")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Profile of Remimazolam in Anesthesiology: A Narrative Review of Clinical Research Progress
Authors Wang M, Zhao X, Yin P, Bao X, Tang H, Kang X
Received 24 May 2022
Accepted for publication 30 August 2022
Published 3 October 2022 Volume 2022:16 Pages 3431—3444
DOI https://doi.org/10.2147/DDDT.S375957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Mi Wang,1,* Xian Zhao,2,* Pengfei Yin,1 Xiuxia Bao,1 Hongli Tang,3 Xianhui Kang1
1Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Anesthesiology, Shulan (Hangzhou) Hospital Affiliated to Zhejiang Shuren University Shulan International Medical College, Hangzhou, People’s Republic of China; 3Department of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianhui Kang, Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun Road, Hangzhou, Zhejiang, People’s Republic of China, Tel +86-0571-87236169, Fax +86-21-57643271, Email [email protected] Hongli Tang, Department of Anaesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Tel +86-577-87236169, Fax +86-21-57643371, Email [email protected]
Abstract: Remimazolam is a novel short-acting γ-aminobutyric acid (GABA) receptor agonist with typical characteristics of benzodiazepine sedative drugs, nonorgan-dependent metabolism, long-term infusion without accumulation, and no injection pain. It is quite different from the other current sedative drugs and has broad prospects for application. It has been established that the metabolites of remimazolam are inactive, and the interactions with other drugs are weak with slight cardiopulmonary suppressive effects, showing good effectiveness and safety. During the 2-year period that it has been on the market, remimazolam has been used in multiple clinical scenarios, such as the induction and maintenance of general anesthesia and sedation in outpatient minor procedures or examinations. However, it’s use has also prompted widespread concern around the world. Therefore, given its short- and rapid-acting, controllable characteristics remimazolam deserves in-depth study in order for it to be used in fast-track surgery, comfort diagnosis and treatment. Notably, such agents might be of great significance, especially in elderly individuals, patients with critical diseases or patients with liver and kidney insufficiency. The current study reviews recent clinical studies (2015– 2022) on remimazolam and summarizes the characteristics of its applications. Specifically, the use of remimazolam in some specific populations are described. This study attempts to provide scientific support for the clinical application of this novel sedative drug in the field of anesthesia.
Keywords: remimazolam, anesthesia, sedation, benzodiazepine, clinical
Introduction
Remimazolam is a novel ester-benzodiazepine sedative drug that has been approved for use in the clinic since 2020. It is derived from midazolam and synthesized via the introduction of a methyl-propionate side chain of metabolic potential.1 Therefore, remimazolam combines the properties of midazolam and remifentanil. It belongs to class 1.1 of new drugs with two major salt forms: benzene sulfonic acid and toluenesulfonic acid.2 With the promotion of fast-track surgery, increasing attention has been given to optimizing perioperative medication, advancing the early recovery of organ function and decreasing the incidence of adverse events.3 Remimazolam has multiple advantages, such as a slight circulatory suppressive effect and liver and kidney function-independent metabolism.4 During the 2-years it has been on the market, remimazolam has prompted widespread concern and has emerged as an ideal sedative drug for populations at an advanced age or in a vulnerable state. In addition, it possesses unique advantages in outpatient endoscopy and treatment, procedures, and regional blockade with adjuvant sedation, owing to its being rapid- and short-acting, slight respiratory suppressive effects and the absence of injection pain. Preliminary clinical studies have also been conducted in some specific surgeries, such as cardiopulmonary bypass surgery and neurosurgery requiring intraoperative awakening.
Given the advantages mentioned above, remimazolam, as a new sedative drug, is mainly used in endoscopic examination and treatment, induction and maintenance of general anesthesia and sedation in intensive care unit (ICU) patients. However, the pharmacological characteristics and application scenarios of remimazolam in the clinic remain to be fully clarified due to the short time it has been on the market and limited clinical trials with a small sample size. In this review, we describe the progress of the clinical application of remimazolam, introduce its methods and advantages, and finally, briefly, discuss the current research hotspot and future application prospects.
Pharmacological Characteristics
Remimazolam selectively has high affinity for cerebral γ-aminobutyric acid receptors (GABA) but shows no significant selectivity for receptor subtypes and no off-target activity. Remimazolam binding with receptors can lead to chloride influx and neural cell membrane hyperpolarization, which subsequently suppresses neuronal activity and exerts sedative, anterograde amnesia and anticonvulsant effects.2 CNS7054 is the metabolite of remimazolam with shared properties but decreased affinity to the receptor (300–400 times lower).3 An animal experiment revealed that remimazolam could suppress neuronal firing from the substantia nigra pars reticulata (a region that receives striatal GABA afferent innervation), resulting in the disappearance of the righting reflex and then a sedative effect.1,2 It was reported that flumazenil, a benzodiazepine receptor antagonist, can antagonize the sedative effect of remimazolam.
A clinical study reported that the systemic clearance of remimazolam at 0.01–0.35 mg/kg after 1 min of a single intravenous injection in a healthy volunteer was 70.3 L/h, 3 times higher than that of midazolam at 0.075 mg/kg. In addition, this study reported a steady state volume of 88.1 L, terminal half-life 0.75 h and average duration time 0.51 h after remimazolam administration.4 The dose of remimazolam shows a linear relationship with pharmacokinetics, and the clearance property is fitted to a first-order pharmacokinetic model and independent of body weight. Furthermore, the specific chemical structure of remimazolam enables its metabolism to be nonspecific, degraded by widespread tissue esterases and independent of the cytochrome-dependent liver pathways. In this context, its sedative effect is short-acting with a short recovery time.5 Research also revealed that long-term or high-dose infusion of remimazolam is associated with a low risk of accumulation and prolonged drug efficacy.6
Procedural Sedation
Gastrointestinal Endoscopy
A phase IIa clinical study in 2015 reported that a single dose of remimazolam had an increased sedative effect under gastroscopy. An increase in the dose (0.10–0.20 mg/kg) resulted in shorter times to onset but disappearance of the effect.7
In a subsequent phase IIb study in 2016, a comparative analysis was done between remimazolam and midazolam, a typical benzodiazepine drug, in terms of the sedative effect colonoscopically.8 In that study, a total of 162 patients were given remimazolam (loading/maintenance doses: 8.0/3.0 mg, 7.0/2.0 mg, 5.0/3.0 mg) or midazolam (loading/maintenance doses: 2.5/1.0 mg) at random. The results revealed that adequate sedation was achieved in over 82.5% of patients receiving remimazolam at a loading dose, which was much greater than in patients receiving midazolam (46.3%). In addition, a significantly higher sedation success rate was demonstrated upon remimazolam administration during the entire procedure (92.5–97.5% vs 75.0%), and the time to onset was shorter (2.23–3.03 min vs 4.8 min). According to the Hopkins Verbal Learning Test–Revised (HVLT-R), which defines good recovery of neuropsychiatric function with a small change from baseline, patients receiving remimazolam obtained higher scores than those receiving midazolam (mean: −3.8 to −5.2 vs −8.7), suggesting a shorter time for recovery of neuropsychiatric function to normal in this population.
To verify the effectiveness and safety of remimazolam versus midazolam in clinical colonoscopy, a Phase III clinical trial was performed by Rex et al.9 In that trial, 461 patients were enrolled and randomized into 1 of 3 groups: remimazolam (5 initial/2.5 mg top-up dose), placebo, or open label midazolam (1.75 or 1 initial/1 or 0.5 mg top-up dose). It was found that the time to onset of the sedative effect of remimazolam was significantly shorter than that of midazolam (mean: 4.0 vs 19 min), and the consumption of fentanyl was smaller as well (88.6 vs 106.9 μg). In addition, remimazolam led to remarkably shorter recovery time from the end of the procedure to be being fully alert (7.35 vs 15.84 min) and to being fully conscious (3.2 h vs 6.1 h). The HVLT-R scores also revealed that, consistent with previous clinical trials, the best recovery of neuropsychiatric function in patients was following remimazolam. In terms of safety, there was no significant difference between remimazolam and midazolam regarding adverse events, despite a lower incidence of hypotension in patients with remimazolam. Notably, the advantage of remimazolam in rehabilitation might be underestimated, as the dose of midazolam was based on the US package guidelines, which is lower than that used in clinical trials.
Chen et al devised a noninferiority study on remimazolam and propofol in gastroscopy10 and colonoscopy11 examinations. This study included 384 and 388 patients who were scheduled for gastroscopy and colonoscopy, respectively, and randomly assigned them to take remimazolam (loading/maintenance doses: 5.0/2.5 mg) or propofol (loading/maintenance doses: 1.5/0.5 mg/kg). The results showed that the sedation success rate of remimazolam was 97.34% in gastroscopy and 96.91% in colonoscopy, both of which were noninferior to propofol. Additionally, the time to onset of sedation was longer with remimazolam than with propofol. Gait disturbances and vertigo were the main adverse events in populations that received both remimazolam and propofol. However, the incidence of total adverse events, bradycardia and respiratory suppression in the population treated with remimazolam was significantly lower than that in the population treated with propofol. These results indicated that remimazolam, as a fast-acting benzodiazepine sedative agent, has a longer time to onset of sedation than propofol, but it is much safer.
Bronchoscopy
To the best of our knowledge, there has been only one study on the effectiveness and safety of remimazolam in bronchoscopy.12 This US prospective, randomized, and double-blind clinical trial included 446 patients from 30 medical centers who were given remimazolam (5 initial/2.5 mg top-up dose), placebo or midazolam (1.75 or 1 initial/1 or 0.5 mg top-up dose). This study found that the sedation success rate was 80.6% with remimazolam, which was much higher than the rate of 32.9% with midazolam. In addition, shorter times to onset of sedation (mean: 6.4 min vs 16.3 min) and recovery to full alertness (mean: 6.0 vs 12.0 min) occurred in the patients with remimazolam. Furthermore, HVLT-R scores 5 min after being fully alert were shown in the patients with remimazolam, demonstrating the best recovery of neuropsychiatric function among the three groups. All these findings were consistent with the previously published literature. It was also noted that there was no remarkable difference between remimazolam and midazolam in terms of the incidence of treatment-emergent adverse events and laboratory indicators, which suggests that remimazolam is safe to use for procedural sedation in bronchoscopy.
Hysteroscopy
Remimazolam has recently been used in hysteroscopic examination, and there are only two relevant articles published in 2021. One study reported that the induction and maintenance doses of remimazolam in hysteroscopy were 0.2 mg/kg and 1.0 mg/kg/h, respectively, and the target concentration during the operation was maintained at 1.5 ng/mL via target-controlled infusion.13 In another study, the induction and maintenance doses of remimazolam were 0.25 mg/kg and 0.48–0.6 mg/kg/h, respectively.14 Both studies used adverse events as the main therapeutic outcome and revealed a significantly lower incidence of adverse events with remimazolam than with propofol. In addition, the incidence of oxygen saturation (SPO2), bradycardia and hypotension were significantly lower in the patients treated with remimazolam, demonstrating smaller effects on patient circulatory and respiratory functions. The sedation success rate was reported as 100% in patients in both studies.
General Anesthesia
The feasibility of remimazolam in general anesthesia has been extensively studied. For example, in a multicenter, single-blind phase IIb/III clinical trial conducted by Doi et al, 375 ASA I/II patients were enrolled and randomly divided into the remimazolam (6 or 12 mg/kg/h) and propofol (2.0–2.5 mg/kg) groups.15 They found that the sedation success rate of remimazolam was 95%, which was higher than the noninferiority threshold. This demonstrated that remimazolam at either 6 mg/kg/h or 12 mg/kg/h used in general anesthesia was not inferior to propofol. In addition, the loss of consciousness (LoC) time of remimazolam was significantly longer than that of propofol (mean: 102.0 s vs 88.7 s vs 78.7 s, respectively). Notably, this does not mean the prolongation of the time from induction to intubation in clinical practice. During that process, the order of induction medicines used in anesthesia can also affect the duration, and remimazolam, since it is free of injection pain, can be used first, followed by analgesics and muscle relaxants. Therefore, such a prolonged duration is not always of clinical significance. The cumulative dose of remimazolam (SD) upon LoC was 0.17 (0.04) mg/kg and 0.29 (0.08) mg/kg, respectively, but the difference requires further exploration.
Another recent clinical trial investigated the safety and feasibility of single dose remimazolam used for general anesthesia.16 In that trial, 189 ASA I/II patients who were scheduled for elective surgery under general anesthesia were included and divided into remimazolam (single doses: 0.2 mg/kg, 0.3 mg/kg, 0.4 mg/kg, within 1 min) or propofol (2.0 mg/kg, within 1 min) groups at random. The results demonstrated that the sedation success rate of propofol was significantly higher than that of remimazolam at 0.2 mg/kg (100% vs 89%), while there was no difference between the two drugs when remimazolam was used at a higher dose (0.3 mg/kg, 94%; 0.4 mg/kg, 100%). Regarding adverse events, the incidence of hypotension was significantly lower after remimazolam was used at low doses compared to propofol (13% vs 24% vs 44%) but exhibited no difference when the dose of remimazolam was 0.4 mg/kg (34% vs 44%). Given these findings, the authors recommended remimazolam at 0.3 mg/kg for the induction of general anesthesia.
Doi et al observed the maintenance effect of remimazolam during surgery.15 The mean optimal dose of remimazolam for the maintenance of anesthesia was 0.99 mg/kg/h. During the treatment, 20.0% and 24.0% of patients receiving remimazolam experienced a decline in blood pressure, much lower than the 49.3% in patients receiving propofol. In addition, the overall incidence of adverse events was also higher in patients receiving propofol versus remimazolam (61.3% vs 39.3% vs 42.7%). Therefore, remimazolam was much safer than propofol when used in the induction and maintenance of general anesthesia. Furthermore, the study also revealed a significantly prolonged extubation time with remimazolam administration. In clinical practice, the pharmacokinetic characteristics of remimazolam should be fully acknowledged when used, and the time to extubation could be reduced by reducing the dose of remimazolam or applying flumazenil.
Mao et al evaluated patients’ recovery quality who were induced and maintained by general anesthesia with remimazolam.17 The data showed that the score of remimazolam group on the first day after surgery was significantly lower than propofol group, especially the physical comfort and emotional state. Whether the occurrence of this phenomenon is universal, high-risk factors and potential mechanisms need to be further explored.
Application in Special Populations
ASA Class III or IV
A recent study reported better safety of remimazolam than midazolam in colonoscopy in a vulnerable patient population.18 This study included 79 American Society of Anesthesiologists (ASA) physical status ratings of class III or IV patients and randomly divided them into the remimazolam (2.5–5 initial/1.5–2.5 mg top-up dose) and placebo or midazolam (1.0 initial/0.5 mg top-up dose) groups. The overall incidence of emergency adverse events was similar between the groups (10.8% vs 6.7%). In addition, the percutaneous PCO2 during sedation did not vary with the baseline level in all groups, and there were no significant differences between remimazolam and midazolam regarding the minimal levels of any vital signs, including HR, RR, SPO2). It was also noted that remimazolam was associated with significantly shorter times to onset of sedation (mean: 8.0 vs 18.6 min) and to full alertness (mean: 11.0 vs 18.8 min), consistent with the results in ASA I/II patients.9 Therefore, remimazolam was considered safe and effective in ASA III or IV patients receiving colonoscopy.
Another study by Doi et al also revealed the safety and effectiveness of remimazolam used in the induction and maintenance of general anesthesia in ASA III patients.19 All 67 patents included were at ASA III scheduled for general surgery under general anesthesia using remimazolam at an initial dose of 6 mg/kg/h or 12 mg/kg/h. Under the same induction dose, the LoC time of remimazolam was shorter in ASA III patients than in ASA I/II patients (6 mg/kg/h: 97.2 s vs 102.0 s; 12 mg/kg/h: 81.7 s vs 88.7 s), and the optimal maintenance dose was significantly lower as well (0.56 mg/kg/h vs 0.57 mg/kg/h vs 0.99 mg/kg/h). However, no differences were observed in terms of the incidence of adverse events, including a decline in blood pressure (54.8% vs 67.7%). This demonstrated that the LoC time decreased with increasing induction dose of remimazolam. Additionally, dose-dependent circulatory suppression did not occur owing to the high stability of the hemodynamics of remimazolam. Considering the reduction in physical functioning in fragile patients and the more than 50% incidence of decline in blood pressure in the study above, we feel that the dose of remimazolam should be properly reduced in clinical practice.
Mechanical Ventilation in ICU
Lohmer et al reviewed four Phase II–III studies and analyzed the possible covariates that may affect the pharmacodynamic characteristics of remimazolam.20 The data revealed that there was no cumulative sedation effect during the 9 h surgery under general anesthesia, without an effect on the time to extubation. Another study exposed primary human hepatocytes to a clinical dose of remimazolam for 5 days and found that remimazolam had stable metabolic activity and a stable concentration within 8 h, without any effect on the integrity and metabolism of hepatocytes.21 In a Japanese study involving 49 ICU patients who took remimazolam for sedation, the blood drug concentration at 24 h in 7 patients was higher than that in healthy volunteers.22 Because of its pharmacokinetic properties, remimazolam has great potential for application in ICU sedation, but further studies are required to confirm its pharmacokinetic or clinical features under long-term mechanical ventilation. To date, there have been clinical trials devoted to studying the effect of remimazolam on weaning and extubation in ICU patients receiving mechanical ventilation.23
Elderly Patients
Since the elderly have comorbidities and decreased organ function, the incidence of perioperative complications and mortality is significantly higher than that in young adults. In this context, maintenance of circulatory stability during anesthesia in the elderly is a focus in anesthesiology. In addition, whether remimazolam can reduce the incidence of postoperative delirium in the elderly and advance their recovery of cognitive function requires further in-depth studies.
Remimazolam was first studied for its application in the induction and maintenance of general anesthesia in the elderly in 2014.24 First, the pharmacokinetic features of remimazolam in elderly individuals and young healthy adults were compared. It was found that young adults reached LoC when remimazolam was used at 0.2 mg/kg, while the elderly patients reached LoC when remimazolam was used at only 0.1 mg/kg. In addition, the elimination half-life of remimazolam in plasma was 48 min (39–53 min) on average in elderly individuals, which was not significantly different from that in young adults. It was also found that the elimination half-life, clearance rate, steady state volume, three-compartment model half-life, and the central volume were basically independent of the administration dose and the blood drug concentration. In terms of the maintenance characteristic of remimazolam in general anesthesia, this study reported that the average pump rate of remimazolam in the elderly and young adults was 0.72 mg/kg/h and 1.02 mg/kg/h, respectively, and the time to awakening from pump discontinuation was 14 min and 11 min, respectively. No data on safety were reported in this study.
In another observational pilot study, the feasibility of remimazolam in the induction of anesthesia in elderly individuals receiving aortic valve replacement was preliminarily explored.25 The study included 20 patients aged 65 or older with severe aortic stenosis. Remimazolam was infused at 6 mg/kg/h until LoC. Anesthesia was successfully induced in all patients. There were 14 patients receiving ephedrine or phenylephrine (3 doses in 1 patient, 2 doses in 4 patients, and one dose in 9 patients). No severe adverse events were observed, including severe bradycardia <40 bpm, life-threatening arrhythmia, or myocardial ischemia.
Liu et al directed a clinical trial to explore the feasibility of remimazolam for enteroscopy in elderly patients.26 A total of 260 subjects were randomly assigned to the remimazolam group (initial dose: 0.15 mg/kg; maintenance dose: 0.075 mg/kg) or the etomidate combined with propofol group. The data showed that the operation success rate of the remimazolam group was not inferior to that of the combined group (96.52% vs 100%), which suggested that remimazolam could be effectively used in elderly patients undergoing enteroscopy. At the same time, the incidence of complete alertness time (3 min vs 4 min), discharge time (13.92 min vs 14.97 min), muscle fibrillation and injection pain (3.48% vs 12.82%) were lower in the remimazolam group.
Moreover, remimazolam was also studied in the elderly for its optimal dose used in gastroscopic examination.27 The cognitive function of patients receiving remimazolam (0.1 mg/kg or 0.2 mg/kg) and propofol was comprehensively assessed via the digit symbol substitution test, the number connection test, and the Auditory Verbal Learning Test-Huashan. The results showed that cognitive function after administration of 0.1 mg/kg remimazolam was not significantly different from the baseline level. In addition, there were no remarkable differences between remimazolam and propofol in terms of the sedation duration (8.27 vs 8.21 min) and recovery time (3.82 vs 4.33 min). However, remimazolam was associated with a much lower incidence of hypotension (3.0% vs 38.5%).
Cardiac Surgery
Cardiac surgery is characterized by great trauma and associated with a high incidence of postoperative complications and patient mortality. Much attention has been given to how to optimize anesthesia schemes to reduce organ injuries and improve prognosis.
In 2015, German researchers performed a Phase II trial on the effect of remimazolam in cardiac surgery.28 This was a single-blind trial involving 90 patients who were scheduled for cardiac surgery with cardiopulmonary bypass, including 41 patients over 65. Two groups were generated: remimazolam (initial dose: 6 or 12 mg/kg/h; maintenance dose: 1–3 mg/kg/h) and a combination of propofol with sevoflurane. Statistically, the sedation success rate between the two groups was comparable (98% vs 96%). The LoC time of patients with remimazolam (6 mg/kg/h and 12 mg/kg/h) was longer than that of patients with combination treatment, but the difference was not statistically significant. In addition, the LoC time shortened with the increased induction dose of remimazolam. There was no relevant report on the relationship between the induction dose and incidence of adverse events. This study also showed that the dose of norepinephrine applied during anesthesia was much lower in the remimazolam group than in the combination group (mean: 23.676 ng/kg/min vs 43.171 ng/kg/min), which supports the slight circulatory suppressive effect of remimazolam. A much longer extubation time in the remimazolam group was also demonstrated (mean: 145.5 min vs 97 min).
A recently published double-blind clinical trial explored the effect of remimazolam anesthesia induction on hemodynamics in patients undergoing valve replacement.29 A total of 60 patients were randomly assigned to the remimazolam group (0.3 mg/kg) or the propofol group. Data analysis showed that during the induction period, the change in mean arterial pressure (19.5 mmHg vs 26.7 mmHg), the incidence of hypotension (5% vs 13%), and the dose of norepinephrine used (8.3 µg vs 33.3 µg) in the remimazolam group were significantly lower than those in the control group.
In the future, the optimal timing and dose of remimazolam used in cardiac surgery needs to be further identified to formulate better medication strategies. In the meantime, whether remimazolam is protective for the organs and its underlying mechanism requires further study.
Hepatic or Renal Impairment
There were two independent clinical trials guided by Stohr et al, where the pharmacokinetic features of remimazolam (liver, 0.1 mg/kg; kidney, 1.5 mg) in patients with liver and kidney dysfunction were observed.30 The results demonstrated that the clearance rate of remimazolam in patients with severe liver injury was reduced by 38.1% compared to that in healthy volunteers, and the recovery time was correspondingly prolonged (healthy 8.0 min; moderate 12.1 min; severe 16.7 min). In addition, the clearance rate of remimazolam in patients with renal injury was equivalent to that of healthy volunteers, but the clearance rate of its nonactive metabolite CNS7054 was consistent with the decline in renal function. The peak blood drug concentration was independent of the decline in liver or renal function. Moreover, the overall incidence of adverse events in patients with liver and renal function receiving remimazolam was low, without any severe side effects. Current research found that carboxylesterase can be found in the liver, lung, colon, large arteries31 and adipose tissue32 at both the mRNA and protein levels. Despite the strong extrahepatic metabolic activity, remimazolam can be affected to some extent by severe liver injury.
Studies on the effect of remimazolam in patients with poor liver and renal function are few at present, and caution is needed in clinical practice. According to the specifications, remimazolam can be used on a regular basis in populations with no need for dialysis for renal injury and with mild-moderate liver injury. Additionally, a low maintenance dose is recommended in populations with severe liver injury. Table 1 shows the details of clinical trials related to remimazolam.
 |
Table 1 Published Studies of Remimazolam Clinical Trials |
Case Report
To our knowledge, there were many reports that reported the use of remimazolam in specific surgeries, including spinal operation,33 thyroid surgery,34 awake craniotomy35–37 and cardiopulmonary bypass.38,39
More attention should be given to the application of remimazolam in the induction and maintenance of general anesthesia in patients with respiratory impairment (such as mitochondrial encephalomyopathy40 and muscular dystrophy).41–43 Nakayama et al reported two superaged females (95 and 103 years old) who were treated following hip fracture surgery under general anesthesia using low-dose remimazolam.44
There are also two cases in which patients suffered precipitation formation when remimazolam and Ringer’s solution were combined.45,46 The two cases had no serious consequences. This suggests that when remimazolam is used, the dose should be properly reduced, the infusion rate should be increased, and the infusion drip should be closely monitored. Ringer’s solution should be used cautiously, especially in combination with remimaxolam.
Yamamoto et al reported a case of a patient who was sedated again after the use of flumazenil, an antagonist of remimazolam.47 Theoretically, the half-life of flumazenil is approximately 50 min, which is comparable to the 0.7 h of remimazolam. However, there is still a risk of sedation after remimazolam is antagonized. Furthermore, given that remimazolam is structurally derived from midazolam, there is also a risk of cross resistance or allergy when remimazolam is used in combination with other benzodiazepine drugs.48,49 Table 2 presents details of remimazolam-related case reports.
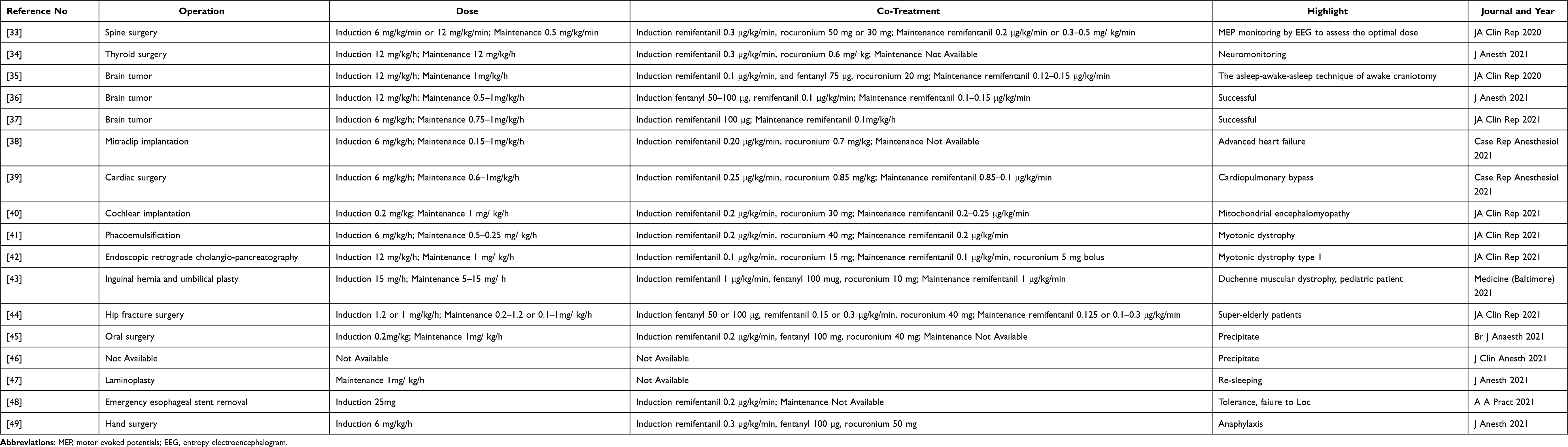 |
Table 2 Case Reports |
Adverse Reactions
Common adverse events of remimazolam include hypotension, dizziness, headache, reduced respiratory frequency, and increased blood bilirubin.50,51 Phase I–III studies reported a 2.65–6.45% incidence of hypotension.4,8–10 In a phase III clinical trial, the incidence of respiratory suppression in ASA III/IV patients receiving remimazolam was as high as 19.4%.18 There were no severe consequences, and the patients then underwent routine treatments, such as lower jaw lifting. Spontaneous resolution of the symptoms was observed. Comparatively, remimazolam is associated with a lower incidence of adverse events than midazolam and propofol, and the events tend to be mild,52 as evidenced by a series of clinical trials. It is noted that during the application of remimazolam, patient blood pressure should be closely monitored, and vasoactive drugs can be prescribed if needed.53
Summary and Prospects
Remimazolam is a novel “soft drug” with typical pharmacological effects of benzodiazepines (such as sedation, hypnosis, anti-anxiety) and multiple characteristics (such as fast-acting, short duration and nonorgan-dependent). It is superior to midazolam and propofol, with better controllability and smaller effects on the respiratory and circulatory systems. Therefore, it has outstanding advantages in clinical sedation, which were shown in the quality of recovery from anesthesia and the turnover efficiency. Moreover, remimazolam can be used in more patients and has wider applications. For instance, remimazolam might be effective as an adjuvant sedative agent in painless examinations or local anesthesia in populations with advanced age, obesity, and ASA III/IV.
Nevertheless, remimazolam still has some limitations. First, its effects in pediatric cases and patients with poor liver and renal functions require further exploration, and the safe use of the antagonist flumazenil needs further testing in the future. In addition, the pharmacokinetic characteristics of prolonged remimazolam in ICU patients with mechanical ventilation need to be identified in future studies. Second, whether remimazolam is cardioprotective during cardiac surgery with cardiopulmonary bypass should be confirmed, although it has a small effect on heart rate and blood pressure. Third, the interactions between remimazolam and volatile anesthetics are elusive, and more evidence is required to support its effect on postoperative neural disorders, such as delirium.
Currently, more challenges are being met by anesthesiologists because of the development of new anesthetics and increased levels of surgical techniques. More studies are needed on remimazolam to maximize its clinical advantages and minimize adverse events in order to provide patients with better diagnosis and treatment.
Acknowledgments
This project was supported by Bethune Charitable Foundation (BCF-RF-WSQZTZJ-202011-031), NSFC 81973620, Zhejiang basic public welfare project LGD20H290002.
Disclosure
The authors declare no potential conflicts of interest.
References
1. Kilpatrick GJ, McIntyre MS, Cox RF, et al. CNS 7056: a novel ultra-short-acting benzodiazepine. Anesthesiology. 2007;107:60–66. doi:10.1097/01.anes.0000267503.85085.c0
2. Brohan J, Goudra BG. The role of GABA receptor agonists in anesthesia and sedation. CNS Drugs. 2017;31:845–856. doi:10.1007/s40263-017-0463-7
3. Upton R, Martinez A, Grant C. A dose escalation study in sheep of the effects of the benzodiazepine CNS 7056 on sedation, the EEG and the respiratory and cardiovascular systems. Br J Pharmacol. 2008;155:52–61. doi:10.1038/bjp.2008.228
4. Wiltshire HR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo- and midazolam-controlled Phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): part II. Population pharmacokinetic and pharmacodynamic modeling and simulation. Anesth Analg. 2012;115:284–296. doi:10.1213/ANE.0b013e318241f68a
5. Freyer N, Knöspel F, Damm G, et al. Metabolism of remimazolam in primary human hepatocytes during continuous long-term infusion in a 3-D bioreactor system. Drug Des Devel Ther. 2019;13:1033–1047. doi:10.2147/DDDT.S186759
6. Antonik LJ, Goldwater DR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo- and midazolam-controlled phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): part I. Safety, efficacy, and basic pharmacokinetics. Anesth Analg. 2012;115:274–283. doi:10.1213/ANE.0b013e31823f0c28
7. Borkett KM, Riff DS, Schwartz HI, et al. A Phase IIa, randomized, double-blind study of remimazolam (CNS 7056) versus midazolam for sedation in upper gastrointestinal endoscopy. Anesth Analg. 2015;120:771–780. doi:10.1213/ANE.0000000000000548
8. Pambianco DJ, Borkett KM, Riff DS, et al. A phase IIb study comparing the safety and efficacy of remimazolam and midazolam in patients undergoing colonoscopy. Gastrointest Endosc. 2016;83:984–992. doi:10.1016/j.gie.2015.08.062
9. Rex DK, Bhandari R, Desta T, et al. A phase III study evaluating the efficacy and safety of remimazolam (CNS 7056) compared with placebo and midazolam in patients undergoing colonoscopy. Gastrointest Endosc. 2018;88:427–437 e426. doi:10.1016/j.gie.2018.04.2351
10. Chen SH, Yuan TM, Zhang J, et al. Remimazolam tosilate in upper gastrointestinal endoscopy: a multicenter, randomized, non-inferiority, phase III trial. J Gastroenterol Hepatol. 2021;36:474–481. doi:10.1111/jgh.15188
11. Chen SH, Wang J, Xu XH, et al. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, phase III clinical trial. Am J Transl Res. 2020;12:4594.
12. Pastis NJ, Yarmus LB, Schippers F, et al. Safety and efficacy of remimazolam compared with placebo and midazolam for moderate sedation during bronchoscopy. Chest. 2019;155:137–146. doi:10.1016/j.chest.2018.09.015
13. Zhang X, Li S, Liu J. Efficacy and safety of remimazolam besylate versus propofol during hysteroscopy: single-centre randomized controlled trial. BMC Anesthesiol. 2021;21:156. doi:10.1186/s12871-021-01373-y
14. Zhang S, Wang J, Ran R, Peng Y, Xiao Y. Efficacy and safety of remimazolam tosylate in hysteroscopy: a randomized, single-blind, parallel controlled trial. J Clin Pharm Ther. 2021;47:55–60 doi:10.1111/jcpt.13525.
15. Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34:543–553. doi:10.1007/s00540-020-02788-6
16. Dai G, Pei L, Duan F, et al. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021;87. doi:10.23736/S0375-9393.21.15517-8
17. Mao Y, Guo J, Yuan J, Zhao E, Yang J. Quality of recovery after general anesthesia with remimazolam in patients’ undergoing urologic surgery: a randomized controlled trial comparing remimazolam with propofol. Drug Des Devel Ther. 2022;16:1199–1209. doi:10.2147/DDDT.S359496
18. Rex DK, Bhandari R, Lorch DG, Meyers M, Schippers F, Bernstein D. Safety and efficacy of remimazolam in high risk colonoscopy: a randomized trial. Dig Liver Dis. 2021;53:94–101. doi:10.1016/j.dld.2020.10.039
19. Doi M, Hirata N, Suzuki T, Morisaki H, Morimatsu H, Sakamoto A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): results of a multicenter, randomized, double-blind, parallel-group comparative trial. J Anesth. 2020;34:491–501. doi:10.1007/s00540-020-02776-w
20. Lohmer LL, Schippers F, Petersen KU, Stoehr T, Schmith VD. Time-to-event modeling for remimazolam for the indication of induction and maintenance of general anesthesia. J Clin Pharmacol. 2020;60:505–514. doi:10.1002/jcph.1552
21. Zhou J, Curd L, Lohmer LL, et al. Population pharmacokinetics of remimazolam in procedural sedation with nonhomogeneously mixed arterial and venous concentrations. Clin Transl Sci. 2021;14:326–334. doi:10.1111/cts.12875
22. Zhou J, Leonowens C, Ivaturi VD, et al. Population pharmacokinetic/pharmacodynamic modeling for remimazolam in the induction and maintenance of general anesthesia in healthy subjects and in surgical subjects. J Clin Anesth. 2020;66:109899. doi:10.1016/j.jclinane.2020.109899
23. Liu S, Su L, Zhang B, et al. The availability and safety study of remimazolam besylate for injection on sedation of ERAS patients under mechanical ventilation in ICU: protocol for a randomized, open-label, controlled trial. Front Med. 2021;8:735473. doi:10.3389/fmed.2021.735473
24. Matsuyuki DOI. Remimazolam. J Japan Soc Clin Anesthesia Japanese. 2014;34(7):860–866.
25. Nakanishi T, Sento Y, Kamimura Y, Tsuji T, Kako E, Sobue K. Remimazolam for induction of anesthesia in elderly patients with severe aortic stenosis: a prospective, observational pilot study. BMC Anesthesiol. 2021;21:306. doi:10.1186/s12871-021-01530-3
26. Liu X, Ding B, Shi F, et al. The efficacy and safety of remimazolam tosilate versus etomidate-propofol in elderly outpatients undergoing colonoscopy: a prospective, randomized, single-blind, non-inferiority trial. Drug Des Devel Ther. 2021;15:4675–4685. doi:10.2147/DDDT.S339535
27. Yingjie T, Wen O, Yongzhong T, Ning F, Chao F, Chengxuan Q. Effect of remimazolam tosilate on early cognitive function in elderly patients undergoing upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2021;37:576–583.
28. Bevilacqua C, Probst S, Soehngen M, Ender J. The sedative effect of remimazolam in general anesthesia for cardiac surgery measured by Narcotrend. J Cardiothorac Vasc Anesth. 2015;29:S50–S51. doi:10.1053/j.jvca.2015.05.267
29. Liu T, Lai T, Chen J, et al. Effect of remimazolam induction on hemodynamics in patients undergoing valve replacement surgery: a randomized, double-blind, controlled trial. Pharmacol Res Perspect. 2021;9:e00851. doi:10.1002/prp2.851
30. Stohr T, Colin PJ, Ossig J, et al. Pharmacokinetic properties of remimazolam in subjects with hepatic or renal impairment. Br J Anaesth. 2021;127:415–423. doi:10.1016/j.bja.2021.05.027
31. Kilpatrick GJ. Remimazolam: non-clinical and clinical profile of a new sedative/anesthetic agent. Front Pharmacol. 2021;12:690875. doi:10.3389/fphar.2021.690875
32. Shimamoto Y, Sanuki M, Kurita S, Ueki M, Kuwahara Y, Matsumoto A. Factors affecting prolonged time to extubation in patients given remimazolam. PLoS One. 2022;17:e0268568. doi:10.1371/journal.pone.0268568
33. Kondo T, Toyota Y, Narasaki S, et al. Intraoperative responses of motor evoked potentials to the novel intravenous anesthetic remimazolam during spine surgery: a report of two cases. JA Clin Rep. 2020;6:97. doi:10.1186/s40981-020-00401-z
34. Hayamizu K, Chaki T, Tachibana S, Hirata N, Yamakage M. Effect of remimazolam on intraoperative neuromonitoring during thyroid surgery: a case series. J Anesth. 2021;35:581–585. doi:10.1007/s00540-021-02955-3
35. Sato T, Kato Y, Yamamoto M, Nishiwaki K. Novel anesthetic agent remimazolam as an alternative for the asleep-awake-asleep technique of awake craniotomy. JA Clin Rep. 2020;6:92. doi:10.1186/s40981-020-00398-5
36. Sato T, Nishiwaki K. Comparison of remimazolam and propofol in anesthetic management for awake craniotomy: a retrospective study. J Anesth. 2021;36:152–155. doi:10.1007/s00540-021-03021-8
37. Yoshida A, Kurata S, Kida K, Tsubokawa T. Anesthetic management for the sleep-awake-sleep technique of awake craniotomy using a novel benzodiazepine remimazolam and its antagonist flumazenil. JA Clin Rep. 2021;7:14. doi:10.1186/s40981-021-00417-z
38. Satoh T, Nishihara N, Sawashita Y, Ohno S, Hirata N, Yamakage M. Remimazolam anesthesia for MitraClip implantation in a patient with advanced heart failure. Case Rep Anesthesiol. 2021;2021:5536442. doi:10.1155/2021/5536442
39. Saito K, Ohno S, Maeda M, Hirata N, Yamakage M. Remimazolam anesthesia for cardiac surgery with cardiopulmonary bypass: a case report. JA Clin Rep. 2021;7:21. doi:10.1186/s40981-021-00424-0
40. Suzuki Y, Doi M, Nakajima Y. General anesthesia with remimazolam in a patient with mitochondrial encephalomyopathy: a case report. JA Clin Rep. 2021;7:51. doi:10.1186/s40981-021-00454-8
41. Morimoto Y, Yoshimatsu A, Yoshimura M. Anesthetic management for a patient with myotonic dystrophy with remimazolam. JA Clin Rep. 2021;7:10. doi:10.1186/s40981-021-00413-3
42. Fukuda M, Tachibana S, Nishihara N, Yamakage M. Remimazolam for a patient with myotonic dystrophy type 1 who underwent endoscopic retrograde cholangiopancreatography under general anesthesia: a case report. JA Clin Rep. 2021;7:17. doi:10.1186/s40981-021-00422-2
43. Horikoshi Y, Kuratani N, Tateno K, et al. Anesthetic management with remimazolam for a pediatric patient with Duchenne muscular dystrophy. Medicine. 2021;100:e28209. doi:10.1097/MD.0000000000028209
44. Nakayama J, Ogihara T, Yajima R, Innami Y, Ouchi T. Anesthetic management of super-elderly patients with remimazolam: a report of two cases. JA Clin Rep. 2021;7:71. doi:10.1186/s40981-021-00474-4
45. Sasaki H, Hoshijima H, Mizuta K. Ringer’s acetate solution-induced precipitation of remimazolam. Br J Anaesth. 2021;126:e87–e89. doi:10.1016/j.bja.2020.11.021
46. Yoshida K, Tanaka S, Watanabe K. A case of intravenous line occlusion when using Acetated Ringer’s solution and remimazolam. J Clin Anesth. 2021;70:110190. doi:10.1016/j.jclinane.2021.110190
47. Yamamoto T, Kurabe M, Kamiya Y. Re-sleeping after reversal of remimazolam by flumazenil. J Anesth. 2021;35:322. doi:10.1007/s00540-021-02915-x
48. Yoshikawa H, Hosokawa M, Kashima Y, Oki S, Masui K. Remimazolam tolerance in long-term benzodiazepine users: a case report of 2 cases. A a Pract. 2021;15:e01460. doi:10.1213/XAA.0000000000001460
49. Tsurumi K, Takahashi S, Hiramoto Y, Nagumo K, Takazawa T, Kamiyama Y. Remimazolam anaphylaxis during anesthesia induction. J Anesth. 2021;35:571–575. doi:10.1007/s00540-021-02934-8
50. Lee B, Kim MH, Kong HJ, et al. Effects of remimazolam vs. sevoflurane anesthesia on intraoperative hemodynamics in patients with gastric cancer undergoing robotic gastrectomy: a propensity score-matched analysis. J Clin Med. 2022;11:2643.
51. Morimoto Y. Efficacy and safety profile of remimazolam for sedation in adults undergoing short surgical procedures. Ther Clin Risk Manag. 2022;18:95–100. doi:10.2147/TCRM.S304556
52. Chen X, Xin D, Xu G, Zhao J, Lv Q. The efficacy and safety of remimazolam tosilate versus dexmedetomidine in outpatients undergoing flexible bronchoscopy: a prospective, randomized, blind, non-inferiority trial. Front Pharmacol. 2022;13:902065. doi:10.3389/fphar.2022.902065
53. Zhang Y, Dai G, Xu H, Liu Y, Liao M, Zhang X. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia: a reply. Minerva Anestesiol. 2022;88:194–195. doi:10.23736/S0375-9393.21.16169-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.