")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Profile of Overweight and Obesity in Children and Adolescents and Frequency of Type 2 Diabetes Mellitus and Glucose Intolerance: A Study in Public School in Brazil
Authors Zaccarelli-Marino MA, Fonseca FLA, Gascón TM, Filipini R
Received 16 January 2020
Accepted for publication 29 April 2020
Published 21 May 2020 Volume 2020:13 Pages 1733—1741
DOI https://doi.org/10.2147/DMSO.S246061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Maria Angela Zaccarelli-Marino,1 Fernando Luiz Affonso Fonseca,2,3 Thaís Moura Gascón,2 Rosangela Filipini4
1Internal Medicine Department, Endocrinology Service, ABC Medical School Foundation, Santo André, SP, Brazil; 2Clinical Laboratory Analysis of ABC Medical School Foundation, Santo André, SP, Brazil; 3Federal University of São Paulo, Diadema, SP, Brazil; 4Nursing Course ABC Medical School Foundation, Santo André, SP, Brazil
Correspondence: Thaís Moura Gascón
Clinical Analysis Laboratory of Faculdade de Medicina ABC, 2000, Lauro Gomes Avenue, Santo André CEP 09060-650, SP, Brazil
Tel +55 11 972280763
Email [email protected]
Objective: To verify if there is an increase in frequency of type 2 diabetes mellitus (DM2) and glucose intolerance in children and adolescents who are overweight and obese.
Methods: This was a cross-sectional survey. The study population consisted of 2757 students of both sexes (1415 girls and 1342 boys) attending public schools in São Paulo state, Brazil,aged 10– 19 years, from 2011 to 2012. Students not within this age range and those with type 1 diabetes mellitus were excluded. Upon interview, anthropometry, capillary blood glucose testing, fasting glucosemia (FG) and glucosemia 2 hours after 75 g of dextrose (AD) variables were obtained. We emphasize that, inspite of the 2757 students included in the next stage, only 88 students agreed to participate, and low compliance of those participants is due to the fact that they were children and adolescents who depend on the authorization of their parents or tutors, who have demonstrated deficient knowledge of familial chronic diseases such as obesity and its consequences, and the risk of DM2.
Results: More often girls, 1415 (51.3%). A total of 27.3% was overweight/obese/severely obese. Capillary blood glucose testing was performed in 88 (3.2%) children and adolescents with low values of glycemic results after the glucose load. There was no statistical significance between sex and glucosemia, with an average FG and AD of 92.8 mg/dL (male), 91.8 mg/dL (female) and 89.1 mg/dL (male) and 88.9 mg/dL (female), respectively.
Conclusion: This survey emphasizes that more attention should be paid to diet interventions and practicing of physical activities demanding habit changes and acquisition of special behaviour for self-care, and provision of a better educational health program, suggesting the effective participation of the family.
Keywords: obesity, diabetes mellitus, glucose intolerance, adolescents, public school, Brazil
Introduction
Type 2 diabetes mellitus (DM2) is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both1 and is present in 90% to 95% of cases of diabetes and the majority of patients are overweight or obese. DM2 has always been regarded as a disease of adults.2 Up to the present time, the majority of children with diabetes mellitus (DM), have presented with type 1 diabetes mellitus (DM1), and 1% to 2% of American children presented with DM2 or other form.2 However, over the past two decades, in children and adolescents, in several regions of the world, an augmentation in the prevalence of pediatric DM2 has been observed,3 particularity among children of certain ethnic backgrounds.4
The increase in prevalence of obesity in adolescence registered in the last few years would explain, in great part, the advancement of DM2 in the younger population, as well as, the upsurge of metabolic syndrome, associated with cardiovascular diseases in maturity.5
The prevalence estimate for DM2 in the United States (US) ranges from about 1 in 5000 white children to close to 1 in 500 American Indian children. This is equivalent to approximately 3700 new cases of DM2 in children in the United States each year.6
Recent data published by the World Health Organization (WHO), suggest that 19% of the world’s diabetic population resides in India. Screening performed in 126 Indian students, in order to evaluate the chance of developing DM2 in the future, found 8%, 13% and 79% at risk of developing the disease.7
Although the great majority of children with DM2 are overweight or obese,8 there have been no systematic studies of the prevalence of impaired glucose tolerance or DM2 in cohorts of overweight or obese children.
In Brazil, the prevalence of being overweight in adolescents has increased 6 times (3.7–21.7%) among boys and 3 times (7.6–19.0%) among girls in the period 1974–1975 and 2008–2009, respectively, according to the Brazilian Institute of Geography and Statistics.9 In relation to obesity, the increase was 5 times (0.4–5.9%) among boys and 6 times among girls (0.7–6.0%), respectively.9 It is important to emphasize that being overweight increases the risk of type 2 diabetes mellitus (DM2) 3 times.10
Although the great majority of children with DM2 are overweight or obese,8 there have been no systematic studies of the prevalence of impaired glucose tolerance or DM2 in cohorts of overweight or obese children, and in Brazil the studies are still rare.
The objective of this study was to verify if there is in Brazil, in the city of Santo André, state of São Paulo, a profile of overweight and obese children and adolescents from public schools and the frequency of type 2 diabetes mellitus and glucose intolerance.
Subjects and Methods
Study Design and Data Collection
This was a cross-sectional survey. We evaluated students from Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, state of São Paulo, Brazil, during the period March 2011 through November 2012. The research population was defined starting with 30 schools, however, after the explanation about this study to their directors, only 7 schools agreed to participate, thus the sampling had a probabilistic character for convenience with a total of 2757 students (1415 girls and 1342 boys).
The inclusion criteria for the analysis of data included aged between 10 and 19 years; students not in this age range and those with DM1 were excluded.
The data collection consisted of obtaining information of students and adolescents and their biological variations (gender and age), anthropometry and capillary blood glucose testing, which comprised the variables of the study. Their ages, for analysis purposes, were classified according to their age groups in sets of ten.
Prior to data collection, free consent was signed by the father, mother or responsible person and authorization to this realization was obtained from the Management of Teaching of the Santo André Municipality and the Directors of the State School (SS): SS Cristina Fittipaldi, SS Rener Caran, SS Celso Gama, SS Nadir Lessa, SS Marajoara II, SS Maria de Lourdes Guimarães, SS Adib Chammas.
The anthropometric study was performed in the participating schools by a previously trained team, utilizing the methodology recommended by the WHO.11 Thus, the evaluations were obtained without shoes, light clothes, an anthropometric scale (Filizola brand), and weight (Kg) and height (m) were evaluated. Later, Body Mass Index (BMI) was calculated through weight (Kg)/height2 (m2). The classification adopted the 2006–2007 WHO curves.11 The choice of this classification was based on the fact that the WHO curves of growth is a very relevant instrument in the evaluation of growth of children and adolescents from 5–19 years, and is independent of ethnic group, socioeconomic status, and nourishment. It adapted quite well to the patterns of growth of this group and its cut-off points for overweight and obesity recommended for adults were the best reference for their nutritional evaluation.
Considering that this study group corresponded to 10–19 year-old children and adolescents, we used the BMI/age classification for this age group11 according to scores Z, for instance: < escore-Z −3= accentuated thinness; ≥ escore-z −3 and < escore-z −2= thinness; ≥ escore-z −2 and ≤ escore-z +1= eutrophy; ≥ escore-z +1 and ≤ escore-z +2= overweight; ≥ escore-z +2 and ≤ escore-z +3= obesity; > escore-z +3= severe obesity. For presentation of data we decided to convert scores Z to percentiles in order to facilitate the presentation of data to families and schools.
Collection of Blood
Before collecting blood, ethical clearance for the study was obtained from the Committee of Ethics in Research of the Medical School of the ABC Foundation, SP, Brazil. Permission for data and sample collection was obtained from the father, mother or responsible person and authorization to this realization was obtained from the Management of Teaching of the Santo André Municipality and the Directors of the State School (SS): SS Cristina Fittipaldi, SS Rener Caran, SS Celso Gama, SS Nadir Lessa, SS Marajoara II, SS Maria de Lourdes Guimarães, SS Adib Chammas.
After this phase, children and adolescents were called in order to have glucosemia tests in their own schools. The tests intended to evaluate glucose intolerance or DM2, that is, to verify the conditions of capillary glucose in these subjects. The glucosemia dosages, capillary blood glucose testing, fasting glucosemia (FG) and glucosemia 2 hours after 75 g of dextrose (AD), were evaluated only in 88 children and adolescents, in spite of the request performed during the data collection.
We emphasize that, in spite of the 2757 students included for the next stage, only 88 students agreed to participate, and low compliance of those participants is due to the fact that they were children and adolescents that depend on the authorization of their parents or tutors, that have demonstrated deficient knowledge of familial chronic diseases such as obesity and its consequences, and the risk of DM2.
Of the total 2757 students, 752 (27.3%) children and adolescents were classified as being overweight/obese/severely obese, and 88 (11.7%) of those participated in the collection of blood.
The 88 subjects were examined after 8 to 16 hours of fasting. Fasting was defined as the lack of caloric ingestion, minimum of 8 hours.12 In order to obtain the oral test 2 hours after 75 g of dextrose (AD), we considered: period of fasting between 8 to 16 hours; normal physical activity; communication of presence of infections and ingestion of medications or inactivity; utilization of 1.75 g of dextrose for kilogram (Kg) of weight up to 75 g maximum.13
After evaluation, a digital puncture was obtained with a disposable needle to produce a drop of blood. Immediately after, the drop was placed on a reagent strip (Roche), followed by a glucometer reading. The results were kept for future analysis.
Three criteria were accepted for the diagnosis of normal fasting glucosemia, impaired fasting glucose tolerance and fasting DM: normal fasting glucosemia < 100 mg/dL and 2h after 75 g of dextrose < 140 mg/dL; impaired fasting glucose tolerance ≥ 100 and < 126 mg/dL and 2h after 75 g of dextrose ≥ 140 and < 200 mg/dL; fasting diabetes mellitus ≥ 126 mg/dL and 2h after 75 g of dextrose ≥ 200 mg/dL.12
Theory/Calculation
Elaboration and analysis of data was performed by statistical Software’s Epi-Info, 7 and JMP Statistical Discovery from SAS - “Statistical Analysis System”, Version 11. Variance analysis and Pearson’s Correlation were also performed.
Level of significance was 5%.
Results
Among children and adolescents followed in the 7 Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, state of São Paulo, Brazil, 2757 were analyzed between 10 and 19 years of age. In this study group, we observed a higher frequency of girls, 1415 (51.3%). The average age was 14 years, with a variation between 10 to 19 years and low standard deviation (1.9 years), which characterized the sample with a normal distribution according to age.
As to the nutritional conditions verified by BMI, as presented in “Methods”, they were classified in percentiles in agreement with WHO 2007.11
The result can be seen in Table 1, showing the evidence of a predominance of eutrophic children and adolescents (69.9%), however, with the presence of children and adolescents who are overweight/obese (25.9%) and cases of severe obesity (1.4%).
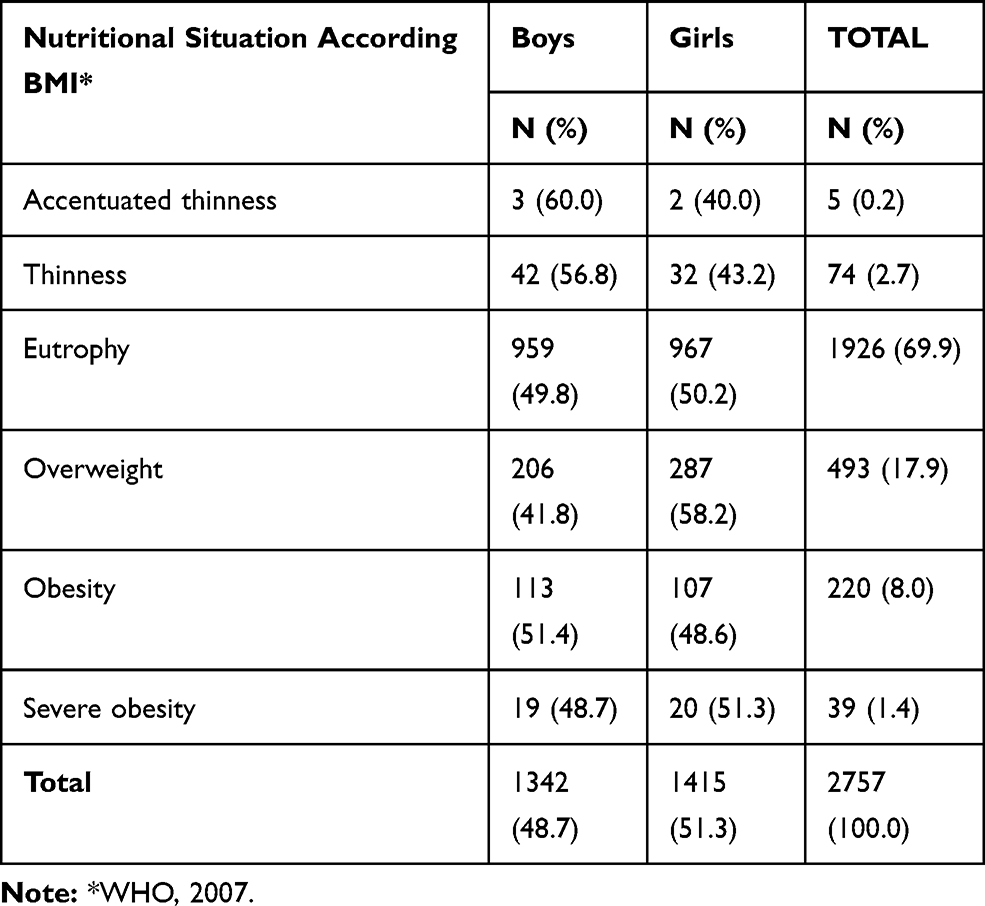 |
Table 1 Distribution of Children and Adolescents, According Gender and Nutritional Situation in Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, State of São Paulo, Brazil, from 2011 to 2012 |
Still, Figure 1 shows the distribution of BMIs with a tendency to distribute on the right, where the more elevated ones are located. Figure 2 shows a comparison between the average BMIs for gender and age groups. Notice that there is a significant difference between the BMI average for sex and age groups (p<0.001). This test confirms the univariant analysis performed between BMI for sex and BMI for age groups, that is, female groups presented with average BMI greater than males and average BMI increased according to the increase of age group. It is important to notice that Table 1 also demonstrates a greater proportion of girls who are overweight.
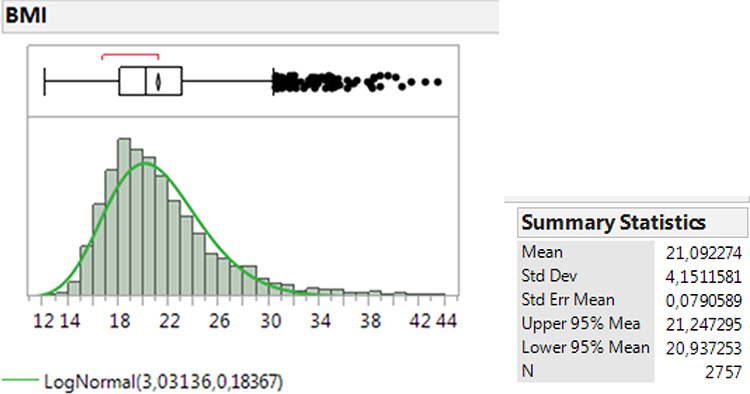 |
Figure 1 Distribuition of BMI in 2.757 children and adolescents in Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, state of São Paulo, Brazil, from 2011 to 2012. |
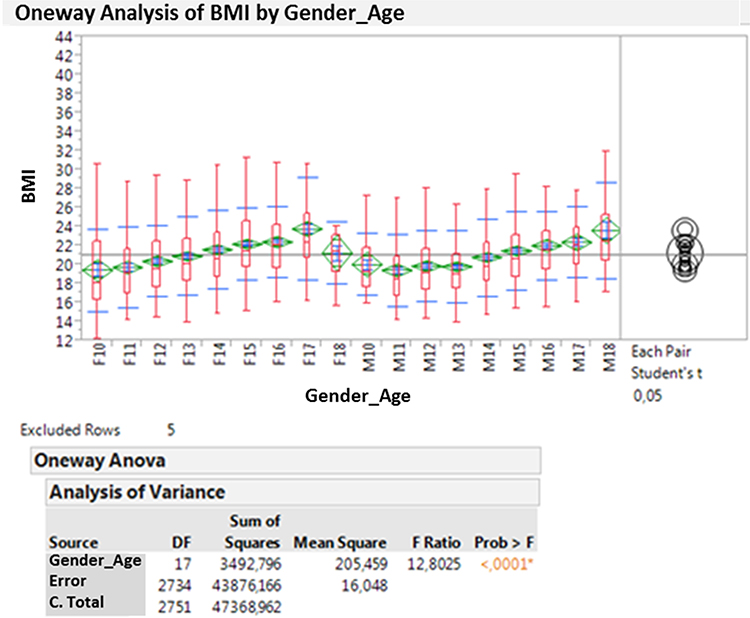 |
Figure 2 Differences between average BMIs with age group and gender of children and adolescents of Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, state of São Paulo, Brazil, from 2011 to 2012. *p<0.05, ANOVA one way. |
As shown in Table 1, 27.3% (752) of these children and adolescents were classified as being overweight/obese/severely obese. Thus, according to described methodology, they were called for the glycemic testing, and only 88 were present. We have verified that the FG and AD of these children and adolescents presented, respectively, averages close to 90 mg (Figure 3).
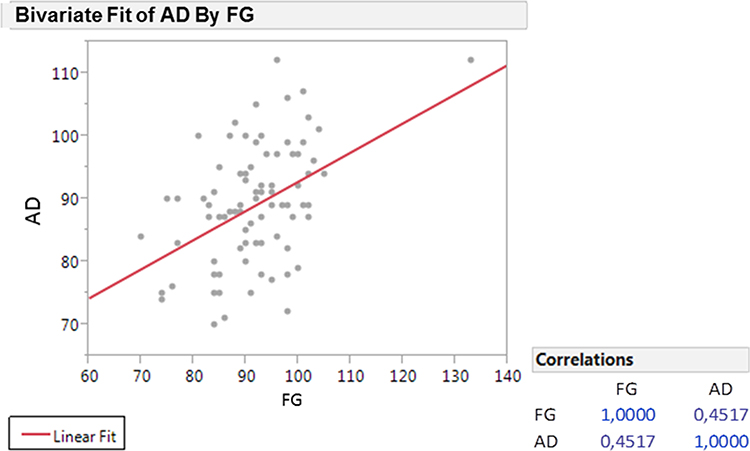 |
Figure 3 Correlation between fasting glucosemia (FG) and glucosemia 2 hours after 75 g of dextrose (AD) in 88 children and adolescents in Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, state of São Paulo, Brazil, from 2011 to 2012. 3= eutrophy; 4= overweight; 5= obese; 6= severely obese (WHO, 2007). |
Comparing the values of FG and AD performed in 88 (3.2%) children and adolescents, results are presented in Figure 3, a significant correlation between them was not noticed. The same was observed in relation to sex, that is, there was no statistical significance between sex and glucosemia, with an average of FG and AD of 92.8 mg/dL (male), 91.8 mg/dL (female) and 89.1 mg/dL (male) and 88.9 mg/dL (female), respectively.
The correlation between the nutritional percentile variables with fasting glucosemia (FG) and glucosemia 2 hours after 75 g of dextrose (AD) showed no statistical significance in both cases (Figure 4).
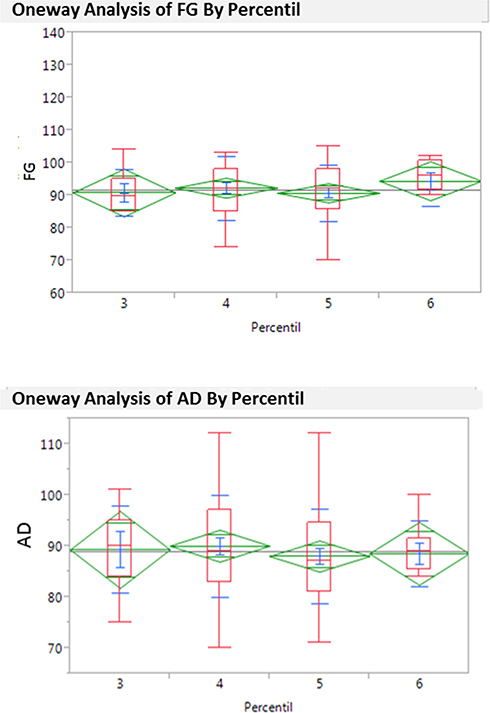 |
Figure 4 Average differences between fasting glucosemia (FG) and glucosemia 2 hours after 75 g of dextrose (AD) with nutritional percentiles of the 88 children and adolescents in Public State Schools of Fundamental and Medium Teaching in Santo André Municipality, state of São Paulo, Brazil, from 2011 to 2012. The blue lines represent the percentile and the green lines represent the variances. |
Discussion
According to our results, we did not find cases of DM2, and FG and AD studies did not produce significant results, although they showed lower values after glucose overload. This test was carried out during fasting, since the concentration of glucose in venous and capillary blood is similar during fasting and in AD samples it can be 20 to 25% more elevated in capillary blood.14 In this study we employed strips with reactive agents and capillary blood, and these data can be relevant in the analysis of our results, since AD could present results 20 to 25% lower.
Simultaneous dosimetry of glucose with capillary glucosemia determination may be employed to test the accuracy of the results of self-monitored blood glucose, although the preferential method to detectglucosemia is its determination in the plasma. The present study, besides its results relating to glucosemia, has also verified that about 27.3% of the studied children and adolescents were classified as overweight (17.9%), obese (8.0%) and severely obese (1.4%) (Table 1). The transition of normal glucose tolerance to glucose intolerance and from this to DM2 is associated with a significant increase in weight and this has an important effect on the glucosemia levels, independently from the changes in insulin sensitivity or in β-cells demand.15
The evolution to DM2 occurs along a variable period of time, passing through intermediate stages that are called impaired fasting glucose and impaired glucose tolerance. Such stages would be caused by a combination of resistance to insulin action and dysfunction of beta cells.12
Decreased glucose tolerance represents an abnormality in glucose regulation in post overload state diagnosed by AD, which includes the determination of FG. In this study, when comparing the values of FG and AD performed in 88 (3.2%) children and adolescents, represented in Figure 3, a significant correlation between them was not noticed. The same was observed in relation to sex, that is, there was no statistical significance between sex and glucosemia, with an average of FG and AD of 92.8 mg/dL (male), 91.8 mg/dL (female) and 89.1 mg/dL (male) and 88.9 mg/dL (female), respectively. Despite a total of 2757 students being included for the next stage, only 88 students agreed to participate, and children and adolescents depend on the authorization of their parents or tutors who have demonstrated deficient knowledge of familial chronic diseases such as obesity and its consequences, and risk of DM2.
Altered FG and decreased glucose tolerance are categories of augmented risk for the development of DM2. This way, hyperinsulinemia may compensate for insulin resistance, resulting in normal tolerance to glucose, but when insulin resistance exceeds the functional and adaptive capacity of β-cells, there is a deterioration of glucose intolerance, that may end in DM2.16
The deterioration of function of β-cells and insulin action start years before the diagnosis of diabetes, and usually chronic hyperglycemia is associated with deficient insulin secretion and insulin resistance.17 When a decompensation of β-cells function occurs, insulinemia is no longer a good parameter to estimate insulin resistance. We could define resistance to insulin (RI) as a state in which normal concentration of the hormone produces a subnormal biological response.17
In this study, since the averages being in the limits of normality of the dosages of capillary glucosemia, we have verified glucosemia above 99 mg/dL, and percentage during fasting with 18.2% and AD with 13.6%.
We know that maintained hyperinsulinemia inhibits either the secretion as the action of insulin and chronic hyperglycemia is able to inhibit either the secretion of insulin induced by glucose as the cellular sensitivity to insulin.18
We could assert that, up to the present moment, DM2 in young people is present in minority groups and the term epidemic should not be used. However, there is an epidemic obesity in infancy associated with pathologies such as hypertension, dyslipidemia and fatty liver disease that are more common than DM2. Obesity, especially the visceral kind, is one of the most important factors for the development of diabetes, through several mechanisms, as the increase of free circulating fatty acids, decrease of adiponectin and secretion of cytocins by the adipose tissue, as the of tumour necrosis factor alpha (TNF-α) and interleukin-6, that as a final analysis exacerbate insulin resistance.19
The elevated rate of obesity in children and adolescents are related to growing sedentariness and the changes in alimentary habits, usually with hypercaloric and hyperfatty diets.20
The possible factors that link obesity to metabolic changes of carbohydrates could be the increase of the free fatty acids, the inflammatory cytocines, and the low levels of adiponectin.
This situation may have occurred in children and adolescents studied here, mainly in the group classified as overweight, obese, and severely obese (Table 1).
In this study, we observed that 27.3% of the evaluated students were above normal weight, with an average age of 14 years; other authors have shown that, according to the average age of these youngsters, of approximately 13 years, that coincides with puberty, it is the period of relative insulin resistance, in which there is a decrease of approximately 30% of insulin action,21 and, in obesity, the presence of augmented levels of insulin during fasting and the exaggerated response of insulin to intravenous glucose,22 evolving to diagnosis of DM2.
It is important to note that this group corresponded to 27.3% of the studied population that was called to proceed to this investigation of this health condition through the glycemic tests. However, only a small number of children and adolescents attended (88 students) and, from these, several have shown altered glycemic test results, although without a significant relation with BMI. Although this group was not representative of the total sample of this study, it has allowed some thoughts, particularly in reference to the strategies adopted as to the prevention and control of weight gain in their youth. The partial compliance in this phase of our research suggests a low sensibility of their families. The role of schools in the control of infantile obesity has been analyzed in a search of the failure of their programs, since their intervention should occur in school environments, as incentive to sporting practises and healthy nutrition. However, the weight gain is maintained; for instance, it has been observed that the young American population gains more weight during summer vacation time and less during school time.23
Thus, we may assert that the familiar context shown be incorporated into the programs of alimentary education.
It is difficult to find, in greater populations, the incidence of DM2, since it involves periodic glucosemia examinations and follow-up for a few years. The incidence studies are usually restricted to DM1, since its initial manifestations tend to be quite characteristic.3
A recent study performed in a region in Spain did not find DM2 in young obese Caucasians. However, they found glucose intolerance in 9.6%, and insulin resistance in 13.5%, with a correlation of these two parameters with the severity of obesity, the presence of acantose nigricans, and cardiovascular risk.24
As to DM2, a condition in which the majority of the individuals also present with obesity, arterial hypertension and dyslipidemia, the interventions must include those multiple metabolic abnormalities, which, besides preventing the appearance of diabetes, also avoid cardiovascular illness, reducing mortality.25
According to authors,26 studies in adolescents with DM2 have evidenced the effect of diabetes and obesity over vascular complacence, in augmenting the rigidity of vessels, thus demonstrating that precocious DM2 may be more aggressive from a cardiovascular point of view than in adults.
In Brazil, DM2 studies in children and adolescents are still rare, and recently a group of 100 adolescents with familial cases of DM2 was evaluated, as well as other risk factors for developing the illness, and no case of DM2 was found.27
Effective prevention, primary and secondary, include more attention to health, and these may occur through the prevention of the onset of DM and acute and chronic complications, respectively.
The primary prevention program of DM2 is based on diet interventions and practicing of physical activities, aiming to fight the excess weight in individuals with major risk of developing diabetes, mainly those with impaired glucose tolerance.
The results of the Diabetes Prevention Program has shown a reduction of 58% in the incidence of cases of DM using the stimulus of healthy diet and exercise, and this intervention has become more effective with the use of Metformin.28
Diabetes education as a continuous process facilitating access to knowledge, must help the development of necessary abilities for self-care and control of diabetes by the individuals themselves and or family/care worker. The results become more effective if there is an available educational structure, and the different educational processes occur through a multi-professional team, working and preparing in an interdisciplinary way, in interaction, attention and involvement of diabetics and their care worker in all the events.29
Teamwork of an interprofessional team is essential, always considering the involvement of individuals in taking decisions.30
In this study, we have verified that altered BMI in young students (children) and adolescents is more prevalent among girls and older youngsters. We have also observed that approximately 30% of children and adolescents were overweight and obese with little reduction of glucosemia 2h after 75 g of dextrose evaluated by glycosimetry.
Declaration
This study was conducted in accordance with the Declaration of Helsinki.
Ethics Statement
The project was approved by the Research Ethics Committee of the Faculdade de Medicina do ABC (FMABC), São Paulo, Brazil, under the number 2012/000045689.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2004;27(Suppl 1):S5–S9. doi:10.2337/diacare.27.2007.S5
2. Rosenbloon AL, Arseanian S, Brink S, et al. Type 2 diabetes in children and adolescents. Diabetes Care. 2000;23(3):381–389.
3. Pinhas-Hamiel O, Zeitler P. The global spread of type 2 diabetes mellitus in children and adolescents. J Pediatr. 2005;146:693–700. doi:10.1016/j.jpeds.2004.12.042
4. Fagot-Campagna A, Pettitt DJ, Engeugau MM, Rios-Burrows N, Geiss LS, Valdez R. Type 2 diabetes among North American children and adolescents: an epidemiologic review and a public health perspective. J Pediatr. 2000;136(5):664–672. doi:10.1067/mpd.2000.105141
5. Goran MI, Davis J, Kelly L, et al. Low prevalence of pediatric type 2 diabetes. Where’s the epidemic? J Pediatr. 2008;152:753–755. doi:10.1016/j.jpeds.2008.02.004
6. Liese AD, D’Agostino RB
7. Pranita A, Phadke AV, Kharche JS, Balsubramaniyan B, Joshi AR. Screening of young adults for future risk of type 2 diabetes mellitus - a big concern for society & nation. J Clin Diagn Res. 2012;6(9):1610–1616. doi:10.7860/JCDR/2012/4442.2578
8. Fagot-Campagna A. Emergence of type 2 diabetes mellitus in children: the epidemiological evidence. J Pediatr Endocrinol Metab. 2000;13(6):1395–1402.
9. Brazilian Institute of Geography and Statistics. Family Budgets Research 2008–2009 - Anthropometry and Nutritional Status of Children, Adolescents and Adults in Brazil, Ministry of Planning, Budget and Management. Rio de Janeiro; 2010.
10. Soliman A, De Sanctis V, Elalaily R. Nutrition and pubertal development. Indian J Endocrinol Metab. 2014;Suppl 18:S39–S47.
11. World Health Organization (WHO). Growth reference data for 5–19 years; 2007. Available from: http://www.who.int/growthref/en/.
12. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36(Suppl 1):S11–S66. doi:10.2337/dc13-S011
13. Report of expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. 1997;20:1183–1197. doi:10.2337/diacare.20.7.1183
14. Sacks DB, Bruns DE, Goldstein DE, Maclaren NK, McDonals JM, Parrott M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Diabetes Care. 2003;25:750–786. doi:10.2337/diacare.25.4.750
15. Sinha R, Fisch G, Teague B, et al. Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med. 2002;346:802–810. doi:10.1056/NEJMoa012578
16. DeFronzo RA. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58:773–795. doi:10.2337/db09-9028
17. Ferrannini E. Insulin resistance versus insulin deficiency in non-insulin- dependent diabetes mellitus: problems and prospects. Endocr Rev. 1998;19:477–490. doi:10.1210/edrv.19.4.0336
18. Unger RH, Grundy S. Hyperglycaemia as an inducer as well as a consequence of impaired islet cell function and insulin resistance: implications for the management of diabetes. Diabetologia. 1985;28:119–125. doi:10.1007/BF00273856
19. Ravussin E, Smith SR. Increased fat intake, impaired fat oxidation, and failure of fat cell proliferation result in ectopic fat storage, insulin resistance, and type 2 diabetes mellitus. Ann N Y Acad Sci. 2002;967:363–367. doi:10.1111/j.1749-6632.2002.tb04292.x
20. Kitagawa T, Owada M, Urakami T, Yamauchi K. Increased incidence of non-insulin dependent diabetes mellitus among Japanese schoolchildren correlates with an increased intake of animal proteins and fat. Clin Pediatr. 1998;37:111–115. doi:10.1177/000992289803700208
21. Pinhas-Hamiel O, Standifort D, Hamiel D, Dolan LM. The type 2 family: a setting for development and treatment of adolescent type 2 diabetes mellitus. Arch Pediatr Adolesc Med. 1999;153:1063–1067. doi:10.1001/archpedi.153.10.1063
22. McCance DR, Pettitt DJ, Hanson RL, Jacobsson LT, Bennett PH, Knowler WC. Glucose insulin concentration and obesity in childhood and adolescence as predictors of NIDDM. Diabetologia. 1994;37(6):617–623. doi:10.1007/BF00403382
23. Wake M. The failure of anti-obesity programmes in schools. BMJ. 2018;360:507. doi:10.1136/bmj.k507
24. Aguayo A, Vela A, Aniel-Quiroga A, et al. Absence of diabetes mellitus type 2 in obese children and adolescents in the north of Spain. J Pediatr Endocrinol Metab. 2013;26(1–2):25–29. doi:10.1515/jpem-2012-0200
25. World Health Organization. The World Health Organization Report: Reducing Risks, Promoting Healthy Life. Geneve: WHO; 2002.
26. Gungor N, Thompson T, Sutton-Tyrrell K, Janosky J, Arslanian S. Early signs of cardiovascular disease in youth with obesity and type 2 diabetes. Diabetes Care. 2005;28(5):1219–1221. doi:10.2337/diacare.28.5.1219
27. Silva RCQ, Miranda WL, Chacra AR, Dib SA. Metabolic syndrome and insulin resistance in normal glucose tolerance Brazilian adolescents with family history of type 2 diabetes. Diabetes Care. 2005;28:716–718. doi:10.2337/diacare.28.3.716
28. Diabetes Prevention Program Research Group. Reduction of the incidence of type 2 diabetes with life style intervention or metformin. N Engl J Med. 2001;346(6):393–403.
29. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. 2010;33(Suppl 1):S89–S96. doi:10.2337/dc10-S089
30. Loveman E, Frampton GK, Clegg AJ. The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review. Health Technol. 2008;9:1–116.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.