")
Back to Journals » OncoTargets and Therapy » Volume 14
Prognostic Significance of Preoperative Lymphocyte-to-C-Reactive Protein Ratio in Patients with Non-Metastatic Colorectal Cancer
Authors Ou W , Zhou C , Zhu X, Lin L, Xu Q
Received 4 November 2020
Accepted for publication 31 December 2020
Published 12 January 2021 Volume 2021:14 Pages 337—346
DOI https://doi.org/10.2147/OTT.S290234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Wenting Ou,1 Caijin Zhou,2 Xiaoqing Zhu,2 Lin Lin,2 Qingwen Xu2
1Department of Oncology, The Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong 524001, People’s Republic of China; 2Department of Gastrointestinal Surgery, The Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong 524001, People’s Republic of China
Correspondence: Caijin Zhou
Department of Gastrointestinal Surgery, The Affiliated Hospital of Guangdong Medical University, No. 57, South of Renmin Avenue, Zhanjiang, Guangdong 524001, People’s Republic of China
Email [email protected]
Background: The inflammatory indexes are attracting increasing attention as a prognostic predictor for colorectal cancer (CRC). However, the prognostic value of the preoperative lymphocyte-to-C-reactive protein ratio (LCR) in patients with non-metastatic CRC remains to be established.
Methods: A total of 955 patients from 2010 to 2014 at a single center were included. Receiver operating characteristic curves (ROC) were generated to define the optimal cutoff value of the inflammatory indexes, and the areas under the curve (AUC) were calculated to compare the predictive value among the inflammatory indexes. The Fine and Gray competing risk regression model and Cox proportional hazard model were used to determine the prognostic factors for cancer-specific survival (CSS) and overall survival (OS) by using sub-distribution hazard ratio (SHR) and hazard ratio (HR) as size effects, respectively.
Results: A ratio of 6500 was defined as the optimal cutoff value for LCR for dividing CRC patients into the high (> 6500, n = 528) and low (≤ 6500, n = 427) LCR groups. The LCR had the highest value of prognostic prediction among all inflammation-based scores. Low LCR was significant correlated with several clinicopathological features of tumor invasion and development. The patients with low LCR had poorer CSS and OS as compared to those with high LCR. Multivariate analyses showed that low LCR was independently associated with worse OS (HR = 0.61, 95% CI: 0.53– 0.70) and CSS (SHR = 0.55, 95% CI: 0.43– 0.71).
Conclusion: Preoperative LCR can be a useful biomarker for prognostic prediction in non-metastatic CRC patients with a better predictive value than other inflammatory indexes.
Keywords: lymphocyte-to-C-reactive protein ratio, colorectal cancer, prognosis, competing risk model
Introduction
Globally, colorectal cancer (CRC) accounts for about 10% of all newly diagnosed malignancies and cancer-related deaths per year.1 According to the reports from the International Agency for Research on Cancer in 2018, CRC contributed to approximately 1.8 million new cases and 900,000 deaths, making it the third most frequent cancer and the second leading cause of cancer deaths worldwide.2 While CRC incidence keeps stable at high levels or even begins to decline in some affluent Western countries, incidence rates continue to increase strongly with economic development in other countries, which may probably due to population growth, demographic aging, and unfavorable trends in major risk factors such as physical inactivity, overweight, obesity, and Western dietary habits.3
At present, curative-intent treatment for CRC, especially the early stage, is still predominantly surgical resection. Despite recent advances in diagnostic techniques and comprehensive therapy, more than half of CRC patients are diagnosed at an advanced stage, and recurrence or distant metastasis remains the main cause of poor prognosis.4 Until now, the most common prognostic factor for CRC is the Tumor-Node-Metastasis (TNM) staging system. However, each patient and tumor is unique. Heterogeneity in survival outcomes has been observed among the patients with the same stage, indicating that the accuracy level of the TNM staging system is still controversial.5 Given that patients with a high risk of poor prognosis have to undergo additional treatments, more precise predictors should be developed to supplement the current staging system and improve therapeutic decisions.
The interaction between systematic inflammation and the local immune response has been shown to promote the development and progression of CRC.6 The severity of cancer-related inflammation is determined by the levels of several serum components, including neutrophils, lymphocytes, platelets, and acute-phase proteins such as C-reactive protein (CRP).7,8 Accumulating evidence have suggested that the combinations of these systematic inflammatory parameters, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR), can provide prognostic information in some malignancies, including CRC.9,10 Recently, another alternative composite inflammatory index, lymphocyte-to-C-reactive protein (LCR), represented as a combination of circulating lymphocyte and C-reactive protein counts, has been gained notable attention as a prognostic factor in gastric cancer, rectal cancer, and cholangiocarcinoma.11–13 However, the prognostic potential of LCR has not been explored for patients with non-metastatic CRC. Moreover, it remains unclear which combination of inflammatory markers might be best in predicting survival outcome in patients with CRC. This study aimed to investigate the prognostic significance of LCR in patients with non-metastatic cancer and determine whether it was better than other inflammatory indexes.
Patients and Methods
Study Population
Our study enrolled 955 patients with non-metastatic CRC (Stage I-III) who underwent laparoscopic resection at the Affiliated Hospital of Guangdong Medical University from January 2010 to December 2014. The inclusion criteria were defined as follows: (1) histology confirmed newly diagnosed adenocarcinoma; (2) age older than 18 years; (3) without previous anticancer treatment or surgery; (4) available clinical information and blood test data; (5) complete follow-up data. Patients were excluded if they had another malignancy, end-stage liver disease, or chronic inflammatory disease including autoimmune disorder and infection. This study was approved by the Ethics Committee of the Affiliated Hospital of Guangdong Medical University and was conducted in accordance with the Declaration of Helsinki. Because this study was retrospectively designed, written informed consent was waived, but patients’ confidentiality was protected by the research institution and the researchers.
Data Collection
The following information was extracted from electronic medical records: sex, age at diagnosis, tumor site, histological differentiation, clinical stage, pT stage, pN stage, and maximum tumor diameter. The laboratory test results obtained from the same blood samples were collected within 1 week before surgery, including lymphocyte, neutrophil, platelet, monocyte, CRP, and carcinoembryonic antigen (CEA). The inflammatory indexes were calculated as following: (1) LCR = lymphocyte count (number/L)/CRP (mg/L); (2) NLR = neutrophil count (number/L)/lymphocyte count (number/L); (3) PLR = platelet count (number/L)/lymphocyte count (number/L); and (4) LMR = lymphocyte count (number/L)/monocyte count (number/L). The upper level of serum CEA was 5 ng/mL. Tumors were staged according to the 8th edition of the American Joint Committee on Cancer (AJCC) guidelines.
Treatment
All patients were treated with laparoscopic surgery with standard curative resection. Patients with Stages II-III additionally received adjuvant chemotherapy after surgery, including mFOLFOX6 and CAPOX regimens. The regimen of mFOLFOX6 consisted of oxaliplatin 85 mg/m2 in a 3-h infusion, racemic leucovorin 400 mg/m2 in a 2-h infusion, bolus fluorouracil 400 mg/m2 on day 1, and a 46-h infusion of fluorouracil 2400 mg/m2, which was repeated every 2 weeks for 12 cycles. The CAPOX regimen contained oxaliplatin 130 mg/m2 in a 3-h infusion on day 1 and capecitabine 1000 mg/m2 twice daily on day 1–14, which was every 3 weeks for 8 cycles. Dosage adjustments during chemotherapy were conducted if absolute platelet count was lower than 25,000 cells/μL, and chemotherapy was discontinued if Grade 4 toxic effects developed.
Follow-Up
After all the treatments have been completed, all patients were routinely followed up every 3 months for the first 3 years, every 6 months for the following 3 years, and annually thereafter. Patients’ follow-up was completed up to December 31, 2019. The median follow-up period was 44 months with a range from 2 to 83 months. The primary endpoint of this study was cancer-specific survival (CSS), which was measured from the date of surgery to death due to CRC in the absence of other causes. The secondary endpoint was overall survival (OS), which was defined as the time from surgery until the date of death from any cause.
Statistics
The optimal cutoff values of inflammatory indexes in this study were determined through receiver characteristic (ROC) curve analyses using the primary endpoint of OS and CSS to avoid a predetermined cutoff point. The best cutoff value of LCR was defined as 6500 because it was related to the maximum Youden index (sensitivity + specificity - 1), and all patients were divided into either high or low LCR groups accordingly. Similarly, the most appropriate cutoff values for NLR, PLR, and LMR were 3.68, 175, and 4.15, respectively, to classify the patients into high or low risk subsets. The DeLong and bootstrap tests were applied to compare the area under the curve (AUC) between LCR and other inflammatory indexes.14
Categoric variables were compared using the χ2 test or Fisher’s exact test. In the presence of competing events, we treated the non-cancer specific death and death before tumor progression as competing events for CSS. The impact of LCR on CSS was measured by the cumulative incidence function (CIF) of the competing risk model, and the equality in the CIFs across groups was determined by the Gray’s test. In order to identify the variables associated with CSS, univariate and multivariate analyses were performed in sequence by the Fine and Gray proportional sub-distribution hazard model, of which sub-distribution HRs (SHR) and 95% confidence intervals (CIs) were calculated.15 The survival curve was estimated through the Kaplan-Meier (KM) method to explore the effect of LCR on OS, and the between-group difference was determined by the Log rank test. The parameters associated with OS were identified by the Cox proportional hazards regression model for univariate and multivariate survival analyses, in which size effects were reported by hazard ratios (HRs) and 95% CIs. All the statistical analyses were performed with R software version 3.5.3. All tests were two-sided with P values less than 0.05 regarded as statistically significant.
Results
Patient Characteristics
Baseline and clinical characteristics of the enrolled patients are summarized in Table 1. A total of 955 patients were included in this study, of which the median age was 65 years old with a range from 18 to 85 years old and 540 cases (56.54%) were males. Most patients had tumor located in colon (n = 695, 72.77%) and showed well or moderate differentiation (n = 759, 79.48%). Among the patients, 333 cases had Stage II malignancy (34.87%), 566 cases were classified as T3 (59.27%), and 395 cases had no lymph nodal involvement (41.36%). The maximum tumor diameter ranged from 10 to 110 mm with a median value of 55 mm. Approximate two-thirds of patients had negative serum CEA levels (< 5 ng/mL).
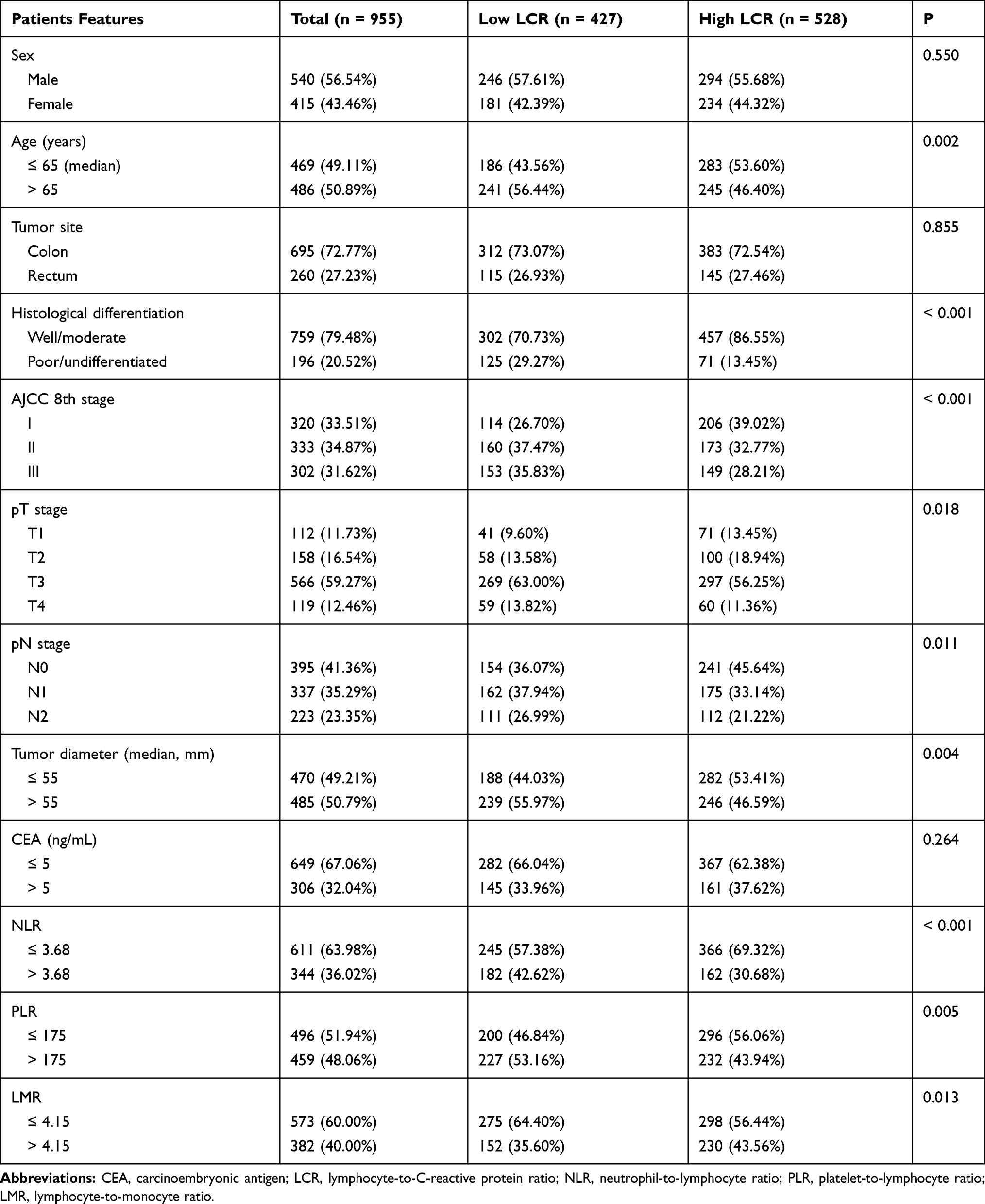 |
Table 1 Clinicopathological Features of the Included Patients |
Prognostic Value of LCR as Compared to Other Inflammatory Indexes
To compare the predictive value of LCR with other inflammatory indexes for prognosis, we calculated the AUCs of the ROC curves for all inflammatory indexes (Table 2). For OS, the LCR had the higher AUC value (0.748) as compared to NLR (AUC = 0.675, P = 0.032), PLR (AUC = 0.666, P = 0.018), and LMR (AUC = 0.650, P = 0.004). With respect to CSS, the AUC of LCR (0.750) was also superior to NLR (AUC = 0.680, P = 0.039), PLR (AUC = 0.672, P = 0.024), and LMR (AUC = 0.659, P = 0.004).
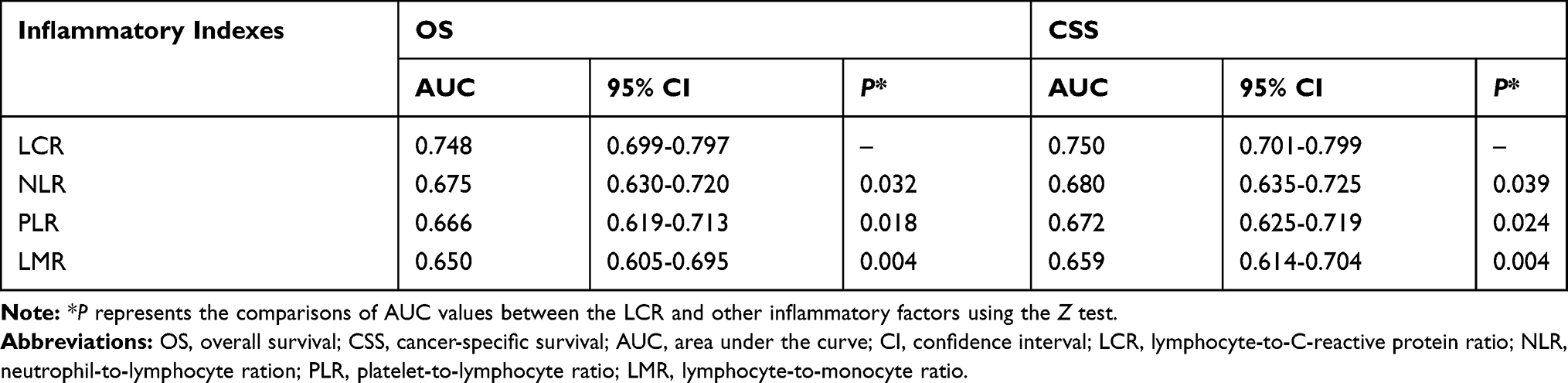 |
Table 2 Comparison of the AUC Between the LCR and Other Systematic Inflammatory Factors |
Correlation Between LCR and Clinicopathological Features
A total of 528 and 427 patients were classified into the high (> 6500) and low (≤ 6500) LCR group, respectively, according to the optimal cutoff value of LCR. As shown in Table 1, the low LCR level was significantly associated with poor clinical characteristics, such as worse histological differentiation (P < 0.001), advanced tumor stage (P < 0.001), advanced T stage (P = 0.018), positive lymph node metastasis (P = 0.011), larger tumor diameter (P = 0.004). Moreover, the patients with decreased LCR had significantly older age (P = 0.002), higher NLR (P < 0.001), higher PLR (P = 0.005), and lower LMR (P = 0.013).
Correlation Between LCR and Prognosis
The 5-year OS and CSS of the whole cohort were 76.5% and 80.8%, respectively. The 5-year OS and CSS of the high LCR group versus the low LCR group were 80.4% vs 72.0% (P = 0.003, Figure 1A), and 82.9% vs 78.7 (P = 0.027, Figure 1A), respectively.
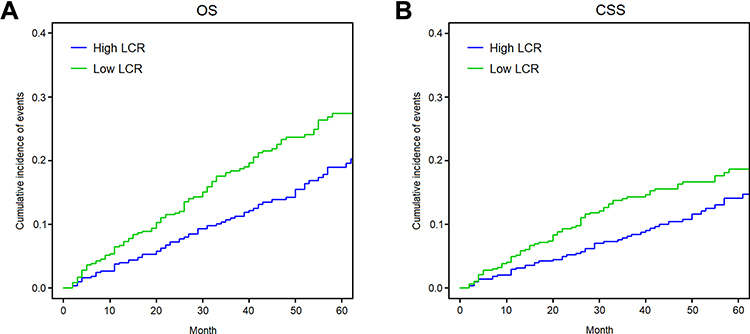 |
Figure 1 Cumulative incidence of all-cause death (A) and cancer-specific death (B) in nonmetastatic colorectal cancer patients with preoperative lymphocyte-to-C-reactive protein ratio ≤ 6500 or > 6500. We defined the all-cause death as the targeted event for overall survival and cancer-specific death for cancer-specific survival. The Kaplan-Meier method was used to generate the cumulative incidence of all-cause death, while the cumulative incidence function considering the competing events was used to obtain the cumulative incidence of cancer-specific death. |
The results of the univariate and multivariate analyses concerning the survival outcomes of OS and CSS are shown in Tables 3 and 4, respectively. Univariate analyses suggested that patients in the low LCR group had worse OS (HR = 0.53, 95% CI: 0.47–0.61, P < 0.001; Table 3) and CSS (SHR = 0.48, 95% CI: 0.35–0.62, P < 0.001; Table 4). Moreover, after adjusted by the confounding factors with statistical significance in the univariate analyses, including age, histological differentiation, T stage, N stage, serum CEA, NLR, PLR, and LMR, multivariate analyses indicated that the LCR was an independent prognostic factor for OS (HR = 0.61, 95% CI: 0.53–0.70, P < 0.001; Table 3) and CSS (SHR = 0.55, 95% CI: 0.43–0.71, P < 0.001; Table 4).
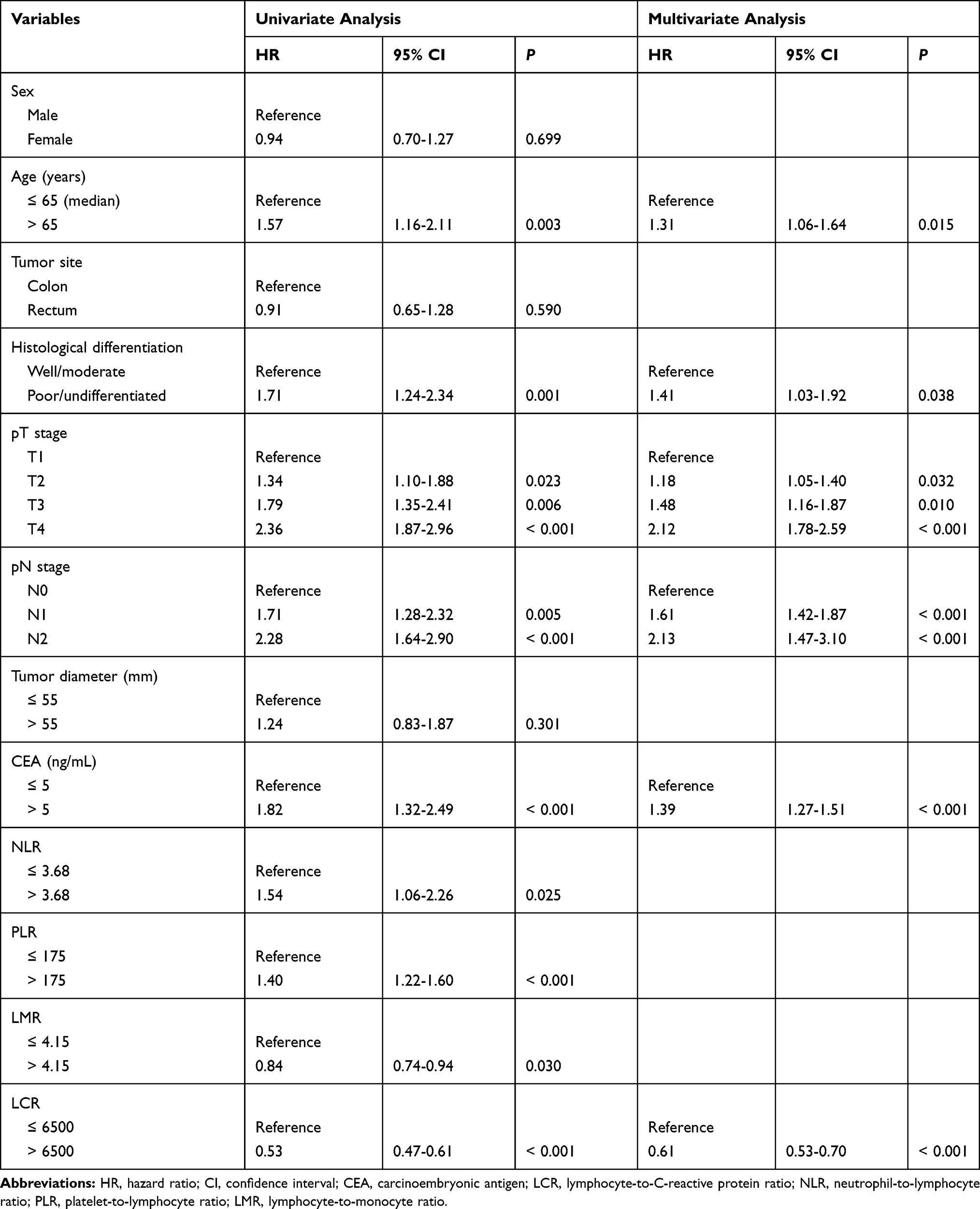 |
Table 3 Univariate and Multivariate Analyses of Overall Survival by Cox Proportion Hazard Regression |
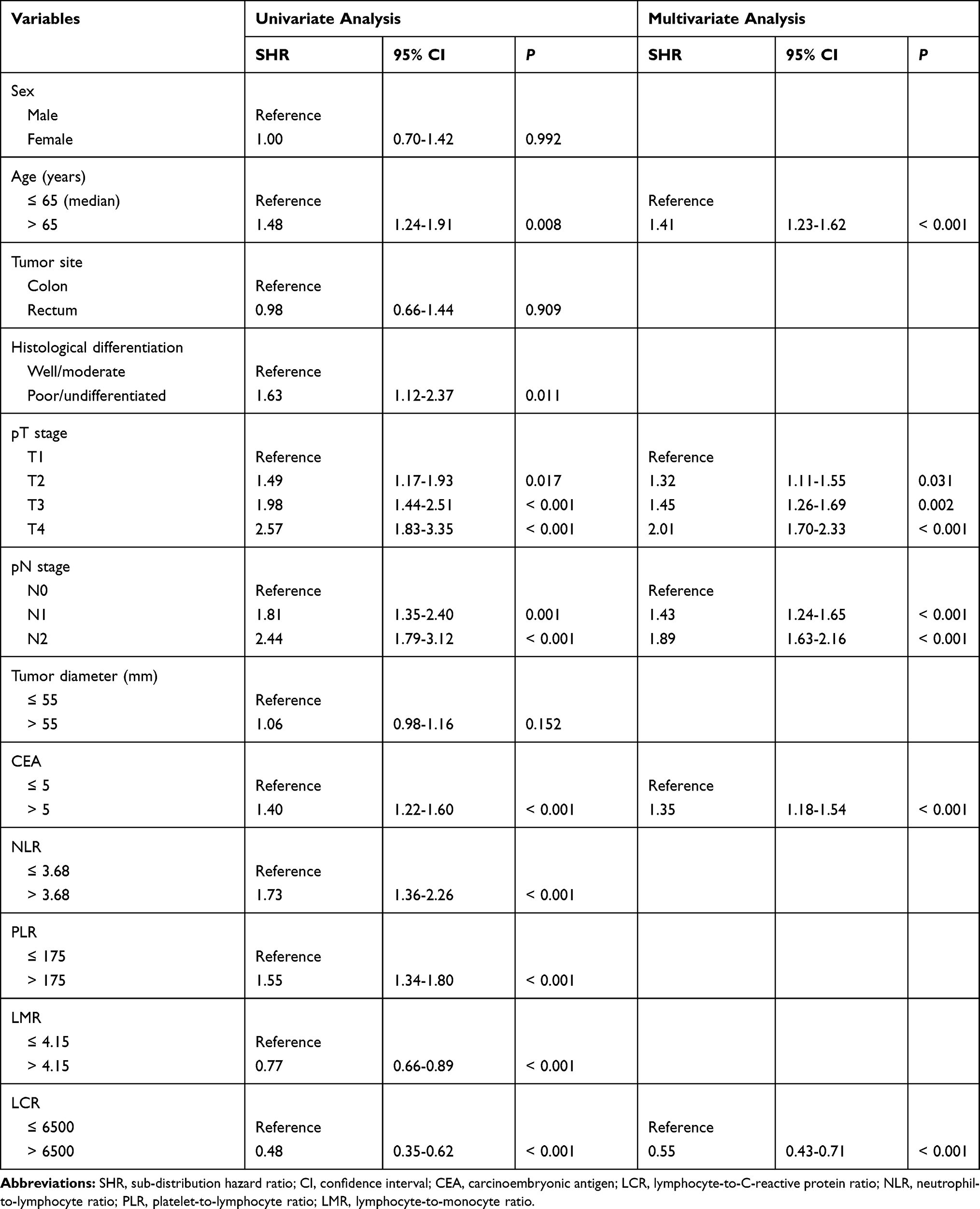 |
Table 4 Univariate and Multivariate Analyses of Cancer-Specific Survival by Fine and Gray Proportional Sub-Distribution Hazard Model |
Discussion
Various types of systematic inflammatory indexes have been frequently used to be prognostic factors in solid tumors.16 However, the optimal choice of the composite indexes based on the peripheral blood examination for predicting the long-term survival outcome in CRC patients remains uncertain. In this study, we validated the prognostic values of various combinations of systematic inflammatory parameters in patients with non-metastatic CRC, and obtained the following important findings: 1) non-metastatic CRC patients with decreased preoperative LCR level had poor prognosis in terms of OS and CSS; 2) LCR had a superior accuracy in the prognostic prediction as compared with other composite inflammatory parameters; and 3) a low level of LCR was prominent among patients with tumor progression, suggesting that these patients would be probably to benefit more from preoperative LCR measurement for clinical-decision making. Therefore, we believed that preoperative LCR can be served as a useful and effective index for the algorithm concerning the prognostic significance in patients with non-metastatic CRC.
Projection of postoperative prognosis in CRC patients is critical for decision-making of clinical treatment. In this regard, biomarkers that reflect the patients’ inflammation status have attracted considerable attention. CRP is a representative acute-phase protein whose level rapidly increases in response to the inflammation status.17 In clinical practice, CRP has been a definitive marker to evaluate the inflammation status in vivo. Tumor growth or invasion triggers the inflammatory response of the surrounding tissue and further promotes the release of pro-inflammatory cytokines, such as IL-6, resulting in an increased production of CRP.18 Therefore, cancer patients, including those with CRC, often have an elevated CRP level. In fact, previous studies have revealed that preoperative CRP might be a prognostic indicator in patients with CRC.19 Lymphocytes are a pivotal player in the tumor microenvironment, of which the subtypes, including CD3+ T cells, CD8+ T cells, Th1 CD4+ T cells, and natural killer cells, are essential to the anti-cancer activity.20 A high level of tumor-infiltrating lymphocytes surrounding the primary tumor site has been reported to be strongly associated with a favorable prognosis in CRC.21 Lymphopenia has been found in many human malignancies and is often correlated to disease severity, immunosuppression status, and poor survival outcome.22 Therefore, low LCR, caused by a decreased lymphocyte count and increased CRP level, denotes that the immunological response has been impaired and the tumor microenvironment is skewed to a pro-tumor inflammatory status, leading to tumor progression and worse prognosis.
As LCR can be measured quickly, noninvasively, and inexpensively, it is frequently used in clinical settings, which allows us to take advantage of our current understandings of the systematic inflammatory response in cancer patients. This has some profound implications for clinical practice. Firstly, the incorporation of the LCR into routine assessment may help to guide long-term prognosis. Secondly, the routine use of preoperative LCR may also guide the postoperative therapeutic strategies by targeting the systematic inflammatory response itself. Indeed, it is well known that cancer-associated systematic inflammation can cause many consequences and may finally lead to chronic cancer-related wasting, cachexia.23 However, this process can be attenuated using nonsteroidal anti-inflammatory drugs.24 Thus, incorporating LCR into the management of cancer patients may be conducive to improve the prognosis. For instance, among CRC patients with Stage III, those with a low level of preoperative LCR may benefit from concurrent chemoradiotherapy alone, whereas those with increased LCR may benefit from the addition of anti-inflammatory agents.25,26 However, it is necessary to validated by prospective studies with the incorporation of both routine assessments of the systematic inflammatory response and use of anti-inflammatory agents.
Except for LCR, independent factors associated with poor prognosis in patients with non-metastatic CRC included age, histological differentiation, T stage, N stage, and serum CEA level according to the multivariate analysis. First, older patients had worse survival outcomes than younger patients, which might be probably attributed to the higher risk of perioperative comorbidities in older patients.27 Second, worse histological differentiation was related to poor prognosis, which can be a useful supplement of the current TNM staging system. Third, the magnitude of poor prognosis was consistent with the changes in T stage and N stage, which are the primary components of the TNM staging system. Finally, patients with high CEA level represented unfavorable prognosis during the follow-up period, indicating that preoperative CEA measurement should be incorporated into the comprehensive assessment to identify patients with a high risk of cancer-related death.28
Previous reports by Suzuki et al showed that LCR might be most useful to predict OS and disease-free survival in patients with stage II and III colon cancer among the 16 systematic inflammatory biomarkers, including NLR, PLR, and LMR.29 Similarly, several researchers demonstrated that the LCR was the most reliable prognostic indicator as compared to other inflammatory indexes in patients with gastric cancer and renal cell cancer.11,12 The present study also found that the operative LCR had the strongest discriminative ability in assessing the survival outcome of non-metastatic CRC and might complement the existing AJCC staging system to a certain degree.
Some limitations of this study should be acknowledged. First, although this study contained a relatively large cohort, it was retrospectively designed, of which the data were retracted from medical records and lacked consistent clinical data collection and record-keeping. Second, the cutoff value of LCR needs to be further validated. Third, because the LCR may have changed during treatment, whether this alternation can predict oncological outcomes is still unknown. Fifth, some therapeutic factors, such as the efficacy of chemotherapy and postoperative adverse reactions, might affect the prognosis; however, we were unable to analyze the effect of LCR on these outcomes due to insufficient information. Finally, with all patients included in this study were from a single institution, our results require external validation. To overcome these shortcomings, multicenter prospective studies are needed.
Conclusion
In conclusion, this study provided novel evidence for the prognostic value of LCR in patients with non-metastatic CRC. Our study demonstrated that the low level of preoperative LCR was significantly associated with poor survival outcomes, and outperformed other composite inflammatory indexes in predictive accuracy. Therefore, the preoperative LCR may provide more detailed prognostication and could be used as an effective tool for prognostic assessment in routine clinical settings due to its convenience, inexpensiveness, and simpleness. Quantification of the preoperative LCR may be helpful for patient classification and clinical decision-making on further therapy and follow-up strategies for clinicians.
Acknowledgments
This study was supported by Guangdong Province Medical Scientific Research Fund Project (No. A2019537), Guangdong Medical University Scientific Research Fund Project (No. GDMUM201806), and Affiliated Hospital of Guangdong Medical University Clinical Research Program (No. LCYJ2019C001). The funding agency had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394:1467–1480. doi:10.1016/S0140-6736(19)32319-0
2. International Agency for Research on Cancer. Globocan 2018: cancer fact sheets colorectal cancer. IARC. 2018.
3. Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. 2019;16:713–732.
4. Brenner H, Chen C. The colorectal cancer epidemic: challenges and opportunities for primary, secondary and tertiary prevention. Br J Cancer. 2018;119:785–792. doi:10.1038/s41416-018-0264-x
5. Li C, Yang J, Xu F, et al. A prognostic nomogram for the cancer-specific survival of patients with upper-tract urothelial carcinoma based on the surveillance, epidemiology, and end results database. BMC Cancer. 2020;20:534. doi:10.1186/s12885-020-07019-5
6. Chen J, Pitmon E, Wang K. Microbiome, inflammation and colorectal cancer. Semin Immunol. 2017;32:43–53. doi:10.1016/j.smim.2017.09.006
7. Tuomisto AE, Mäkinen MJ, Väyrynen JP. Systemic inflammation in colorectal cancer: underlying factors, effects, and prognostic significance. World J Gastroenterol. 2019;25:4383–4404. doi:10.3748/wjg.v25.i31.4383
8. Chen JH, Zhai ET, Yuan YJ, et al. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J Gastroenterol. 2017;23:6261–6272. doi:10.3748/wjg.v23.i34.6261
9. Tan D, Fu Y, Tong W, Li F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. Int J Surg. 2018;55:128–138. doi:10.1016/j.ijsu.2018.05.030
10. Xia LJ, Li W, Zhai JC, Yan CW, Chen JB, Yang H. Significance of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and prognostic nutritional index for predicting clinical outcomes in T1-2 rectal cancer. BMC Cancer. 2020;20:208. doi:10.1186/s12885-020-6698-6
11. Cheng CB, Zhang QX, Zhuang LP, Sun JW. Prognostic value of lymphocyte-to-C-reactive protein ratio in patients with gastric cancer after surgery: a multicentre study. Jpn J Clin Oncol. 2020;50:1141–1149. doi:10.1093/jjco/hyaa099
12. Okugawa Y, Toiyama Y, Fujikawa H, et al. Prognostic potential of lymphocyte-c-reactive protein ratio in patients with rectal cancer receiving preoperative chemoradiotherapy. J Gastrointest Surg Epub. 2020. doi:10.1007/s11605-019-04495-4
13. Lu LH, Zhong C, Wei W, et al. Lymphocyte-C-reactive protein ratio as a novel prognostic index in intrahepatic cholangiocarcinoma: A multicentre cohort study. Liver Int Epub. doi: 10.1111/liv.14567
14. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–845. doi:10.2307/2531595
15. Donoghoe MW, Gebski V. The importance of censoring in competing risks analysis of the subdistribution hazard. BMC Med Res Methodol. 2017;17:52. doi:10.1186/s12874-017-0327-3
16. Matsuoka H, Ando K, Hu Q, et al. Postoperative C-reactive protein/albumin ratio is a biomarker of risk of recurrence and need for adjuvant chemotherapy for stage III colorectal cancer. Int J Clin Oncol. 2020;25:1318–1326. doi:10.1007/s10147-020-01672-3
17. Holm M, Saraswat M, Joenväärä S, Ristimäki A, Haglund C, Renkonen R. Colorectal cancer patients with different C-reactive protein levels and 5-year survival times can be differentiated with quantitative serum proteomics. PLoS One. 2018;13:e0195354. doi:10.1371/journal.pone.0195354
18. Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Shibuya N, Kubota K. Clinical significance of the C-reactive protein to albumin ratio for survival after surgery for colorectal cancer. Ann Surg Oncol. 2016;23:900–907. doi:10.1245/s10434-015-4948-7
19. Yamamoto M, Saito H, Uejima C, et al. Prognostic value of the combination of pre- and postoperative C-reactive protein in colorectal cancer patients. Surg Today. 2018;48:986–993. doi:10.1007/s00595-018-1689-9
20. Silva TH, Schilithz AOC, Peres WAF, Murad LB. Neutrophil-lymphocyte ratio and nutritional status are clinically useful in predicting prognosis in colorectal cancer patients. Nutr Cancer. 2020;72:1345–1354.
21. Inamoto S, Kawada K, Okamura R, Hida K, Sakai Y. Prognostic impact of the combination of neutrophil-to-lymphocyte ratio and Glasgow prognostic score in colorectal cancer: a retrospective cohort study. Int J Colorectal Dis. 2019;34:1303–1315. doi:10.1007/s00384-019-03316-z
22. Jakubowska K, Koda M, Kisielewski W, Kańczuga-Koda L, Grudzińska M, Famulski W. Pre- and postoperative neutrophil and lymphocyte count and neutrophil-to-lymphocyte ratio in patients with colorectal cancer. Mol Clin Oncol. 2020;13:56. doi:10.3892/mco.2020.2126
23. VanderVeen BN, Fix DK, Carson JA. Disrupted skeletal muscle mitochondrial dynamics, mitophagy, and biogenesis during cancer cachexia: a role for inflammation. Oxid Med Cell Longev. 2017;2017:3292087. doi:10.1155/2017/3292087
24. Roxburgh CS, McMillan DC. Cancer and systemic inflammation: treat the tumour and treat the host. Br J Cancer. 2014;110:1409–1412. doi:10.1038/bjc.2014.90
25. Hamada T, Cao Y, Qian ZR, et al. Aspirin use and colorectal cancer survival according to tumor CD274 (Programmed Cell Death 1 Ligand 1) expression status. J Clin Oncol. 2017;35:1836–1844. doi:10.1200/JCO.2016.70.7547
26. Veettil SK, Lim KG, Ching SM, Saokaew S, Phisalprapa P, Chaiyakunapruk N. Effects of aspirin and non-aspirin nonsteroidal anti-inflammatory drugs on the incidence of recurrent colorectal adenomas: a systematic review with meta-analysis and trial sequential analysis of randomized clinical trials. BMC Cancer. 2017;17:763. doi:10.1186/s12885-017-3757-8
27. Wu JY, Wang YF, Ma H, Li SS, Miao HL. Nomograms predicting long-term survival in patients with invasive intraductal papillary mucinous neoplasms of the pancreas: A population-based study. World J Gastroenterol. 2020;26:535–549. doi:10.3748/wjg.v26.i5.535
28. Wang Y, Wu J, He H, et al. Nomogram predicting cancer-specific mortality in early-onset rectal cancer: a competing risk analysis. Int J Colorectal Dis. 2020;35:795–804. doi:10.1007/s00384-020-03527-9
29. Suzuki S, Akiyoshi T, Oba K, et al. Comprehensive comparative analysis of prognostic value of systemic inflammatory biomarkers for patients with stage II/III colon cancer. Ann Surg Oncol. 2020;27:844–852.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.