")
Back to Journals » International Journal of General Medicine » Volume 15
Prognostic Nomograms for Predicting Overall Survival and Cancer-Specific Survival in Patients with Head and Neck Mucosal Melanoma
Authors Lu Z, Zhou Y, Nie G, Miao B, Lu Y, Chen T
Received 10 December 2021
Accepted for publication 25 February 2022
Published 10 March 2022 Volume 2022:15 Pages 2759—2771
DOI https://doi.org/10.2147/IJGM.S352701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zhenzhang Lu,1,2,* Yuxiang Zhou,3,* Guohui Nie,1 Beiping Miao,1 Yongtian Lu,1 Tao Chen1
1Department of Otorhinolaryngology, The First Affiliated Hospital of Shenzhen University/Shenzhen Second People’s Hospital, Shenzhen, Guangdong Province, 518000, People’s Republic of China; 2Department of Otorhinolaryngology, South China Hospital of Shenzhen University, Shenzhen, Guangdong Province, 518000, People’s Republic of China; 3Department of Otorhinolaryngology, People’s Hospital of Shenzhen Baoan District, Shenzhen, Guangdong Province, 518000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tao Chen, Department of Otorhinolaryngology, The First Affiliated Hospital of Shenzhen University/Shenzhen Second People’s Hospital, No. 3002 Sungang West Road, Shenzhen, Guangdong Province, 518000, People’s Republic of China, Tel +86755-83366388, Email [email protected]
Background: Accurate forecasting of the risk of death is crucial for people living with head and neck mucosal melanoma (HNMM). We aimed to establish and validate an effective prognostic nomogram for HNMM.
Methods: Patients with HNMM who underwent surgery between 2010 and 2015 were selected from the Surveillance, Epidemiology, and End Results (SEER) database for model construction. After eliminating invalid and missing clinical information, 288 patients were ultimately identified and randomly divided into a training cohort (199 cases) and a validation cohort (54 cases). Univariate and multivariate Cox proportional hazards regression analyses were performed in the training cohort to identify prognostic variables. Independent influencing factors were used to build the model. Through internal verification (training cohort) and external verification (validation cohort), the concordance indexes (C-indexes) and calibration curves were used to evaluate the predictive value of the nomogram.
Results: For the training cohort, five independent risk predictors, namely age, location, T stage, N stage, and surgery, were selected, and nomograms with estimated 1- and 3-year overall survival (OS) and cancer-specific survival (CSS) were established. The C-index showed that the predictive performance of the nomogram was better than that of the TNM staging system and was internally verified (through the training queue: OS: 0.764 vs 0.683, CSS: 0.783 vs 0.705) and externally verified (through the verification queue: OS: 0.808 vs 0.644, CSS: 0.823 vs 0.648). The calibration curves also showed good agreement between the prediction based on the nomogram and the observed survival rate.
Conclusion: The nomogram prediction model can more accurately predict the prognosis of HNMM patients than the traditional TNM staging system and may be beneficial for guiding clinical treatment.
Keywords: head and neck mucosal melanoma, SEER, nomogram, overall survival, cancer-specific survival
Introduction
Melanoma can be divided into uveal tract, cutaneous and mucosal melanoma (MM) according to the primary location of the tumor. Their clinical manifestations and pathological characteristics are quite different.1 Head and neck mucosal melanoma (HNMM) is a rare and aggressive disease that accounts for 1–4% of all melanomas and 50–60% of all MMs.2–4 A previous study showed that the incidence of HNMM in the United States has risen over time since 1987.5 The most common sites of HNMM are the nasal cavity, paranasal sinus and oral cavity, and HNMM rarely occurs in the nasopharynx, oropharynx, hypopharynx or larynx.6,7 Among the causes of skin MM, there is clear evidence that it is related to excessive exposure to ultraviolet light.8 However, the etiology of HNMM is still unclear but is not related to excessive UV exposure. The current possible factors associated with HNMM include bad dentures, smoking, mechanical trauma, and family history.9
The prognosis of HNMM is extremely poor, and the 5-year overall survival (OS) rate is only 20%-40%.10,11 Due to the rarity of HNMM, large-scale prospective trials cannot be performed to evaluate the efficacy of various treatment modalities, and the optimal treatment strategy remains uncertain. At present, various methods such as surgery, postoperative radiotherapy, postoperative chemotherapy, and targeted therapy are used to treat head and neck mucosal melanoma.12 However, surgery for early-stage lesions is still the preferred choice. Surgical resection to a negative margin and the surgeon’s management of HNMM patients in a multidisciplinary team (MDT) plays an important role.13–15 Besides, postoperative radiotherapy is still a controversial approach. The United Kingdom national guidelines concluded that there was insufficient evidence to suggest that conventional postoperative adjuvant radiation therapy was necessary for patients, and therefore adjuvant postoperative radiation therapy was recommended for patients with risk factors, thus helping to ensure local disease control.16 A recently published meta-analysis confirmed that surgery combined with postoperative adjuvant radiotherapy can control the local recurrence rate and reduce patient mortality. However, it also stated that the control effect of distant metastasis is unclear.17 Due to differences in biological characteristics, immunotherapy seems to be much less effective against mucosal melanoma than in cutaneous melanoma.18
Considering the poor prognosis of HNMM, high-risk HNMM should be accurately identified. Several risk stratifications have been established in previous studies. In 1970, Ballantyne19 proposed the Ballantyne staging system for HNMM based on the presence or absence of metastasis and treatment. Although the Ballantyne staging system is simple and easy to use, there are few patients with simple lymph node metastasis, as most of the lesions are classified as stage I. It is good to distinguish patients with different prognoses. For this reason, Prasad et al20 proposed a new staging method based on the Ballantyne staging system in 2004, which increased the assessment of the depth of invasion; however, this staging system requires surgery to be evaluated. In 2009, the American Joint Committee on Cancer (AJCC) established a specific TNM staging system for HNMM that defined three T stages, T3, T4a and T4b, but did not consider the location of the primary tumor. Although Moya-Plana et al21 proposed combining the TNM stage for HNMM and the primary tumor separately to improve the risk stratification of HNMM patients, it undoubtedly increases the practicality of clinical operations. In addition, patient age, treatment and other clinical factors may also play a role in the prognosis of HNMM. Considering the comprehensive influence of these different prognostic factors, it is necessary to propose a comprehensive prediction model that contains more prognostic information.
In recent years, the use of nomograms to construct predictive models has received increasing attention. By comprehensively considering a variety of prognostic indicators and quantifying risks with intuitive charts, nomograms have become a common tool for the prognostic evaluation of cancer patients. Therefore, this study aimed to construct an effective HNMM nomogram prediction model. HNMM patients were selected from the Surveillance, Epidemiology, and End Results (SEER) database,22 which has recorded in detail demographic information, such as tumor location and morphology, diagnostic stage, and treatment since 1973, and patients were randomly divided into a training cohort and an internal verification cohort. We selected independent risk factors through single-factor and multifactor Cox regression analyses and built a model. Finally, we propose a new predictive tool to guide clinical prognosis and treatment decisions.
Materials and Methods
Patient Enrollment and Variables
The data used in this study were extracted from the SEER database, which includes 18 registries and covers approximately 30% of the US population. The study cohort consisted of patients diagnosed with melanoma between 2010 and 2015 who were analyzed using SEER*Stat software (version 8.3.8), as previous data did not include TNM staging for these cases. The inclusion criteria were as follows: (1) diagnosis of melanoma (ICD-O-3 histology codes 8720–8790); (2) the sites were limited to the following ICD-O-3 codes: tongue mucosa (C00.3–C00.8) topographic map code (C01.9–C02.9), salivary glands (C07.9–C08.9), mouth (C04.0–C04.9), gums (C03.0–C03.9), other mouth (C05.0–C06.9), nasopharyngeal (C11.0–C11.9), tonsils (C09.0–C09.9), oropharynx (C10.0–C10.9), hypopharyngeal (C12.9–C13.9), other pharynx (C14.0–C14.8), nasal cavity (C30.0), middle ear (C30.1), paranasal sinuses (C31.0–C31.9) or throat (C32.0–C32.9); and (3) the survival time and cause of death were given. The exclusion criteria were as follows: (1) not the first primary tumor; (2) less than 18 years old; (3) the survival time and cause of death were not provided; (4) n race and age at diagnosis were not provided; (5) the clinical TNM stage was not provided; and (5) the use of surgery, radiotherapy, and chemotherapy was not provided.
From the SEER database, we collected the following clinical characteristics: age, race, sex, TNM stage, radiotherapy, chemotherapy, survival time, cause of death, and survival status. These steps of patient selection are shown in a flow diagram (Figure 1). X-Tile software (Yale University, New Haven, Connecticut, USA) was used to assess the optimal cutoff value of age (Figure 2). The best cutoffs for age were 69 years and 83 years.
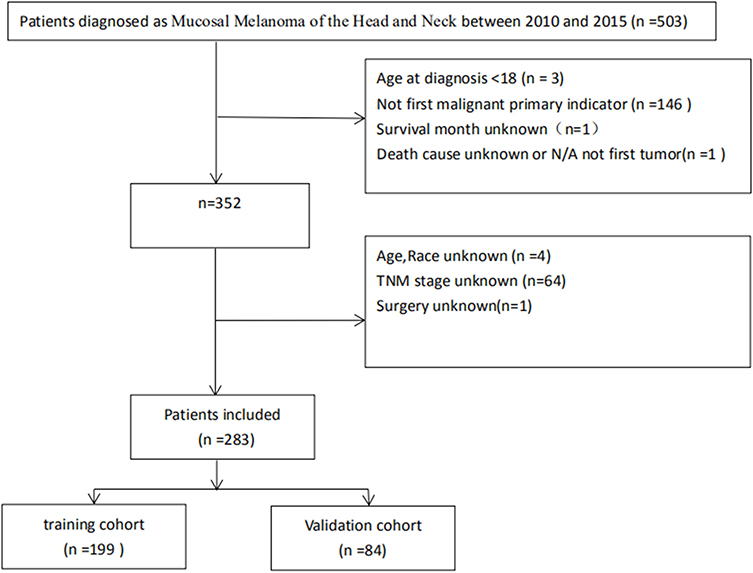 |
Figure 1 Flowchart of the patient selection in the study group. |
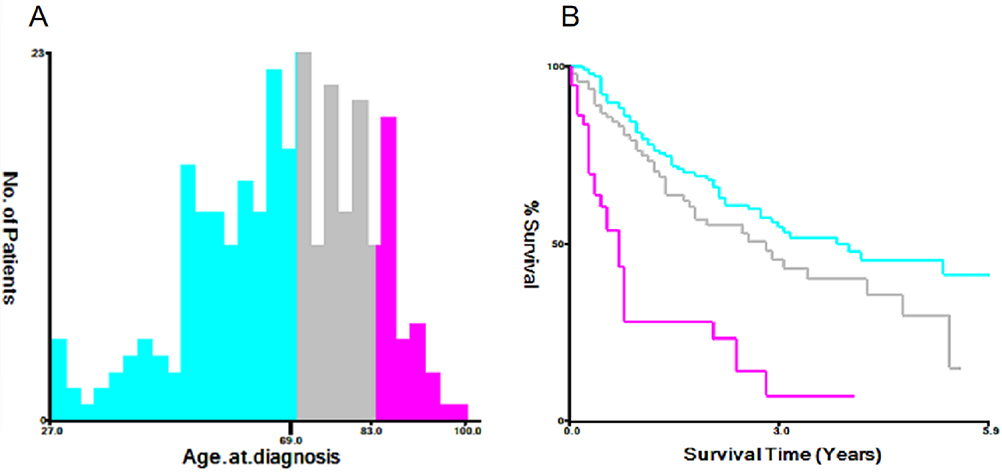 |
Figure 2 Identification of optimal cut-off values of year of diagnosis (A and B) via X-tile software analysis. |
According to the inclusion and exclusion criteria, patients were selected and randomly divided into a training cohort (n=199) and a validation cohort (n=84) at a ratio of 7:3. The study endpoints included cancer-specific survival (CSS) and OS, but the 1- and 3-year survival rates of these two endpoints were also considered.
OS was defined as the time from diagnosis to death from any cause. CSS was defined as the time from diagnosis to death due to a specific type of MM. Patients who were alive at the last follow-up were censored.
Statistical Analysis
The X 2 test was used to compare the performance of patients in the training and validation cohorts. Univariate Cox regression analysis was used to determine independent factors associated with survival time. Then, significant factors (P<0.2) were further identified through backward stepwise analysis in the multivariate Cox proportional hazards model. The results of the multivariate analyses were utilized to construct a nomogram for predicting 1- and 3-year OS and CSS. The nomogram was validated by constructing discrimination and calibration curves (bootstrapping with 1000 resamples) in both the development and validation cohorts. The concordance index (C-index), which measures the differences in predictive ability between observed and nomogram-predicted results, was used to evaluate the discrimination of the nomogram.
Results
Patient Characteristics
According to the inclusion and exclusion criteria, 283 of the 503 patients diagnosed with HNMM between 2010 and 2015 were registered in the SEER database. These patients were randomly divided into a training cohort (n=199) and a validation cohort (n=84). The basic information of these patients is listed in Table 1. There were no significant differences between the training and validation groups (P>0.05). Of these 283 patients, 233 were white (82.3%), and 50 were nonwhite (17.7%). The numbers of people aged ≤69, 69–83 and ≥83 years at the time of diagnosis were 149 (52.7%), 88 (31.1%) and 46 (16.3%), respectively. In all, 150 patients (53%) were female, and 133 patients (47%) were male. The numbers of patients with T stages T3, T4a, and T4b were 160 (56.5%), 98 (34.6%), and 25 (8.8%), respectively; those with N stages N0 and N1 were 236 (83.4%) and 47 (16.6%), respectively; and those with metastatic statuses of M0 and M1 were 250 (88.3%) and 33 (11.7%), respectively. The numbers of patients whose primary tumor was located in the sinuses, nasal cavity, oral cavity, and other sites were 41 (14.5%), 160 (56.5%), 69 (24.4%), and 13 (4.6%), respectively. In addition, most patients underwent surgery (83.7%), and approximately half of the patients received radiotherapy. The majority of people (90.5%) did not receive radiotherapy.
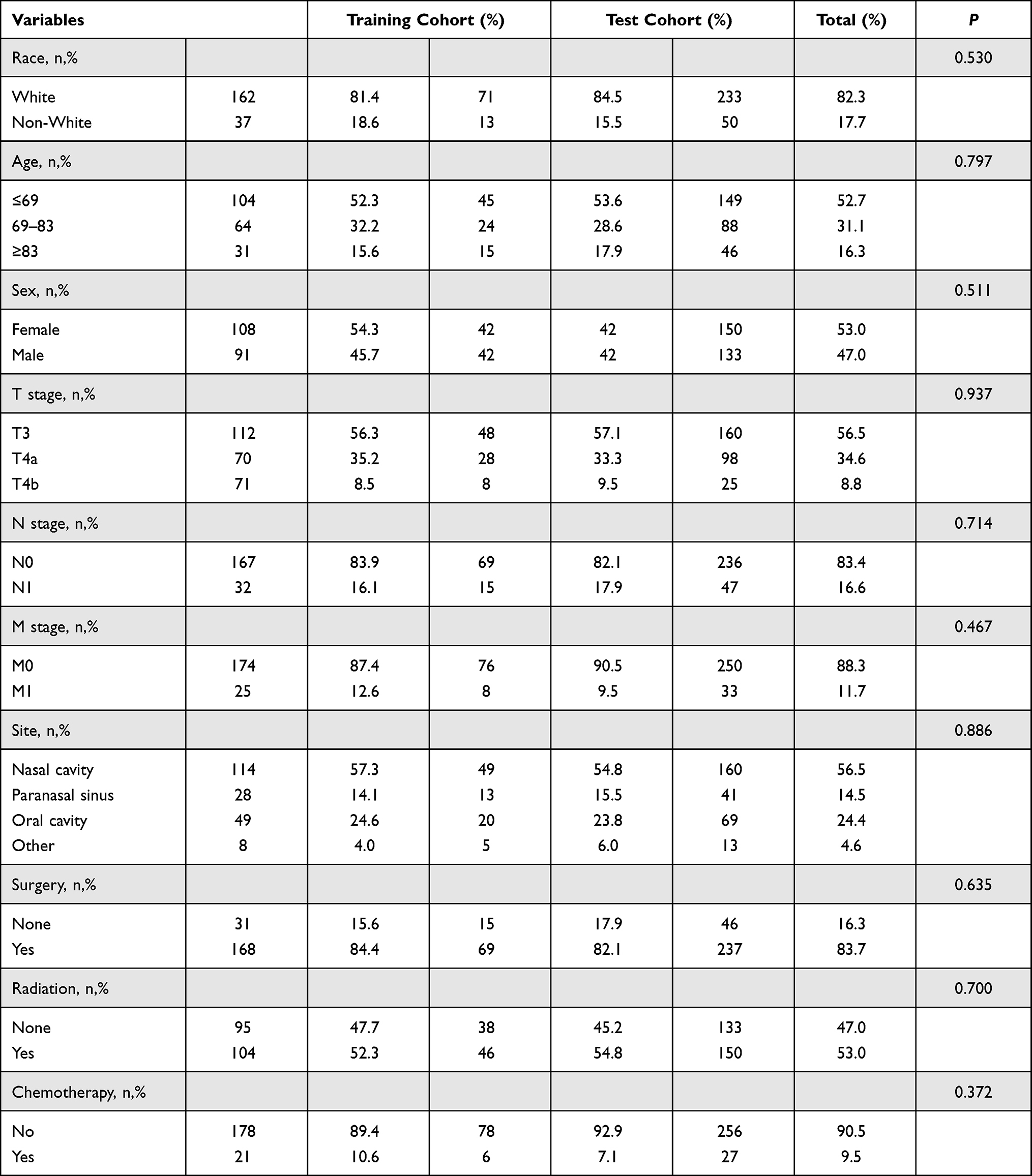 |
Table 1 Baseline Demographic and Clinical Characteristics of Patient with Mucosal Melanoma of the Head and Neck |
Factors Associated with OS and CSS
For the training cohort, in the univariate Cox regression analysis of OS and CSS, the variables age, T stage, N stage, M stage, site, and surgery were significant (P<0.05) (Table 2). We incorporated the significant factors (P<0.2) from the univariate analysis into the multivariate Cox regression analysis to control for confounding variables (Table 3). In the multivariate Cox analyses, age carried significant prognostic value for patients aged 69–83 years (hazard ratio (HR): 1.988, 95% confidence interval (CI) 1.183–3.341) and aged ≥83 years (HR: 2.905, 95% CI 1.447–5.832), and age ≥ 83 years was also significantly associated with disease-specific survival (DSS) (HR: 2.465, 95% CI 1.158–5.247). T4a classification (OS: HR 1.723, 95% CI 1.045–2.841; DSS: HR 1.940, 95% CI 1.133–3.323) and T4b classification (OS: HR 3.801, 95% CI 1.813–7.970; DSS: HR 3.774, 95% CI 1.686–8.449) were associated with the highest risk of death. Patients with a higher N status had poorer OS (HR: 2.979, 95% CI 1.586–5.597) and DSS (HR: 3.135, 95% CI 1.625–6.050), as did patients whose primary tumor was located in the sinuses (OS: HR 2.121, 95% CI 1.195–3.764; DSS: HR 2.071, 95% CI 1.108–3.870). Surgery was a significant independent predictor of both OS (HR: 0.471, 95% CI 0.248–0.897) and DSS (HR: 0.334, 95% CI 0.166–0.669).
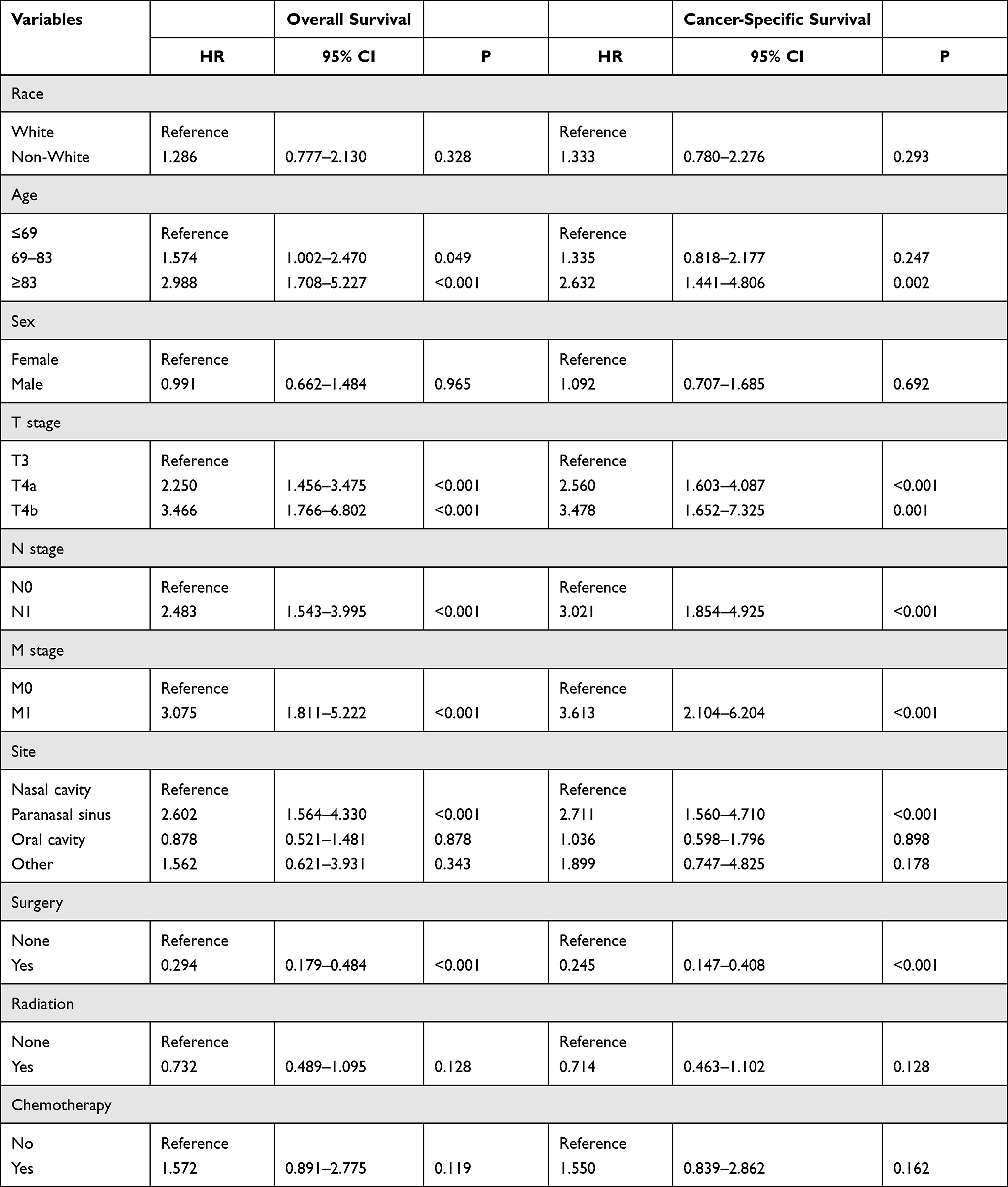 |
Table 2 Univariate Cox Regression Analysis of Overall Survival and Cancer-Specific Survival in the Training Cohort |
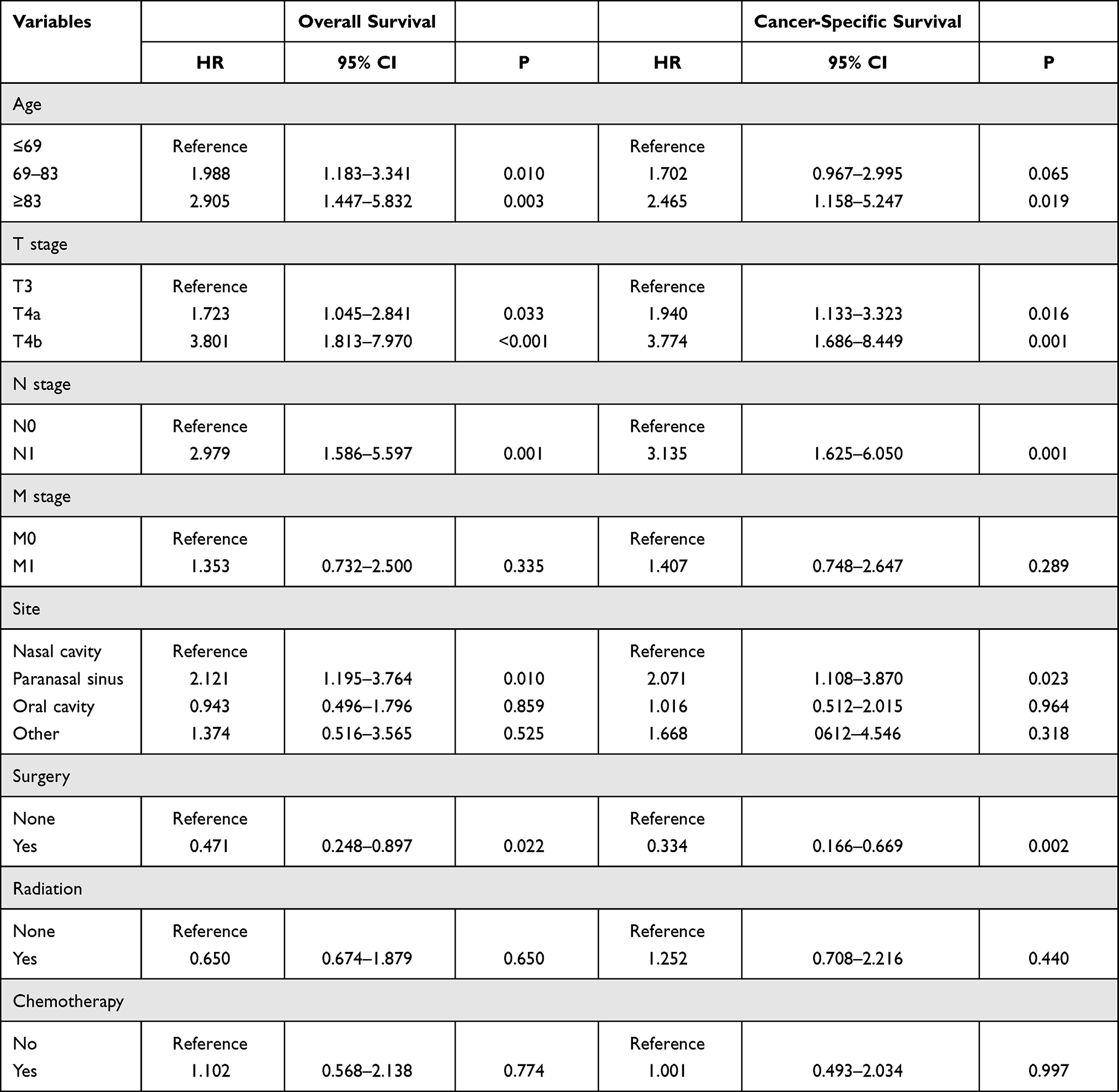 |
Table 3 Multivariate Cox Regression Analysis of Overall Survival and Cancer-Specific Survival in the Training Cohort |
Construction and Validation of the Nomograms for OS and CSS
Ultimately, patient age, T stage, N stage, site, and surgery were used to construct a nomogram in the training cohort for predicting 1- and 3-year OS and CSS (Figures 3 and 4). We validated the nomograms internally and externally. The C-index was used to evaluate the prediction accuracy of the nomogram. For internal verification of the nomogram, the C-indexes to predict OS and CSS were 0.764 (0.717–0.811) and 0.783 (0.734–0.832), respectively. For external verification of the nomogram, the C-indexes to predict OS and CSS were 0.808 (0.730–0.886) and 0.823 (0.754–0.832), respectively. We also compared the distinction between the nomogram and the AJCC staging system. In the training cohort, the C-indexes of the TNM staging system to predict OS and CSS were 0.683 (0.630~0.736) and 0.705 (0.650~0.760), respectively, both of which were lower than those of the current nomogram. In the validation cohort, the C-indexes of the TNM staging system to predict OS and CSS were 0.644 (0.542~0.746) and 0.648 (0.544~0.752), respectively. Moreover, calibration plots demonstrated an excellent correlation between the predicted and observed values of OS and CSS in the training and validation cohorts (Figures 5 and 6). Validation of both nomograms showed a good level of agreement with the predictive value.
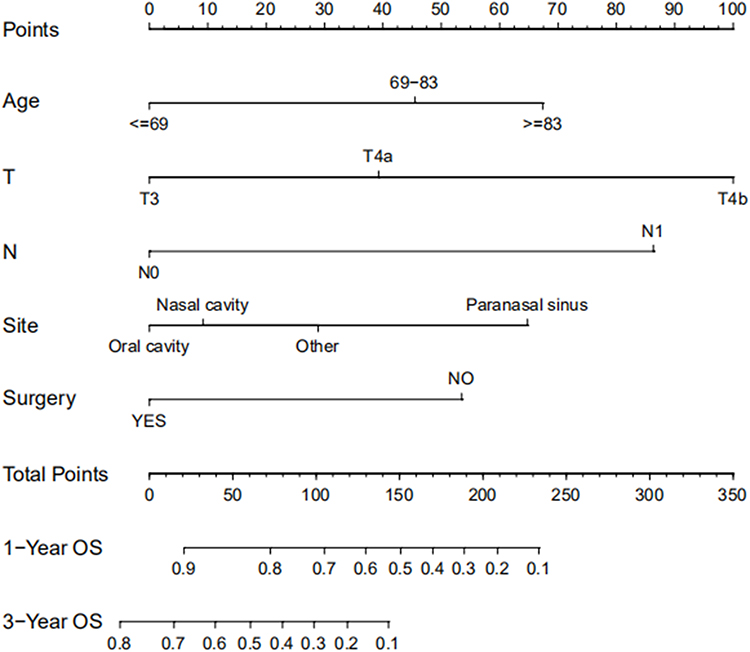 |
Figure 3 Nomogram estimating the 1- and 3-year overall survival of HNMM patients. |
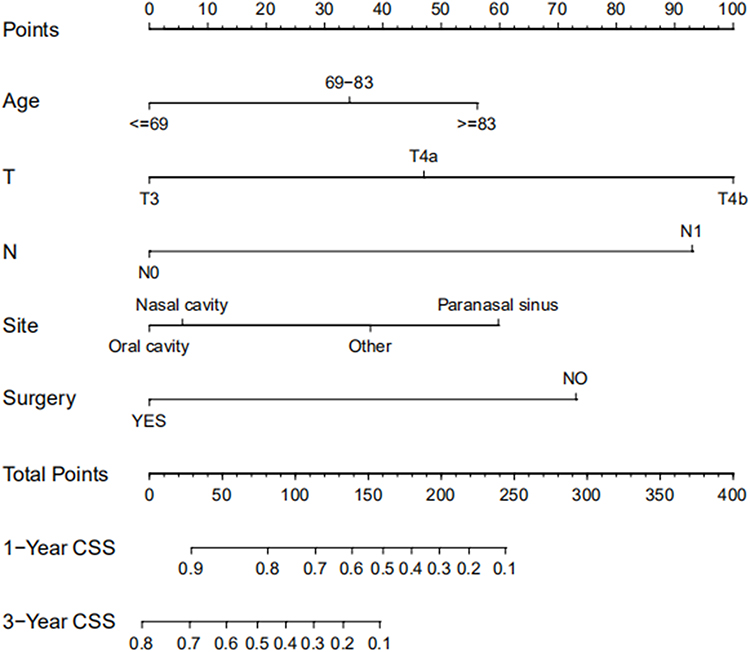 |
Figure 4 Nomogram estimating the 1-and 3-year cancer-specific survival of HNMM patients. |
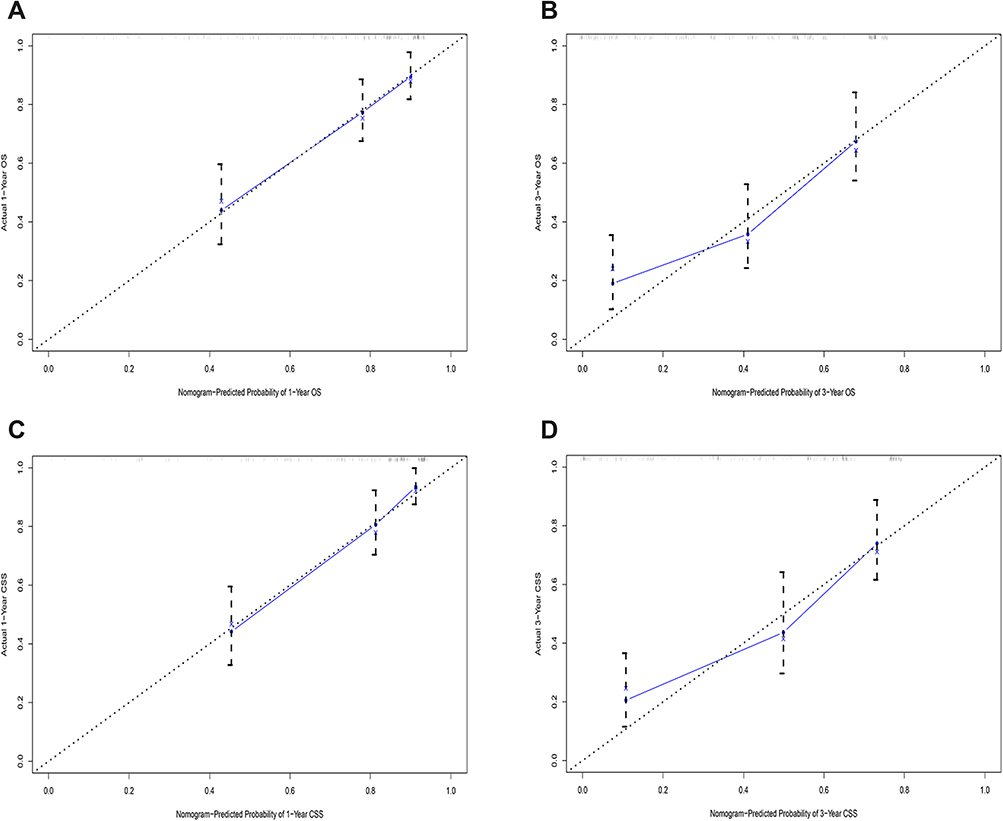 |
Figure 5 Calibration curves showing the probability of 1-, and 3-year overall survival (A and B) and cancer-specific survival (C and D) between the nomogram prediction and the actual observation in the training cohort of patients with HNMM. |
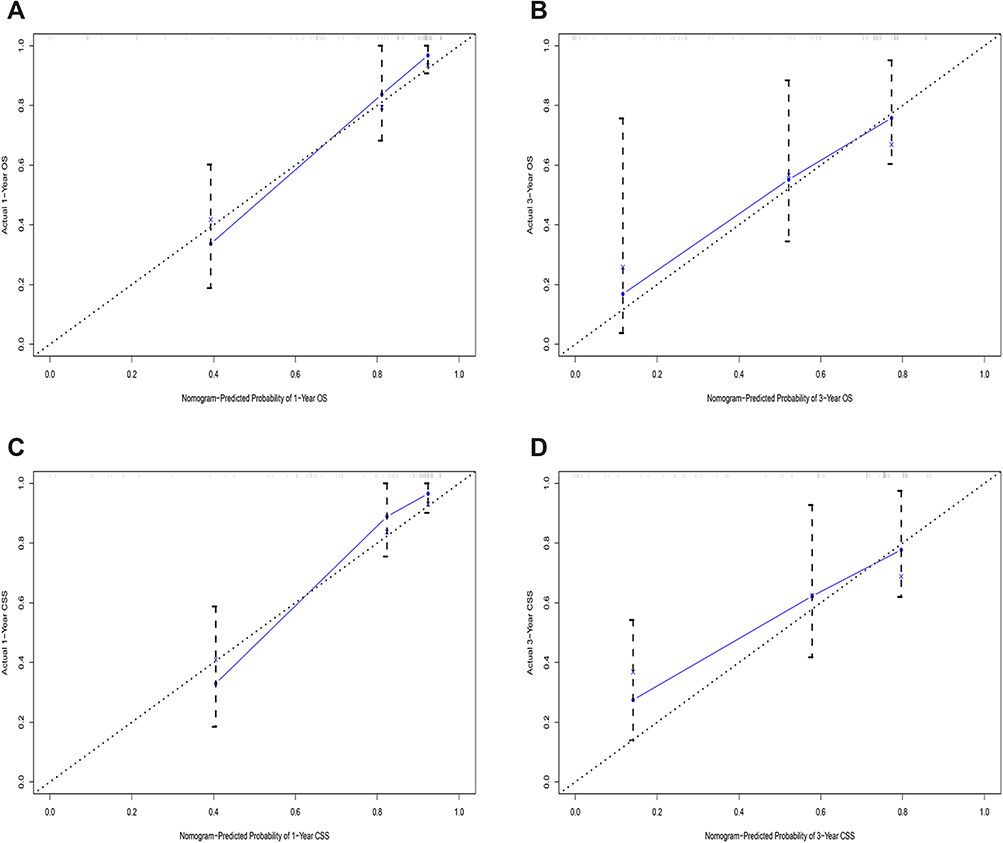 |
Figure 6 Calibration curves showing the probability of 1-, and 3-year overall survival (A and B) and cancer-specific survival (C and D) between the nomogram prediction and the actual observation in the validation cohort of patients with HNMM. |
Discussion
HNMM is a highly invasive malignant tumor with an unknown etiology. Due to the complex anatomical structure of the head and neck and the easy recurrence and metastasis of tumors, the treatment of HNMM has always been a great challenge for clinicians. Undoubtedly, an accurate and effective prediction of the prognosis of HNMM patients has important clinical significance for individualized treatment and follow-up. However, due to the high degree of malignancy and aggressiveness of HNMM, the TNM staging system of the AJCC is different from the traditional tumor staging system: T stage is divided only into the T3 and T4a/b stages, which seems to be too limited to be predictive.23,24 Therefore, it is essential to build a more effective forecasting tool. The nomogram is a statistical tool that can effectively predict patient prognosis, and it has been proven to be more accurate than the AJCC TNM staging system.25–27 Therefore, this research developed a clinical nomogram model based on the SEER database to predict the OS and CSS of HNMM patients so that clinicians can intuitively predict patient prognosis and conduct individualized treatment. It is worth noting that using this training queue, the C-indexes of the OS and CSS nomograms reached 0.764 and 0.783, respectively, which exceed those of the TNM staging system, thus showing greater reliability.
In this study, through univariate and multivariate Cox regression analyses, five independent prognostic indicators, namely age at diagnosis, primary site, T stage, N stage, and surgery, were ultimately included in the nomogram prediction model. We used X-Tile software to evaluate the cutoff point for age in the patient population. When 69 and 83 years were used as the cutoff points, the model better distinguished the survival rate. In our analysis, we found that the OS and DSS outcomes of elderly patients were worse than those of young patients. It was confirmed that age is an independent factor for the prognosis of HNMM, consistent with previous studies.21,25,28,29 Regarding the location of the primary tumor, as previously reported,28,30 we found that MM originating in the paranasal sinuses is associated with a poor prognosis, and HNMM occurring in the paranasal sinuses should be considered high risk. This may be because tumors are usually close to or invade important anatomical structures (such as orbital contents, the skull base, and cranial nerves), and it is not easy to obtain negative surgical margins.31,32
After controlling for other factors, such as location and N stage, we found that T stage has a good predictive effect on HNMM, consistent with previous studies.36 Schmidt et al11 reported no difference in the survival rate of patients with T3 and T4a HNMM, although they were not stratified by anatomical location. Torabi et al33 found a significant difference in prognosis between T3 and T4a MM occurring in the sinonasal cavity but no significant difference in the prognosis of MM occurring in the non-sinonasal cavity. HNMM has a low incidence of lymph node metastasis and remote metastasis. Amit et al34 noted that lymph node metastasis was not an important predictor of the prognosis of sinonasal MM. Moya-Plana et al21 supported this view, suggesting that cervical lymph node treatment should be gradually degraded. Similar to other studies,11,29 we found that an advanced N stage is a risk factor for the prognosis of HNMM. Interestingly, unlike previous studies,11,29,42 our study suggests that M stage has no role in tumor prognosis.
At present, there is no standard treatment for HNMM. It is generally accepted that surgical resection is the preferred treatment, especially for patients in stages T3 and T4a, the purpose of which is to achieve complete resection and obtain a negative margin. Our research suggests that surgery plays an important role in the survival of HNMM patients. There are many controversies about whether postoperative radiotherapy (including the radiotherapy plan and dose) should be administered. In our research, we did not find that patients receiving radiotherapy had improved OS and DSS. Radiotherapy as an adjunctive therapy is mainly used to prevent local recurrence. Under certain circumstances, adjunctive radiotherapy may be effective in local control of the tumor, but there are no data to show that it provides a survival advantage.35–37 Although it has also been shown that radiotherapy has no effect on OS in patients with non-sinonasal cavity tumors, it improves OS in patients with sinonasal cavity tumors.33 Preliminary studies have proven that MM is sensitive to heavy ion 12C6 + radiotherapy, which can improve the local control rate and OS rate.38 Recent studies have reported no difference in OS between HNMM patients who receive radiotherapy and those who do not receive radiotherapy.39,40 Although postoperative radiotherapy can achieve better local control, it cannot reduce the risk of distant metastasis.35 Therefore, improving the survival rate by increasing the intensity of local treatment is not very optimistic at this stage.
Our research was limited by the inherent restrictions of the SEER database. First, there is no detailed information on targeted therapy. Based on the high frequency of c-kit mutations in mucocutaneous melanoma, molecular targeted therapy and immunotherapy targeting mutated genes in melanomas may be beneficial to the long-term survival of patients with advanced and distant metastases who cannot be treated by surgery, and targeted therapy and immunotherapy have proven to be promising adjuvant therapies.41,42 Second, important clinical manifestations, such as surgical margins and nerve infiltration, are not recorded in the SEER database, so they were not included in our study. Third, HNMM has a high risk of recurrence and metastasis. However, there is no recurrence or reoperation data in the SEER database. Finally, our nomogram was verified only on data from the SEER database because we could not access other data sources. Further research is still needed to verify the accuracy of the model based on other overall external verifications.
Conclusion
In summary, independent prognostic factors of OS and CSS for patients with HNMM include age, location, T stage, N stage, and surgery. This study is the first to establish an HNMM nomogram based on the SEER database and evaluate it using a range of indicators. The nomogram can be used to calculate the survival probability in individual patients. Compared to the AJCC staging system alone, both the C-index and calibration curves of the nomogram performed well and made accurate predictions for OS and CSS after one and three years for HNMM patients. The nomogram offers further reference information for clinicians to provide personalized prognoses and help them to more confidently plan mucosal melanoma treatment for patients with HNMM by integrating easily available factors, such as whether the patient had undergone surgery. In the next phase of our study, we will attempt to optimize the nomogram by collecting prospective data on HNMM and exploring and utilizing unknown prognostic factors. With the help of external validation methods, we will verify the effectiveness of the model.
Statement of Ethics
All procedures performed in this study involving human participants were in accordance with the World Medical Association Declaration of Helsinki. This study protocol was reviewed and the need for approval was waived by Clinical Research Ethics Committee of Shenzhen Second People’s Hospital in accordance with the local legislation and institutional requirements. Furthermore, Informed consent was also waived as SEER is a de-identified, publicly available cancer database.
Acknowledgments
We would like to thank to all the staff members of the National Cancer Institute, who have been involved with the Surveillance, Epidemiology and End Results (SEER) Program.
Funding
The National Natural Science Foundation of China (NO.81970875). Supported by Shenzhen Fund for Guangdong Provincial High-level Clinical Key Specialties (No.SZGSP004).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patrick RJ, Fenske NA, Messina JL. Primary mucosal melanoma. J Am Acad Dermatol. 2007;56(5):828–834. doi:10.1016/j.jaad.2006.06.017
2. Chang AE, Karnell LH, Menck HR. The national cancer data base report on cutaneous and noncutaneous melanoma. Cancer. 1998;83(8):1664–1678. doi:10.1002/(SICI)1097-0142(19981015)83:8<1664::AID-CNCR23>3.0.CO;2-G
3. Manolidis S, Donald PJ. Malignant mucosal melanoma of the head and neck. Cancer. 1997;80(8):1373–1386. doi:10.1002/(SICI)1097-0142(19971015)80:8<1373::AID-CNCR3>3.0.CO;2-G
4. Troussier I, Baglin A-C, Marcy P-Y, et al. [Mucosal melanomas of the head and neck: state of the art and current controversies]. Bull Cancer. 2015;102(6):559–567. French. doi:10.1016/j.bulcan.2015.04.013
5. Marcus DM, Marcus RP, Prabhu RS, et al. Rising incidence of mucosal melanoma of the head and neck in the United States. J Skin Cancer. 2012;2012:231693. doi:10.1155/2012/231693
6. Seetharamu N, Ott PA, Pavlick AC. Mucosal melanomas: a case-based review of the literature. Oncologist. 2010;15(7):772–781. doi:10.1634/theoncologist.2010-0067
7. Patel SG, Prasad ML, Escrig M, et al. Primary mucosal malignant melanoma of the head and neck. Head Neck. 2002;24(3):247–257. doi:10.1002/hed.10019
8. Leiter U, Garbe C. Epidemiology of melanoma and nonmelanoma skin cancer—the role of sunlight. In: Reichrath J, editor. Sunlight, Vitamin D and Skin Cancer. New York: Springer New York; 2008:89–103. doi:10.1007/978-0-387-77574-6_8
9. Desmond RA, Soong S-J. Epidemiology of malignant melanoma. Surg Clin. 2003;83(1):1–29. doi:10.1016/S0039-6109(02)00092-0
10. Tyrrell H, Payne M. Combatting mucosal melanoma: recent advances and future perspectives. Melanoma Manag. 2018;5(3):MMT11. doi:10.2217/mmt-2018-0003
11. Schmidt MQ, David J, Yoshida EJ, et al. Predictors of survival in head and neck mucosal melanoma. Oral Oncol. 2017;73:36–42. doi:10.1016/j.oraloncology.2017.08.002
12. Xu -Q-Q, Lai Y-Z, Huang Z-L, et al. Clinical outcomes and patterns of failure of head and neck mucosal melanoma treated with multiple treatment modalities. Radiat Oncol. 2021;16(1):138. doi:10.1186/s13014-021-01860-z
13. Langan EA, Terheyden P. Melanoma of the oral cavity. In: Schmidt E, editor. Diseases of the Oral Mucosa: Study Guide and Review. Cham: Springer International Publishing; 2021:371–377. doi:10.1007/978-3-030-82804-2_34
14. Sahovaler A, Ziai H, Cardemil F, et al. Importance of margins, radiotherapy, and systemic therapy in mucosal melanoma of the head and neck. Laryngoscope. 2021;131(10):2269–2276. doi:10.1002/lary.29555
15. Edmond M, Nenclares P, Harrington K, et al. What is the role of the surgeon in the management of head and neck mucosal melanoma in the immunotherapy era? Head Neck. 2021;43(11):3498–3503. doi:10.1002/hed.26849
16. Nenclares P, Ap Dafydd D, Bagwan I, et al. Head and neck mucosal melanoma: the United Kingdom national guidelines. Eur J Cancer. 2020;138:11–18. doi:10.1016/j.ejca.2020.07.017
17. Grant-Freemantle MC, Lane O’Neill B, Clover AJP. The effectiveness of radiotherapy in the treatment of head and neck mucosal melanoma: systematic review and meta-analysis. Head Neck. 2021;43(1):323–333. doi:10.1002/hed.26470
18. Yin G, Guo W, Huang Z, Chen X. Comparative analysis of postoperative adjuvant therapy for head and neck mucosal melanoma in China. Acta Otolaryngol. 2021;141(11):1014–1021. doi:10.1080/00016489.2021.1921263
19. Ballantyne AJ. Malignant melanoma of the skin of the head and neck: an analysis of 405 cases. Am J Surg. 1970;120(4):425–431. doi:10.1016/S0002-9610(70)80001-0
20. Prasad ML, Patel SG, Huvos AG, Shah JP, Busam KJ. Primary mucosal melanoma of the head and neck. Cancer. 2004;100(8):1657–1664. doi:10.1002/cncr.20201
21. Moya-Plana A, Mangin D, Dercle L, et al. Risk-based stratification in head and neck mucosal melanoma. Oral Oncol. 2019;97:44–49. doi:10.1016/j.oraloncology.2019.07.026
22. Cronin KA, Ries LAG, Edwards BK. The surveillance, epidemiology, and end results (SEER) program of the national cancer institute. Cancer. 2014;120(S23):3755–3757. doi:10.1002/cncr.29049
23. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
24. Moya-Plana A, Aupérin A, Obongo R, et al. Oncologic outcomes, prognostic factor analysis and therapeutic algorithm evaluation of head and neck mucosal melanomas in France. Eur J Cancer. 2019;123:1–10. doi:10.1016/j.ejca.2019.09.007
25. Xiao Y, Peng S, Hu Y, Zhang J, Cao X. Development and validation of prognostic nomogram in patients with nonmetastatic malignant melanoma: a SEER population-based study. Cancer Med. 2020;9(22):8562–8570. doi:10.1002/cam4.3318
26. Zhou H, Zou X, Li H, Chen L, Cheng X. Construction and validation of a prognostic nomogram for primary vulvar melanoma: a SEER population-based study. Jpn J Clin. 2020;50(12):1386–1394. doi:10.1093/jjco/hyaa137
27. Yang J, Pan Z, Zhao F, et al. A nomogram for predicting survival in patients with nodular melanoma: a population-based study. Medicine (Baltimore). 2019;98(24):e16059–e. doi:10.1097/MD.0000000000016059
28. Samstein RM, Carvajal RD, Postow MA, et al. Localized sinonasal mucosal melanoma: outcomes and associations with stage, radiotherapy, and positron emission tomography response. Head Neck. 2016;38(9):1310–1317. doi:10.1002/hed.24435
29. Jethanamest D, Vila PM, Sikora AG, Morris LGT. Predictors of survival in mucosal melanoma of the head and neck. Ann Surg Oncol. 2011;18(10):2748–2756. doi:10.1245/s10434-011-1685-4
30. Sun S, Huang X, Gao L, et al. Long-term treatment outcomes and prognosis of mucosal melanoma of the head and neck: 161 cases from a single institution. Oral Oncol. 2017;74:115–122. doi:10.1016/j.oraloncology.2017.09.020
31. Lund V, Stammberger H, Nicolai P. European position paper on endoscopic management of tumours of the nose and paranasal sinuses and skull base. Rhinology. 2010;22:30–31.
32. Paré A, Blanchard P, Rosellini S, et al. Outcomes of multimodal management for sinonasal squamous cell carcinoma. J Cranio Maxill Surg. 2017;45(8):1124–1132. doi:10.1016/j.jcms.2017.05.006
33. Torabi SJ, Benchetrit L, Spock T, Cheraghlou S, Judson BL. Clinically node-negative head and neck mucosal melanoma: an analysis of current treatment guidelines & outcomes. Oral Oncol. 2019;92:67–76. doi:10.1016/j.oraloncology.2019.03.017
34. Amit M, Tam S, Abdelmeguid AS, et al. Approaches to regional lymph node metastasis in patients with head and neck mucosal melanoma. Cancer. 2018;124(3):514–520. doi:10.1002/cncr.31083
35. Li W, Yu Y, Wang H, Yan A, Jiang X. Evaluation of the prognostic impact of postoperative adjuvant radiotherapy on head and neck mucosal melanoma: a meta-analysis. BMC Cancer. 2015;15(1):758. doi:10.1186/s12885-015-1750-7
36. Wushou A, Hou J, Zhao Y-J, Miao X-C. Postoperative adjuvant radiotherapy improves loco-regional recurrence of head and neck mucosal melanoma. J Craniomaxillofac Surg. 2015;43(4):553–558. doi:10.1016/j.jcms.2015.02.011
37. Jarrom D, Paleri V, Kerawala C, et al. Mucosal melanoma of the upper airways tract mucosal melanoma: a systematic review with meta-analyses of treatment. Head Neck. 2017;39(4):819–825. doi:10.1002/hed.24652
38. Naganawa K, Koto M, Takagi R, et al. Long-term outcomes after carbon-ion radiotherapy for oral mucosal malignant melanoma. J Radiat Res. 2017;58(4):517–522. doi:10.1093/jrr/rrw117
39. Temam S, Mamelle G, Marandas P, et al. Postoperative radiotherapy for primary mucosal melanoma of the head and neck. Cancer. 2005;103(2):313–319. doi:10.1002/cncr.20775
40. Benlyazid A, Thariat J, Temam S, et al. Postoperative radiotherapy in head and neck mucosal melanoma: a GETTEC study. Arch Otolaryngol Head Neck Surg. 2010;136(12):1219–1225. doi:10.1001/archoto.2010.217
41. Satzger I, Schaefer T, Kuettler U, et al. Analysis of c-KIT expression and KIT gene mutation in human mucosal melanomas. Br J Cancer. 2008;99(12):2065–2069. doi:10.1038/sj.bjc.6604791
42. Na’ara S, Mukherjee A, Billan S, Gil Z. Contemporary multidisciplinary management of sinonasal mucosal melanoma. Onco Targets Ther. 2020;13:2289–2298. doi:10.2147/OTT.S182580
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.