")
Back to Journals » Drug Design, Development and Therapy » Volume 15
Progestin-Primed Ovarian Stimulation with Clomiphene Citrate Supplementation May Be More Feasible for Young Women with Diminished Ovarian Reserve Compared with Standard Progestin-Primed Ovarian Stimulation: A Retrospective Study
Authors Lin Y, Chen Q, Zhu J, Teng Y, Huang X, Chen X
Received 26 September 2021
Accepted for publication 7 December 2021
Published 21 December 2021 Volume 2021:15 Pages 5087—5097
DOI https://doi.org/10.2147/DDDT.S338748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Yue Lin,* Qianqian Chen,* Jing Zhu, Yili Teng, Xuefeng Huang, Xia Chen
Reproductive Medicine Center, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Chen; Xuefeng Huang
Reproductive Medicine Center, First Affiliated Hospital of Wenzhou Medical University, 96 Fuxue Road, Wenzhou, Zhejiang, People’s Republic of China
Tel +86-577-88069380
Email [email protected]; [email protected]
Purpose: The present study was designed to compare the efficiency of the progestin-primed ovarian stimulation (PPOS) protocol with clomiphene citrate (CC) supplementation (PPOS+CC) and the standard PPOS protocol for women of different ages with diminished ovarian reserve (DOR).
Patients and Methods: This retrospective cohort study included 364 DOR women who underwent controlled ovarian stimulation with PPOS+CC (n = 223) or standard PPOS (n = 141). They were divided into subgroups based on age: ≤ 35 years and > 35 years. Differences in baseline characteristics, ovarian stimulation characteristics, endocrinological characteristics, and clinical outcome between the two groups were assessed. Statistical analyses were stratified by age.
Results: In all women with DOR, PPOS+CC was associated with a lower percentage of women with profound pituitary suppression than standard PPOS (0.0% vs 18.6%, P < 0.001 and 1.3% vs 11.0%, P = 0.002). In young women with DOR, more high-quality cleavage-stage embryos were harvested (1.96 vs 1.38, P = 0.018) and a lower dosage of gonadotropin per oocyte retrieved was required (558.37 vs 909.82, P = 0.036) in PPOS+CC. In older women with DOR, PPOS+CC led to an increase in the incidence of luteinizing hormone (LH) surge levels above 10 IU/L on trigger day (12.7% vs 4.9%, P = 0.028) and a decrease in the rate of oocyte maturation (84.7% vs 89.9%, P = 0.034) compared to standard PPOS.
Conclusion: Clomiphene citrate is an effective adjuvant to alleviate pituitary suppression in PPOS protocols; for young women with DOR, CC supplementation had a positive impact on the number of high-quality embryos. However, older women with DOR would be at risk of developing a premature LH surge and having poor oocyte maturation rate under the PPOS+CC protocol.
Keywords: diminished ovarian reserve, clomiphene citrate, medroxyprogesterone acetate, controlled ovarian stimulation, in vitro fertilization, luteinizing hormone surge
Plain Language Summary
To evaluate clomiphene citrate (CC) supplementation in the progestin-primed ovarian stimulation (PPOS) protocol for women with diminished ovarian reserve (DOR), our study included 364 women with DOR who underwent controlled ovarian stimulation with the PPOS protocol and CC supplementation (PPOS+CC; n = 223) or standard PPOS (n = 141) from June 2018 to February 2020. Our results suggest that, for young women with DOR, PPOS+CC led to an increase in the number of high-quality embryos and a reduction of gonadotropin dosage compared to standard PPOS. That is, PPOS+CC can be doubly beneficial for young women with DOR. However, older women (>35 years) with DOR would be at risk of developing a premature luteinizing hormone surge and poor oocyte maturation rate after PPOS+CC. CC supplementation in the PPOS protocol may not improve clinical outcomes for older women with DOR; rather it may lead to more risky outcomes.
Introduction
In assisted reproduction technologies (ART), the number of retrieved oocytes largely depends on a woman’s ovarian reserve. Diminished ovarian reserve (DOR), which can be either age dependent or independent, is manifested mainly as increased follicle-stimulating hormone (FSH), decreased anti-Müllerian hormone (AMH) level, and low antral follicle count (AFC).1 A reduced ovarian reserve often leads to some predictable clinical results, such as cycle cancellation, increased gonadotropin (Gn) consumption, or decreased number of oocytes retrieved, and consequent stress and disappointment to the women and their partners. As a decreased oocyte count is the major issue for DOR, it is critical to collect sufficient high-quality oocytes for subsequent embryo transfer in women with DOR. Although many stimulation protocols have been established to improve the number and quality of retrieved oocytes for women with DOR, identification of the most patient friendly protocol remains controversial.2
Progestin-primed ovarian stimulation (PPOS) has been approved for its effect in reducing cycle cancellation and preventing an endogenous luteinizing hormone (LH) surge during controlled ovarian stimulation.3–7 Medroxyprogesterone acetate (MPA) is a simple, convenient, effective, and cheap treatment that can be delivered orally. Previous studies show that PPOS improves the quantity and quality of oocytes and is a more feasible controlled ovarian stimulation protocol for women with DOR or poor ovarian response compared with conventional protocols and mild/minimal stimulation.8–10 However, the continuous supply of progestin during PPOS can lead to profound pituitary suppression.4–6 Profound pituitary suppression is positively correlated with Gn consumption.4–6 Clomiphene citrate (CC) is used to block negative feedback triggered by estrogen, thereby resulting in elevated FSH and LH.11,12 PPOS supplemented with CC (PPOS+CC) significantly reduces the occurrence of profound pituitary suppression in women with normal ovarian reserve or polycystic ovarian syndrome, and the combination treatment is likely to reduce Gn consumption compared with PPOS treatment alone.5,6
Currently, the efficacy of PPOS+CC in women with DOR compared with standard PPOS is unclear. DOR reflects a quantitative rather than qualitative decline of the ovarian reserve, whereas age is considered a reliable marker for oocyte quality.13 Relationship between maternal age and risk of chromosomal abnormalities has been clearly demonstrated by epidemiological studies.14 Physiological decline in the ovarian follicle pool with ageing is often accompanied by decreased ovarian response to Gn stimulation with advancing age.15 It is known that young women with DOR may have a different prognosis from older women.16–18 Therefore, the present study was designed to comprehensively compare the efficiency of PPOS+CC and standard PPOS in young and older women with DOR.
Materials and Methods
Study Design and Participants
We conducted a retrospective cohort study at the Reproductive Medicine Center of the First Affiliated Hospital of Wenzhou Medical University. From June 2018 to February 2020, women who met two or more of the following conditions were diagnosed with DOR: (a) basal FSH level ≥10 IU; (b) FSH/LH ≥2; (c) AFC ≤8; and (d) AMH ≤1.1. Both in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) cycles were included. Women who were diagnosed with uterine cavity abnormalities, untreated hydrosalpinx, and immunologic disease were excluded. Every woman contributed to the study with one stimulation cycle. In women with multiple treatment cycles, the first chronological cycle was chosen. For analysis, couples were grouped as follows: women using PPOS+CC were grouped into the “PPOS+CC group,” while women using standard PPOS were grouped into the “standard PPOS group”. Subpopulations of women were classified based on different age cut-offs, namely ≤35 years and >35 years. All participants provided informed consent after counseling regarding infertility treatments and routine IVF procedures. Using the unique personal identification number, all data were retrospectively collected from computer databases and stored in an anonymous database. This study was approved by the ethics committee of the First Affiliated Hospital of Wenzhou Medical University (no. 2020–02) and performed according to the principles embodied in the Declaration of Helsinki.
Stimulation Protocols and Pituitary Suppression
In PPOS+CC, HMG (Shanghai Livzon Pharmaceutical Company, Zhuhai, China) 150-225 IU; CC (Codal Synto Limited, Limassol, France) 100 mg; and MPA (Shanghai Xinyi Pharmaceutical Co., China) 10 mg daily were administered from menstrual cycle days 2–3 (MC2-3) or after an episode of withdrawal bleeding. In standard PPOS, HMG 150-225 IU and MPA 10 mg daily were initiated from menstrual cycle days 2–3 (MC2-3) or after an episode of withdrawal bleeding. The initial dose of Gn (150-225 IU) was based on patient age, basic FSH, AFC, and body mass index (BMI). Follicle monitoring and hormone assay (FSH, LH, estradiol [E2], and progesterone [P]) were performed 5 days later. The dose of Gn was adjusted according to follicle development, and MPA dose was consistent up to trigger day. When the dominant follicle diameter reached >17 mm and the majority of growing follicles, if any, reached ≥14 mm, recombinant human chorionic gonadotropin (Ovitrelle, Serono, Bari, Italy) was administered to trigger ovulation. Oocytes were retrieved 36–38 h later. All follicles >10 mm in diameter were aspirated.
Fertilization was carried out in vitro after oocyte retrieval depending on the semen parameters and previous fertilization conditions. Embryos were examined for the number or regularity of blastomeres and the degree of fragmentation. One or two high-quality cleavage-stage embryos (7–9 cells and <20% fragmentation) were frozen via vitrification on day 3 after oocyte retrieval, and the remaining embryos were placed in extended culture.19,20 Subsequently, blastocysts with good morphological grades were frozen on days 5 or 6 of culture.
Hormone Measurement
Serum FSH, LH, E2, and P were measured on menstrual cycle days 2–3, days 7–10, and trigger day. Hormone levels were determined by immunofluorescence assays (Roche Diagnostics, Mannheim, Germany). The lower limits of sensitivity were as follow: FSH, 0.06 IU/L; LH, 0.09 IU/L; E2, 10 pg/mL; and P, 0.1 ng/mL. A serum LH concentration <1.0 IU/L on trigger day was set as the cut-off for profound pituitary suppression.21
Endometrium Preparation and Frozen Embryo Transfer
All women in the present study received frozen-thawed embryo transfer (FET). Hormone replacement treatment was used for endometrial preparation. Briefly, the timing of embryo transfer was scheduled on day 3 or day 5 after progestin administration depending on the embryo stage. All embryo transfers were performed under abdominal ultrasound guidance in our center. Each patient received no more than two embryos at one time. Women received luteal support after embryo transfer in the form of intravaginal progestin 200 mg, twice daily. Once pregnancy was achieved, the luteal support was continued until 10 weeks of gestation.
Outcome Measures
We analyzed pregnancy outcomes of the chronological first cycle after oocyte retrieval that transferred at least one high-quality cleavage-stage embryo or good morphology blastocyst (blastocysts better than grade 322).19 Clinical pregnancy was defined as the presence of fetal cardiac activity confirmed by transvaginal ultrasound. Ongoing pregnancy rate was defined as the proportion of women with ongoing pregnancy after a gestational age of 12 weeks. The implantation rate was calculated as the number of gestational sacs visualized on transvaginal ultrasound divided by the number of transferred embryos.
Statistical Analysis
Data were evaluated by Student’s t-test for continuous variables of normal distribution, Mann–Whitney U-test for continuous variables of non-normal distribution, and chi-square test or Fisher’s exact for categorical variables, as appropriate. All tests were two-sided, and P < 0.05 was considered statistically significant. SPSS software (version 25; IBM Corporation, Armonk, NY, USA) was used for data analysis. The dynamic changes in hormones during controlled ovarian stimulation were presented by a broken line graph created using Microsoft Excel.
Results
Patient Characteristics
In total, 364 women were enrolled. Table 1 shows the comparison of basic patient characteristics between ovarian stimulation groups stratified by age. No statistically significant differences were found between the groups with respect to age, duration of infertility, proportion of secondary infertility, BMI, AMH, AFC, and baseline hormones (P > 0.05).
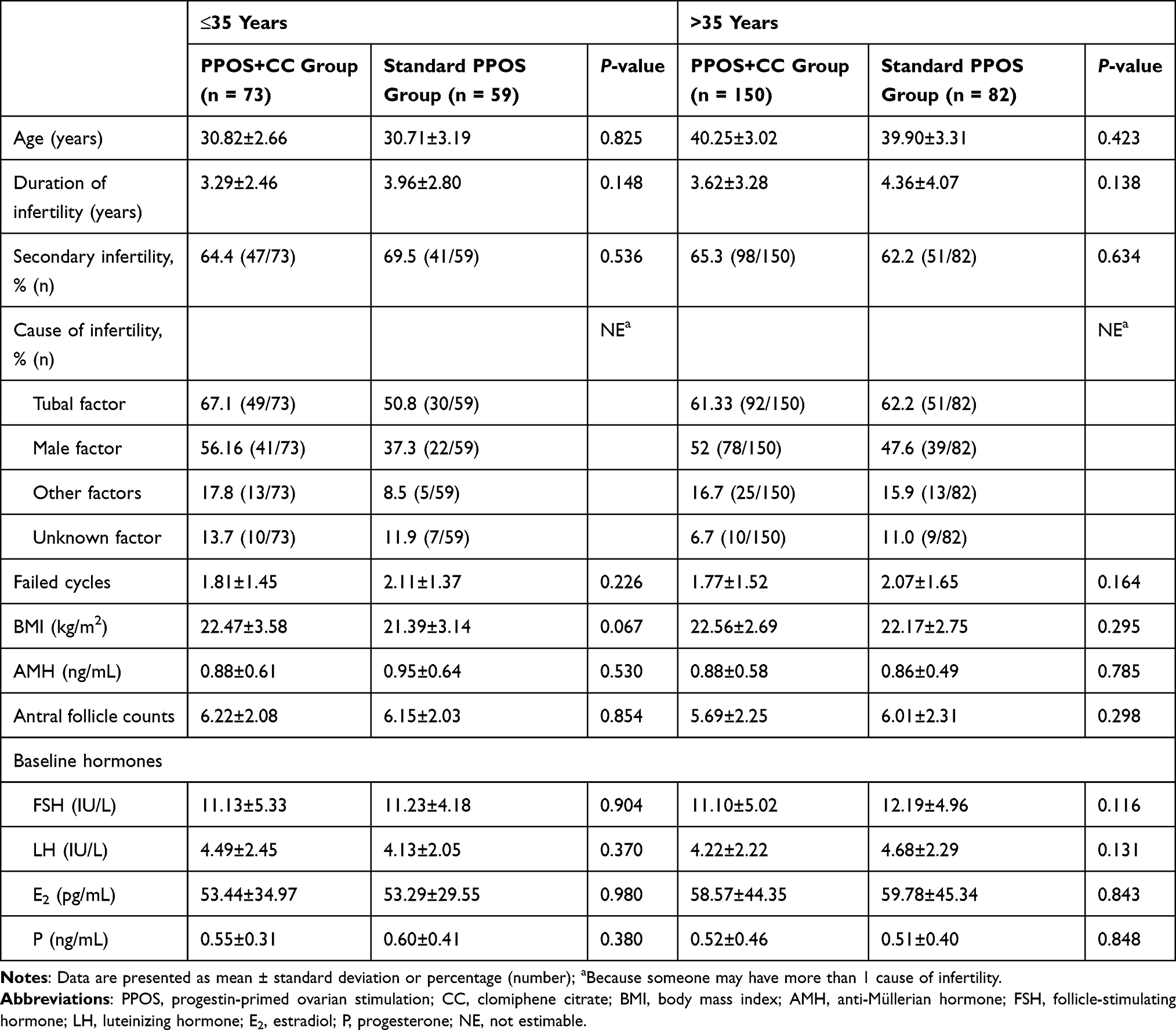 |
Table 1 Basic Patient Characteristics Between Ovarian Stimulation Groups Stratified by Age |
Controlled Ovarian Stimulation and Embryological Outcomes
The controlled ovarian stimulation and embryological outcomes of both groups are presented in Table 2. No statistical differences were found in Gn duration, two pro-nucleate (2PN) rate, number of 2PN cleavage, and cancellation rate prior to oocyte retrieval between the groups (P > 0.05). PPOS+CC had lower doses of Gn per oocyte retrieved than standard PPOS, especially for women ≤35 years (558.37 ± 499.71 vs 909.82 ± 1183.15, P = 0.036). In addition, women aged ≤35 years in the PPOS+CC group showed a significantly higher number of high-quality cleavage-stage embryos compared with those in standard PPOS group (1.96 vs 1.38, P = 0.018). For women >35 years, the mean number of oocytes retrieved in PPOS+CC was significantly higher than those in standard PPOS group (4.23 vs 3.50, P = 0.034). However, the oocyte maturation rate in PPOS+CC was significantly lower than those in standard PPOS (84.7% vs 89.9%, P = 0.034).
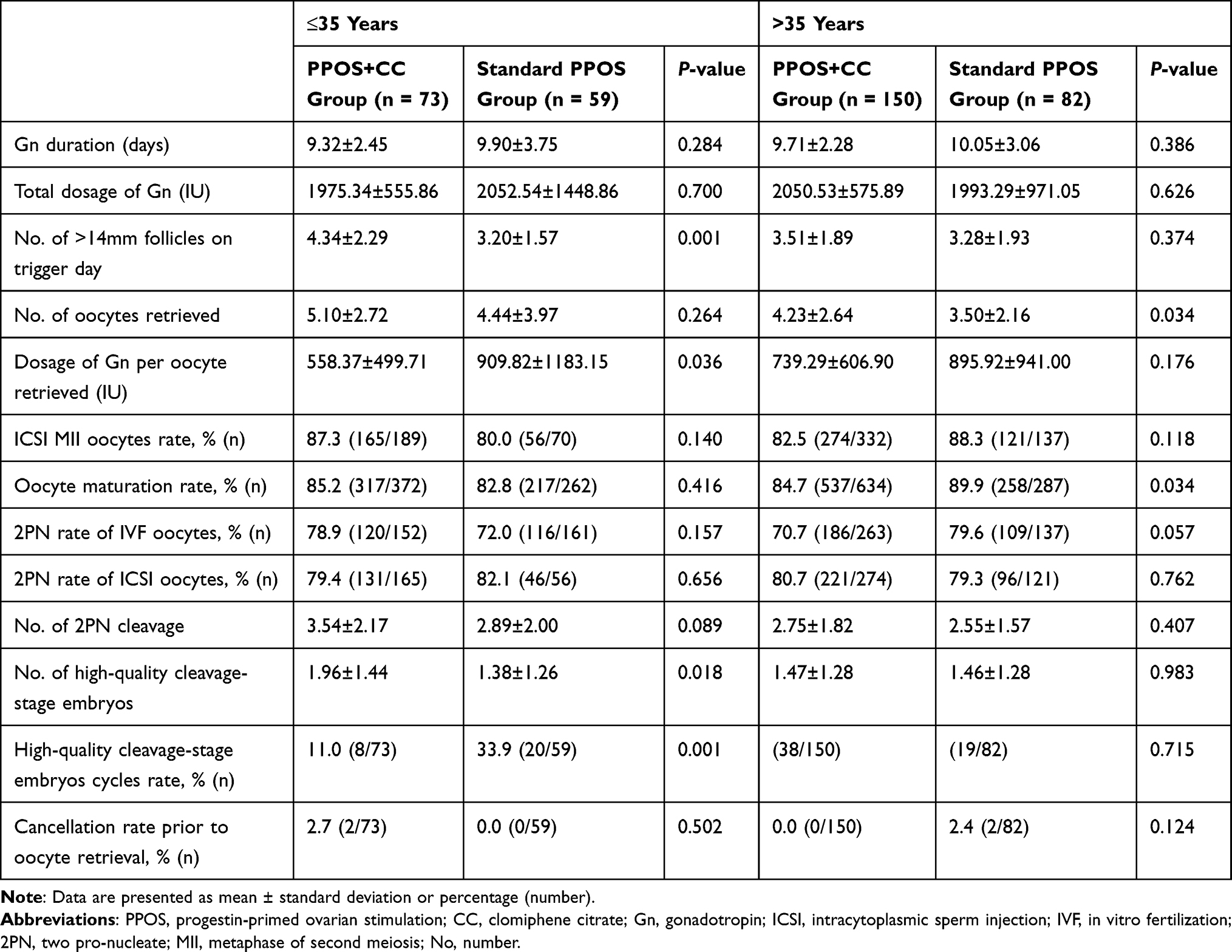 |
Table 2 Controlled Ovarian Stimulation and Embryological Outcomes of Both Groups |
Hormone Profile During Treatment
Serum concentrations of FSH, LH, E2, and P in the two groups stratified by age are presented in Figure 1. In both groups, FSH levels increased after Gn administration, and no difference was found between the groups (P > 0.05). Serum E2 levels and P levels increased gradually in both groups after Gn administration and on trigger day in PPOS+CC they were significantly higher than those in all subgroups of standard PPOS (1974.68 ± 1239.05 pg/mL vs 1143.19 ± 742.72 pg/mL, P < 0.001; 1777.37 ± 1148.10 pg/mL vs 1220.22 ± 796.84 pg/mL, P < 0.001; 1.02 ± 0.50 ng/mL vs 0.83 ± 0.53 ng/mL, P = 0.043; and 0.99 ± 0.87 ng/mL vs 0.69 ± 0.40 ng/mL, P < 0.001, respectively).
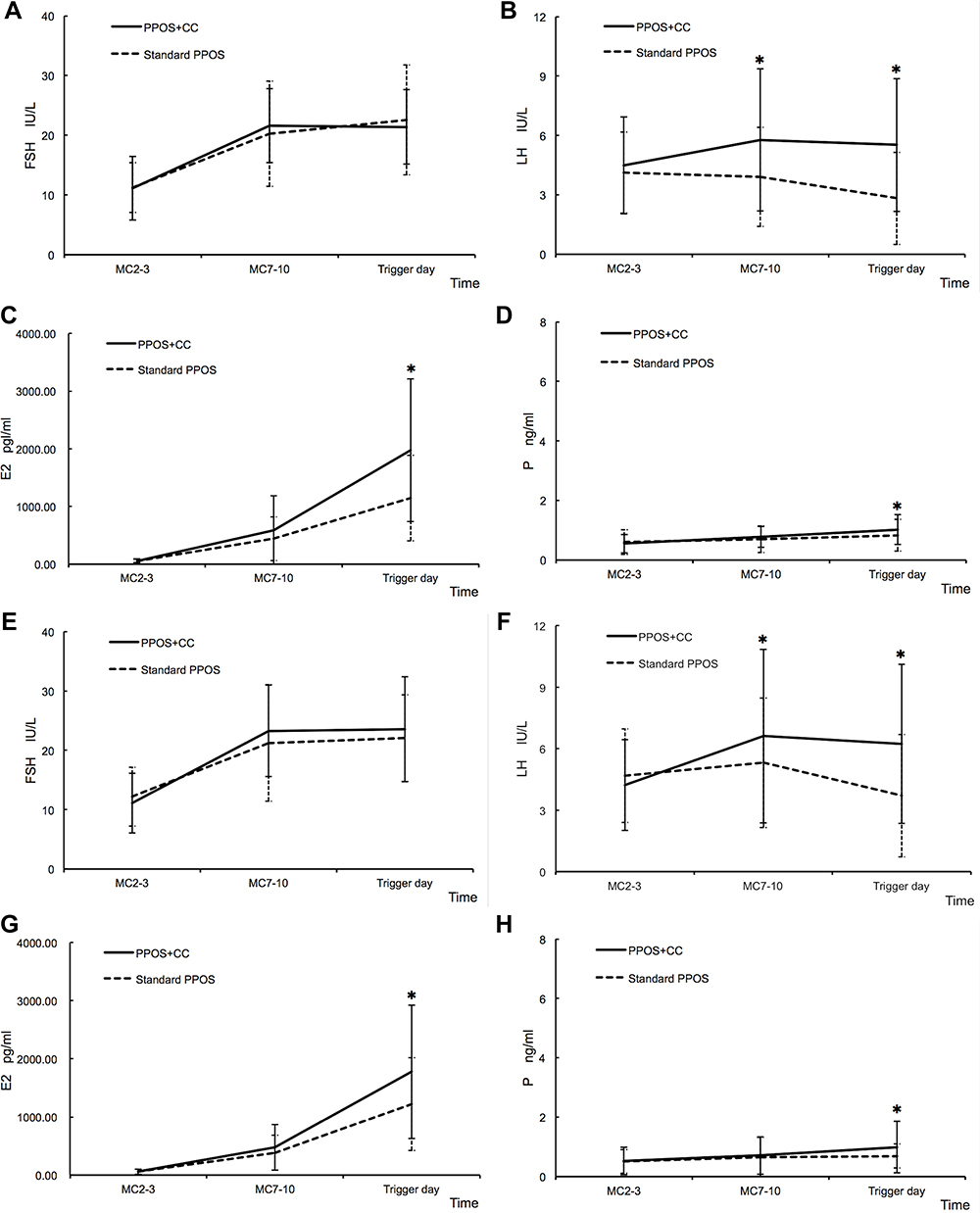 |
Figure 1 The dynamic changes in hormones during ovarian stimulation in the two groups stratified by age. (A–D) Hormone measurement for women aged ≤35 years, (E–H) Hormone measurement for women aged >35 years. The asterisk (*) represents P <0.05 at the time point. Abbreviations: PPOS, progestin-primed ovarian stimulation; CC, clomiphene citrate; MC, menstrual cycle day; FSH, follicle-stimulating hormone; LH, luteinizing hormone; E2, estradiol; P, progesterone. |
LH levels of the two groups showed different trends. LH levels in PPOS+CC initially increased and then remained steady at a range of 5.52–6.61 IU/L; by contrast, the LH levels in standard PPOS remained at a certain level initially and then decreased slightly. There was no significant difference in the value of basal LH between the groups (P > 0.05), whereas LH levels on days 7–10 and on the day of trigger in PPOS+CC were significantly higher than those in all subgroups of standard PPOS (P < 0.05).
The percentage of women with profound pituitary suppression was significantly lower in PPOS+CC than in standard PPOS (0.0% [0/73] vs 18.6% [11/59], P < 0.001 and 1.3% [2/150] vs 11.0% [9/82], P = 0.002). In addition, compared with standard PPOS, the percentage of women with LH levels >10 IU/L on the trigger day was higher in PPOS+CC, especially for women aged >35 years (12.7% [22/150] vs 4.9% [4/82], P = 0.028). For all women with LH levels >10 IU/L on trigger day, the presence of sonolucent follicles was confirmed by transvaginal ultrasound just before the planned oocyte retrieval. Of all these women who underwent oocyte retrieval, two had no oocytes retrieved and one woman had no mature oocytes for retrieval.
Pregnancy Outcomes
A total of 279 women achieved at least one high-quality cleavage-stage embryo or good morphology blastocyst after oocyte retrieval, among which 35 women declined FET for personal reasons before the end of the study, and four women were transferred with embryos collected from two oocyte retrievals in subsequent FET. Thus, only 240 FET cycles were included in the analysis of pregnancy outcomes (Table 3). The rate of blastocyst transfers was similar between the groups and in all subgroups (5.4% [3/56] vs 14.3% [5/35]; 6.5% [6/92] vs 0% [0/57]; P > 0.05). The clinical pregnancy rate, ongoing pregnancy rate, implantation rate, miscarriage rate, ectopic pregnancy rate, and live birth rate were comparable between the two groups across all subgroups (P > 0.05).
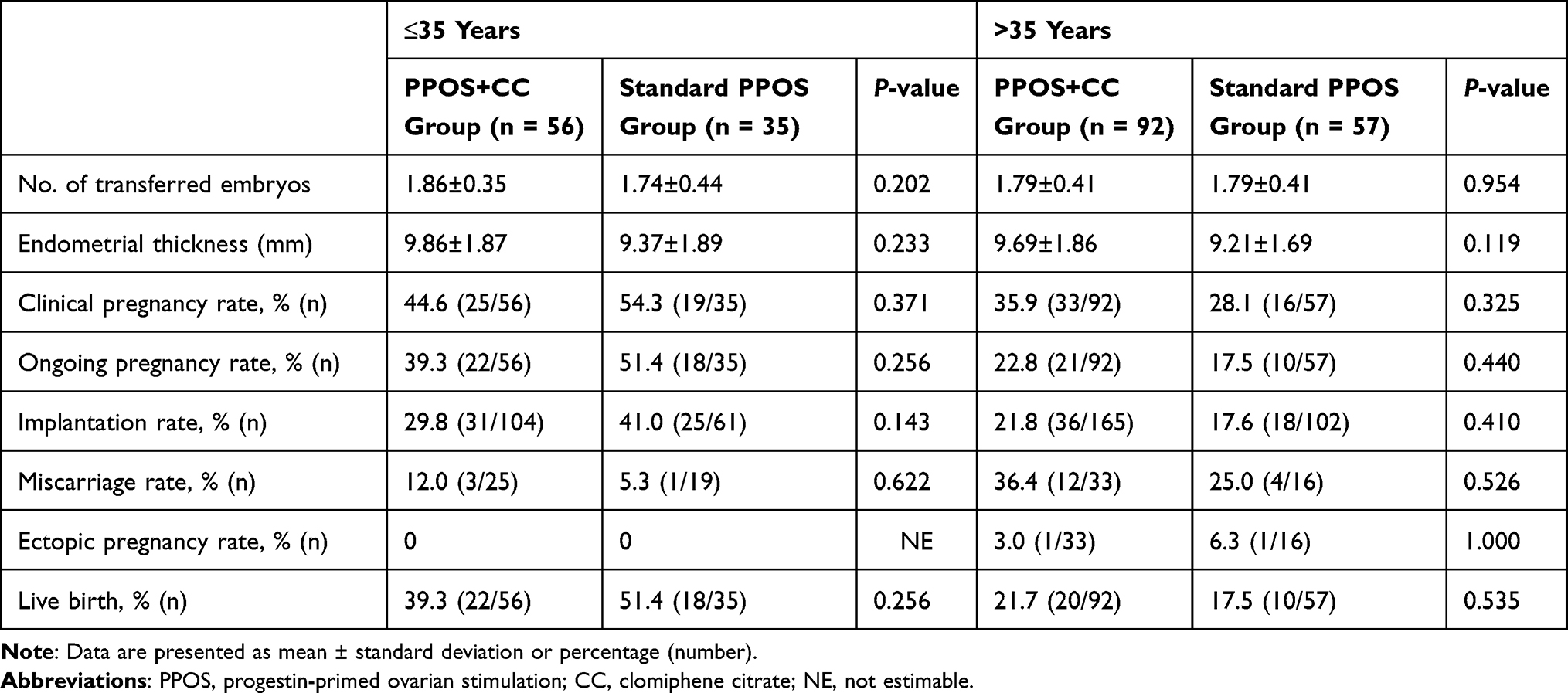 |
Table 3 Pregnancy Outcomes of Both Groups |
All newborns were examined for congenital malformation: one infant from the PPOS+CC group had esophageal atresia, and another infant from standard PPOS had cleft lip and palate.
Furthermore, we assessed the clinical outcomes of women with LH levels above 1 IU/L, but below 10 IU/L on the trigger day (Tables 4 and 5). We found a similar trend of outcomes in these women as in the whole population.
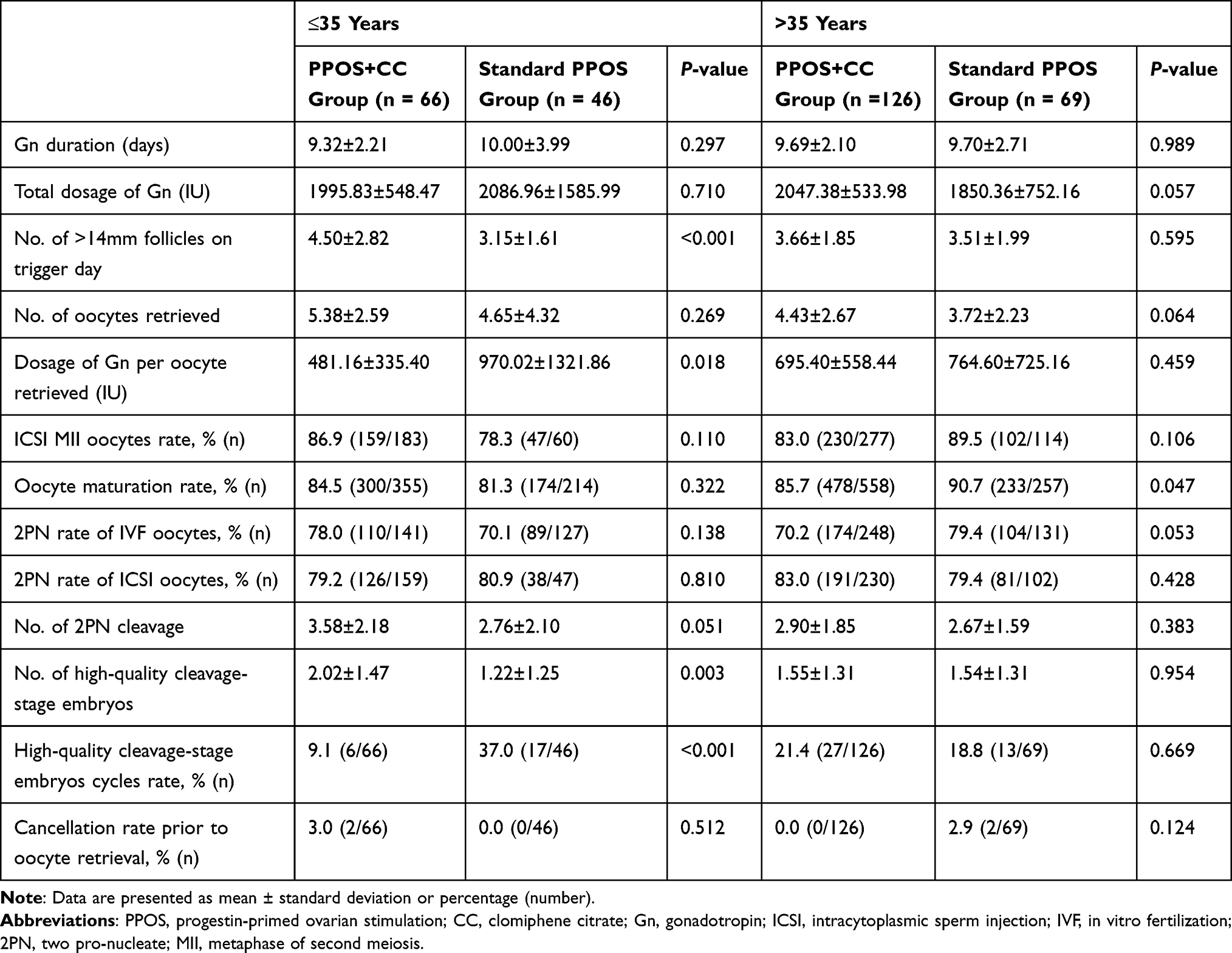 |
Table 4 Controlled Ovarian Stimulation and Embryological Outcomes of Women with LH Levels >1 IU/L, but <10 IU/L on the Trigger Day |
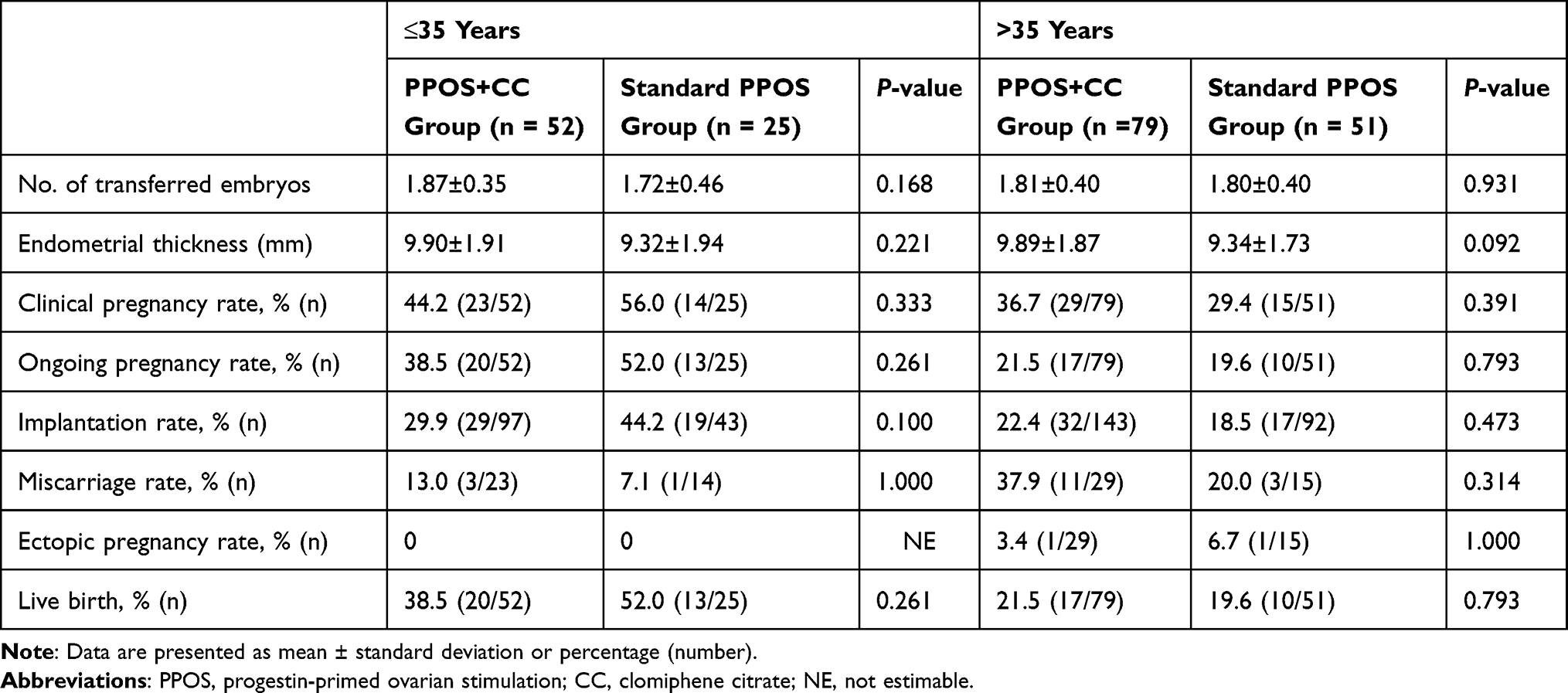 |
Table 5 Pregnancy Outcomes of Women with LH Levels >1 IU/L, but <10 IU/L on the Trigger Day |
Discussion
This retrospective cohort trial showed that the percentage of women with profound pituitary suppression was significantly lower in PPOS+CC than in standard PPOS, in all subgroups. For young women with DOR, PPOS+CC, compared to standard PPOS, led to an increase in the number of high-quality cleavage-stage embryos and a decrease in the dosage of Gn per number of oocytes retrieved. For older women with DOR, the efficiency of the two protocols in embryological outcomes was similar, but a significantly higher incidence of LH levels >10 IU/L on trigger day and significantly lower rate of oocyte maturation were found in PPOS+CC than in standard PPOS.
According to the action of progesterone in the blockade of estradiol-induced gonadotropin discharges, concurrent administration of progestin with estrogen inhibits an estrogen-positive feedback, resulting in suppression of a premature LH surge.22,23 It was shown that the number of retrieved oocytes and high-quality embryos in standard PPOS was significantly higher than that in the group of conventional protocols and mild/minimal stimulation.8–10 However, several previous studies have indicated that the application of progestin from the beginning of ovarian stimulation may lead to profound pituitary suppression, and the extent of pituitary suppression is directly associated with the total dosage of Gn.4–6 This was consistent with our results showing that women in standard PPOS exhibited higher rates of profound pituitary suppression and required a higher dosage of Gn per number of oocytes retrieved than those in PPOS+CC, especially for women ≤35 years. CC interacts with hypothalamic estrogen receptors and increases endogenous FSH and LH secretion by blocking the estrogen-negative feedback mechanism.11,24,25 Our data are consistent with previous findings5,6 and showed that LH levels on days 7–10 and the day of trigger in PPOS+CC were significantly higher than in all subgroups of standard PPOS (P < 0.05). Furthermore, the E2 levels and P levels on trigger day were significantly higher in PPOS+CC than in standard PPOS (P < 0.01). The key role of LH in synthesizing and secreting androgens, which are required for further production of E2 and P is widely acknowledged.26 Our results support previous findings that CC supplementation alleviates profound LH suppression.
According to the concept of a therapeutic window for LH, proposed by Hillier, there is a threshold requirement for LH for an optimal cycle outcome.27 In the present study, the number of high-quality cleavage-stage embryos was higher among younger women treated with PPOS+CC than those treated with standard PPOS. These findings further support the notion that LH plays a critical role in normal follicular development.28 However, for older women with DOR, although the number of >14 mm follicles on trigger day was comparable between the groups (P > 0.05), PPOS+CC led to a decrease in the rate of oocyte maturation compared to standard PPOS. In addition, we found a similar trend of outcomes in women with LH levels >1 IU/L, but <10 IU/L, on trigger day in the entire population. Thus, our study indicated that elevated serum LH during controlled ovarian stimulation might be associated with decreases in the oocyte maturation rate for elderly women with DOR. A possible explanation is that women of different ages with DOR may require a different range of therapeutic window for LH;28 however, the optimal LH level required for folliculogenesis and oocyte maturation for women of different ages remains unknown. Nevertheless, pregnancy outcomes were comparable between the groups in all subgroups, demonstrating a similar developmental potential of embryos despite different LH levels. On the basis of these results, we suggest that early stage embryo development may differ slightly between oocytes retrieved after PPOS+CC compared with standard PPOS. Additional fundamental research should be performed to determine alterations in the follicular microenvironment, which may help determine the optimal range of LH levels, elucidate the mechanisms by which LH affects oocyte quality, and provide evidence for the use of PPOS.
In the present study, the incidence of LH levels >10 IU/L on trigger day was higher in PPOS+CC, especially for women aged >35 y (P < 0.05). Guo et al reported that a higher percentage of premature LH surge (10.2%) is found in women aged >35 y after PPOS protocols using utrogestan were applied.29 Three previous independent studies have found a similar correlation between diminished ovarian reserve and premature LH elevation.30–32 These results suggest that, although CC supplementation alleviates profound LH suppression, older women with DOR would be at risk of developing a premature LH surge and poor oocyte maturation. The reason for this remarkable variability needs to be clarified. It is speculated that dysregulation of ovarian factors could be an underlying mechanism in women of advanced maternal age. According to animal and human studies, the transition towards menopause involves not only the loss of ovarian follicles but also a dysregulation of E2 feedback mechanisms.33
With a relatively large sample size, the current study was able to verify the feasibility of CC co-administration in the PPOS protocol in women of different ages with DOR. These results from using a CC combination regimen may provide new insights to develop an individualized treatment regimen for women with DOR to improve clinical outcomes.
Our study also has some limitations. Firstly, data were derived from a post-hoc analysis. Secondly, the LH assays currently used do not always accurately reflect LH bioactivity.34
Conclusion
This retrospective cohort trial showed that CC supplementation could mitigate the profound LH suppression caused by progestin administration. For young women with DOR, the PPOS protocol with CC supplementation led to an increase in the number of high-quality cleavage-stage embryos and a decrease in the dosage of Gn per oocyte retrieved as compared to the standard PPOS protocol. However, older women with DOR would be at risk of developing a premature LH surge and experience poor oocyte maturation rate after the PPOS+CC protocol.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81901551).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Coccia ME, Rizzello F. Ovarian reserve. Ann N Y Acad Sci. 2008;1127:27–30. PMID: 18443326. doi:10.1196/annals.1434.011
2. La Marca A, Sunkara SK. Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: from theory to practice. Hum Reprod Update. 2014;20(1):124–140. PMID: 24077980. doi:10.1093/humupd/dmt037
3. Kuang Y, Chen Q, Fu Y, et al. Medroxyprogesterone acetate is an effective oral alternative for preventing premature luteinizing hormone surges in women undergoing controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril. 2015;104:62–70. PMID: 25956370. doi:10.1016/j.fertnstert.2015.03.022
4. Zhu X, Ye H, Fu Y. Use of utrogestan during controlled ovarian hyperstimulation in normally ovulating women undergoing in vitro fertilization or intracytoplasmic sperm injection treatments in combination with a “freeze all” strategy: a randomized controlled dose-finding study of 100 mg versus 200 mg. Fertil Steril. 2017;107(2):379–386. PMID: 27865446. doi:10.1016/j.fertnstert.2016.10.030
5. Liu Y, Chen Q, Yu S, et al. Progestin-primed ovarian stimulation with or without clomiphene citrate supplementation in normal ovulatory women undergoing in vitro fertilization/intracytoplasmic sperm injection: a prospective randomized controlled trial. Clin Endocrinol. 2018;88(3):442–452. PMID: 29247457. doi:10.1111/cen.13532
6. Ye H, Tian H, He W, et al. Progestin-primed milder stimulation with clomiphene citrate yields fewer oocytes and suboptimal pregnancy outcomes compared with the standard progestin-primed ovarian stimulation in infertile women with polycystic ovarian syndrome. Reprod Biol Endocrinol. 2018;16(1):53. PMID: 29807533. doi:10.1186/s12958-018-0373-7
7. Cai R, Zheng B, Lin Q, et al. A meta-analysis of the efficacy of progestin-primed ovarian stimulation with medroxyprogesterone acetate in ovulation induction in poor ovarian responders. J Gynecol Obstet Hum Reprod. 2020;50(7):102049. PMID: 33387677. doi:10.1016/j.jogoh.2020.102049
8. Yu CM, Dai XL, Wang YF, et al. Progestin-primed ovarian stimulation improves the outcomes of IVF/ICSI cycles in infertile women with diminished ovarian reserve. J Chin Med Assoc. 2019;82(11):845–848. PMID: 31453864. doi:10.1097/JCMA.0000000000000177
9. Huang P, Tang M, Qin A. Progestin-primed ovarian stimulation is a feasible method for poor ovarian responders undergoing in IVF/ICSI compared to a GnRH antagonist protocol: a retrospective study. J Gynecol Obstet Hum Reprod. 2019;48(2):99–102. PMID: 30321608. doi:10.1016/j.jogoh.2018.10.008
10. Mu Z, Sa Y, Sun Z, Yi Y. Ovulation induction with high progesterone levels may be more suitable for elderly patients with low ovarian response. J Gynecol Obstet Hum Reprod. 2021;50(2):101661. PMID: 31809957. doi:10.1016/j.jogoh.2019.101661
11. Adashi EY. Clomiphene citrate: mechanism(s) and site(s) of action-A hypothesis revisited. Fertil Steril. 1984;42:331–344. PMID: 6432584. doi:10.1016/s0015-0282(16)48069-6
12. Tavaniotou A, Albano C, Smitz J, Devroey P. Effect of clomiphene citrate on follicular and luteal phase luteinizing hormone concentrations in in vitro fertilization cycles stimulated with gonadotropins and gonadotropin-releasing hormone antagonist. Fertil Steril. 2002;77:733–737. PMID: 11937125. doi:10.1016/s0015-0282(01)03265-4
13. Nagaoka SI, Hassold TJ, Hunt PA. Human aneuploidy: mechanisms and new insights into an age-old problem. Nat Rev Genet. 2012;13(7):493–504. PMID: 22705668. doi:10.1038/nrg3245
14. Perheentupa A, Huhtaniemi I. Aging of the human ovary and testis. Mol Cell Endocrinol. 2009;299(1):2–13. PMID: 19059459. doi:10.1016/j.mce.2008.11.004
15. Ferraretti AP, La Marca A, Fauser BC, Tarlatzis B, Nargund G, Gianaroli L; ESHRE working group on Poor Ovarian Response Definition. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011;26:1616–1624. PMID: 21505041. doi:10.1093/humrep/der092
16. Gleicher N, Barad D. “Ovarian age-based” stimulation of young women with diminished ovarian reserve results in excellent pregnancy rates with in vitro fertilization. Fertil Steril. 2006;86(6):1621–1625. PMID: 17074322. doi:10.1016/j.fertnstert.2006.04.046
17. Morin SJ, Patounakis G, Juneau CR, Neal SA, Scott RT, Seli E. Diminished ovarian reserve and poor response to stimulation in patients <38 years old: a quantitative but not qualitative reduction in performance. Hum Reprod. 2018;33(8):1489–1498. PMID: 30010882. doi:10.1093/humrep/dey238
18. Hu S, Xu B, Jin L. Perinatal outcome in young patients with diminished ovarian reserve undergoing assisted reproductive technology. Fertil Steril. 2020;114(1):118–124 e1. PMID: 32622406. doi:10.1016/j.fertnstert.2020.02.112
19. de Los Santos MJ, Arroyo G, Busquet A, et al. A multicenter prospective study to assess the effect of early cleavage on embryo quality, implantation, and live-birth rate. Fertil Steril. 2014;101(4):981–987. PMID: 24502893. doi:10.1016/j.fertnstert.2013.12.043
20. Qin N, Chen Q, Hong Q, et al. Flexibility in starting ovarian stimulation at different phases of the menstrual cycle for treatment of infertile women with the use of in vitro fertilization or intracytoplasmic sperm injection. Fertil Steril. 2016;106(2):334–341. PMID: 27114329. doi:10.1016/j.fertnstert.2016.04.006
21. Dong J, Wang Y, Chai WR, et al. The pregnancy outcome of progestin-primed ovarian stimulation using 4 versus 10 mg of medroxyprogesterone acetate per day in infertile women undergoing in vitro fertilisation: a randomised controlled trial. BJOG. 2017;124(7):1048–1055. PMID: 28276192. doi:10.1111/1471-0528.14622
22. Dierschke DJ, Yamaji T, Karsch FJ, Weick RF, Weiss G, Knobil E. Blockade by progesterone of estrogen-induced LH and FSH release in the rhesus monkey. Endocrinol. 1973;92(5):1496–1501. PMID: 4633016. doi:10.1210/endo-92-5-1496
23. Wildt L, Hutchison JS, Marshall G, Pohl CR, Knobil E. On the site of action of progesterone in the blockade of the estradiol-induced gonadotropin discharge in the rhesus monkey. Endocrinol. 1981;109(4):1293–1294. PMID: 6793348. doi:10.1210/endo-109-4-1293
24. Kerin JF, Liu JH, Phillipou G, Yen SS. Evidence for a hypothalamic site of action of clomiphene citrate in women. J Clin Endocrinol Metab. 1985;61(2):265–268. PMID: 3924949. doi:10.1210/jcem-61-2-265
25. Emons G, Ortmann O, Thiessen S, Knuppen R. Effects of estradiol and some antiestrogens (clomiphene, tamoxifen, and hydroxytamoxifen) on luteinizing hormone secretion by rat pituitary cells in culture. Arch Gynecol. 1986;237(4):199–211. PMID: 3516082. doi:10.1007/BF02133782
26. Hillier SG. Gonadotropic control of ovarian follicular growth and development. Mol Cell Endocrinol. 2001;179:39–46. PMID: 11420129. doi:10.1016/s0303-7207(01)00469-5
27. Hillier SG. Current concepts of the roles of follicle stimulating hormone and luteinizing hormone in folliculogenesis. Hum Reprod. 1994;9(2):188–191. PMID: 8027271. doi:10.1093/oxfordjournals.humrep.a138480
28. Weghofer A, Schnepf S, Barad D, Gleicher N. The impact of luteinizing hormone in assisted reproduction: a review. Curr Opin Obstet Gynecol. 2007;19(3):253–257. PMID: 17495642. doi:10.1097/GCO.0b013e3280bad843
29. Guo YC, Chen PY, Li TT, et al. Different progestin-primed ovarian stimulation protocols in infertile women undergoing in vitro fertilization/intracytoplasmic sperm injection: an analysis of 1188 cycles. Arch Gynecol Obstet. 2019;299(4):1201–1212. PMID: 30852654. doi:10.1007/s00404-019-05065-4
30. Kummer NE, Weitzman VN, Benadiva CA, Schmidt DW, Engmann LL, Nulsen JC. In vitro fertilization outcomes in patients experiencing a premature rise in luteinizing hormone during a gonadotropin-releasing hormone antagonist cycle. Fertil Steril. 2011;95(8):2592–2594. PMID: 21292260. doi:10.1016/j.fertnstert.2010.12.046
31. Reichman DE, Zakarin L, Chao K, Meyer L, Davis OK, Rosenwaks Z. Diminished ovarian reserve is the predominant risk factor for gonadotropin-releasing hormone antagonist failure resulting in breakthrough luteinizing hormone surges in in vitro fertilization cycles. Fertil Steril. 2014;102(1):99–102. PMID: 24882557. doi:10.1016/j.fertnstert.2014.04.010
32. Kochhar PK, Ghosh P. Diminished ovarian reserve predisposes to premature luteinizing hormone surges in gonadotropin-releasing hormone antagonist cycles in in vitro fertilization. J Hum Reprod Sci. 2020;13(3):191–195. PMID: 33311904. doi:10.4103/jhrs.JHRS_133_19
33. Neal-Perry G, Nejat E, Dicken C. The neuroendocrine physiology of female reproductive aging: an update. Maturitas. 2010;67(1):34–38. PMID: 20570066. doi:10.1016/j.maturitas.2010.04.016
34. Jaakkola T, Ding YQ, Kellokumpu-Lehtinen P, et al. The ratios of serum bioactive/immunoreactive luteinizing hormone and follicle-stimulating hormone in various clinical conditions with increased and decreased gonadotropin secretion: reevaluation by a highly sensitive immunometric assay. J Clin Endocrinol Metab. 1990;70(6):1496–1505. PMID: 2140831. doi:10.1210/jcem-70-6-1496
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.