")
Back to Journals » International Journal of General Medicine » Volume 14
Prognostic Nomogram for Predicting Overall Survival of Solitary Bone Plasmacytoma Patients: A Large Population-Based Study
Authors Feng G , Shu WB, Li AB
Received 28 August 2021
Accepted for publication 8 November 2021
Published 23 November 2021 Volume 2021:14 Pages 8621—8630
DOI https://doi.org/10.2147/IJGM.S335976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Gong Feng,1 Wu-Bin Shu,2 A-Bing Li2
1School of Medicine, Ningbo University, Ningbo, Zhejiang, 315211, People’s Republic of China; 2Department of Orthopedics, Ningbo Yinzhou Second Hospital, Ningbo, 315100, Zhejiang, People’s Republic of China
Correspondence: A-Bing Li
Department of Orthopedics, Ningbo Yinzhou Second Hospital, Ningbo, Zhejiang, 315100, People’s Republic of China
Tel +86-15088557621
Email [email protected]
Background: The aim of the study was to develop a nomogram to predict the overall survival (OS) of patients with solitary plasmacytoma of bone (SBP).
Materials and Methods: Patients diagnosed with SBP between 1993 and 2012 were collected from the Surveillance, Epidemiology, and End Results (SEER) database. All eligible patients were randomly allocated to the training sets and the validation sets. The nomogram was developed with the training set and validated with the validation set using the concordance index (C-index), calibration plots, and decision curve analyses (DCA).
Results: Age, marital status, tumor grade, treatment were independent prognostic indicators for OS (P< 0.05) and were integrated to construct the nomogram. C-indexes for OS prediction in the training and validation sets were 0.78 and 0.73, respectively. The calibration plots demonstrated good consistency between the predicted and actual survival. DCA demonstrated that the new model has great benefits. In the total cohort, the median OS of patients in the low- and high-risk groups were 12.17 (95% CI 11.92– 12.42) and 3.92 (95% CI 2.83– 5.01) years, respectively.
Conclusion: The nomogram showed excellent applicability and accuracy, which could be a reliable tool for predicting OS in SBP patients.
Keywords: solitary bone plasmacytoma, cancer risk factors, SEER, nomogram
Introduction
Solitary plasmacytoma (SP) is a rare type of plasma cell dyscrasia, being cytological and immuno-phenotypically identical to plasma cell myeloma. SP can be divided into two types: solitary plasmacytoma of bone (SPB) and solitary extramedullary plasmacytoma (SEP).1 SPB is caused by the colonel proliferation of plasma cells, which does not share other features with multiple myeloma (MM)2 or show evidence of systemic disease originating from bones.3 Approximately 5% of all cases of plasma cell disorders are SPB,1 and 70% of all SP cases are SPB that mainly occurs on the axial skeleton.4,5 Approximately half of the SBP patients are associated with a high risk of developing MM in 2 to 3 years.6 The primary therapy was radiotherapy, though surgery is also required in some cases,1,7 while the use of chemotherapy remains controversial.8 As a rare disease, most previous studies on SBP only included small sample sizes.9 The Surveillance, Epidemiology, and End Results (SEER) database covers approximately 30% of the US population. Sufficient cases could be collected from this database for investigation,10 therefore, it was an excellent resource for studying special malignancies.11
Previous literature revealed that age, gender, race, tumor site, tumor grade, surgery, and the use of radiation were independent prognostic indicators of SBP patients.5,12 However, these factors act as a sole indicator to estimate prognosis. To overcome the single-factor limitation that cannot accurately predict survival rate, a novel nomogram prognostic model was built. In our work, we analyzed the clinicopathologic characteristics correlating with the overall survival (OS) of SBP patients, and establish a nomogram to predict 3-, 5-, and 10-year OS for SPB patients. To our best knowledge, this was the first study that attempted to establish a nomogram of SBP patients. Furthermore, a novel nomogram prognostic model could help clinicians estimate the prognosis of individual patients more precisely by considering multiple factors.13
Materials and Methods
Patient Eligibility and Variables
We used SEER Stat software to identify patients who were diagnosed with SPB. The inclusion criteria included: (1) diagnosed with solitary plasmacytoma of bone (International Classification of Diseases for Oncology [ICD-O]:9731) between 1993 and 2012; (2) primary malignancy; (3) primary site was selected codes (C40.0-C41.9). Patients who progressed to MM were also identified. The exclusion criteria included: (1) missing or incomplete clinicopathologic data (tumor grade, marital status, survival time, etc.); (2) multiple primary cancers. This study was approved by the local Ethics Committee of Ningbo Yinzhou Second Hospital.
Variables
Information on patient age, gender, race, marital status, grade, tumor site, and treatments was examined. Patient age was stratified into three groups (≤40 years, 41–60 years, and >60 years). Tumor grade was classified as Pre-B, B precursor; Grade I, well-differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated or anaplastic. The tumor site was categorized as an appendicular skeleton (long and short bones of limbs and associated joints, scapula) and axial skeleton (pelvis, vertebra, ribs, sternum, clavicle, and associated joints). Treatments were categorized as radiation only, radiation combined with surgery, and surgery only.
Nomogram Construction and Validation
Based on the inclusion and exclusion criteria, 376 patients were randomly allocated to the training set (n = 188) and the validation set (n = 188) to establish and verify the nomogram. Categorical data were shown as frequencies and proportions. The Chi-square test and Fisher’s exact test were used to compare variables between the two groups. The independent prognostic variables were evaluated by univariable and multivariable Cox proportional hazard regressions. The multivariable regression analysis was performed to obtain the significant prognosis that was used to establish the nomogram for 3-, 5-, and 10-year OS. The concordance index (C-index) and receiver operating characteristic (ROC) were used to determine the discrimination of survival probability and actual observations. Calibration plots were constructed to determine whether nomogram prediction agreed with the actual survival. Decision curve analysis (DCA) was performed to assess the clinical value of the novel nomogram by calculating the net benefits. According to the total risk scores of each patient, we stratified the score into two risk groups, using the optimal cut-off value. Kaplan-Meier curves and the Log rank test were used to compare between different risk groups. The cutoff points of the risk scores were identified by the maximum Youden index of the ROC curve in the training set. P<0.1 was considered statistically significant in univariate Cox proportional hazard regressions. The significant factors were selected by univariate analysis, and then incorporated into the multivariate regression analysis. Statistical software R (version 3.34, http://www.r-project.org) was used for all data analyses. The P-value of <0.05 was considered statistically significant.
Results
Patient Characteristics
According to the inclusion and exclusion criteria, all the 376 patients were identified from the SEER database. Sixty patients developed to multiple myeloma. The 376 patients were randomly allocated into the training set (n = 188) and the validation set (n = 188). Demographic and clinical features are shown in Table 1. No obvious differences between the two groups were identified (Table 1).
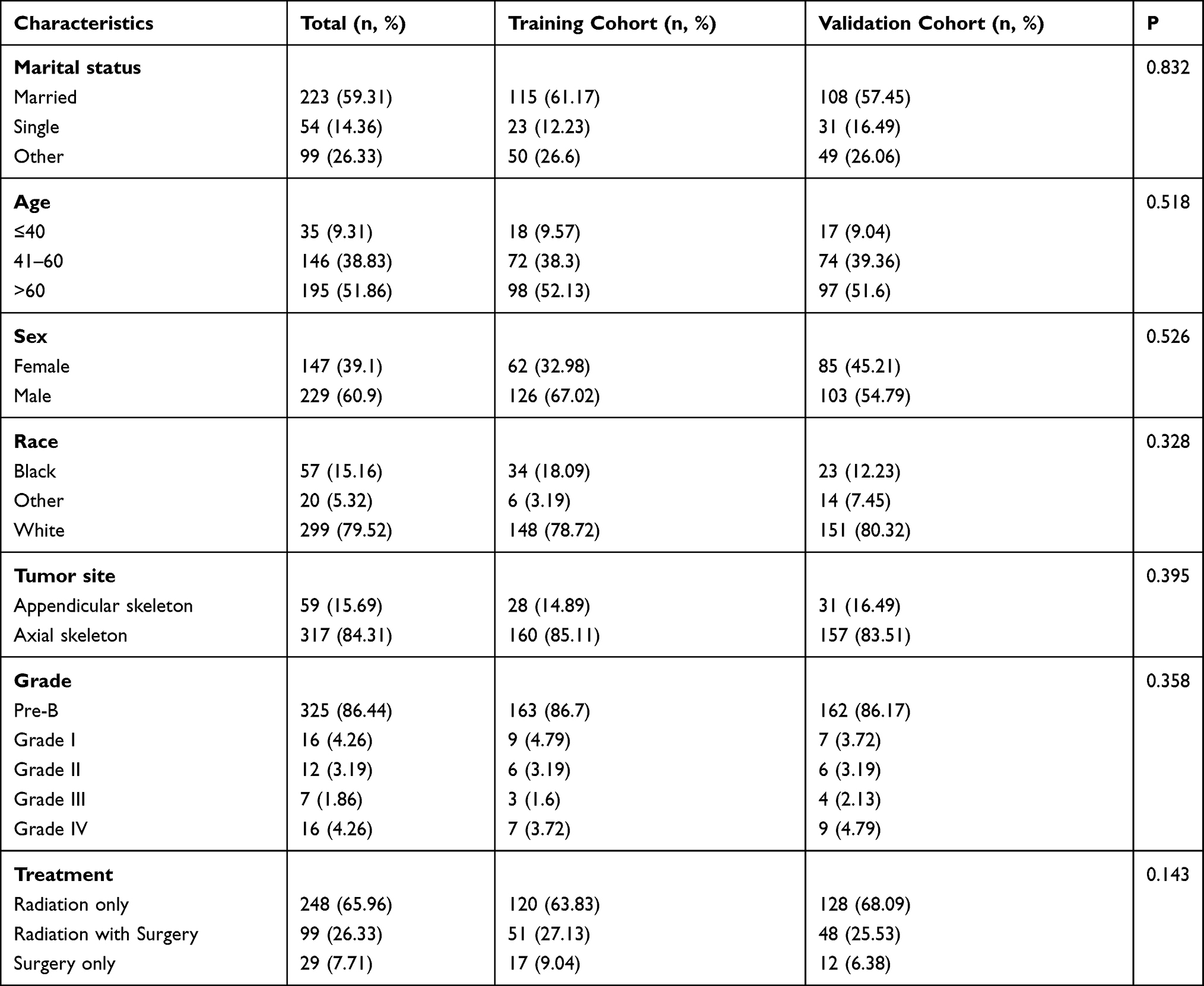 |
Table 1 Patient Demographics and Pathological Characteristics |
Of these patients, 229 patients (60.9%) were male and 147 patients (39.1%) were female; 325 patients (86.4%) were diagnosed with pre-B, 16 (4.3%) with grade I, 12 (3.2%) with grade II, 7 (1.9%) with grade III, and 16 (4.3%) with grade IV. The median age of the patients was 61 years (range: 22–96 years), the median follow-up time was 4.67 years (range: 4.42–4.92 years), and the number of deaths was 135.
Nomogram Construction
Based on the training cohort, age, sex, race, marital status, grade, tumor site, treatments were analyzed. Univariable analyses revealed that these variables, except for gender, race, and tumor site, were obviously correlated with OS (P<0.1) (Table 2).
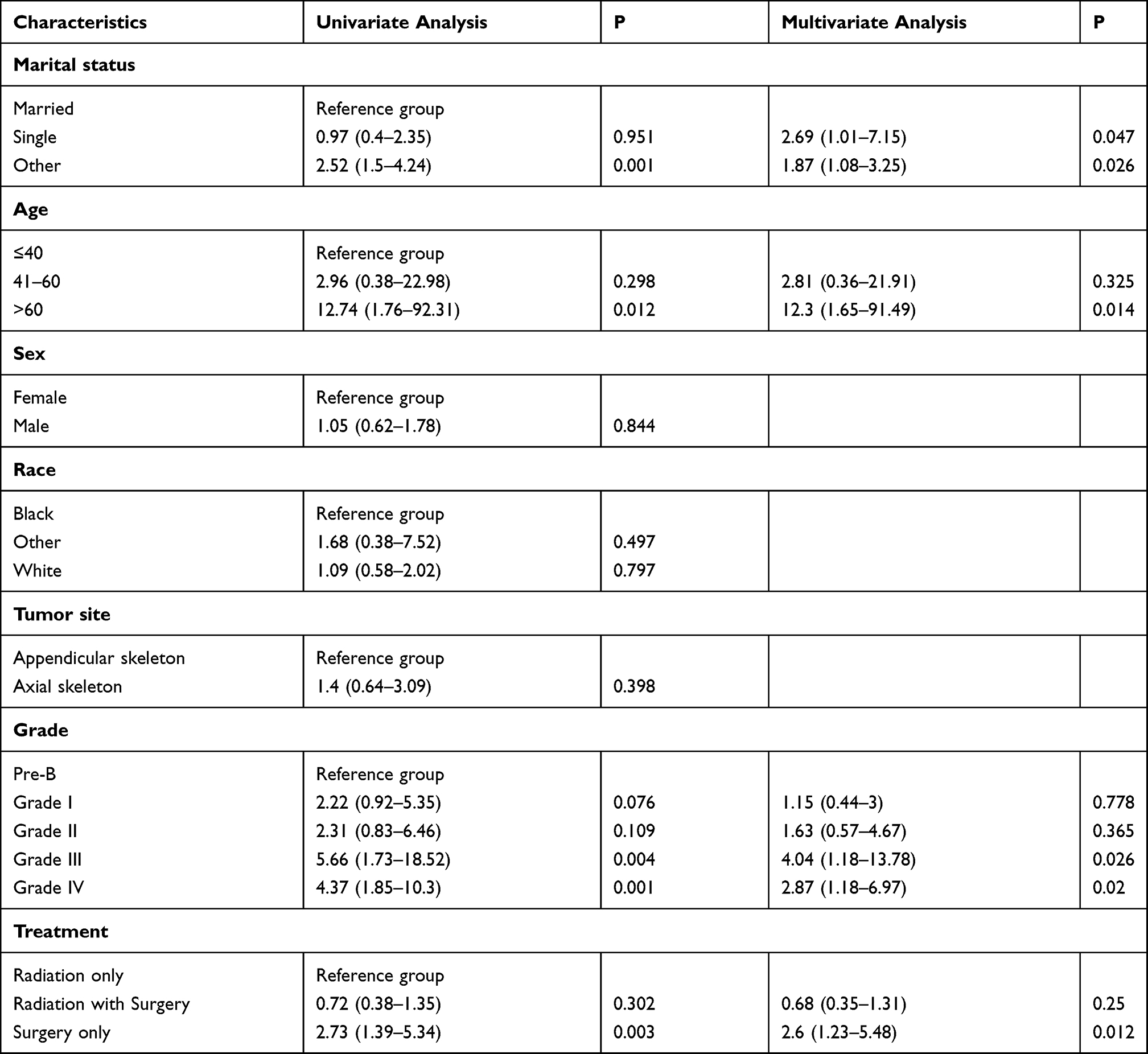 |
Table 2 Univariate and Multivariate Analyses of Overall Survival in the Training Set |
After adapting to potential confounding factors, the multivariable Cox proportional hazards analysis demonstrated that age, marital status, tumor grade, and treatment were independent prognostic factors for OS (P<0.05). Nomograms that integrated all these independent factors based on the multivariate models were constructed to predict the 3-, 5-, and 10-year OS in the training set (Figure 1). The nomogram endows each prognostic factor a detailed score (Table 3). By accumulating 4 characteristics points and locating total points on the OS total scale, the estimated probability of 3-, 5-, and 10-year OS of the individual patient could be identified.
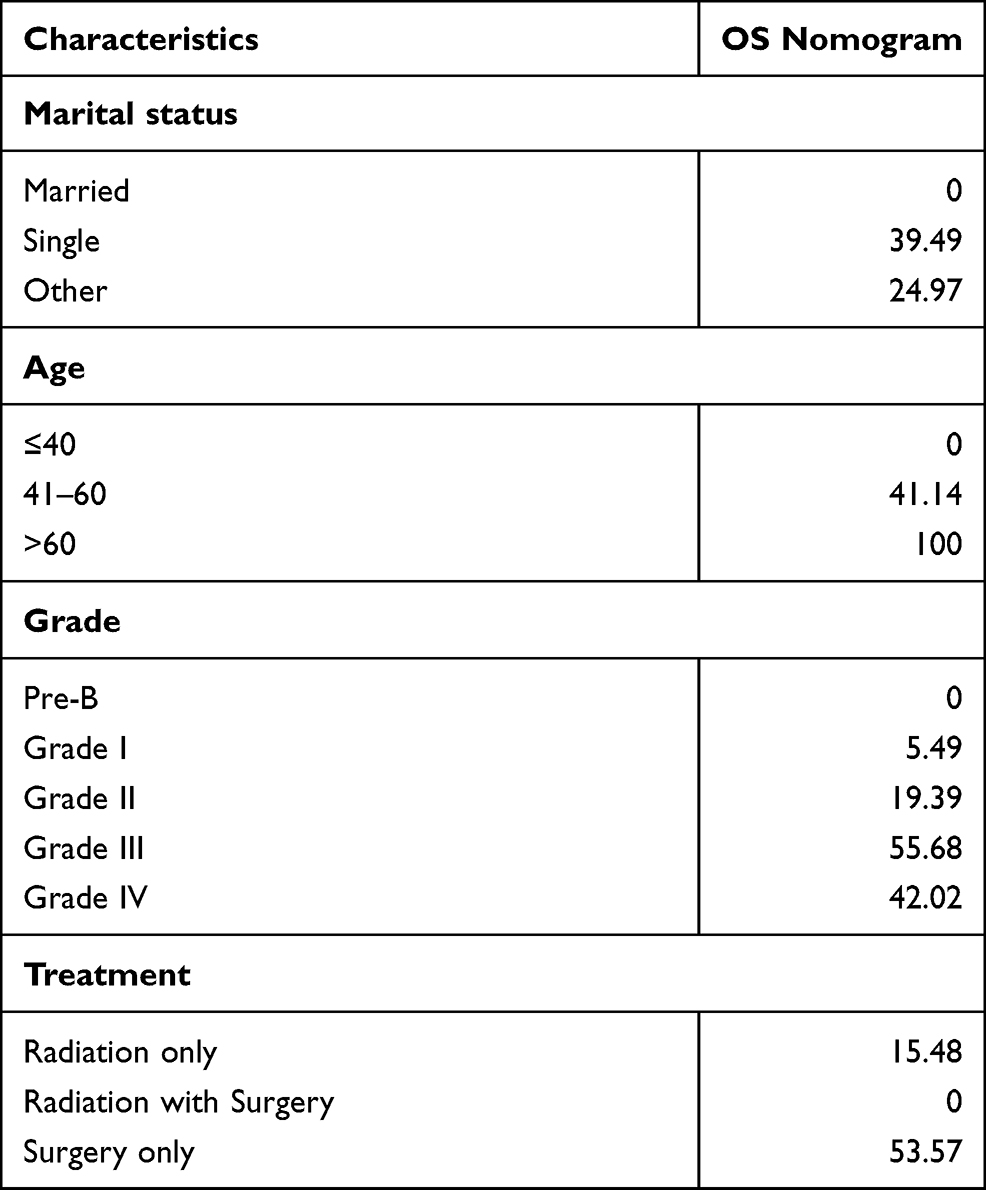 |
Table 3 Detailed Scores of Prognostic Factors in the Overall Survival Nomograms |
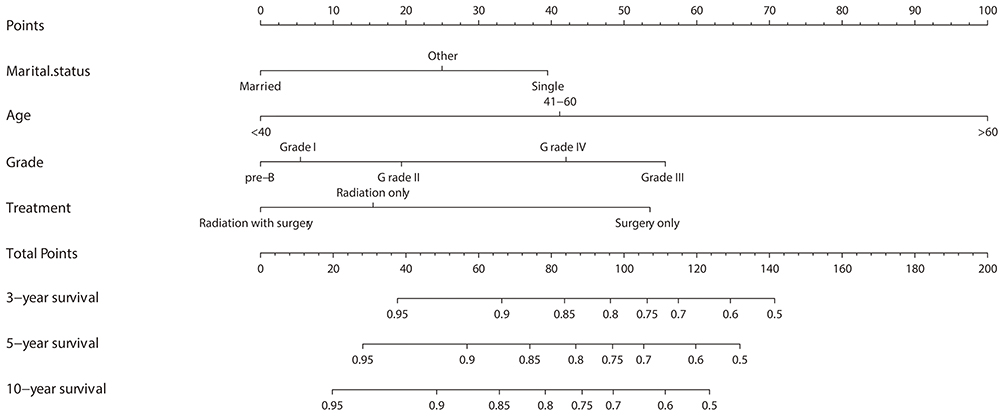 |
Figure 1 Nomograms for predicting the 3-,5-, and 10-year overall survival of solitary bone plasmacytoma patients. Description using nomograms: First, each feature point of the patient is assigned by plotting a vertical line to a point scale from the variable. Then, sum all the points and draw a vertical line from the total point scale to the liver metastasis axis to obtain the probability. |
Nomogram Validation
The C-index was 0.78 (95% CI, 0.73–0.83) and 0.73 (95% CI, 0.66–0.80) in the training and validation sets, respectively, demonstrating the good discrimination ability of the model. For the training cohort, the 3-, 5-, and 10-year area under the curve (AUC) values of the nomogram of OS were 0.807, 0.787, and 0.824, respectively (Figure 2A); those for the validation cohort were 0.738, 0.792, and 0.916, respectively (Figure 2B). The calibration plots of OS nomograms also demonstrated satisfactory consistency between the predicted and actual survival (Figures 3 and 4).
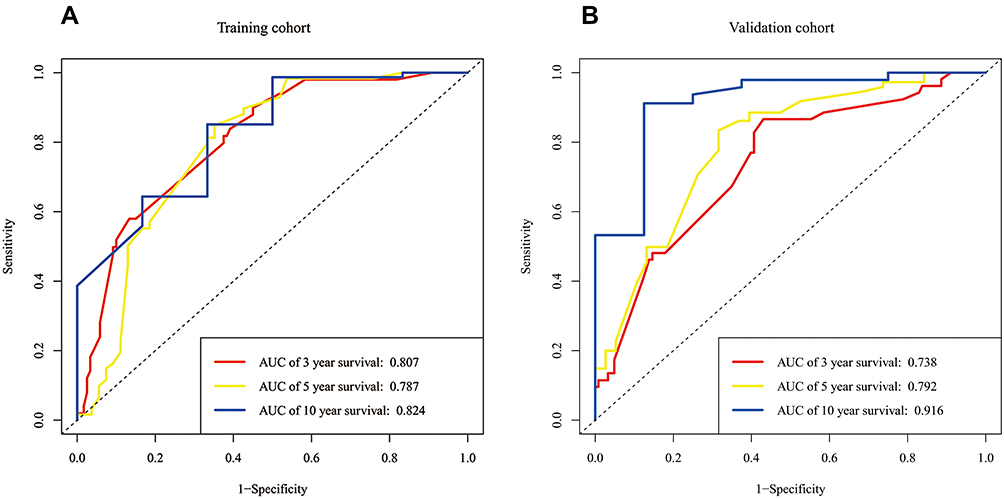 |
Figure 2 AUC values of ROC predicted overall survival rates of Nomogram in the training cohort (A) and the validation cohort (B). |
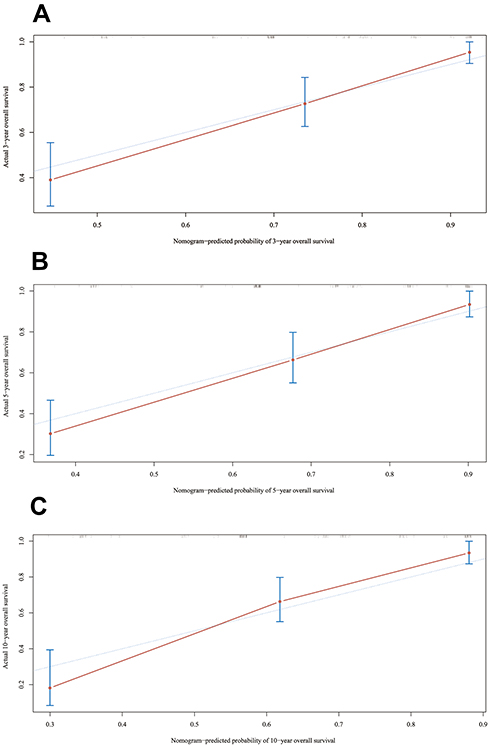 |
Figure 3 Internal calibration plot. (A) 3-Year, (B) 5-year and (C) 10- year overall survival nomogram calibration curves. The 45-degree line represents an ideal match between the actual survival (Y-axis) and nomogram-predicted survival (X-axis). The perpendicular line means 95% confidence intervals. |
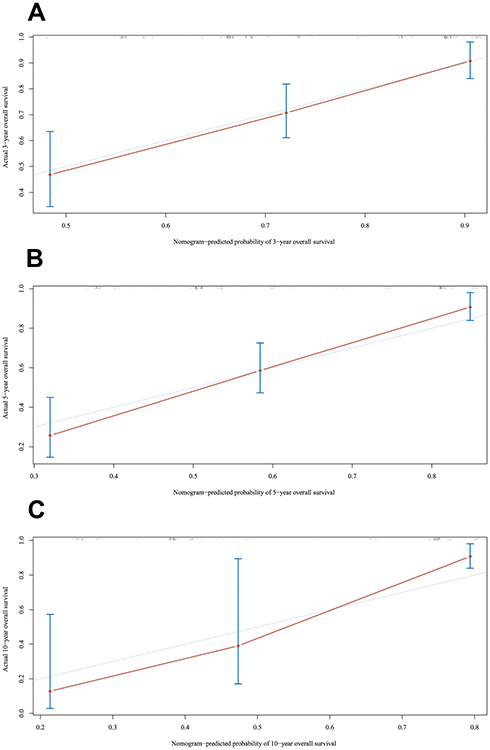 |
Figure 4 External calibration plot. (A) 3-Year, (B) 5-year and (C) 10- year overall survival nomogram calibration curves. The 45-degree line represents an ideal match between the actual survival (Y-axis) and nomogram-predicted survival (X-axis). The perpendicular line means 95% confidence intervals. |
Clinical Value and Risk Stratification System
DCA demonstrated that the new model had great benefits at different time points (Figure 5). The optimal cut-off value of the total score was 100. The score range in the risk stratification model was defined as low risk (total score 0–100) and high risk (total score >100). In the total cohort, Kaplan-Meier curves showed that the low-risk group had higher survival rate than the high-risk group (all P<0.0001) (Figure 6), and the median OS of patients in the low- and high-risk groups were 12.17 (95% CI 11.92–12.42) and 3.92 (95% CI 2.83–5.01) years, respectively.
 |
Figure 5 Decision curves of the nomogram predicting OS at (A) 3 years, (B) 5 years and (C) 10 years in the training cohort and at (D) 3 years, (E) 5 years and (F) 10 years in the validation cohort. |
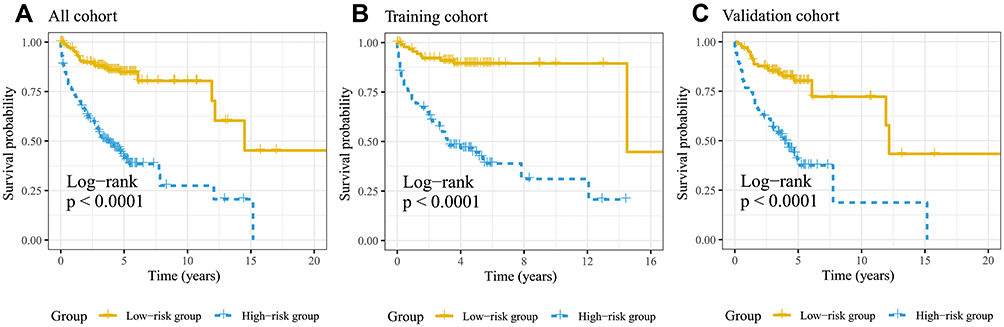 |
Figure 6 Kaplan–Meier curves of overall survival for patients in the low-, and high-risk groups (A–C). |
Discussion
Nomogram is a powerful prognosis tool in oncology and medicine.14 However, no prognostic nomogram for SBP has been constructed. We are the first to establish and validate nomograms to estimate the OS of SBP patients by using the SEER database. In addition, we developed a risk classification system that separates the entire cohort into two prognostic groups, according to the total scores of each patient. Due to the database population diversity and the rigor of inclusion and exclusion criteria, our nomograms are quite credible and can be easily promoted for individualized diagnosis and treatment of SBP patients. From the aspects of C-index, ROC, and DCA, our nomograms showed good performance for predicting OS. The individual likelihood of a clinical event can be predicted by integrating various prognostic and determinant factors. Nomograms are excellent tools for comprehensive biological and clinical statistical models, which serve as a great step for the promotion of personalized medicine.
In our study, 376 SPB patients from the SEER database were analyzed. Multivariable analysis indicated that age, marital status, histological grade, and tumor treatments are independent prognostic factors for OS. Several studies suggested that age is a vital predictor in the survival of malignant tumors.15–17 In our study, we found that patients older than 60 years had worse survival rates. A similar result was found in another previous study.3 Dores et al reported that the 5-year survival for SBP patients was the most favorable among the younger age group (<60 years; 76.8%) and the poorest among the older age group (≥60 years; 53.3%) (P<0.0001).9 A possible explanation is that with the increase of age, the immune function gradually weakens, and the immune monitoring and elimination of mutant cells are compromised.
Marital status was a benefit factor that increases the survival of SPB.12 Some studies have shown that marital status is an independent prognostic factor for the survival of cancer patients.18–21 Aizer et al reported that social support has a potentially significant impact on the survival of cancer patients.18 Gao et al reported that marital status is an independent prognostic factor for chondrosarcoma and also emphasized the importance of social support for improving the survival rate of chondrosarcoma patients.22 Considering our statistical results, we speculate that married patients have a better survival rate because of their better social networks and social support that lead to a relatively better psychological state.
In the current study, we found that patients with grade III tumor had a worse outcome. Wang et al found that Grade II tumor had a worse outcome.12 However, Folk et al reported that Grade IV tumor had worse survival rates because it shared some common pathological features with invasive B-cell lymphoma.23 The grade was based on the variable “Grade” in the SEER database. The SEER database has no other variables to represent grade. However, the grade is a measure of the aggressiveness of tumor and an important prognostic indicator for many types of tumors. We included the cases of grade I–IV tumors at a relatively small sample size, while the results of our study need to be carefully explained.
Most treatment recommendations are based on expert consensus and are still controversial. Radiotherapy, surgery, and chemotherapy are the three main treatments. Radiotherapy is the primary treatment for SBP that is highly sensitive to radiation,24 which usually has a local control rate of about 94% at doses of 40 to 45 Gy.25 Surgery is a reliable option for patients with nerve injury and spinal instability.26 It is not only a part of the diagnostic procedure but also the treatment of fracture fixation, laminectomy, or spinal stabilization.4 Surgery is a milestone for the histological diagnosis and specific treatment for plasmacytoma with distinct localizations.3 However, our study found that surgery combined with radiotherapy was a protective factor of OS, compared with radiation only or surgery only. Moreover, patients who were only treated with surgery were associated with a nearly 2.7-time higher risk of death. This result is consistent with other previous reports.17,27 Therefore, we speculate that surgical interventions could reduce the local symptoms such as neurological symptoms, vertebral fractures, etc., and improve the quality of life, while it does not help to prevent the progression of the disease substantially.
There were several limitations in our study. Firstly, since the patient’s laboratory test results, including serum quantitative immunoglobulin, and Bence-Jones protein, were not available in the database, the patient’s predictive index was not sufficiently complete. Secondly, other factors, including marrow involvement by clonal plasma cells and skewed serum-free light chain ratio, were also not available in the database. Thirdly, due to the retrospective nature of the SEER database, the inevitable missing data might lead to sample size reduction (eg, only few patients were categorized as grade I–IV). Fourthly, due to the unavailable data of chemotherapy, whether chemotherapy has any benefit for SBP patients is unknown. Finally, detailed radiation regime and surgical procedure were not recorded, which might confound the results. Despite these shortcomings, the SEER database serves as an unparalleled resource for studying rare cancers.
Conclusion
Based on the SEER cohort, marital status, age, grade, treatment were identified as independent prognostic indicators for OS in SBP patients. We constructed a nomogram and risk classification system to predict the OS of SBP patients. The nomogram showed good applicability and great accuracy, and it could serve as a reliable tool for predicting OS in SBP patients, though further clinical verification is needed.
Ethics Approval and Consent to Participate
This study was approved by the local Ethics Committee of Ningbo Yinzhou Second Hospital.
Acknowledgments
The authors thank the National Cancer Institute for providing the SEER data. We thank TopEdit for its linguistic assistance during the preparation of this manuscript.
Author Contributions
G.F and A.B.L contribute to the conception and design of the study, G.F and W.B.S contribute to analysis and interpretation of data, G.F and A.B.L contribute to drafting the article. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soutar R, Lucraft H, Jackson G, et al. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Br J Haematol. 2004;124(6):717–726. doi:10.1111/j.1365-2141.2004.04834.x
2. International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol. 2003;121(5):749–757. doi:10.1046/j.1365-2141.2003.04355.x
3. Grammatico S, Scalzulli E, Petrucci MT. Solitary plasmacytoma. Mediterr J Hematol Infect Dis. 2017;9(1):e2017052. doi:10.4084/MJHID.2017.052
4. Caers J, Paiva B, Zamagni E, et al. Diagnosis, treatment, and response assessment in solitary plasmacytoma: updated recommendations from a European Expert Panel. J Hematol Oncol. 2018;11(1):10. doi:10.1186/s13045-017-0549-1
5. Thumallapally N, Meshref A, Mousa M, Terjanian T. Solitary plasmacytoma: population-based analysis of survival trends and effect of various treatment modalities in the USA. BMC Cancer. 2017;17(1):13. doi:10.1186/s12885-016-3015-5
6. Paiva B, Chandia M, Vidriales MB, et al. Multiparameter flow cytometry for staging of solitary bone plasmacytoma: new criteria for risk of progression to myeloma. Blood. 2014;124(8):1300–1303. doi:10.1182/blood-2014-04-567909
7. Suh YG, Suh CO, Kim JS, Kim SJ, Pyun HO, Cho J. Radiotherapy for solitary plasmacytoma of bone and soft tissue: outcomes and prognostic factors. Ann Hematol. 2012;91(11):1785–1793. doi:10.1007/s00277-012-1510-6
8. Finsinger P, Grammatico S, Chisini M, Piciocchi A, Foa R, Petrucci MT. Clinical features and prognostic factors in solitary plasmacytoma. Br J Haematol. 2016;172(4):554–560. doi:10.1111/bjh.13870
9. Dores GM, Landgren O, McGlynn KA, Curtis RE, Linet MS, Devesa SS. Plasmacytoma of bone, extramedullary plasmacytoma, and multiple myeloma: incidence and survival in the United States, 1992–2004. Br J Haematol. 2009;144(1):86–94. doi:10.1111/j.1365-2141.2008.07421.x
10. Dong F, Shen Y, Gao F, et al. Nomograms to predict individual prognosis of patients with primary small cell carcinoma of the bladder. J Cancer. 2018;9(7):1152–1164. doi:10.7150/jca.23344
11. Clegg LX, Reichman ME, Miller BA, et al. Impact of socioeconomic status on cancer incidence and stage at diagnosis: selected findings from the surveillance, epidemiology, and end results: national longitudinal mortality study. Cancer Causes Control. 2009;20(4):417–435. doi:10.1007/s10552-008-9256-0
12. Wang Y, Li H, Liu C, Chen C, Yan J. Solitary plasmacytoma of bone of the spine: results from Surveillance, Epidemiology, and End Results (SEER) registry. Spine (Phila Pa 1976). 2019;44(2):E117–e125. doi:10.1097/brs.0000000000002777
13. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–80. doi:10.1016/s1470-2045(14)71116-7
14. Bianco FJ
15. Ostrowski ML, Unni KK, Banks PM, et al. Malignant lymphoma of bone. Cancer. 1986;58(12):2646–2655. doi:10.1002/1097-0142(19861215)58:12<2646::aid-cncr2820581217>3.0.co;2-u
16. Ren J, Niu G, Wang X, Song T, Hu Z, Ke C. Effect of age on prognosis of gastric signet-ring cell carcinoma: a SEER database analysis. Med Sci Monit. 2018;24:8524–8532. doi:10.12659/msm.911766
17. Kilciksiz S, Karakoyun-Celik O, Agaoglu FY, Haydaroglu A. A review for solitary plasmacytoma of bone and extramedullary plasmacytoma. Sci World J. 2012;2012:1–6. doi:10.1100/2012/895765
18. Aizer AA, Chen MH, McCarthy EP, et al. Marital status and survival in patients with cancer. J Clin Oncol. 2013;31(31):3869–3876. doi:10.1200/JCO.2013.49.6489
19. Nelles JL, Joseph SA, Konety BR. The impact of marriage on bladder cancer mortality. Urol Oncol. 2009;27(3):263–267. doi:10.1016/j.urolonc.2008.04.016
20. Wang L, Wilson SE, Stewart DB, Hollenbeak CS. Marital status and colon cancer outcomes in US surveillance, epidemiology and end results registries: does marriage affect cancer survival by gender and stage? Cancer Epidemiol. 2011;35(5):417–422. doi:10.1016/j.canep.2011.02.004
21. Denberg TD, Beaty BL, Kim FJ, Steiner JF. Marriage and ethnicity predict treatment in localized prostate carcinoma. Cancer. 2005;103(9):1819–1825. doi:10.1002/cncr.20982
22. Gao Z, Ren F, Song H, et al. Marital status and survival of patients with chondrosarcoma: a population-based analysis. Med Sci Monit. 2018;24:6638–6648. doi:10.12659/msm.911673
23. Folk GS, Abbondanzo SL, Childers EL, Foss RD. Plasmablastic lymphoma: a clinicopathologic correlation. Ann Diagn Pathol. 2006;10(1):8–12. doi:10.1016/j.anndiagpath.2005.07.009
24. Liebross RH, Ha CS, Cox JD, Weber D, Delasalle K, Alexanian R. Solitary bone plasmacytoma: outcome and prognostic factors following radiotherapy. Int J Radiat Oncol Biol Phys. 1998;41(5):1063–1067. doi:10.1016/S0360-3016(98)00186-2
25. Albano D, Bosio G, Treglia G, Giubbini R, Bertagna F. 18F-FDG PET/CT in solitary plasmacytoma: metabolic behavior and progression to multiple myeloma. Eur J Nucl Med Mol Imaging. 2018;45(1):77–84. doi:10.1007/s00259-017-3810-5
26. Zadnik PL, Goodwin CR, Karami KJ, et al. Outcomes following surgical intervention for impending and gross instability caused by multiple myeloma in the spinal column. J Neurosurg Spine. 2015;22(3):301–309. doi:10.3171/2014.9.Spine14554
27. Huang W, Cao D, Ma J, et al. Solitary plasmacytoma of cervical spine: treatment and prognosis in patients with neurological lesions and spinal instability. Spine (Phila Pa 1976). 2010;35(8):E278–84. doi:10.1097/BRS.0b013e3181c9b431
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.