")
Back to Journals » Infection and Drug Resistance » Volume 12
Profile of sofosbuvir/velpatasvir/voxilaprevir in the treatment of hepatitis C
Authors Childs-Kean LM, Brumwell NA , Lodl EF
Received 10 May 2019
Accepted for publication 23 June 2019
Published 23 July 2019 Volume 2019:12 Pages 2259—2268
DOI https://doi.org/10.2147/IDR.S171338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Lindsey M Childs-Kean, Natalie A Brumwell, Emma F Lodl
Department of Pharmacotherapy and Translational Research, University of Florida College of Pharmacy, Gainesville, FL, USA
Abstract: The treatment of chronic hepatitis C has been revolutionized with the introduction of direct-acting antivirals (DAAs). However, some patients are not cured with first-line treatment. Sofosbuvir/velpatasvir/voxilaprevir is a fixed-dose combination of a polymerase inhibitor, an NS5A inhibitor, and a protease inhibitor with activity against strains of the hepatitis C virus that show resistance to other first-line antiviral regimens. Sofosbuvir/velpatasvir/voxilaprevir has been studied in four Phase III randomized trials: POLARIS-1, −2, −3, and −4, which enrolled both treatment naïve and experienced patients with and without compensated cirrhosis. In these trials, at least 95% of patients treated with sofosbuvir/velpatasvir/voxilaprevir achieved sustained virological response (SVR). This includes favorable treatment outcomes in patients who had previously failed a regimen containing sofosbuvir or an NS5A inhibitor. Patient-reported outcomes also improved during and after treatment with sofosbuvir/velpatasvir/voxilaprevir. Treatment with sofosbuvir/velpatasvir/voxilaprevir is well tolerated, with the most commonly reported adverse events being headache, fatigue, diarrhea, and nausea. The approval of sofosbuvir/velpatasvir/voxilaprevir allows a treatment option for patients who have failed treatment with certain DAA regimens.
Keywords: hepatitis C, direct-acting antivirals, protease inhibitors, resistance
Introduction
Viral hepatitis remains a public health threat in parts of the world, with 71 million people estimated to have chronic hepatitis C virus (HCV) infection in 2015.1 Yearly, an estimated 1.75 million people are newly diagnosed with HCV worldwide.1 In the United States, HCV is the most common blood-borne infection, and about 3.5 million people (range of 2.5–4.7 million) are currently infected.2,3 Left untreated, complications of HCV include cirrhosis, hepatocellular carcinoma (HCC), and eventually death.1 HCV is classified into 7 genotypes with 67 different subtypes.4 Genotype 1 is most common in the United States (75%), followed by Genotypes 2 and 3 (20–25%), and the smallest group includes genotypes 4 through 7.5
The goal of HCV treatment is to reduce mortality and liver complications through virologic cure.6 The surrogate marker for virologic cure is sustained virological response (SVR), which is an undetectable viral load (serum HCV RNA <15 IU/mL) at least 12 weeks after completing treatment.6 Since the development of the direct-acting antivirals (DAAs) and the movement away from ribavirin and interferon-based treatment, SVR rates have increased to above 90%, and there has been a reduction in side effects and treatment duration.7 The DAAs target various proteins throughout the HCV replication cycle and include the NS3/4A protease inhibitors, NS5A inhibitors, nucleoside and nucleotide NS5B polymerase inhibitors, and the non-nucleoside NS5B polymerase inhibitors.8 Although there has been increased success of HCV treatment with DAAs, there is still a concern for virological failure due to baseline resistance-associated substitutions (RASs).6 DAA-resistant viruses can also be selected for during treatment.
On July 18, 2017, Vosevi® (sofosbuvir/velpatasvir/voxilaprevir [SOF/VEL/VOX]) was approved by the Food and Drug Administration (FDA) for the treatment of chronic HCV genotypes 1–6 in patients without cirrhosis or with compensated cirrhosis.5 SOF/VEL/VOX was the first treatment approved for patients who had been previously treated with an NS5A inhibitor.5 The specific indications for SOF/VEL/VOX include: (1) genotypes 1 through 6 infection with prior treatment of an NS5A inhibitor or (2) genotype 1a or 3 infection with prior treatment of sofosbuvir without an NS5A inhibitor.9 Soon after, Vosevi® was authorized for use in Europe by the European Medicines Agency on July 26, 2017.10 SOF/VEL/VOX is available as a fixed-dose combination tablet containing 400 mg sofosbuvir, 100 mg velpatasvir, and 100 mg voxilaprevir.9 The recommended administration for all patients is to take one tablet once daily with food for a duration of 12 weeks.9 The objective of this review is to examine the efficacy and safety of SOF/VEL/VOX, and then to propose considerations for clinical patient use.
Materials and methods
PubMed and Google Scholar were searched (August 2016–March 2019) using the following terms: “voxilaprevir,” “Vosevi,” “voxilaprevir resistance,” and “voxilaprevir patient reported outcomes.” All results in English were reviewed. Data from Phase III trials and post-marketing studies are included in this review. Other resources included the Food and Drug Administration Adverse Event Reporting System and the drug’s prescribing information.
Efficacy
The efficacy and safety of SOF/VEL/VOX was evaluated in four Phase III trials: POLARIS-1, −2, −3, and −4.11,12 A summary of the POLARIS trials can be found in Table 1. The primary efficacy endpoint for all four trials was achievement of SVR.11,12 Exclusion criteria that was applied to all POLARIS studies included failure of previous DAA therapy due to ADRs or non-adherence, HBV or HIV co-infection, HCC, hepatic decompensation, renal impairment (defined as creatinine clearance <50 mL/min), thrombocytopenia, or anemia.11,12 The mean age of patients in all four trials was 56 years, and the majority of patients in all studies were male.11,12
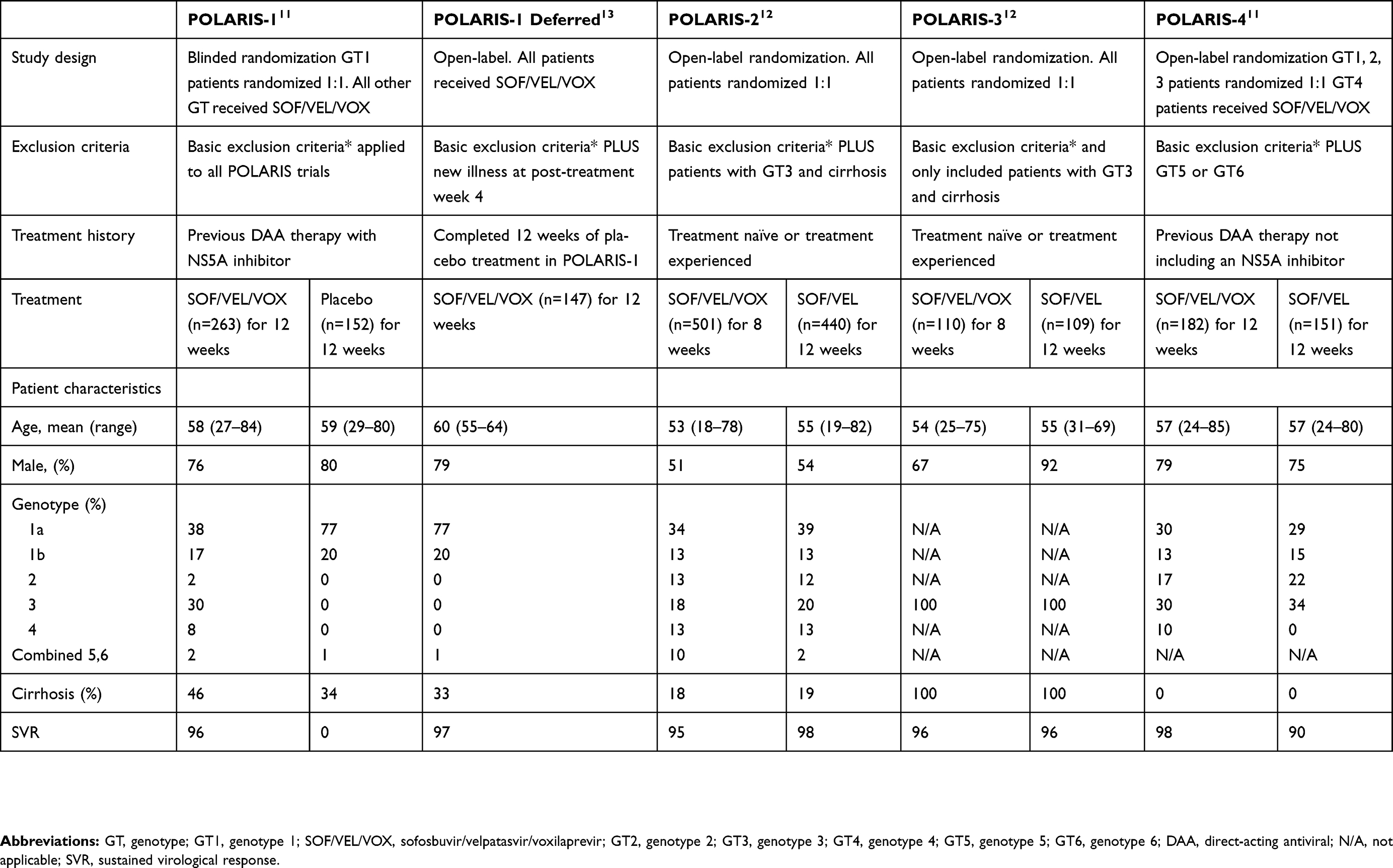 |
Table 1 Summary of POLARIS Phase III clinical trials |
POLARIS-1 was a randomized, double-blind study that included adult HCV patients with genotypes 1, 2, 3, 4, 5, or 6 with or without compensated cirrhosis who had received previous treatment with an NS5A inhibitor-containing regimen.11 Patients with genotype 1 were randomized to 12 weeks of SOF/VEL/VOX once daily or placebo.11 Patients with all other genotypes were assigned to receive SOF/VEL/VOX.11 Most patients had genotypes 1a, 1b, or 3, and almost half of the patients had compensated cirrhosis at baseline.11 SVR for patients who received treatment was 96% compared with 0% in the placebo group.11 The 96% SVR rate was significantly above the prespecified performance goal of 85% (p<0.001).
Patients who completed 12 weeks of placebo treatment in POLARIS-1 had the option to enroll in an open-label substudy after the completion of POLARIS-1, where they received 12 weeks of SOF/VEL/VOX treatment.13 Patients were excluded from this study if they had any of the exclusion criteria for enrollment in the POLARIS trials, did not complete 12 weeks of placebo treatment, or had new clinically significant illness at post-treatment week 4.13 Patient characteristics were similar to that of the POLARIS-1 study except that there was a more narrow age range.13 Of the 152 patients who completed treatment with placebo in the POLARIS-1 trial, 147 completed the 12-week treatment with SOF/VEL/VOX.13 Of these patients, 143 (97%; 95% CI 93–99) achieved SVR.13
POLARIS-2 was a randomized, open-label study that included adult HCV patients with genotypes 1, 2, 3, 4, 5, or 6 with or without compensated cirrhosis and no prior exposure to a DAA regimen, excluding patients with genotype 3 and cirrhosis.12 Patients were randomized to receive SOF/VEL/VOX for 8 weeks or sofosbuvir/velpatasvir (SOF/VEL) for 12 weeks.12 Genotype 1a was the most prevalent genotype in this study, and 18% of patients had compensated cirrhosis.12 The overall SVR rate for patients of any genotype with cirrhosis in the SOF/VEL/VOX group was 91% compared with 99% in the SOF/VEL group, for a difference of −3.2% (95% CI −6.2 to −0.4).12 Because the lower threshold of the 95% CI was less than the pre-established limit of −5%, 8 weeks of SOF/VEL/VOX was concluded to be inferior to 12 weeks of SOF/VEL in this patient population.12
POLARIS-3 was a randomized, open-label study that enrolled patients with genotype 3 with compensated cirrhosis and no prior DAA exposure.12 Similar to POLARIS-2, patients were randomized to 8 weeks of SOF/VEL/VOX or 12 weeks of SOF/VEL.12 SVR for both treatment groups was 96%.12 This was significantly above the prespecified performance goal of 83% (p<0.001 for both groups).12
POLARIS-4 was a randomized, open-label study that enrolled adult HCV patients with genotypes 1, 2, 3, or 4 with or without compensated cirrhosis and prior non-NS5A inhibitor DAA therapy.11 Genotypes 1a and 3 were most common, each present in about 30% of patients.11 There were no patients in this study with compensated cirrhosis.11 Patients were randomized to 12 weeks of SOF/VEL/VOX or SOF/VEL. SVR was 98% for the SOF/VEL/VOX group and 90% for the SOF/VEL group.11 The SVR for SOF/VEL/VOX was significantly above the prespecified performance goal of 85% (p<0.001).11
Across all POLARIS studies, only thirty-four patients experienced virological relapse with SOF/VEL/VOX treatment (six in POLARIS-1, four in POLARIS-1 Deferred, 21 in POLARIS-2, two in POLARIS-3, and one in POLARIS-4).11–13 Additionally, only one patient experienced virologic breakthrough while assigned to the SOF/VEL/VOX treatment arm; this was likely due to medication nonadherence based on evaluation of plasma drug concentration, although the details of this evaluation were not included in the publications. No patients experienced nonresponse to SOF/VEL/VOX.11–13 Patient characteristics associated with virological relapse from POLARIS-1 and POLARIS-4 were genotype 3a (4/7), compensated cirrhosis (7/7), and NS3/NS5A RASs at baseline (5/7).11–14
Several recent studies have focused on patient-reported outcome (PRO) data as another measurement of efficacy for HCV treatment regimens.15,16 PROs are a useful metric for determining the impact of an intervention on a patient’s quality of life and can measure the efficacy of the intervention in terms of functionality (eg, days absent from work). Available PRO studies included a series of post-hoc analyses from the POLARIS trials and a cohort study from France.15–17 All PRO studies utilized 26 domains from four validated PRO measurement tools: the Short-Form-36 (SF-36), the chronic liver disease questionnaire-HCV Version (CLDQ-HCV), the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), and the work productivity activity index: specific health problem (WPAI-SHP).15–17 These tools have also been used in other studies assessing efficacy of DAA regimens for the treatment of HCV in adults.18–20 All four tools were self-administered to study participants at baseline, at the end of treatment, and at varying post-treatment intervals (post-treatment weeks 4 and 12 in the POLARIS post-hoc studies and post-treatment weeks 4,12, and 24 in the French cohort study).15–17
In the POLARIS post-hoc studies, patient data were stratified by treatment regimen and presence or absence of compensated cirrhosis. Cirrhotic patients had an overall lower baseline PRO score compared to non-cirrhotic patients (p< 0.05) regardless of treatment with SOF/VEL or SOF/VEL/VOX. Both cirrhotic and non-cirrhotic patients demonstrated improvements in 25 of 26 PRO domains during and following treatment with SOF/VEL/VOX for 8 or 12 weeks or SOF/VEL for 12 weeks (range of improvement +2.7 to +16.7 points on a universal PRO scale ranging from 0 to 100).15,16 The improvement of these scores was similar or greater in cirrhotic patients compared to non-cirrhotic patients (range of improvement +4.5 to +18.7 points for cirrhotic patients).15,16 The only domain that did not improve for both cirrhotic and non-cirrhotic patients in both analyses was the Absenteeism component of the WPAI-SHP.15,16 There was no difference in improvement in PROs between patients who received SOF/VEL/VOX and those who received SOF/VEL (p> 0.05 for all measures).15,16
The other major PRO study was conducted in a French cohort with matched American controls treated with the same regimens. French subjects had similar clinicodemographic characteristics to American subjects but had lower baseline PRO scores in nearly every category, which did not affect the outcomes of the study.17 Since the objective of the study was to determine differences in PROs between interferon (IFN)- and ribavirin (RBV)-based treatment regimens, the data were stratified into the broad categories of IFN + RBV-containing, IFN-free RBV-containing, IFN-free RBV-free, and placebo. Patients in the IFN-free RBV-free group, which included patients on ledipasvir/sofosbuvir (n=107), SOF/VEL (n=285), or SOF/VEL/VOX (n=202), demonstrated improvements in PROs from baseline that were sustained throughout treatment and post-treatment.17 Since there was no stratification by individual treatment regimen, the true effects of SOF/VEL/VOX on PROs could not be determined from this study.17
Ruane et al evaluated the efficacy of SOF/VEL/VOX in the setting of retreatment for patients who had previously failed a DAA regimen, including patients who failed on a previous regimen of SOF/VEL/VOX.21 This open-label study included patients with or without compensated cirrhosis who were previously enrolled in a POLARIS trial and had failed to achieve SVR after receiving 12 weeks of SOF/VEL (11/31) or 8 weeks of SOF/VEL/VOX (17/31), or were enrolled in another manufacturer-sponsored study and had received a DAA-based treatment regimen (3/31).21 This study applied the same exclusion criteria as the POLARIS trials.11,12,21 The primary efficacy endpoint was the proportion of patients who achieved SVR.21 Half of the enrollees had genotype 1a infection, and half had compensated cirrhosis present at baseline.21 The other genotypes present in this study were genotype 3 (26%), genotype 1b (13%), and all other genotypes (<10%).21 Over half (55%) of the study population had previously failed 8 weeks of SOF/VEL/VOX, and 35% had failed 12 weeks of SOF/VEL.21 All patients enrolled in the study achieved SVR.21 RASs were screened at the start of the trial revealing that 32% of the study population had baseline NS5A RASs and 26% had baseline NS3 RASs (no patient had both NS5A and NS3 RASs).21
Resistance
Because SOF/VEL/VOX contains three DAAs, the activity of the drug could theoretically be diminished if the virus has resistance to any of the three drug classes: NS5B (SOF), NS5A (VEL), or NS3/4A (VOX). In cell culture, HCV replicons with reduced voxilaprevir susceptibility were selected and NS3/4A PI-resistance-associated positions at 41, 156, and 168 were identified.9 A >100-fold reduction in voxilaprevir susceptibility was shown at NS3 sites A156L/T in genotype 1a, A156T/V in genotype 1b, A156L/V in genotype 2a, A156T/V in genotype 3a, and A156L/T/V in genotype 4.9 Having a combination of substitutions, compared to a single substitution, led to higher reductions in voxilaprevir susceptibility.9 However, other studies show that voxilaprevir has improved coverage against NS3 RASs compared to other NS3/4A protease inhibitors.22–24
Data from the POLARIS-1 and −4 trials were analyzed to determine the impact of baseline NS3 and NS5A RASs on SVR rates in patients who were treated with 12 weeks of SOF/VEL/VOX.14 RAS testing was conducted at baseline and at the time of virologic failure for patients who did not achieve SVR.14 Patients who did not complete treatment for reasons other than virologic failure were not included.14 The rates of NS5A and NS3 RASs in POLARIS-4 treatment-experienced patients who had not received an NS5A inhibitor were equivalent (40/169 and 39/169, respectively).14 Of the total 417 patients who were treatment-experienced, 39% (164/417) had NS5A RASs, 12% (48/417) had NS3 RASs, and 18% (76/417) had both NS3 and NS5A RASs.14 NS5A RASs were also the most common type of RAS in patients with genotypes 2, 3, 4, 5, and 6.14
Among the 248 patients in POLARIS-1 who were NS5A inhibitor treatment-experienced, 52% (129/248) exhibited NS5A RASs that conferred 2.5 to 100-fold reduced susceptibility to VEL and 26.6% (66/248) patients had NS5A RASs that conferred >100-fold resistance to VEL.14 The most common VEL-specific NS5A RAS was Y93H. Less common RASs included A30K and L31M, usually in combination with each other or with Y93H. NS3 RASs were more common in patients with genotype 1 (45/217) which was mainly driven by the high prevalence of the Q80K RAS in patients with genotype 1a infection. Of the patients with NS3 RASs, 1.4% (6/417) of patients had VOX-specific NS3 RASs which were not specified in this study.14 Despite the high prevalence of baseline NS3 and NS5A RASs, there was no significant difference in SVR between treatment-experienced patients with baseline RASs and those who did not have these substitutions at baseline (97.9% and 98.5%, respectively).14 Similarly, 97% (32/33) of patients with baseline NS5B RASs achieved SVR. In the POLARIS-1 Deferred Treatment substudy, 131 patients had baseline NS3 or NS5A RASs, and 10 patients had baseline NS5B RASs.13 The four patients who experienced virological relapse all had genotype 1a and baseline RASs: all patients had at least one NS5A RAS, and three had at least one NS3 RAS.13
Treatment-emergent RAS development was rare across all studies. Only one patient in POLARIS-1 and one patient in POLARIS-2 who experienced virologic failure on SOF/VEL/VOX developed an additional RAS during treatment, both associated with NS5A.11 In POLARIS-1, a genotype 4 patient with the L30R RAS at baseline developed the additional Y93H RAS; in POLARIS-2, a genotype 1a patient with the Q30Q/H RAS at baseline developed the additional L31M RAS.11,12 No patients experiencing treatment failure on SOF/VEL/VOX in POLARIS-3 or POLARIS-4 developed additional RASs during treatment.11,12 In the POLARIS-1 Deferred Treatment substudy, two of the four patients who had virological relapse developed RASs during treatment: one patient developed Y56H and D168A/V NS3 RASs as well as a L31L/M NS5A RAS; another patient developed a V36V/A NS3 RAS.13
Therefore, regardless of duration of treatment with SOF/VEL/VOX (8 weeks vs 12 weeks), there has been no significant difference in SVR shown between patients with baseline RASs and those without the presence of baseline RASs in the POLARIS trials. The only exception to this was demonstrated in POLARIS-2, where patients treated with 8 weeks of SOF/VEL/VOX who had genotype 1a and Q80K NS5A RAS at baseline achieved lower SVR compared to patients who did not have the Q80K RAS at baseline (88% vs 94%, respectively).12
Wyles et al analyzed the emergence and long-term persistence of NS3 and NS5A RASs in patients who received treatment with a DAA regimen in a manufacturer-sponsored study and failed to achieve SVR.25 Patients were included in this study if they were enrolled in a follow-up sequence registry and were exposed to an NS5A or NS3 inhibitor.25 Patients were discontinued if they were initiated on HCV treatment or if RASs were no longer detectable.25 The study population was divided into non-sofosbuvir-based, sofosbuvir-based, and SOF/VEL/VOX treatment groups.25 The SOF/VEL/VOX group contained only 10 patients.25 Only one patient had NS5A RASs detectable at baseline which persisted through week 48 of follow-up, indicating that RASs in SOF/VEL/VOX-treated patients appear to be rare.25 There were no treatment-emergent NS3 RASs in the SOF/VEL/VOX group, and there were no data available for these patients after week 12 of follow-up.25
Safety
Adverse events
Overall, treatment with SOF/VEL/VOX is well tolerated.9,11–13 The most common adverse reactions observed in the POLARIS trials included headache, fatigue, diarrhea, and nausea (see Table 2).9,11–13 In the POLARIS-1 trial, one patient discontinued treatment of SOF/VEL/VOX due to an adverse event of angioedema after starting ramipril.11 No patients discontinued SOF/VEL/VOX treatment in the other POLARIS trials.11,12
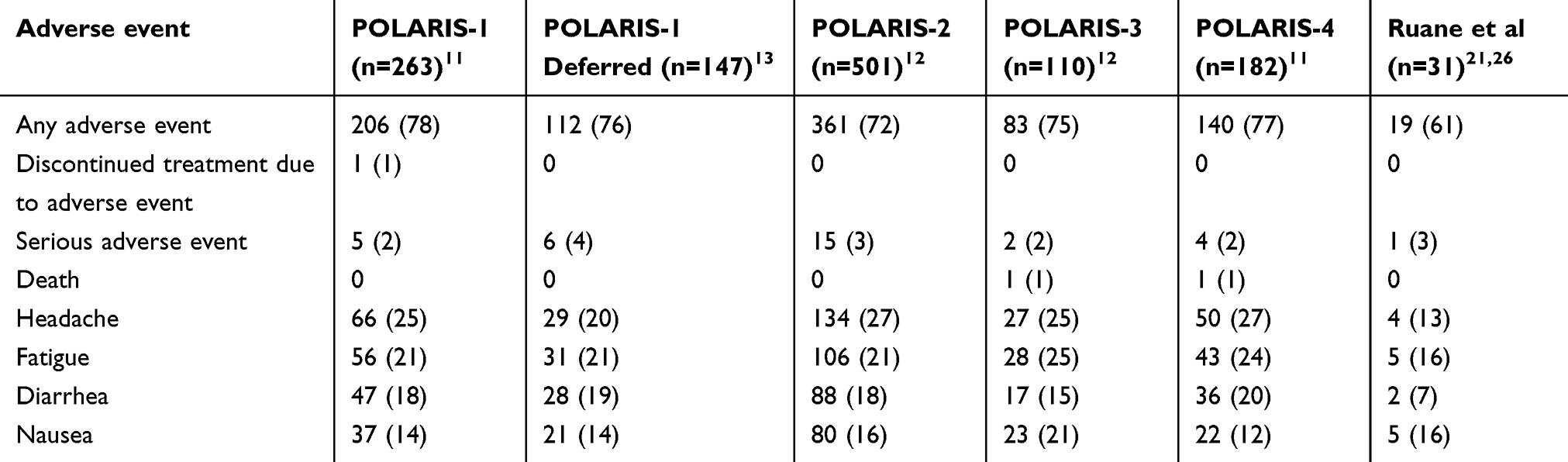 |
Table 2 Overview of adverse events |
Results from the Ruane et al study show that none of the 31 patients who received 12 week SOF/VEL/VOX retreatment discontinued treatment due to adverse events (Table 2).21,26 One 63-year-old male patient with a history of cirrhosis and Dieulafoy lesion was hospitalized with a Grade 3 serious adverse event of gastrointestinal hemorrhage on day 12 of treatment.21,26 Treatment was interrupted only on days 13 and 17. The patient also had the Grade 3 serious adverse events of acute respiratory failure, asthenia, and cellulitis.21,26 Overall, 61% of patients experienced adverse events while on treatment.21,26 The common (>10% of patients) adverse events were fatigue, nausea, and headache, similar to what was seen in the POLARIS trials.11–13,21,26
A search of the FDA Adverse Event Reporting System (FAERS) using the search term “voxilaprevir” resulted in a total of five reports between 2016 and 2018.27 All five reports were categorized as serious reaction types, but none resulted in death.27 The 2016 report involved a 50-year-old female taking SOF/VEL/VOX and ribavirin.27 Alanine aminotransferase and aspartate aminotransferase were reported as increased.27 In 2017, there was one report for an unreported age/gender patient who was taking SOF/VEL/VOX and ribavirin with a reaction of lymphocyte count, hemoglobin, and platelet count decreased, and blood glucose and alanine aminotransferase increased.27 Three reports were sent between November and December of 2018, all involving a 65-year-old male from the same country.27 These cases may involve the same patient, with different drug companies sending in separate reports.27 The drugs included sofosbuvir, boceprevir, daclatasvir, ledipasvir, voxilaprevir, peginterferon alfa-2b, ribavirin, and daclatasvir dihydrochloride, and the reactions reported were HCC, asthenia, upper abdominal pain, nausea, and drug ineffective.27 Therefore, no additional significant safety signals have been reported to FAERS since the drug’s approval.
Drug–drug interactions
There are several important drug interactions to consider when a patient is going to start treatment with SOF/VEL/VOX. All three HCV drugs are substrates of p-glycoprotein (P-gp) and breast cancer resistant protein (BCRP).9 Voxilaprevir is also a substrate of OATP1B1, OATP1B3, CYP3A4, CYP1A2, and CYP2C8.9 Therefore, concomitant administration with P-gp inducers and/or moderate to potent CYP inducers (eg, carbamazepine, phenytoin, St. John’s Wort) will decrease the therapeutic effect of SOF/VEL/VOX and is not recommended.9 The concomitant administration of rifampin and cyclosporine is not recommended due to the increased concentration of voxilaprevir.9 An important warning to note is the risk for serious symptomatic bradycardia when patients take amiodarone with SOF/VEL/VOX.9 Due to a potential decrease in absorption of VEL, antacid and VEL administration times should be separated by 4 hrs.9 H2-receptor antagonists, at a dose not exceeding famotidine 40 mg twice daily, and omeprazole 20 mg can be given simultaneously with SOF/VEL/VOX.9 However, higher doses of omeprazole and other proton-pump inhibitors have not been studied.9
There are many antiretroviral drugs that interact with SOF/VEL/VOX. Atazanavir, fosamprenavir, indinavir, lopinavir, and saquinavir should not be coadministered due to an increase in voxilaprevir plasma concentrations.28 There are a lack of coadministration studies with various HIV drugs, and efavirenz, etravirine, nevirapine, and tipranavir are not recommended at this time due to potential decreases in efficacy of the HCV drugs.28
Special populations
There are no dosage adjustments needed for SOF/VEL/VOX in mild (eGFR 50–79 mL/min/1.73m2) to moderate (eGFR 30–49 mL/min/1.73m2) renal impairment.9 At this time, there are insufficient data regarding the safety and efficacy in patients with severe renal impairment (eGFR <30 mL/min/1.73m2) or end-stage renal disease (ESRD) as it has not been studied in these patients.9 Sofosbuvir is primarily eliminated through the kidneys, so an increased exposure to the sofosbuvir metabolite would occur in severe renal impairment or ESRD, and use should be avoided.9 In patients with mild-hepatic impairment (Child-Pugh A, compensated cirrhosis), no dosage adjustment is required.9 In patients with moderate-severe hepatic impairment (Child-Pugh B or C, decompensated cirrhosis), use of SOF/VEL/VOX is currently not recommended.9 Voxilaprevir is mostly eliminated through biliary excretion; thus, use in patients with decompensated cirrhosis could lead to increased exposure to voxilaprevir.9
There is some evidence to support that a transjugular intrahepatic portosystemic shunt (TIPS) may be a risk factor for DAA failure due to the impact on pharmacokinetic and pharmacodynamic properties. A small retrospective study found that SVR was achieved in 3/3 patients treated with SOF/VEL/VOX without a TIPS versus 0/1 patients treated with SOF/VEL/VOX with a TIPS.29 Post-transplant patient studies are lacking; however, one case report showed successful SVR in a post-liver transplant, DAA-experienced patient with genotype 3 HCV.30 This patient was treated for 16 weeks with SOF/VEL/VOX along with the addition of ribavirin starting at 8 weeks.30 Further studies are needed to establish safety and efficacy in this patient population.
In patients with opioid substitution therapy (OST), there is some evidence to support the use of SOF/VEL/VOX to achieve SVR without additional safety concerns. When comparing patients on SOF/VEL/VOX who received OST or did not receive OST, SVR rates were similar, 95.9% (47/49) and 95.8% (965/1007), respectively.31 Safety and efficacy have not been established in pediatric patients, pregnant patients, or lactating patients.9 There is a black box warning for risk of Hepatitis B Virus (HBV) reactivation in patients co-infected with HCV/HBV while taking SOF/VEL/VOX.9 Reactivation of HBV has been reported in some patients who were not on HBV treatment, and some cases led to fulminant hepatitis, hepatic failure, and death.9 Therefore, all patients should be tested for current or prior HBV infection before initiating treatment with SOF/VEL/VOX.9
In patients who are co-infected with HCV/HIV, it is important to check for interactions with antiretroviral drugs, as discussed above. Both the European AIDS Clinical Society (EACS) and the American Association for the Study of Liver Diseases/Infectious Diseases Society of America (AASLD/IDSA) guidelines include SOF/VEL/VOX as a treatment option for HCV/HIV co-infected persons.6,32 Despite the lack of supporting data, AASLD/IDSA guidelines state that this treatment is predicted to have similar response to HCV mono-infected patients.6 Similarly, the 2018 US Department of Health and Human Services (DHHS) HIV Guidelines suggest that DAA regimens are just as effective in HCV/HIV co-infection as compared to HCV monoinfection.33 The DHHS guidelines do not have a specific statement on SOF/VEL/VOX; however, this treatment is included in the table of DAA drugs for HCV treatment in adults with HIV.33
Access
Bacon et al examined the accessibility and utilization of SOF/VEL/VOX in practice, focusing on patients with a history of treatment failure with an NS5A inhibitor-containing HCV regimen.34 Data for this study were acquired from Trio Health’s disease management program database and included patients who had initiated treatment with SOF/VEL/VOX between July and October of 2017.34 Accessibility was assessed by determining the proportion of patients who initiated therapy (termed “starts”), those who were prescribed therapy but did not initiate therapy (termed “non-starts”), and those who were prescribed the therapy but did not initiate the treatment within the study period (termed “pending”). The majority of patients enrolled in this study were male (99/136) with compensated cirrhosis (60/136).34 The mean age was 60, although the age range was mid-30s to early-80s for all groups except the non-start group which had a narrower range of age 55–84.34 Most patients had initiated treatment within the sampling window (83/136), with the second-largest group pending treatment (41/136) and the smallest percentage having not initiated treatment (12/136).34 The most common reason for not starting therapy was insurance denial, 75% of which were from Medicare and Medicaid, which may have been due to the patient population and not necessarily the strictness of the insurance plan.34 Other reasons for not starting treatment were physician choice (8%) and patient choice (17%).34 An interesting finding from this study was that 34% of patients with a known treatment status were treatment naïve.34 However, the reasoning why SOF/VEL/VOX was selected as initial treatment of HCV in these patients was not described.34 Treatment-experienced patients tended to have prior exposure to an NS5A inhibitor-containing regimen (22/26) or a regimen containing SOF without an NS5A inhibitor (1/26).34
Place in therapy
The approval of SOF/VEL/VOX made available an evidence-based DAA regimen for patients who experienced virologic failure on a previous NS5A or sofosbuvir-containing regimen. The evidence from the POLARIS trials, as well as the publications since gaining market approval, illustrate that the presence of baseline NS3, NS5A, and NS5B RASs that confer resistance to the individual components of SOF/VEL/VOX do not appear to have a negative impact on the efficacy of a 12-week regimen of SOF/VEL/VOX. Therefore, retreatment utilizing a 12-week regimen of SOF/VEL/VOX should be attempted in DAA-experienced patients with and without compensated cirrhosis regardless of the presence of baseline RASs. Patients who should especially be targeted to receive SOF/VEL/VOX treatment include DAA-experienced patients with advanced fibrosis or compensated cirrhosis to halt the deterioration of liver disease. Targeting this patient population before they reach the point of decompensated cirrhosis is especially important as treatment options for patients with decompensated cirrhosis are limited, and there are no high quality, evidence-based options for DAA-experienced patients with decompensated cirrhosis. Additionally, treating patients with compensated cirrhosis will likely improve the patients’ quality of life significantly, as seen for the patients enrolled in the POLARIS trials.15,16
Even though SOF/VEL/VOX was studied in some treatment naïve patient populations, its use should be reserved for DAA-experienced patients. This is owed to the fact that there are other highly effective and well-tolerated DAA regimens that include only two DAAs. SOF/VEL/VOX use should also be avoided in patients with severe renal impairment and ESRD. Until more data regarding safety are available, use of SOF/VEL/VOX in pediatric patients and patients who are pregnant and lactating should be avoided.
Of note, this literature search did not identify any studies besides the Ruane et al study21 outlined above that described how to manage a patient who may fail SOF/VEL/VOX treatment; additional research is needed in this area. For those patients who do achieve SVR with SOF/VEL/VOX, post-treatment monitoring is the same as for other DAAs: patients without advanced fibrosis should be followed-up as if they never had HCV, patients with advanced fibrosis, including cirrhosis, should be screened for HCC twice per year, and assessing for HCV recurrence or reinfection is only recommended in patients who have ongoing risk factors for HCV infection or show unexplained hepatic dysfunction.6
Conclusion
Sofosbuvir/velpatasvir/voxilaprevir is a once-daily, fixed-dose combination tablet for the treatment of HCV in adult patients with genotypes 1 through 6 who have failed treatment with an NS5A inhibitor or genotype 1a or 3 who have failed treatment with sofosbuvir without an NS5A inhibitor. Its approval has added an effective and safe option for DAA-experienced patients to the extremely effective group of DAA treatments for chronic HCV.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global hepatitis report, 2017. Available from: http://apps.who.int/iris/bitstream/10665/255016/1/9789241565455-eng.pdf?ua=1.
2. Ditah I, Ditah F, Devaki P, et al. The changing epidemiology of hepatitis C virus infection in the United States: national health and nutrition examination survey 2001 through 2010. J Hepatol. 2014;60:691–698. doi:10.1016/j.jhep.2013.11.014
3. Edlin BR, Eckhardt BJ, Shu MA. Toward a more accurate estimate of the prevalence of hepatitis C in the United States. Hepatology. 2015;62:1353–1363. doi:10.1002/hep.27978
4. Smith DB, Bukh J, Kuiken C, et al. Expanded classification of hepatitis C virus into 7 genotypes and 67 subtypes: updated criteria and genotype assignment web resource. Hepatology. 2013;59(1):318–327. doi:10.1002/hep.26639
5. US Food and Drug Administration. FDA approves Vosevi for hepatitis C [press release]. https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm567467.htm. Accessed January 21, 2019.
6. AASLD/IDSA HCV Guidelines. Recommendations for testing, managing, and treating hepatitis C. Available from: https://www.hcvguidelines.org/sites/default/files/full-guidance-pdf/HCVGuidance_May_24_2018b.pdf.
7. Wang LS, Dsouza LS, Jacobson IM. Hepatitis C- A clinical review. J Med Virol. 2016;88:1844–1855. doi:10.1002/jmv.24554
8. Poordad F, Dieterich D. Treating hepatitis C: current standard of care and emerging direct-acting antiviral agents. J Viral Hepat. 2012;19(7):449–464. doi:10.1111/j.1365-2893.2012.01617.x
9. Vosevi® [prescribing Information]. Foster City, CA: Gilead Sciences, Inc; 2017.
10. European Medicines Agency. Vosevi EPAR summary for the public. https://www.ema.europa.eu/en/documents/overview/vosevi-epar-summary-public_en.pdf. Accessed April 28, 2019
11. Bourlière M, Gordon SC, Flamm SL, et al. Sofosbuvir, velpatasvir, and voxilaprevir for previously treated HCV infection. N Engl J Med. 2017;376:2134–2146. doi:10.1056/NEJMoa1613512
12. Jacobson IM, Lawitz E, Gane EJ, et al. Efficacy of 8 Weeks of sofosbuvir, velpatasvir, and voxilaprevir in patients with chronic HCV infection: 2 phase 3 randomized trials. Gastroenterology. 2017;153(1):113–122. doi:10.1053/j.gastro.2017.03.047
13. Bourliere M, Gordon SC, Schiff ER, et al. Deferred treatment of sofosbuvir-velpatasvir-voxilaprevir for patients with chronic hepatitis C virus who were previously treated with an NS5A inhibitor: an open-label substudy of POLARIS-1. Lancet Gastroenterol Hepatol. 2018;3:559–565. doi:10.1016/S2468-1253(18)30118-3
14. Sarrazin C, Cooper CL, Manns MP, et al. No impact of resistance-associated substitutions on the efficacy of sofosbuvir, velpatasvir, and voxilaprevir for 12 weeks in HCV DAA-experienced patients. J Hepatol. 2018;69:1221–1230. doi:10.1016/j.jhep.2018.07.023
15. Younossi ZM, Stepanova M, Gordon S, et al. Patient-reported outcomes following treatment of chronic hepatitis C virus infection with sofosbuvir and velpatasvir, with or without voxilaprevir. Clin Gastroenterol Hepatol. 2018;16(4):567–574. doi:10.1016/j.cgh.2017.11.023
16. Younossi ZM, Stepanova M, Jacobson IM, et al. Sofosbuvir and velpatasvir with or without voxilaprevir in direct-acting antiviral-naïve chronic hepatitis C: patient-reported outcomes from POLARIS 2 and 3. Aliment Pharmacol Ther. 2018;47(2):259–267. doi:10.1111/apt.14423
17. Cacoub P, Bourliere M, Asselah T, et al. French patients with hepatitis C treated with direct-acting antiviral combinations: the effect of patient-reported outcomes. Value Health. 2018;21(10):1218–1225. doi:10.1016/j.jval.2018.01.006
18. Younossi ZM, Stepanova M, Afdhal N, et al. Improvement of health-related quality of life and work productivity in chronic hepatitis C patients with early and advanced fibrosis treated with ledipasvir and sofosbuvir. J Hepatol. 2015;63:337–345. doi:10.1016/j.jhep.2015.03.014
19. Younossi ZM, Stepanova M, Sulkowski M, et al. Sofosbuvir and ribavirin for treatment of chronic hepatitis C in patients co-infected with hepatitis C virus and HIV: the impact on patient‐reported outcomes. J Infect Dis. 2015;212:
20. Younossi ZM, Stepanova M, Nader F, et al. Patient‐reported outcomes in chronic hepatitis C patients with cirrhosis treated with sofosbuvir‐containing regimens. Hepatology. 2014;59:
21. Ruane P, Strasser SI, Gane EJ, et al. Sofosbuvir/velpatasvir/voxilaprevir for patients with HCV who previously received a sofosbuvir/velpatasvir-containing regimen: results from a retreatment study. J Viral Hepat. 2019;00:1–4.
22. Rodriguez-Torres M, Glass S, Hill J. GS-9857 in patients with chronic hepatitis C virus genotype 1-4 infection: a randomized, double-blind, dose-ranging phase 1 study. J Viral Hepat. 2016;23(8):614–622. doi:10.1111/jvh.12527
23. Han B, Parhy B, Zhou E, et al. In vitro susceptibility of hepatitis C virus genotype 1 through 6 clinical isolates to the pangenotypic NS3/4A inhibitor voxilaprevir. J Clin Microbiol. 2019;57(4):e01844–18. doi:10.1128/JCM.01844-18
24. Pham LV, Jensen SB, Fahnøe U, et al. HCV genotype 1-6 NS3 residue 80 substitutions impact protease inhibitor activity and promote viral escape. J Hepatol. 2019;70(3):388–397. doi:10.1016/j.jhep.2018.10.031
25. Wyles DL, Lawitz E, Cheinquer N, et al. Emergence and long-term persistence of NS3, NS5A, and NS5B resistance associated substitutions after treatment with direct-acting antivirals. Gastroenterology. 2018;54(6 Suppl1):S1104. doi:10.1016/S0016-5085(18)33672-2
26. Gilead Sciences. Safety and efficacy of sofosbuvir/velpatasvir/voxilaprevir fixed-dose combination for 12 weeks in adults who participated in a prior gilead-sponsored HCV treatment study - study results. NLM Identifier: NCT03118843. Available from: https://clinicaltrials.gov/ct2/show/results/NCT03118843.
27. Food and Drug Administration. FDA adverse event reporting system (FAERS) public dashboard. Available from: https://www.fda.gov/drugs/fda-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard.
28. University of Liverpool. HEP drug interactions. Available from: http://hep-druginteractions.org/ .
29. Piecha F, Gänßler J-M, Jordan S, et al. Transjugular intrahepatic portosystemic shunt: a possible risk factor for direct‐acting antiviral treatment failure in patients with hepatitis C? Hepatol Commun. 2019;3(5):614–619. doi:10.1002/hep4.1337
30. Cardona‐Gonzalez MG, Goldman JD, Narayan L, Brainard DM, Kowdley KV. Sofosbuvir, velpatasvir, and voxilaprevir for treatment of recurrent hepatitis c virus infection after liver transplantation. Hepatol Commun. 2018;2(12):1446–1450. doi:10.1002/hep4.1280
31. Grebely J, Feld JJ, Wyles D, et al. Sofosbuvir-based direct-acting antiviral therapies for HCV in people receiving opioid substitution therapy: an analysis of phase 3 studies. Open Forum Infect Dis. 2018;5:2. doi:10.1093/ofid/ofy001
32. European AIDS Clinical Society. Guidelines Version 9.1 October 2018. Available from: http://www.eacsociety.org/files/2018_guidelines-9.1-english.pdf.
33. Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Available from: http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf.
34. Bacon B, Curry MP, Flamm SL, et al. Access to and utilization of sofosbuvir/velpatasvir/voxilaprevir in care of chronic hepatitis c patients; data from the trio network. Gastroenterology. 2018;54(6 Suppl1):S1192–S1193. doi:10.1016/S0016-5085(18)33942-8
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.