")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 12
Primary Juvenile Sjögren’s Syndrome in a 3-Year-Old Pediatric Female Patient: Diagnostic Role of Salivary Gland Ultrasonography: Case Report
Authors Aburiziza AJ
Received 9 February 2020
Accepted for publication 13 May 2020
Published 29 May 2020 Volume 2020:12 Pages 73—78
DOI https://doi.org/10.2147/OARRR.S248977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Abdullah Jameel Aburiziza
Pediatric Department, Faculty of Medicine, Umm Al Qura University, Makkah, Saudi Arabia
Correspondence: Abdullah Jameel Aburiziza
Pediatric Department, Faculty of Medicine, Umm Al Qura University, Makkah, Saudi Arabia
Tel +966 530530940
Email [email protected]
Abstract: Sjögren’s syndrome (SS) is a chronic inflammatory autoimmune disease affecting mainly the salivary and lacrimal glands characterized by lymphocytic infiltration which results in gland destruction and impairment of functions. SS rarely affects pediatric patients, and there are no clear diagnostic criteria as there are with adult SS. The present case reports an atypical case of SS in a 3-year-old female who was closely followed up with for 5 years. The important role of salivary gland ultrasonography (SGUS) in early diagnosis, the change in clinical picture, as well as fluctuation of serology, are noticed.
Keywords: primary juvenile Sjogren’s syndrome, seronegative, salivary gland ultrasonography, autoimmune, anti-Ro
Introduction
Sjögren’s syndrome (SS) is typically considered a systemic T-cell-mediated autoimmune chronic inflammatory condition. It mainly involves the salivary and lacrimal glands more than other exocrine glands. Though the affected salivary glands show a characteristic histopathological feature of focal sialadenitis with mononuclear cell infiltrate, accumulating around ducts and even extending to replace the glandular secretory functional units, the exact etiology and detailed pathogenesis of such autoimmune exocrinopathy is still not fully understood.1 Yet, some significant mechanisms are proven to be involved in its pathogenesis, such as aberrant apoptosis,2 anti-muscarinic receptors, autoantibodies targeting both lacrimal and salivary glands,3 autoantibodies against some extractable nuclear antigens like the ribonucleoproteins Ro and La (also known as SS‐A and SS‐B, respectively)4 and selective aquaporin-1 downregulation in myoepithelial cells of both salivary and lacrimal glands that results in reduced salivary and tear flow.5 Recent studies also reported that salivary glands of SS patients showed an aberrant distribution of aquaporin-five water channel protein.6 Though many studies support a genetic predisposition from human leukocyte antigen class II marker alleles mainly HLA DR3,7 there is no proven dependence on the HLA haplotype for susceptibility to SS. Surprisingly, several studies reported a stronger correlation between anti-Ro auto-antibodies and HLADR3 (as well as other confirmed non-HLA genetic markers like Km1 allotype) than with the SS disease itself.8 Nevertheless, the association between SS and these genetic markers was proven to be restricted to seropositive SS patients expressing anti-Ro and La auto-antibodies. Thus, such genetic markers are of no use in seronegative SS patients.9
Sjögren’s syndrome may either exist as a single entity or is more commonly associated with other coexisting autoimmune diseases (ADs). Accordingly SS has been traditionally classified as primary SS (p-SS) and secondary SS (s-SS) respectively10 or more recently classified by the American College of Rheumatology as “isolated SS” and “associated SS” respectively.11
As with most other autoimmune diseases, SS occurs predominately in women and, some studies have reported both p-SS and SLE to have the same women to men ratio of 9:1,12 while others even reported much higher ratios of 16–20:1 for SS.13,14 Sjögren’s syndrome has two distanced peaks of appearance, the 1st peak occurs early around the age of 30 in child-bearing years and the 2nd much more frequent peak occurs shortly after the post-menopausal years around the age of 55.13 Pre-2017, adult diagnoses of SS followed the Revised International Classification Criteria of the AEG (American European Group),10 where the diagnosis of SS required the presence of at least four of the following six criteria: 1) oral symptoms; 2) evidence of focal sialadenitis in minor salivary gland biopsy; 3) ocular symptoms; 4) evidence of keratoconjunctivitis sicca; 5) presence of anti-Ro and anti-La auto-antibodies; and 6) instrumental evidence of salivary gland involvement.10 Nowadays, diagnoses of adult SS follows another slightly more sensitive15 classification coined by the American College of Rheumatology and the European League against Rheumatism (ACR/EULAR) (last updated in 2017).11
Primary (isolated) SS has rarely been reported in children, usually diagnosed around the age of 10 years and classified as primary juvenile SS or pediatric primary SS. Such diagnosis is still based on expert opinion and the classifications are based on various criteria for research purposes.16 Primary juvenile SS affects girls much more than boys (77% vs 33% respectively). The pathologic and laboratory findings are similar to those of primary SS among adults, including the characteristic lymphocytic infiltration of exocrine glands, the presence of anti-Ro and anti-La auto-antibodies, antinuclear antibody (ANA), hypergammaglobulinemia, rheumatoid factor (RF) and elevated ESR (erythrocyte sedimentation rate) in most cases.16
We report a case of primary juvenile SS in a seronegative 3-year-old pediatric female patient who visited our immunology clinic back in January 2012. Informed consent was taken from the patient’s parent declaring his approval to publish his daughter’s detailed information (related to disease history and investigational results including photographs and images) in our scientific research under the condition of retaining full privacy of the patient’s identity.
Case Report
A 3-year-old female presented to our immunology clinic in January 2012 with bilateral enlarged parotid glands, badly decayed teeth and painful micturition. Her past medical history revealed that she had frequent doses of antibiotics for recurrent urinary tract infections and recurrent parotitis. Her vaccinations were up to date including mumps, measles and Rubella (MMR) vaccine aged 12 and 18 months. Family history is positive for consanguineous marriages. Her mother gave a disease history of Hashimoto’s thyroiditis with no history of other autoimmune diseases. Careful extraoral examinations revealed dry lips, and intraoral examination revealed multiple dental caries, candida infection on her tongue (Figure 1A and B), difficulty in swallowing and parotid swelling and tenderness. Examination of her vulva area showed redness, irritation and scratch marks.
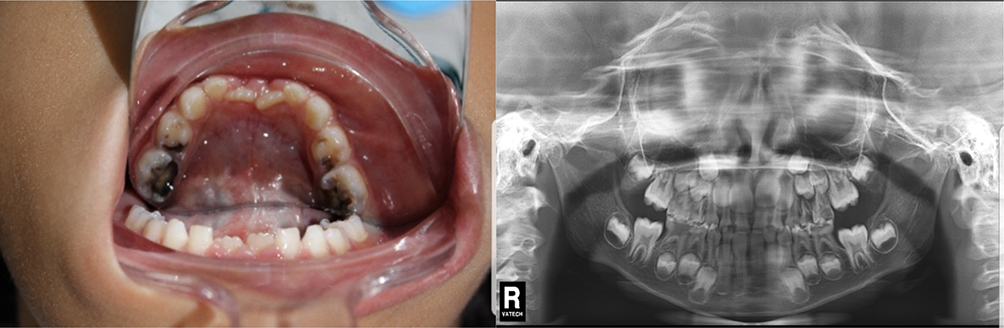 |
Figure 1 Intraoral examination and imaging. (A) (to the left) The patient’s oral cavity revealing multiple dental caries, and candida infection on her tongue. (B) (to the right) Panoramic x-ray image of the patient’s teeth. |
After her hematological, serological and urine examinations were complete it was found that she was anemic, with elevated ESR 45 mm/first hour and weakly positive antinuclear antibodies (indirect immunofluorescence with Hep‐2 cell lines). She had normal urine analysis, and negative results of anti-Ro and anti-La auto-antibodies by enzyme‐linked immunosorbent assay, and rheumatoid factor (RF) by nephelometric assay. Parotid (Figure 2A) and submandibular salivary gland ultrasonography (SGUS) showed enlarged glands with inhomogeneity with many central hypoechoic round foci permeating parenchyma, and narrowing of ducts. The hypoechoic round foci proved to be prominent vessels by the color Doppler ultrasound (Figure 2B). Another follow up SGUS was done after 6 months but showed no significant differences. Renal and pelvic US was also done and reported to be normal and no urinary tract abnormalities were detected. Vaginal swab was done twice, growing normal flora, with negative fungal culture. Ophthalmological examination was insignificant. Histopathology was denied by parents at first and 2 years after first presentation biopsy was compatible with the diagnosis of SS, infiltration of lymphocytes in the periductal field and obliteration of the lumen. Before the biopsy the diagnosis was not confirmed but relied on the clinical picture and salivary gland ultrasonography features, Sjögren was expected and the patient managed accordingly. Her repeated serology at 5 years showed positive results of anti-Ro and anti-La auto-antibodies with the same enzyme‐linked immunosorbent assay used for the first serological testing 2 years before.
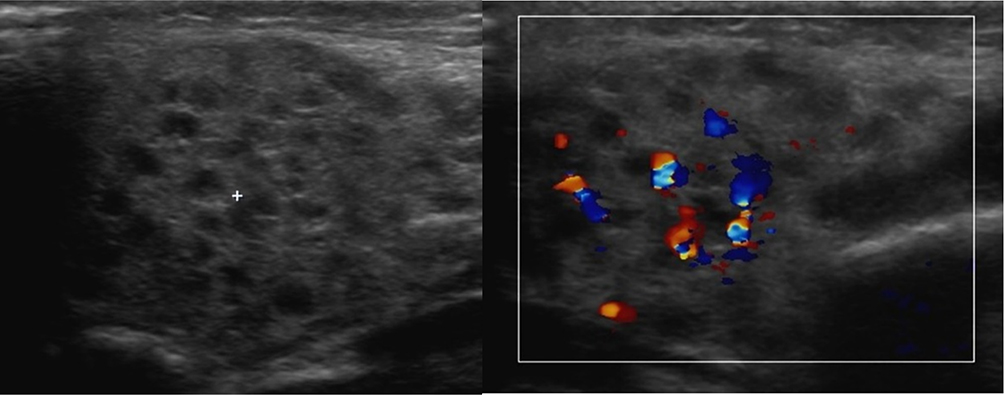 |
Figure 2 US images of the patient’s parotid gland. (A) (to the left) Enlarged, heterogeneous parotid gland, with many central hypoechoic round foci permeating its parenchyma. (B) (to the right) The hypoechoic round foci proved to be prominent vessels by the color Doppler ultrasound. |
The patient was referred to a dentist and an ophthalmologist. Oral hygiene instructions were given to the parents, and vulvar moisturizer cream and 1% hydrocortisone cream given for intermittent use. A short course of oral prednisolone was given once with antibiotics when she presented with parotitis.
Despite regular dental care and oral hygiene, she continues to have new dental caries. Vulvar itchiness and irritation were quite a prominent clinical problem in the last 2 years since presentation.
Discussion
Clinically, Primary juvenile Sjögren’s syndrome is difficult to diagnose during childhood, owing to the difficulty of obtaining reliable history data, the rarity of reported cases with diversity of mostly atypical clinical presentation, and the nonexistence of specific diagnostic criteria for SS in children and thus the use of adult criteria which are frequently not clear in children at disease onset, all of which accounts for a higher frequency of underdiagnosed cases of primary juvenile Sjögren’s syndrome. The clinical feature in this young girl was not obvious in the beginning of her presentation, even before the age of 3 years, and the patient was managed with frequent doses of antibiotics as urinary tract infections and parotid infection before the Sjögren syndrome was suspected. Salivary gland enlargement or recurrent parotitis is the most common clinical presentation of primary juvenile Sjögren’s syndrome while sicca symptoms are rarely observed.17 Urinary tract infection (UTI) is occasionally reported in the literature among adult patients with SS and is mainly attributed to the deficiency of urinary mucosal secretion, vaginal and vulva dryness and impairment in immune functions increasing the risk of recurrent bacterial and fungal vaginal and UTI.18 Both vaginal mycosis and UTI were excluded at time of presentation of our patient by negative cultures. However, the parents did report a history of frequent doses of antibiotic for recurrent previous UTI which we could neither deny nor confirm, the only clearly evident clinical problem was that of recurrent severe vulvovaginitis. Another more common condition called painful bladder syndrome, or interstitial cystitis known to affect adult females with Sjögren’s syndrome and causes signs and symptoms similar to those of a UTI like urinary frequency, urgency and painful micturition without any evidence of infection.18 Unfortunately, at that time we could not perform a cystoscopy to clearly prove or exclude such a condition existed, and the very young patient could not of course give a detailed history that clearly differentiated between symptoms of painful micturition versus valvular or vaginal dryness and irritation alone.
At presentation, this young girl's serological test results were weakly positive for antinuclear antibodies (ANA), and seronegative for anti-Ro and anti-La auto-antibodies and rheumatoid factor (RF). The literature review shows that 29% of patients with primary SS can present seronegative for anti-Ro antibodies and about 33% can present seronegative for anti-La auto-antibodies.19 Two years later her repeated serology showed positive seroconversion for both anti-Ro and anti-La auto-antibodies. Such a finding advocates that periodic reappraisal of these auto-antibodies may be recommended among seronegative patients with a suspected diagnosis of primary juvenile SS. In fact, longitudinal fluctuation of auto-antibodies directed against extractable nuclear antigens (ENA, Sm, U1-RNP, Ro and La) are reported in diseases like systemic lupus erythematosus (SLE), with time after diagnosis ranging from 1 to 8 years to positive seroconversion.20
The confirmed diagnosis of primary juvenile Sjögren’s syndrome for this young girl was delayed for 2 years until a positive biopsy showed typical histopathological findings of SS. Such a delay should not only be blamed on the two-year denial of the parents to allow such a conclusive but rather invasive and risky procedure in such a young girl, but also should be blamed on the current international classification criteria of SS not including major salivary glands ultrasonography in the diagnostic algorithm for primary SS. This young girl's parotid and submandibular salivary gland ultrasonography showed enlarged glands with inhomogeneity and narrowing of ducts at the time of presentation. Such parenchymal inhomogeneity is reported by many authors as the most important sonographic feature of salivary gland involvement in primary SS and the most reliable feature to distinguish SS from other pathological mimicker conditions.21–23 With the international classification criteria of SS as their gold standard, recent meta-analysis studies traced the diagnostic performance of major salivary glands' US in diagnosing SS. Delli et al24 revealed a pooled sensitivity of 69% and specificity of 92%. Similarly, Song et al25 reported a pooled sensitivity of 77.4% (73.7–80.9) and specificity of 81.5% (77.6–85.0).
Owing to the gradual damage of glands along the insidious course of SS, sicca symptoms as well as the objective signs of salivary and lacrimal gland involvement would eventually become more evident over time. Due to the rather short duration of disease and thus the infrequent sicca symptoms at presentation and the tendency to avoid invasive salivary gland biopsy even in cases where the diagnosis is highly probable, many pediatric patients with Primary juvenile SS would end up not fulfilling the adult criteria.26 Until the present day, pediatric criteria have not been standardized. In 1999, Bartunkova et al26 suggested a preliminary pediatric diagnostic criteria for primary juvenile SS. These criteria took into account the infrequent presence of sicca signs and symptoms among children and thus proposed some important modifications to the adult criteria, like the addition of the presence of recurrent parotitis, conjunctivitis, vaginitis, some systemic symptoms (like fever, abdominal pain, arthralgias and hypokalemic paralysis) and some laboratory features (leukopenia, polyclonal hypergammaglobulinemia, raised ESR and serum amylases and RTA (renal tubular acidosis)).26 Though, the inclusion of recurrent parotitis actually increased the sensitivity of the pediatric over the adult criteria.27 These preliminary proposed pediatric criteria have not been adopted nor validated in later studies. In our case, both recurrent parotitis and recurrent vaginitis were the most prominent presenting features of the syndrome, in fact the vulvovaginitis was even persistent after diagnosis and despite topical steroids treatment.
Regarding the treatment of our case, unfortunately so far there is no cure for SS, but treatments can be used to relieve symptoms. Changes in both the salivary flow and composition prompt opportunistic infections and dental caries. Dental treatment is mainly supportive and symptomatic, including salivary substitutes, moisturizing mouthwashes, local cholinergic stimulators, topical fluoride application, optimal oral hygiene, diet control and good hydration.16 Besides dental and eye palliative topical care, the treatment regimen of our case may also require the use of systemic anti‐inflammatory and immunosuppressive drugs, such as oral steroids and methotrexate, to reduce the over activity of the immune system. Hydroxychloroquine, a drug primarily used to treat malaria, may also be used as an immunomodulatory drug that is proved to be helpful in controlling the symptoms of SS.28
B-cell non-Hodgkin lymphoma (NHL) development represents a severe complication, afflicting approximately 5% of SS patients.29 The risk of NHL occurrence in the setting of SS, the highest among systemic autoimmune diseases, has been previously estimated to be 7- to 19-fold higher compared to the general population.30 So periodic salivary gland ultrasonography was recommended to provide a complementary view of the status of the glandular parenchyma and to monitor lymphoma development.
Recommendations
- The findings of this case highlighted the great diagnostic potential of salivary gland ultrasonography especially in young seronegative cases. Though not included in the most recent classification criteria for primary SS by ACR/EULAR11 we recommend the prompt inclusion of this accessible, accurate, non-invasive, easily performed and feasible tool, in the diagnostic algorithm for primary SS patients. We support all scientific effort in this direction like the “UTOPIA PROJECT: Integration of Salivary-Gland Ultrasonography in Classification Criteria for Primary Sjögren’s Syndrome: an International Vignette-Based Study” by Devauchelle et al which we believe will make it possible to include this promising tool in the diagnostic algorithm for primary SS patients in the near future.31,32
- The serological findings also point out the importance of periodic serological reappraisal of SS‐A (anti‐Ro) seronegative patients with a suspect diagnosis of Primary juvenile Sjögren’s syndrome.
- Though recurrent parotitis is still the most common presentation of primary juvenile SS in children, the initial presentation of this case also highlighted the importance of other extra-salivary manifestations like recurrent vulvovaginitis, and the physician must maintain a high index of suspicion for underlying SS.
- Our findings call for the need to develop specific diagnostic criteria for primary juvenile SS in children rather than the current practice of applying adult criteria which are frequently not clear in children at disease onset, resulting in a higher frequency of underdiagnosed cases.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Voulgarelis M, Tzioufas AG. Current aspects of pathogenesis in Sjögren’s syndrome. Ther Adv Musculoskelet Dis. 2010;2(6):325–334. doi:10.1177/1759720X10381431
2. Bolstad AI, Jonsson R. The role of apoptosis in Sjogren’s syndrome. Ann Med Interne. 1998;149(1):25–29.
3. Beroukas D, Goodfellow R, Hiscock J, Jonsson R, Gordon TP, Waterman SA. Up-regulation of M3-muscarinic receptors in labial salivary gland acini in primary Sjogren’s syndrome. Lab Invest. 2002;82(2):203–210. doi:10.1038/labinvest.3780412
4. Gordon TP, Bolstad AI, Rischmueller M, Jonsson R, Waterman SA. Autoantibodies in primary Sjogren’s syndrome: new insights into mechanisms of autoantibody diversification and disease pathogenesis. Autoimmunity. 2001;34(2):123–132. doi:10.3109/08916930109001960
5. Beroukas D, Hiscock J, Gannon BJ, Jonsson R, Gordon TP, Waterman SA. Selective down-regulation of aquaporin-1 in salivary glands in primary Sjogren’s syndrome. Lab Invest. 2002;82(11):1547–1552.
6. Steinfeld S, Cogan E, King LS, Agre P, Kiss R, Delporte C. Abnormal distribution of aquaporin-5 water channel protein in salivary glands from Sjögren’s syndrome patients. Lab Invest. 2001;81(2):143–148. doi:10.1038/labinvest.3780221
7. Criswell LA, Pfeiffer KA, Lum RF, et al. Analysis of families in the multiple autoimmune disease genetics consortium (MADGC) collection: the PTPN22 620W allele associates with multiple autoimmune phenotypes. Am J Hum Genet. 2005;76(4):561–571. doi:10.1086/429096
8. Arnett FC, Hamilton RG, Reveille JD, Bias WB, Harley JB, Reichlin M. Genetic studies of Ro (SS-A) and La (SS-B) autoantibodies in families with systemic lupus erythematosus and primary Sjogren’s syndrome. Arthritis Rheum. 1989;32(4):413–419. doi:10.1002/anr.1780320410
9. Gottenberg JE, Busson M, Loiseau P, et al. In primary Sjogren’s syndrome, HLA class II is associated exclusively with autoantibody production and spreading of the autoimmune response. Arthritis Rheum. 2003;48(8):2240–2245. doi:10.1002/art.11103
10. Vitali C, Bombardieri S, Jonsson R, et al. Classification criteria for Sjogren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis. 2002;61(6):554–558. doi:10.1136/ard.61.6.554
11. Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League against Rheumatism classification criteria for primary Sjogren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheum. 2017;69(1):35–45. doi:10.1002/art.39859
12. Fairweather D, Petri MA, Coronado MJ, Cooper LT. Autoimmune heart disease: role of sex hormones and autoantibodies in disease pathogenesis. Expert Rev Clin Immunol. 2012;8(3):269–284. doi:10.1586/eci.12.10
13. Brandt JE, Priori R, Valesini G, Fairweather D. Sex differences in Sjögren’s syndrome: a comprehensive review of immune mechanisms. Biol Sex Differ. 2015;6:19. doi:10.1186/s13293-015-0037-7
14. Patel R, Shahane A. The epidemiology of Sjögren’s syndrome. Clin Epidemiol. 2014;6:247–255. doi:10.2147/CLEP.S47399
15. Le Goff M, Cornec D, Jousse-Joulin S, et al. Comparison of 2002 AECG and 2016 ACR/EULAR classification criteria and added value of salivary gland ultrasonography in a patient cohort with suspected primary Sjögren’s syndrome. Arthritis Res Ther. 2017;19(1):269. doi:10.1186/s13075-017-1475-x
16. Civilibal M, Canpolat N, Yurt A, et al. A child with primary Sjogren syndrome and a review of the literature. Clin Pediatr. 2007;46(8):738–742. doi:10.1177/0009922807301945
17. Fox RI. Sjogren’s syndrome. Lancet. 2005;366(9482):321–331. doi:10.1016/S0140-6736(05)66990-5
18. Emmungil H, Kalfa M, Zihni FY, et al. Interstitial cystitis: a rare manifestation of primary Sjögren’s syndrome, successfully treated with low dose cyclosporine. Rheumatol Int. 2012;32(5):1215–1218. doi:10.1007/s00296-010-1782-x
19. Hammi AR, Al-Hashimi IH, Nunn ME, Zipp M. Assessment of SS-A and SS-B in parotid saliva of patients with Sjogren’s syndrome. J Oral Pathol Med. 2005;34(4):198–203. doi:10.1111/j.1600-0714.2004.00301.x
20. Faria AC, Barcellos KS, Andrade LE. Longitudinal fluctuation of antibodies to extractable nuclear antigens in systemic lupus erythematosus. J Rheumatol. 2005;32(7):1267–1272.
21. Hocevar A, Ambrozic A, Rozman B, Kveder T, Tomsic M. Ultrasonographic changes of major salivary glands in primary Sjogren’s syndrome. Diagnostic value of a novel scoring system. Rheumatology. 2005;44(6):768–772. doi:10.1093/rheumatology/keh588
22. Luciano N, Baldini C, Tarantini G, et al. Ultrasonography of major salivary glands: a highly specific tool for distinguishing primary Sjogren’s syndrome from undifferentiated connective tissue diseases. Rheumatology. 2015;54(12):2198–2204. doi:10.1093/rheumatology/kev253
23. Jousse-Joulin S, Nowak E, Cornec D, et al. Salivary gland ultrasound abnormalities in primary Sjogren’s syndrome: consensual US-SG core items definition and reliability. RMD Open. 2017;3(1):e000364. doi:10.1136/rmdopen-2016-000364
24. Delli K, Dijkstra PU, Stel AJ, Bootsma H, Vissink A, Spijkervet FK. Diagnostic properties of ultrasound of major salivary glands in Sjogren’s syndrome: a meta-analysis. Oral Dis. 2015;21(6):792–800. doi:10.1111/odi.12349
25. Song GG, Lee YH. Diagnostic accuracies of sialography and salivary ultrasonography in Sjogren’s syndrome patients: a meta-analysis. Clin Exp Rheumatol. 2014;32(4):516–522.
26. Bartunkova J, Sediva A, Vencovsky J, Tesar V. Primary Sjogren’s syndrome in children and adolescents: proposal for diagnostic criteria. Clin Exp Rheumatol. 1999;17(3):381–386.
27. Houghton K, Malleson P, Cabral D, Petty R, Tucker L. Primary Sjogren’s syndrome in children and adolescents: are proposed diagnostic criteria applicable? J Rheumatol. 2005;32(11):2225–2232.
28. Gottenberg JE, Ravaud P, Puechal X, et al. Effects of hydroxychloroquine on symptomatic improvement in primary Sjogren syndrome: the JOQUER randomized clinical trial. JAMA. 2014;312(3):249–258. doi:10.1001/jama.2014.7682
29. Voulgarelis M, Dafni UG, Isenberg DA, Moutsopoulos HM. Malignant lymphoma in primary Sjogren’s syndrome: a multicenter, retrospective, clinical study by the European Concerted Action on Sjogren’s Syndrome. Arthritis Rheum. 1999;42(8):1765–1772. doi:10.1002/1529-0131(199908)42:8<1765::AID-ANR28>3.0.CO;2-V
30. Liang Y, Yang Z, Qin B, Zhong R. Primary Sjogren’s syndrome and malignancy risk: a systematic review and meta-analysis. Ann Rheum Dis. 2014;73(6):1151–1156. doi:10.1136/annrheumdis-2013-203305
31. Jousse-Joulin S, Milic V, Jonsson MV, et al. Is salivary gland ultrasonography a useful tool in Sjogren’s syndrome? A systematic review. Rheumatology. 2016;55(5):789–800. doi:10.1093/rheumatology/kev385
32. Cornec D, Jousse-Joulin S, Marhadour T, et al. Salivary gland ultrasonography improves the diagnostic performance of the 2012 American College of Rheumatology classification criteria for Sjogren’s syndrome. Rheumatology. 2014;53(9):1604–1607. doi:10.1093/rheumatology/keu037
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.