")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Prognostic factors for cesarean section outcome of pregnant women with gestational diabetes mellitus: a systematic review and meta-analysis
Authors Wang J, Chen K, Jin X, Li X, An P , Yang N , Chen Y, Fang Y, Mu Y
Received 21 September 2018
Accepted for publication 15 February 2019
Published 21 June 2019 Volume 2019:12 Pages 913—929
DOI https://doi.org/10.2147/DMSO.S188293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Jinjing Wang,1,2,* Kang Chen,1,* Xinye Jin,1 Xueqiong Li,3 Ping An,1 Nan Yang,4 Yaolong Chen,4 Yi Fang,2 Yiming Mu1
1Department of Endocrinology, Chinese PLA General Hospital, Beijing 100853, People’s Republic of China; 2Department of Endocrinology, Fifth Medical Center of PLA General Hospital, Beijing 100071, People’s Republic of China; 3Department of Gerontology, First Affiliated Hospital of Kunming Medical University, Kunming 650031, People’s Republic of China; 4Evidence-Based Medicine Center, School of Basic Medical Sciences, Lanzhou University, Lanzhou, 730000, People’s Republic of China
*These authors contributed equally to this work
Objective: To evaluate the prognostic factors for cesarean section outcome of pregnant women with diabetes mellitus.
Methods: MEDLINE, EMBASE, Cochrane Library, CBM, CNKI and Wanfang database were searched. Two researchers independently screened the literature, extracted data, and evaluated the risk of bias of included studies. For pooled data with factors of perioperative outcome, the RevMan software was used for data translation and meta-analysis. The result is shown intuitively with the bubble diagram of evidence mapping by Excel 2016.
Results: We included 12 randomized controlled trials (RCTs) in the meta-analysis. Twelve RCTs with 1,390 patients were included in the systematic review. The results show that the perioperative blood glucose management regimens, preoperative fasting and water deprivation, anesthesia regimens, postoperative fluid regimens, postoperative analgesia regimens, postoperative wound care regimens, psychological interventions, different dosing regimens for antibiotics, and obesity may affect the cesarean section outcome of diabetic mothers and newborns. The evidence for all the outcomes was low quality.
Conclusion: Many prognostic factors have shown significant association with postoperative outcomes of cesarean section. More clinical research evidence with high-quality is needed.
Keywords: gestational diabetes mellitus, caesarean section, prognostic factors, systematic review, meta-analysis, evidence mapping
Background
In pregnant women with gestational diabetes mellitus (GDM), the overall cesarean section rate was accounted for 35.3%.1 Simultaneously, compared with nondiabetic pregnant women, diabetic maternal acute cesarean section rate was reported 1.52 times of GDM.2 Diabetes is an important risk factor for surgical incision infection,3 and for cesarean section, diabetes is an important risk factor for maternal postoperative wound infection as well.4 Thus, the pregnancy with diabetes and the management of special risk factors are important, and the existing systematic evaluation shows that effective treatment and control of GDM can reduce preeclampsia, shoulder dystocia, and the incidence of huge children.5 In addition, several systematic reviews have concentrated on the effects of certain specificc factors based on the health outcomes of pregnant women with GDM, such as the effects of different glycemic management regimens on glycemic control and maternal and child outcomes,6–10 and effects of dietary intervention or nutritional therapy based on maternal and child outcomes.11,12 For patients with cesarean section with GDM, there have been several studies evaluating differences in patients’ outcomes under different conditions, such as anesthesia,13–15 postoperative fluid regimen,16,17 and postoperative wound care.18 However, there is no systematic review regarding the current evaluation of the factors affecting the maternal and child’s outcomes during the period of affecting by GDM. This study was designed to assess the risk factors associated with perioperative outcomes in pregnant women with GDM.
Methods
Inclusion and exclusion criteria
Inclusion criteria: 1) pregnant women suffered cesarean section with GDM; 2) exposure factors for cesarean outcomes; 3) RCTs; and 4) reported perioperative outcomes, such as blood glucose level, Apgar scores, adverse effects, and so on. Exclusion criteria: 1) there were no specific outcome data to assess the impact of exposure factors on patients with perioperative outcomes; 2) non-English and Chinese published research, 3) summary of unpublished meeting.
Literature search
We conducted a systematic search on Medline (via PubMed), EMBASE, Cochrane Library, CBM, CNKI and Wanfang, using the terms Diabetes, Gestational, Diabet*, “Cesarean Section”, caesarean, “diabetes, pregnancy”, “gestational diabetes mellitus”, “cesarean section”, “cesarean section”, “caesarean section”. The retrieval date was February 28, 2018.
Study screening
Two researchers independently screened the literature titles, abstracts, and the full text. A pre-test was performed prior to formal screening of the literature to ensure that each researcher truly perceived the screening criteria and process. Discrepancies between the two reviewers were resolved by consensus discussion.
Data extraction
The two researchers independently extracted the following data from the pre-designed information extraction table: year of publication, name of journal, the first author’s affiliation, place and duration of study, funding, conflict of interest, type of study, sample size, basic characteristics of study object, exposure factors, and associated outcome data. A pretest was conducted before formal extraction to ensure that each researcher agrees with the extraction criteria and process. If there are some differences, they could be solved through discussion.
Risk of bias assessment
Two researchers used the Cochrane risk of bias tool was used for bias risk assessment of randomized controlled trials. A pretest was conducted before the formal evaluation to ensure that each researcher agrees with the evaluation criteria and process. In case of existence of some differences, they could be solved by a third researcher.
Data consolidation and analysis
In the RevMan 5.3 software, the RR and 95% CI were used to combine the binary data, and the data were merged using the mean difference (MD) and 95% CI. The data combination uses a random-effect model. The heterogeneity was included in the study by Cochran’s Q test (P<0.05 denotes heterogeneity) and I2 test. When the number of inclusion indicators is ≥10, the publication bias is evaluated by making a funnel plot; conversely, the qualitative analysis was included in the study funding, the conflict of interest, and the outcome to discuss the possibility of publication bias.
Quality of evidence
The quality of the evidence was graded according to the principles of the GRADE approach used in the evaluation of prognostic studies19,20 and in a previous study (as example).21 (These factors may lead to rating down the quality of evidence in GRADE system) and the three upgraded factors (large effect, dose-response, and plausible confounders) to determine the final level of evidence. Quality of evidence was ranked as high, medium, low, and very low-level using the results of summary table.
Evidence mapping
Excel 2016 was used to integrate the RR value from meta-analysis and GRADE. The result is shown intuitively with the bubble diagram. Due to heterogeneity of MD for the outcome, we did not make a bubble diagram for MD value from meta-analysis.
Results
Study selection
There are 13,447 articles identified by literature search. After duplicates were removed in endnote, 11,585 records titles and abstractswere reviewed, 142 articles were retrieved full-text reviewing. Finally, a total of 12 randomized controlled trials14,16–18,22–29 involving 1,390 patients were included for meta-analysis (Figure 1).
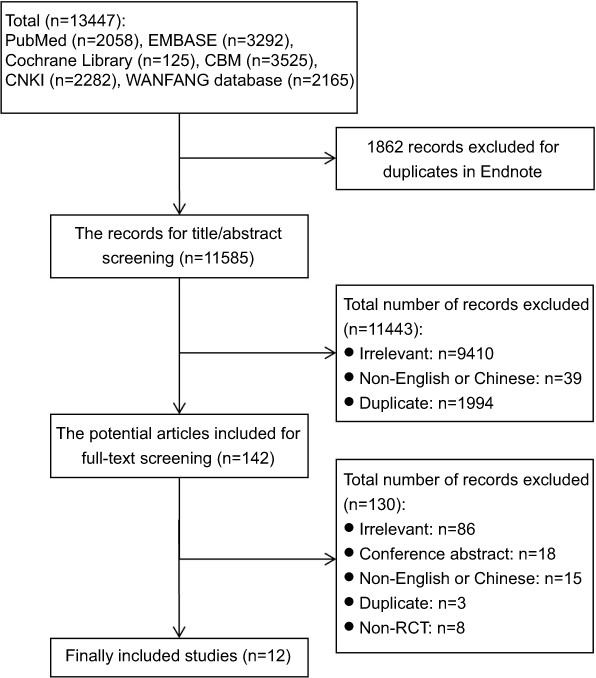 | Figure 1 The screening flow chart. |
Characteristics of the included studies
The studies were published in 2010 and 2017, the sample sizes ranged from 33 to 201. All studies were from China. The participant age was from 24 to 39. The two studies16,23 were funded by nonprofit funds, one study reported that there was not the conflict of interest, and the rest of the study did not report funding (Table 1).
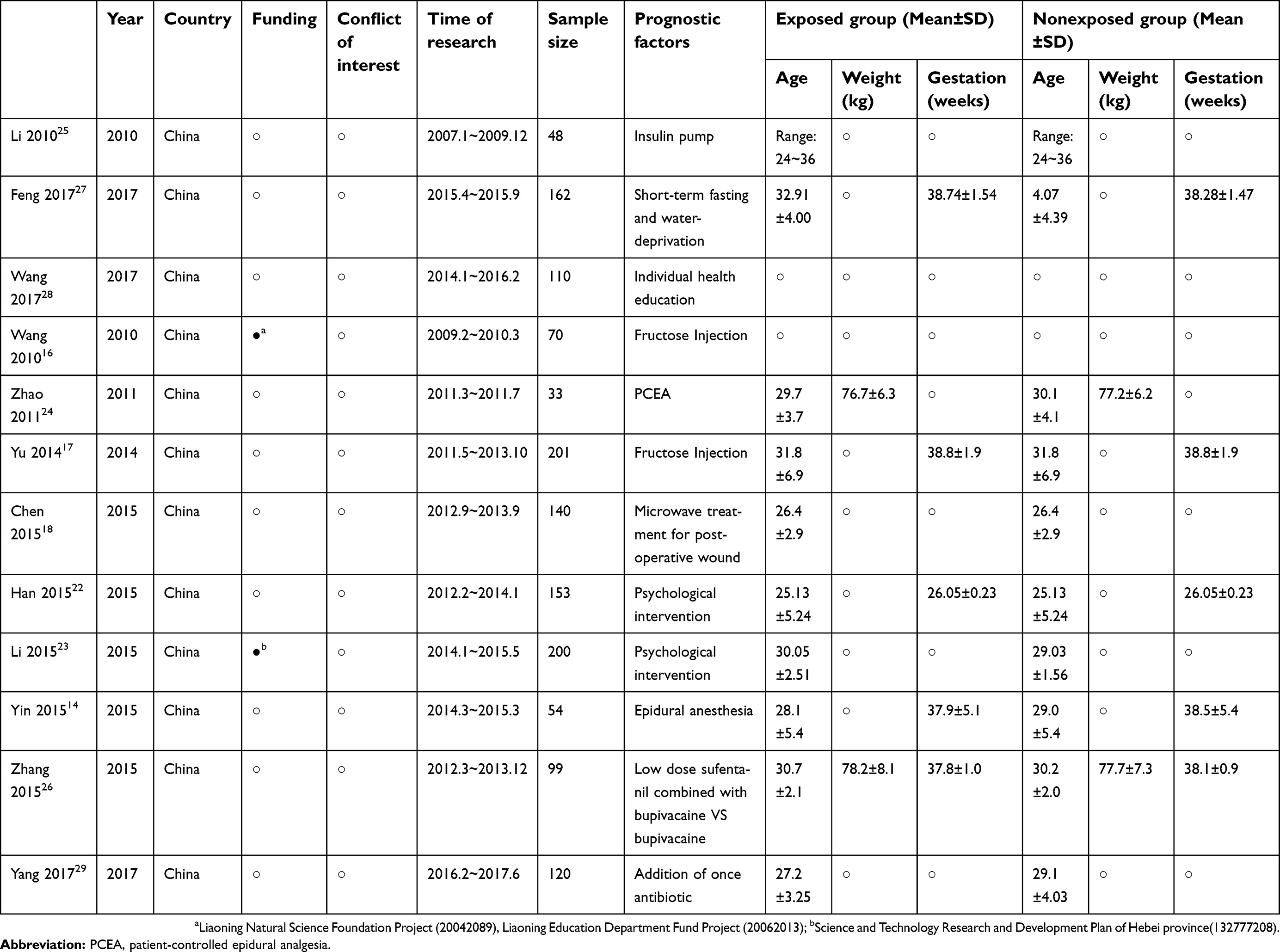 | Table 1 Basic characteristics of included studies |
Risk of bias for included studies
The included RCTs were only low risk of bias in incomplete outcome data and selective reporting (Figure 2); 8 studies14,17,18,24–26,29 did not report random sequences; 1 study27 reported that there was a high risk of bias in random sequences; none of the studies reported allocation concealment; 6 studies16,18,26–29 did not blind the researchers and patients, and they likely contained an impact on the results; 8 studies14,18,22–26,29 did not blind the outcome evaluators, and they likely contained an influence on the results.
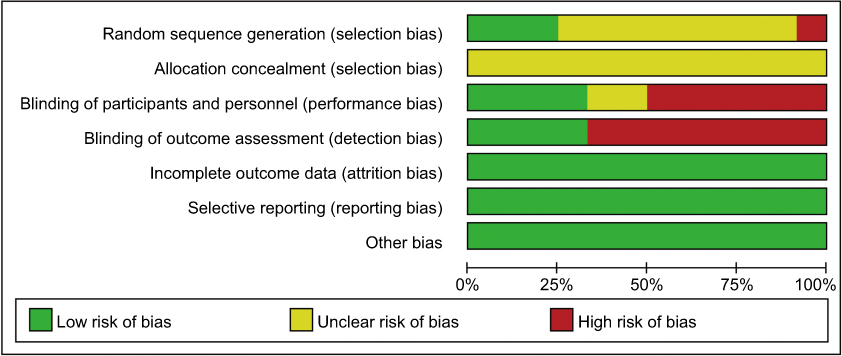 | Figure 2 Risk of bias graph. |
Prognostic factors
Insulin pump
One randomized controlled study25 reported a total of 3 outcomes. It was revealed that duration of treatment process (MD=−5.30, 95% CI: −5.78~−4.82, P<0.00001), insulin dosage (MD=17.00, 95% CI: −23.04~−10.96, P<0.00001), and the incision healing duration (MD=−4.40, 95% CI: −5.58~−3.22, P<0.00001) of the repeated subcutaneous injection for insulin group were superior to those of the insulin pump group, and the difference was statistically significant (
Short-term fasting and water deprivation
One randomized controlled study27 reported a total of 11 outcomes. Preoperative blood glucose concentrations (MD=0.84, 95% CI: 0.42~1.26, P=0.001) and the level of blood glucose in newborn infants after birth (MD=0.45, 95% CI: −0.03~0.87, P=0.038) for short-term group were superior to those of long-term group, and the difference was statistically significant. Bleeding volume during cesarean section (MD=−42.71, 95% CI:−82.55~−2.86, P=0.039) for short-term group was inferior to long-term group, and the difference was statistically significant. There were no significant differences in postoperative blood sugar concentrations, the rates of nausea and vomiting, incidence of hypoglycemia in newborn infants after birth and mothers before cesarean section, duration of anus exhausting of puerpera, Apgar score 1 and 5 mins after delivery (
Individual health education
A randomized controlled study28 reported a total of 4 outcomes. Control rates for 2 hr plasma glucose (PG) (RR=1.31, 95% CI: 1.04~1.66, P<0.05) and midnight blood glucose (RR=1.23, 95% CI: 1.01~1.50, P<0.05) and the satisfaction rate of nursing services (MD=6.51, 95% CI: 5.80~7.22, P<0.01) for individualized health education group were superior to those of conventional health education group, and the difference was statistically significant. There were no significant differences in control rates of fasting blood glucose (FBG) as well (
Fructose injection
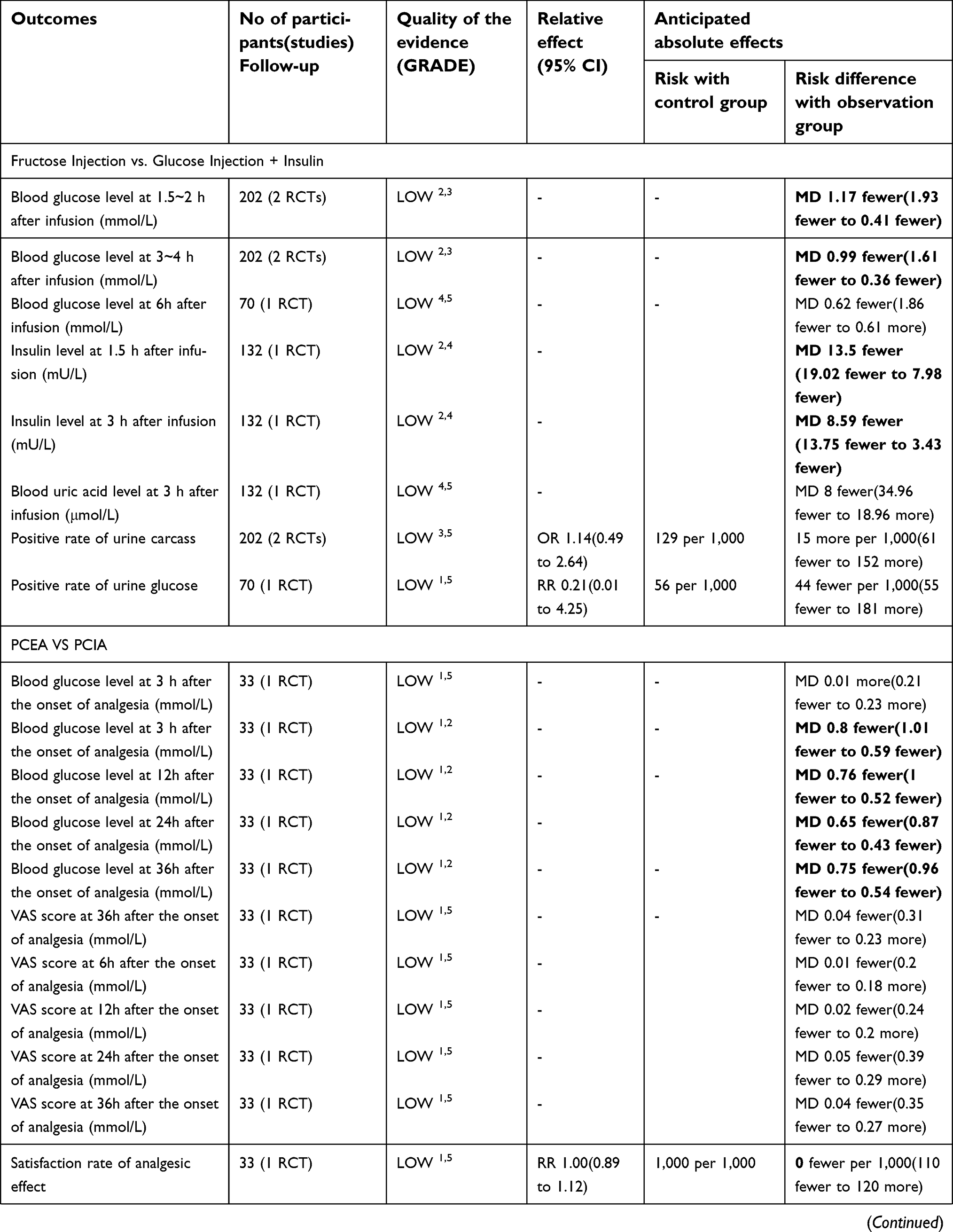
Two randomized controlled trials16,17 reported a total of 8 outcomes. The blood glucose levels 1.5–2 hours after infusion (MD=−1.17, 95% CI: −1.93~−0.41, P=0.003), blood glucose levels 3–4 hours after infusion (MD=−0.99, 95% CI: −1.61−0.36, P=0.002), the level of insulin 1.5 hours after infusion (MD=−13.50, 95% CI: −19.02~−7.98) (P<0.00001), and the level of insulin 3 hours after infusion (MD=−8.59, 95% CI: −13.75~−3.43, P=0.001) for fructose injection were superior to glucose and Insulin injection. The difference was statistically significant. There were no significant differences in blood glucose level, blood glucose level, urinary carcass positive rate, and urine sugar positive rate after transfusion, and no significant difference was found between the two groups (
Patient-controlled epidural analgesia (PCEA)
A randomized controlled trial24 reported a total of 13 outcomes. The level of blood glucose in presence of analgesia after 6 hours (MD=−0.80, 95% CI: −1.01 to −0.59, P<0.00001), 12 hours (MD=−0.76, 95% CI: −1.00 to −0.52, P<0.00001), 24 hours (MD=−0.65, 95% CI: −0.87 to −0.43, P<0.00001), and 36 hours (MD=−0.75,95% CI: −0.96~−0.54, P<0.00001) for the patient-controlled intravenous analgesia (PCIA) group was superior to PCIA group. The difference was statistically significant. There was no significant difference between the two groups (
Microwave treatment for postoperative wound
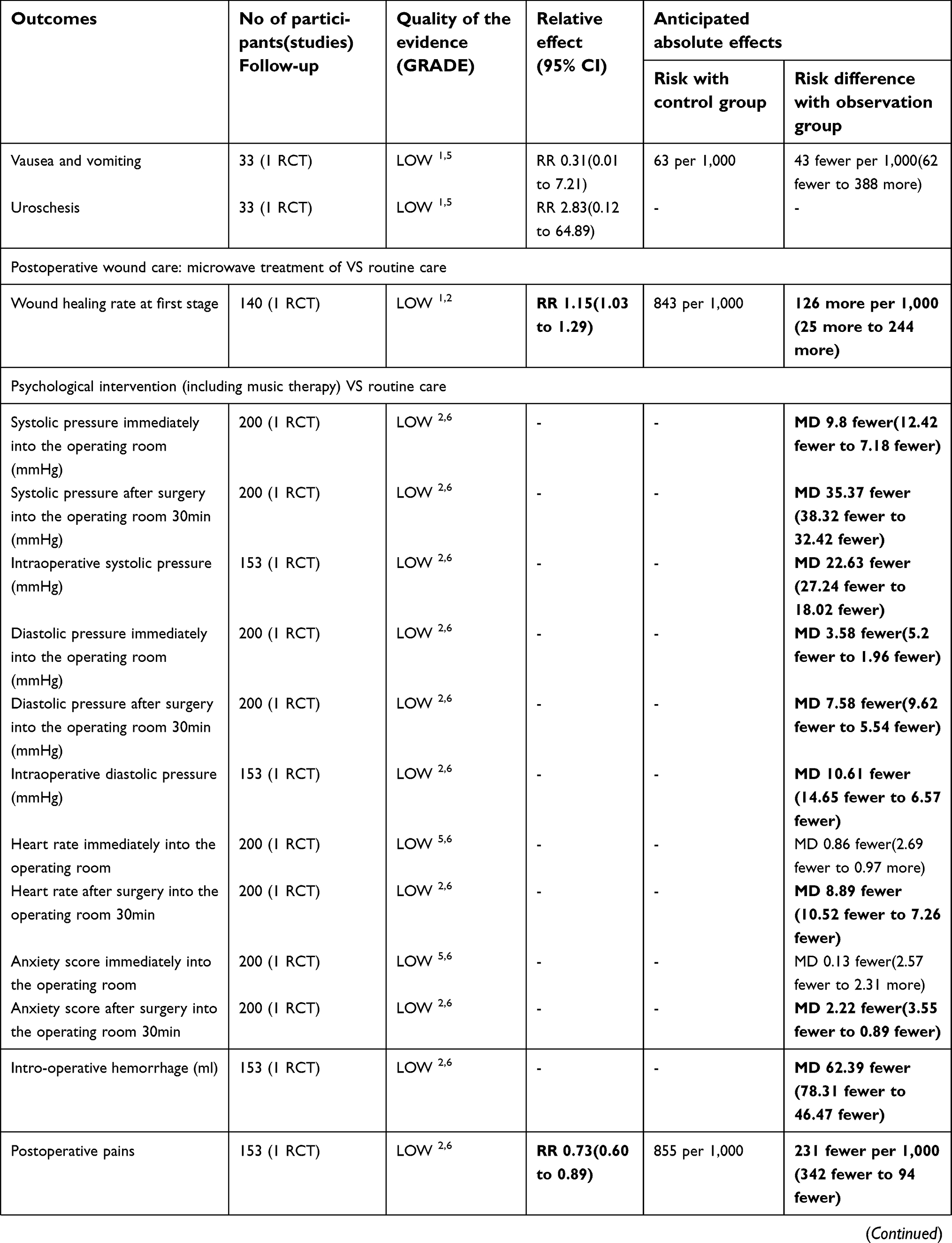
A randomized controlled trial18 reported a outcome (RR=1.15, 95% CI: 1.03~1.29, P=0.01, see Appendix 1, in which the difference was statistically significant (P<0.01) (
Psychological intervention (including music therapy)
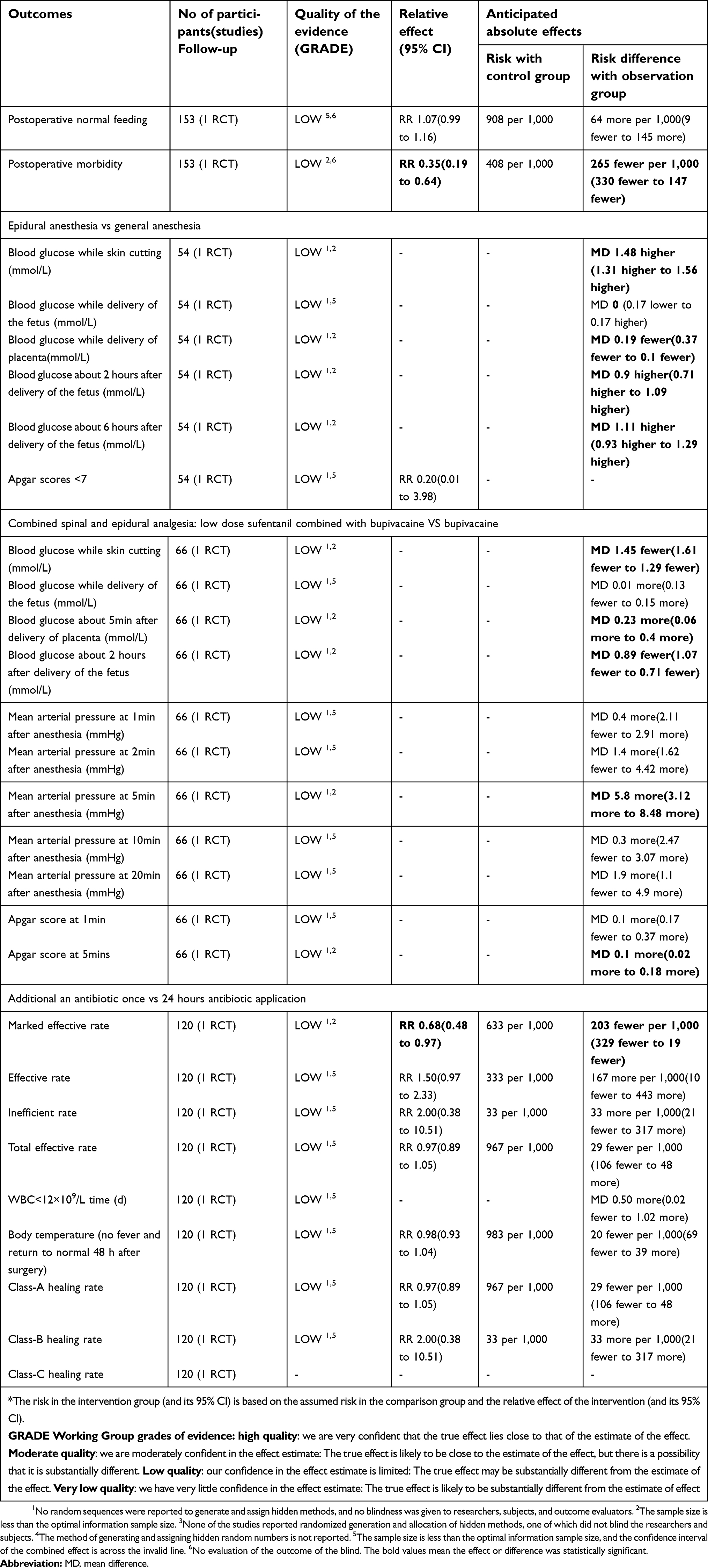
Two randomized controlled trials22,23 reported a total of 14 outcome indicators, in addition to entering the operating room immediately with heart rate (MD=−0.86, 95% CI: −2.69~0.97, P=0.36), entering the operating room immediately with anxiety score (MD=−0.13, 95% CI: −2.57~2.31, P=0.92), and the normal feeding rate (RR=1.07, 95% CI: 0.99–1.16, P=0.09). The difference between the two groups was not statistically significant. The rest of the outcome indicators for the psychological intervention group were inferior to the conventional nursing group, and the difference between the two groups was statistically significant (
Epidural anesthesia
A randomized controlled trial14 reported a total of six outcomes: glucose concentration at the of cutting skin (MD=1.48, 95% CI: 1.31~1.65, P<0.00001, 2 hours after delivery (MD=0.90, 95% CI: 0.71 to 1.09, P<0.00001) and 6 hours after delivery (MD=1.11, 95% CI: 0.93 to 1.29, P<0.00001), the epidural group were higher than the general anesthesia group, and the difference was statistically significant. The differences in the other outcomes between the two groups were not statistically significant (
Low-dose sufentanil combined with bupivacaine of spinal-epidural anesthesia
One randomized controlled study26 reported a total of 11 outcomes. Based on the report, glucose concentration at the time of cutting skin (MD=−1.45, 95% CI: −1.61~−129, P<0.00001), the blood glucose concentration 2 hours after delivery (MD=−0.89, 95% CI: −1.07~−071, P<0.00001), and the mean arterial pressure 5 mins after anesthesia (MD=5.80, 95% CI: 3.12~8.48, P<0.00001) were assessed. The difference was statistically significant. However, the differences for the other outcome indicators between the two groups were not statistically significant (
Addition of once antibiotic
One randomized controlled study29 reported a total of 12 outcomes. The treatment efficiency (RR=0.68, 95% CI: 0.04~1.66, P<0.05) of the addition of an antibiotic once group was inferior to 24 hours antibiotic application group, and the difference was statistically significant. There were no significant differences in response rate, overall response rate, the inefficiency rate, the duration of WBC <12×109/L, body temperature (without fever or returned to normal status 2 hours after surgery), and the grades A, B, and C of healing (
Publication bias
The number of studies included in every outcome was <10; thus, it was unattempted to use funnel plot to assess the publication bias. All studies have not reported conflict of interest, and only 2 studies reported that the funding originated from the nonprofit grants.
Quality of evidence
The levels of evidence for all the outcome all is low on the GRADE system (see
Evidence mapping
Each bubble corresponds to one outcome for the prognostic factors. The size, color, and position of the bubbles were used to indicate the current research status. The size of the bubbles indicates the sample size, and the color of the bubbles indicates the quality of the evidence. The horizontal coordinate indicates the prognostic factors, the vertical coordinate indicates the RR of meta-analysis (Figure 3).
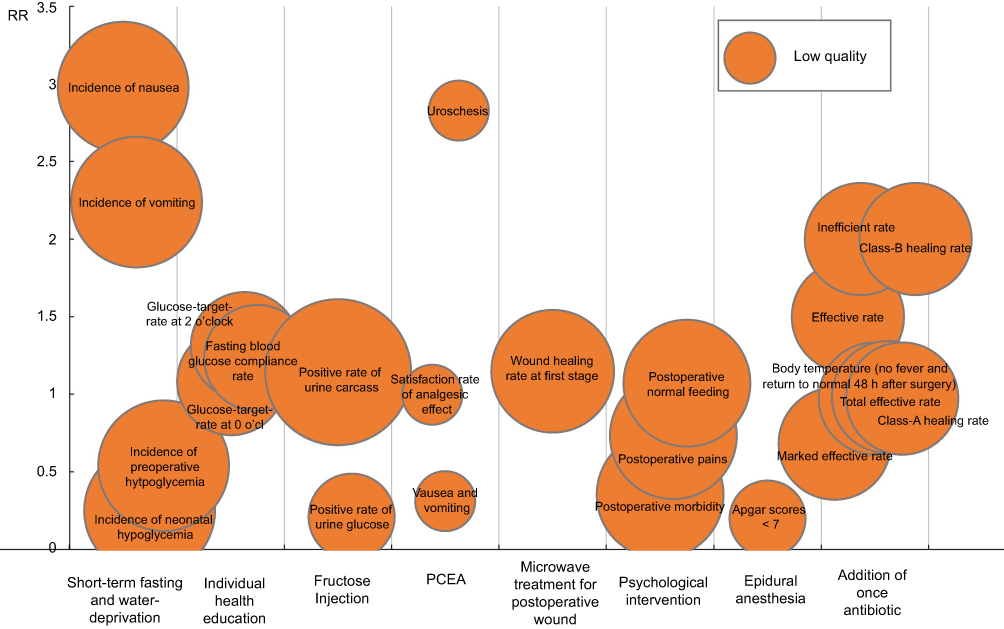 | Figure 3 Summary of risk ratio and quality of evidence of outcomes for the prognostic factors with the bubble diagram.Abbreviation: PCEA, patient-controlled epidural analgesia. |
Discussion
The International Federation of Gynecology and Obstetrics (FIGO) guideline recommended to receive cesarean section to prevent shoulder dystocia or birth injury, when fetal weight would be>4,000 g.30 For pregnant women with cesarean section, in addition to the conventional perinatal management, the integration of perioperative management is required, including blood sugar control, anesthesia, healthcare, etc. This study is the first systematic review of the prognostic factors. The results of the systematic review show that the perioperative blood glucose management regimens, preoperative fasting and water-deprivation regimens, anesthesia regimens, postoperative regimens, postoperative analgesia regimens, postoperative wound care regimens, psychological interventions, and different dosing regimens for antibiotics may affect the health outcomes of diabetic maternal and newborns. However, the quality of evidence was low, and more high-quality clinical research evidence is required.
According to the principle of GRADE method in the evaluation of a prognosis research system,10,11 the quality of evidence for each outcome is low, and the reason of downgrading is mainly bias risk and inaccuracy. The bias risks included in the randomized controlled trials were assessed by the Cochrane Bias Risk Assessment Tool, in which the main source of bias was the nonreported random sequence generation and allocation concealment, which did not blind the researchers, the patients, and the outcome evaluators, and did not report the source of the information and the method of recruiting or joining the patients. The reason for the imprecision is that the sample size is less than the optimal sample size, and the CI of the effect sizes spans the invalid line. For publication bias, as the number of included studies was <10, the publication bias was not evaluated using a funnel plot. In addition, the included studies did not report the conflict of interest, considering the research topics and manufacturers that may be the interests of the relationship, and in addition to psychological intervention and obesity factors, the rest of the comparison groups were assessed by the possibility of publication bias. However, it was not possible to quantify the possibility of publication bias; thus, the publication bias was not considered in this study. In addition, because most of outcomes included only 1 study, a few outcomes included only 2 studies, and I2 values are small, it is not been downgraded due to heterogeneity. We performed meta-analyses by using the random effects model for multiple risk factors and outcomes. The qualities of the evidence for all outcomes were low. As the number of studies increases and the quality of the research improves, new research data may change the results of this system review. Therefore, it needs to more new high-quality research to update the review in the future.
The main advantages of this systematic review are: 1) for the first time on the impact of pregnancy in patients with diabetes maternal–perinatal outcome of the perioperative factors were evaluated; 2) the original research carried out a systematic, comprehensive search, greatly reducing the possibility of missing; 3) the quality of evidence was graded by GRADE method, and the factors affecting the outcome of perioperative period of cesarean section in pregnant women with diabetes mellitus were clearly presented and interpreted. The limitations of the system review: 1) Only the studies published in Chinese and English were searched, the other languages were not be considered; 2) All the studies are from China, the results may not been applied to other countries and regions.
Conclusion
Low-quality evidence shows that perioperative blood glucose management regimens, anesthesia regimens, postoperative fluid regimens, postoperative analgesia regimens, postoperative wound care, and psychological interventions may affect the health outcomes of diabetic maternal and newborns.
Details of ethics approval
No ethics approval was required or sought for this review.
Data sharing statement
This review does not involve any analysis of individual patient data.
Acknowledgment
This review was supported by Beijing Municipal Science and Technology Commission (Project no. D141107005314004).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goldman M, Kitzmiller JL, Abrams B, Cowan RM, Laros RK. Obstetric complications with GDM. Diabetes. 1991;40(Suppl 2):79–82.
2. Gorgal R, Gonçalves E, Barros M, et al. Gestational diabetes mellitus: a risk factor for non-elective cesarean section. J Obstet Gynaecol Res. 2012;38(1):154–159. doi:10.1111/j.1447-0756.2011.01659.x
3. Martin ET, Kaye KS, Knott C, et al. Diabetes and risk of surgical site infection: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2016;37(1):88–99. doi:10.1017/ice.2015.249
4. Leth RA, Uldbjerg N, Nørgaard M, Møller JK, Thomsen RW. Obesity, diabetes, and the risk of infections diagnosed in hospital and post-discharge infections after cesarean section: a prospective cohort study. Acta Obstet Gynecol Scand. 2011;90(5):501–509. doi:10.1111/j.1600-0412.2011.01090.x
5. Hartling L, Dryden DM, Guthrie A, Muise M, Vandermeer B, Donovan L. Benefits and harms of treating gestational diabetes mellitus: a systematic review and meta-analysis for the U.S. Preventive Services Task Force and the National Institutes of Health Office of Medical Applications of Research. Ann Intern Med. 2013;159(2):123–129. doi:10.7326/0003-4819-159-2-201307160-00661
6. Nicholson W, Bolen S, Witkop CT, Neale D, Wilson L, Bass E. Benefits and risks of oral diabetes agents compared with insulin in women with gestational diabetes: a systematic review. Obstet Gynecol. 2009;113(1):193–205. doi:10.1097/AOG.0b013e318190a459
7. Amin M, Suksomboon N, Poolsup N, Malik O. Comparison of glyburide with metformin in treating gestational diabetes mellitus: a systematic review and meta-analysis. Clin Drug Investig. 2015;35(6):343–351. doi:10.1007/s40261-015-0289-3
8. González Blanco C, Chico Ballesteros A, Gich Saladich I, Corcoy Pla R. Glycemic control and pregnancy outcomes in women with type 1 diabetes mellitus using lispro versus regular insulin: a systematic review and meta-analysis. Diabetes Technol Ther. 2011;13(9):907–911. doi:10.1089/dia.2011.0032
9. Lv S, Wang J, Xu Y. Safety of insulin analogs during pregnancy: a meta-analysis. Arch Gynecol Obstet. 2015;292(4):749–756. doi:10.1007/s00404-015-3692-3
10. Zeng YC, Li MJ, Chen Y, et al. The use of glyburide in the management of gestational diabetes mellitus: a meta-analysis. Adv Med Sci. 2014;59(1):95–101. doi:10.1016/j.advms.2014.03.001
11. Viana LV, Gross JL, Azevedo MJ. Dietary intervention in patients with gestational diabetes mellitus: a systematic review and meta-analysis of randomized clinical trials on maternal and newborn outcomes. Diabetes Care. 2014;37(12):3345–3355. doi:10.2337/dc14-1530
12. Thomaz de Lima H, Lopes Rosado E, Ribeiro Neves PA, et al. Systematic review; Nutritional therapy in gestational diabetes mellitus. Nutr Hosp. 2013;28(6):1806–1814. doi:10.3305/nutrhosp.v28in06.6892
13. Datta S, Brown WU
14. Yin X. The clinical effectiveness of different methods of anesthesia for the puerperants with gestational diabetes mellitus. Chin J Mod Drug Appl. 2015;9(17):128–130. Chinese.
15. Zheng W, Huang X. The analysis of hypopiesia led by different options of anesthesia for the patients with gestational diabetes mellitus in cesarean section. Contemp Med Forum. 2015;13(16):221–222. Chinese.
16. Wang X, Jin Z, Xu Q, et al. Effects of fructose on metabolic changes after cesarean section in gestational diabetes mellitus patients. Chin J Pract Gynecol Obstet. 2010;26(12):933–935. Chinese.
17. Yu R. The effect of fructose in fusion on the levels of blood glucose and insulin in gestationai diabetes mellitus patients after cesarean section. Strait Pharm J. 2014;26(12):102–105. Chinese.
18. Chen H. The analysis of effectiveness of microwave therapy for surgical site healing in the puerperae with diabetes. Henan Med Res. 2015;24(11):76–77. Chinese.
19. Huguet A, Hayden JA, Stinson J, et al. Judging the quality of evidence in reviews of prognostic factor research: adapting the GRADE framework. Syst Rev. 2013;2:71. doi:10.1186/2046-4053-2-71
20. Iorio A, Spencer FA, Falavigna M, et al. Use of GRADE for assessment of evidence about prognosis: rating confidence in estimates of event rates in broad categories of patients. BMJ. 2015;350:h870. doi:10.1136/bmj.h870
21. Goldsmith R, Wright C, Bell SF, Rushton A. Cold hyperalgesia as a prognostic factor in whiplash associated disorders: a systematic review. Man Ther. 2012;17(5):402–410. doi:10.1016/j.math.2012.02.014
22. Han M. The applying of psychological interventions for the patients with gestational diabetes mellitus in peri-operative period. Chin J Prim Bled Pharm. 2015;22(5):757–759. Chinese.
23. Li D, Liu Z, Xu P, et al. The effect of music therapy for anxiety and hemodynamics of gestational diabetes mellitus patients with cesarean section. J Hebei Med Univ. 2015;36(12):1464–1466. Chinese.
24. Zhao L, Zhai J, Shen X. The effect of two analgesia options on the blood sugar of gestational diabetes mellitus patients with cesarean section. Shanghai Med J. 2011;34(12):955–956. Chinese.
25. Li N, Zhang H, Jiang S. The effectiveness of peri-operative insulin pump on the patients with gestational diabetes mellitus. Chin J Misdiagn. 2010;10(12):2845–2846. Chinese.
26. Zhang Y, Zhao Y, Zhao E, et al. The effectiveness of small dose of sulfentanyl combining with bupivacaine on cesarean section in the puerperants with gestational diabetes mellitus. China Pharm. 2015;24(1):9–10. Chinese.
27. Feng J, Bao A, Lu Y, et al. Effects of preoperative fasting and liquid-fasting time before caesarean section on blood glucose of puerperae with GDM and neonates. Chin J Mod Nurs. 2017;23(4):509–512. Chinese.
28. Wang T, Miao P, Hu J. Effects of individualized health education on blood glucose after cesarean section in diabetes mellitus with pregnancy. Contemp Med. 2017;23(27):168–170. Chinese.
29. Yang G, Abulaiti Z, Qian Y, et al. Effect comparison of different antibiotic regimens in the prevention infection after cesarean in patients with gestational diabetes mellitus. Xinjiang Med J. 2017;47(4):366–368.
30. Hod M, Kapur A, Sacks DA, et al. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int J Gynaecol Obstet. 2015;131(Suppl 3):S173–S211. doi:10.1016/S0020-7292(15)30033-3
Supplementary materials
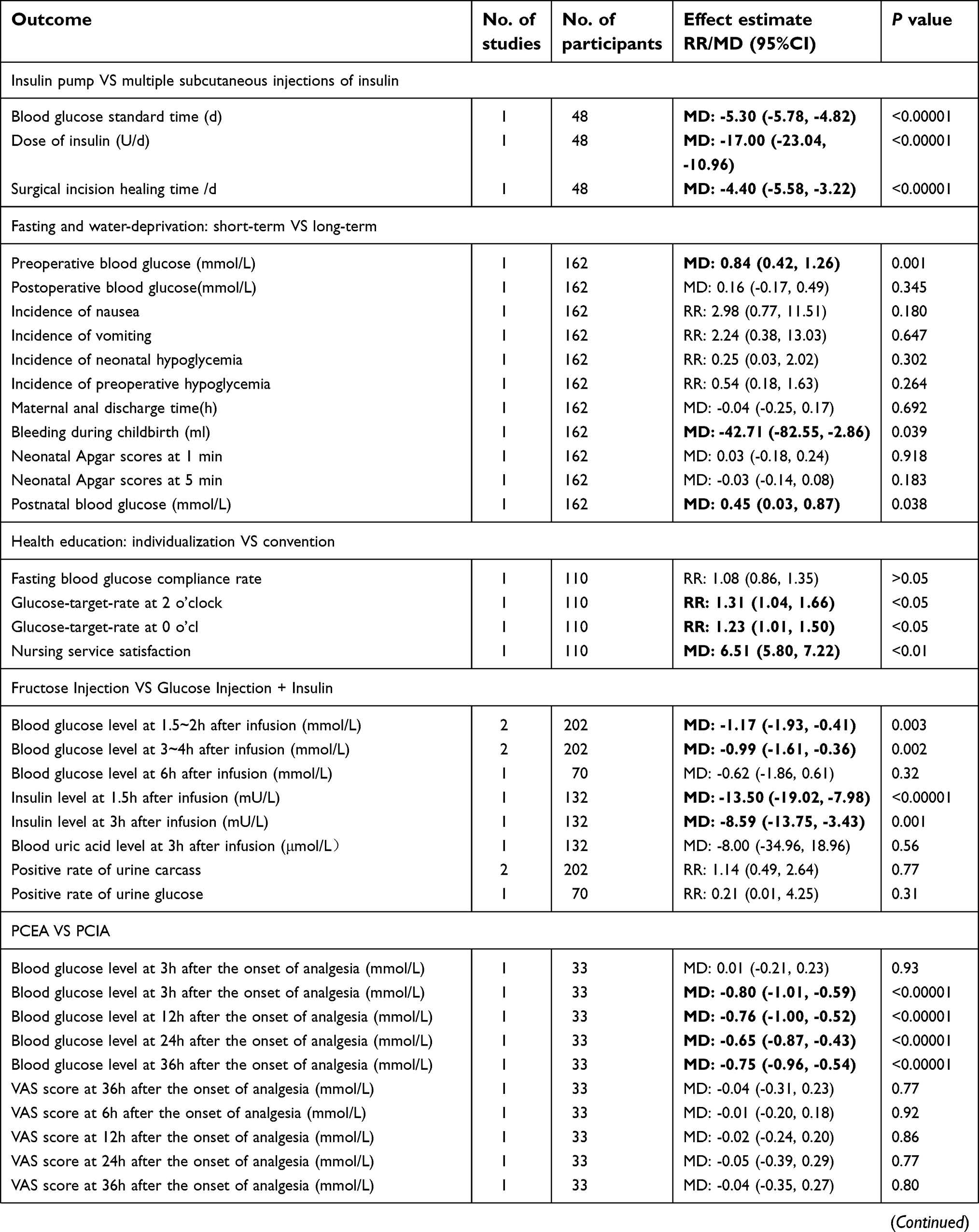 | 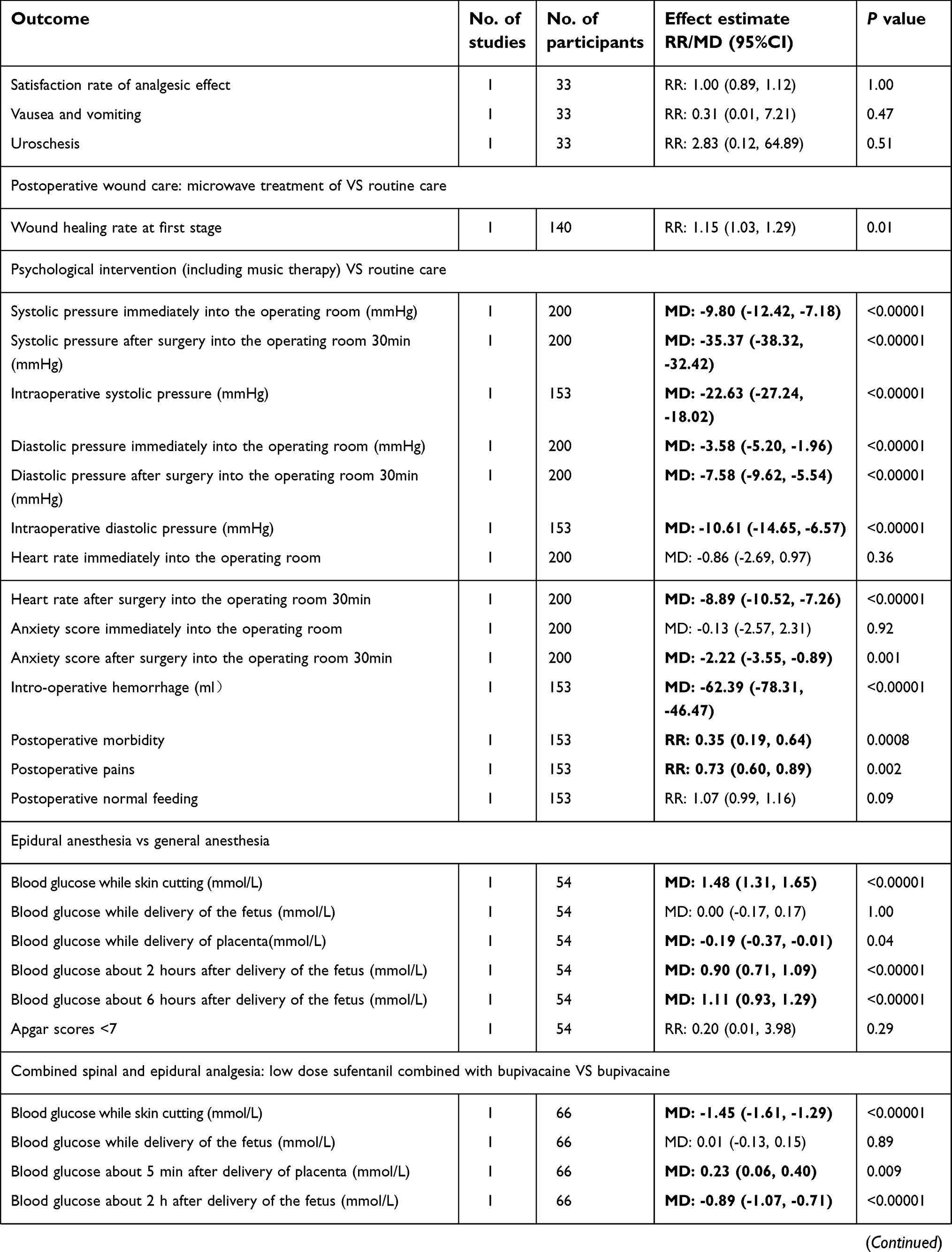 | 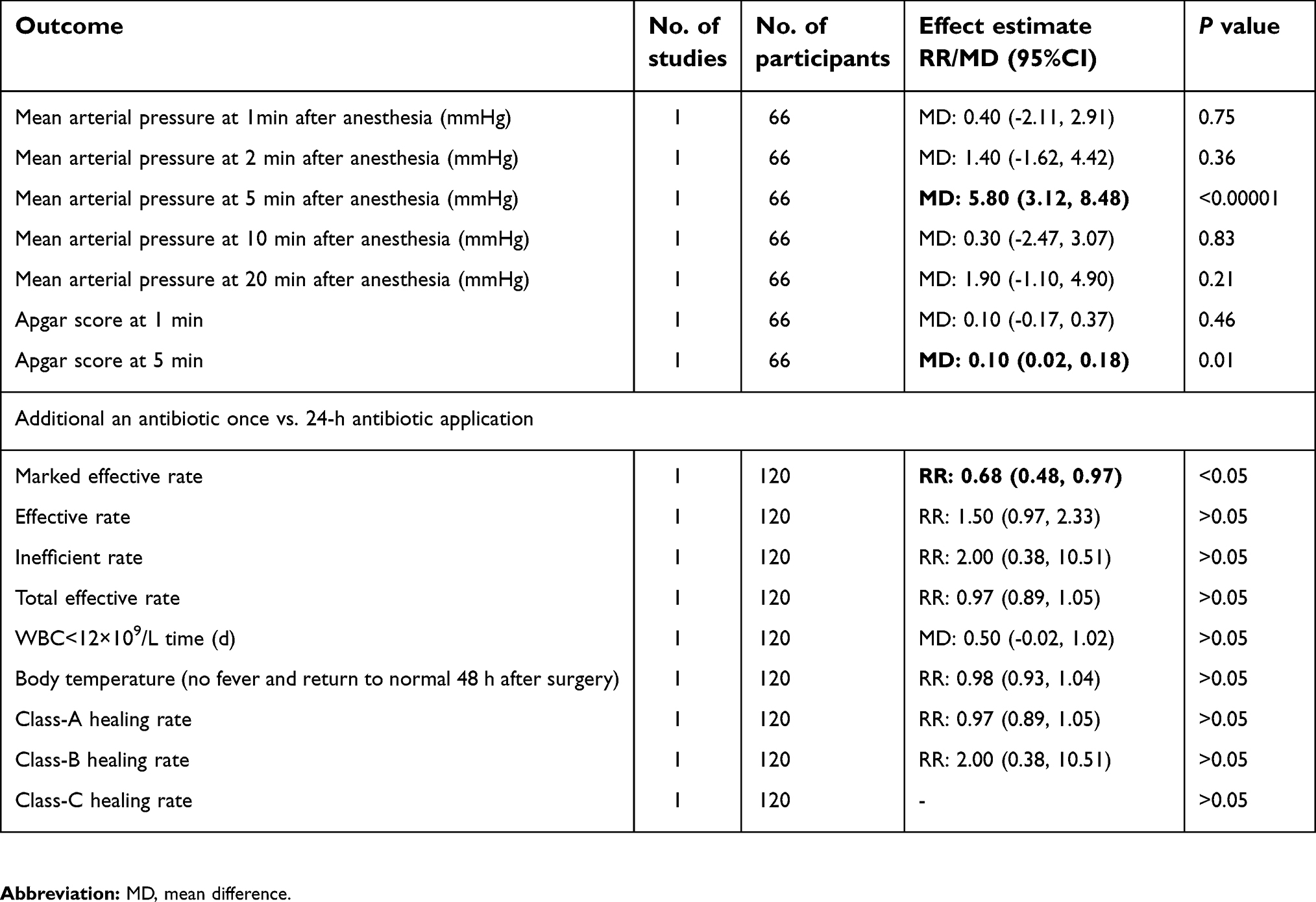 | Appendix 1. Effect evaluation results |
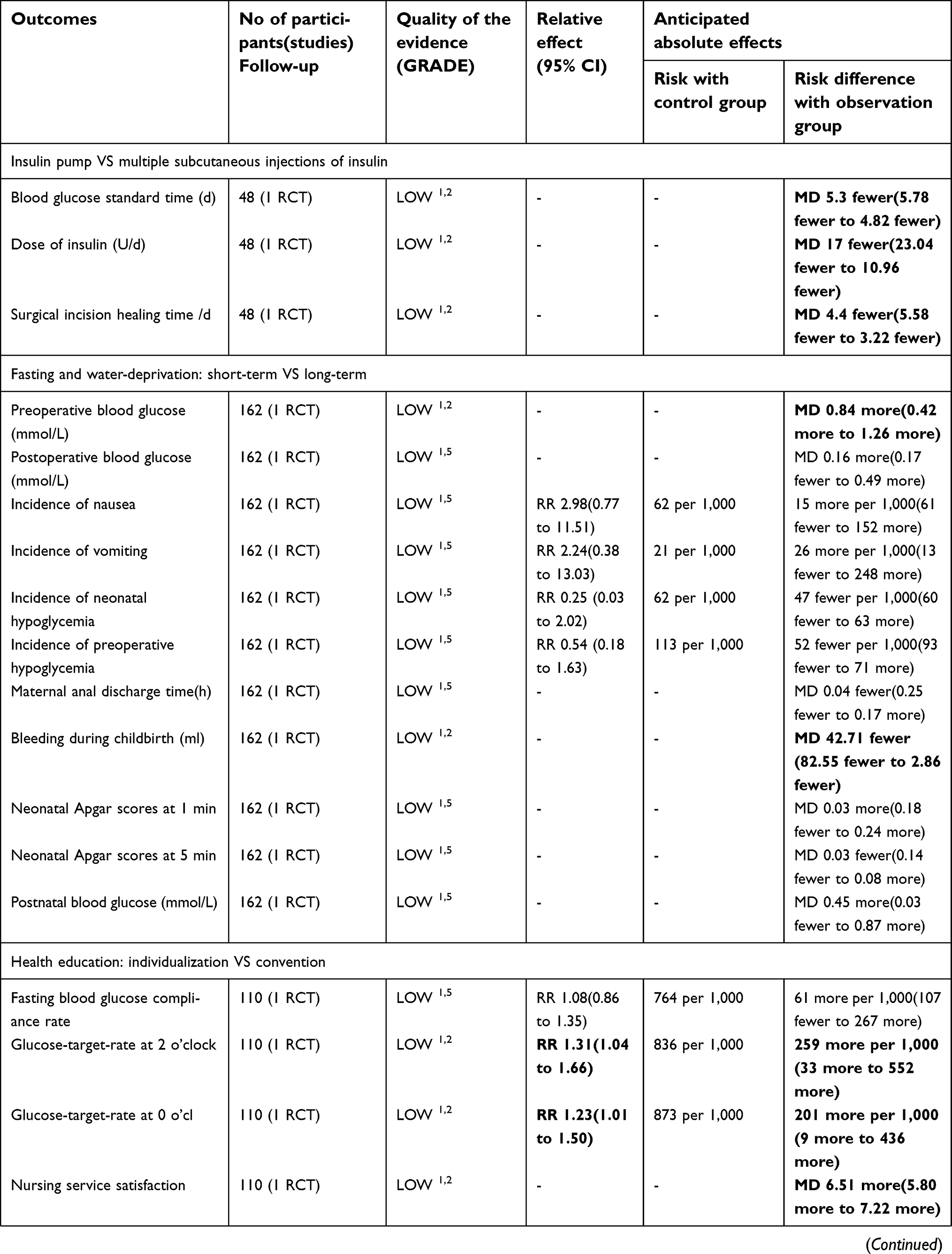 |  |  |  | Appendix 2. Summary of Evidence |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.