")
Back to Journals » OncoTargets and Therapy » Volume 8
Prognostic impact of initial maximum standardized uptake value of 18F-FDG PET/CT on treatment response in patients with metastatic lung adenocarcinoma treated with erlotinib
Authors Kus T, Aktas G , Sevinc A, Kalender M, Yilmaz M, Kul S, Oztuzcu S, Oktay C, Camci C
Received 22 August 2015
Accepted for publication 5 November 2015
Published 15 December 2015 Volume 2015:8 Pages 3749—3756
DOI https://doi.org/10.2147/OTT.S94945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Daniele Santini
Tulay Kus,1 Gokmen Aktas,1 Alper Sevinc,1 Mehmet Emin Kalender,1 Mustafa Yilmaz,2 Seval Kul,3 Serdar Oztuzcu,4 Cemil Oktay,5 Celaletdin Camci1
1Department of Internal Medicine, Division of Medical Oncology, Gaziantep Oncology Hospital, 2Department of Nuclear Medicine, 3Department of Biostatistics, Faculty of Medicine, 4Department of Medical Biology, Faculty of Medicine, University of Gaziantep, Gaziantep, 5Department of Radiology, Faculty of Medicine, University of Akdeniz, Antalya, Turkey
Purpose: To investigate whether the initial maximum standardized uptake value (SUVmax) on fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) has a prognostic significance in metastatic lung adenocarcinoma.
Patients and methods: Sixty patients (24 females, mean age: 57.9±12 years) with metastatic stage lung adenocarcinoma who used erlotinib and underwent 18F-FDG PET/CT at the time of diagnosis between May 2010 and May 2014 were enrolled in this retrospective study. The patients were stratified according to the median SUVmax value, which was found as 11. Progression-free survival (PFS) rates for 3, 6, and 12 months were examined for SUVmax values and epidermal growth factor receptor (EGFR) mutation status.
Results: The number of EGFR-sensitizing mutation positive/negative/unknown was 26/17/17, respectively, and the number of patients using erlotinib at first-line, second-line, and third-line therapy was 15, 31, and 14 consecutively. The PFS rates of EGFR mutation positive, negative, and unknown patients for 3 months were 73.1%, 35.3%, and 41.2% (P=0.026, odds ratio [OR]=4.39; 95% confidence interval [CI]: 1.45–13.26), respectively. The PFS rates of EGFR positive, negative, and unknown patients for 6 months were 50%, 29.4%, and 29.4% (P=0.267, OR: 2.4; 95% CI: 0.82–6.96), respectively. The PFS rates of EGFR positive, negative, and unknown patients for 12 months were 42.3%, 29.4%, 23.5% (P=0.408, OR: 2.0; 95% CI: 0.42–5.26), respectively. Thirty-one of 60 patients had SUVmax values ≤11. The PFS rates for 3, 6, and 12 months were 70.5%/28% (P=0.001, OR=9.0; 95% CI: 2.79–29.04), 61.7%/8% (P<0.001, OR=28.35; 95% CI: 5.5–143), and 52.9%/8% (P<0.001, OR=18.69; 95% CI: 3.76–92.9) for low SUVmax (≤11) group/high SUVmax (>11) group, respectively.
Conclusion: Initial SUVmax value on 18F-FDG PET/CT is found to be a prognostic factor anticipating the response to erlotinib for 3, 6, and 12-month rates of PFS in both EGFR-sensitizing mutation and wild-type tumor group.
Keywords: lung adenocarcinoma, erlotinib, 18F-fluorodeoxyglucose positron emission tomography/computed tomography, maximum standardized uptake value, treatment response, prognosis
Introduction
Predictive factors may help choose the priority for the treatment and, eventually, more and more to develop individualized therapeutic strategies in patients with cancer. In advanced non-small cell lung cancer (NSCLC), several pretherapeutic prognostic factors have been identified, such as performance status (PS), age, sex, weight loss, neutrophil counts, C-reactive protein, albumin, serum calcium level.1–3 Moreover, genetic mutations having predictive and prognostic significance led to changes in the treatment algorithm of advanced NSCLC in consequence of developed targeted therapies. Sensitizing mutation within the kinase domain of the epidermal growth factor receptor (EGFR) predicts greatly improved the clinical outcome in NSCLC treated with the EGFR-tyrosine kinase inhibitors (TKIs) including erlotinib, gefitinib, and afatinib.4,5 The incidence of EGFR-sensitizing mutations is approximately 16.6% and the mostly detected and prognostic significant types of EGFR kinase mutations are exon-19 deletions and L858R mutation in exon 21.6,7 EGFR-sensitizing mutations of exons 19 and 21 are more frequent in females, non-smokers, patients with adenocarcinoma, and Asian origin patients. Those features have been associated with positive responses to TKIs.8,9
Positron emission tomography/computed tomography with fluorine-18 fluorodeoxyglucose (18F-FDG PET/CT) is used to visualize the metabolic activity of tumors. In early stage NSCLC, the maximum standardized uptake value (SUVmax) of FDG on PET was found to be the strongest prognostic factor among the patients treated with curative surgery or radiotherapy.10 However, there was no evidence proving prognostic value of baseline FDG PET uptake in patients with advanced NSCLC who were treated with standard chemotherapy.11 In this regard, we aimed to assess the prognostic significance of SUVmax value of 18F-FDG PET/CT in patients with metastatic lung adenocarcinoma treated with erlotinib for the first-line therapy, after chemotherapy failure, or maintenance therapy.
Patients and methods
Study design
This retrospective-observational study was conducted in single center Gaziantep University Hospital in Turkey. The study and informed consent documentation were reviewed and approved by the Independent Ethics Committee of Gaziantep University, and the participants all provided informed, written consent. This study was conducted in compliance with the ethical principles according to the Declaration of Helsinki. This trial was designed to assess whether 18F-FDG PET pretreatment SUVmax is prognostic for the response to erlotinib treatment.
Patient selection
Between May 2010 and May 2014, 60 patients with histologically confirmed metastatic lung adenocarcinoma who underwent 18F-FDG PET/CT prior to systemic therapy were analyzed. The following parameters were assessed prior to the beginning of therapy: age, sex, Eastern Cooperative Oncology Group PS (0–2), EGFR mutation status, smoking habit, treatment line, and the presence of cranial metastasis. The patients over 18 years old with an Eastern Cooperative Oncology Group PS 0–2 and normal blood glucose level (150 mg/dL) were allowed. Patients with brain and/or bone metastasis requiring further local treatment prior to 18F-FDG PET/CT were included in the study. Highest SUVmax in the primary tumor or metastatic lesion on 18F-FDG PET/CT was recorded. In patients using erlotinib at second line or more, 18F-FDG PET/CT SUVmax values after the detection of progression were noted. For the patients on maintenance treatment, initial 18F-FDG PET/CT SUVmax values were noted. The study population was divided into two groups according to the median SUVmax value as 11. Three, 6, and 12-month progression-free survival (PFS) rates were investigated according to both SUVmax values and EGFR mutation status.
18F-FDG PET/CT imaging
All patients fasted for at least 6 hours before FDG injection and their blood glucose levels were less than 150 mg/dL before radiotracer injection. Eight to 15 mCi (296–555 MBq) 18F-FDG was administered intravenously. All patients received an oral contrast (a solution containing sodium amidotrizoate and meglumine amidotrizoate) before PET/CT imaging. Whole-body 18F-FDG PET/CT images were acquired from vertex to proximal thigh 60 minutes after FDG injection, using a Biograph Duo LSO PET/CT system (Siemens Medical Solutions, Hoffman Estates, IL, USA). After the CT topogram, a spiral CT scan and subsequent PET scan with an acquisition time of 2–3 minutes for each bed position according to patient weight were performed. After CT-based attenuation correction, PET images were reconstructed with an ordered subset expectation maximization iterative reconstruction algorithm. A circular region of interest was drawn manually on hypermetabolic lesions on axial fused PET/CT images. The SUVmax value, a semiquantitative index of FDG uptake in tissue, was calculated as the maximum measured activity concentration divided by injected activity divided by body weight of the subject as in the following formula: SUVmax = decay corrected selected region activity (mCi/mL)/(injected dose [mCi]/body weight [kg]).
Molecular analysis
DNA was extracted from 1 cm2 of 10 mm thick paraffin-embedded tissue containing at least 20% tumor tissue. Genomic DNA was extracted using a QIAamp DNA formalin-fixed, paraffin-embedded tissue kit (Qiagen NV, Venlo, the Netherlands) according to the manufacturer’s instructions with overnight proteinase K digestion and eluting in 50 μL of water. Pyrosequencing for pyrosequencing analysis, the protocol was followed according to the manufacturer’s instructions (EGFR Pyro Assay; Qiagen). The pyrosequencing results were analyzed using the PyroMark Q24 version 2.0.6 software (Qiagen), which identifies the presence of a specific mutation and its percentage. Manufacturer-supplied logarithm of the odds (LOD) thresholds were used to call a mutation for LOD studies (≥% LOD is positive).
Treatment
All patients were allowed to receive erlotinib 150 mg/day for at least 6 weeks. Erlotinib treatment was continued until disease progression or toxicity. It was either given as a first-line treatment or as a second-line treatment after platinum-doublet failure or as a maintenance treatment.
Response evaluation
The response was assessed using the response evaluation criteria in solid tumors version 1.1. The first CT scan and 18F-FDG PET/CT were performed prior to treatment and follow-up CT scans or 18F-FDG PET/CT were performed every 12 weeks or in case of clinically suspected progression.
Statistical analysis
First, univariate analyses were performed to compare baseline characteristics. To compare the two groups, chi-squared tests (for categorical variables) were used. The Mann–Whitney U test was used to show the difference between independent groups according to non-normally distributed numerical variables. Multivariate binary logistic regression analyses were performed to determine odds ratio (OR) and 95% confidence intervals (CIs). All univariate analyses were performed in SPSS for Windows version 22.0 (SPSS Inc., Chicago, IL, USA).
Result
Patients
Sixty patients who underwent 18F-FDG PET scans prior to erlotinib treatment were enrolled in this study. The mean age was 57.9 years (SD 12; range: 36–84 years) and 24 (40%) were women. Forty-three (71.6%) patients had tumor tissue available for EGFR mutation analysis. Twenty-six patients (12.5%) had EGFR-sensitizing mutations (mostly; deletions in exon 19, L858R mutation in exon 21), 17 patients had wild-type tumor, and 17 patients had unknown EGFR status. In this population of 60 patients, SUVmax ranged between 3.8 and 24.6, with a mean of 11.5 (SD 4.4) and a median of 11. SUVmax of 31 patients were ≤11 and 29 patients were >11. Demographic features of the patients were recorded (Table 1).
 | Table 1 Demographic characteristics of patients |
Association of initial SUVmax and PFS according to EGFR mutation analysis
The 3-month PFS rates were 73.1% in the EGFR-sensitizing mutation group, 35.3% in the EGFR negative group, and 41.2% in the rEGFR unknown group (P=0.026); the 6-month PFS rates were 50%, 29%, and 29.4% (P=0.267), respectively; and the 12-month PFS rates were 42.3%, 29.4%, 23.5%, respectively (P=0.408). Using Mann–Whitney U test, OR for 3, 6, and 12-month PFS rates based on EGFR positivity were 4.39 (95% CI: 1.45–13.26, P=0.009), 2.4 (95% CI: 0.82–6.96, P=0.107), and 2.0 (95% CI: 0.42–5.26, P=0.20), respectively (Table 2). Thirty-one of the patients had SUVmax values ≤11 and 29 patients had SUVmax values >11. The 3-month PFS rate was 77.4% in patients who have SUVmax ≤11 and was 27.6 in patients who have SUVmax >11 (OR=9.0; 95% CI: 2.79–29.04, P<0.001). The 6-month PFS rates were 67.7% vs 6.9% (OR=28.35; 95% CI: 5.5–143, P<0.001) and the 12-month PFS rates were 58.1% vs 6.9% (OR=18.69; 95% CI: 3.76–92.9, P<0.001) (Table 2 and Figure 1).
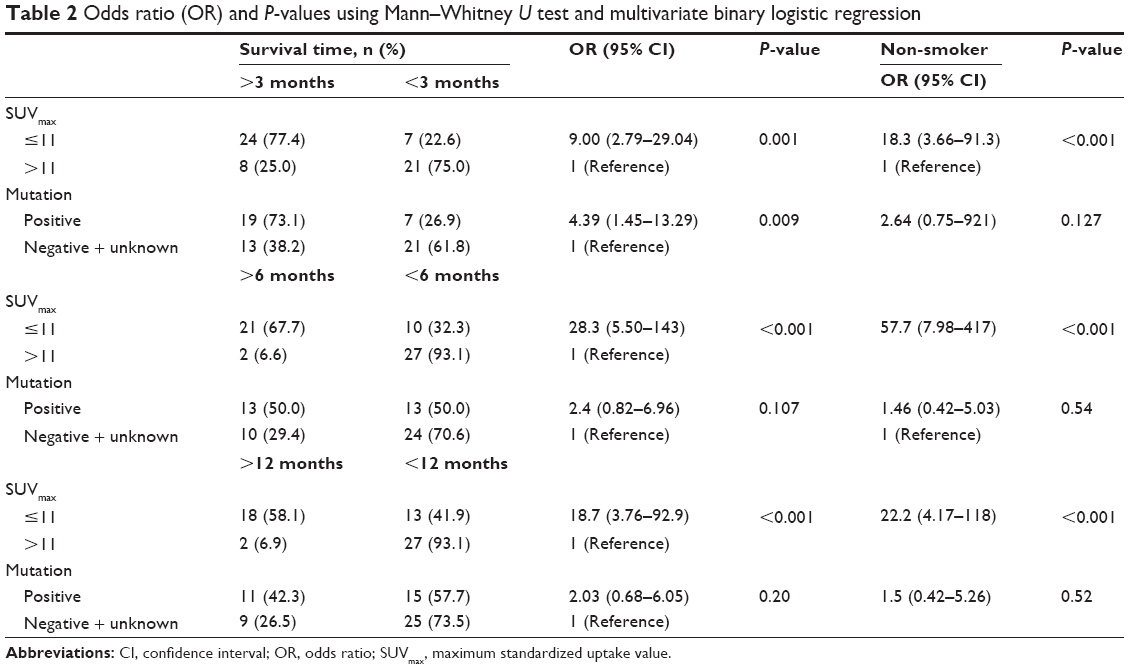 | Table 2 Odds ratio (OR) and P-values using Mann–Whitney U test and multivariate binary logistic regression |
 | Figure 1 The (A) 3, (B) 6, and (C) 12-month rates of progression-free survival according to SUVmax values. |
Subgroup analysis
In EGFR-sensitizing mutation group, eleven of the patients had SUVmax values ≤11 and 15 of the patients had SUVmax values >11. Accordingly, the 3-month PFS rates were 100% vs 53.3% (P=0.08), 6-month PFS rates were 100% vs 13.3% (P<0.001), and 12-month PFS rates were 81.3% vs 13.3% (P<0.001), favoring the group having SUVmax ≤11.
In the EGFR negative group, ten of the patients had SUVmax values ≤11 and seven of the patients had SUVmax values >11. Accordingly, the 3-month PFS rates were 60% vs 0% (P=0.01), 6-month PFS rates were 50% vs 0% (P=0.026), and 12-month PFS rates were 50% vs 0% (P=0.026), favoring the group having SUVmax ≤11.
In the EGFR unknown group, ten of the patients had SUVmax values ≤11 and seven of the patients had SUVmax values >11. Accordingly, 3-month PFS rates were 70% vs 0% (P=0.004), 6-month PFS rates were 50% vs 0% (P=0.026), and 12-month PFS rates were 40% vs 0% (P=0.056), favoring the group having SUVmax ≤11.
Subgroup analysis according to smoking habit
Eleven of the patients were smokers and 15 of the patients were non-smokers in patients who had SUVmax ≤11. Using multivariate binary logistic regression analyses, OR for 3, 6, and 12-month PFS rates were 18.29 (95% CI: 3.66–91.3, P=0.001), 57.7 (95% CI: 7.98–417, P<0.001), and 22.2 (95% CI: 4.17–118, P<0.001), respectively, in patients who had SUVmax value ≤11 and were non-smokers (Table 2). Fourteen of the patients were smokers and 15 of the patients were non-smokers in patients who had SUVmax >11. The 3-month PFS rates of these patient groups were 0% and 53.3% (P=0.002), 6-month PFS rates were 0% and 13.3% (P=0.483), and 12-month PFS rates were 0% and 13.3% (P=0.483).
According to EGFR mutation status, there were five smokers and 21 non-smokers in the EGFR-sensitizing group. The 3-month PFS rates were 20% and 85.7% (P=0.03), 6-month PFS rates were 20% and 57.1% (P=0.322), and 12-month PFS rates were 20% and 47.6% (P=0.356) in the smoker and non-smoker groups, respectively. There were 13 smokers and four non-smokers in the EGFR negative group. The 3-month PFS rates were 30% and 50% (P=0.482), 6-month PFS rates were 23.1% and 50% (P=0.301), and 12-month PFS rates were 23.1% and 50% (P=0.301) in the smoker and non-smoker groups. There were eleven smokers and six non-smokers in EGFR unknown group. Three-month PFS rates were 45.5% and 33.3% (P=0.627), 6-month PFS rates were 27.3% and 33.3% (P=0.793), and 12-month PFS rates were 37.3% and 16.7% (P=0.622) in the smoker and non-smoker groups, respectively. Using multivariate binary logistic regression analyses based on EGFR-sensitizing mutation and non-smoking, OR was 2.64 (95% CI: 0.75–921, P=0.127) for 3 months PFS rate, OR was 1.46 (95% CI: 0.42–5.03, P=0.54) for 6 months PFS rate, and OR was 1.5 (95% CI: 0.42–5.26, P=0.52) for 12 months PFS rate (Table 2).
Discussion
New diagnostic and treatment strategies provide more successful survival rates in patients with lung cancer. For the first-line treatment of NSCLC, use of platinum-doublet chemotherapy for patients with good PS has been widely accepted. According to one meta analysis, the 1-year survival for the platinum-containing regimens was 34% (95% CI: 33%–36%) and 29% (95% CI: 27%–30%) for the nonplatinum therapies.12 The standard first-line treatment for patients with EGFR-sensitizing mutations is EGFR TKIs.13 Mok et al showed that the 12-month rates of PFS were 24.9% with gefitinib and 6.7% with carboplatin–paclitaxel in patients having EGFR mutation in the first-line treatment of advanced NSCLC patients selected on the basis of clinical characteristics that included a history of no smoking or light smoking as well as histologic evidence of adenocarcinoma. The gefitinib group had a significantly longer median PFS (10.8 vs 5.4 months in the chemotherapy group; hazard ratio [HR] 0.30; 95% CI: 0.22–0.41; P<0.001) and the median overall survival was 30.5 vs 23.6 months, respectively (P=0.31).14 And also it was shown that afatinib is associated with prolongation of PFS when compared with standard doublet chemotherapy in patients with advanced lung adenocarcinoma with EGFR mutations (median PFS was 11.1 months for afatinib and 6.9 months for chemotherapy (HR 0.58; 95% CI: 0.43–0.78; P=0.001).15 Similar finding was achieved with erlotinib in ENSURE study.16 Although EGFR-sentizing mutations are the most important predictive markers of clinical outcome for EGFR-TKIs treatment in advanced NSCLC, according to DELTA trial there was not statistically differences after the first-line treatment. DELTA trial which assessed the efficacy of erlotinib versus docetaxel in second-line and third-line therapy in 255 patients with EGFR-mutant and wild-type tumors. A total of 51 EGFR-mutant patients assessed and PFS was 9.3 vs 7 months in erlotinib vs docetaxel group (HR 0.96; 95% CI: 0.51–1.79; P=0.91) and it was 1.3 vs 2.9 months in patients with EGFR wild-type tumor (HR 1.45; 95% CI: 1.09–1.94; P=0.01).17 Thus, the presence of EGFR-sensitizing mutation was insufficient to predict the outcome of treatment after the first-line therapy.
Despite the EGFR-sentizing mutations, drug resistance may unavoidably appear, and the disease eventually progresses. The mechanisms of secondary resistance to EGFR TKIs include the acquisition of the T790M gatekeeper mutation, mesenchymal–epithelial transition amplification, and transformation into small-cell lung cancer. And also, approximately 30% of the patients with EGFR-sensitizing mutations do not exhibit objective responses to EGFR TKIs within 3 months. Although possible mechanisms have been investigated in several preclinical and retrospective studies, the mechanism of primary resistance to EGFR TKIs in EGFR-mutant NSCLC has not been clearly understood. V-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations, mesenchymal-epithelial transition amplification, and phosphatase and tensin homolog loss could be related to the response to TKIs in these groups.18
Erlotinib is registered for the treatment of all patients with advanced NSCLC and prolongs survival after first-line, second-line chemotherapy, and maintenance therapy in patients having an EGFR mutation and also wild-type tumors. The survival benefit of erlotinib is unlikely to be solely due to the EGFR mutations and other molecular mechanisms probably also contribute to the effect. The SATURN trial showed that patients with wild-type tumors who had been treated with first-line platinum-doublet chemotherapy also benefit from maintenance treatment with erlotinib and have prolonged PFS when compared with placebo in patients with stable disease and complete response/partial response. The HR for erlotinib benefit was 0.68 in the stable disease group (95% CI: 0.56–0.83; P<0.0001) with a median PFS of 12.1 vs 11.3 weeks (2.8 vs 2.6 months), respectively. The HR in the complete response/partial response group was 0.74 (0.60–0.92; P=0.0059) with a median PFS of 12.4 vs 11.1 weeks (2.9 vs 2.6 months), respectively.19 One placebo-controlled phase III study investigated the effect of gefitinib on survival as second-line or third-line treatment for patients with advanced NSCLC with unknown EGFR status. Subgroup analyses showed significantly longer survival in the gefitinib group than the placebo group for never-smokers (P=0.012; median survival 8.9 vs 6.1 months) and patients of Asian origin (P=0⋅01; median survival 9.5 vs 5.5 months).20
TKIs, docetaxel, and pemetrexed are approved for the second-line treatment of NSCLC.21 TITAN trials were conducted to show that was no significant differences in efficacy between patients treated with erlotinib and those treated with docetaxel or pemetrexed in second-line therapy. Median PFS in the erlotinib group was 6.3 weeks (95% CI: 6.1–6.9) vs 8.6 weeks (7.1–12.1) in the chemotherapy group. There was no statistically significant difference in PFS between the two treatment groups (HR: 1.19, 95% CI: 0.97–1.46; P=0⋅089). In this study, the detected rate of EGFR-sensitizing mutation was only 3% and 2% in erlotinib group and chemotherapy group, respectively, and smoking status was not a predictive factor.22 Hellenic Oncology Research Group study assesses the efficacy of pemetrexed versus erlotinib in pretreated patients with advanced NSCLC. The median PFS was 2.9 months (range: 0.4–27.3 months) and 3.6 months (range: 0.2–47.8 months) for the pemetrexed and erlotinib arms, respectively (P=0.136). No difference was observed in treatment line or smoking status between the treatment arms. However, the presence of KRAS mutation was reported to be a possible negative predictive factor for response to EGFR TKIs.23 In contrast, TAILOR study, which compared erlotinib and docatexel in the treatment of NSCLC showed that KRAS mutational status and smoking status were not predictive for response.24
In this context, new instruments are needed to predict the response to TKIs, which have a wide indication of use in first-line and sequential therapies. This study specifically focused on the role of pretreatment 18F-FDG PET in providing prognostic information in response to erlotinib for patients with metastatic-stage lung adenocarcinoma at first-line and after first-line therapy. Nevertheless, EGFR-sensitizing mutation is an absolute predictor for TKIs selection at first-line therapy, TKIs were not statistically superior to chemotherapy after first-line treatment. Studies investigating the predictive value of smoking habit and K-RAS mutation showed controversial results as mentioned earlier. Along with various studies done on many genetic mutations, these tests are both costly and also cannot explain the majority of cases who have primary and secondary resistance in EGFR-sensitizing patient and patients with wild-type tumors.
Scheffler et al showed that the identification of the lesion with the highest metabolic activity in FDG PET has significant prognostic relevance before the initiation of erlotinib therapy independent to EGFR mutation status in patients with advanced NSCLC.25 Accordingly, patients with an 18F-FDG SUVmax value less than 6.6 had a significantly better overall survival (16.3 months, 95% CI 7.1–25.4 months) compared to patients with an 18F-FDG SUVmax value more than 6.6 (3.1 months, 95% CI: 0.6–5.5 months, P<0.001) in the first-line therapy. However, five patients had an EGFR-sensitizing mutation in this study. The current retrospective study shows that for patients with metastatic lung adenocarcinoma with EGFR-sensitizing patients or wild-type tumor, there is a correlation between treatment response to erlotinib and 18F-FDG PET activity for first-line and after first-line therapy.
EGFR-sensitizing mutation provided a statistically better 3-month PFS rate compared with wild-type and EGFR unknown groups; however, it was not significantly different for 6 and 12-month rates of PFS (P=0.026, P=0.267, and P=0.408, respectively). However, the stratification of EGFR-sensitizing group according to SUVmax value revealed that 3, 6, and 12-month rates of PFS were statistically significant favoring the SUVmax≤11 group (P=0.08, P<0.001, and P<0.001, respectively). Also, none of the patients who had SUVmax>11 responded to erlotinib treatment in wild-type and EGFR unknown groups. Although cranial metastasis is a worse prognostic factor for lung cancer, 3, 6, and 12-month PFS rates were not associated with the presence of cranial metastasis (P=0.78, P=1.0, and P=0.31, respectively). This finding suggests the better efficiency of tyrosine kinase inhibitors for cranial metastasis.
Although there is not a hypothesis indicating the association between smoking and SUVmax values, one retrospective study analyzed the relations between the smoking history and SUVmax value in operated patients with NSCLC. Accordingly, the SUVmax of never-smokers (median 6.0, range: 1.2–24) was lower than the ever-smokers (median 10.9, range: 1.0–29.0, P<0.001). In our study, the median SUVmax value of smokers (median 11, range: 4.0–24.6) vs non-smokers was not different (median 11, range: 3.8–20.1, P=0.303), unlike this study.26
Smoking habit was a predictive variable for 3, 6, and 12-month PFS rates in patients who have SUVmax value ≤11; however, according to the EGFR mutation status, smoking habit was not associated with 3, 6, and 12-month PFS rates. Furthermore, independent to EGFR mutation status, none of the smoker patients who have SUVmax value above 11 responded to erlotinib treatment. This data suggest that non-smoking may predict the response to erlotinib treatment when evaluated with SUVmax value.
A limitation of this study is the low number of patients in each group. However, despite the low number of patients, we were able to find a remarkable significance in all groups. Therefore, we think that it is worthy of consideration on the findings of this study to pave the way of designing prospective studies with more patients.
Conclusion
Despite the predictive value of the EGFR-sensitizing mutation, erlotinib performed a low efficiency in patients who have SUVmax values >11. Additionally, erlotinib had no efficiency in patients who have SUVmax values >11 in wild-type and EGFR-unknown groups. This study indicated that initial 18F-FDG PET/CT SUVmax value is a prognostic instrument for lung cancer patients who treated with erlotinib, which is an approved drug in the sequential treatment of lung adenocarcinoma independent to EGFR mutation status.
Disclosure
The authors report no conflicts of interest in this work.
References
Paesmans M, Sculier JP, Libert P, et al. Prognostic factors for survival in advanced non-small-cell lung cancer: univariate and multivariate analyses including recursive partitioning and amalgamation algorithms in 1,052 patients. J Clin Oncol. 1995;13:1221–1230. | ||
Jiang AG, Chen HL, Lu HY. The relationship between glasgow prognostic score and serum tumor markers in patients with advanced non-small cell lung cancer. BMC Cancer. 2015;15:386. | ||
Simmons CP, Koinis F, Fallon MT, et al. Prognosis in advanced lung cancer – a prospective study examining key clinicopathological factors. Lung Cancer. 2015;88:304–309. | ||
Maemondo M, Inoue A, Kobayashi K, et al. North-East Japan Study Group. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–2388. | ||
Engle JA, Kolesar JM. Afatinib: a first-line treatment for selected patients with metastatic non-small-cell lung cancer. Am J Health Syst Pharm. 2014;71:1933–1938. | ||
Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–2139. | ||
Rosell R, Moran T, Queralt C, et al; Spanish Lung Cancer Group. Screening for epidermal growth factor receptor mutations in lung cancer. N Engl J Med. 2009;361:958–967. | ||
Pircher A, Ulsperger E, Hack R, et al. Basic clinical parameters predict gefitinib efficacy in non-small cell lung cancer. Anticancer Res. 2011;31:2949–2955. | ||
Miller VA, Kris MG, Shah N, et al. Bronchioloalveolar pathologic subtype and smoking history predict sensitivity to gefitinib in advanced non-small-cell lung cancer. J Clin Oncol. 2004;22:1103–1109. | ||
Sasaki R, Komaki R, Macapinlac H, et al. [18F]fluorodeoxyglucose uptake by positron emission tomography predicts outcome of non-small-cell lung cancer. J Clin Oncol. 2005;23:1136–1143. | ||
Hoang JK, Hoagland LF, Coleman RE, Coan AD, Herndon JE, Patz EF Jr. Prognostic value of fluorine-18 fluorodeoxyglucose positron emission tomography imaging in patients with advanced-stage non-small-cell lung carcinoma. J Clin Oncol. 2008;26:1459–1464. | ||
D’Addario G, Pintilie M, Leighl NB, Feld R, Cerny T, Shepherd FA. Platinum-based versus non-platinum-based chemotherapy in advanced non-small-cell lung cancer: a meta-analysis of the published literature. J Clin Oncol. 2005;23:2926–2936. | ||
Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–742. | ||
Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. | ||
Sequist LV, Yang JC, Yamamoto N, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31:3327–3334. | ||
Wu YL, Zhou C, Liam CK, et al. First-line erlotinib versus gemcitabine/cisplatin in patients with advanced EGFR mutation-positive non-small-cell lung cancer: analyses from the phase III, randomized, open-label, ENSURE study. Ann Oncol. 2015;26:1883–1889. | ||
Kawaguchi T, Ando M, Asami K, et al. Randomized phase III trial of erlotinib versus docetaxel as second- or third-line therapy in patients with advanced non-small-cell lung cancer: Docetaxel and Erlotinib Lung Cancer Trial (DELTA). J Clin Oncol. 2014;32:1902–1908. | ||
Lee JK, Shin JY, Kim S, et al. Primary resistance to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) in patients with non-small-cell lung cancer harboring TKI-sensitive EGFR mutations: an exploratory study. Ann Oncol. 2013;24:2080–2087. | ||
Coudert B, Ciuleanu T, Park K, et al. SATURN Investigators. Survival benefit with erlotinib maintenance therapy in patients with advanced non-small-cell lung cancer (NSCLC) according to response to first-line chemotherapy. Ann Oncol. 2012;23:388–394. | ||
Thatcher N, Chang A, Parikh P, et al. Gefitinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebo-controlled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet. 2005;366:1527–1537. | ||
Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clin Oncol. 2000;18:2095–2103. | ||
Ciuleanu T, Stelmakh L, Cicenas S, et al. Efficacy and safety of erlotinib versus chemotherapy in second-line treatment of patients with advanced, non-small-cell lung cancer with poor prognosis (TITAN): a randomised multicentre, open-label, phase 3 study. Lancet Oncol. 2012;13:300–308. | ||
Karampeazis A, Voutsina A, Souglakos J, et al. Pemetrexed versus erlotinib in pretreated patients with advanced non-small cell lung cancer: a Hellenic Oncology Research Group (HORG) randomized phase 3 study. Cancer. 2013;119:2754–2764. | ||
Garassino MC, Martelli O, Broggini M, et al. Erlotinib versus docetaxel as second-line treatment of patients with advanced non-small-cell lung cancer and wild-type EGFR tumours (TAILOR): a randomised controlled trial. Lancet Oncol. 2013;14:981–988. | ||
Scheffler M, Zander T, Nogova L, et al. Prognostic impact of [18F]fluorothymidine and [18F]fluoro-D-glucose baseline uptakes in patients with lung cancer treated first-line with erlotinib. PLoS One. 2013;8:e53081. | ||
Na II, Park JY, Kim KM, et al. Significance of smoking history and FDG uptake for pathological N2 staging in clinical N2-negative non-small-cell lung cancer. Ann Oncol. 2011;22:2068–2072. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.