")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Profile of inhaled levodopa and its potential in the treatment of Parkinson’s disease: evidence to date
Authors Patel AB, Jimenez-Shahed J
Received 18 May 2018
Accepted for publication 20 September 2018
Published 2 November 2018 Volume 2018:14 Pages 2955—2964
DOI https://doi.org/10.2147/NDT.S147633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Ami B Patel, Joohi Jimenez-Shahed
Department of Neurology, Baylor College of Medicine, Houston, TX, USA
Abstract: Inhaled levodopa is a newly emerging therapeutic option in the treatment of “off” symptoms associated with Parkinson’s disease (PD). Its mode of delivery offers more rapid absorption of levodopa and shorter onset of clinical benefit compared to oral formulations, and has been shown to be feasible for use in patients with PD experiencing worse motor function due to declining plasma levodopa levels. Clinical development of this compound is supported by preclinical, Phase I–III, long-term-safety studies and studies in special populations, including otherwise-healthy asthmatics and smokers. These investigations demonstrated that the drug is well tolerated without risk of long-term (up to 1 year) changes in pulmonary function or spirometry measures. The most common side effects among PD patients were a mild cough, upper respiratory tract infection, nausea, sputum discoloration, and dyskinesia. Inhaled levodopa offers a different administration method and side-effect profile from the currently available options for rescue therapy for Off periods in PD, though comparative studies have not been performed. The drug is presently under review by the US Food and Drug Administration.
Keywords: levodopa, dry-powder inhalation, motor fluctuations, dyskinesia, spirometry
Introduction
Parkinson’s disease (PD) is a neurodegenerative disorder characterized by three principal motor features – resting tremor, rigidity, and bradykinesia – though others may exist.1 A major pathophysiological mechanism for motor symptoms in PD is preferential neurodegeneration in the nigrostriatal dopaminergic pathways involved in movement.2 Levodopa, an amino acid that serves as the immediate precursor for catecholamines, can cross the blood–brain barrier and become decarboxylated to dopamine, in order to interact with the denervated nigrostriatal neural networks.3 Modulation of dopaminergic circuitry with levodopa has been the gold standard of treatment since its introduction in the 1960s.
The treatment of PD with levodopa can be associated with both short-term side effects and long-term complications. Short-term side effects of levodopa can include nausea, hypotension, and hallucinations, while long-term complications can include motor fluctuations and dyskinesias.4 Some of the short-term side effects can be managed by coadministration of a peripheral decarboxylase inhibitor, such as carbidopa or benserazide, which also serves to increase the amount of levodopa available to pass into the central nervous system.5 If nausea persists, nonsedating antiemetics, such as domperidone, can be used.6 On the other hand, management of long-term complications is more complex. The term “motor fluctuations” refers to the “On” and “Off” times that PD patients experience, describing the periods of relatively good and poor motor functions, respectively, which also correlate with higher and lower levodopa concentrations in the periphery. Dyskinesias, on the other hand, are involuntary movements that frequently occur during On times at the peak plasma concentration (Cmax) of levodopa, and can be described as choreic (ie, abnormal unpatterned body movements) or dystonic (ie, patterned muscle contractions causing more sustained abnormal posture).7 Less commonly, dyskinesias can occur in a diphasic pattern, when medications begin to wear in or wear off. Regardless, for some individuals, these can become more disabling than their primary motor symptoms. 50%–60% of levodopa-naïve patients will develop motor complications within 3–4 years after initiating levodopa therapy.8 In a study of levodopa in patients with early PD,9 PD signs were most diminished with the highest daily levodopa dose (600 mg), but this was associated with the greatest incidence of dyskinesias and motor fluctuations.
Improving the constancy of levodopa drug delivery is a principal strategy to address motor complications of PD,10 in order to approximate continuous dopamine stimulation within the central nervous system.11 Difficulty in achieving this is related to several factors. Levodopa itself has a short half-life (t½=0.7–1.4 hours), and time to Cmax (Tmax) is 15–60 minutes in the fasting state, despite coadministration with peripheral decarboxylase inhibitors.12 Other factors that contribute to the pharmacokinetic variability of levodopa include delayed gastric emptying (which occurs as a common nonmotor feature of PD), competition with dietary proteins for active transport across the gut wall into the bloodstream, and competition for transport across the blood–brain barrier.3 Lastly, the nonphysiological nature of dopaminergic signaling following levodopa administration is thought to underlie the predisposition for development of motor complications in PD by desensitizing postsynaptic receptors.13 Several adjunctive strategies must thus eventually be used alongside levodopa to help mitigate the development or impact of motor complications.3 These include the use of dopamine agonists with longer half-lives than levodopa, injectable short-acting dopamine agonists (eg, apomorphine) for rescue therapy during Off times, use of a catechol-O-methyltransferase inhibitor to prevent levodopa metabolism in the periphery and levodopa and dopamine metabolism in the central nervous system (thereby reducing Off time), use of monoamine oxidase type B inhibitors to prevent metabolism of dopamine in the central nervous system (thereby extending On times), or addition of amantadine, the only antidyskinetic agent currently approved in the US.
Despite these strategies, levodopa remains the most effective therapy for managing PD symptoms, and both novel oral and nonoral systems have and are being developed to deliver this therapy with optimized pharmacokinetics. In this review, we place a novel dry-powder aerosol self-administered inhaled levodopa formulation, CVT301 (Acorda Therapeutics, Ardsley, NY, USA), in the clinical context of other levodopa formulations currently available or in development, describe its clinical development program, efficacy, and safety, and discuss its potential role in the treatment of PD.
Currently available and developing levodopa formulations
Large and inconsistent fluctuations in plasma concentrations cause difficulty with the long-term management of PD patients with conventional levodopa formulations.3 Although extended-release formulations are available, they do not completely eliminate the unfavorable pharmacokinetics of regular carbidopa/levodopa (C/L; Table 1) or benserazide/levodopa (B/L). Although each levodopa formulation that is currently available has potential advantages over regular C/L or B/L, newer formulations in development may offer alternatives that can further compensate for the various difficulties with oral levodopa delivery to the central nervous system, thereby presumably enhancing the likelihood of more continuous dopaminergic stimulation (Table 2).3 The treating clinician will need to determine the best treatment strategies for his/her individual PD patient without the assistance of data providing comparative efficacy and/or cost-effectiveness and may need to rely more heavily on ease of access, practicality of use, or patient preferences. Furthermore, despite these varied options and developments in levodopa delivery to optimize On periods, any intermittently administered levodopa formulation, including inhaled levodopa, is likely to continue to be complicated by the presence of motor fluctuations and dose-limiting dyskinesias, highlighting the continued need for alternate therapies.
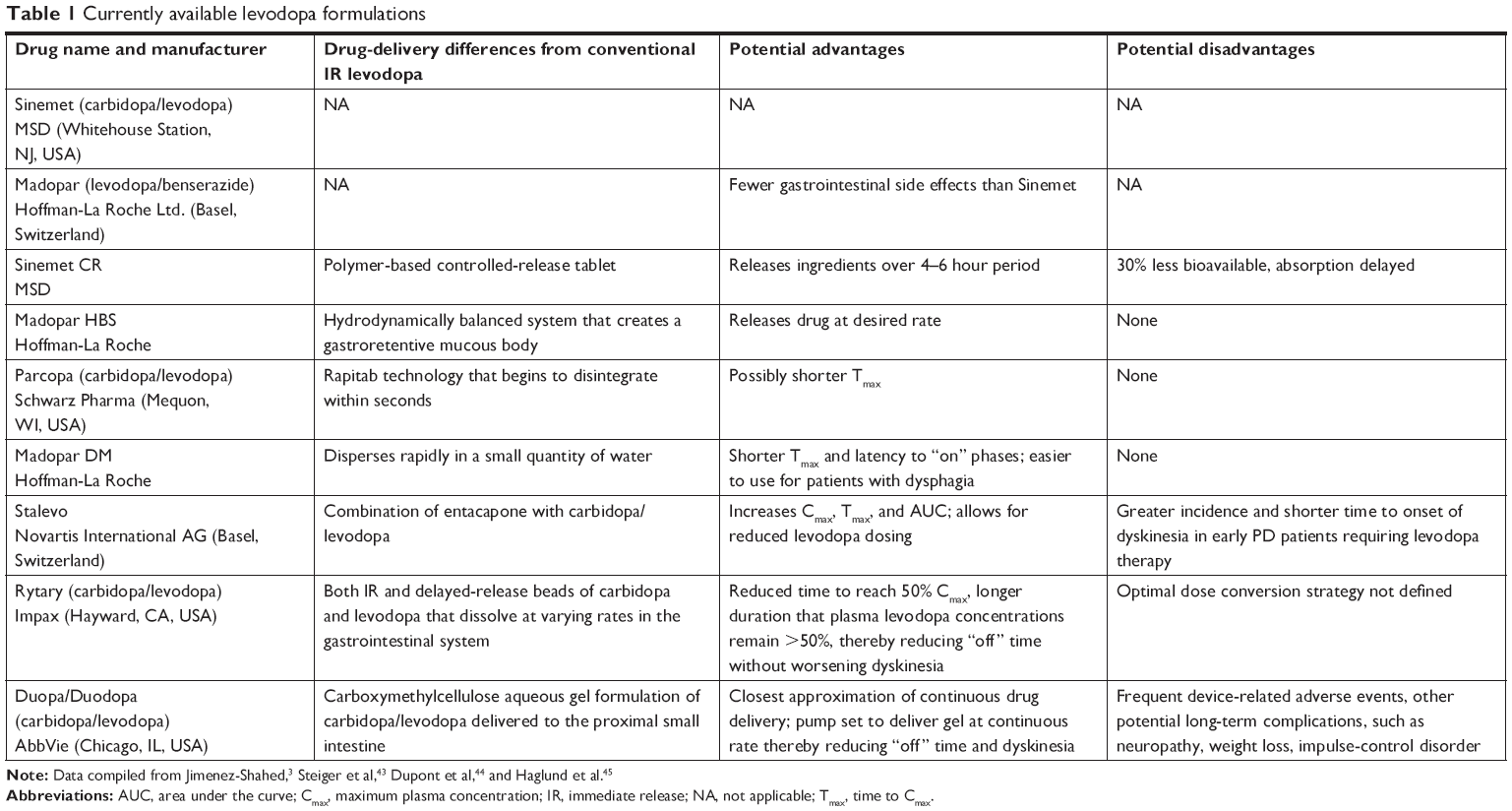 | Table 1 Currently available levodopa formulations |
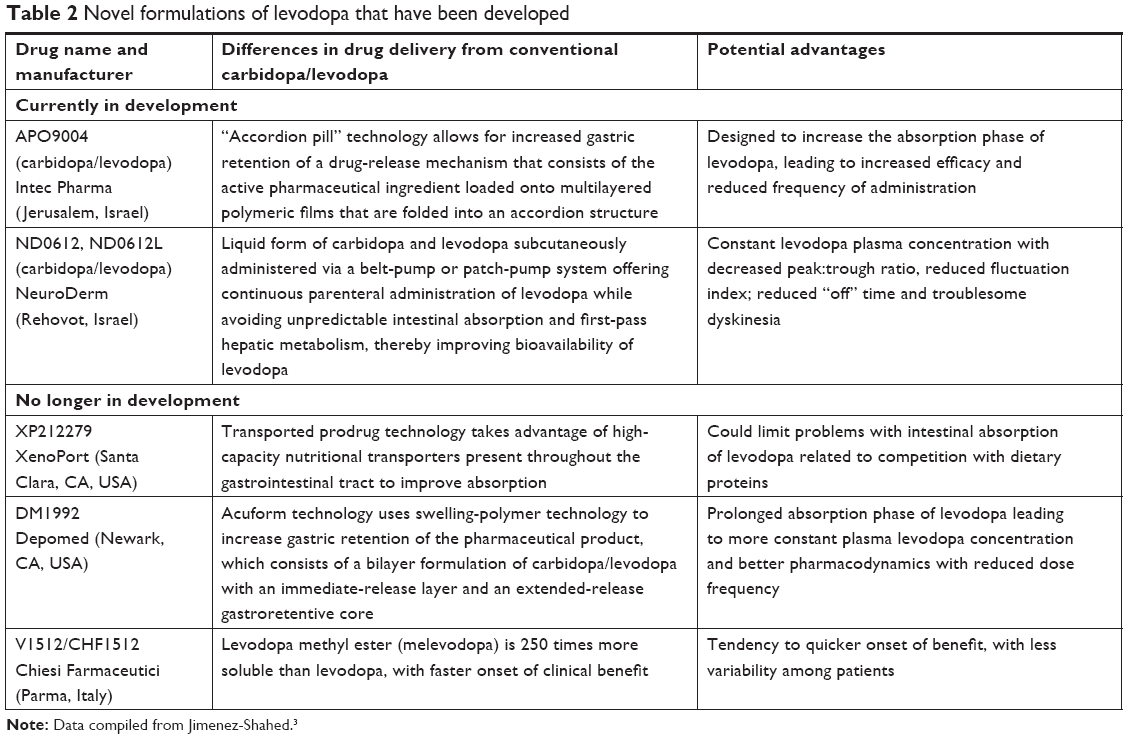 | Table 2 Novel formulations of levodopa that have been developed |
Inhaled levodopa (CVT301) preclinical and clinical development
Formulation of CVT301
CVT301 is an inhaled dry-powder formulation of levodopa that has been investigated for use in treating the Off episodes of PD. The drug was developed with the goal of producing rapid, consistent increases in circulating drug concentrations associated with a rapid clinical response.14 Levodopa is formulated into a large, porous particle complex with low density whose excipients (10%) form an aerodynamic structure and are biocompatible.15 These large particles can aerosolize from a dry-powder inhaler more efficiently and can avoid phagocytic clearance from the lungs. Use of large porous particles allows the levodopa molecules to be delivered to the alveolar membranes, where they can be readily absorbed to the pulmonary capillary network and thus into the arterial circulation and quickly to the brain via the aorta and carotid arteries, thereby avoiding the delays associated with enteral administration.16 The initial delivery method employed a novel pulmonary delivery technology (Advanced Inhalation Research; Alkermes, Cambridge, MA, USA) combined with an inhalation device.17 Use of standard inhalation devices limit the quantity of drug that can be delivered. However, CVT301 uses Arcus technology, developed by Alkermes and Civitas Therapeutics (Chelsea, MA, USA) and currently held by Acorda Therapeutics, which is a proprietary capsule-based, breath-actuated passive dry-powder inhaler that allows larger medication doses to be carried to the lungs. The fine-particle dose (FPD) is the quantity of levodopa estimated to reach the lungs, which may differ from the stated milligram content of the inhalation capsule. Although other dry-powder inhalers exist,18 with the Arcus inhaler, patients may self-administer the medication simply by breathing in, avoiding the need for coordination between inhalation and pump.19
Preclinical
Preclinical results using aerosolized formulations of levodopa were first reported by Bartus et al using the 6-hydroxydopamine rat model of PD.16 Animals were pretreated with an intraperitoneal injection of carbidopa and then received oral or inhaled levodopa at various doses in a randomized order. Clinical and pharmacokinetic testing was performed 15, 30, 60, and 120 minutes after administration. In each case, oral levodopa administration was associated with longer Tmax than inhaled levodopa administration. Cmax was achieved 15–20 minutes after administration and decreased gradually over 1–2 hours. Following inhaled administration, Tmax was reached at 2 minutes and decreased within 15 minutes, though levodopa could still be measured for over 120 minutes. Clinical effects in these rats were observed within 10 minutes, with peak benefits observed within 5–30 minutes. Analysis of dosing equivalency revealed a tenfold difference in the dose of drug required to produce equivalent peak efficacy. Qualitative examination of the lung tissue by a trained pathologist revealed no histological abnormalities.
Lipp et al also reported another preclinical study of CVT301 in beagles with similar results.14 Six beagles received inhaled CVT301 (3.8±0.4 mg/kg) and single doses of levodopa orally (10.6±0.9 mg/kg). Pulmonary delivery resulted in more rapid and less variable absorption, with Tmax at 2.5 minutes and a gradual decline starting within 5 minutes and continuing through 2 hours. By contrast, following oral delivery, Tmax was 30–120 minutes, with a mean of 30 minutes. Together, these preclinical studies provided the rationale for the first-in-human pharmacokinetic studies of CVT301.
Phase I
A Phase I study examined the safety and pharmacokinetics of inhaled CVT301 levodopa compared to oral levodopa in healthy humans.14,20 This study included 18 healthy male volunteers (17 Caucasian) aged 30–65 years. Inclusion criteria required subjects to have an FEV1 ≥80% based on age, sex, race, and height with FEV1:FVC ratio of ≥70%, and inspiratory flow rate of ≥45 L/min. Each volunteer received three open-label study-drug doses on different days at least 2 days apart. The subjects first received a single dose of oral C/L (25/100 mg), followed by a second and third dose of inhaled CVT301. They were randomized between one of two groups of doses, with nine participants receiving 10 and 30 mg CVT301 and the remaining nine participants 20 and 50 mg of CVT301. During each CVT dose, all subjects also took 50 mg oral carbidopa 1 hour before and 7 hours and 15 minutes after CVT301. For each 24-hour postdose period, venous blood samples were obtained prior to dosing and at regular intervals following dosing, in order to perform a pharmacokinetic analysis of levodopa concentration over 24 hours.
All CVT301 doses led to a more rapid increase in plasma levodopa concentrations in a dose-proportional manner, including within 10 minutes of administration, when compared to oral C/L in either fasted or fed states. Furthermore, between-subject variability in plasma levodopa concentrations was less following treatment with CVT301. A total of four adverse events, all mild in intensity and resolved without incident, were reported by four subjects: dizziness (n=2) after the 50 mg dose, headache (n=1) after a 10 mg dose, and muscle spasm (n=1) after a 10 mg dose. Nausea was not reported. It was concluded that the rapid and reliable increase in plasma levodopa concentrations associated with CVT301 administration made it a suitable therapy to investigate further for the rapid treatment of Off symptoms in patients with PD.20
Phase II
A Phase IIA study examined the potential benefit of CVT301 for Off episodes in PD.21 In order to be eligible for the study, patients needed a clinical diagnosis of idiopathic PD diagnosed at an age of 30–80 years and currently at stage 1–3 in an On state according to the modified Hoehn and Yahr scale. All eligible patients needed to be levodopa-responsive, currently taking oral levodopa at least four times a day, and experiencing at least 2 hours or more recognizable and predictable Off periods during the waking day, excluding early-morning Off time. While in the On state, patients were required to have FEV1 >70% and FEV1:FVC ratio >75%. A total of 27 patients were screened; 24 were randomized and received at least one dose of inhaled study treatment, and one patient discontinued prematurely.14 In order to investigate the potential benefit of CVT301 against parkinsonian Off episodes, patients received single in-clinic doses of test medications during observed Off episodes caused by withholding the patient’s PD medication for at least 4 hours after their usual morning dose of oral levodopa taken with a dopamine decarboxylase inhibitor. During the Off period after their usual first oral C/L dose, all patients then received a single dose of oral C/L 25/100 mg, 25 mg CVT301 (FPD), 50 mg CVT301 (FPD), and placebo inhalation on different days. Study medication was administered on each of the 4 days, with at least 2 days interval between doses. Plasma levodopa concentrations were measured prior to dosing and periodically through 180 minutes (3 hours) after dosing, along with timed finger tapping and Unified Parkinson’s Disease Rating Scale (UPDRS) part III scores. The examiner also observed the presence and severity of dyskinesia. Because patients received their usual first dose of oral C/L before performing study procedures, observed plasma concentrations were adjusted for predose levels on an individual basis.21
Patients treated with 50 mg CVT301 subsequently experienced a median Tmax of 15 minutes vs 66 minutes. Levodopa absorption was also more variable between patients after oral C/L administration compared to levodopa absorption after CVT301 administration: 77% of PD patients receiving 50 mg CVT301 achieved a clinically relevant increase in plasma levodopa concentration (>400 ng/mL) within 10 minutes, while only 27% of those treated with oral C/L did. Subjects receiving 50 mg CVT301 also achieved clinical improvement (timed finger tapping and motor UPDRS score) within 5 minutes of dosing, with an effect lasting 90–100 minutes, while oral C/L dosing led to such improvement starting at 30 minutes.14 No changes in lung function were seen. The most common side effect was mild–moderate cough (n=6, 25%), which tended to become less frequent after the initial dosing of inhaled drug. Nausea was reported in only one patient following oral C/L dosing. The rate of dyskinesia was lower following both CVT301 doses compared to oral levodopa and was rated as mild or moderate. This study concluded that CVT301 was safe, well tolerated, and led to rapid and more consistent levodopa absorption compared to oral levodopa in the Off state, which was associated with a more rapid improvement in motor function following individual doses. In this dose-finding study, the 50 mg dose was found to be clinically effective.21
A Phase IIB study of CVT301 sought to establish the efficacy and safety of self-administered CVT301 in relieving Off episodes assessed by the UPDRS part III compared to placebo.22 In this trial, subjects who were 30–80 years old with typical PD features, modified Hoehn and Yahr scale ratings of 1–3 in the On state, experiencing recognizable and predictable Off periods lasting ≥2 hours per day (excluding early-morning Off time), and taking oral levodopa doses at least four times per day were eligible to participate. In addition, subjects had to meet entry criteria of ≥25% improvement from Off to On state following the first usual morning dose, FEV1 >60% of the predicted value, and FEV1:FVC ratio ≥75%. Exclusion criteria included history of respiratory disease within the past 5 years and Mini-Mental State Examination score <25. The subjects were randomized 1:1 to self-administer CVT301 or placebo for 4 weeks to treat Off periods up to three times per day to be taken in combination with their regular schedule of oral PD medications, which were also kept constant throughout the study. CVT301 dosing was increased from 35 mg (FPD) in weeks 1 and 2 to 50 mg (FPD) in weeks 3 and 4. Primary outcome measures included UPDRS part III score at screening (unblinded) and at the end of weeks 1, 2, and 4 (blinded-rater pre- and postdose at 0, 10, 20, 30, and 60 minutes), subjective assessment of the On state, patient diaries, and the Patient Global Impression of Change (PGIC) scale. Safety assessments included treatment-emergent adverse effects, physical examination findings, clinical laboratory values, electrocardiography, and spirometry.
A total of 86 study participants used either CVT301 or placebo 2.1 times daily on average and experienced a mean treatment effect of 7 points on the UPDRS part III using the 50 mg FPD at week 4. The onset of benefit was achieved at 10 minutes postdose (first time point assessed): 78% of subjects achieved an On state in the examiner’s judgment at week 4 compared to 36% in the placebo group, and 72% of the CVT301-treated patients compared to 46% of those treated with placebo rated their PD as improved on the PGIC scale. Patient diaries revealed a least-squares mean decrease of 1.6 hours per day in Off time at week 4 without increase in On time with troublesome or untroublesome dyskinesia. The clinical effects of CVT301 did not vary by baseline patient characteristics, including sex, Hoehn and Yahr scale score, daily Off time, or presence of dyskinesia.23
The most common treatment emergent adverse effects in the Phase IIB study of CVT301 included dizziness, cough, and nausea, each present in 7% of subjects (n=3). Other adverse effects occurring in 5% of subjects included headache, peripheral edema, anxiety, and discoloration of sputum. Dose reductions were related to headache and nausea (same patient, receiving CVT301), chest pain, and dyskinesia (n=1 each in placebo group). Discontinuation (n=5) was related to painful respiration and sputum discoloration in the CVT301-treated group, and bradykinesia, chest pain, and wrist fracture in the placebo-treated group. A prospective longitudinal evaluation of pulmonary function measured by spirometry was also described in this group of subjects,24,25 in which patients were evaluated for 4 weeks in both Off and On states throughout the study. FEV1 and FVC variability was greater than that for FEV1:FVC ratio, and about 25% of spirograms did not meet quality metrics, most commonly due to inability to perform reproducible tracings. Subjects did not report any respiratory symptoms, and 45% of tracings were classified as having normal morphology. A sawtooth curve, which suggests upper-airway obstruction, has been previously described in 29%–67% of PD patients,25 but was only observed in 3% of the subjects in this study, possibly related to careful patient selection. Other abnormalities were attributed to neuromuscular dysfunction (19%) or poor effort (34%). There were no differences in these patterns noted between treatment groups, and there were no major differences between the On and Off states. These patterns are consistent with those previously reported in PD patients. Together, these Phase IIA and IIB studies support the preferred pharmacokinetic profile and clinical efficacy of CVT301 50 mg (FPD) in the reduction of Off episodes in patients with fluctuating PD.
Phase III
A Phase III study of CVT301 (SPAN-PD) has been completed26 and formed the basis of the product’s new-drug application. This study was designed as a 12-week double-blind, placebo-controlled investigation of PD subjects with motor fluctuations. Enrolled subjects were randomized 1:1:1 to receive placebo, CVT301 60 mg (35 mg FPD), or CVT301 84 mg (50 mg FPD). A total of 339 subjects who met the same inclusion criteria as the aforementioned Phase IIB study were enrolled.22 Additional exclusion criteria included dyskinesia that could interfere with performing study procedures, known contraindications to C/L, prior treatment with deep-brain stimulation, history of chronic lung disease within the past 5 years, and concomitant use of apomorphine HCl. A total of 351 subjects were randomized, and 339 were enrolled and allowed to take study-drug doses up to five times daily. The primary efficacy end point was change in UPDRS part III score at 30 minutes after dosing at 84 mg at 12 weeks. Key secondary end points included On responders within 60 minutes, change in UPDRS part III score at 10 minutes postdose, and total daily Off time.
Mean change in UPDRS part III score at 30 minutes after CVT301 84 mg (50 mg FPD) dosing at 12 weeks was −9.83 to −5.91 for placebo (P=0.009), indicating an effect size of −3.9 points.27 A dose-dependent response was observed.28 Also at week 12, 58% of subjects receiving CVT301 84 mg (50 mg FPD) were On responders by the 60-minute mark compared to 36% of those receiving placebo (P<0.05),26 and 71% of subjects treated with CVT301 84 mg (50 mg FPD) compared to 47% treated with placebo reported an improvement in PGIC scale (P<0.05). The onset of benefit measured by the UPDRS part III score occurred at 10 minutes after dosing and persisted at 1 hour. There was not a statistically significant reduction in average daily Off time measured by patient diaries, and any dyskinesia observed was rated as mild.28 Approximately 85% of subjects completed the study, with a 13%–15% withdrawal rate (any reason) across groups and a 3%–5% withdrawal rate due to adverse effects across groups. The most common treatment-emergent adverse effects of CVT301 compared to placebo were cough (14.9% vs 1.8%), upper respiratory tract infection (6.1% vs 2.7%), nausea (5.3% vs 2.7%), sputum discoloration (5.3% vs 0%), and dyskinesia (3.5% vs 0%). Two subjects in the active-treatment group discontinued the study due to cough, though cough was classified overall as mild in all subjects who experienced it. There were no statistically significant differences in FEV1 or diffusion capacity of lungs for carbon monoxide (DLCO) in CVT301-treated or placebo-treated subjects.28
This Phase III study confirmed that there is a clinically meaningful response to CVT301 in reduction of motor symptoms experienced by PD patients and that the drug is safe and tolerable. A long-term, open-label extension study (NCT02242487) has enrolled 295 subjects who are dose-blinded to two open-label doses (60 and 84 mg of CVT301, equivalent to 35 and 50 mg FPD, respectively).27 No control arm is included. The results are unavailable at this time.
Long-term and other safety studies
A prospective 12-month, open-label, randomized controlled study in PD patients has recently been reported, with the primary objective of assessing open-label efficacy29 and pulmonary function30 with long-term exposure to CVT301. Subjects meeting entry criteria were randomized 2:1 to receive CVT301 84 mg (50 mg FPD) or to an observational cohort (without CVT301) receiving standard-of-care therapy for PD. Subjects were excluded if they had a history of asthma or other chronic lung disease.
A total of 408 subjects were randomized (278 to the CVT301 arm), and 204 had completed the study at the time of reporting. The mean usage of CVT301 was 2.3 doses per day. The mean change in UPDRS part III scores after dosing at 10, 20, 30, and 60 minutes was −5.7, −12.0, −15.5, and −16.1 points, respectively, at 4 weeks, with similar findings at 52 weeks (−5.0, −11.5, −15.3, and −14.8 points, respectively); ≥80% of subjects achieved an On state within 60 minutes and remained On. PGIC scores revealed that >75% of subjects reported improvement. Diary reports showed approximately 1.4 hours’ reduction in Off time. Effects were maintained at 52 weeks.
In a separate report,27 all subjects had completed the 36-week visit and 199 had completed the 52-week visit. Mean changes in FEV1 and DLCO from baseline to week 52 in the CVT301-treated group were not statistically different from the observational control group. Serious adverse effects were experienced in 10.2% (n=13) of the control arm and 14.9% (n=40) of the CVT301 arm. Urinary tract infection was the only serious adverse event reported in >1% of subjects, occurring in four subjects (1.4%). The most common adverse effects were cough (12.9% [n=35] in the CVT301 group vs 0.8% [n=1] in the placebo group), nasopharyngitis (6.4% [n=17] vs 4.7% [n=6]), dyskinesia (5.5% [n=15] vs 3.1% [n=4]), fall (5.2% [n=14] vs 2.4% [n=3]), and bone fracture (5.2% [n=14] vs 2.4% [n=3]). All fractures were adjudicated as unlikely related or unrelated to the study drug. Two subjects discontinued the study due to cough, though 91% of cough was rated as mild. These long-term safety reports suggest that CVT301 84 mg (50 mg FPD) is effective in treating Off episodes in PD29 and does not alter the natural progression of pulmonary function in PD subjects.30
Other safety studies have been completed in special populations, such as healthy asthmatics (NCT2633007), healthy smoking and nonsmoking volunteers (NCT02633839), and individuals with fluctuating PD with early-morning Off episodes (NCT02807675). Safety and exploratory efficacy assessments from the last of these three have been recently reported.31,32 In a randomized, double-blind, two-way crossover study,31,32 36 eligible PD subjects experiencing morning Off episodes received a single dose of CVT301 84 mg (50 mg FPD) or placebo immediately after their morning dose of usual medication, including levodopa. Primary assessments included safety and tolerability,31 followed by exploratory efficacy analyses.32 The subjects turned On faster based on examiner assessment in the CVT301 group compared to placebo (25.0 vs 35.5 minutes), and an On event was 35% more likely to occur after CVT301 dosing than after placebo. It is important to note that this study was not powered to assess efficacy. In the safety and tolerability assessment, no serious adverse effects were noted, and no subjects discontinued the study. No differences in the occurrence of orthostatic hypotension were observed (n=7 in each group, none symptomatic), and the incidence and severity of examiner-rated dyskinesia over 3 hours were similar in both groups. The most common treatment-emergent adverse effect was cough, occurring in 11% of CVT301-treated patients vs 2.8% in those receiving placebo. All cough was rated as mild, and none led to discontinuation. This study concluded that single doses of CVT301 used in conjunction with oral C/L for early-morning Off symptoms are safe and tolerated.31
Potential for inhaled levodopa in treatment of Parkinson’s disease
Rescue therapy for Off periods in PD is an established therapeutic strategy, albeit one that does not address the underlying cause of motor fluctuations. Apomorphine hydrochloride injection (Apokyn; Britannia Pharmaceuticals, Reading, UK) is a currently available fast-acting dopamine agonist that offers onset of clinical benefit within 10–20 minutes, but requires a subcutaneous injection to be administered and may be associated with nausea, hypotension, and development of subcutaneous nodules at injection sites.33 Premedication with an antiemetic is often required to avoid dose-related nausea and vomiting. Patients may experience difficulty manipulating the injection device in their Off state, requiring the assistance of a caregiver. A sublingual formulation of apomorphine hydrochloride is under clinical development,34 and may offer a more user-friendly delivery method. Adverse events can include dizziness, somnolence, and nausea.
Of note, inhaled levodopa administered via a dry-powder inhaler has been studied by other investigators.35 While conducting investigations into the ability of PD patients to perform an inhalation maneuver during an Off period,36,37 the authors developed an alternate process to manufacture the dry powder with lower volume and fewer excipients, in conjunction with a preloaded unit-dose inhaler (rather than a capsule inhaler) that may be easier for PD patients to use, called Cyclops.35 Dose reproducibility and deposition into the peripheral airways was demonstrated due to the high resistance and low flow rate of the inhaler. Clinical data are unavailable at this time, but these studies validate the ease of use of inhaled dry-powder doses of levodopa for PD patients in the Off state.
It is important to note that evidence to date does not support the use of CVT301 as primary therapy for PD that would replace oral C/L or B/L. While the clinical data support the persistent clinical effect of CVT301 at 90–100 minutes postdose, the full duration of effect is not well characterized.21 The Cmax of CVT301 50 mg FPD is only 500 ng/mL in an Off state after a morning dose of oral C/L. By contrast, other levodopa formulations (100 mg levodopa in C/L IR, C/L ER, C/L extended-release capsules, and C/L/entacapone) achieve Cmax of 700–1,000 ng/mL in isolation.38 The clinical effects of 50 mg FPD CVT301 are thus unlikely to be similar to oral doses of C/L, and the two therapies have not been directly compared. Furthermore, the effects of doses >50 mg FPD of CVT301 have not been reported.
Rather, CVT301 could potentially provide an alternative rescue therapy to reduce Off times that is easy to self-administer, is well-tolerated, and reliably achieves an On state when administered. Its clinical effects are not associated with major worsening of dyskinesia or nausea. The inhaled-delivery mechanism allows for improved systemic bioavailability, rapid onset of drug action, avoidance of first-pass drug metabolism and other pharmacokinetic issues, and avoidance of injection. It may serve as an adjunct or alternative therapy for patients who are unable to tolerate or have insufficient benefit from other pharmacologic agents, such as dopamine agonists or monoamine oxidase inhibitors, for management of their motor fluctuations, or are not candidates for advanced therapies, such as deep-brain stimulation or levodopa–carbidopa intestinal gel administration.
The spectrum of emerging therapies for motor symptoms of PD is broad, and includes additional symptomatic therapies, neuroprotective therapies, those directed at specific genetic variants, immunotherapies, and neurosurgery/neuromodulation.39–42 Some of these agents involve novel compounds or delivery mechanisms, while others entail repurposing of old drugs. Many engage nondopaminergic pathways, but are unlikely to restore impaired dopamine signaling in PD patients. Therefore, it is likely that it will be necessary to administer oral agents, such as various formulations of levodopa (including CVT301, if approved) and other symptomatic therapies for PD alongside these novel agents. Whether or not any of these strategies will yield disease-modifying effects is yet to be determined. In the meantime, however, patients and practitioners will benefit from having more options available to combat the disabling motor complications of PD.
Conclusion
Based on data from the Phase III safety and efficacy study (SPAN-PD), as well as results from two long-term safety studies, a new-drug application for CVT301 under the brand name Inbrija was successfully filed in February 2018. The proposed indication is for use on an as-needed basis to address symptoms of Off periods in patients on a C/L regimen.
In summary, CVT301 leads to a rapid rise in plasma levodopa concentration with onset of effect within 5–10 minutes in most studies, peak effect at 30 minutes, and a predictable dose-dependent response. In a majority of cases, Off periods transition to On periods without associated dyskinesias. The clinically effective dose appears to be 84 mg (50 mg FPD) with as-needed use averaging roughly twice per day alongside a regular oral C/L regimen in most of the PD patients with >2 hours of daily Off periods. The primary adverse events reported in the Phase III study consisted of mild cough, upper respiratory tract infection, nausea, sputum discoloration, and dyskinesia. The mild–moderate cough was generally not debilitating, resolved after initial treatment, and did not cause study participants to withdraw or abstain from using this medication. No adverse effects were noted on spirometry parameters, and overall CVT301 was considered safe and well tolerated across several studies, including in special populations (eg, asthmatics and smokers). CVT301 is demonstrated to be a safe and effective rescue therapy for management of Off symptoms associated with PD. While CVT301 does not directly address the problem of motor fluctuations, it can help manage troublesome symptoms for patients experiencing these problems, and has the potential to provide clinicians with another option to optimize individualized therapeutic regimens for patients with PD.
Disclosure
The authors report no conflicts of interest in this work.
References
Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591–1601. | ||
Braak H, del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197–211. | ||
Jimenez-Shahed J. A review of current and novel levodopa formulations for the treatment of Parkinson’s disease. Ther Deliv. 2016;7(3):179–191. | ||
Tolosa E, Martí MJ, Valldeoriola F, Molinuevo JL. History of levodopa and dopamine agonists in Parkinson’s disease treatment. Neurology. 1998;50(6 Suppl 6):S2–S10. | ||
Rinne UK, Mölsä P. Levodopa with benserazide or carbidopa in Parkinson disease. Neurology. 1979;29(12):1584–1589. | ||
Soykan I, Sarosiek I, Shifflett J, Wooten GF, Mccallum RW. Effect of chronic oral domperidone therapy on gastrointestinal symptoms and gastric emptying in patients with Parkinson’s disease. Mov Disord. 1997;12(6):952–957. | ||
Calabresi P, di Filippo M, Ghiglieri V, Tambasco N, Picconi B. Levodopa-induced dyskinesias in patients with Parkinson’s disease: filling the bench-to-bedside gap. Lancet Neurol. 2010;9(11):1106–1117. | ||
Olanow CW, Stocchi F. Levodopa: A new look at an old friend. Mov Disord. 2018;33(6):859–866. | ||
Fahn S, Oakes D, Shoulson I, et al. Levodopa and the progression of Parkinson’s disease. N Engl J Med. 2004;351(24):2498–2508. | ||
Chaudhuri KR, Rizos A, Sethi KD. Motor and nonmotor complications in Parkinson’s disease: an argument for continuous drug delivery? J Neural Transm. 2013;120(9):1305–1320. | ||
Olanow CW, Obeso JA, Stocchi F. Continuous dopamine-receptor treatment of Parkinson’s disease: scientific rationale and clinical implications. Lancet Neurol. 2006;5(8):677–687. | ||
Contin M, Martinelli P. Pharmacokinetics of levodopa. J Neurol. 2010;257(Suppl 2):253–261. | ||
Blanchet PJ, Grondin R, Bédard PJ, Shiosaki K, Britton DR. Dopamine D1 receptor desensitization profile in MPTP-lesioned primates. Eur J Pharmacol. 1996;309(1):13–20. | ||
Lipp MM, Batycky R, Moore J, Leinonen M, Freed MI. Preclinical and clinical assessment of inhaled levodopa for OFF episodes in Parkinson’s disease. Sci Transl Med. 2016;8(360):360ra136. | ||
Edwards DA, Hanes J, Caponetti G, et al. Large porous particles for pulmonary drug delivery. Science. 1997;276(5320):1868–1872. | ||
Bartus RT, Emerich D, Snodgrass-Belt P, et al. A pulmonary formulation of L-dopa enhances its effectiveness in a rat model of Parkinson’s disease. J Pharmacol Exp Ther. 2004;310(2):828–835. | ||
Dunbar C, Scheuch G, Sommerer K, Delong M, Verma A, Batycky R. In vitro and in vivo dose delivery characteristics of large porous particles for inhalation. Int J Pharm. 2002;245(1–2):179–189. | ||
Hoppentocht M, Hagedoorn P, Frijlink HW, de Boer AH. Technological and practical challenges of dry powder inhalers and formulations. Adv Drug Deliv Rev. 2014;75:18–31. | ||
Acorda Therapeutics Inc. ARCUS Technology. n.d. Available from: http://www.acorda.com/products/arcus-technology. Accessed September 18, 2018. | ||
Freed MI, Batycky R, Merica E. Safety, tolerability and levodopa pharmacokinetics following inhaled administration of CVT-301, a levodopa dry powder aerosol, in healthy, adult subjects. Mov Disord. 2013;28 Suppl1:430. | ||
Freed MI, Moore JA, Batycky R, Tia DF. Pharmacokinetics (PK) following inhaled levodopa delivery with CVT-301: Rapid augmentation of systemic levodopa (LD) levels and improvement in motor function in PD patients with motor fluctuations. Mov Disord. 2014;29 Supple 1:647. | ||
Lewitt PA, Hauser RA, Grosset DG, et al. A randomized trial of inhaled levodopa (CVT-301) for motor fluctuations in Parkinson’s disease. Mov Disord. 2016;31(9):1356–1365. | ||
Lewitt P, Freed M, Leinonen M, Sedkov A, Murck H. Effect of Patient Characteristics on Motor Function in Response to 35–50 mg of Inhaled Levodopa (CVT-301) in Patients with Parkinson’s Disease: Results from a Phase 2b Study. Neurology. 2016;86(16 Suppl):P5.372. | ||
Freed MI, Hampson NB, Defeo-Fraulini T, Gentile A. Spirometric abnormalities in Parkinson’s disease (PD) with motor fluctuations: A prospective, longitudinal study. Mov Disord. 2014;29 Suppl 1:1022. | ||
Hampson NB, Kieburtz KD, Lewitt PA, Leinonen M, Freed MI. Prospective evaluation of pulmonary function in Parkinson’s disease patients with motor fluctuations. Int J Neurosci. 2017;127(3):276–284. | ||
LeWitt PA, Fernandez HH, Hauser RA, et al. Inhaled levodopa (CVT-301 84mg) significantly improves motor function during off periods in Parkinson’s disease (PD) subjects: A phase 3 study (SPAN-PD). Mov Disord. 2017;32(9):e1. | ||
Acorda Therapeutics Inc. CVT-301 Phase 3 Data Showed Significantly Improved Motor Function During OFF Periods in Parkinson’s Disease; 2017. Available from: http://s1.q4cdn.com/271808180/files/doc_news/CVT-301-Phase-3-Data-Showed-Significantly-Improved-Motor-Function-During-OFF-Periods-in-Parkinsons-Disease.pdf. Accessed September 18, 2018. | ||
Cohen R, Stern M, Batycky R, Blank B, Lewitt P, Grosset D. CVT-301 Phase 3 Program Overview; 2017. Available from: http://s1.q4cdn.com/271808180/files/doc_presentations/2017/ACOR-MDS-Presentation-060517-(1).pdf. Accessed Septermber 18, 2018. | ||
Grosset D, Dhall R, Gurevich T. Long-term Efficacy of Inhaled Levodopa in Parkinson’s Disease Subjects With Motor Fluctuations: a Phase 3 Open-Label Randomized Study. Neurology. 2018;90 (15 Suppl):S26.008. | ||
Grosset D, Dhall R, Gurevich T. Long-Term Pulmonary Safety of Inhaled Levodopa in Parkinson’s Disease Subjects With Motor Fluctuations: a Phase 3 Open-Label Randomized Study. Neurology. 2018;90 (15 Suppl):S26.006. | ||
Ellenbogen A, Hauser RA, Isaacson SH. Inhaled Levodopa Administered With Oral Carbidopa/Levodopa for Early Morning OFF Symptoms in Patients With Parkinson’s Disease: Safety Assessment. Neurology. 2018;90 (15 Suppl):S26.005. | ||
Isaacson SH, Ellenbogen A, Hauser RA. Inhaled Levodopa Administered With Oral Carbidopa/Levodopa for Early Morning OFF Symptoms in Patients With Parkinson’s Disease: Exploratory Efficacy Analysis Neurology. 2018;90 (15 Suppl):S26.004. | ||
Pfeiffer RF, Gutmann L, Hull KL, Bottini PB, Sherry JH; APO302 Study Investigators. Continued efficacy and safety of subcutaneous apomorphine in patients with advanced Parkinson’s disease. Parkinsonism Relat Disord. 2007;13(2):93–100. | ||
Hauser RA, Olanow CW, Dzyngel B, et al. Sublingual apomorphine (APL-130277) for the acute conversion of OFF to ON in Parkinson’s disease. Mov Disord. 2016;31(9):1366–1372. | ||
Luinstra M, Grasmeijer F, Hagedoorn P, Moes JR, Frijlink HW, de Boer AH. A levodopa dry powder inhaler for the treatment of Parkinson’s disease patients in off periods. Eur J Pharm Biopharm. 2015;97(Pt A):22–29. | ||
Luinstra M, Rutgers AW, Dijkstra H, Al E. Inhalation manoevre performed by Parkinson’s patients during an off period. Eur Respir J. 2015;46(Suppl 59):PA1586. | ||
Luinstra M, Rutgers AW, Dijkstra H, et al. Can Patients with Parkinson’s Disease Use Dry Powder Inhalers during Off Periods? PLoS One. 2015;10(7):e0132714. | ||
Hsu A, Yao HM, Gupta S, Modi NB. Comparison of the pharmacokinetics of an oral extended-release capsule formulation of carbidopa-levodopa (IPX066) with immediate-release carbidopa-levodopa (Sinemet()), sustained-release carbidopa-levodopa (Sinemet() CR), and carbidopa-levodopa-entacapone (Stalevo()). J Clin Pharmacol. 2015;55(9):995–1003. | ||
Lotia M, Jankovic J. New and emerging medical therapies in Parkinson’s disease. Expert Opin Pharmacother. 2016;17(7):895–909. | ||
Lang AE, Espay AJ. Disease Modification in Parkinson’s Disease: Current Approaches, Challenges, and Future Considerations. Mov Disord. 2018;33(5):660–677. | ||
Athauda D, Foltynie T. Drug Repurposing in Parkinson’s Disease. CNS Drugs. 2018;32(8):747–761. | ||
Lee DJ, Dallapiazza RF, de Vloo P, Lozano AM. Current surgical treatments for Parkinson’s disease and potential therapeutic targets. Neural Regen Res. 2018;13(8):1342–1345. | ||
Steiger MJ, Stocchi F, Bramante L, Ruggieri S, Quinn NP. The clinical efficacy of single morning doses of levodopa methyl ester: dispersible Madopar and Sinemet plus in Parkinson disease. Clin Neuropharmacol. 1992;15(6):501–504. | ||
Dupont E, Andersen A, Boas J, et al. Sustained-release Madopar HBS compared with standard Madopar in the long-term treatment of de novo parkinsonian patients. Acta Neurol Scand. 1996;93(1):14–20. | ||
Haglund L, Crevoiser C, Hoogkamer JFW. Relative bioavailability of the novel Madopar Dispersible tablet compared with standard Madopar. Focus on Parkinson’s Disease. 1997;9:7–10. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.