")
Back to Journals » Drug Design, Development and Therapy » Volume 8
Profile and potential of ixabepilone in the treatment of pancreatic cancer
Authors Smaglo B, Pishvaian M
Received 14 August 2013
Accepted for publication 18 March 2014
Published 14 July 2014 Volume 2014:8 Pages 923—930
DOI https://doi.org/10.2147/DDDT.S52964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Brandon G Smaglo, Michael J Pishvaian
Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC, USA
Abstract: The management of metastatic pancreatic adenocarcinoma is a challenge for medical oncologists because of both the aggressive nature of the disease and the relative paucity of effective systemic treatments with activity against this type of tumor. In the effort to discover new agents and combinations that may augment the therapeutic arsenal available for the management of this cancer, early phase clinical trials have been performed using ixabepilone, an epothilone B analog, with promising results. Targeting the microtubule system with certain taxanes in the management of pancreatic adenocarcinoma has been validated; ixabepilone also targets the microtubule system, interfering with it in an alternate manner from the taxane mechanism. Ixabepilone has demonstrated activity in cancers that have become taxane-resistant as well as those that never had any demonstrable taxane susceptibility. The available data for the use of ixabepilone in the management of pancreatic adenocarcinoma are limited but promising. Single-arm studies have demonstrated both clinical efficacy and tolerable toxicity for the use of ixabepilone as monotherapy. The trial data available for ixabepilone used as a part of combination therapy are similar: it has been paired with chemotherapy (carboplatin, irinotecan) and biologic therapy (dasatinib, sunitinib) at the Phase I level to treat solid tumors in general, again with tolerable side effects and a suggestion of benefit. A single Phase II study has evaluated combination therapy with ixabepilone in the management of patients with pancreatic cancer, pairing it with cetuximab with clinical benefit. Although these trials are promising with regard to addition of ixabepilone to the slim armamentarium for management of pancreatic cancer, further work is still to be done. Importantly, this work bears the burden of not only validating the clinical benefit of ixabepilone, but also of determining whether this benefit is enhanced in any way by combination therapy, and where ixabepilone fits in the sequence of management for patients with metastatic pancreatic cancer.
Keywords: ixabepilone, pancreatic cancer, microtubules
Introduction
Pancreatic adenocarcinomas are among the deadliest malignancies. At the time of diagnosis, this cancer has progressed to the point of being surgically unresectable and is thus incurable in 80%–90% of patients.1,2 Among the minority of patients for whom surgical resection is an option, recurrence rates remain at 60%–80%, with 5-year survival rates reported to be between 8% and 26% for resected patients (but <5% for all patients).1–3 With the vast majority of pancreatic patients ultimately faced with metastatic disease, the development of clinically beneficial and tolerable systemic treatment options remains an important area of ongoing research. One important focus of the research into pancreatic adenocarcinoma therapy that has been and continues to be explored is targeting of the microtubule system.
The microtubule system in cancer management
Broadly speaking, pharmacologic targeting of the microtubule system remains an important component of anticancer therapy. Microtubules take part in a number of diverse intracellular roles, including maintenance of cellular structure, protein trafficking, and mitosis. The structure of the microtubules is far from static.4 Rather, the microtubule network functions in a dynamic equilibrium of polymerization and depolymerization, which is essential for progression through the cell cycle in both healthy and cancerous tissue through the formation and then disassembly of the mitotic spindle.5 Given the important role of microtubules in cellular mitosis, this network remains an important target for anticancer chemotherapy, and has been validated by the development of a number of anticancer agents.6–8 The additional role of the microtubule machinery in other cellular functions, including vesicle and organelle transport, cellular scaffolding, secretory processes, and receptor signaling, can also lead to apoptosis through the disruption of these additional processes during cellular interphase.5,7,8
Accomplishing its wide variety of intracellular roles necessitates a significant degree of heterogeneity among the microtubule polymers. This heterogeneity develops from the variety of tubulin building blocks of the microtubules as well as from post-translational modification of the assembled polymer. Microtubule polymerization is accomplished by heterodimerization of two different forms of the protein tubulin (α and β), each of which has several further distinct isotypes. Once the microtubule is assembled from these isotypic proteins, it undergoes further post-translational modifications, enhancing their structural and functional diversity.5
Having this diversity of assembly, that leads to a diversity of function, allows ample potential for induction of apoptosis through microtubule targeting. Such targeting of the microtubules to instigate disruption of both cellular division and intracellular activity during interphase is a mainstay of the pharmacotherapeutic management of many cancers. Several different classes of drugs have been developed to target the microtubule array in a number of different ways. The taxanes function by stabilizing the microtubule and preventing its depolymerization, which leads ultimately to microtubule overpolymerization within the cell, and thus to cell death.8 The vinca alkaloids bind to tubulin and prevent polymerization of the dimers, ultimately inhibiting spindle formation.6 Additional classes of agents and microtubule targets continue to be developed.4 As is always the case, the utility and efficacy of these agents vary widely according to the type of cancer.
Ixabepilone as a microtubule-targeting anticancer agent
Ixabepilone is an epothilone B analog, and one of a unique class of antimicrotubule-targeting agents.4 The epothilones bind to β-tubulin, stabilizing the microtubule and preventing its depolymerization. Disruption of the microtubules in this way prevents cell cycle progression and ultimately induces cellular apoptosis.9 Epothilone binding may also induce apoptosis during interphase by interfering with the various other cellular processes that the microtubules are involved with, such as structure and trafficking, as described in the previous section. Although the taxanes and epothilones share a common binding site on β-tubulin, the binding mechanism is different.10 Moreover, structural differences between the two classes of agents allow the epothilones to tolerate resistance mechanisms, to which the taxanes are susceptible, such as drug efflux via P-glycoprotein and tubulin mutation.11,12 These differences extend the clinical utility of the epothilones over that of the taxanes. The epothilones demonstrate wider and more potent activity than the taxanes, and typically remain effective even in patients whose tumors have demonstrated taxane resistance.8,12,13
In early studies, while the naturally occurring epothilones demonstrated impressive in vitro activity, only modest anticancer activity was observed in vivo. This discrepancy was attributed to a combination of poor metabolic stability, unfavorable pharmacokinetics, and a narrow therapeutic window with the natural compound.12 In order to overcome these weaknesses, synthetic epothilone analogs such as ixabepilone have been developed.8,12
Microtubule targeting in pancreatic adenocarcinoma
For many years, targeting the microtubule system as a management strategy for pancreatic adenocarcinoma yielded little clinical benefit. However, studies in 2012 and 2013 have demonstrated that the use of certain taxane-containing regimens does offer clinical benefit to these patients. The greatest benefit of targeting the microtubule system in the management of pancreatic adenocarcinoma has been observed with the addition of a taxane to a gemcitabine-based regimen. The one prospectively validated microtubule-targeting agent currently approved in the chemotherapeutic management of metastatic pancreatic cancer is albumin-bound paclitaxel (nab-paclitaxel, Abraxane®; Celgene Corporation, San Diego, CA, USA). The 2013 MPACT study reported a survival advantage was demonstrated with the addition of Abraxane to a standard gemcitabine monotherapy regimen for the management of metastatic pancreatic cancer.14 Several retrospective studies have also suggested a survival advantage for the triple-drug regimen of gemcitabine, docetaxel, and capecitabine (GTX), two of which were published as a manuscript pair in 2012. Dakik et al published a retrospective analysis of patients who had received GTX as a second-line or higher treatment. They demonstrated a median survival of 38.3 weeks for 21 of 59 patients whose disease remained stable on treatment.15 The median survival was 15 weeks for the 29 patients who progressed and 7.4 weeks for the nine patients who were not evaluable. None of the patients had a radiologic response to treatment. The second retrospective review by De Jesus-Acosta et al included 154 patients treated with GTX in any line of therapy for metastatic disease, with 51% of patients receiving first-line GTX.16 Patients who were chemotherapy-naïve demonstrated a median overall survival of 11.6 months, while those who received it as a second line or greater had a median overall survival of 5.7 months. However, among those patients who received GTX as a second-line or higher therapy, median overall survival was higher among those who demonstrated a partial response (21.93 months), compared with patients who had stable disease (12.13 months), progressive disease (7.93 months), or were not evaluable (4.6 months); a similar breakdown of survival according to response has not been reported for those who received this therapy as a first line. While these two retrospective studies are encouraging, prospective trials are necessary to confirm the clinical utility of this docetaxel-containing combination regimen in the management of metastatic pancreatic cancer. As these studies with docetaxel and Abraxane demonstrate, the utility of microtubule-targeting agents in the management of metastatic pancreatic cancer is presently limited to combination therapy, and there is no current evidence for benefit of microtubule-targeting drugs as single agents in the management of pancreatic cancer. In this context, ixabepilone is emerging as an important anticancer agent targeting the microtubule system that may provide clinical benefit for patients with pancreatic cancer.
To date, the in vivo clinical utility of ixabepilone has been most strongly established in the management of metastatic breast cancer, where Phase III trials have demonstrated a survival benefit.17 Correspondingly, the indication approved by the US Food and Drug Administration for ixabepilone is for the management of metastatic or locally advanced breast cancers no longer responsive to other standard chemotherapies.18 While the management of metastatic breast cancer remains the only clinical scenario where ixabepilone currently holds an approval in the USA, its utility continues to be explored in the management of a number of different malignancies, including pancreatic cancer.17 The late emergence of clinical utility in targeting the microtubule network in pancreatic adenocarcinoma supports further exploration of such agents, such as ixabepilone, in this disease. A number of early phase studies have evaluated the safety and efficacy of ixabepilone in the management of solid tumors, including pancreatic cancer, both as a single agent and as a part of combination therapy.19–22
Ixabepilone as a single agent in metastatic solid tumors
Three Phase I trials have demonstrated the safety, tolerability, and preliminary clinical efficacy of single-agent ixabepilone.19–22 These trials, which are summarized in Table 1, enrolled patients with any metastatic solid tumor and were not limited to pancreatic cancers. Both the oral and intravenous formulations of ixabepilone have been investigated.
 | Table 1 Summary of Phase I trials designed to evaluate the tolerability and safety of ixabepilone as a single agent in the management of solid tumors refractory to standard therapies, including pancreatic cancer* |
Evaluation of the oral formulation of ixabepilone was initially presented in abstract form in 2010, with a final publication in 2012.21,22 This Phase I trial evaluated treatment of patients with ixabepilone administered orally every 6 hours for three doses on day 1 of a 21-day cycle. Eighteen patients were treated in this dose-escalation trial (three at the 30 mg/dose, nine at the 40 mg/dose, and six at the 50 mg/dose). The specific tumor types of the patients were not reported. Due to high interpatient and intrapatient variability in pharmacokinetics, both this study and any further development of oral ixabepilone were terminated. Although there were no untoward adverse events observed with the oral formulation when compared with what had been observed with intravenous formulations in other trials, this pharmacokinetic variability was deemed sufficient to prevent any further development of the oral formulation.
A Phase I trial conducted in Belgium and the USA evaluated the tolerability of intravenous ixabepilone in 86 patients with metastatic solid tumors who had progressed on standard therapy.19 The tumor types for these 86 patients were not summarized. Thirty-four of the patients were treated on a 21-day cycle, where a maximum tolerated dose of 25 mg/m2 administered on day 1 was reached; 52 of the patients were treated on a 28-day cycle, where a maximum tolerated dose of 20 mg/m2 administered weekly was reached. Five patients, two from the 21-day cycle and three from the 28-day cycle, achieved an objective partial response. None of these patients had pancreatic cancer. A 2007 report of a Phase I study from Japan similarly reported on the tolerability of ixabepilone in 14 patients with previously treated solid tumors.20 None of the enrolled patients had pancreatic cancer. All patients were treated on a 21-day cycle, arriving at a maximum tolerated dose of 50 mg/m2 on day 1. However, with two patients experiencing a dose-limiting toxicity at this dose, the recommended Phase II dose was 40 mg/m2. One patient experienced a partial response and six more achieved stable disease.19,20
A single Phase II study of single-agent ixabepilone in pancreatic cancer was published in 2006 by the Southwest Oncology Group. The results demonstrated an encouraging survival profile in the management of treatment-naïve patients. In this single-arm study, 60 patients were treated with ixabepilone every 21 days; the dose of treatment was reduced from 50 mg/m2 to 40 mg/m2 early in the trial due to neurotoxicity, and the patients treated at both dose levels were evaluated together.23 Median survival was 7.2 months, and the overall response rate was 21%. These results compared favorably with the single-agent standard of care at that time, ie, gemcitabine, and were better than results from similar trials of paclitaxel (overall survival of 5 months, with an overall response rate of only 8%).24,25
Ixabepilone as part of combination therapy in metastatic solid tumors
Simultaneous to the development of ixabepilone as a single agent, the tolerability and efficacy in combination with different chemotherapies and biologic therapies was being explored.
Combination ixabepilone and chemotherapies in metastatic solid tumors
Ixabepilone was paired with irinotecan in the management of a variety of solid tumors, including gastrointestinal tumors, as a regimen where both agents were intravenously administered every 2 weeks.26 This study evaluated toxicity by treating 41 patients with advanced solid tumors using escalating doses of both agents, reporting maximum doses of 20 mg/m2 for ixabepilone combined with 180 mg/m2 of irinotecan. None of the patients in this trial had pancreatic cancer; five of the patients demonstrated objective responses to treatment. In a separate trial, ixabepilone was paired with carboplatin, where carboplatin was administered on day 1 and ixabepilone on either day 1 (25 patients) or days 1 and day 8 (27 patients), both on a 21-day cycle.27 The maximum tolerated dose of ixabepilone was 30 mg/m2 when administered only on day 1 and 20 mg/m2 when administered on both days 1 and 8. For both dosing schedules of ixabepilone, the paired maximum carboplatin dose had an area under the concentration-time curve of 6. Six patients in this trial demonstrated a partial response to therapy (three from each treatment schedule). While none of these patients had pancreatic cancer, two of the six had adenocarcinoma of unknown origin. Both of these trials demonstrated that ixabepilone could be tolerably combined with cytotoxic chemotherapies, and there were no pharmacokinetic interactions. The results are summarized in Table 2.
 | Table 2 Summary of Phase I trials designed to evaluate the tolerability and safety of ixabepilone in combination with chemotherapy in the management of solid tumors refractory to standard therapies, including pancreatic cancer* |
Combination of ixabepilone and biologic therapies in metastatic solid tumors
Ixabepilone has also been combined with biologic agents, ie, sunitinib and dasatinib. Sunitinib, a multitargeted receptor tyrosine kinase inhibitor, is approved for the management of gastrointestinal stromal tumors and renal cell carcinoma, and continues to be investigated in the management of other tumor types. In one study, sunitinib was administered orally at a constant dose in combination with one of two intravenous ixabepilone dose-escalation schedules.28 For these pairings, the maximum tolerated doses were ixabepilone of 20 mg/m2 (when given on days 1, 8, and 15 in a 28-day cycle) and 30 mg/m2 (when given on day 1 in a 21-day cycle); in both pairings, sunitinib was administered at a dose of 37.5 mg/m2 daily, starting on day 8 of cycle 1. Tumor types were not reported, and while there were three patients with a partial response and eight with stable disease, none of these responses were seen in patients with pancreatic cancer. The dosing and maximum tolerated dose are reported in Table 3, but no pharmacokinetic data are reported. A separate trial paired orally administered dasatinib with a single intravenous ixabepilone dose schedule, for which the dosing and efficacy information is also in Table 3.29 Dasatinib is a tyrosine kinase inhibitor with activity against BCR-ABL, c-KIT, EPH receptor A2, platelet-derived growth factor receptor-beta, and the SRC family, and is approved in the management of chronic myeloid leukemia.30 The maximal tolerated doses for this combination were ixabepilone 40 mg/m2 every 21 days with dasatinib 100 mg daily. Four of 19 patients had to come off study for toxicity before arriving at the first assessment. Of the 15 patients who remained on therapy at first assessment, 87% demonstrated clinical benefit, as defined by either a partial response (one patient) or stable disease (12 patients). One patient in this study had pancreatic cancer, and demonstrated stable disease in response to treatment.
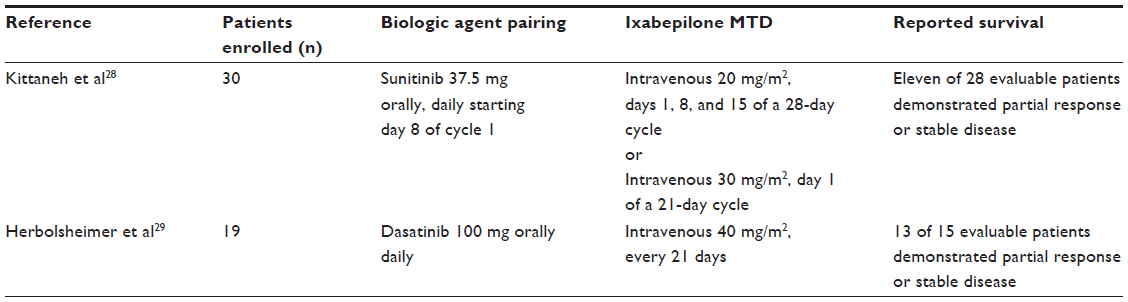 | Table 3 Summary of Phase I trials designed to evaluate the tolerability and safety of ixabepilone in combination with biologic therapy in the management of solid tumors refractory to standard therapies, including pancreatic cancer* |
The only higher phase trial evaluation of ixabepilone paired with a biologic agent in the management of metastatic pancreatic cancer is a Phase II study of ixabepilone and the monoclonal antibody cetuximab. A distinguishing characteristic of this study when compared with the earlier reported Phase I trials of ixabepilone combinations is that patients were treatment-naïve.31 In this trial, 54 patients were managed on a 3-week cycle, receiving ixabepilone intravenously at a dose of 32 mg/m2 on day 1 and cetuximab intravenously at a dose of 250 mg/m2 on days 1, 8, and 15. The 6-month survival rate, the primary endpoint of this study, was 57%. The median overall survival was 7.6 months, which is similar to that in the Southwest Oncology Group trial of ixabepilone monotherapy in a similar patient subset. An interesting observation in this trial was that those patients who developed the cetuximab-associated adverse reaction of acneiform rash had a longer median survival (8.8 months) than those who did not develop the rash (2.6 months). Whether this is a valid finding or whether it relates to the addition of ixabepilone to cetuximab is uncertain from this one study. Importantly, it is not clear whether cetuximab added any value to the clinical efficacy.
Safety and tolerability of ixabepilone in metastatic pancreatic cancer
Equally important to any efficacy discussion of ixabepilone in the management of metastatic pancreatic cancer is how well the treatment is tolerated. This therapy does not offer a hope of cure, but rather another option designed to prolong life with the disease; therefore, as is the case with all metastatic cancer regimens, if the price of that prolongation is an unpalatable panel of adverse effects, any benefit has been undone. Fortunately, the trial data evaluating ixabepilone suggests that it is highly tolerable.
When used as a single agent in the management of solid tumors, commonly occurring side effects included fatigue, neutropenia, neurotoxicity, gastrointestinal discomfort, mucositis, and arthralgia.19,20 These were generally well managed, and no treatment-related deaths were seen in the monotherapy trials. As noted, a range of maximum tolerated doses was determined from the different trials evaluating the intravenous formulation of ixabepilone. For the Phase II monotherapy trial in patients with pancreatic cancer, a dose of 40 mg/m2 was used. Adverse events in this Phase II trial were similar to those in the Phase I trials, although one patient death occurred that was deemed to be “possibly” treatment-related.23 Overall, ixabepilone was discontinued in 22% of patients because of potentially treatment-related adverse events.
Similar side effects were seen when intravenous ixabepilone was paired with chemotherapy. However, the grade of neutropenia was higher for similar doses of ixabepilone when paired with carboplatin than was seen for single-agent ixabepilone.27 A similar direct comparison of a combination of ixabepilone and irinotecan versus ixabepilone monotherapy cannot be considered, due to the differing dose schedules between the various trials.26 When ixabepilone was paired with sunitinib, the side effect profile was again similar to that of ixabepilone monotherapy, with the addition of a single event of deep vein thrombosis.28 While a similar adverse event profile was again seen when dasatinib was combined with ixabepilone, four patients did have to come off study due to drug intolerance before the first efficacy assessment.29 In the Phase II evaluation of ixabepilone and cetuximab in pancreatic cancer, a similar side effect profile was observed, with the acneiform rash known to occur with cetuximab being the only additional side effect observed.
Ixabepilone in the treatment paradigm of metastatic pancreatic cancer
The efficacy and toxicity data summarized above are promising in terms of further evaluation of ixabepilone or ixabepilone-based combinations in the treatment of metastatic pancreatic cancer. Clearly, given that the amount of data addressing the use of ixabepilone in this type of disease remains limited, further randomized prospective trials will be required before it can be considered a part of the treatment paradigm. In addition, an important question to address is where the drug should be inserted in the sequence of chemotherapeutic agents.
Currently, a limited number of treatment regimens are available in the metastatic setting for pancreatic cancer. As discussed earlier, the combination of systemic therapy with Abraxane and gemcitabine is one option that is often well tolerated. The other widely accepted option is the multidrug combination, FOLFIRINOX, which consists of both bolus and infusional administrations of 5-fluorouracil given with leucovorin, along with irinotecan, and oxaliplatin, all administered on a 14 day cycle.32 Although demonstrating an impressive survival benefit over single-agent gemcitabine, FOLFIRINOX can have a significant side effect profile, limiting its utility in patients with poor baseline performance status. Potential considerations for the exploration of ixabepilone either as a single agent or in combination could be following gemcitabine plus Abraxane in the second-line setting, or as combination therapy in the first-line setting, both in patients with poor performance status. Ixabepilone could also be considered as a substitute for a taxane in other regimens including gemcitabine plus Abraxane, or GTX.
Conclusion
Early trial data for the management of metastatic pancreatic adenocarcinoma using the epothilone analog ixabepilone are encouraging, but a great deal of work remains to be done. From the Phase I and limited Phase II trials, ixabepilone does seem to be adequately tolerated, which is critical for patients with pancreatic cancer who are often fairly debilitated by their disease. With regards to efficacy, there are both Phase I and II data to support the exploration of ixabepilone in further clinical trials. At present, given the limited amount of data regarding use of ixabepilone in pancreatic adenocarcinoma, no further conclusions can be drawn beyond that further such exploration is warranted and that the agent should not be recommended for use in this population outside of a clinical trial. That said, there is both ample clinical need and reason to expect benefit to justify proceeding with such trial development. As noted earlier, the number of available agents with activity in pancreatic cancer remains limited, thus justifying the exploration of agents that may be added to this panel. Moreover, while previously found to be lacking in benefit for this disease population, two microtubule-targeting regimens have emerged as efficacious options in the management of pancreatic cancer. Their emergence occurred contemporaneously to the development of ixabepilone, suggesting that drugs using this pharmacologic strategy are worthy of further development in the treatment of pancreatic adenocarcinoma. An important additional question will be where to place ixabepilone in the sequence of management for metastatic pancreatic cancer.
These questions will only be answered in the context of well designed (randomized) clinical trials. Given the prevalence and high mortality of pancreatic cancer, which are compounded by the paucity of effective, tolerable treatments available, the work necessary to answer these questions is justified.
Disclosure
The authors report no conflicts of interest in this work.
References
Sener SF, Fremgen A, Menck HR, et al. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985–1995, using the National Cancer Database. J Am Coll Surg. 1999;189(1):1–7. | |
Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg. 1993;165(1):68–72. | |
seer.cancer.gov [homepage on the Internet]. Bethesda, MD, USA: National Cancer Institute. Available from: http://seer.cancer.gov/statfacts/html/pancreas.html. Accessed July 9, 2013. | |
Stanton RA, Gernert KM, Nettles JH, Aneja R. Drugs that target dynamic microtubules: a new molecular perspective. Med Res Rev. 2011;31(3):443–481. | |
Goodin S. Novel cytotoxic agents: epothilones. Am J Health Sys Pharm. 2008;65(10):s10–s15. | |
Jordan A, Hadfield JA, Lawrence NJ, McGown AT. Tubulin as a target for anticancer drugs: agents which interact with the mitotic spindle. Med Res Rev. 1998;18(4):259–296. | |
Abu-Khalaf MM, Harris LN. Antimicrotubule agents. In: DeVita VT, Lawrence TS, Rosenberg SA, editors. DeVita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA, USA: Lippincott, Williams and Wilkins; 2011. | |
Morris PG, Fornier MN. Microtubule active agents: beyond the taxane frontier. Clin Cancer Res. 2008;14(22):7167–7172. | |
Fumoleau P, Coudert B, Isambert N, Ferrant E. Novel tubulin-targeting agents: anticancer activity and pharmacologic profile of epothilones and related analogues. Ann Oncol. 2007;18 Suppl 5:v9–v15. | |
Giannakakou P, Gussio R, Nogales E, et al. A common pharmacophore for epothilone and taxanes: molecular basis for drug resistance conferred by tubulin mutations in human cells. Proc Natl Acad Sci U S A. 2000;97(6):2904–2909. | |
Bollag DM, McQueeney PA, Zhu J, et al. Epothilones, a new class of microtubule-stabilizing agents with a taxol-like mechanism of action. Cancer Res. 1995;55(11):2325–2333. | |
Lee FY, Borzilleri R, Fairchild CR, et al. BMS-247550: a novel epothilone analog with a mode of action similar to paclitaxel but possessing superior antitumor efficacy. Clin Cancer Res. 2001;7(5):1429–1437. | |
Kowalski RJ, Giannakakou P, Hamel E. Activities of the microtubule-stabilizing agents epothilones A and B with purified tubulin and in cells resistant to paclitaxel. J Biol Chem. 1997;272(4):2534–2541. | |
Von Hoff DD, Ervin TJ, Arena FP, et al. Randomized phase III study of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic adenocarcinoma of the pancreas (MPACT). J Clin Oncol. 2012;30(Suppl 34):LBA148. | |
Dakik HK, Moskovic DJ, Carlson PJ, et al. The use of GTX as a second-line and later chemotherapy for metastatic pancreatic cancer: a retrospective analysis. Cancer Chemother Pharmacol. 2012;69(2):425–430. | |
De Jesus-Acosta A, Oliver GR, Blackford A, et al. A multicenter analysis of GTX chemotherapy in patients with locally advanced and metastatic pancreatic adenocarcinoma. Cancer Chemother Pharmacol. 2012;69(2):415–424. | |
Rivera E, Lee J, Davies A. Clinical development of ixabepilone and other epothilones in patients with advanced solid tumors. Oncologist. 2008;13(12):1207–1223. | |
US Food and Drug Administration. FDA approves Ixempra for advanced breast cancer patients. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm109015.htm. Accessed July 31, 2013. | |
Awada A, Piccart M, Jones SF, et al. Phase I dose escalation study of weekly ixabepilone, an epothilone analog, in patients with advanced solid tumors who have failed standard therapy. Cancer Chemother Pharmacol. 2009;63(3):417–425. | |
Shimizu T, Yamamoto N, Yamada Y, et al. Phase I clinical and pharmacokinetic study of 3-weekly, 3-h infusion of ixabepilone, an epothilone B analog, in Japanese patients with refractory solid tumors. Cancer Chemother Pharmacol. 2008;61(5):751–758. | |
He AR, Kunz PL, Pishvaian MJ, et al. A phase I study of an oral formulation of ixabepilone in patients with advanced cancer. J Clin Oncol. 2010;28(Suppl 15):e13090. | |
Kunz PL, He AR, Colevas AD, et al. Phase I trial of ixabepilone administered as three oral doses each separated by 6 hours every 3 weeks in patients with advanced solid tumors. Invest New Drugs. 2012;30(6):2364–2370. | |
Whitehead RP, McCoy S, Rivkin SE, et al. A Phase II trial of epothilone B analogue BMS-247550 (NSC #710428) ixabepilone, in patients with advanced pancreas cancer: a southwest oncology group study. Invest New Drugs. 2006;24(6):515–520. | |
Whitehead RP, Jacobson J, Brown TD, Taylor SA, Weiss GR, Macdonald JS. Phase II trial of paclitaxel and granulocyte colony-stimulating factor in patients with pancreatic carcinoma: a Southwest Oncology Group study. J Clin Oncol. 1997;15(6):2414–2419. | |
Burris HA, Moore, MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15(6):2403–2413. | |
Faivre S, Delbaldo C, Boige V, et al. Safety of repeated administrations of ixabepilone given as a 3-hour infusion every other week in combination with irinotecan in patients with advanced malignancies. Eur J Cancer. 2008;44(5):674–682. | |
Plummer R, Woll P, Fyfe D, et al. A phase I and pharmacokinetic study of ixabepilone in combination with carboplatin in patients with advanced solid malignancies. Clin Cancer Res. 2008;14(24):8288–8294. | |
Kittaneh M, Montero AJ, Kovacs K. Phase I trial of weekly and every 3 weeks ixabepilone and sunitinib in advanced solid tumors. J Clin Oncol. 2011;29(Suppl 15):3081. | |
Herbolsheimer P, Kapoor R, Smith KL, et al. Phase I trial of dasatinib and ixabepilone in patients with solid tumors. Invest New Drugs. 2013;31(1):92–98. | |
Sprycel [package insert]. Princeton, NJ, USA: Bristol-Myers Squibb Company; 2013. | |
Rocha Lima CM, Lin EH, Kim GP, et al. A phase 2 trial of ixabepilone plus cetuximab in first line-treatment of metastatic pancreatic cancer. Gastrointest Cancer Res. 2012;5(5):155–160. | |
Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.