")
Back to Journals » Journal of Asthma and Allergy » Volume 8
Profile of lebrikizumab and its potential in the treatment of asthma
Authors Maselli D, Keyt H, Rogers L
Received 11 March 2015
Accepted for publication 22 April 2015
Published 10 August 2015 Volume 2015:8 Pages 87—92
DOI https://doi.org/10.2147/JAA.S69932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Amrita Dosanjh
Diego Jose Maselli,1 Holly Keyt,1 Linda Rogers,2
1Department of Medicine, Division of Pulmonary Diseases and Critical Care, University of Texas Health Science Center at San Antonio, San Antonio, TX, 2Pulmonary, Critical Care, and Sleep Medicine Division, Mount Sinai-National Jewish Health Respiratory Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Abstract: Interleukin (IL)-13 has been associated with multiple inflammatory features of asthma. It affects multiple cellular lines in asthma and is a key mediator in airway hyperreactivity and remodeling. Periostin, an extracellular protein, has been used as a surrogate marker of IL-13 activity and has been linked to airway remodeling by inducing subepithelial fibrosis. Lebrikizumab is a humanized monoclonal antibody that targets IL-13. Studies have demonstrated promising results with lebrikizumab therapy in asthma with regard to pulmonary function and exacerbation rates, especially on those patients with surrogate markers of T helper cell type 2-driven inflammation (ie, elevated immunoglobulin E levels, eosinophil counts, periostin levels). Lebrikizumab appears to be a safe therapy, but there are ongoing studies evaluating its efficacy and safety profile. Other therapies that target IL-13 and the receptor of IL-4/IL-13 have been studied, but future studies are needed to determine their role in the treatment of asthma.
Keywords: asthma, severe asthma, lebrikizumab, IL-13, periostin
Introduction
Patients with refractory asthma account for approximately 5%–10% of all patients with asthma, but these experience significant impairment, poorer outcomes, and consume greater resources than mild-to-moderate asthmatics.1–3 For these reasons, novel asthma therapies are needed.
Phenotypic characterization of asthma patients has led to great advances in the “personalization” of treatment.4 With the aid of biomarkers, patients can receive targeted therapy, thus potentially yielding improved outcomes. An example of this approach is the use of omalizumab, a monoclonal antibody that targets immunoglobulin E (IgE). In patients with allergic asthma and IgE production against perennial allergens, omalizumab has been shown to decrease exacerbations, reduce steroid requirements, reduce hospitalizations, and improve quality of life.5,6 Mepolizumab, a humanized monoclonal antibody that targets interleukin (IL)-5, also has shown potential in improving asthma symptoms, exacerbation rates, and need for corticosteroids in asthmatics with an eosinophilic inflammatory profile.7,8 Despite some patients showing improved asthma outcomes, others fail to respond to these therapies, revealing a need for other options. IL-13 has been shown to be a central mediator in T helper cell type 2 (Th2) inflammatory response and has a prominent role in the pathophysiology of asthma.9,10 In this article, we review lebrikizumab, a monoclonal antibody targeting IL-13 and showing early promise for the treatment of asthma. Studies and reports were identified from the databases of PubMed/Medline and ClinicalTrials.gov from the US National Institutes of Health and the Cochrane Register of Controlled Trials. The search was performed using the combined keywords lebrikizumab or anti-IL-13 or IL-13 blockage or IL-13 antibody with asthma. No language or date restrictions were used.
IL-13
IL-13 has been linked to multiple inflammatory features of asthma. In the airways, IL-13 increases the migration and survival of eosinophils, activates macrophages, and increases the production of mucus by inducing goblet cell hyperplasia.11,12 With regard to immunoglobulin production, both IL-13 and the related cytokine IL-4 are key requirements for the class switch to IgE production by B cells.13 IL-13 has been associated with increased subepithelial collagen deposition through activation of fibroblasts.12 This process may be mediated by activation of IL-13Rα2 and induction of transforming growth factor-beta.14 Impact on these particular pathways suggests the potential for both anti-inflammatory and possible airway remodeling effects, making IL-13 an attractive cytokine to target for treatment of severe asthma.
Periostin
Periostin, previously known as osteoblast-specific factor 2, is an extracellular protein that is expressed in multiple cellular lines.15 Periostin expression is augmented during skeletal fracture or stress and our initial understanding of it was in relation to its role in bone development and remodeling. Comprehensive studies of IL-13-inducible genes in human bronchial epithelial cells found that periostin was highly expressed.16 In pulmonary fibroblasts and bronchial epithelial cells, its expression is also induced by IL-4 in a similar intensity to IL-13. The role of periostin has only been partially elucidated in asthma. It has been linked to airway subendothelial fibrosis through activation of transforming growth factor-beta as well as through activation of fibroblasts, leading to increased collagen deposition.17–19 It is a ligand for integrin receptors and supports adhesion and migration of epithelial cells.20 Immunohistochemical assays in subjects with asthma have demonstrated that periostin is concentrated in the epithelial basement membrane.21 Genome-wide profiling has confirmed the role of periostin as part of the Th2-driven inflammatory response in asthma.22,23
Periostin is a more stable surrogate of Th2 inflammation than IL-13, which is unstable and difficult to measure. Periostin likely moves easily from the affected tissues to the vessels. Additionally, basal levels are low, approximately 50 ng/mL, compared to other serum proteins; so, increased production may be easily detected.15 These unique properties make periostin a very attractive serum biomarker to study targeted therapies in patients with Th2-type inflammation, more specifically, to identify those with high IL-13 activity. Periostin is currently undergoing validation as a serum marker of Th2-driven inflammation in asthma.20,24
Lebrikizumab
Lebrikizumab is a humanized monoclonal antibody that targets IL-13. Studies of IL-13 performed in heterogeneous asthma populations have shown mixed results (Table 1). A study by Corren et al24 evaluated the use of lebrikizumab in uncontrolled asthmatics despite the use of inhaled corticosteroids (ICS). The study was a Phase II, double-blind, placebo-controlled trial that included 219 adults. All of the patients used ICS and the majority (80%) used a long-acting beta agonist (LABA). Before randomization, the patients were classified as having a high or low “Th2” status based on IgE levels and peripheral blood eosinophil counts. This grouping was performed to equally balance the surrogate markers of IL-13. The patients were then randomized using a dynamic scheme following a 1:1 ratio with regard to “Th2” status. Additionally, all patients had their baseline periostin level measured. The patients received 250 mg of lebrikizumab or placebo subcutaneously monthly for 6 months. At Week 12, the mean increase in forced expiratory volume in 1 second (FEV1) was 5.5% higher in the treatment group compared to that in the placebo group (9.8%±1.9% vs 4.3%±1.5%; P=0.02). In patients with a high periostin level, FEV1 was higher by 8.2% in the lebrikizumab group compared to the value in the placebo group (14.0%±3.1% vs 5.8%±2.1%; P=0.03). Patients with a low periostin level who received lebrikizumab had no significant improvement in FEV1. Between the two groups, there was no significant difference in quality of life or exacerbation rates. However, the high “Th2” subgroup of patients who received lebrikizumab had a 60% decrease in exacerbation rates compared to the placebo group. The patients who received lebrikizumab had a 19% mean decrease in fractional exhaled nitric oxide (FeNO) levels compared to an increase of 10% in the placebo group at the end of the study. Importantly, the improvement of FeNO levels was more pronounced in the high-periostin subgroup compared to the low-periostin subgroup (34% vs 4.3%, respectively). Patients with high FeNO levels also had greater improvement in lung function and fewer exacerbations.
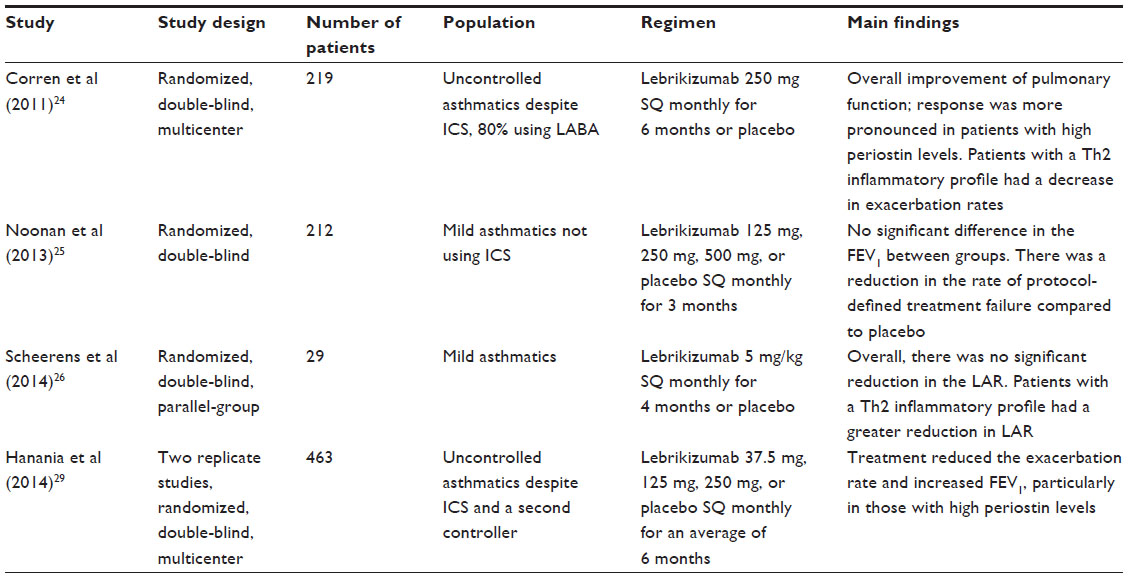 | Table 1 Studies of lebrikizumab in asthma |
This study has important implications. The FEV1 improvements were modest in patients who received lebrikizumab; however, a greater improvement was seen in those with surrogate markers of Th2-driven inflammation. The study suggests that eosinophil counts, IgE levels, FeNO, and periostin could potentially be used to predict which patients would benefit from treatment with lebrikizumab. Additionally, the effects on FEV1 were seen relatively early in the course of treatment, suggesting that the inhibition of IL-13 has a rapid effect.
Noonan et al25 tested lebrikizumab in mild asthmatics in a Phase II, randomized, placebo-controlled, double-blind study. Lebrikizumab in three different doses (125 mg, 250 mg, or 500 mg administered subcutaneously) or placebo were given monthly for 3 months to 212 patients with asthma not using ICS. The primary efficacy end point was the relative change in FEV1. The investigators found no significant difference, either statistically or clinically, in FEV1 among the groups. However, the lebrikizumab treatment groups had a reduction in the rate of protocol-defined treatment failure compared to the placebo group. Moreover, the treatment groups had a reduction in FeNO levels, suggesting positive effect. Despite these encouraging observations, the primary efficacy end point findings are not consistent with the study by Corren et al,24 suggesting that the severity of asthma, and possibly steroid resistance, may influence the response to lebrikizumab.
Another study recently explored the efficacy of lebrikizumab in patients with mild asthma who underwent airway allergen challenge.26 This technique consists of administering doubling doses of a standardized extract of an allergen to which the patients previously had a positive skin response. The dose of the extract that induced a ≥20% reduction in FEV1 in the early asthmatic response (5–30 minutes) is recorded. During the second part of the airway challenge, the dose previously recorded is readministered at a later time point (typically weeks) to test a therapy for asthma. The responses to the allergen challenge before and after a therapy being evaluated for asthma are then compared. Airway allergen challenge testing has limitations, as it may be influenced by infections, exposure to other allergens, and the inherent variability of FEV1 in asthmatics, but it has been validated to evaluate effects of treatments in asthma.27,28 The study evaluating lebrikizumab was a Phase II, randomized, double-blind, parallel-group study that included 29 subjects.26 Patients who received lebrikizumab had a reduction of 48% in the late asthmatic response (LAR) at Week 13, defined as the area under the curve of FEV1 measured 2–8 hours following an inhaled allergen challenge compared to the placebo group. Although this finding was not statistically significant, the investigators noted that patients treated with lebrikizumab with elevated eosinophil counts, elevated IgE, or high periostin levels had a greater reduction in LAR compared to those with low levels of these biomarkers. These results are in line with the study by Corren et al24 demonstrating that patients with asthma and a Th2 inflammatory profile are more likely to respond to this therapy.
Similarly, preliminary results reported by the investigators of the VERSE and LUTE trials demonstrated that lebrikizumab has greater effect in patients with high IL-13 activity.29 These two replicate studies were performed in a multicenter, double-blind, randomized fashion in uncontrolled asthmatics despite therapy with ICS and a second controller. The combined studies compared placebo to varying doses of lebrikizumab (37.5 mg, 125 mg, or 250 mg) in 463 patients at a ratio of 1:1:1:1. Compared to the placebo group, patients receiving lebrikizumab had greater improvement in FEV1 and lower exacerbation rates, but the effect was most pronounced in those with high periostin levels.
Why is lebrikizumab not effective in all patients? Asthma is a heterogeneous disease where the Th2 phenotype is only one major pathway involved in pathogenesis. This is one of the major drawbacks of biologics-based therapies; they target a very specific cytokine/component of the inflammatory cascade in asthma. It is clear that many other cytokines and inflammatory pathways other than those mediated by IL-13 are involved in allergic and other forms of asthma. Further, compliance and cost may be prohibitive for some patients. In the case of lebrikizumab, the IL-13 pathway may be only partially activated or not activated at all in mild asthmatics, potentially explaining the lack of response in this subset of patients.25 Steroid resistance may also play a role in patients with inadequately controlled asthma despite ICS therapy, with the IL-13 pathway not completely inhibited. Therefore, it is plausible that in these steroid-insensitive patients, the blockage of IL-13 may be substantially more beneficial.24 Which patients would potentially benefit clinically from lebrikizumab based on the available data? This medication has not been approved for clinical use yet, but patients who theoretically would benefit could be those who have uncontrolled asthma despite ICS and LABA use and with a Th2-driven inflammatory pattern, as determined by biomarkers (ie, high levels of periostin, eosinophils, FeNO, and/or IgE).24–26,29
Safety
Lebrikizumab appears to be a safe therapy.24–26,29 The reported rates of adverse reactions are similar compared to placebo, with the exception of an increase in the incidence of musculoskeletal events.24 Potential adverse effects of biologics in general include injection site reactions, hypersensitivity reactions, infection, and malignancy. Although there has been no safety signal suggesting increased rates of these outcomes associated with lebirkizumab treatment in published data to date, studies of efficacy and safety are currently ongoing.
Other IL-13 inhibitors
Tralokinumab is a humanized monoclonal antibody that targets IL-13.30,31 This agent was evaluated in a Phase-II, double-blind, placebo-controlled, randomized study that included 194 moderate-to-severe uncontrolled asthmatics.32 This Phase II study found modest improvement in lung function and a reduction in beta agonist use, and a Phase III development program for tralokinumab in asthma is currently under way. IL-13 has also been identified as a key inflammatory cytokine in ulcerative colitis (UC).33 A study using tralokinumab in patients with UC failed to show an improvement in clinical response, but there was evidence of superior remission rates.34 Future studies on the applications of tralokinumab on asthma and UC are needed.
Anrukinzumab, a monoclonal antibody to IL-13, blocks the interaction of IL-13 with the IL-4α receptor, thus halting the IL-13-driven inflammatory response.35,36 Preliminary pharmacokinetic studies have been performed in patients with asthma and UC, and further studies of safety and efficacy are currently ongoing.37
GSK679586, a humanized monoclonal antibody that inhibits IL-13 activity by targeting the α1 and α2 subunits of the IL-13 receptors, has been studied in severe asthma.38 In a study of 237 patients with asthma refractory to maximal doses of ICS, no differences in Asthma Control Questionnaire symptom scores, FEV1, or exacerbation rates were seen in GSK679586-treated subjects vs placebo. A subgroup analysis did not detect differences in outcomes in patients with high eosinophil counts or IgE levels. Periostin was not measured as an indicator of IL-13 activity in these studies. A lack of improved asthma outcomes with GSK679586 compared with other inhibitors of IL-13 may be related to differences in potency, blunting of identification of effect in the presence of other treatments, high IL-4 activity, or other unknown mechanisms.
IL-4/IL-13 inhibitors
Early attempts to develop cytokine therapies for asthma focused on antagonizing key Th2 cytokines such as IL-4 by blocking the cytokine directly or by blocking its receptor. Although initial preclinical studies of anti-IL4 therapies seemed promising, subsequent human studies surprisingly were unsuccessful.39,40 More recently, dupilumab, a fully human monoclonal antibody to the alpha subunit of the IL-4 receptor and that blocks the effects of both IL-4 and IL-13, is under investigation for treatment of Th2 inflammatory disease, including atopic dermatitis and asthma.41,42 In a unique study design, patients with moderate-to-severe asthma and either peripheral blood eosinophil count of ≥300 cells/μL or at least 3% sputum eosinophils were randomized to dupilimab or placebo (n=52 in each group).41 Participants then underwent structured tapering of their standard controllers, first with discontinuation of their LABA and then stepwise reduction of their ICS. The primary end point of asthma exacerbation was observed in three patients treated with dupilumab (6%) vs 23 receiving placebo (44%), an 87% reduction in exacerbations over the 12-week treatment period (odds ratio: 0.08; 95% confidence interval: 0.02–0.28; P<0.001). Although these results appear dramatic, only 20% of patients screened for the study were eligible based on the criteria for eosinophilic asthma; thus, the efficacy may only apply to a limited population of patients. Moreover, at least during the brief run-in period, there was no difference in exacerbation rates prior to standard therapy withdrawal. The treatment withdrawal design, while excellent for proof of concept of efficacy, did not demonstrate efficacy of the drug as it would likely be used, as an add-on treatment for those not controlled on standard therapies. Another dual IL-4/IL-13 antagonist, Pitrakinra, has been investigated as both a subcutaneous and inhaled treatment. It has been shown to diminish both the early and late allergic responses and reduce exacerbations of eosinophilic asthma, but it did not show efficacy in a general population of patients with asthma.43,44
Future directions
There is great interest in the potential benefits of lebrikizumab in the treatment of patients with asthma not controlled with the currently available therapies. There are two ongoing placebo-controlled studies that will explore the efficacy of lebrikizumab despite daily treatment with ICS therapy and at least one additional controller medication in two different asthma populations (NCT01868061, NCT01875003). Another study will compare lebrikizumab vs placebo vs montelukast (1:1:1 ratio) for the therapy of mild-to-moderate asthmatics who are receiving treatment with short-acting beta-agonist alone (NCT02104674). Lastly, an ongoing study will evaluate the use of lebrikizumab in patients with severe asthma who depend on daily corticosteroid therapy (NCT01987492).
Conclusion
Although there are promising results with IL-13 inhibitors in asthma, it is important to put these therapies in perspective. Patients with severe asthma should be always adequately assessed for asthma-mimicking diseases and treated for asthma-aggravating conditions before moving unnecessarily to expensive biologics-based therapies, especially in the primary care setting were these might not be available. Additionally, asthma education, trigger avoidance, and medication compliance should be addressed thoroughly. Despite these measures, a significant subset of patients with asthma are either not controlled with high-dose ICS and LABA or require chronic oral steroids for disease control, putting them at risk of significant long-term adverse health effects. Although patients with asthma and Th2 inflammation who are uncontrolled with current standard treatments represent a small segment of the total population of patients with asthma, as one of the most common chronic conditions, a large population of patients who are significantly impaired or are experiencing adverse effects of systemic steroids stand to potentially benefit from anti-IL13 if ongoing studies provide further support of safety and efficacy.
Disclosure
The authors report no conflicts of interest in this work.
References
To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12:204. | |
Sadatsafavi M, Rousseau R, Chen W, Zhang W, Lynd L, FitzGerald JM. The preventable burden of productivity loss due to suboptimal asthma control: a population-based study. Chest. 2014;145(4):787–793. | |
Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–373. | |
Lin TY, Poon AH, Hamid Q. Asthma phenotypes and endotypes. Curr Opin Pulm Med. 2013;19(1):18–23. | |
Humbert M, Busse W, Hanania NA, et al. Omalizumab in asthma: an update on recent developments. J Allergy Clin Immunol Pract. 2014; 2(5):525. e–536. e. | |
Bousquet J, Cabrera P, Berkman N, et al. The effect of treatment with omalizumab, an anti-IgE antibody, on asthma exacerbations and emergency medical visits in patients with severe persistent asthma. Allergy. 2005;60(3):302–308. | |
Bel EH, Wenzel SE, Thompson PJ, et al; SIRIUS Investigators. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014;371(13):1189–1197. | |
Ortega HG, Liu MC, Pavord ID, et al; MENSA Investigators. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. | |
Wills-Karp M, Luyimbazi J, Xu X, et al. Interleukin- 13: central mediator of allergic asthma. Science. 1998;282:2258–2261. | |
Grünig G, Warnock M, Wakil AE, et al. Requirement for IL-13 independently of IL-4 in experimental asthma. Science. 1998;282(5397):2261–2263. | |
Brandt EB, Zimmermann N, Muntel EE, et al. The alpha4bbeta7-integrin is dynamically expressed on murine eosinophils and involved in eosinophil trafficking to the intestine. Clin Exp Allergy. 2006;36(4):543–553. | |
Zhu Z, Homer RJ, Wang Z, et al. Pulmonary expression of interleukin-13 causes inflammation, mucus hypersecretion, subepithelial fibrosis, physiologic abnormalities, and eotaxin production. J Clin Invest. 1999; 103(6):779–788. | |
Van der Pouw Kraan TC, Van der Zee JS, Boeije LC, De Groot ER, Stapel SO, Aarden LA. The role of IL-13 in IgE synthesis by allergic asthma patients. Clin Exp Immunol. 1998;111(1):129–135. | |
Fichtner-Feigl S, Strober W, Kawakami K, Puri RK, Kitani A. IL-13 signaling through the IL-13alpha2 receptor is involved in induction of TGF-beta1 production and fibrosis. Nat Med. 2006;12(1):99–106. | |
Izuhara K, Arima K, Ohta S, Suzuki S, Inamitsu M, Yamamoto K. Periostin in allergic inflammation. Allergol Int. 2014;63(2):143–151. | |
Yuyama N, Davies DE, Akaiwa M, et al. Analysis of novel disease-related genes in bronchial asthma. Cytokine. 2002;19(6):287–296. | |
Norris RA, Damon B, Mironov V, et al. Periostin regulates collagen fibrillogenesis and the biomechanical properties of connective tissues. J Cell Biochem. 2007;101(3):695–711. | |
Sidhu SS, Yuan S, Innes AL, et al. Roles of epithelial cell-derived periostin in TGF-beta activation, collagen production, and collagen gel elasticity in asthma. Proc Natl Acad Sci U S A. 2010;107(32):14170–14175. | |
Parulekar AD, Atik MA, Hanania NA. Periostin, a novel biomarker of TH2-driven asthma. Curr Opin Pulm Med. 2014;20(1):60–65. | |
Jia G, Erickson RW, Choy DF, et al. Periostin is a systemic biomarker of eosinophilic airway inflammation in asthmatic patients. J Allergy Clin Immunol. 2012;130(3):647–654.e10. | |
Takayama G, Arima K, Kanaji T, et al. Periostin: a novel component of subepithelial fibrosis of bronchial asthma downstream of IL-4 and IL-13 signals. J Allergy Clin Immunol. 2006;118(1):98–104. | |
Woodruff PG, Boushey HA, Dolganov GM, et al. Genome-wide profiling identifies epithelial cell genes associated with asthma and with treatment response to corticosteroids. Proc Natl Acad Sci U S A. 2007;104(40):15858–15863. | |
Woodruff PG, Modrek B, Choy DF, et al. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am J Respir Crit Care Med. 2009;180(5):388–395. | |
Corren J, Lemanske RF, Hanania NA, et al. Lebrikizumab treatment in adults with asthma. N Engl J Med. 2011;365(12):1088–1098. | |
Noonan M, Korenblat P, Mosesova S, et al. Dose-ranging study of lebrikizumab in asthmatic patients not receiving inhaled steroids. J Allergy Clin Immunol. 2013;132(3):567. e–574. e. | |
Scheerens H, Arron JR, Zheng Y, et al. The effects of lebrikizumab in patients with mild asthma following whole lung allergen challenge. Clin Exp Allergy. 2014;44(1):38–46. | |
Inman MD, Watson R, Cockcroft DW, Wong BJ, Hargreave FE, O’Byrne PM. Reproducibility of allergen-induced early and late asthmatic responses. J Allergy Clin Immunol. 1995;95(6):1191–1195. | |
Gauvreau GM, Watson RM, Rerecich TJ, et al. Repeatability of allergen-induced airway inflammation. J Allergy Clin Immunol. 1999;104(1):66–71. | |
Hanania NA, Noonan MJ, Corren J, et al. Efficacy and safety of lebrikizumab in severe uncontrolled asthma: results from the lute and verse phase II randomized, double-blind, placebo-controlled trials. J Allergy Clin Immunol. 2014;133(2):AB402. | |
Blanchard C, Mishra A, Saito-Akei H, Monk P, Anderson I, Rothenberg ME. Inhibition of human interleukin-13-induced respiratory and oesophageal inflammation by anti-human-interleukin-13 antibody (CAT-354). Clin Exp Allergy. 2005;35(8):1096–1103. | |
May RD, Monk PD, Cohen ES, et al. Preclinical development of CAT-354, an IL-13 neutralizing antibody, for the treatment of severe uncontrolled asthma. Br J Pharmacol. 2012;166(1):177–193. | |
Piper E, Brightling C, Niven R, et al. A phase II placebo-controlled study of tralokinumab in moderate-to-severe asthma. Eur Respir J. 2013;41(2):330–338. | |
Jovani M, Fiorino G, Danese S. Anti-IL-13 in inflammatory bowel disease: from the bench to the bedside. Curr Drug Targets. 2013;14(12):1444–1452. | |
Danese S, Rudzinski J, Brandt W, et al. Tralokinumab for moderate-to-severe UC: a randomised, double-blind, placebo-controlled, phase IIa study. Gut. 2015;64(2):243–249. | |
Kasaian MT, Tan XY, Jin M, et al. Interleukin-13 neutralization by two distinct receptor blocking mechanisms reduces immunoglobulin E responses and lung inflammation in cynomolgus monkeys. J Pharmacol Exp Ther. 2008;325(3):882–892. | |
Hua F, Ribbing J, Reinisch W, Cataldi F, Martin S. A pharmacokinetic comparison of Anrukinzumab, an anti- IL-13 monoclonal antibody, among healthy volunteers, asthma and ulcerative colitis patients. Br J Clin Pharmacol. Epub 2015 Jan 22. | |
Reinisch W, Panés J, Khurana S, et al. Anrukinzumab, an anti-interleukin 13 monoclonal antibody, in active UC: efficacy and safety from a phase IIa randomised multicentre study. Gut. 2015;64(6):894–900. | |
De Boever EH, Ashman C, Cahn AP, et al. Efficacy and safety of an anti-IL-13 mAb in patients with severe asthma: a randomized trial. J Allergy Clin Immunol. 2014;133(4):989–996. | |
Steinke JW. Anti-interleukin-4 therapy. Immunol Allergy Clin North Am. 2004;24(4):599–614. | |
Hart TK, Blackburn MN, Brigham-Burke M, et al. Preclinical efficacy and safety of pascolizumab (SB 240683): a humanized anti-interleukin-4 antibody with therapeutic potential in asthma. Clin Exp Immunol. 2002;130(1):93–100. | |
Wenzel S, Ford L, Pearlman D, et al. Dupilumab in persistent asthma with elevated eosinophil levels. N Engl J Med. 2013;368(26):2455–2466. | |
Beck LA, Thaçi D, Hamilton JD, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Engl J Med. 2014; 371(2):130–139. | |
Wenzel S, Wilbraham D, Fuller R, Getz EB, Longphre M. Effect of an interleukin-4 variant on late phase asthmatic response to allergen challenge in asthmatic patients: results of two phase 2a studies. Lancet. 2007;370(9596):1422–1431. | |
Slager RE, Otulana BA, Hawkins GA, et al. IL-4 receptor polymorphisms predict reduction in asthma exacerbations during response to anti-IL-4 receptor a antagonist. J Allergy Clin Immunol. 2012;130(2):516–522. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.