")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Process Evaluation of a National Elderly Nutrition–Care Program in Iran: Perspectives of Clients and Providers
Authors Foroumandi E , Alizadeh M, Khodayari-Zarnaq R , Kheirouri S
Received 6 May 2020
Accepted for publication 28 July 2020
Published 13 August 2020 Volume 2020:13 Pages 1135—1147
DOI https://doi.org/10.2147/RMHP.S261121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Elaheh Foroumandi,1,2 Mohammad Alizadeh,1 Rahim Khodayari-Zarnaq,3 Sorayya Kheirouri1
1Nutrition Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 2Students’ Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran; 3Iranian Center of Excellence in Health Management, School of Management and Medical Informatics, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Sorayya Kheirouri
Department of Nutrition, Faculty of Nutrition, Tabriz University of Medical Sciences, Attar Nishabouri Street, POBOX: 14711, Tabriz 5166614711, I. R. Iran
Tel +98-41-33362117
Fax +98-41-33340634
Email [email protected]
Objective: As aging populations increase, many countries have begun implementation of policies to improve elder health and nutrition. This study evaluated key process components of nutrition sections of a national elderly integrated–care program in health-care centers in Iran.
Methods: With stratified three-stage random cluster sampling, a total of 256 elderly subjects (clients) and 76 staff members of health-care centers (providers) participated in the study. Quantitative and qualitative data were collected using two self-administrated questionnaires to evaluate various components of process evaluation for clients and providers. Program reach was measured by the ratio of the number in the target group who underwent the program to the number of eligible individuals. Exposure rate was measured as clients’ awareness of program services. Delivery and fidelity were assessed from providers’ reports for each service. Satisfaction rates were assessed for the whole program and for each service of the program. All reasons behind strengths and weaknesses in each of the process-evaluation components were examined and are reported in detail.
Results: The clients reported low-reach (20.0%) and moderate-exposure rates of 77.5%, with a program target of 90%. Primary training sessions were delivered to the providers as intended (100%), but most planned services for clients, especially vitamin and mineral supplementation, follow-up, and physical activity sessions, were poorly implemented, as they were delivered correctly to 24.7% (n=63, vitamin and mineral supplementation), 24% (n=62, follow-up), and 40.3% (n=103, physical activity sessions) of the clients, with a set program goal of 60%. An overall low level of implementation fidelity was observed, and 39.3% (n=30) of the providers believed that most clients did not benefit from the nutritional services. Overall, less than half (42.8%, n=101) the clients were highly satisfied with the program.
Conclusion: The process evaluation showed insufficient reach, exposure, and fidelity of the program, as well as imprecise delivery of some services, which resulted in low levels of client satisfaction. The findings may have implications for further reinforcement of the program, and indicate the importance of continuous monitoring and evaluation of such programs.
Keywords: process evaluation, elder, nutrition, elderly integrated–care program, national, Iran
Background
Population aging is considered one of the most important social transformations of the century, and can significantly affect every nation’s health, social, and economic levels.1 Elder, or old age, refers to those >65 years in age in developed countries and >60 years in most developing countries.2 Worldwide, the elder population is increasing rapidly, with one in eleven individuals categorized in this age-group.3 According to the World Health Organization, the elder population will rise to 2 billion by 2050.4 It has been reported that 23.1% of the total disease burden can be attributed to disorders among the elderly, as this is in high-income countries is estimated at 49.2% and at 19.9% in low- and middle-income countries.5
An effective partnership between government, the private sector, and international organizations helps developed countries increase quality of life and prevent disabilities among this age-group.6 Prevention or amelioration of the high burden of cost and promotion of health among the elderly can be achieved through dedicated population approaches to nutrition and physical activity (PA) using public services.7 Although there are different types of national elderly-nutrition strategies in developed countries,8,12 developing nations are still struggling, indicating a substantial need for formulation of appropriate policies to improve elder health.
The elder population of Iran is growing faster than in Western countries: currently, one in ten people in the country is older than 60 years. It is predicted that in just 35 years, this proportion will have increased to around one in three.13 Iran is facing emerging challenges related to this demographic transition, including population aging, changes in people’s needs, unsustainability of resources, and hospital-centered health services.14,16 In 2006, the Ministry of Health and Medical Education began a comprehensive intervention initiative: the elderly integrated–care program (EICP). Before nationwide implementation, EICP pilots were conducted in four selected provinces.17 In 2014, the EICP was implemented in the Tabriz metropolitan area (capital of East Azerbaijan province), located in the northwest of Iran. According to the latest population census of Iran in 2016, the Tabriz population was 1,558,693, among whom 108,184 (11.56%) were elderly.18
Overview of the Elderly Integrated–Care Program
The EICP is a part of the first-level health-service program in Iran. The goal of this health program is to improve the health of people, decrease public- health costs, and boost social protection. This program focuses on various health dimensions of the elderly, including lifestyle, nutrition, PA, mental disorders, and chronic disorders, such as hypertension, diabetes, abnormalities in lipid profile, and osteoporosis, as well as smoking, vaccination status, dental health, and high-risk behaviors. The activities are specified in accordance with seven strategies: periodic assessment, classification of clients, prevention and therapeutic care, public health education, health consultation, required follow-up, and referral to upper health-care centers (Table 1). The nutritional components of the program are also summarized in Figure 1. After implementation of the EICP for 4 years, there is a substantial need to evaluate dimensions, depth, and consequences of the program, aiming at making revisions in the process levels of the program. This is a report on the process evaluation of the elderly integrated nutritional–care program (EINCP) from the perspectives of both clients and providers, in order to clarify both strengths and weaknesses of the program.
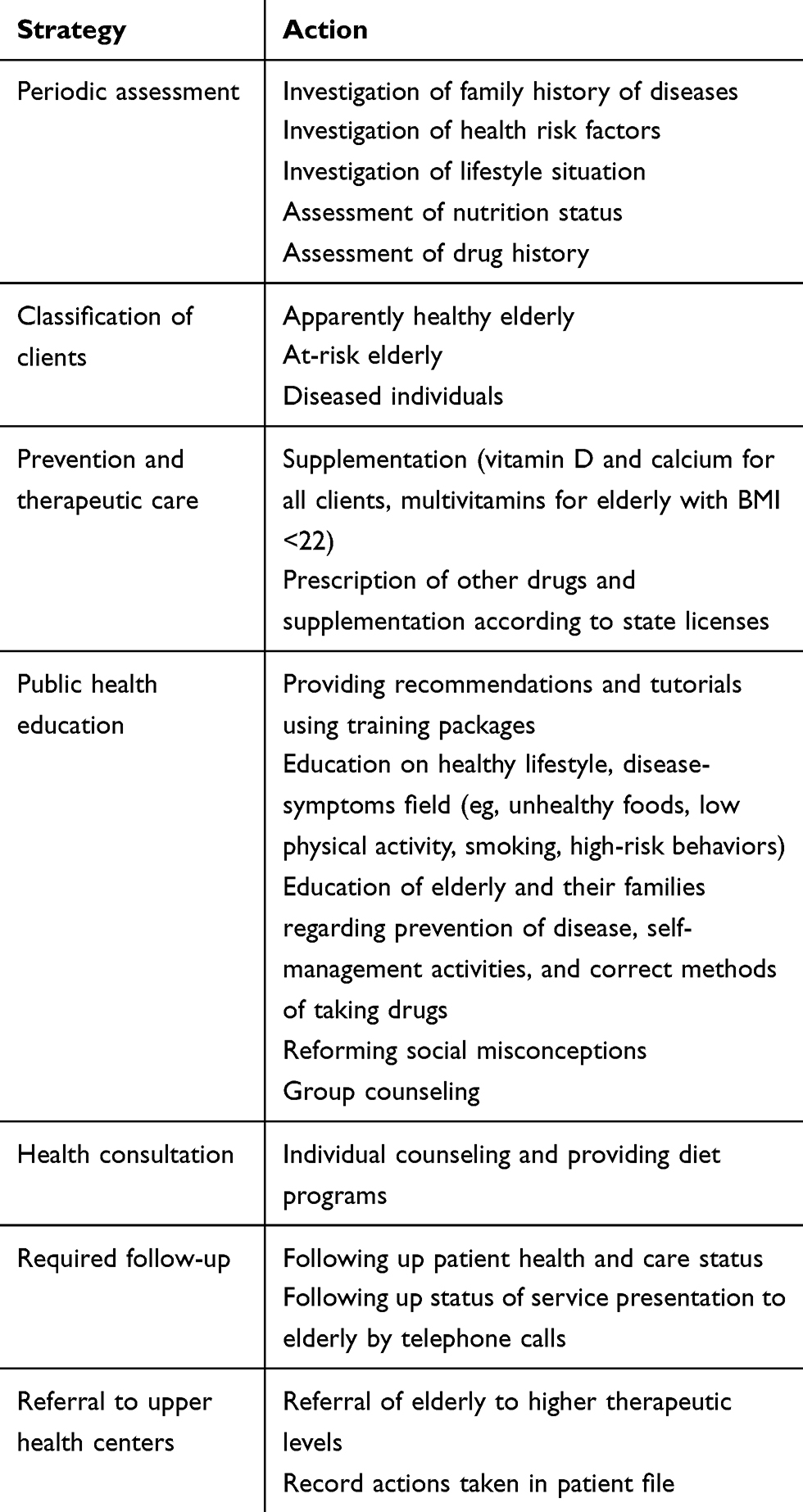 |
Table 1 Nutritional components of elderly integrated–care program in Iran |
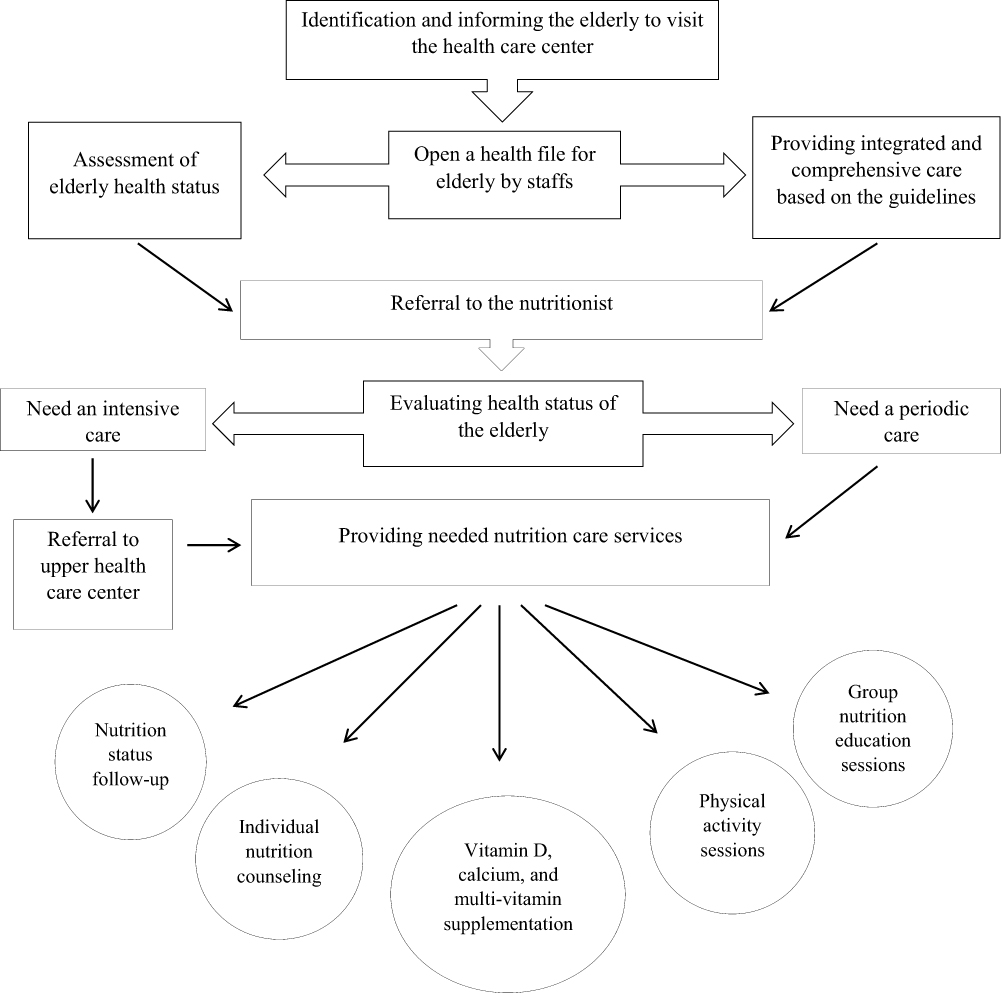 |
Figure 1 Process and components of elderly integrated nutrition–care program in health-care centers of Iran. |
Methods
Field of Study and Participants
This cross-sectional study was conducted in Tabriz between February and June 2019. The EINCP process was evaluated in two dimensions using perspectives of the clients (elderly) and providers (health-care staff). A stratified three-stage random cluster–sampling method was used to select the participants. Tabriz has 19 health-care complexes, all of which were selected by census for the first stage. The second stage was the selection of 32 of 57 health-care centers as clusters. The clusters were selected in such a way that all health complexes and municipal areas of the city were covered. The third stage was random selection of subjects from each cluster using simple randomization tables, based on a probability proportion-to-size sampling technique. The inclusion criterion was residents >60 years of age who had been covered by one of the health-care centers of Tabriz for at least 1 year. According to α-risk of 5%, margin of error of 5%, and confidence level of 95%, the minimum samples of clients and providers were estimated at 246 and 66, respectively. Based on a 25% loss in participation, final sample sizes were 308 clients and 83 providers. Ultimately, 256 clients and 76 providers participated in the study (Figure 2) and signed an informed consent. This study was performed in accordance with the Declaration of Helsinki. The protocol was approved by the Ethical Committee of Tabriz University of Medical Sciences, Tabriz, Iran (IR.TBZMED.REC.1397.1018).
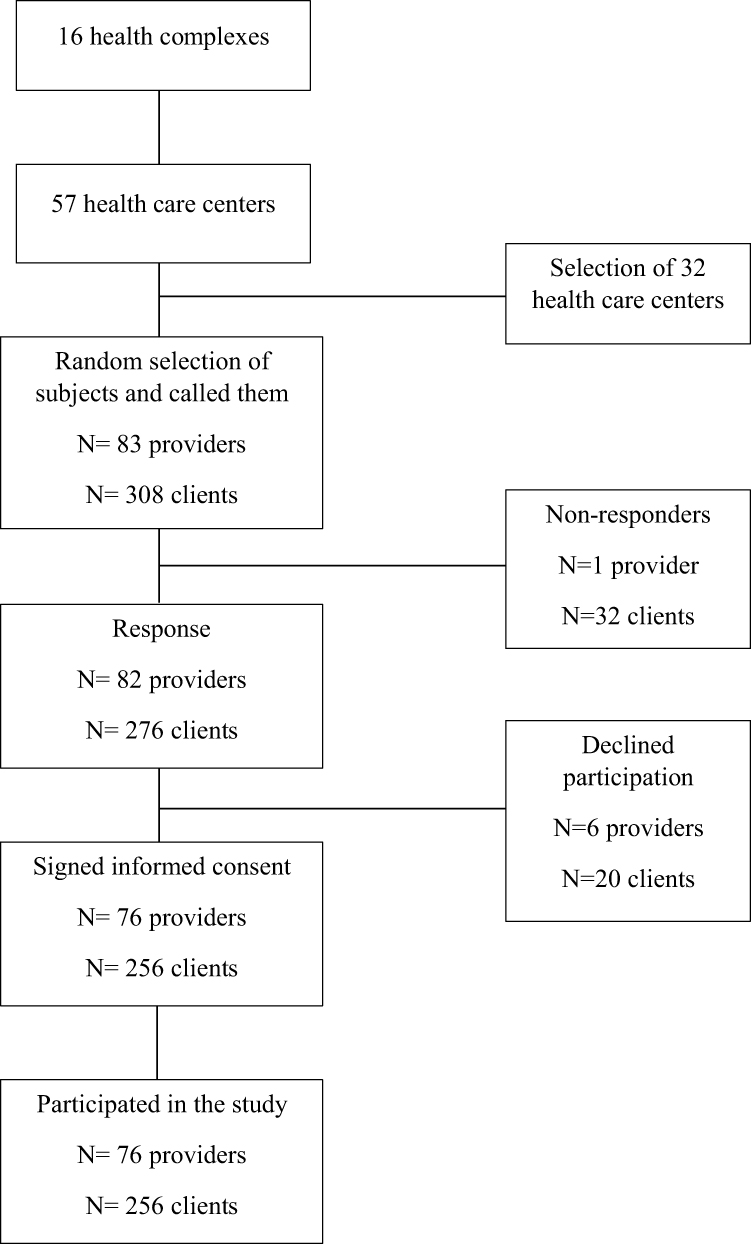 |
Figure 2 Flowchart of the study. |
Design and Process-Evaluation Components
This process-evaluation study was conducted using the process-assessment framework developed by Hughes and Margaretts.19 Components of the process evaluation and their description are shown in Table 2. Both clients and providers evaluated the program using two distinct self-administered questionnaires. Elements of process evaluation were translated into structured questions to develop these study questionnaires.20,22 For the next stage, a panel of experts specializing in the fields of gerontology (n=2), nutrition (n=3), and health policy (n=5) validated the instruments. Content-validity index and content-validity ratio values of both questionnaires were calculated and found acceptable: 0.93 and 0.89 for the clients’ questionnaire and 0.79 and 0.88 for the providers’ questionnaire, respectively. Reliability of the scales was assessed through the questionnaires being completed by 36 eligible clients and seven providers. After 4 weeks, a retest was conducted using the same participants. Cronbach’s α for both provider and client scales was 0.89 and 0.83, respectively. Scores >0.80 are generally considered acceptable.23
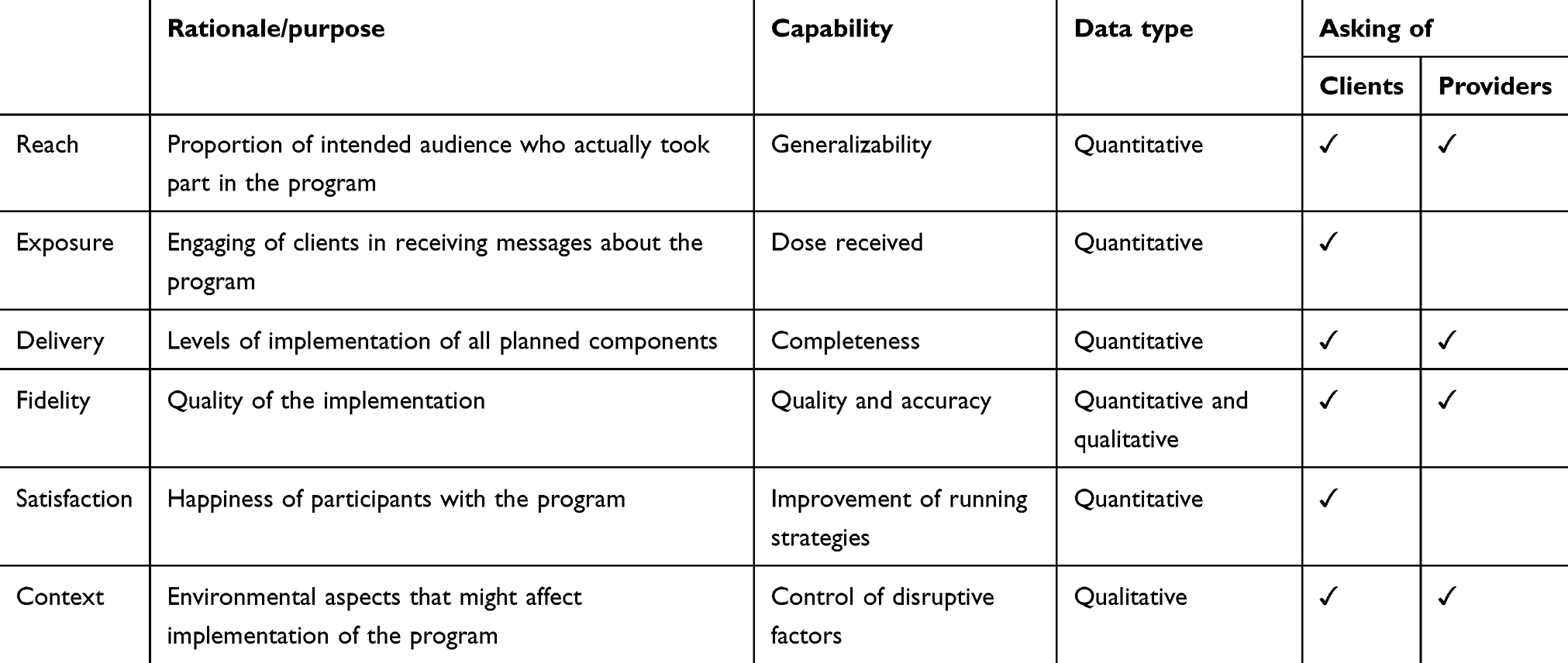 |
Table 2 Process-evaluation components |
Data Analysis
All responses to open-ended questions were transcribed to analyze qualitative data. Two researchers independently categorized answers to open-ended questions to identify relevant themes, which were then organized by topic and summarized. Disagreement between the reviewers was resolved through consultation with a third reviewer. Quantitative data are represented by means ± SD or n (%). Descriptive statistics were obtained using SPSS version 20.0.
Results
Characteristics of Study Participants
A total of 256 clients (104 men and 152 women) participated in the study. The mean age was 64.7±3.92 years. In all, 89.8% of clients had no academic education, and nearly all (97.3%) were married. The full questionnaire-response rate was 92.2% (n=236). A total of 76 program providers of mean age 38.6±5.80 years also responded to the providers’ questionnaire (response rate of 100%).
General Perspective of Participants
Program reach was calculated by the number of elderly who underwent the first evaluation, divided by the number of those potentially eligible. According to the latest national census, a total of 168,744 elderly reside in Tabriz.18 Process evaluation showed that health-care centers provided nutrition screening to 33,789 elderly, and thus EINCP reach was estimated at 20%. The program suggests arranging a quarterly schedule (four meetings per year) of introductory meetings for the providers. These meeting sessions were held as suggested. Further, according to results of postinstruction analysis, components of the EINCP (Table 1) were correctly and fully delivered to all providers (100%; n=76).
Tables 3–6 show the perspectives of clients toward the EINCP. Of the responders visiting the health-care centers at least once, 77.5% (n=183) were exposed to the nutritional services provided through the EINCP. This did not reach the program target of 90%. Although 86.8% (n=178) of clients believed that providers gave them enough time to provide and discuss their health needs, only 58.5% (n=138) were fully satisfied with their meeting time. The limited number of providers and unrelated fields of expertise, particularly regarding weight and blood-pressure measurements, were the principal factors that affected client satisfaction. All providers were aware of basic principles of the nutritional-care intervention and tried to follow them in the intended manner. From the providers’ perspective, fidelity of intervention components and tools were not adequate, as 39.3% (n=30) of them believed that most of the referred elderly did not benefit from these services.
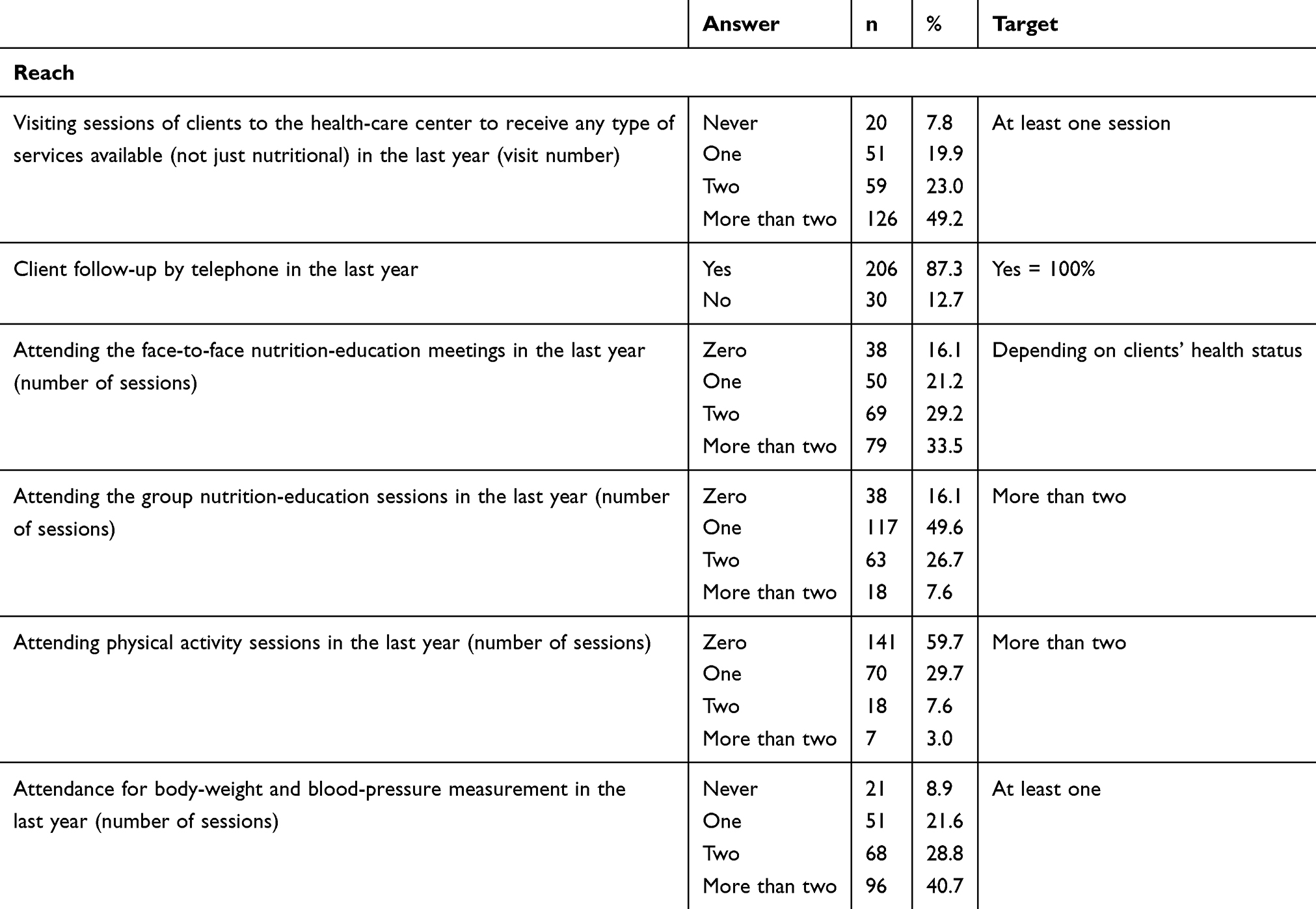 |
Table 3 Process evaluation of elderly integrated nutrition–care program (clients’ perspectives, n=256) |
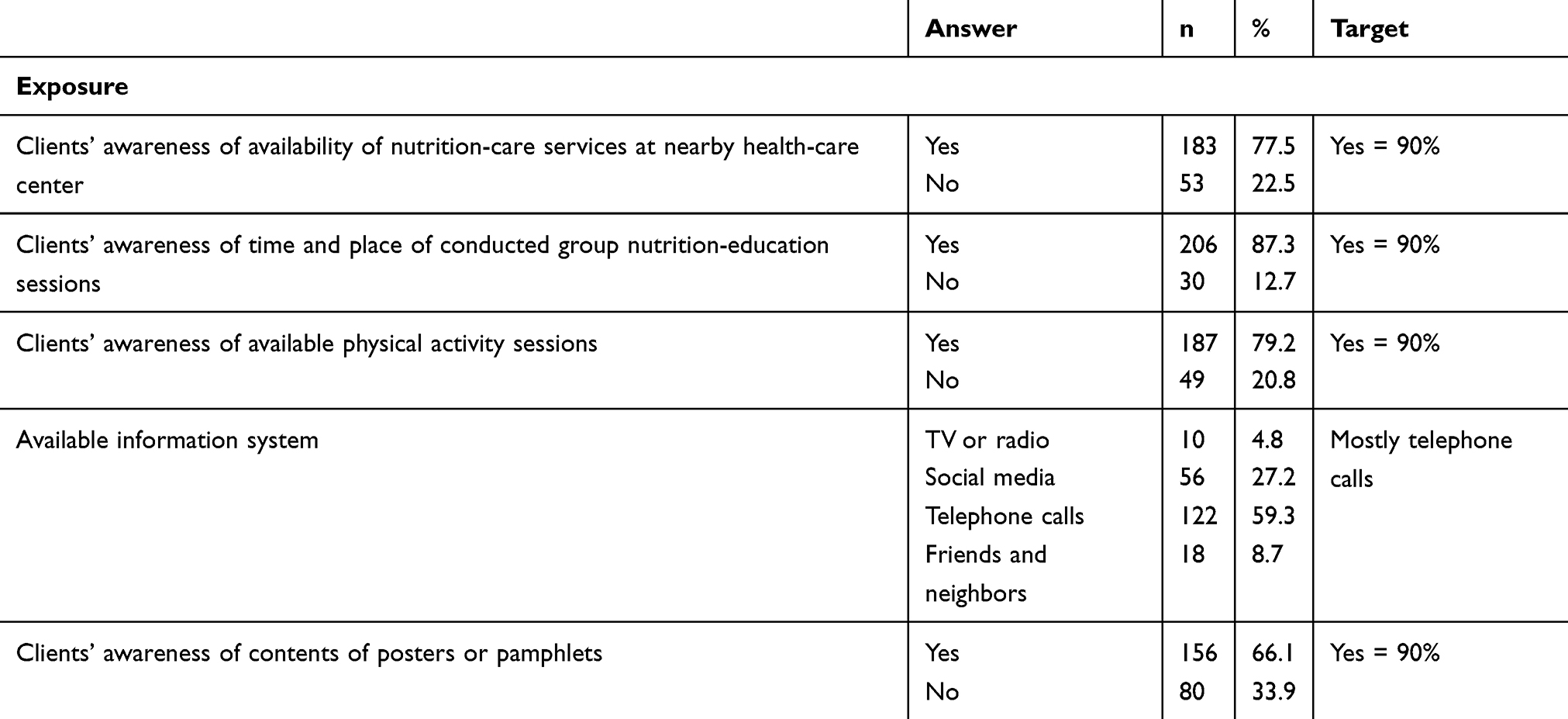 |
Table 4 Process evaluation of elderly integrated nutrition–care program (clients’ perspectives, n=256) |
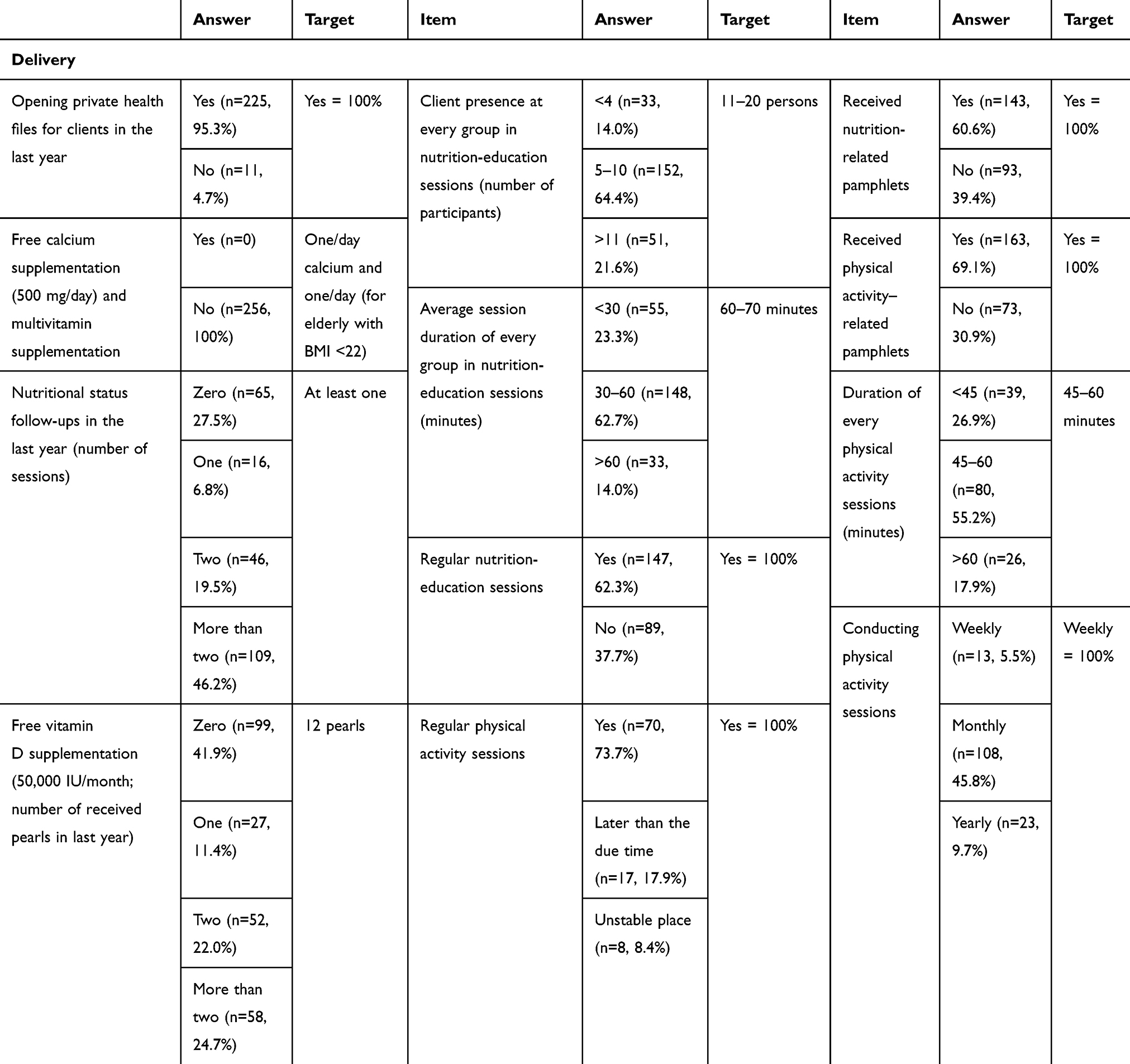 |
Table 5 Process evaluation of elderly integrated nutrition–care program (clients’ perspectives, n=256) |
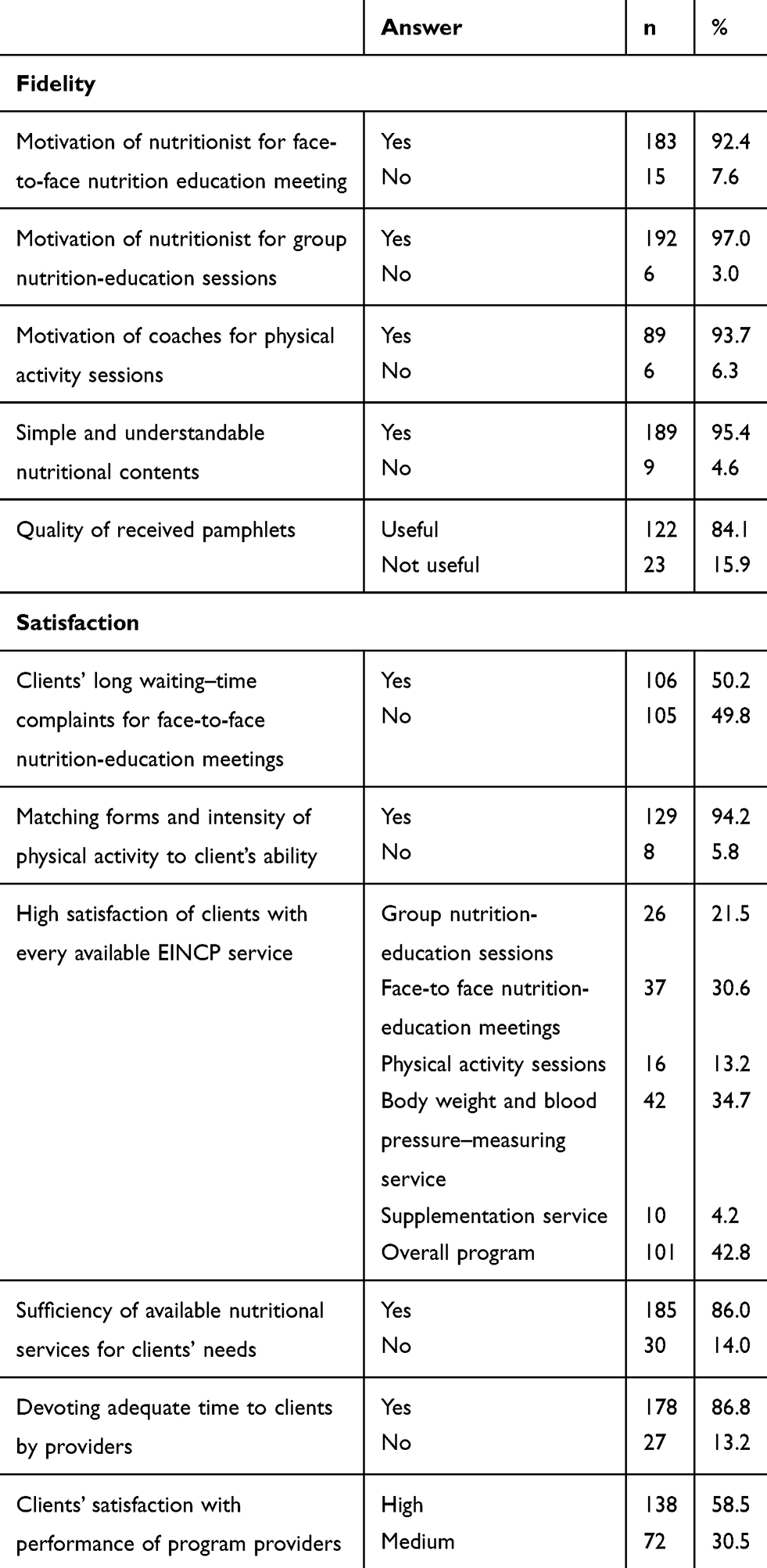 |
Table 6 Process evaluation of elderly integrated nutrition–care program (clients’ perspectives, n=256) |
Face-to-Face Nutrition-Education Meetings
With regard to face-to-face nutrition-education services for clients who had nutrition-related disorders, 16.1% (n=38) reported that the service was not delivered. The rest reported receiving one (21.2%), two (29.2%), or more than three (33.5%) sessions. Depending on the individual’s condition, the optimal meeting time for nutritionists for these program meetings was 20–40 minutes.24 The vast majority (83.3%; n=165) of clients attending these meetings reported that the duration of the session was <20 minutes. Nearly half the clients (50.2%) had a long wait before receiving service. Most of them (92.4%) found the nutritionists to be well motivated, but only 30.6% (n=37) had high satisfaction with this service.
Table 7 shows barriers to implementation of the EINCP from the providers’ perspective. In all, over three in four (77.6%, n=59) of the providers stated that the limited time for face-to-face nutrition-education meetings was due to the high number of referrals. A total of 78.9% (n=60) also believed that some early caregivers did not properly assess the health status of referred clients nor pay enough attention to convince the elderly in need of nutrition education to be referred to the nutritionist. Three in four (76.3%; n=58) providers did not have an appropriate space for face-to-face education meetings, and 67.1% (n=51) did not have nutritionists stationed in the health-care center, which greatly affected attendance of clients at face-to-face nutrition-education meetings. Also, 89.4% (n=68) of providers believed that elderly clients preferred to use available nutrition services in specialized clinics as an alternative to health-care centers.
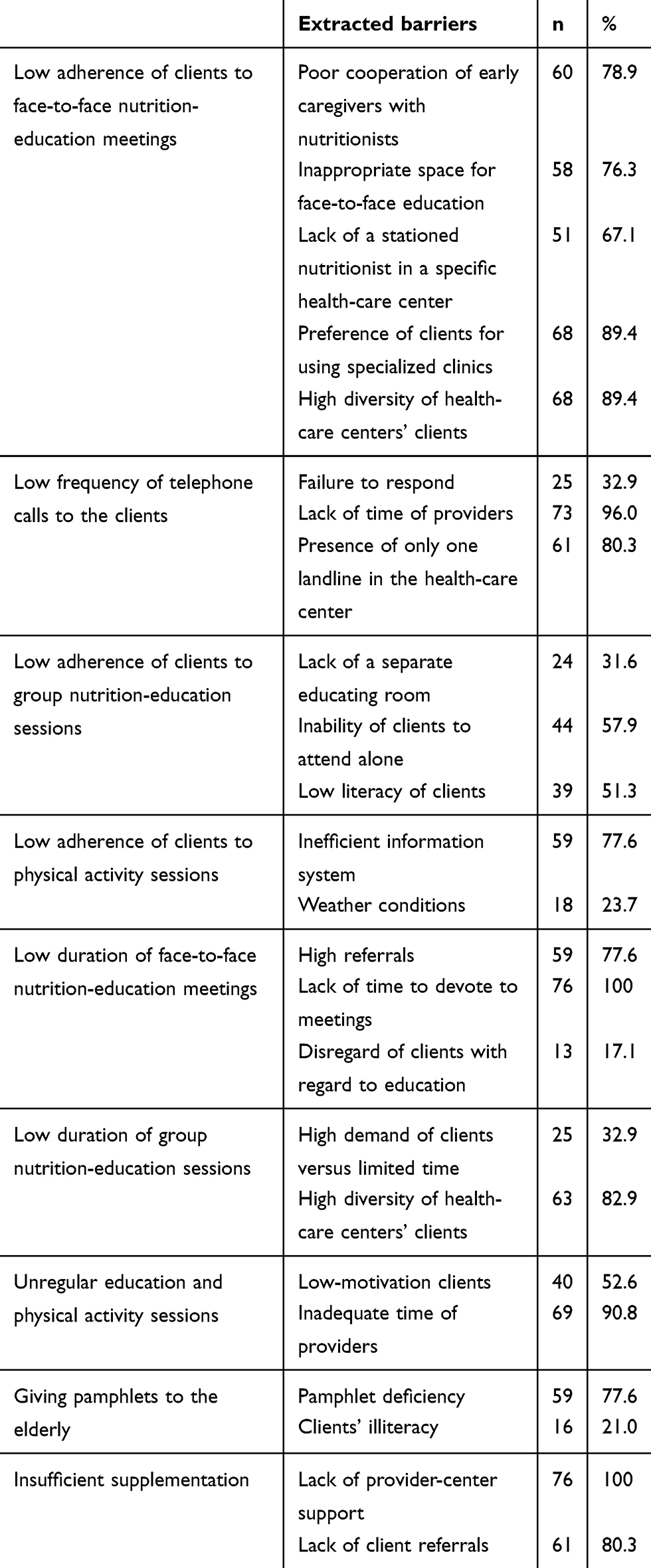 |
Table 7 Barriers to implementation of elderly integrated nutrition–care program (providers’ perspectives, n=76) |
Group Nutrition-Education Sessions
According to the EINCP, group nutrition-education sessions should be conducted once a week at a specific place and time in each health-care center, as well as in other public places, such as mosques and parks. The suggested duration and number of participants for these classes is 60–70 minutes and 11–20 persons, respectively. Every elder should participate in at least three group nutrition-education sessions. The package of instructions for these sessions is shown in Table 8.
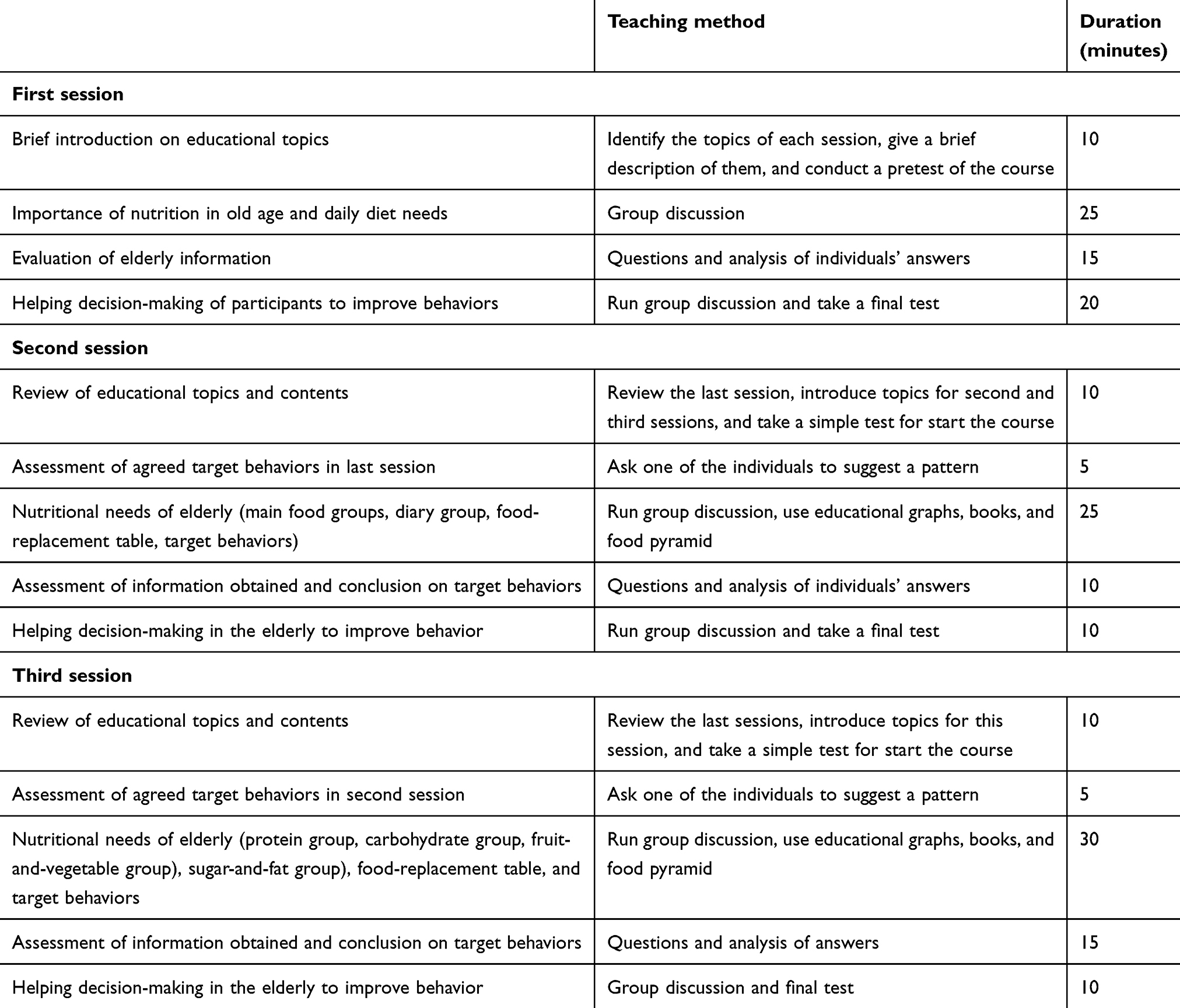 |
Table 8 Instructions for elderly group nutrition-education sessions |
Just 7.6% (n=18) of clients reported that they had participated in all three sessions, although 87.3% (n=206) had been exposed to these sessions. Of theclients participating in the sessions, 21.6% (n=51) stated that the number of participants in these group sessions was more than eleven. Most clients (86.0%) reported that the duration of the sessions was less than an hour, considered inadequate. On the other hand, 95.4% (n=189) of the clients reported that the content of the group nutrition-education sessions was simple, understandable, and attractive. Almost half (43.6%; n=103) the clients stated that these sessions were also conducted in public places, such as parks and mosques.
Providers were enthusiastic about the elderly group nutrition-education sessions, though 32.9% (n=25) reported not having enough time to fulfilltheir assigned tasks, as they provided health-care services to other age-groups at the same time. Over half (52.6%; n=40) pointed out that the lack of elder attendance and their low motivation in these sessions led to disruptions in holding timely and weekly sessions. Furthermore, lack of a separate education meeting room, inability of clients to attend at the health-care centers, and low literacy of clients were other barriers that affected adherence of clients to these sessions.
Physical Activity Sessions
It was found that 40.3% (n=95) of clients had participated in PA sessions within the last 12 months (EINCP goal 60%). The exposure rate of clients to these sessions was 79.2%. In all, 73.7% (n=70) of them reported that they had not had enough motivation to participate in the PA sessions. Only 5.5% (n=13) stated that the sessions were conducted periodically. The expected duration of every PA session was 45–60 minutes, and over half (55.2%; n=80) the clients observed this. Almost all (94.2%) reported that the format and intensity of the PA sessions were compatible with their ability. However, only 13.2% (n=16) had high satisfaction with these sessions. Providers believed that low adherence of clients to PA sessions was due to an inefficient information system (77.6%, n=59) and to weather conditions (23.7%, n=18).
Notification Framework for the Elderly
The staff of the health-care centers are responsible for regularly informing elders about ongoing programs via telephone. Most clients (87.3%, n=206) had received telephone calls from health-care centers with information on how to use their health services. Telephone (59.3%) and social media (27.2%) were the most frequently used methods to inform participants of the nutritional services of the health-care centers. Providers stated that some barriers greatly affected their telephone-contact success. For instance, 32.9% (n=25) of providers had failed to receive a response from clients in the last year, and 96.0% (n=73) had not had have enough time. In addition, 80.3% (n=61) reported that the presence of only one landline in the health-care center interfered with their assigned tasks.
Program Follow-Up
Health-center staff are expected to provide monthly follow-ups for elderly with special needs and once a year for those without any disorders. Almost half (46.2%, n=109) the clients had monthly follow-ups. Regular body-weight and blood-pressure monitoring is another task of health-center staff. It was reported that 40.7% (n=96) of clients had regular checkups for body weight or blood pressure, while 8.9% (n=21) had never received this service.
Posters, Banners, and Pamphlets
According to the EINCP, health-care centers should post banners and information media with the content of community health services in every neighborhood. Most clients (81.3%) did not notice the presence of any poster or banners in their neighborhoods. Nearly 60% of clients received nutrition and PA-related pamphlets in the classes. Further, 84.1% (n=122) mentioned that the pamphlets they received were useful. Over three in four (77.6%, n=59) providers felt that the pamphlets were not delivered on time or in sufficient quantities to distribute, resulting in low delivery of this service. They stated that the banners’ shapes and colors were not interesting enough to attract clients’ attention. They also suggested designing the banners and pamphlets with more conceptual colors and shapes, suitable for the elderly population, especially for individuals who cannot read or write.
Vitamin and Mineral Supplementation
The EINCP recommends health-care centers provide free supplements of vitamin D (50,000 IU/month) and calcium (500 mg/day) to all elders following examination by a general practitioner. The centers should also give multivitamin supplements to elders with BMI <22 kg/m2. In this regard, just 24.7% (n=58) of clients had received vitamin D supplements in the last year. Only 4.2% (n=10) had high satisfaction with the supplementation service. Importantly, none of the clients had received free calcium or multivitamin supplements. From the provider perspective, 80.3% (n=61) reported that clients were not referred to them to take supplements. All providers stated that health-care centers did not have adequate financial support to provide the supplements.
Overall Contextual Aspects Affecting the Program
Almost all participating providers (97.4%; n=74) believed that the main reasons for the shortcomings in providing high-quality and sufficient nutritional services to clients were late payment of staff salaries and the heavy workload assigned to them. Generally, since all staff members at health-care centers provide services for various age-groups within a limited time, it is not possible to focus just on elderly clients. Many health-care centers lack enough service space, a hindrance in responding simultaneously to the large number of clients. Interestingly, 65.2% (n=58) of clients stated that they did not have good access to the health-care centers.
Discussion
The present study evaluated the process of EINCP implementation in Tabriz, Iran. We found that the program’s overall reach and exposure rates of clients to the program were 20.0% and 77.5%, respectively, considered inadequate (program target 90%). Although the primary training sessions were largely delivered to providers as intended (100%), most planned services for clients were poorly implemented and had some important weaknesses. An overall low level of implementation fidelity was observed from perspectives of both clients and providers. The satisfaction rate of the clients with various parts of the EINCP was varied: 42.8% reported high satisfaction with the overall program. The program also suffered from some external barriers, such as lack of financial support of responsible centers.
The results of the current process evaluation illustrate that a main problem with the EINCP has been inadequate and irregular attendance of clients. The reported reach of the evaluated program (20%) was considered low. In line with our study, low reach has also been reported in other health-related intervention programs for the elderly.25,26 A health intervention for Brazilian elderly reported a reach of 17.2%.27 Another study reported that low attendance of clients at nutrition-education and PA sessions was largely due to inadequate attention of trainers or coaches paid to activities of participants.28 In the current study, some clients stated that the prescribed physical activities were not suitable for their health conditions and they sometimes experienced difficulties in carrying them out. In addition, they reported that the content of the education sessions was poor and did not meet their needs. In addition, the sessions were deemed were not informative or interesting enough, as most clients stated that they were unwilling to participate in the sessions due to low motivation. As such, it is suggested that customized support for each elder individual should be taken into consideration in order to promote the presence of older adults in education and PA sessions at the health-care centers. The low availability of health-care centers for the elderly was another factor affecting the reach of the EINCP. The availability of locally accessible programs with quick and easy access for all target individuals is one of the main strategies helping providers to get closer to desired outcomes.29 Policy-makers should design efficient programs to ensure that participants follow the intervention, and the program would gain in compliance.
Compared to the high delivery rate of the program to providers, program delivery to the clients had some shortcomings, as follow-up sessions, number and duration of nutrition-education and PA sessions, and vitamin or mineral supplementation did not go as planned. In contrast to the current study, process evaluations in Nigeria and the US have shown a delivery rate of 100%.30,31 In the current study, several factors may have contributed to the low level of delivery, including insufficient time on the part of the providers and lack of attention to providers’ specialties. It is speculated that poor delivery of the program components might have resulted in diminished EINCP effects, as confirmed by another study.32
Although all clients were familiar with the health-care centers of their resident area, 22.5% reported no exposure to the EINCP. In this study, the principal strategy to inform the elderly about the EINCP was telephone calls; however, this approach did not sufficiently raise awareness of the target group. There was no comprehensive information on nutritional services provided to the elderly, ie, many people regarded the health centers as a place to provide first-level services to children and pregnant women. Raising awareness of the target group about their needs is a key plank of the public health approach to health care.33 It is suggested that program providers invest in raising residents’ awareness of the EINCP by using appropriate and varied methods.
Although 42.8% of clients were satisfied with the providers’ performances and 58.5% were satisfied with overall EINCP services available, there were still some shortcomings in the satisfaction of the clients with some services, including education and PA sessions, as well as supplementation and follow-up sessions. A high percentage of providers were adequately motivated to their assigned tasks; however, they reported many barriers related to the program. Many providers had not received enough training in the field of elder care and reported not having adequate time. It is recommended that health centers use senior educated staff with more experience in elder care. It is also recommended to employ more related staff to meet the needs of the elderly.
Conclusion
According to the findings of the current study, reach, exposure, and fidelity of the program and delivery of some services were not implemented as planned, resulting in a low level of client satisfaction. Fidelity of program implementation, especially education materials, should be revisited for quality enhancement, and more resources should be allocated to improve the delivery rate. Additionally, it is necessary to improve financial support to the responsible centers and to increase awareness among the elderly and their families. Strategies related to recruitment of the target population should be improved, in order to minimize the barriers highlighted in this study. These findings may be beneficial in guiding public health policy-makers to design and successfully implement national-level public health interventions in developing countries. It is vital to note the importance of considering the perspectives of both clients and providers to ensure the achievement of expected outcomes and impacts of any public health-intervention programs.
Abbreviations
EICP, elderly integrated–care program; EINCP, elderly integrated nutrition–care program.
Data-Sharing Statement
The data gathered and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all study participants. The protocol was approved by the ethical committee of Tabriz University of Medical Sciences, Tabriz, Iran IR.TBZMED.REC.1397.1018). The anonymity and confidentiality of participants were assured and their decision to participate voluntarily in this study respected.
Acknowledgments
The results of this article are derived from the PhD thesis of the first author, registered at Tabriz University of Medical Sciences, Tabriz, Iran.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflict of interest.
References
1. United Nations. Ageing. 2019. Available from: https://www.un.org/en/sections/issues-depth/ageing/.
2. Cole J. The Demographic Transition. Planetary Health: Human Health in an Era of Global Environmental Change. CABI; 2019:54–57.
3. Zimmer Z, McDaniel S. Global Ageing in the Twenty-First Century: An Introduction. Global Ageing in the Twenty-First Century. Routledge; 2016:21–32.
4. World Health Organization. Ageing and life course. 2019. Available from: www.who.int/ageing/age_friendly_cities/en/index.html.
5. World Health Organization. The Global Burden of Disease: 2004 Update. Geneva: WHO Press; 2008:3–110.
6. Wilson BS, Tucci DL, Merson MH, O’Donoghue GM. Global hearing health care: new findings and perspectives. Lancet. 2017;390(10111):2503–2515. doi:10.1016/S0140-6736(17)31073-5
7. Whittaker AC, Asamane EA, Aunger JA, et al. Physical activity and nutrition INfluences in ageing: current findings from the PANINI project. Adv Geriatr Med Res. 2019;1:1–38.
8. Carey R, Caraher M, Lawrence M, Friel S. Opportunities and challenges in developing a whole-of-government national food and nutrition policy: lessons from Australia’s National Food Plan. Public Health Nutr. 2016;19(1):3–14. doi:10.1017/S1368980015001834
9. Warren AM, Frongillo EA, Alford S, McDonald E. Taxonomy of seniors’ needs for Food and Food Assistance in the United States. Qual Health Res. 2020;30(7):988–1003. doi:10.1177/1049732320906143
10. Bergia III RE, Jun S, Byers A, Savaiano D. Overhauling nutrition assistance programs to provide comprehensive nutrition support for older adults. Nutr Today. 2020;55(1):30–37. doi:10.1097/NT.0000000000000395
11. Sheats JL, Winter SJ, King AC. Nutrition Interventions for Aging Populations. Handbook of Clinical Nutrition and Aging. Springer; 2015:3–19.
12. Sadarangani TR, Beasley JM, Yi SS, Chodosh J. Enriching nutrition programs to better serve the needs of a diversifying aging population. Fam Community Health. 2020;43(2):100–105. doi:10.1097/FCH.0000000000000250
13. United Nations. World Population Ageing. Department of Economic and Social affairs; 2019. https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf.
14. Lankarani KB, Alavian SM, Peymani P. Health in the Islamic Republic of Iran, challenges and progresses. Med J Islam Repub Iran. 2013;27(1):4.
15. Gharaee H, Tabrizi JS, Azami-Aghdash S, Farahbakhsh M, Karamouz M, Nosratnejad S. Analysis of public-private partnership in providing primary health care policy: an experience from Iran. J Prim Care Community Health. 2019;10:1–17. doi:10.1177/2150132719881507
16. Sajadi HS, Ehsani-Chimeh E, Majdzadeh R. Universal health coverage in Iran: where we stand and how we can move forward. Med J Islam Repub Iran. 2019;33:9.
17. Nayeri ND, Abazari F, Pouraboli B. Challenges in caring for the elderly in Iran: a systematic review. Ethiop Med J. 2018;56:2.
18. Statistical Center of Iran. Population and housing censuses. 2016. Available from: https://www.amar.org.ir/english/Population-and-Housing-Censuses.
19. Hughes R, MargarettsMM. Practical Public Health Nutrition. Wiley-Blackwell; 2010:193–206.
20. Linnan L, Steckler A. Process Evaluation for Public Health Interventions and Research. Jossey-Bass San Francisco; 2002:5–10.
21. Baranowski T, Stables G. Process evaluations of the 5-a-day projects. Health Educ Behav. 2000;27(2):157–166. doi:10.1177/109019810002700202
22. Wong EY, Lee AH, James AP, Jancey J. Process evaluation of the ‘Singapore physical activity and nutrition study’. Eval Program Plann. 2020;10:1–27.
23. Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity. Res Social Adm Pharm. 2019;15(2):214–221. doi:10.1016/j.sapharm.2018.03.066
24. Rea J, Walters K, Avgerinou C. How effective is nutrition education aiming to prevent or treat malnutrition in community-dwelling older adults? A systematic review. Eur Geriatr Med. 2019;1–20.
25. Røyset B, Talseth-Palmer BA, Lydersen S, Farup PG. Effects of a fall prevention program in elderly: a pragmatic observational study in two orthopedic departments. Clin Interv Aging. 2019;14:145. doi:10.2147/CIA.S191832
26. Gille D, Bütikofer U, Chollet M, et al. Nutrition behavior of the middle-aged and elderly: compliance with dietary recommendations of the food pyramid. Clin nutr. 2016;35(3):638–644. doi:10.1016/j.clnu.2015.04.002
27. Borges RA, Tomicki C, Almeida FA, Schwingel A, Chodzko-Zajko W, Benedetti TRB. Reach of “VAMOS” program in basic healthcare-organizational barriers and facilitators. Rev Bras Geriatr Gerontol. 2019;22(3):2–11. doi:10.1590/1981-22562019022.180225
28. Stewart AL, Grossman M, Bera N, et al. Multilevel perspectives on diffusing a physical activity promotion program to reach diverse older adults. J Aging Phys Act. 2006;14(3):270–287. doi:10.1123/japa.14.3.270
29. Gerage AM, Benedetti TRB, Ritti-Dias RM, Dos Santos ACO, De Souza BCC, Almeida FA. Effectiveness of a behavior change program on physical activity and eating habits in patients with hypertension: a randomized controlled trial. J Phys Act Health. 2017;14(12):943–952. doi:10.1123/jpah.2016-0268
30. Bello TK, Gericke GJ, MacIntyre UE. Development, implementation, and process evaluation of a theory-based nutrition education programme for adults living with HIV in Abeokuta, Nigeria. Front Public Health. 2019;7:1–8. doi:10.3389/fpubh.2019.00030
31. Hatsu I, Campa A, Johnson P, Huffman F, Thomlison B, Baum M. Nutrition education intervention for low-income human immunodeficiency virus-infected adults. J Behav Health. 2014;3:161–168. doi:10.5455/jbh.20140726034114
32. Elliott DS, Mihalic S. Issues in disseminating and replicating effective prevention programs. Prev Sci. 2004;5(1):47–53. doi:10.1023/B:PREV.0000013981.28071.52
33. Seymour J. The impact of public health awareness campaigns on the awareness and quality of palliative care. J Palliat Med. 2018;21(S1):30–36. doi:10.1089/jpm.2017.0391
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.