")
Back to Journals » Journal of Pain Research » Volume 8
Priority interventions to improve the management of chronic non-cancer pain in primary care: a participatory research of the ACCORD program
Authors Lalonde L, Choinière M , Martin E, Lévesque L, Hudon E, Bélanger D, Perreault S, Lacasse A , Laliberté M
Received 26 November 2014
Accepted for publication 18 December 2014
Published 30 April 2015 Volume 2015:8 Pages 203—215
DOI https://doi.org/10.2147/JPR.S78177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael Schatman
Lyne Lalonde,1–4 Manon Choinière,3,5 Elisabeth Martin,3 Lise Lévesque,3 Éveline Hudon,2,3,6 Danielle Bélanger,2 Sylvie Perreault,1,7 Anaïs Lacasse,8 Marie-Claude Laliberté1,9
1Faculty of Pharmacy, Université de Montréal, Montreal, QC, Canada; 2Équipe de recherche en soins de première ligne, Centre de santé et de services sociaux de Laval, Laval, QC, Canada; 3Centre de recherche, Centre hospitalier de l'Université de Montréal (CRCHUM), Montreal, QC, Canada; 4Sanofi Aventis Endowment Chair in Ambulatory Pharmaceutical Care, Faculty of Pharmacy, Université de Montréal and Centre de santé et de services sociaux de Laval, QC, Canada; 5Department of Anesthesiology, Faculty of Medicine, Université de Montréal, Montreal, QC, Canada; 6Department of Family Medicine and Emergency, Faculty of Medicine, Université de Montréal, Montreal, QC, Canada; 7Sanofi Aventis Endowment Chair in Drug Utilization, Faculty of Pharmacy, Université de Montréal, Montreal, QC, Canada; 8Département des sciences de la santé, Université du Québec en Abitibi-Témiscamingue, Rouyn-Noranda, QC, Canada; 9AbbVie Corporation, St-Laurent, QC, Canada
Purpose: There is evidence that the management of chronic non-cancer pain (CNCP) in primary care is far from being optimal. A 1-day workshop was held to explore the perceptions of key actors regarding the challenges and priority interventions to improve CNCP management in primary care.
Methods: Using the Chronic Care Model as a conceptual framework, physicians (n=6), pharmacists (n=6), nurses (n=6), physiotherapists (n=6), psychologists (n=6), pain specialists (n=6), patients (n=3), family members (n=3), decision makers and managers (n=4), and pain researchers (n=7) took part in seven focus groups and five nominal groups.
Results: Challenges identified in focus group discussions were related to five dimensions: knowledge gap, “work in silos”, lack of awareness that CNCP represents an important clinical problem, difficulties in access to health professionals and services, and patient empowerment needs. Based on the nominal group discussions, the following priority interventions were identified: interdisciplinary continuing education, interdisciplinary treatment approach, regional expert leadership, creation and definition of care paths, and patient education programs.
Conclusion: Barriers to optimal management of CNCP in primary care are numerous. Improving its management cannot be envisioned without considering multifaceted interventions targeting several dimensions of the Chronic Care Model and focusing on both clinicians and patients.
Keywords: chronic pain, community-based participatory research, health service accessibility, patient-centered care, primary health care
Introduction
In Canada, approximately 25% of the population suffers from chronic non-cancer pain (CNCP).1 This disorder is associated with anxiety, depression, reduced productivity, and increased health care costs.1–5 Patient satisfaction regarding treatment efficacy and information on treatment is low.6 Current clinical guidelines for CNCP recommend multifaceted interventions delivered by various health professionals, including primary care physicians, pharmacists, nurses, physiotherapists, kinesiologists, and psychologists.7–11 Recent studies indicate chronic pain is often undertreated, and management practices do not always conform to current practice guidelines.12–18
Considering CNCP as a chronic disease, its management could be addressed through the use of the Chronic Care Model (CCM),19 a multi-dimensional guide to designing effective chronic care.20 The CCM recommends building chronic health care based on six dimensions, namely: 1) self-management support; 2) delivery system design; 3) decision support; 4) clinical information systems; 5) community resources and policies; and 6) health care organization. Positive effects on care processes and clinical outcomes of CCM-based interventions have been reported.21,22 However, the CCM is a general model, each dimension can be addressed in several alternative ways, and there is no evidence-based algorithm to determine how to prioritize and translate these elements into specific interventions adapted to a particular clinical context. To our knowledge, the CCM has also never been explicitly used to specifically improve CNCP management in primary care.19
When designing knowledge translation interventions based on practice guidelines, it is recommended to address the specific challenges and the context of care.23 Participatory research approaches involving primary care actors have also been recommended to learn about potential challenges to optimal disease management.24,25 These approaches could thus be used to translate CCM dimensions and practice guidelines into interventions that meet the needs of patients and family members, are appropriate to the context of primary care, and appeal to clinicians. A participatory workshop has previously been used to identify challenges of and priority interventions inspired by the CCM for improving cardiovascular disease prevention in primary care.25
We therefore organized a 1-day workshop involving members of the primary care and pain management community, including patients and family members, with the objective to identify challenges to optimal CNCP management, as posited by the CCM, and to identify priority interventions to improve its management in primary care. In this article, we report the results of this participatory workshop. These results will be used to develop and assess an intervention program in primary care, as part of a broader research program aiming at improving the management of CNCP – ie, the program ACCORD.
Methods
Participant recruitment and sampling
Physicians (n=6); pharmacists (n=6); nurses (n=6); physiotherapists (n=6); psychologists (n=6); pain specialists (n=6); patients (n=3); family members (n=3); decision makers and managers (n=4); and pain researchers (n=7) were recruited to participate in a 1-day workshop held in Laval, Quebec, Canada, on April 30, 2010. Pain specialists included one physician, one psychologist, one nurse, one pharmacist, one kinesiologist, and one physiotherapist, all of them being actively involved in following patients with CNCP in the primary sector of care. All the participants (total =53) were purposively selected, based on their general experience in primary care and chronic pain. Participants of each category were recruited to represent diverse contexts of care in various regions of the Province of Quebec (Montréal, Laval, Mauricie, Montérégie, Lanaudière, and Laurentides) and clinical settings (family medicine groups, conventional medical clinics, family medicine units, and local community service centers) through the Réseau universitaire intégré de santé (RUIS) of the Université de Montréal. Decision makers and managers working within a health and social services center (Centre de santé et de services sociaux, CSSS) or a health and social services agency (Agence de la santé et des services sociaux, ASSS) were selected based on their role and active involvement in health care organization. Pain researchers were selected by the principal investigators and co-investigators. We partnered with the Quebec Association for Chronic Pain (Association québécoise de douleur chronique) and Quebec Federation of Seniors (Fédération de l’âge d’or du Québec) to recruit patients and family members. In addition, clinicians could also refer their eligible patients for participation in this study. Patients recruited met with six inclusion criteria: 1) be 18 years or older; 2) reported CNCP for at least 6 months; 3) felt pain at least twice a week; 4) reported an average pain intensity in the past 7 days of at least 4 on a 0–10 intensity numerical scale (0= no pain; 10= the worst possible pain);26 5) had an active prescription from a primary care physician for one or more pain medication; and 6) spoke and understood French. Patients were excluded if they met any of the following criteria: 1) suffered cancer-related pain; 2) reported having only migraines or chronic headaches; or 3) had a disabling physical or mental disorder that prevented giving informed consent and/or active participation in the workshop.
This participatory research was approved by the Research Ethics Committee of the Centre de santé et de services sociaux de Laval. All participants signed an informed consent form. A CAD $500 financial compensation was offered to all participants except researchers, decision makers and managers. Transportation and hotel accommodation were paid for participants from outside Montreal.
Workshop
The workshop included three sets of activities: 1) presentation of the current management strategies in primary care; 2) focus group discussions; and 3) nominal group discussions.27 The workshop schedule and descriptions of activities are shown in Figure 1. The composition of the focus and nominal groups was predetermined by pain researchers, based on participant expertise and experience. All discussions were audio-recorded and were conducted by qualitative-research professionals from the Ad hoc Research firm who acted as facilitators.
 | Figure 1 Workshop schedule and descriptions of activities. |
Presentation of the current management strategies of CNCP in primary care
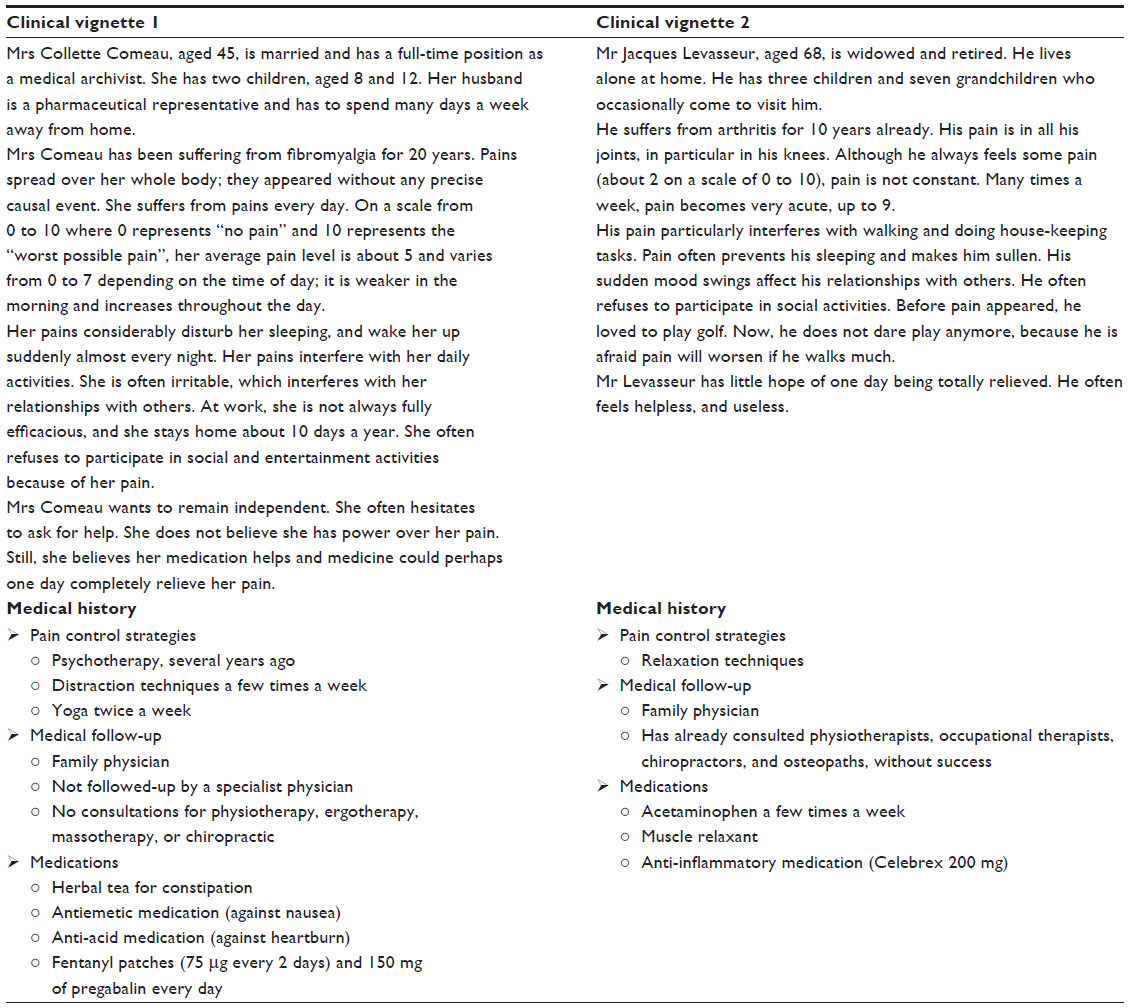
All participants attended a 30-minute presentation summarizing the results of a cohort study, performed in primary care in Quebec during Phase I of the program ACCORD.6,28,29 The presentation emphasized complexity of the health profile of patients followed-up in primary care for chronic pain, practice gaps, as well as the relatively low level of pain knowledge, inappropriate attitudes and beliefs of clinicians regarding CNCP, and low levels of patient satisfaction. Physical, psychosocial, and economic impacts of chronic pain were also evidenced. In addition, participants were provided with two clinical vignettes describing typical primary care CNCP patients (Supplementary material). They were asked to keep in mind the above results and these two clinical vignettes throughout the rest of the workshop.
Focus group discussions
A total of seven parallel focus groups were conducted. Each group included a decision maker, a researcher, and six other participants from the same discipline (eg, primary care physicians) or profile (eg, patients). The homogenous grouping of participants allowed them to voice innovative suggestions for interventions pertaining to their own clinical practice or experience. Within each CCM-related domain, participants were asked to: 1) indicate what they perceived as the most important challenges in CNCP management; and 2) propose specific interventions or practice changes to improve CNCP management. Organization of care and services delivery had to be discussed first in all groups. For each group, pain researchers purposively pre-selected and pre-assigned two additional CCM-related domains for discussion, taking into consideration participant preference and expertise (Table 1). Participants were provided with a list of possible interventions for the two clinical vignettes corresponding to each CCM domain. In a plenary session, each facilitator summarized the discussed challenges and proposed interventions.
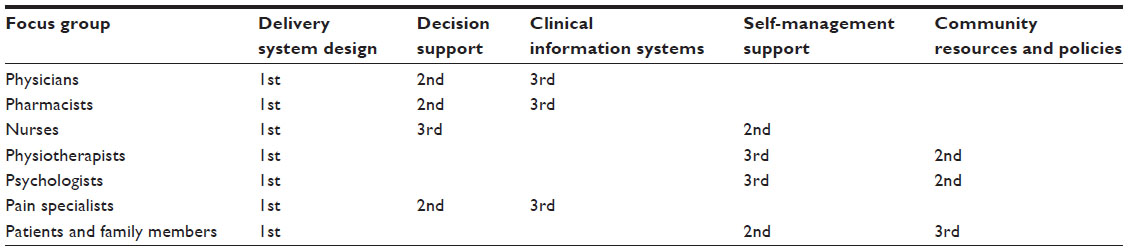 | Table 1 Order of domains of the Chronic Care Model discussed in each focus group |
Nominal group discussions
Five nominal groups, each including all types of participants, were formed to identify priority interventions to improve the management of CNCP. Nominal groups went through a four step process (Figure 1). Steps 1 to 3 were conducted within each of the five nominal groups while step 4 involved all participants in a plenary session. Step 1 – priority intervention proposals: all participants were asked to select three interventions and order them in terms of priority. The facilitator listed all the collected interventions on a large board, and led discussions with the participants to pool similar interventions and clarify them if needed. Step 2 – first vote: each participant had to select five priority interventions from the list and scored them by distributing 100 points according to their importance. An intervention could be given 0 to 100 points by each participant (0= not important, 100= very important). The total number of points distributed by each participant could not exceed 100. Facilitator calculated the “total score” of each intervention – ie, the sum of all points all participants had given to an intervention. The number of “votes” for each intervention was also calculated. A top ten list of interventions was made based on the total score. In order to have an understanding of the justification of the scores and votes, participants were asked to voice their opinion on the list and explain their rating. Step 3 – second vote: participants were asked to select five priority interventions in the previous top ten list, and to distribute 100 points according to their relative importance. The facilitator calculated total scores and votes, and listed top five interventions based on total score. Step 4 – third vote: in a plenary session, each facilitator (acting as representative of the five nominal groups) presented their top five interventions to all participants. Interventions from all five nominal groups were pooled together, and equivalent interventions were merged. At the end of the process, there were 12 single interventions. For the last time, all participants were asked to rate five priority interventions among the 12, by distributing 100 points to those five interventions. The total score and number of votes of each priority intervention were calculated.
Analyses
Focus group discussions at step 1, intervention proposals, scores and votes made in each nominal group at step 2, the five priority interventions selected in each nominal group at step 3, and the results of step 4 were summarized. Priorities identified in step 4, were classified by researchers in broader themes. Thereafter, thematic qualitative analyses30 were done manually. Priorities were retrospectively used to thematically review the nominal and focus group audio-recordings to gain a better understanding of the reasons for which those priorities were selected.
Results
Participation of the primary care community
As mentioned earlier, 53 members of the primary care community (clinicians, managers, patients, family members, and researchers) took part in this participatory research. Table 2 describes their respective background, the region they came from, and the work environment of the health care professionals and managers. All participants attended the initial presentation and participated in the focus and nominal groups.
 | Table 2 Participants’ characteristics |
Challenges to pain management in primary care
In focus group discussions, participants identified challenges related to five dimensions: 1) knowledge gap; 2) “work in silos”; 3) lack of awareness that CNCP represents an important clinical problem; 4) difficulties in access to health professionals and services; and 5) patient empowerment needs. The right panel of Table 3 shows illustrative quotes for each dimension.
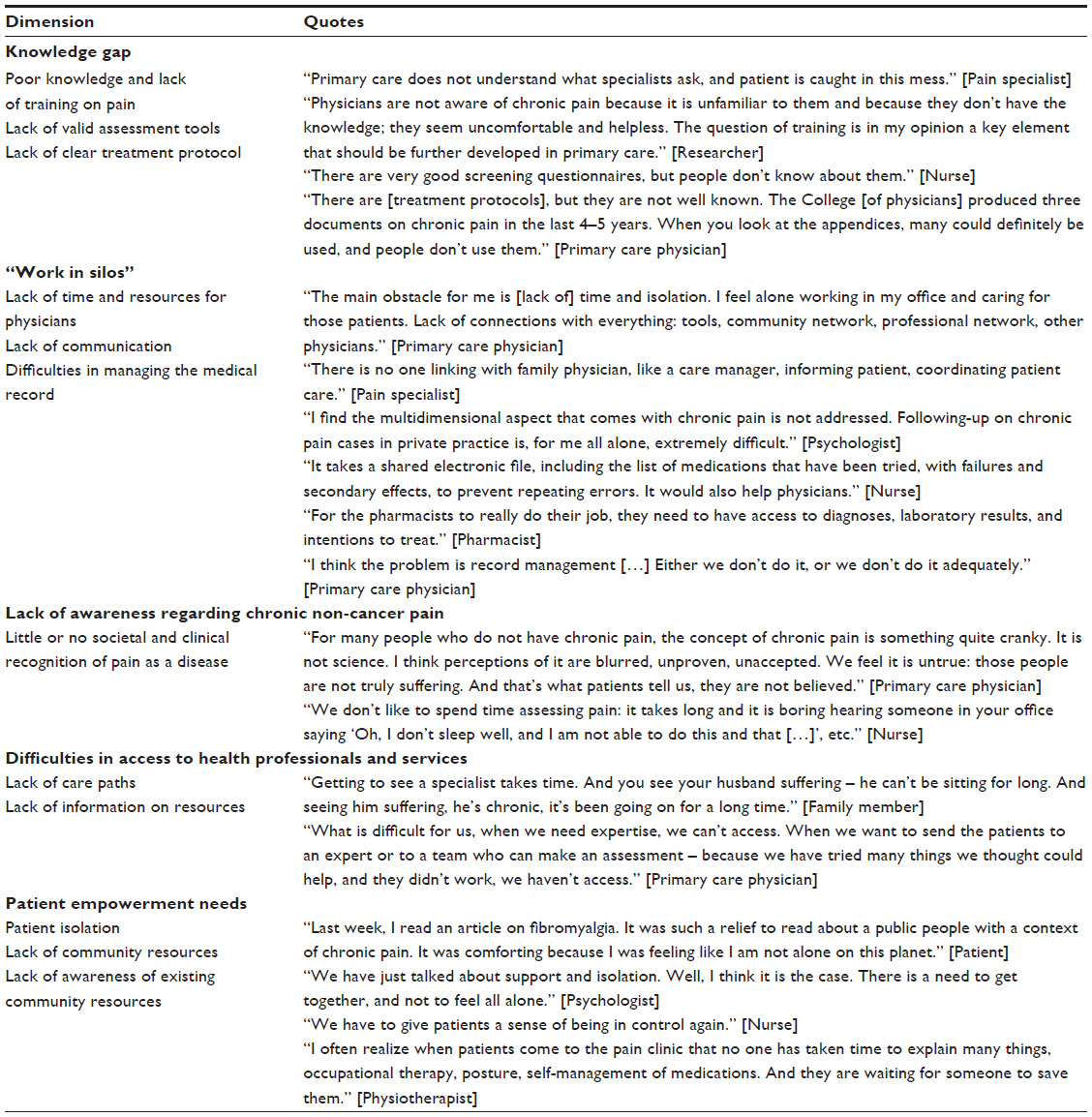 | Table 3 Challenges in the management of chronic non-cancer pain in primary care, grouped by dimension, with illustrative participants’ quotes for each dimension |
Participants reported a knowledge gap in CNCP in primary care due to a lack of clinician training and continuing education and of supportive tools to assess and treat CNCP in primary care. Difficulties to organize interdisciplinary care in current clinical settings were also reported. Some participants believed practice guidelines are missing for CNCP management. However, some participants pointed out that such guidelines and tools do exist but many health care professionals have a limited knowledge of them. One more challenge to CNCP management is “work in silos” where clinicians feel isolated and unsupported. The situation is exacerbated by poorly implemented clinical information systems and the absence of feedback on patient follow-up by other health professionals.
The results also showed that there was a lack of awareness of CNCP as an important clinical problem among clinicians. Pain is difficult to diagnose, and there is a perception that the definitions and causes of various types of chronic pain are blurred or unproven. Providing care to patients with chronic pain is time consuming, and there is also a suspicion that patients may fake or exaggerate their pain.
The participants further reported that many difficulties in access to health professionals and services, and to community resources are due to the lack of clearly defined care paths and limited information on available resources like pain specialists and multidisciplinary pain treatment clinics. In addition, clinicians are unaware of community resources for pain management. Finally, patients continue to be viewed (or view themselves) as care consumers rather than active partners in their treatment. Patients’ empowerment needs are not addressed, and many of them are unaware of basic self-management strategies that could contribute to improve their pain. Furthermore, available health care facilities and community resources are often unknown to the patients and their family members. As a result, patients feel isolated, helpless, and out of control.
Priority interventions for better pain management in primary care
Table 4 shows the 12 priority interventions selected by all nominal groups. Interventions are classified in six themes. Under each theme, interventions are ordered by total score and by number of votes obtained in the final plenary session. An illustrative quote for each priority intervention is provided on the right panel.
 | Table 4 Priority interventions identified grouped by intervention theme, with total score, votes and illustrative participant’s quote for each priority intervention |
Participants recommended developing joint continuing education programs. They should be offered simultaneously to clinicians of various disciplines in order to standardize their knowledge, to get the opportunity to know each other and their respective area of expertise, and to develop a common language. For example, the use of pain scales should be a standard across disciplines to harmonize evaluation and communication of clinical information on pain. Standardized tools such as interdisciplinary electronic records need to be implemented, and clinicians should be trained to use them optimally and appropriately. Clinical expertise should also be enhanced by facilitating patient and clinician access to instruments that are aligned with current clinical guidelines, and by providing electronic decision-support tools.
With regards to the interdisciplinary approach, participants believed primary care nurses should be trained in pain management to support the interdisciplinary approach. It was recommended to widen the range of professional responsibility of clinicians other than the physician to ensure access to and affordability of pain management. Pain diagnoses should be complemented with psychosocial assessments to identify patient needs so as to treat co-morbidities commonly associated with chronic pain (eg, anxiety or depression).
Participants recommended identifying regional pain experts (“champions”) who could disseminate knowledge and bring support to clinicians when needed. Additional training and support need to be offered to these experts on efficient knowledge dissemination strategies and outreach techniques.
Defining care paths in terms of corridors of services across the continuum of care was also recommended. It is a complex process that requires the involvement of primary, secondary, and tertiary care actors to come up with agreements on referral and follow-up modalities.
In order to develop a greater sense of being in control, patients should be involved as active partners in their treatment and taught pain self-management strategies through individual or group education sessions. Patients’ pain-logbook was recommended to support self-monitoring of their disease and improve communication with the different health care professionals.
Discussion
Various types of primary care actors, including patients and family members, took part in this participatory research and contributed to identifying challenges to chronic pain management in primary care along with priority interventions to overcome them. The main challenges included knowledge gap, “work in silos”, lack of awareness regarding chronic pain, difficulties in access to health professionals and services, and to increase patients’ empowerment.
Participants recommended patient-centered interventions aligned with five dimensions of the CCM. To empower patients, it was proposed to promote their active participation in treatment through patient education and to use a paper or web pain-logbook for both patients and clinicians. Improving delivery system design through interdisciplinary collaboration and team work was proposed, to be supported with decision-support tools (eg, standardized evaluation forms, updated guidelines) and clinical information systems (eg, electronic medical records). Interdisciplinary continuing education was also deemed necessary for clinicians to become familiar with use of such tools, and to develop interprofessional collaborative practices in pain management. Taking advantage of the leadership and peer support role of pain experts in the primary care community was also recommended. Participants probably considered that CNCP management need not be addressed by creating new structures in the health system, because they did not suggest any intervention at the level of health care organization.
Awareness and education are keys
While the societal and individual burden of chronic pain is increasingly recognized, the need to provide continuing education on pain management has been emphasized.31 In this research, participants thought credible chronic pain experts should be appointed in each region to take on clinical leadership in order to increase awareness of CNCP and its individual and social burden, to inspire a desire to aim at improving care for patients with CNCP, to disseminate knowledge, and to provide expertise to support other clinicians. A pilot study showed this approach is promising.32
In recent surveys, primary care clinicians demonstrated low levels of knowledge in the field of pain assessment and treatment, and voiced a need for supportive clinical tools and training.14,18 Those findings suggest that clinicians may have inappropriate beliefs on chronic pain, or feel insufficiently knowledgeable or supported to provide appropriate care and services. Participants in this workshop believed that interactive, interdisciplinary, patient-centered, continuing education programs are necessary to fill the knowledge gap, foster mutual acquaintance, develop common discourses among health professionals and thereby, ensure appropriate transmission of information among clinicians. University faculties have developed interdisciplinary education programs, but those programs are usually not available in interdisciplinary continuing education.29,33–35 However, these training programs by themselves are probably insufficient to improve the process, quality and coordination of care, if one wants to improve chronic pain management in primary care.36
Patient empowerment is the overarching priority
While there are prejudices and preconceived ideas about chronic pain and its treatment in the general population and in the health care system as well,37 many patients with CNCP also have erroneous beliefs and judgmental attitudes regarding their disease. Patients may hide their disease and avoid taking pain killers, an attitude they associate with courage and self-control.38,39 Others constantly look for the “magic” pill or treatment while it is well established that a combination of therapeutic modalities is more likely to be successful. Patient education programs along with provision of self-management strategies are needed to empower patients and thereby confer on them a role of active partner in their treatment rather than simply a consumer of care.
Interdisciplinary collaboration is necessary for better care
It is generally thought that increasing interdisciplinary collaboration will suppress useless intermediary steps, and will improve care. The efficacy of nurse-led pain management in primary care has been demonstrated.40 A study suggests pharmacist-nurse collaboration in chronic pain management could improve patient outcomes and experience, and optimize resource use.41 Pharmacist-led interventions (eg, medication review) are promising and more research is needed to support expanding roles for pharmacists in pain management.42 Psychologist-physician collaboration is modestly but significantly more efficient for CNCP management than usual care.43 Timely referrals to consultations for back and neck pain with physiotherapist, chiropractor, or osteopath improve patient self-management and satisfaction, and allow reduction of medication and primary care consultations.44 Interdisciplinary collaboration requires increasing professional autonomy of non-physician clinicians and redefining their roles in consultation with physicians, other clinicians, and health authorities concerned, which currently are major issues in health care policy in Canada.45 Participants in this study recommended the use of clinical tools such as collective prescriptions to support interprofessional collaboration.
Partnerships are essential to ensure access to care
Access to and waiting time for consultation in multidisciplinary pain treatment clinics are problematic in Canada.46 Median waiting time in Canada is 6 months (ranging from 2 to 14) in 2007.46 A study involving more than 700 patients on waitlists of large university-affiliated pain clinics across Canada has highlighted the severe impairment these patients experience in terms of pain intensity and interference, psychological distress (depression and suicidal ideation, anxiety, anger), and poor quality of life.47 The economic burden of chronic pain has also been shown to be substantial in patients on waitlists of multidisciplinary pain clinics. The mean monthly cost has been estimated at CAD $3,112 per patient.48 Deficient interdisciplinary communication across the continuum of care may explain a part of problems experienced with patient referrals and prioritization along with delayed treatments.49
In 2009, as an attempt to solve this problem and help lift the burden of CNCP, the Quebec Health Ministry designated four Pain Centers of Expertise (PCE) across the province with the mandate of improving the management of chronic pain by implementing an integrated and hierarchical continuum of services. Each PCE includes: 1) one or more tertiary care multidisciplinary pain treatment clinic affiliated with one tertiary care rehabilitation center; 2) designated regional secondary pain clinics; and 3) designated local primary care clinics. A series of corridors of services covering the three sectors of care have been or are in the process of being established within each PCE. In addition, a provincial committee involving the PCE medical directors, their coordinators, clinicians, managers, and decision makers of the Health Ministry is mandated to develop common and uniform strategies to improve accessibility, continuity, complementarity, and quality across all sectors of care as well as to reduce variability in the clinical practices and improve process management. These initiatives include: 1) implementation of standardized consultation forms; 2) provision of evidence-based practice guidelines for the treatment of various types of CNCP syndromes and patient clinical pathways across the continuum of care; 3) provision of a formal telephone consultation service for family physicians who wish to discuss cases with pain specialists; 4) production of a patient health care booklet; 5) directory of pain self-management programs available in the community; and 6) introduction of new communication tools including the creation of intranet websites.
Qualitative and participatory methods: strengths and limitations
Our conclusions are compatible with those of another participatory research study on CNCP management in primary care where implementing treatment guidelines and clinical tools, improving processes for opioid prescription renewals, enhancing patient self-management, and involving care managers in primary settings were recommended.19 However, that study used a Delphi method and involved only physicians and care managers. In contrast, we used focus and nominal group discussions to involve a broader range of actors concerned with chronic pain management in primary care with the aim of developing an intervention for CNCP management inspired by the CCM and adapted to the context of this sector of care. We were able to have participants from ten of 17 of Quebec’s administrative regions, in rural and urban areas.
In focus group discussions, participants could share their views with peers. The inclusion of patients and family members in mixed, balanced, facilitated, and non-judgmental nominal groups of primary care actors is an innovative aspect of our research. Nominal group discussions allowed participants to make and be exposed to a wide range of creative proposals, and then select the most relevant by voting on and ranking proposed interventions. The nominal group technique is generally seen as unthreatening and depersonalized,27 and is therefore suitable to raise the expression of minority opinions. Participants had multiple occasions to hear suggestions and arguments put forward by other members of the groups, and thus elaborate a critical reconsideration of their initial views. Nevertheless, the findings of this qualitative and participatory research are context-bound and participants were purposively selected and may not be representative of the entire population. Results must be interpreted in the context of the primary care experienced in Quebec, Canada.
Conclusion
Lack of awareness that CNCP constitutes an important clinical problem coupled with the presence of knowledge gaps in the assessment and management of this type of disorder represent major barriers to the establishment of interdisciplinary collaboration and patient-centered shared care. Pain education needs of both patients and clinicians must therefore be addressed. For carers, interdisciplinary training should help in developing common basic knowledge and shared language that will allow them to provide patients with appropriate treatment. Teaching self-management strategies to patients is crucial to emphasize the importance of optimal self-care, increase empowerment, and make them active partners within the clinical team. These results may constitute a starting point toward the development and implementation of new policies for the management of chronic pain patients in primary care and are of wide interest not only for the community but also for all the health professionals dealing with these patients.
Research funding
Canadian Institutes of Health Research (CIHR) in partnership with AstraZeneca, Pfizer Canada Inc., Janssen-Ortho, Merck Frost Canada Ltd, and Purdue Pharma.
Disclosure
Marie-Claude Laliberté is an employee of AbbVie Corporation and owns AbbVie shares. At the time of analysis, she was a PhD student in pharmaceutical sciences at Université de Montréal. The other authors have no conflicts of interest to declare.
References
Boulanger A, Clark AJ, Squire P, Cui E, Horbay GL. Chronic pain in Canada: have we improved our management of chronic noncancer pain? Pain Res Manag. 2007;12(1):39–47. | |
Reed C, Hong J, Novick D, Lenox-Smith A, Happich M. Health care costs before and after diagnosis of depression in patients with unexplained pain: a retrospective cohort study using the United Kingdom General Practice Research Database. Clinicoecon Outcomes Res. 2013;5:37–47. | |
Watson L, Baird J, Hosel V, Peveler R. The effect of concurrent pain on the management of patients with depression: an analysis of NHS healthcare resource utilisation using the GPRD database. Int J Clin Pract. 2009;63(5):698–706. | |
Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being: a World Health Organization Study in Primary Care. JAMA. 1998;280(2):147–151. | |
Rashiq S, Dick BD. Factors associated with chronic noncancer pain in the Canadian population. Pain Res Manag. 2009;14(6):454–460. | |
Jouini G, Choiniere M, Martin E, et al. Pharmacotherapeutic management of chronic noncancer pain in primary care: lessons for pharmacists. J Pain Res. 2014;7:163–173. | |
Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113–130. | |
Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(7):478–491. | |
Williams NH, Amoakwa E, Burton K, et al. The Hip and Knee Book: developing an active management booklet for hip and knee osteoarthritis. Br J Gen Pract. 2010;60(571):64–82. | |
Ho KY, Chua NH, George JM, et al. Evidence-based guidelines on the use of opioids in chronic non-cancer pain – a consensus statement by the Pain Association of Singapore Task Force. Ann Acad Med Singapore. 2013;42(3):138–152. | |
Frank JW, Bair MJ, Becker WC, Krebs EE, Liebschutz JM, Alford DP. Update in pain medicine for primary care providers: A narrative review, 2010–2012. Pain Med. 2014;15(3):425–431. | |
Williams CM, Maher CG, Hancock MJ, et al. Low back pain and best practice care: A survey of general practice physicians. Arch Intern Med. 2010;170(3):271–277. | |
McDonald DD, Walsh S. Older adult osteoarthritis pain management: Results from the 2008 National Ambulatory Medical Care Survey. J Am Acad Nurse Pract. 2012;24(2):107–112. | |
Porucznik C, Johnson E, Rolfs R, Sauer B. Opioid prescribing knowledge and practices: provider survey following promulgation of guidelines-Utah, 2011. J Opioid Manag. 2013;9(3):217–224. | |
Hall GC, Morant SV, Carroll D, Gabriel ZL, McQuay HJ. An observational descriptive study of the epidemiology and treatment of neuropathic pain in a UK general population. BMC Fam Pract. 2013;14:28. | |
Breuer B, Cruciani R, Portenoy RK. Pain management by primary care physicians, pain physicians, chiropractors, and acupuncturists: a national survey. South Med J. 2010;103(8):738–747. | |
Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern Med. 2013;173(17):1573–1581. | |
Allen MJ, Asbridge MM, Macdougall PC, Furlan AD, Tugalev O. Self-reported practices in opioid management of chronic noncancer pain: a survey of Canadian family physicians. Pain Res Manag. 2013; 18(4):177–184. | |
Clark LG, Upshur CC. Family medicine physicians’ views of how to improve chronic pain management. J Am Board Fam Med. 2007;20(5):479–482. | |
Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. 1998;1(1):2–4. | |
Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, part 2. JAMA. 2002;288(15):1909–1914. | |
Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the Chronic Care Model in the new millennium. Health Aff (Millwood). 2009;28(1):75–85. | |
Straus S, Tetroe J, Graham ID. Knowledge Translation in Health Care – Moving from Evidence to Practice. London: Wiley-Blackwell; 2009. | |
Leykum LK, Pugh JA, Lanham HJ, Harmon J, McDaniel RR Jr. Implementation research design: integrating participatory action research into randomized controlled trials. Implement Sci. 2009;4:69. | |
Lalonde L, Goudreau J, Hudon E, et al. Priorities for action to improve cardiovascular preventive care of patients with multimorbid conditions in primary care – a participatory action research project. Fam Pract. 2012;29(6):733–741. | |
Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23(2):129–138. | |
van de Ven AH, Delbecq AL. The nominal group as a research instrument for exploratory health studies. Am J Public Health. 1972;62(3):337–342. | |
Lalonde L, Choiniere M, Martin E, Berbiche D, Perreault S, Lussier D. Costs of moderate to severe chronic pain in primary care patients – a study of the ACCORD Program. J Pain Res. 2014;7:389–403. | |
Lalonde L, Leroux-Lapointe V, Choiniere M, et al. Knowledge, attitudes and beliefs about chronic noncancer pain in primary care: A Canadian survey of physicians and pharmacists. Pain Res Manag. 2014;19(5):241–250. | |
Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. | |
Breivik H, Eisenberg E, O’Brien T, OPENMinds. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health. 2013;13:1229. | |
Chelimsky TC, Fischer RL, Levin JB, Cheren MI, Marsh SK, Janata JW. The primary practice physician program for chronic pain ((c) 4PCP): outcomes of a primary physician-pain specialist collaboration for community-based training and support. Clin J Pain. 2013;29(12):1036–1043. | |
Allen M, Macleod T, Zwicker B, Chiarot M, Critchley C. Interprofessional education in chronic non-cancer pain. J Interprof Care. 2011;25(3):221–222. | |
Aston SJ, Rheault W, Arenson C, et al. Interprofessional education: a review and analysis of programs from three academic health centers. Acad Med. 2012;87(7):949–955. | |
Lundon K, Shupak R, Reeves S, Schneider R, McIlroy JH. The Advanced Clinician Practitioner in Arthritis Care program: an interprofessional model for transfer of knowledge for advanced practice practitioners. J Interprof Care. 2009;23(2):198–200. | |
Ospina MB, Taenzer P, Rashiq S, et al. A systematic review of the effectiveness of knowledge translation interventions for chronic noncancer pain management. Pain Res Manag. 2013;18(6):e129–e141. | |
The Ennis Centre for pain management. Ennis J. The Prejudice Against Chronic Pain. The Ennis Centre for pain management; 2008. Available from: http://www.enniscentre.com/wp-content/uploads/2012/04/Prejudice-again-chronic-pain.pdf. Accessed September 8, 2014. | |
Cornally N, McCarthy G. Chronic pain: The help-seeking behavior, attitudes, and beliefs of older adults living in the community. Pain Manag Nurs. 2011;12(4):206–217. | |
Allcock N, Elkan R, Williams J. Patients referred to a pain management clinic: beliefs, expectations and priorities. J Adv Nurs. 2007;60(3):248–256. | |
Courtenay M, Carey N. The impact and effectiveness of nurse-led care in the management of acute and chronic pain: a review of the literature. J Clin Nurs. 2008;17(15):2001–2013. | |
Briggs M, Closs SJ, Marczewski K, Barratt J. A feasibility study of a combined nurse/pharmacist-led chronic pain clinic in primary care. Qual Prim Care. 2008;16(2):91–94. | |
Hadi MA, Alldred DP, Briggs M, Munyombwe T, Closs SJ. Effectiveness of Pharmacist-led Medication Review in Chronic Pain Management: Systematic Review and Meta-analysis. Clin J Pain. 2014; 30(11):1006–1014. | |
Dobscha SK, Corson K, Perrin NA, et al. Collaborative care for chronic pain in primary care: a cluster randomized trial. JAMA. 2009; 301(12):1242–1252. | |
Gurden M, Morelli M, Sharp G, Baker K, Betts N, Bolton J. Evaluation of a general practitioner referral service for manual treatment of back and neck pain. Prim Health Care Res Dev. 2012;13(03):204–210. | |
Canadian Health Services Research Foundation. Oandasan I, Baker R, Bosco C, et al. Teamwork in Healthcare: Promoting Effective Teamwork in Healthcare in Canada – Policy Synthesis and Recommendations. Canadian Health Services Research Foundation; 2006. Available from: http://www.cfhi-fcass.ca/Migrated/PDF/ResearchReports/CommissionedResearch/teamwork-synthesis-report_e.pdf. Accessed February 23, 2015. | |
Peng P, Choiniere M, Dion D, et al. Challenges in accessing multidisciplinary pain treatment facilities in Canada. Can J Anaesth. 2007;54(12):977–984. | |
Choiniere M, Dion D, Peng P, et al. The Canadian STOP-PAIN project – Part 1: Who are the patients on the waitlists of multidisciplinary pain treatment facilities? Can J Anaesth. 2010;57(6):539–548. | |
Guerriere DN, Choiniere M, Dion D, et al. The Canadian STOP-PAIN project – Part 2: What is the cost of pain for patients on waitlists of multidisciplinary pain treatment facilities? Can J Anaesth. 2010;57(6):549–558. | |
Wåhlberg H, Valle PC, Malm S, Broderstad AR. Practical health co-operation – the impact of a referral template on quality of care and health care co-operation: study protocol for a cluster randomized controlled trial. Trials. 2013;7(14):7. |
Supplementary material
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.