")
Back to Journals » OncoTargets and Therapy » Volume 9
Pri-let-7a-1 rs10739971 polymorphism is associated with gastric cancer prognosis and might affect mature let-7a expression
Authors Li Y, Xu Q, Liu J, He C, Yuan Q, Xing C, Yuan Y
Received 13 November 2015
Accepted for publication 16 April 2016
Published 4 July 2016 Volume 2016:9 Pages 3951—3962
DOI https://doi.org/10.2147/OTT.S100481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianmin Xu
Ying Li, Qian Xu, Jingwei Liu, Caiyun He, Quan Yuan, Chengzhong Xing, Yuan Yuan
Tumor Etiology and Screening Department of Cancer Institute and General Surgery, the First Affiliated Hospital of China Medical University, and Key Laboratory of Cancer Etiology and Prevention (China Medical University), Liaoning Provincial Education Department, Shenyang, People’s Republic of China
Abstract: The relationship between the pri-let-7a-1 rs10739971 polymorphism and gastric cancer (GC) risk has been reported. However, the role of this polymorphism in the prognosis of GC remains largely elusive. Sequenom MassARRAY platform method and the polymerase chain reaction (PCR)-restriction fragment length polymorphism were used to investigate pri-let-7a-1 rs10739971 G→A in 334 GC patients. Real-time PCR detected expression of mature let-7a in serum and tissue. Patients with AA or GA+AA genotypes of the pri-let-7a-1 rs10739971 polymorphism demonstrated significantly longer survival time than those with the wild GG genotype. Stratified analysis indicated that survival time was significantly longer in women with AA or GA+AA genotypes and in Borrmann type I/II patients with GA heterozygote or GA+AA genotypes. AA genotype was more frequent in the lymphatic-metastasis-negative subgroup. Serum mature let-7a expression in healthy people with the GA heterozygote and the GA+AA genotype was higher than in those with the GG genotype, and the difference remained significant in the female healthy subgroup. Pri-let-7a-1 rs10739971 polymorphism might be a biomarker for GC prognosis, especially for female and Borrmann type I/II patients. The pri-let-7a-1 rs10739971 polymorphism might affect serum mature let-7a expression, and partly explain the mechanism of the relationship between the pri-let-7a-1 rs10739971 polymorphism and GC survival.
Keywords: miRNA, let-7a, polymorphism, gastric cancer, prognosis, expression
Introduction
microRNAs (miRNAs) are involved in a variety of important biological behaviors including tumorigenesis, differentiation, apoptosis, and proliferation.1,2 It is widely accepted that miRNA polymorphisms can be used as biomarkers of tumor prognosis. For example, the miR-196a-2 rs11614913 polymorphism can predict the survival of several tumors, including gastric cancer (GC),3,4 non-small-cell lung cancer,5,6 esophageal squamous cell carcinoma,7 oral squamous cell carcinoma,8–10 kidney cancer,11 and breast cancer.12 The miR-27a rs895819 polymorphism can be used as a prognostic factor for advanced GC4 and non-small-cell lung cancer.13
The let-7 plays a critical role in cell proliferation and differentiation; it is the earliest discovered miRNA and has continued to gain recognition in recent years. Several studies have proved that let-7 miRNA participates in the tumorigenesis and metastasis of different types of cancer, such as breast and lung cancers.14–16 The let-7 family has ten members: let-7a, let-7b, let-7c, let-7d, let-7e, let-7f, let-7g, let7i, miR-98, and miR-202. Recent research has linked polymorphisms of some let-7 family members to cancer, for example, the interaction of the pri-let-7a-1 rs10739971 polymorphism and the ERCC6 rs1917799 polymorphism is significantly correlated with the risk of GC.17 The rs10877887 polymorphism in the promoter region of let-7 is significantly associated with prognosis of hepatocellular carcinoma18 and the pri-let-7a-2 rs629367 polymorphism is significantly related to poor survival of GC.19 The relationship between the pri-let-7a-1 rs10739971 polymorphism and GC risk has been reported; however, few studies have investigated the association of the pri-let-7a-1 polymorphism and cancer prognosis. The relationship between the pri-let-7a-1 rs10739971 polymorphism and GC prognosis has not been reported.
In this study, systematic clinical data were collected for 334 cases of GC and the relationship between the pri-let-7a-1 rs10739971 polymorphism and cancer prognosis was investigated. We analyzed the effect of this polymorphism on mature let-7a expression both in serum and tissue. The aim of this study was to establish the relationship between this polymorphism and GC prognosis, and its possible mechanism.
Materials and methods
Patients and clinicopathological data
This study was approved by the Human Ethics Committee of the First Affiliated Hospital of China Medical University, and conformed to Chinese laws and the Helsinki Declaration. Written informed consent was obtained from the patients, and baseline characteristics (including age, sex, smoking, alcohol drinking, and family history) were obtained by questionnaire and the records above were computerized. Subjects were recruited who underwent gastric surgery in the First Affiliated Hospital of China Medical University, Liaoning Province, People’s Republic of China between 2010 and 2013. Fasting venous blood was collected. Serum and blood coagulation were separated and stored at −20°C. All GC patients were diagnosed based on the histopathological confirmation according to Borrmann’s as well as Lauren’s classification, and the tumors were staged according to the 7th edition of the tumor node metastasis (TNM) staging system of the International Union Against Cancer/American Joint Committee on Cancer (2010), based on postoperative pathological examination. Exclusion criteria were 1) patients with distant metastasis found preoperatively; 2) patients who underwent preoperative radiotherapy or chemotherapy; or 3) patients with incomplete pathological data. Follow-up was completed by August 2013. The basic features of 334 GC patients enrolled in survival analysis are shown in Table S1.
To assess the effect of polymorphism on mature miRNA expression at the tissue level, 131 GC specimens from patients who underwent subtotal gastrectomy in the First Affiliated Hospital of China Medical University between 2010 and 2013 were included. At the serum level, we matched 99 GC patients with 99 healthy individuals. Patients who were endoscopically and histologically diagnosed with normal mucosa or only mild gastritis without other systemic diseases or other gastropathy served as controls. The basic information of all subjects is summarized in Table S2.
Single nucleotide polymorphism genotyping
The genomic DNA was extracted using the method stated previously with proteinase K digestion and phenol/chloroform extraction.20 Sequenom MassARRAY platform method (Sequenom, San Diego, CA, USA) and polymerase chain reaction (PCR) restriction-fragment length polymorphism were used to detect the polymorphism of pri-let-7a-1 rs10739971 G→A. To assess the quality of the genotyping, 5% samples of all were genotyped repeatedly and the results were 100% consistent.
RNA extraction and real-time quantitative PCR reaction for miRNA expression in vivo
miRNAs were extracted from the serum and tissues as described previously,21 with some modifications. One Step Prime Script miRNA cDNA (Perfect Real Time) Kit (TaKaRa Biotechnology, Dalian, People’s Republic of China) was used in the reverse transcription reaction and miRcute miRNA qPCR detection kit SuperReal PreMix Plus (SYBR) (Tiangen Biotech, Beijing, People’s Republic of China) was used for real-time quantitative PCR. Details of the materials are shown in the Supplementary materials.
Statistical analysis
All the statistical analyses were carried out using SPSS Version 16.0 software (SPSS Inc., Chicago, IL, USA). Correlation between the pri-let-7a-1 rs10739971 polymorphism and clinicopathological parameters of GC was estimated by χ2 test. Survival curves were estimated by the Kaplan–Meier method, and the association between the single nucleotide polymorphism (SNP) and different survival times was assessed by the log-rank test. The median survival time was calculated; the hazard ratios (HRs) and their 95% confidence intervals (CIs) were estimated by univariate and multivariate Cox proportional hazards regression models. The log value of copies of miRNA were used to reach a normal distribution, and the effect of miRNA polymorphisms on the expression level was tested by the independent-samples t-test, with the mean and standard deviation calculated.
Results
Characteristics and clinical features of the study subjects
The demographic and clinical features of the 334 patients enrolled in this study are shown in Table S1, including age, sex, tumor size, Borrmann type, Lauren classification, TNM stage, growth pattern, lymphatic metastasis, smoking, alcohol consumption, and family history. Tumor size, Lauren grade, TNM stage, growth pattern, and lymphatic metastasis significantly affected survival time (P<0.05). Therefore, we used these as adjustment factors for a multivariate Cox proportional hazards regression model.
Correlation between the pri-let-7a-1 rs10739971 polymorphism and clinicopathological parameters of GC
The correlation between the pri-let-7a-1 rs10739971 polymorphism and clinicopathological parameters of GC was analyzed, including age, sex, tumor size, Borrmann type, Lauren classification, TNM stage, growth pattern, lymphatic metastasis, smoking, alcohol consumption, and family history. AA genotype was more frequent in the lymphatic-metastasis-negative subgroup than in the subgroup with lymphatic metastasis (52.5% vs 31.6%, P=0.009; 25.2% vs 14.6%, P=0.015). There was no significant correlation between the pri-let-7a-1 rs10739971 polymorphism and other clinicopathological parameters of GC (Table 1).
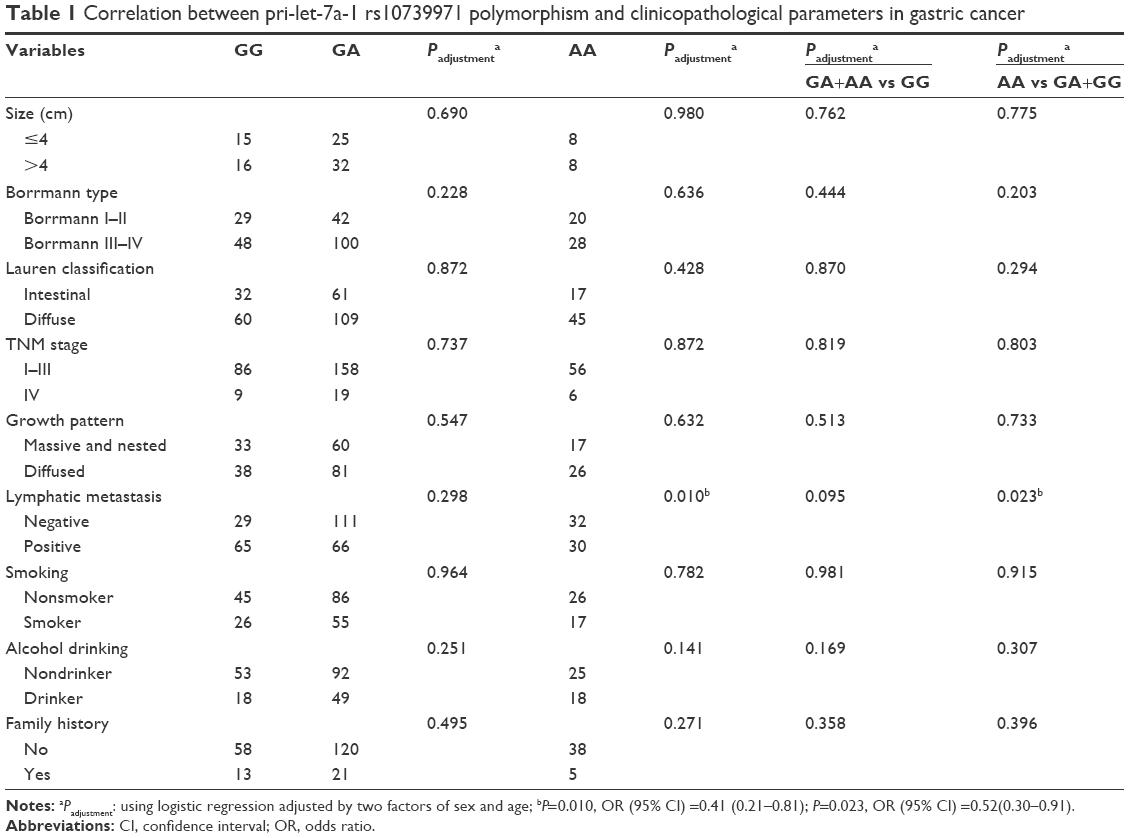 | Table 1 Correlation between pri-let-7a-1 rs10739971 polymorphism and clinicopathological parameters in gastric cancer |
Association of the pri-let-7a-1 rs10739971 polymorphism with survival time of GC patients
We analyzed the association of the pri-let-7a-1 rs10739971 polymorphism with prognosis of GC using a univariate Cox proportional hazards regression model. The log-rank test showed that survival time in patients with the AA or GA+AA genotype was significantly longer than in those with GG genotype (P=0.099, P=0.092, respectively; Table 2). Multivariate Cox proportional hazards regression model analysis showed that survival time was longer in patients with the variant AA genotype polymorphism (HR =0.75, P=0.762; Table 2), with adjustment for potential confounding factors, such as tumor size, Lauren classification, TNM stage, growth pattern, and lymphatic metastasis.
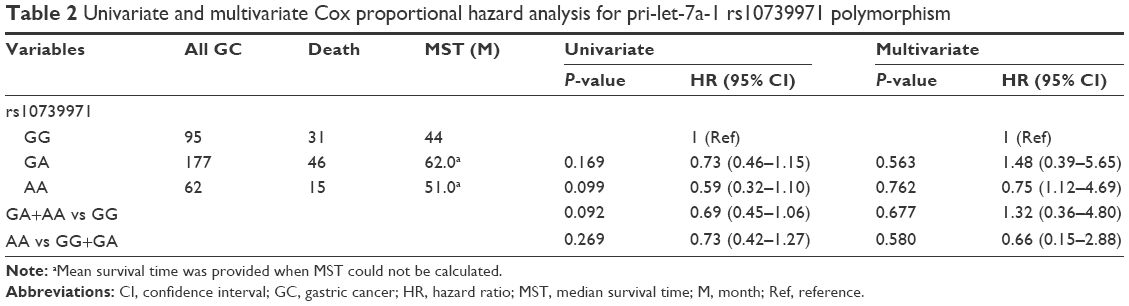 | Table 2 Univariate and multivariate Cox proportional hazard analysis for pri-let-7a-1 rs10739971 polymorphism |
Stratified analysis of the effect of the pri-let-7a-1 rs10739971 polymorphism on survival time of GC patients
To evaluate the influence of different factors on the relationship between the pri-let-7a-1 rs10739971 polymorphism and GC patients’ survival, we performed stratification analysis. This polymorphism was significantly associated with prognosis of GC in certain subgroups: survival time of subjects with AA or GA+AA genotype was significantly longer compared with those with wild-type GG genotype, especially in female patients (HR =0.24, 95% CI =0.07–0.86; HR =0.40, 95% CI =0.19–0.83; Table 3, Figure 1A–D) and Borrmann type I/II patients (HR =0.44, 95% CI =0.20–0.94; HR =0.42, 95% CI =0.21–0.84; Table 3, Figure 1E–H).
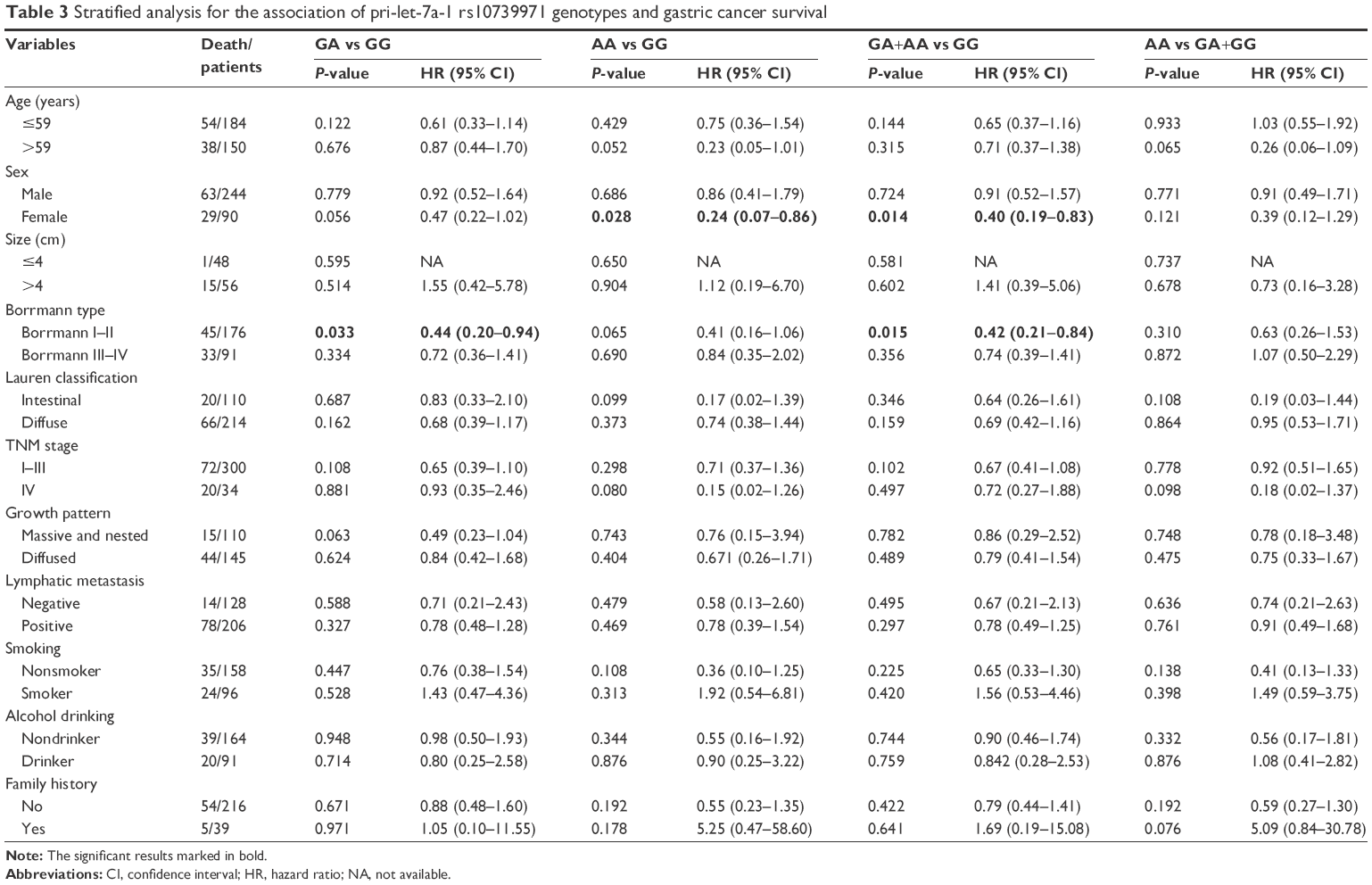 | Table 3 Stratified analysis for the association of pri-let-7a-1 rs10739971 genotypes and gastric cancer survival |
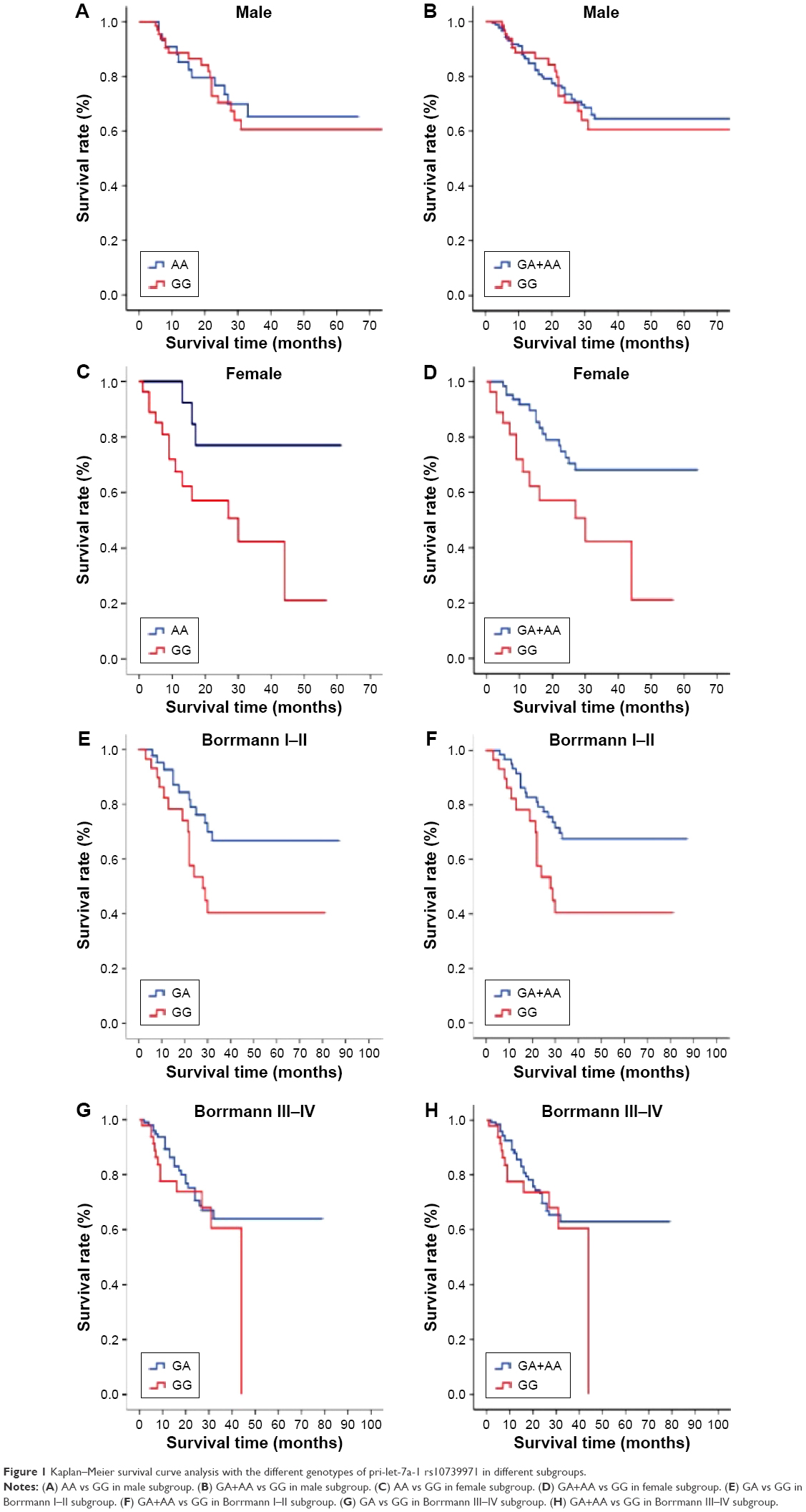 | Figure 1 Kaplan–Meier survival curve analysis with the different genotypes of pri-let-7a-1 rs10739971 in different subgroups. |
Effect of the pri-let-7a-1 rs10739971 polymorphism on mature let-7a expression
To study the possible mechanism of pri-let-7a-1 rs10739971 polymorphism in the survival time of GC patients, we further analyzed the effect of this polymorphism on its mature miRNA expression in serum and tissue. There was no significant difference for age and sex in all subjects (including GC patients and healthy controls, Tables S2 and S3). In serum, mature let-7a expression of this polymorphism in healthy controls with the GA heterozygote and GA+AA genotype showed a significant increase compared with healthy people with the wild-type GG genotype (GA vs GG, P=0.028; GA+AA vs GG, P=0.018; Table 4 and Figure 2A). Mature let-7a expression in healthy women with this polymorphism (GA+AA) was significantly higher than those with GG genotype (GA+AA vs GG, P=0.043; Table 4 and Figure 2B). In GC patients, however, this polymorphism had no significant effect on its mature miRNA expression in serum or tissue (Tables 4 and 5).
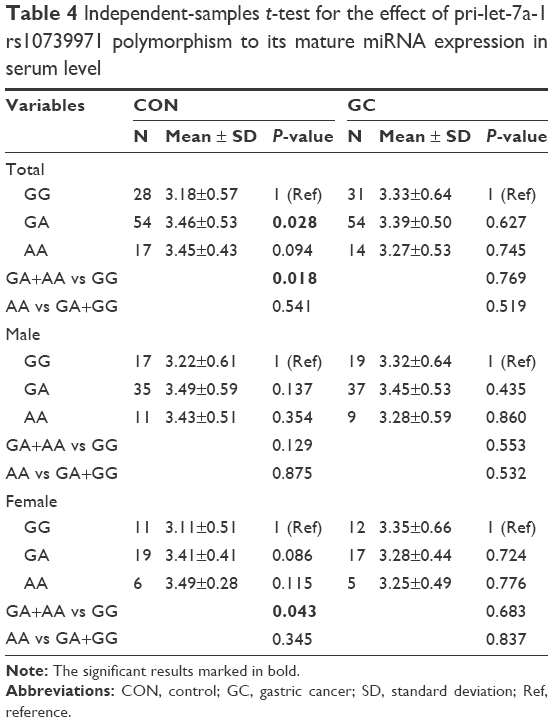 | Table 4 Independent-samples t-test for the effect of pri-let-7a-1 rs10739971 polymorphism to its mature miRNA expression in serum level |
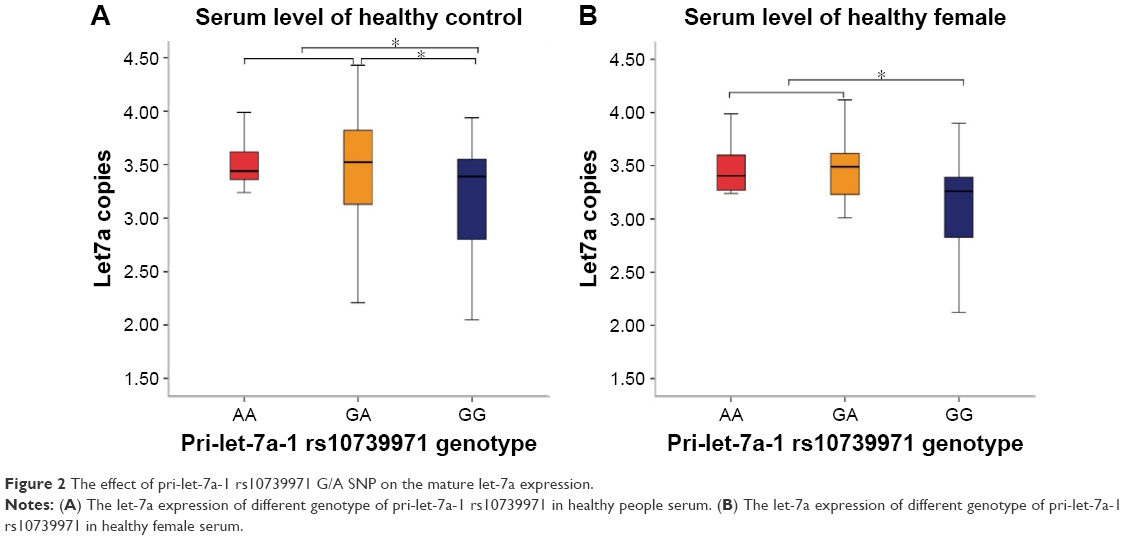 | Figure 2 The effect of pri-let-7a-1 rs10739971 G/A SNP on the mature let-7a expression. |
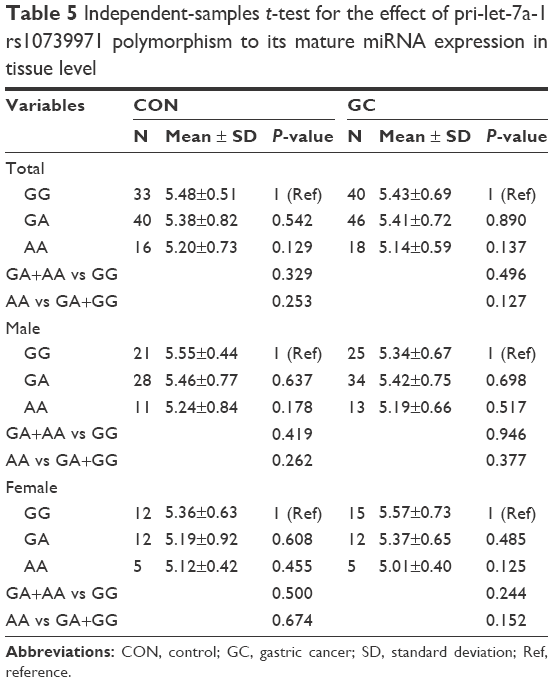 | Table 5 Independent-samples t-test for the effect of pri-let-7a-1 rs10739971 polymorphism to its mature miRNA expression in tissue level |
Discussion
We reported the relationship of the pri-let-7a-1 rs10739971 polymorphism with the prognosis of GC patients in Northern China. Cox proportional hazards regression model analysis showed that AA mutation genotype and GA+AA genotype correlated with GC prognosis (P<0.10), especially in female patients or Borrmann type I/II patients. Further analysis found that AA mutation genotype was significantly correlated with lymphatic metastasis. After analyzing the effect of this polymorphism on its mature miRNA expression in serum and tissue, we found that mature miRNA expression of GA and GA+AA genotype was significantly higher than wild-type GG miRNA expression in the serum of all healthy people and the female healthy controls.
The miRNA polymorphism can act directly (including primary, secondary precursor, and mature polymorphism, which can affect maturation or function of miRNA) or indirectly (promoter region polymorphism affects the transcription and polymorphism-binding sites of the target gene). The pri-let-7a-1 rs10739971 polymorphism is located in −599 bp of mature let-7a-1, which is the primary precursor area of let-7a-1 and may also be the promoter region. We found that carriers of the variant genotype of this polymorphism demonstrated favorable prognosis compared with those with the wild genotype. The relationship between pri-let-7a-1 rs10739971 polymorphism and GC prognosis might arise from that this polymorphism is located at the promoter region. We adopted RNAfold software to predict secondary structure of the let-7a-1 gene near ±600 bp. The minimum free energy of those who carry the rs10739971 variant A allele was lower than that of those who carry the rs10739971 wild G allele. Furthermore, the secondary structure of miRNA with rs10739971 variant A allele tended to be more stable. Therefore, we speculated that the different structure of the rs10739971 G/A polymorphism may lead to a difference in function, because the variant A allele had a more stable secondary structure, which may be more conducive to the maturation process of miRNA. In addition, let-7a is recognized as a tumor suppressor, which might have a positive effect on tumor prognosis. GC patients who carry the variant A allele demonstrated longer survival. The wild-type G allele has a loose secondary structure, which may not be conductive to miRNA maturation, leading to a shorter survival time of GC patients who carry the wild-type G allele. We also found that the rate of lymphatic metastasis in GC patients with the AA mutation genotype was significantly lower than in those with wild GG genotype. This was consistent with our finding that patients with the AA mutation genotype exhibited significantly longer survival time than those with the wild GG genotype. Lymphatic metastasis is a risk factor for GC; thus, we consider that the significantly longer survival time observed for carriers of the AA mutation genotype may be related to the absence of lymphatic metastasis.
Stratified analysis suggested that female patients who carry this polymorphism AA or GA+AA genotype had significantly longer survival. The let-7 is a direct estrogen receptor (ER)-α target gene, and its expression correlates with ER-α in breast, ovarian, and gastric cancer, and it inhibits cancer cell proliferation and promotes cancer cell apoptosis.15,22,23 Previous studies showed that let-7 is an important regulator of ER-α target genes and it shares many binding sites with ER-α. Notably, at shared sites, let-7 inhibits the ER-α signaling pathway, which decreases the survival of cancer cells and increases their rate of apoptosis.14,15 As a result, in female patients with more ER-α, more let-7 polymorphisms, which act as a protective factor, contribute to better prognosis. We speculated that female GC patients who carried variant A allele had increased expression of mature let-7a compared with G allele carriers, which could more efficiently inhibit tumor cell proliferation and induce tumor cell apoptosis, thereby leading to longer survival time. However, the result was not what we expected: expression of mature let-7a was not increased significantly in GC patients with the variant A allele. The binding of mature let-7a and ER-α is due to the variant A allele, which may lead to the result above. In stratified analysis, we also found that Borrmann type I/II patients who carry this polymorphism of GA heterozygous or (GA+AA) genotype demonstrated more favorable prognosis than GG genotype subjects. Yang found that the Borrmann type is an independent prognostic factor only in stage IV GC,24 which showed that it has an important role in GC prognosis. rs10739971 is located in the promoter region of let-7a miRNA, which might affect the post-transcriptional regulation of let-7a miRNA, through the binding of different transcription factors. We conjectured that rs10739971 could affect the Borrmann type through its effect on the expression of mature let-7a. Moreover, the phenomenon that the A allele of this polymorphism was related to favorable prognosis may be because the effect of the variant A allele is great in the case of healthy individuals and patients with primary stage GC. Besides, we found that survival time was not significantly longer in men with AA or GA+AA genotypes and in Borrmann type III/IV patients with GA heterozygote of GA+AA genotypes, which suggest that sex and Borrmann classification might influence the effect of SNP on GC survival.
Mature miRNA is part of the regulatory mechanisms controlling gene expression at both transcriptional and post-transcriptional levels. According to recent research,25 one miRNA can regulate the expression of multiple genes, while a single gene is regulated by a series of different miRNAs, and ~60% of protein-coding genes are regulated by miRNAs. At present, research about the pathogenic mechanism of the miRNA promoter region polymorphism has mainly focused on the functional miR-34b/c rs4938723 polymorphism. This polymorphism might affect the binding ability of transcription factor GATA and further influence mature pri-miR-34b/c expression.26 Xu et al thought it may serve as biomarker of liver cancer prognosis. We speculated that the significant association of the pri-let-7a-1 rs10739971 polymorphism with the prognosis of GC may arise from the influence of mature let-7a expression, like the miR-34b/c rs4938723 polymorphism. Therefore, we explored further the effect of this polymorphism on its mature miRNA expression level. In serum, we found that mature let-7a expression in healthy individuals with the GA heterozygote and GA+AA genotype showed a significant increase, and mature let-7a expression in healthy women with the GA+AA genotype was significantly higher. This indicated that the variant A allele was beneficial to let-7a miRNA maturation, illustrating that the miRNA polymorphism acts as a tumor suppressor by increasing the expression of mature miRNA, which is consistent with the effect of the miR-34b/c rs4938723 polymorphism on the expression of its maturity.26 In tissue, we found that mature let-7a expression in individuals with different genotypes showed no significant difference between the GC and healthy groups, which may be because the tissue of the healthy group was taken from distal GC patients instead of really healthy people. In GC patients, no significant effect of this polymorphism on its mature miRNA expression, either in serum or tissue, was observed. The following reasons may explain the results. First, the state of disease (cancerous) disturbs multiple cellular functions and regulations, which probably weaken the effect of the miRNA SNP on mature miRNA expression. Second, the sample size of expression study was relatively small, which might restrict the results and should be confirmed in a larger sample of future investigation. In addition, it should be further researched that whether other cofactors also affect let-7a expression together with SNP.
In summary, this study analyzed the association of the pri-let-7a-1 rs10739971 polymorphism and GC prognosis stratified by clinicopathological parameters on the basis of overall analysis. We preliminarily studied the effect of the pri-let-7a-1 rs10739971 polymorphism on the expression level of miRNA to explore the possible mechanism of the effect of miRNA polymorphism on GC prognosis. This is believed to be the first study exploring the relationship between the pri-let-7a-1 rs10739971 G/A polymorphism and GC prognosis in Northern China. There were some limitations to our study. First, the sample size was insufficient, and our results need validation with a larger sample of different ethnicities. Second, our study only investigated overall survival time, and other relevant indicators of prognosis research need to be explored, such as disease-free survival time. Third, subsequent experiments concerning function of miRNA are still needed.
Conclusion
The pri-let-7a-1 rs10739971 polymorphism has potential as a prognostic biomarker of GC, especially for female and Borrmann type I/II patients. The pri-let-7a-1 rs10739971 polymorphism might affect serum mature let-7a expression, which might partly explain the mechanism of the pri-let-7a-1 rs10739971 polymorphism in GC survival. Future large-sample studies and mechanism experiments are needed to prove our findings.
Disclosure
The authors report no conflicts of interest in this work.
References
Kobayashi E, Satow R, Ono M, et al. MicroRNA expression and functional profiles of osteosarcoma. Oncology. 2014;86(2):94–103. | ||
Haselmann V, Kurz A, Bertsch U, et al. Nuclear death receptor TRAIL-R2 inhibits maturation of let-7 and promotes proliferation of pancreatic and other tumor cells. Gastroenterology. 2014;146(1):278–290. | ||
Ahn DH, Rah H, Choi YK, et al. Association of the miR-146aC>G, miR-149T>C, miR-196a2T>C, and miR-499A>G polymorphisms with gastric cancer risk and survival in the Korean population. Mol Carcinog. 2013;52(Suppl 1):E39–E51. | ||
Stenholm L, Stoehlmacher-Williams J, Al-Batran SE, et al. Prognostic role of microRNA polymorphisms in advanced gastric cancer: a translational study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Ann Oncol. 2013;24(10):2581–2588. | ||
Hu Z, Chen J, Tian T, et al. Genetic variants of miRNA sequences and non-small cell lung cancer survival. J Clin Invest. 2008;118(7):2600–2608. | ||
Yoon KA, Yoon H, Park S, et al. The prognostic impact of microRNA sequence polymorphisms on the recurrence of patients with completely resected non-small cell lung cancer. J Thorac Cardiovasc Surg. 2012;144(4):794–807. | ||
Wu C, Li M, Hu C, Duan H. Prognostic role of microRNA polymorphisms in patients with advanced esophageal squamous cell carcinoma receiving platinum-based chemotherapy. Cancer Chemother Pharmacol. 2014;73(2):335–341. | ||
De Ruyck K, Duprez F, Ferdinande L, et al. A let-7 microRNA polymorphism in the KRAS 3′-UTR is prognostic in oropharyngeal cancer. Cancer Epidemiol. 2014;38(5):591–598. | ||
Liu CJ, Tsai MM, Tu HF, Lui MT, Cheng HW, Lin SC. miR-196a overexpression and miR-196a2 gene polymorphism are prognostic predictors of oral carcinomas. Ann Surg Oncol. 2013;20(Suppl 3):S406–S414. | ||
Guan X, Sturgis EM, Song X, et al. Pre-microRNA variants predict HPV16-positive tumors and survival in patients with squamous cell carcinoma of the oropharynx. Cancer Lett. 2013;330(2):233–240. | ||
Du M, Lu D, Wang Q, et al. Genetic variations in microRNAs and the risk and survival of renal cell cancer. Carcinogenesis. 2014;35(7):1629–1635. | ||
Kim K, Madak-Erdogan Z, Ventrella R, Katzenellenbogen BS. A MicroRNA196a2 and TP63 circuit regulated by estrogen receptor-alpha and ERK2 that controls breast cancer proliferation and invasiveness properties. Horm Cancer. 2013;4(2):78–91. | ||
Xu J, Yin Z, Shen H, et al. A genetic polymorphism in pre-miR-27a confers clinical outcome of non-small cell lung cancer in a Chinese population. PLoS One. 2013;8(11):e79135. | ||
Sun X, Qin S, Fan C, Xu C, Du N, Ren H. Let-7: a regulator of the ERalpha signaling pathway in human breast tumors and breast cancer stem cells. Oncol Rep. 2013;29(5):2079–2087. | ||
Zhao Y, Deng C, Wang J, et al. Let-7 family miRNAs regulate estrogen receptor alpha signaling in estrogen receptor positive breast cancer. Breast Cancer Res Treat. 2011;127(1):69–80. | ||
Tian T, Shu Y, Chen J, et al. A functional genetic variant in microRNA-196a2 is associated with increased susceptibility of lung cancer in Chinese. Cancer Epidemiol Biomarkers Prev. 2009;18(4):1183–1187. | ||
Xu Q, Liu JW, He CY, et al. The interaction effects of pri-let-7a-1 rs10739971 with PGC and ERCC6 gene polymorphisms in gastric cancer and atrophic gastritis. PLoS One. 2014;9(2):e89203. | ||
Xie K, Liu J, Zhu L, et al. A potentially functional polymorphism in the promoter region of let-7 family is associated with survival of hepatocellular carcinoma. Cancer Epidemiol. 2013;37(6):998–1002. | ||
Xu Q, Dong Q, He C, et al. A new polymorphism biomarker rs629367 associated with increased risk and poor survival of gastric cancer in Chinese by up-regulated miRNA-let-7a expression. PLoS One. 2014;9(4):e95249. | ||
Xu Q, Yuan Y, Sun LP, et al. Risk of gastric cancer is associated with the MUC1 568 A/G polymorphism. Int J Oncol. 2009;35(6):1313–1320. | ||
Liu R, Zhang C, Hu Z, et al. A five-microRNA signature identified from genome-wide serum microRNA expression profiling serves as a fingerprint for gastric cancer diagnosis. Eur J Cancer. 2011;47(5):784–791. | ||
Xie YL, Yang YJ, Tang C, et al. Estrogen combined with progesterone decreases cell proliferation and inhibits the expression of Bcl-2 via microRNA let-7a and miR-34b in ovarian cancer cells. Clin Transl Oncol. 2014;16(10):898–905. | ||
Yi JH, Do IG, Jang J, et al. Anti-tumor efficacy of fulvestrant in estrogen receptor positive gastric cancer. Sci Rep. 2014;4:7592. | ||
Yang B, Wu G, Wang X, Zhang X. Discussion of modifying stage IV gastric cancer based on Borrmann classification. Tumour Biol. 2013;34(3):1485–1491. | ||
Akbari Moqadam F, Pieters R, den Boer ML. The hunting of targets: challenge in miRNA research. Leukemia. 2013;27(1):16–23. | ||
Xu Y, Liu L, Liu J, et al. A potentially functional polymorphism in the promoter region of miR-34b/c is associated with an increased risk for primary hepatocellular carcinoma. Int J Cancer. 2011;128(2):412–417. |
Supplementary materials
Serum RNA extraction and real-time quantitative PCR reaction for miRNA expression in vivo
Approximately 6 mL venous blood was collected from each subject. Serum total RNA was extracted using a method described by Liu et al1 with some modifications. Serum was separated by centrifugation at 3,000× g for 10 minutes, followed by a 15 minutes high-speed centrifugation at 12,000× g to completely remove cell debris. The supernatant serum was recovered and stored at −80°C until further processing. Total RNA was extracted from 200 μL of serum by acid phenol/chloroform purification and centrifugation in isopropyl alcohol. Every sample was all in 20 μL RNA-free ddH2O solution and 6 μL of total RNA was reverse-transcribed to cDNA using One Step PrimeScript miRNA cDNA Synthesis Kit (TaKaRa Biotechnology, Dalian, People’s Republic of China). Real-time PCR was performed using a miRcute miRNA qPCR detection kit (Tiangen Biotech, Beijing, People’s Republic of China) on the Thermal Cycler Dice Real Time System (TaKaRa Biotechnology). To calculate the levels of the miRNAs, synthetic hsa-let-7a at known concentrations (TaKaRa Biotechnology) were also reverse-transcribed and amplified. The concentration of each miRNA was then calculated according to the standard curve. All reactions, including no-template controls, were run in duplicate.
Reference
Liu R, Zhang C, Hu Z, et al. A five-microRNA signature identified from genome-wide serum microRNA expression profiling serves as a fingerprint for gastric cancer diagnosis. Eur J Cancer. 2011;47:784–791. |
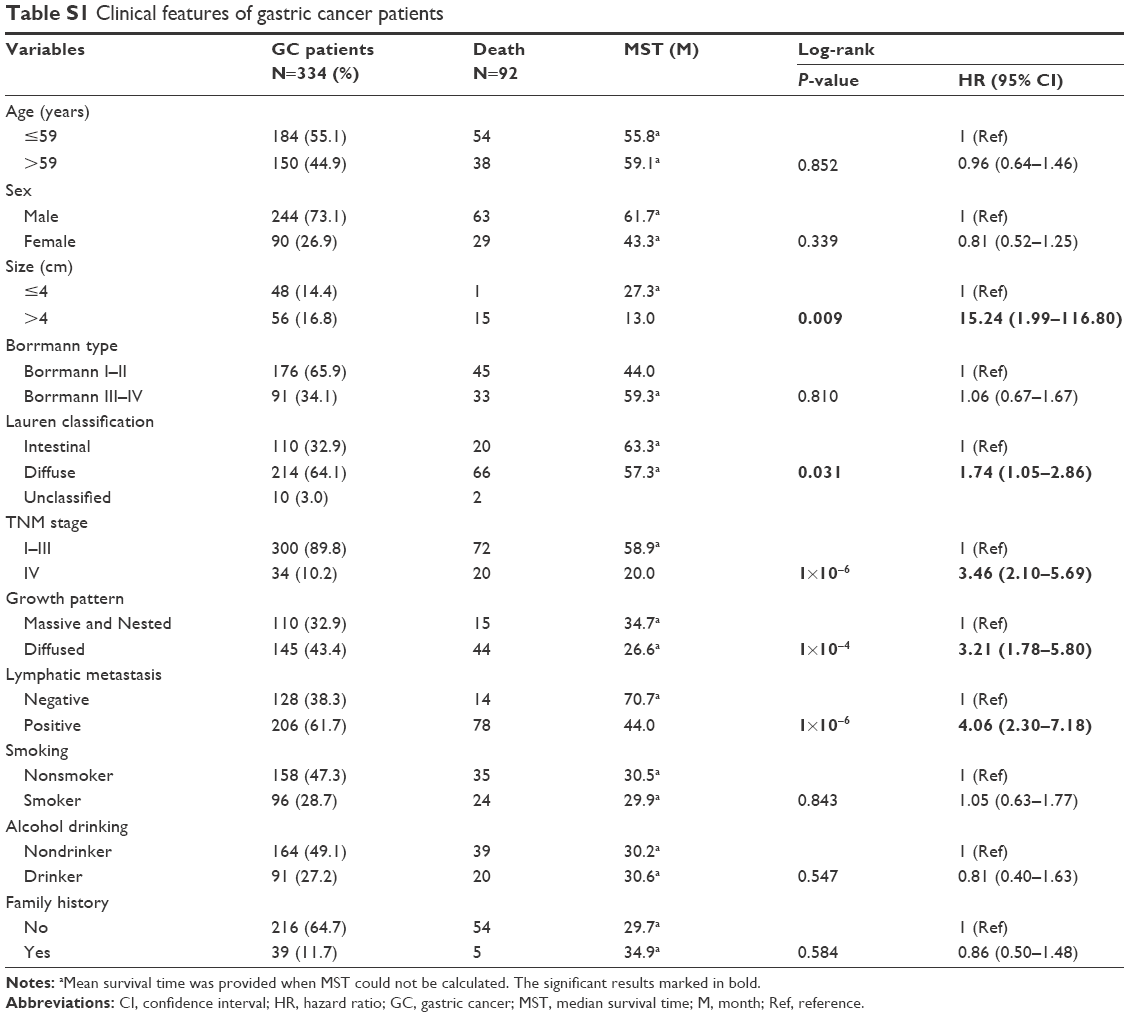 | Table S1 Clinical features of gastric cancer patients |
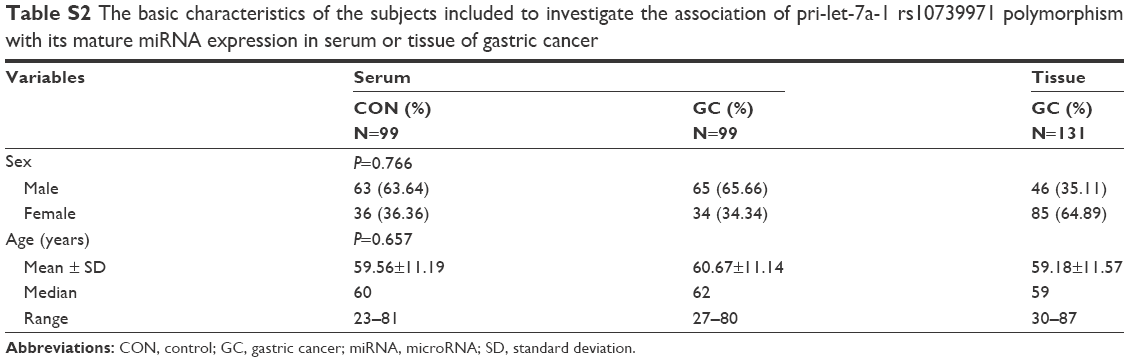 | Table S2 The basic characteristics of the subjects included to investigate the association of pri-let-7a-1 rs10739971 polymorphism with its mature miRNA expression in serum or tissue of gastric cancer |
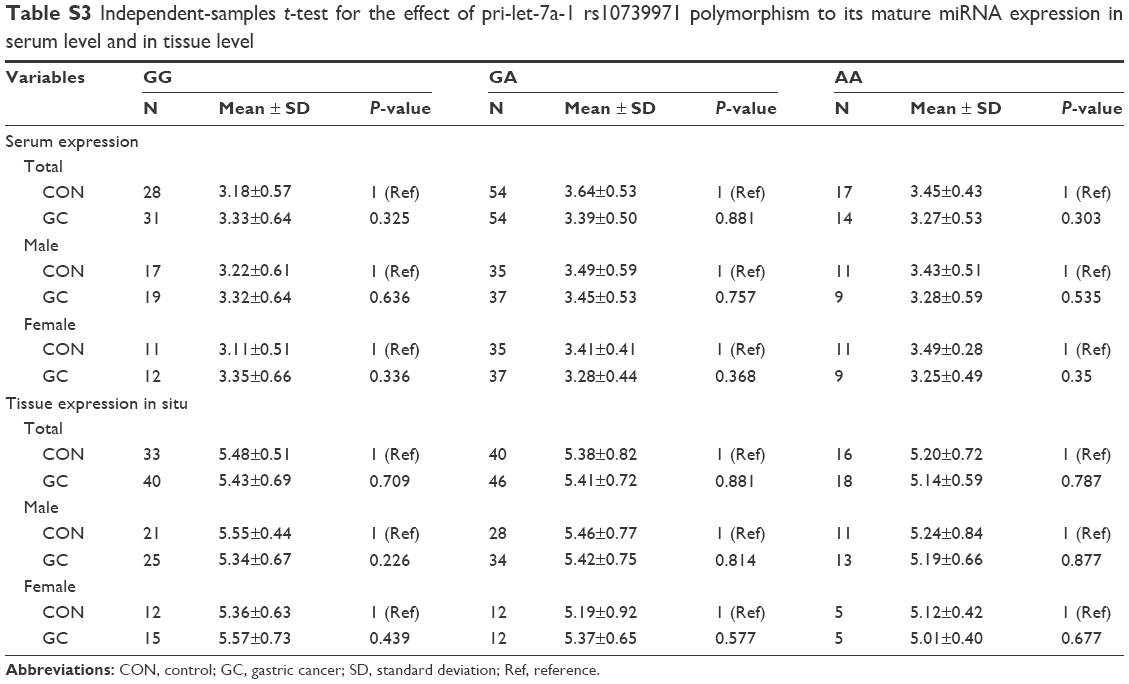 | Table S3 Independent-samples t-test for the effect of pri-let-7a-1 rs10739971 polymorphism to its mature miRNA expression in serum level and in tissue level |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.