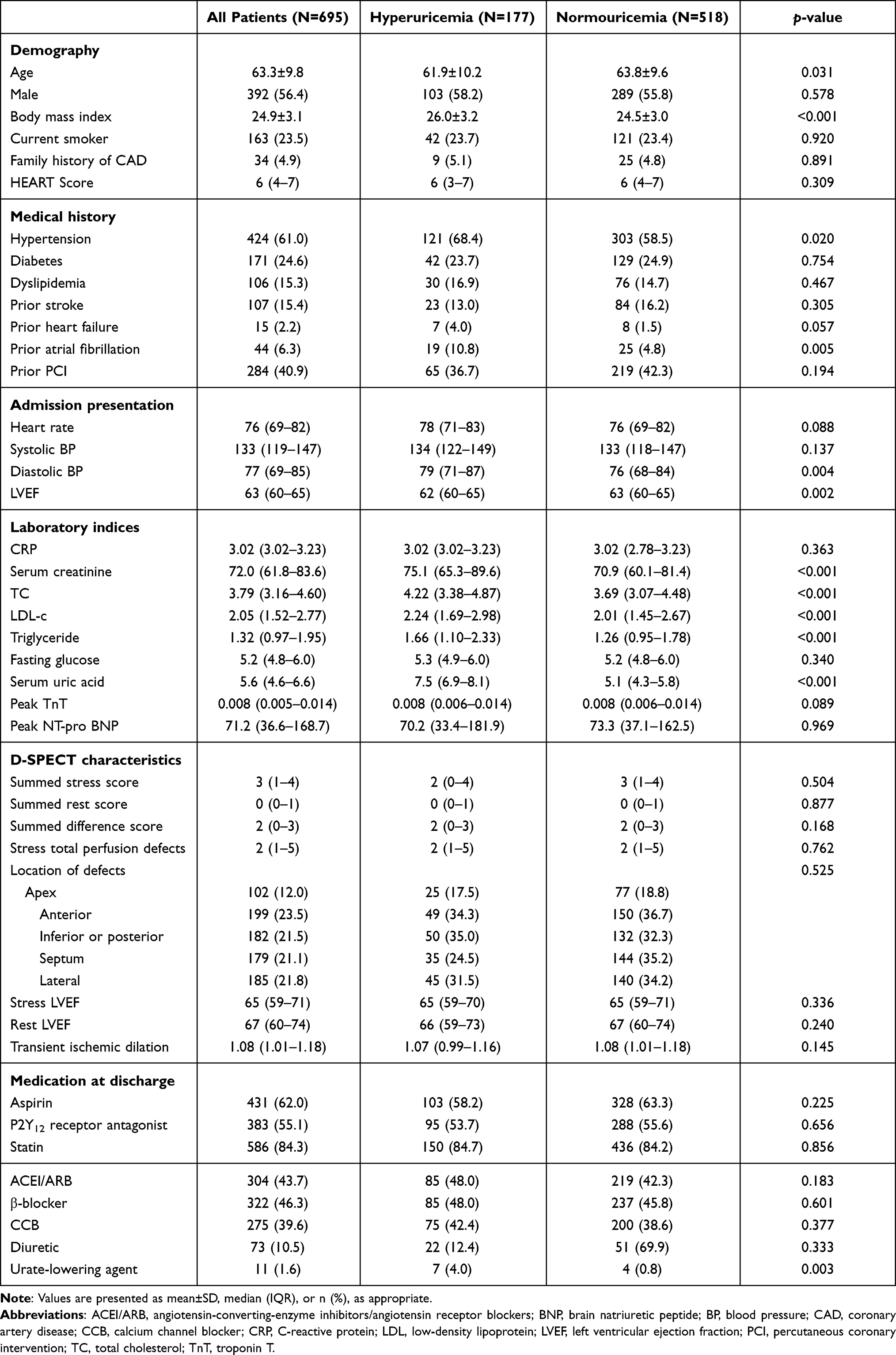 |
Table 1 Baseline Characteristics of Study Cohort by Serum Uric Acid |
Clinical Outcomes in the Whole Cohort
During a median follow-up of 26 (IQR, 21–33) months, the incidence rates of MACE were higher in patients with hyperuricemia compared with the normouricemia group (15.2% and 21.1% per-year, respectively) (Figure 1A). Treating the normouricemia as the reference, the HR and 95% CI was 1.46 (1.09–1.95) for hyperuricemia after accounting for the HEART score; and 1.39 (1.03–1.87) after full adjustment (Table 2). Baseline characteristics of the PSM cohort were well-balanced (Online Figure 2). In the matched cohort, hyperuricemia remained an independent risk factor of MACE after multivariable adjustment (HR: 1.55, 95% CI: 1.06–2.27, p=0.025) (Figure 1B).
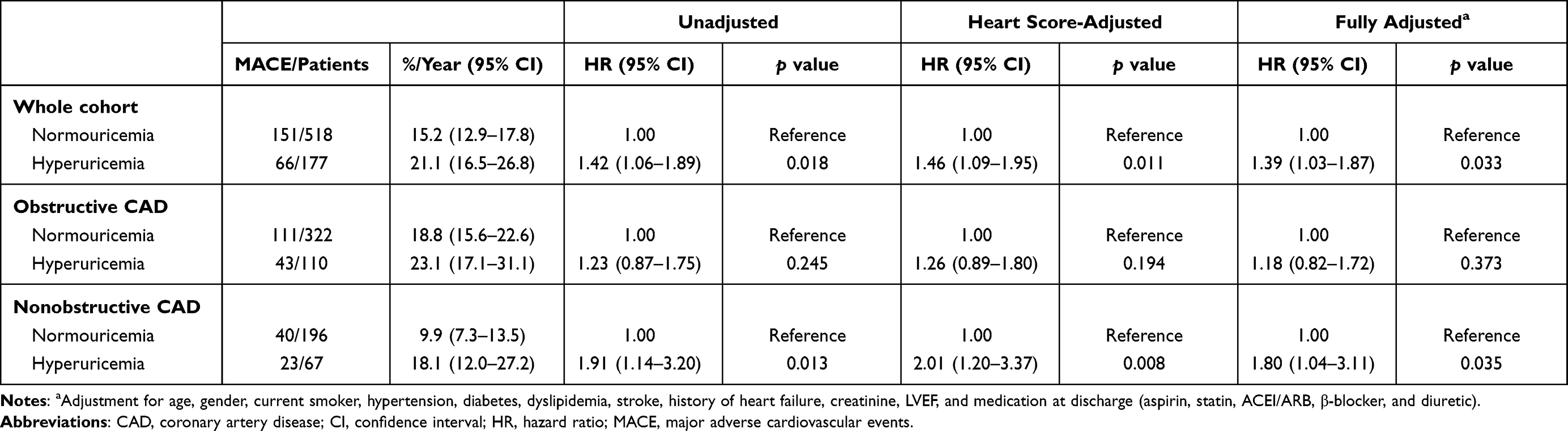 |
Table 2 Risk of Cardiovascular Events by SUA Levels |
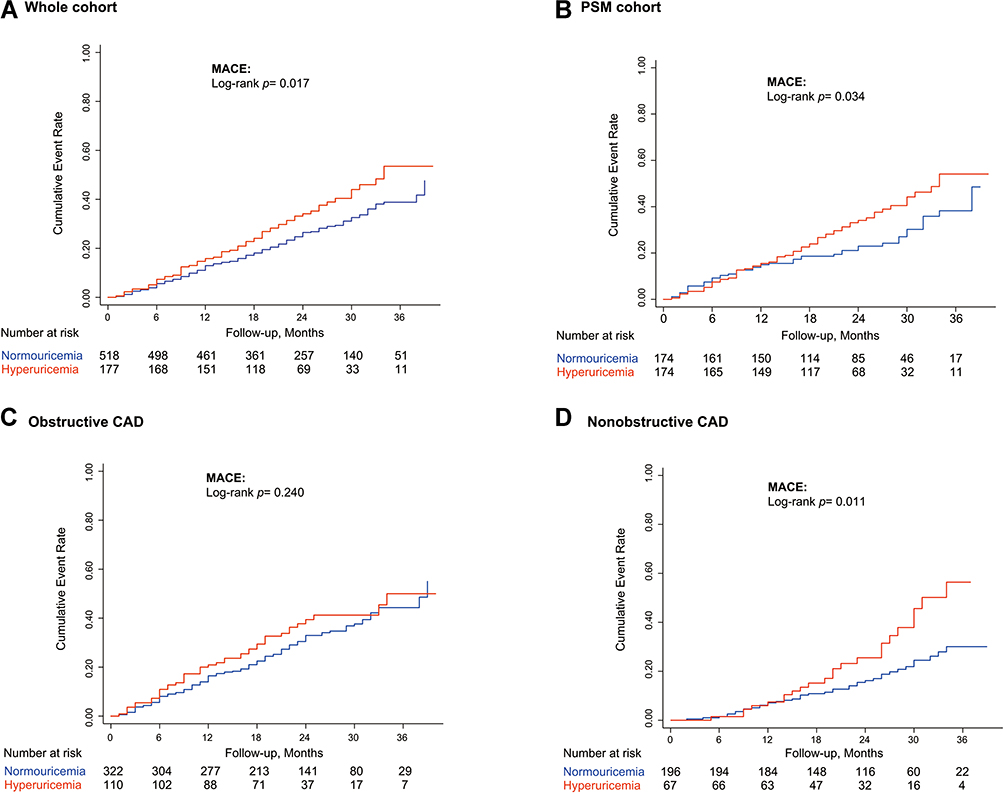 |
Figure 1 Long-term risk of MACE in the whole cohort (A) PSM cohort (B) obstructive CAD cohort (C) and nonobstructive CAD cohort (D) according to the SUA levels. Abbreviations: CAD, coronary artery disease; MACE, major adverse cardiovascular events; PSM, propensity-score matching; SUA, serum uric acid. |
Clinical Outcomes in CAD Subtypes
To investigate the role of CAD severity in hyperuricemia-related cardiovascular outcomes, patients were stratified into obstructive and nonobstructive CAD. Of the 695 patients, 432 (62.2%) presented with obstructive CAD. Baseline characteristics of the patients stratified by coronary stenosis severity are shown in Online Table 3. During the follow-up period, a total of 154 (35.6%) and 63 (24.0%) MACE were recorded in patients with obstructive and nonobstructive CAD, respectively (Figures 1C and D). Hyperuricemia was significantly associated with increased risk of MACE in the nonobstructive CAD group (HEART score-adjusted HR: 2.01, 95% CI: 1.20–3.37, p=0.008; fully adjusted HR: 1.80, 95% CI: 1.04–3.11, p=0.035) instead of the obstructive CAD group (HEART score-adjusted HR: 1.26, 95% CI: 0.89–1.80, p=0.194; fully adjusted HR: 1.18, 95% CI: 0.82–1.72, p=0.373) (Table 2).
The Trajectory Between SUA Levels and MACE
In multivariable-adjusted spline regression models, we illustrated a similar U-shaped association between SUA levels and MACE in the whole cohort (p for nonlinearity = 0.004) and obstructive CAD group (p for linearity = 0.007). However, for the nonobstructive CAD, a linear association was found (p for linearity = 0.479) (Figures 2A–C). Hence, we introduced the SUA as a continuous covariate into the multivariable Cox regression model and showed that each 1 mg/dL increase of SUA was associated with a nearly 25% elevated risk of MACE in the nonobstructive CAD (HR: 1.25, 95% CI: 1.04–1.50, p=0.016).
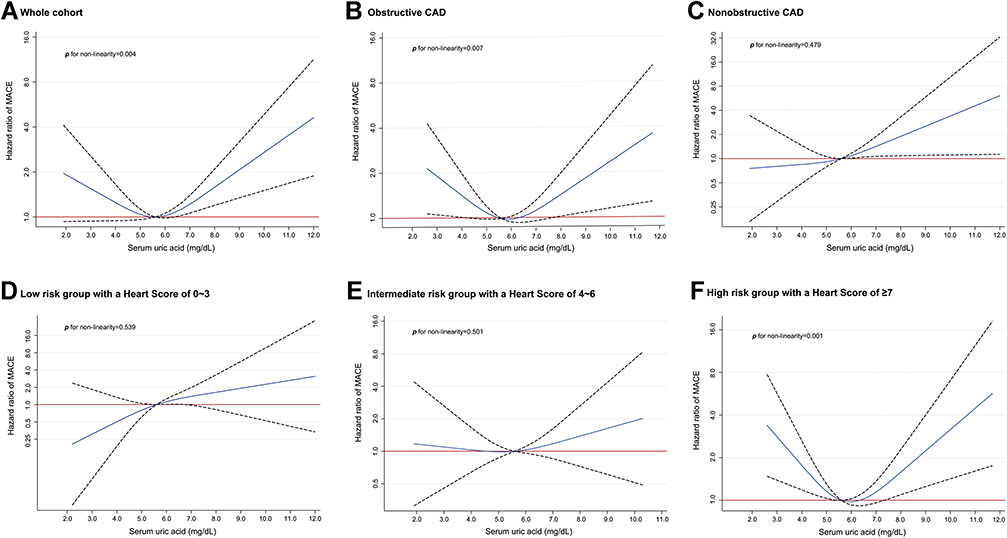 |
Figure 2 The trajectories of SUA levels with MACE in the whole cohort (A) obstructive CAD cohort (B) nonobstructive CAD cohort (C) and low-, intermediate-, and high-risk cohorts stratified by HEART score (D–F) The solid line in each figure indicates the HR, and the dashed lines indicate the 95% CIs. The Orange reference line indicates an HR of 1.00. The median value of SUA levels (5.6 mg/dL) was treated as the reference. Other abbreviations referred to Figure 1. Abbreviations: CI, confidence interval; HR, hazard ratio. |
To evaluate whether the association of SUA with MACE relied on individuals’ cardiovascular risk profiles, we further stratified the whole cohort into low-risk, intermediate-risk, and high-risk subgroups based on the HEART scores of 0~3, 4~6, and ≥7, respectively. The linear trajectory between SUA levels and MACE gradually evolved into a U-shaped as the HEART score increased (Figures 2D–F).
Subgroup and Sensitivity Analysis
Further subgroup analyses for associations of hyperuricemia with MACE were performed. The increased risk of MACE associated with hyperuricemia was consistent with all myocardial ischemia or dysfunction-related subgroups that were detected by the D-SPECT MPI as a whole, obstructive CAD, and nonobstructive CAD cohorts (Figure 3). In addition, hyperuricemia remained an independent predictor of MACE in the whole cohort in an analysis of patients without the use of urate-lowering agents (HR: 1.36, 95% CI: 1.01–1.85, p=0.046). When we repeated the main analysis in the non-missing dataset, such a correlation still existed in the whole cohort (HR: 1.38, 95% CI: 1.02–1.87, p=0.037) but only marginally significant in the nonobstructive cohort (HR: 1.70, 95% CI: 0.97–2.98, p=0.062) (Online Table 4). In the whole population, our sex-specific analysis demonstrated that the detrimental impact of hyperuricemia was only pronounced in males (HR: 1.73, 95% CI: 1.18–2.53, p=0.005) rather than in females (HR: 0.98-0.57-1.66, p=0.933). Similar findings were observed in patients with nonobstructive CAD, whereas a neutral result was obtained in those with obstructive CAD (Online Table 5).
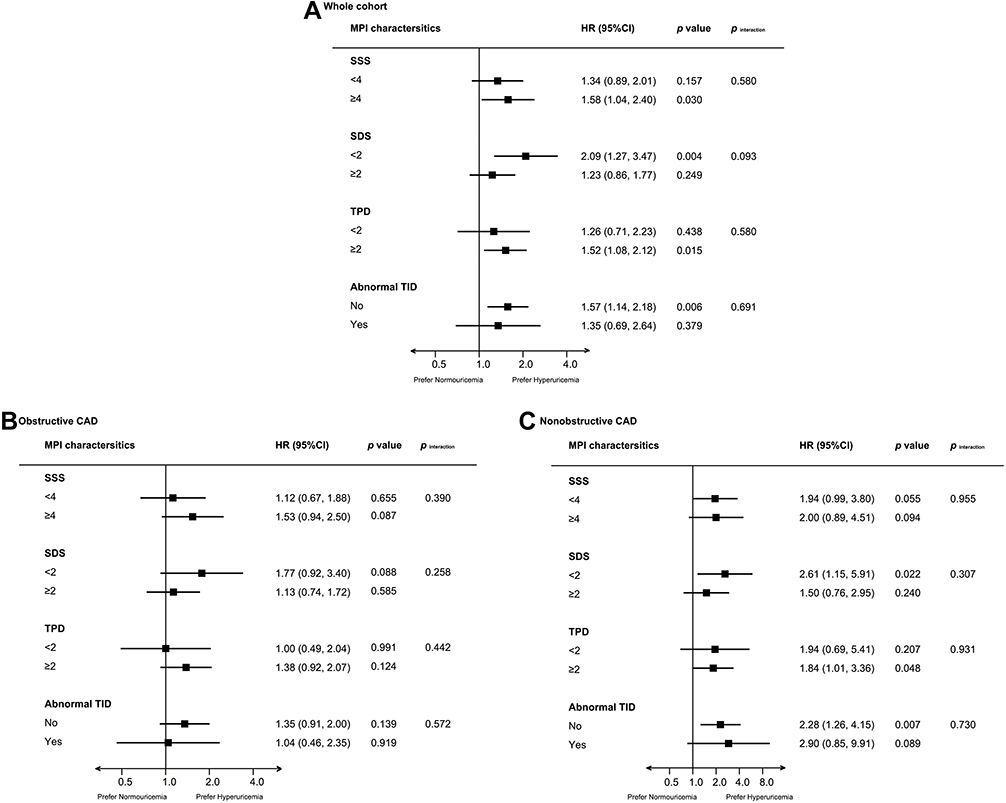 |
Figure 3 Subgroup analyses based on MPI characteristics in the whole cohort (A) obstructive CAD cohort (B) and nonobstructive CAD cohort (C) The risks were demonstrated as HRs and 95% CIs after adjustment for the HEART score. Abbreviations: MPI, myocardial perfusion imaging; SDS, summed difference score; SRS, summed rest score; SSS, summed stress score; TID, transient ischemic dilation; TPD, total perfusion defects. |
Discussion
In this retrospective study of patients with suspected CAD undergoing D-SPECT and coronary angiography, hyperuricemia was significantly associated with a heightened risk of MACE, which was mainly driven by the increased risk in patients with nonobstructive CAD. This correlation remained pronounced even after multivariable adjustment or being analyzed in a PSM cohort. We uncovered a U-shaped association between SUA levels and MACE in the whole and obstructive CAD cohort, whereas a linear association was observed in the nonobstructive CAD.
The association of SUA levels with clinical outcomes has been extensively studied in various settings and yielded conflicting results.17–20 In the Progetto Ipertensione Umbria Monitoraggio Ambulatoriale (PIUMA) registry, SUA was independently associated with adverse cardiovascular events in patients with essential hypertension.21 Differently, in a large population-based observational study with a median follow-up of nearly 6 years, Cheong et al demonstrated that both men and women in the highest quintile of SUA levels were not challenged by higher cardiovascular mortality when compared to the middle SUA quintile after multivariable adjustment.9 More importantly, in an umbrella review that summarized evidence from observational studies, randomized controlled trials, and Mendelian randomization studies, Li et al evaluated the association of high SUA levels with increased CAD mortality as highly suggestive.22 A greater level of SUA has also been demonstrated to predict poor prognosis in established cardiac disease.4,23,24 In the present analysis, we found that hyperuricemia was independently associated with a 39% increased risk of MACE. The results from the PSM analysis further supported this finding. Similarly, in a meta-analysis with 29 prospective studies and a total of 958,410 participants being analyzed, Li et al showed hyperuricemia was significantly associated with increased CAD mortality. Moreover, each 1 mg/dL increment in SUA was associated with an independent 13% increase in the risk of CAD mortality. The underlying mechanisms by which high SUA levels result in poor survival have been explained as the uric acid is involved in multiple biological processes (eg, oxidative stress, systemic inflammation, etc) that could activate the inflammatory cascade reaction and renin-angiotensin system, stimulate vascular smooth cell proliferation, as well as reduce vascular nitric oxide activity,3 all of which have been identified as pivotal regulators during the development of CAD.
On the other hand, several other studies indicated that hyperuricemia can only be treated as a bystander rather than a casual contributor to CAD mortality. The possible explanations for such a conflicting result may be attributed to data from different populations, adjustment for different covariates, or differences in the diagnostic criteria of hyperuricemia. Strasak showed that in a cohort of 83,683 healthy participants from Austria followed for a median of 13.6 years, the initially significant association between SUA levels and CAD mortality completely disappeared after adjusting for several demographic and laboratory parameters, as well as the year of examination.25 However, in their study, individuals’ cardiac function and medication usage had not been adjusted. In the Fremantle Diabetes Study, Ong G et al showed that the SUA levels could not predict the risk of all-cause and cardiovascular death, but only used data from patients with type 2 diabetes.20
Although numerous preceding studies had investigated the clinical implications of hyperuricemia in patients with obstructive CAD or acute coronary syndrome,15,26 data were limited on those with nonobstructive lesions. In our study, we showed that hyperuricemia was significantly associated with an 80% increased risk of MACE in patients with nonobstructive CAD, while no association was observed in those with obstructive CAD. To the best of our knowledge, this is the first study that validates the detrimental impact of hyperuricemia in nonobstructive CAD individuals. Another novel finding was that we uncovered a U-shaped and a linear association of SUA levels with MACE in the obstructive and nonobstructive CAD individuals, respectively. To date, studies concerning the trajectory pattern of the association of SUA levels with cardiovascular events have yielded controversial results.21,27 Lai et al demonstrated a linear correlation of SUA levels with the risk of incident CAD in the middle-aged and elderly Chinese population.28 Virdis et al also reported a linear association of SUA levels with all-cause and cardiovascular mortality in 22,714 participants attending hypertension clinics from the (Uric Acid Right for Heart Health) URRAH project.29 Differently, in a prospective observational study that recruited 4652 patients with chronic heart failure from Japan, T. Fujihashi et al reported a U-shaped relationship between SUA levels and all-cause mortality.30 These disparities indicated the role of low SUA levels varied in different settings, which underscored the clinical importance of a tailored management strategy for SUA levels.
The pathophysiological mechanisms of a low SUA level contributing to the increased risk of cardiovascular events remain unclear. A low SUA level has been proposed as a surrogate for malnourishment due to inadequate protein and calorie intake, which has been recognized as a risk factor for poor survival.27 In addition, low SUA levels may indicate the impaired total antioxidant capacity because uric acid could act as an antioxidant by decreasing the availability of superoxide.3
Concerning the difference in the trajectories between SUA levels and MACE among patients with and without obstructive CAD, we assumed that clinical backgrounds may be one of the possible explanations. Hypertension, diabetes, dyslipidemia, and smoking habits have been associated with excessive production of reactive oxygen species (ROS),31 and in our study, the prevalence of which was significantly higher in patients with obstructive CAD as compared to those with nonobstructive CAD. Given the assumption that the beneficial impact of uric acid acting as an antioxidant can be more pronounced in the obstructive CAD group, but less pronounced in the nonobstructive group, it is plausible that a low SUA level was associated with a poor outcome in patients with obstructive CAD. In line with our hypothesis, in an observational study including 231 patients with chronic coronary syndrome and complete SUA data, Maloberti et al concluded that the adverse impact of SUA may gradually be overshadowed by other risk factors when coronary disease evolved to more advanced stages.32 Qin et al reported that as the increases in the quartiles of SUA, the prevalence of CVD elevated only in those without metabolism syndrome (p for trend <0.001), but not necessarily increased in those with metabolism syndrome (p for trend = 0.217).33 Our exploratory analysis where the whole cohort was stratified by HEART score also corroborated this hypothesis, since the protective value of uric acid gradually became evident with the increases in the HEART score. Further prospective studies were warranted to confirm our findings.
Previous studies have explored the sex-specific relationship between hyperuricemia and the risk of cardiovascular outcomes.34 Fang et al found that the prognostic influence of SUA levels was similar in both men and women.35 Kamei et al reported in a community-based population that hyperuricemia (SUA≥7.0mg/dl) was a significant risk factor of mortality in females (HRs and 95% CIs for all-cause and cardiovascular mortality were 5.92 [2.10–14.60] and 10.70 [1.76–50.20], respectively) rather than in males.36 By contrast, in a prospective study with 3926 elderly participants being analyzed, Winder et al showed that a higher level of SUA (≥8mg/dl) was an independent predictor of overall survival only in men (OR: 1.78, 95% CI: 1.06–2.98) but not in women (odds ratio [OR]: 1.30, 95% CI: 0.84–2.48).37 In our sex-specific analysis, we also demonstrated that hyperuricemia was an independent risk factor for MACE in males with CAD, but not in females, which was particularly pronounced in those with nonobstructive CAD. Although several potential explanations including differences in the study population, clinical settings, covariates used for multivariable adjustment, and the cutoff value of SUA for hyperuricemia identification, as well as the protective effect of estrogen in women, have been proposed, the exact mechanisms for such sex differences remain to be elucidated.
Several limitations should also be noted. First, this analysis was a single-center, retrospective study focusing on patients who had undergone D-SPECT MPI and coronary angiography, which may preclude the extrapolation of our findings to other settings. Second, despite the observed association of SUA levels with cardiovascular outcomes after adjustment for several potential confounders, as well as the use of PSM analysis, the effects of unmeasured confounders still cannot be eliminated. Third, we only analyzed a single measurement of baseline SUA levels and did not consider changes in SUA levels over the follow-up period. Fourth, due to lack of data about individuals’ dietary habits, marital status, and economic factors, we cannot evaluate their impacts on patients’ clinical outcomes.
Conclusions
The present study demonstrated that a greater level of SUA was significantly associated with an increased risk of MACE in patients with nonobstructive CAD. The SUA levels had a U-shaped and a linear prognostic impact in patients with obstructive and nonobstructive CAD, respectively, which underlined the detrimental effects of low SUA levels in the obstructive CAD population. In addition, the adverse impact of hyperuricemia was more pronounced in males than in females. Our results suggested that a tailored SUA management strategy should be considered in the CAD population.
Data Sharing Statement
The analytical methods and study materials will be made available upon reasonable request. Researchers can contact the corresponding author for more information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported in part by Chinese National Natural Science Foundation (82170521), Shanghai Natural Science Foundation of China (21ZR1449500), Foundation of Shanghai Municipal Health Commission (202140263), the Fundamental Research Funds for Central Universities (NO.22120190211), Foundation of Chongming (CKY2021-21, CKY2020-29), and Clinical Research Plan of SHDC (SHDC2020CR4065).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yeboah J, McClelland RL, Polonsky TS, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012;308(8):788–795. doi:10.1001/jama.2012.9624
2. Selvarajah S, Kaur G, Haniff J, et al. Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population. Int J Cardiol. 2014;176(1):211–218. doi:10.1016/j.ijcard.2014.07.066
3. Jayachandran M, Qu S. Harnessing hyperuricemia to atherosclerosis and understanding its mechanistic dependence. Med Res Rev. 2021;41(1):616–629. doi:10.1002/med.21742
4. Wang R, Song Y, Yan Y, et al. Elevated serum uric acid and risk of cardiovascular or all-cause mortality in people with suspected or definite coronary artery disease: a meta-analysis. Atherosclerosis. 2016;254:193–199. doi:10.1016/j.atherosclerosis.2016.10.006
5. Li M, Hu X, Fan Y, et al. Hyperuricemia and the risk for coronary heart disease morbidity and mortality a systematic review and dose-response meta-analysis. Sci Rep. 2016;6(1):19520. doi:10.1038/srep19520
6. Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta. 2018;484:150–163. doi:10.1016/j.cca.2018.05.046
7. Wu AH, Gladden JD, Ahmed M, et al. Relation of serum uric acid to cardiovascular disease. Int J Cardiol. 2016;213:4–7. doi:10.1016/j.ijcard.2015.08.110
8. De Luca G, Secco GG, Santagostino M, et al. Uric acid does not affect the prevalence and extent of coronary artery disease. Results from a prospective study. Nutr Metab Cardiovasc Dis. 2012;22(5):426–433. doi:10.1016/j.numecd.2010.08.005
9. Cheong E, Ryu S, Lee JY, et al. Association between serum uric acid and cardiovascular mortality and all-cause mortality: a cohort study. J Hypertens. 2017;35(Suppl 1):S3–S9. doi:10.1097/HJH.0000000000001330
10. Kunadian V, Chieffo A, Camici PG, et al. An EAPCI expert consensus document on ischaemia with non-obstructive coronary arteries in collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation endorsed by Coronary Vasomotor Disorders International Study Group. Eur Heart J. 2020;41(37):3504–3520. doi:10.1093/eurheartj/ehaa503
11. Nudi F, Iskandrian AE, Schillaci O, et al. Diagnostic accuracy of myocardial perfusion imaging with CZT technology: systemic review and meta-analysis of comparison with invasive coronary angiography. JACC Cardiovasc Imaging. 2017;10(7):787–794. doi:10.1016/j.jcmg.2016.10.023
12. Liu L, Abdu FA, Yin G, et al. Prognostic value of myocardial perfusion imaging with D-SPECT camera in patients with ischemia and no obstructive coronary artery disease (INOCA). J Nucl Cardiol. 2020;31(5):261–266. doi:10.1007/s12350-020-02252-8
13. Henzlova MJ, Duvall WL, Einstein AJ, et al. ASNC imaging guidelines for SPECT nuclear cardiology procedures: stress, protocols, and tracers. J Nucl Cardiol. 2016;23(3):606–639. doi:10.1007/s12350-015-0387-x
14. Sharir T, Germano G, Kang X, et al. Prediction of myocardial infarction versus cardiac death by gated myocardial perfusion SPECT: risk stratification by the amount of stress-induced ischemia and the poststress ejection fraction. J Nucl Med. 2001;42(6):831–837.
15. Zhang C, Jiang L, Xu L, et al. Implications of hyperuricemia in severe coronary artery disease. Am J Cardiol. 2019;123(4):558–564. doi:10.1016/j.amjcard.2018.11.027
16. Poldervaart JM, Reitsma JB, Backus BE, et al. Effect of using the HEART Score in patients with chest pain in the emergency department: a stepped-wedge, cluster randomized trial. Ann Intern Med. 2017;166(10):689–697. doi:10.7326/M16-1600
17. Li X, Meng X, Spiliopoulou A, et al. MR-PheWAS: exploring the causal effect of SUA level on multiple disease outcomes by using genetic instruments in UK Biobank. Ann Rheum Dis. 2018;77(7):1039–1047. doi:10.1136/annrheumdis-2017-212534
18. Pilemann-Lyberg S, Hansen TW, Tofte N, et al. Uric acid is an independent risk factor for decline in kidney function, cardiovascular events, and mortality in patients with type 1 diabetes. Diabetes Care. 2019;42(6):1088–1094. doi:10.2337/dc18-2173
19. Savale L, Akagi S, Tu L, et al. Serum and pulmonary uric acid in pulmonary arterial hypertension. Eur Respir J. 2021;58(2):2000332. doi:10.1183/13993003.00332-2020
20. Ong G, Davis WA, Davis TM. Serum uric acid does not predict cardiovascular or all-cause mortality in type 2 diabetes: the Fremantle Diabetes Study. Diabetologia. 2010;53(7):1288–1294. doi:10.1007/s00125-010-1735-7
21. Verdecchia P, Schillaci G, Reboldi G, et al. Relation between serum uric acid and risk of cardiovascular disease in essential hypertension. The PIUMA study. Hypertension. 2000;36:1072–1078.
22. Li X, Meng X, Timofeeva M, et al. Serum uric acid levels and multiple health outcomes: umbrella review of evidence from observational studies, randomised controlled trials, and Mendelian randomisation studies. BMJ. 2017;357:j2376. doi:10.1136/bmj.j2376
23. Andrikou I, Tsioufis C, Dimitriadis K, et al. Uric acid as an independent predictor of coronary artery disease in essential hypertension: data from an 8-year-follow-up study. Clin Exp Pharmacol Physiol. 2018;45(8):866–869. doi:10.1111/1440-1681.12928
24. Lazzeroni D, Bini M, Camaiora U, et al. Serum uric acid level predicts adverse outcomes after myocardial revascularization or cardiac valve surgery. Eur J Prev Cardiol. 2018;25(2):119–126. doi:10.1177/2047487317744045
25. Strasak A, Ruttmann E, Brant L, et al. Serum uric acid and risk of cardiovascular mortality: a prospective long-term study of 83,683 Austrian men. Clin Chem. 2008;54(2):273–284. doi:10.1373/clinchem.2007.094425
26. Tscharre M, Herman R, Rohla M, et al. Uric acid is associated with long-term adverse cardiovascular outcomes in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Atherosclerosis. 2018;270:173–179. doi:10.1016/j.atherosclerosis.2018.02.003
27. Tseng WC, Chen YT, Ou SM, et al. U-shaped association between serum uric acid Levels with cardiovascular and all-cause mortality in the elderly: the role of malnourishment. J Am Heart Assoc. 2018;7(4). doi:10.1161/JAHA.117.007523.
28. Lai X, Yang L, Légaré S, et al. Dose-response relationship between serum uric acid levels and risk of incident coronary heart disease in the Dongfeng-Tongji cohort. Int J Cardiol. 2016;224:299–304. doi:10.1016/j.ijcard.2016.09.035
29. Virdis A, Masi S, Casiglia E, et al. Identification of the uric acid thresholds predicting an increased total and cardiovascular mortality over 20 years. Hypertension. 2020;75(2):302–308. doi:10.1161/HYPERTENSIONAHA.119.13643
30. Fujihashi T, Sakata Y, Nochioka K, et al. Prognostic impacts of serum uric acid levels in patients with chronic heart failure: insights from the CHART-2 study. ESC Heart Fail. 2021;8(2):1027–1038. doi:10.1002/ehf2.12765
31. Daiber A, Hahad O, Andreadou I, et al. Redox-related biomarkers in human cardiovascular disease - classical footprints and beyond. Redox Biol. 2021;42:101875. doi:10.1016/j.redox.2021.101875
32. Maloberti A, Bossi I, Tassistro E, et al. Uric acid in chronic coronary syndromes: relationship with coronary artery disease severity and left ventricular diastolic parameter. Nutr Metab Cardiovasc Dis. 2021;31(5):1501–1508. doi:10.1016/j.numecd.2021.01.023
33. Qin L, Yang Z, Gu H, et al. Association between serum uric acid levels and cardiovascular disease in middle-aged and elderly Chinese individuals. BMC Cardiovasc Disord. 2014;14(1):26. doi:10.1186/1471-2261-14-26
34. Mazidi M, Katsiki N, Mikhailidis DP, et al. Associations of serum uric acid with total and cause-specific mortality: findings from individuals and pooling prospective studies. Atherosclerosis. 2020;296:49–58. doi:10.1016/j.atherosclerosis.2019.07.019
35. Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. JAMA. 2000;283(18):2404–2410. doi:10.1001/jama.283.18.2404
36. Kamei K, Konta T, Ichikawa K, et al. Serum uric acid levels and mortality in the Japanese population: the Yamagata (Takahata) study. Clin Exp Nephrol. 2016;20(6):904–909. doi:10.1007/s10157-016-1228-1
37. Winder M, Owczarek AJ, Mossakowska M, et al. Serum uric acid is a weak Independent predictor of overall survival in older adults. J Clin Med. 2021;10(19):4505. doi:10.3390/jcm10194505
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.