")
Back to Journals » Clinical Ophthalmology » Volume 15
Preventive Practices of Ophthalmologists During COVID-19 Pandemic
Authors Syed AAO , Jahan S, Aldahlawi AA, Alghazzawi EA
Received 12 December 2020
Accepted for publication 23 February 2021
Published 23 March 2021 Volume 2021:15 Pages 1267—1275
DOI https://doi.org/10.2147/OPTH.S295730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Amjad Ali Omar Syed,1 Saulat Jahan,2 Alaa Ali Aldahlawi,1 Eihab Ali Alghazzawi1
1Ophthalmology Department, King Fahad Specialist Hospital, Ministry of Health, Buraidah, Qassim, Saudi Arabia; 2Research & Innovation Unit, Family Medicine Academy, Buraidah, Qassim, Saudi Arabia
Correspondence: Amjad Ali Omar Syed
Ophthalmology Department, King Fahad Specialist Hospital, PO Box 2290, Buraidah, Saudi Arabia
Tel +966 502668450
Email [email protected]
Purpose: To explore ophthalmologists’ preventive practices, and their perceived seriousness and perceived risk of transmission of coronavirus disease 2019 (COVID-19).
Methods: In a cross-sectional study, a semi-structured questionnaire was distributed online among ophthalmologists. Questions about COVID-19 infection, perceived seriousness, perceived risk of transmission, and recommended COVID-19 preventive practices were asked. Based on the adoption of a preventive measure and its frequency, a maximum preventive score of 25 was computed.
Results: Among 126 respondents, the mean±SD age was 45.3± 10.9 years, and 57.9% worked in a tertiary care hospital. Regarding preventive practices, 96.8% of ophthalmologists wore face masks, 89.6% avoided talking during the slit lamp examination, and 72.2% wore gloves during the ophthalmic examination. Availability of plastic barriers and regular disinfection of slit lamps were reported by 78.6% and 43.7% of ophthalmologists, respectively. The mean preventive score increased with increasing age (p=0.001), and was higher for males (18.96± 4.60) compared to females (17.81± 4.96). The mean score for perceived severity was higher (p< 0.0001) among ophthalmologists with more than 10 years of experience (8.76± 1.58) than those with experience of 10 years or less (7.49± 1.86). Out of 29 ophthalmologists who had been tested for COVID-19, 11 were found to be positive, giving an overall incidence of COVID-19 infection of 8.7%.
Conclusion: The ophthalmologists were generally compliant with recommended preventive measures. Some preventive measures, such as the wearing of gloves and regular disinfection of slit lamps, need improvement. We recommend creating awareness of and monitoring for COVID-19 infection control measures in healthcare settings.
Keywords: coronavirus, infection control, perceived risk, perceived seriousness, SARS-CoV-2, transmission
Introduction
The coronavirus disease 2019 (COVID-19) pandemic is a global health threat to the general population as well as healthcare workers. Although all specialties in the healthcare field have an increased risk of exposure to COVID-19, some specialized fields are more at risk than others. One of these specialties, because of its specific clinical practice, is ophthalmology.
The whistleblower Dr. Li Wenliang, who succumbed to COVID-19, was a young ophthalmologist at Wuhan Central Hospital, China.1,2 An outbreak of COVID-19 was also reported in an ophthalmology department in Oslo, Norway.3
The modes of transmission of COVID-19 include through respiratory droplets by contact with an infected person and via contaminated surfaces.4 The ophthalmic examination requires close proximity with patients, which increases the risk of disease transmission among ophthalmologists as well as ophthalmology patients.3,5,6 Also, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), detected in tears and conjunctival secretions of infected patients with conjunctivitis, poses an increased risk of infection in ophthalmologists.7,8 Direct contact of certain instruments with the conjunctival surface of patients may be another route of disease transmission.9 Transmission of the disease by asymptomatic patients poses another hidden risk to ophthalmologists.10 Moreover, ophthalmologists generally deal with a substantial proportion of elderly patients, who are a high-risk group for COVID-19 infections.11
In the absence of a well-established treatment for COVID-19, infection prevention is an important strategy to mitigate the disease.3 Because of the increased risk of COVID-19 to ophthalmologists,12 they need to adopt strict preventive measures.4,9 International organizations, such as the World Health Organization13 and Centers for Disease Control and Prevention,14 have laid down guidelines for healthcare settings. Various ophthalmology organizations, including the American Academy of Ophthalmology,15 have developed guidelines for COVID-19 infection prevention in ophthalmic settings.4 Furthermore, researchers have revisited strategies used in the ophthalmic setting during previous coronavirus outbreaks, and looked into the effectiveness of those strategies.3
Given the evolving and uncertain situation, and the increased risk to ophthalmologists, it is important that they strictly follow the preventive measures. Therefore, it is also important to explore the ophthalmologists’ compliance with the recommended preventive measures. Thus, this study was designed to determine the preventive practices of ophthalmologists regarding COVID-19.The survey also explored COVID-19 symptoms and tests among respondents, their perception regarding the seriousness of COVID-19, and its risk of transmission to the ophthalmologists during ophthalmic examinations. The results of this study could be used to design strategies to improve the compliance of ophthalmologists with the COVID-19 preventive measures.
Materials and Methods
A cross-sectional study was carried out among ophthalmologists working in diverse healthcare settings in various countries. We carried out a literature review to design our questionnaire according to the study objectives and available literature regarding preventive measures against COVID-19 infection in ophthalmology practice and healthcare settings.3,13–15
A self-administered, semi-structured questionnaire was designed. The survey consisted of 24 questions on demographic characteristics, perceived severity of disease and perceived risk of transmission of COVID-19, awareness about the availability of national and international COVID-19 prevention guidelines for ophthalmologists, COVID-19 symptoms and tests among respondents, and preventive practices of ophthalmologists. Respondents were asked to score the perceived severity of disease and perceived risk of transmission of COVID-19 to the ophthalmologist, on a scale of 1–10.
Nine questions were asked about preventive practices regarding COVID-19. These questions asked respondents to answer “yes” or “no” about COVID-19 preventive practices. The survey explored whether the ophthalmologist and the patient wore face masks, whether social distancing was maintained while taking the patient’s history, and whether talking was avoided during slit lamp examination. Respondents were also asked whether patients were screened for COVID-19 infection. Furthermore, questions were asked about the use of gloves, hand hygiene practices, and slit lamp disinfection after each patient examination. For each of these preventive measures, the frequency of the measure was asked about on a three-point Likert scale, as “occasionally”, “often”, or “always”. From these responses, a “preventive score” variable was created, assigning zero for not adopting a preventive measure, 1 for “occasionally”, 2 for “often”, and 3 for “always” adopting a preventive measure. The respondents were also asked about the availability of a plastic barrier/breath shield on the slit lamp, and this was scored zero for non-availability of a plastic barrier and 1 for its being available. These scores were summed up, resulting in a maximum preventive score of 25.
Three questions were asked about COVID-19 infection. Those questions were whether the respondent had symptoms related to COVID-19, whether they were tested for COVID-19, and the result of the test if were tested for COVID-19.
The study was approved by the Qassim Research Ethics Committee (registration no. H-04-Q-001). The survey was piloted on a small scale before launch. During the pilot testing, the appropriateness of each question was evaluated and wording of the questions and response options were assessed. This was done according to guidelines in the conduct and reporting of survey research.16,17
The data were collected using convenience sampling, by an online survey, designed and submitted to various WhatsApp groups of ophthalmologists, using Google Forms.18 An explanation of the study’s objectives, as well as the informed consent form, were present at the start of the questionnaire. The online survey was anonymous and administered in the English language. The study was conducted in accordance with the principles of the Declaration of Helsinki. The survey was conducted over a period of 18 days from 15 August 2020 to 2 September 2020. To encourage completion of the survey, personal communication with ophthalmologist peers was also established. Three reminder messages were sent to ensure a reasonable participation rate.
The data collected were coded and cleaned in Microsoft Excel (2016). Variables were processed and analyzed using IBM SPSS Statistics (version 21) for Microsoft Windows.19 The results were analyzed using descriptive and inferential statistics. Descriptive statistics of counts with percentages were used for categorical data, and means and standard deviations for continuous variables. Statistical analyses explored the relationships between respondents’ demographics and preventive score, perceived severity score, and perceived risk of transmission score. Differences in continuous variables were analyzed with the independent t-test and ANOVA F-test. Statistical significance was considered as a two-tailed p-value <0.050.
Results
A total of 126 ophthalmologists from 10 countries completed the online survey. The mean age of the ophthalmologists was 45.3±10.9 years. The demographic and specific characteristics of the participating ophthalmologists are detailed in Table 1. Eighty-six (68.3%) participants were male. Most participants were 40 years and above in age (n=81, 64.3%). Ophthalmologists from various countries participated in this survey, with Saudi Arabia being the most represented country (n=71, 56.3%), followed by Pakistan (n=32, 25.4%) and Egypt (n=11, 8.7%). Other countries included Oman, Jordan, the UK, Yugoslavia, South Sudan, Yemen, and Brazil.
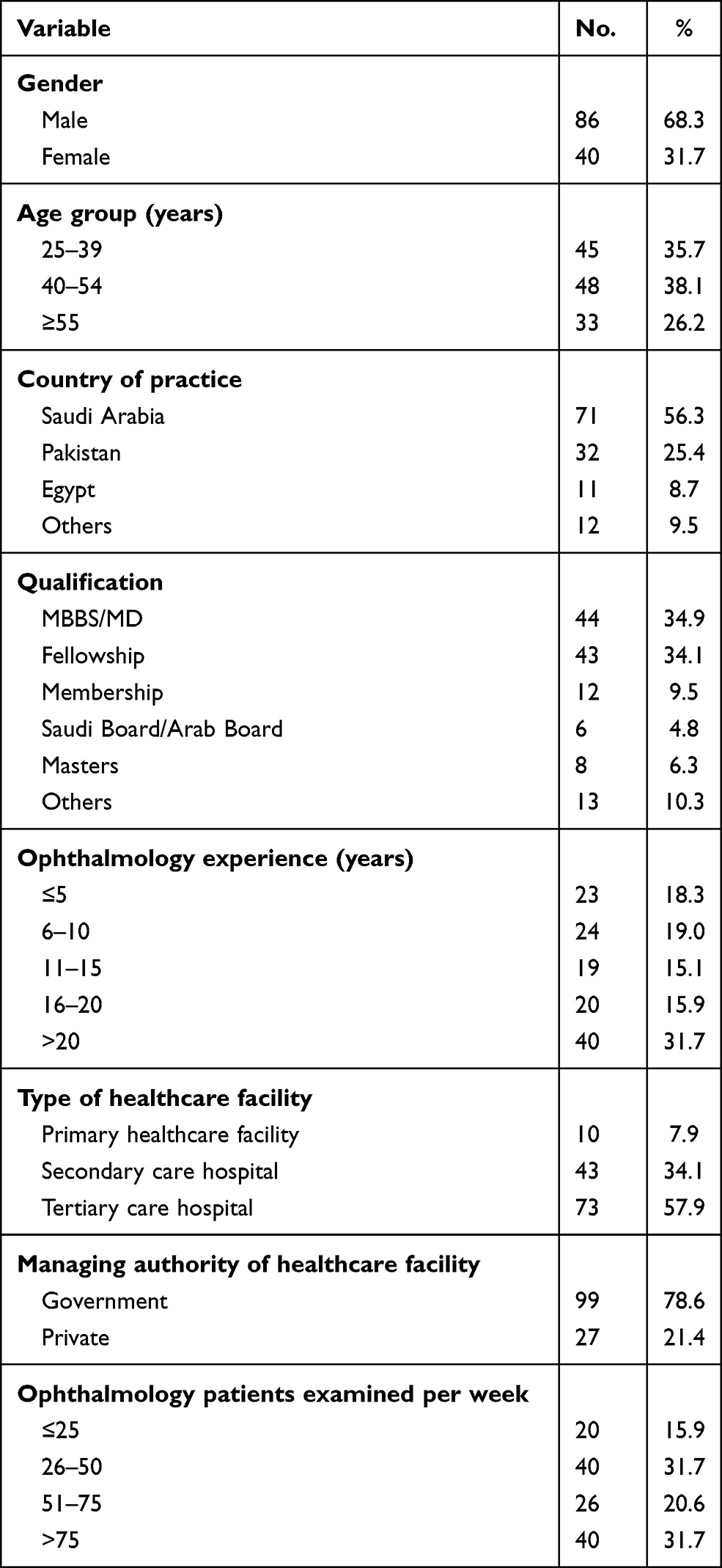 |
Table 1 Demographic and Specific Characteristics of the Ophthalmologists (n=126) |
When asked about the availability of national and international COVID-19 prevention guidelines available for ophthalmologists, 68.5% responded that international guidelines were available and 59.8% stated that national guidelines were available in their country of practice.
The ophthalmologists were asked about their preventive practices against COVID-19. For a practiced preventive measure, the respondents were further asked if it was practiced “always”, “often”, or “occasionally” (Table 2). The most practiced preventive measure was the wearing of face masks (96.8%) by ophthalmologists, while the least practiced preventive measure was disinfection of the slit lamp (43.7%) after examination of each patient. An important finding in our study was that 91 ophthalmologists (72.3%) wore gloves and only 70 (55.6%) stated that they “always” wore gloves. The reasons for not using gloves included discomfort and non-availability; moreover, 15 (11.9%) ophthalmologists stated that they do not use gloves because they are not convinced that the gloves prevent transmission of infection.
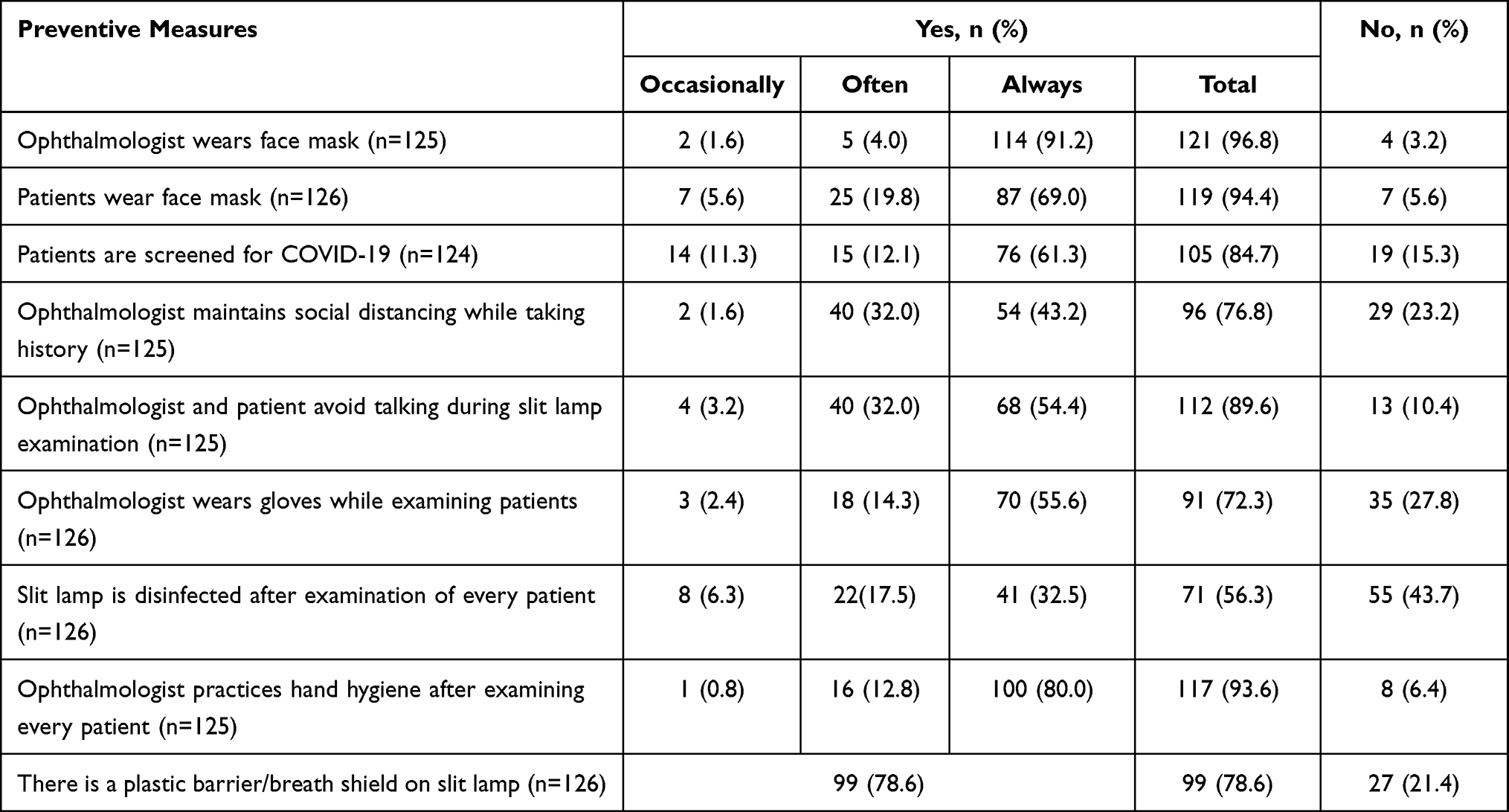 |
Table 2 Preventive Measures Against COVID-19 |
The overall mean preventive score was 18.6±4.73). Table 3 shows the association of demographic characteristics with mean preventive scores. The mean preventive scores increased with increasing age (p=0.001). The mean preventive scores varied significantly (p=0.015) with years of experience, and those with less than 5 years of ophthalmology experience had the lowest mean scores (15.83±6.29).
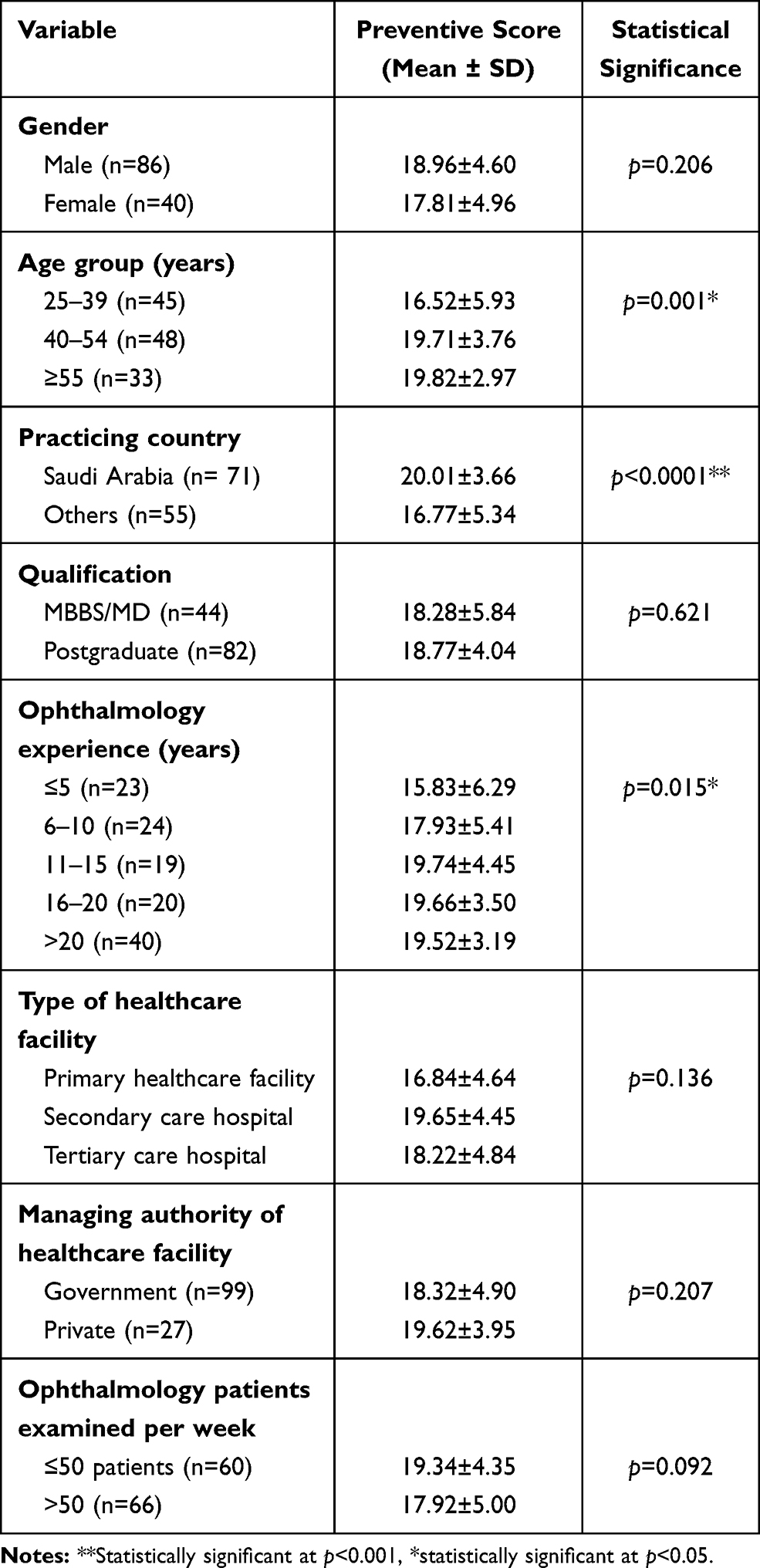 |
Table 3 Association of Demographic Characteristics of the Ophthalmologists with Preventive Scores (n=126) |
Overall, the mean score for perceived severity of COVID-19, on a scale of 1–10, was 8.3±1.8 (range: 2−10). The mean score for perceived risk of COVID-19 transmission to ophthalmologists, on a scale of 1–10, was 8.0±2.0 (range: 2−10). Table 4 displays the association of demographic characteristics with mean scores of perceived severity of COVID-19 and perceived risk of transmission to ophthalmologists. Females had a higher mean score for perceived risk of transmission (8.58±1.65) compared to males (7.70±2.12), and this difference was statistically significant (p=0.022). The perceived risk of severity varied across the three age groups, with the 40–54-year age group having the highest mean score (8.73±1.50). The difference across age groups was statistically significant (p=0.002). The perceived severity (9.20±0.89) and perceived risk of transmission (8.85±1.18) were highest among those who were examining fewer than 25 patients per week.
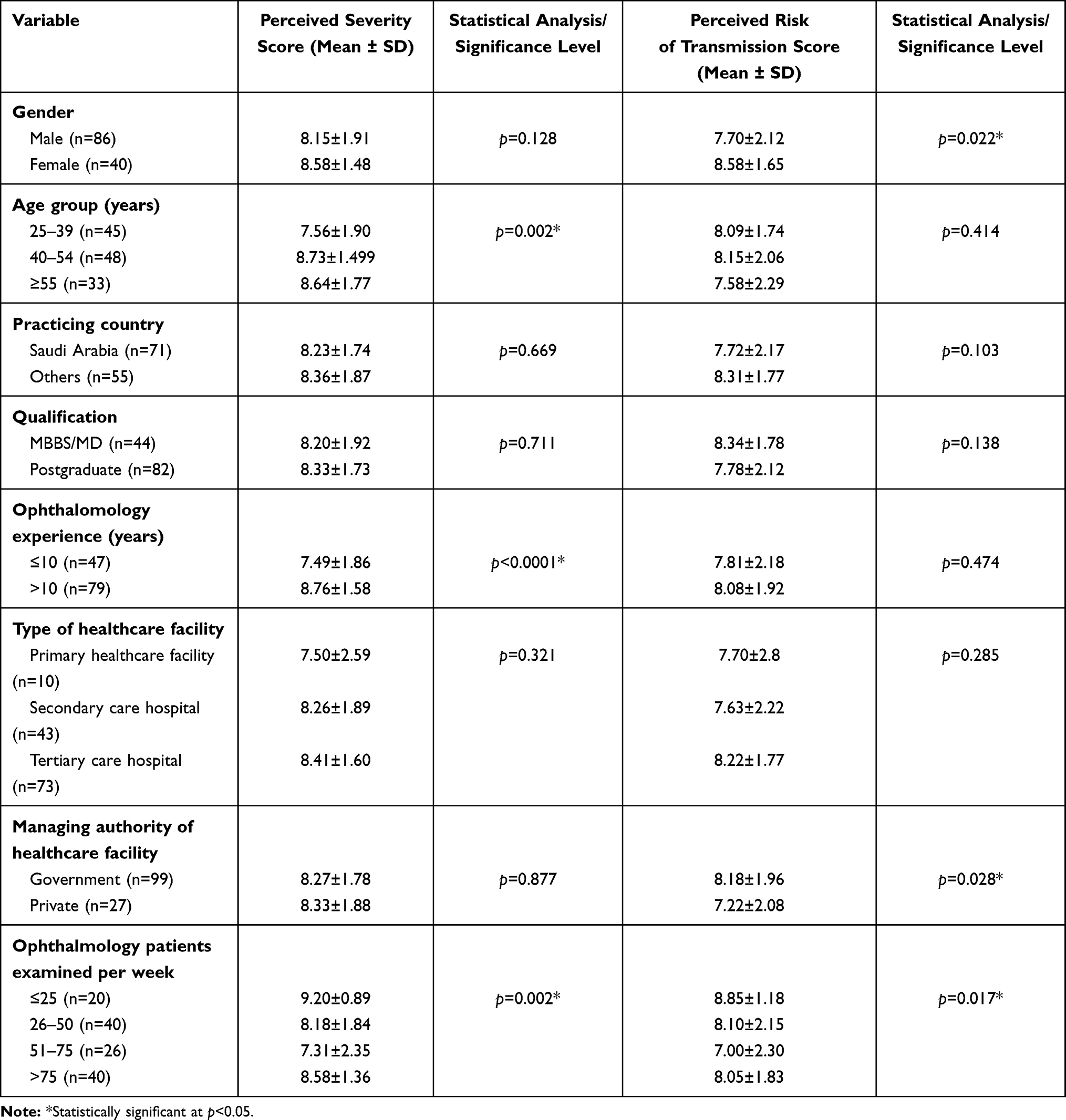 |
Table 4 Association of Demographic Characteristics of the Ophthalmologists with Perceived Severity and Perceived Risk of Transmission Scores (n=126) |
In our study, 33 ophthalmologists (26.2%) stated that they had had symptoms similar to those of COVID-19 infection (fever, dry cough, and fatigue) during the past 6 months. The demographic characteristics of these ophthalmologists are detailed in Table 5. In our sample, 20 males (60.6%) and 13 females (39.4%) reported having had symptoms similar to COVID-19 infection. More than half (54.5%) of those having symptoms belonged to the 25–39-year age group.
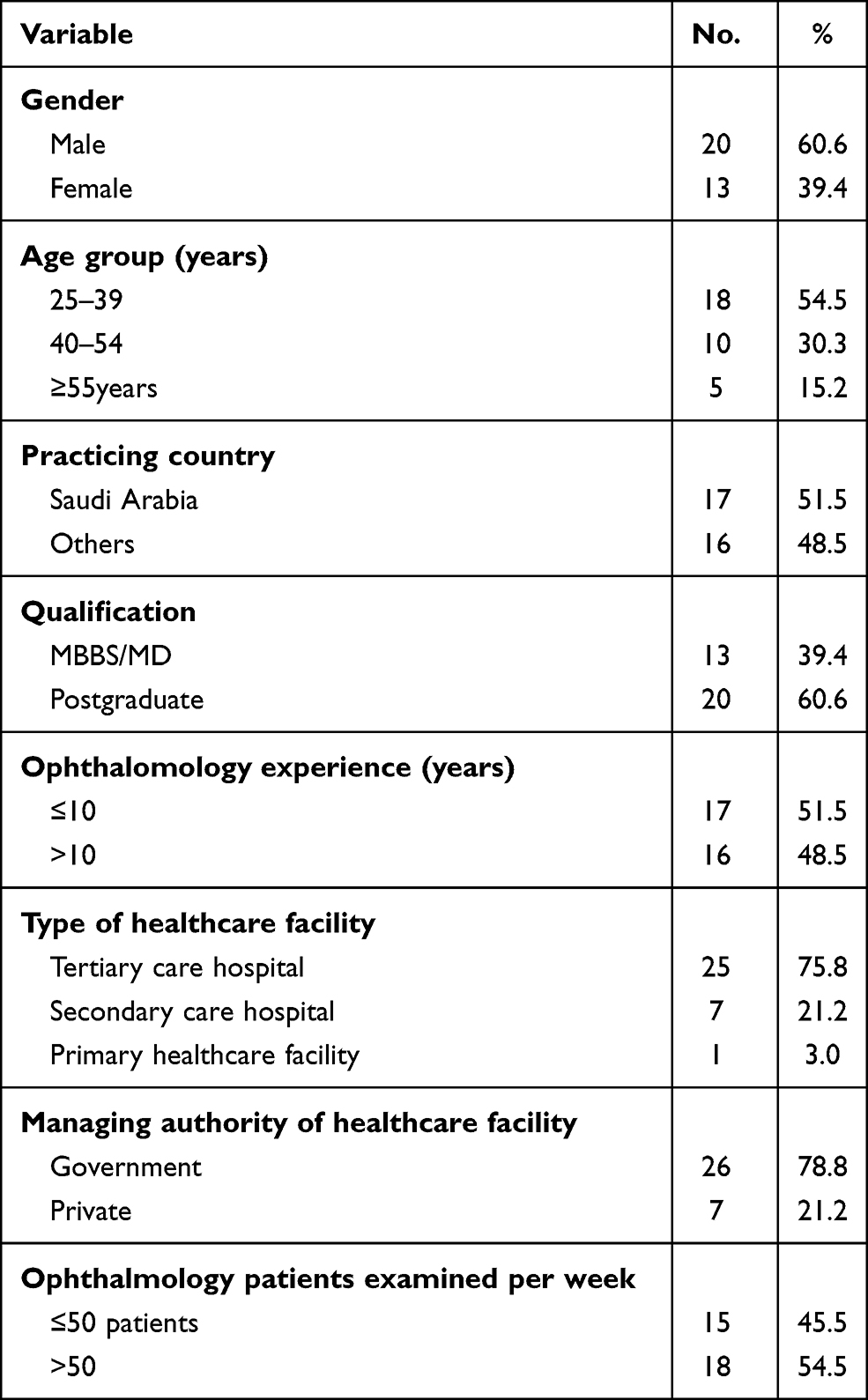 |
Table 5 Demographic Characteristics of the Ophthalmologists with a History of COVID-19 Symptoms (n=33) |
On analyzing the preventive practices of the ophthalmologists reporting COVID-19 symptoms (n=33), it was found that 11 (33.3%) of them did not wear gloves, while for 14 (42.4%) of them, the slit lamp was not disinfected after examination of every patient. However, a plastic barrier/breath shield on the slit lamp was available to 29 ophthalmologists (87.9%). Furthermore, eight ophthalmologists (24.2%) did not maintain social distance while taking a history. Although not statistically significant, the preventive scores of those reporting symptoms (18.10±5.06) were lower than for those who did not report experiencing COVID-19 symptoms (18.78±4.63).
The ophthalmologists who tested positive for COVID-19 perceived it as a more severe disease (8.45±1.75) than those who tested negative (7.83±2.23). Similarly, perceived risk of transmission was higher among those who tested positive (9.55±0.69) than those who were negative (7.50±2.18) for the test (p=0.001). Regarding preventive practices, no statistically significant differences were found on comparing those who tested positive with those testing negative for COVID-19.
In our study, the overall incidence of COVID-19 infection was 8.7% (11/126). A total of 29 ophthalmologists had been tested for COVID-19 infection. Out of these, 11 (37.9%), comprising seven males (63.6%) and four females (36.4%), had tested positive for COVID-19 infection (Figure 1). Eight (72.7%) were working in tertiary care hospitals and 10 (90.9%) in a government healthcare facility.
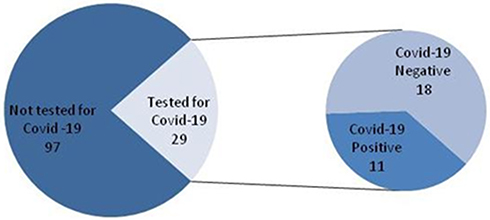 |
Figure 1 Number of COVID-19 tests and their results for respondent ophthalmologists (n=126). |
The preventive score of those with a positive test (17.00±6.99) was lower than for those who had a negative test for COVID-19 (18.06±5.71); however, the difference was not statistically significant. The mean score for perceived seriousness of disease was 8.45±1.75 for those who tested positive compared to 7.83±2.23 for those who tested negative for COVID-19. The mean score for perceived risk of transmission of COVID-19 to ophthalmologists was 9.55±0.69 for those who tested positive compared to 7.50±2.18 for those who tested negative for COVID-19, and the difference was statistically significant (p=0.001).
Regarding the preventive practices of the ophthalmologists who tested positive for COVID-19, five (45.5%) reported that the slit lamps were not disinfected after examination of every patient, while more than one-quarter reported not wearing gloves (n=3, 27.3%), not maintaining social distance while taking history (n=3, 27.3%), not avoiding talking while examining patients (n=3, 27.3%), and non-availability of a plastic barrier/breath shield on the slit lamp (n=3, 27.3%).
Discussion
COVID-19 is a serious disease and has taken a toll on the general population as well as healthcare workers.20 To reduce the risk of transmission of the disease, ophthalmologists need to be very careful in complying with the recommended preventive measures.11,21,22 The previous severe acute respiratory syndrome (SARS) outbreak provides evidence in favor of adopting preventive measures, as those ophthalmologists who adopted these measures had a low risk of being infected with SARS.22
Our study showed that the respondents were well aware of the seriousness of COVID-19 and its risk of transmission to ophthalmologists. Most of the preventive measures recommended for ophthalmologists15,23,24 were followed by the respondent ophthalmologists; however, compliance varied for different preventive measures.
To prevent the viral spread by COVID-19 carriers, face masks are recommended for patients and healthcare workers in ophthalmic clinics.15,23–25 In our study, the majority of the ophthalmologists (96.8%) and their patients (94.4%) were compliant with the wearing of face masks. However, the frequency of “always” wearing a mask was low (69%) for the patients. This underscores the need to increase awareness about the importance of wearing face masks among the general public.
One of the most important preventive measures for COVID-19 is to maintain a social distance of at least 1 meter to avoid transmission of the virus.24 While taking a patient’s history, social distancing was not maintained by approximately one-quarter (23.2%) of the ophthalmologists in our study. However, we did not explore the reasons for not maintaining social distance while taking the history. One of the possible explanations is the setting or small size of some ophthalmic clinics, where it may not be possible to maintain the recommended social distance.
The use of slit lamp barriers or breath shields can reduce the risk of droplet transmission between the patient and the ophthalmologist, thus protecting both of them.15,23–25 The guidelines from major ophthalmic organizations have recommended the installation of slit lamp barriers.15,23,24 In our study, a plastic barrier/breath shield was not available on the slit lamp used by one-fifth (21.4%) of the ophthalmologists. A similar finding is reported by a study from Jordan, where 59.1% of ophthalmologists reported not using a slit lamp barrier.26
The use of gloves is highly recommended for the prevention of COVID-19.24,25 In our study, only 55.6% of ophthalmologists stated that they “always” wore gloves. The reason for not using gloves for around 12% of ophthalmologists was that they were not convinced that gloves prevented transmission of infection. This finding underscores the importance of creating awareness among physicians about the preventive measures for COVID-19. Furthermore, the preventive practices of healthcare staff need to be monitored by the infection control personnel.
For both the ophthalmologist and the patient, refraining from talking during the slit lamp examination is recommended.15,24,27 In our study, 10.4% of the ophthalmologists stated that they did not avoid talking during the slit lamp examination. In our opinion, this simple measure could be practiced by 100% of ophthalmologists if awareness were created in the ophthalmologists, and the patients were also educated on this important preventive measure.
It is recommended that the slit lamp is disinfected after the examination of each patient.15,23,24,27 However, in our study, a substantial proportion (43.7%) of the ophthalmologists reported that the slit lamp was not disinfected after the examination of every patient. This finding highlights the importance of administrative monitoring of infection control measures in healthcare settings.
Screening for patients with symptoms of COVID-19 is important to protect the patients and the healthcare staff at the ophthalmic clinic.11,15,22–24,27 In our study, the majority (84.7%) of the ophthalmologists reported that the patients were screened for COVID-19 infection.
In the present study, the overall incidence of COVID-19 infection was 8.7%, which is lower than the incidence (12.9%) reported for ophthalmologists in Spain where, out of 62 ophthalmologists, eight tested positive for COVID-19 infection.28 In contrast, the incidence in our study was higher than the incidence of symptomatic COVID-19 among ophthalmologists in 10 hospitals in Wuhan, which was reported to be 2.95% (14/475).29
Our study has certain limitations. It was an online survey with convenience sampling. Because of our participant recruitment method, we were unable to determine the number of eligible ophthalmologists accessing the survey and, as a result, the response rate could not be calculated. The use of convenience sampling to recruit survey participants may reduce statistical representativeness, thus limiting the generalizability of the study results. Those who responded may have different preventive practices from those who did not respond. There may have been both self-reporting and social desirability biases in this study, and the accuracy of the responses may vary. The questionnaire was self-administered and some questions may have been misunderstood by the respondents. However, the questionnaire was pretested to identify unclear statements or questions. Even though participants were asked whether social distance was maintained or not, the reason for not maintaining it was not asked about in this study. Similarly, the reasons for the slit lamp not having a barrier were not queried. Although we gathered information about COVID-19-like symptoms and tests for COVID-19 among ophthalmologists, we did not seek information about the possible source of infection, which would have been informative to determine whether those who tested positive acquired the infection in the healthcare setting or whether there was some other source of infection.
Raising awareness, implementing strict regulations, monitoring, and frequent reminders by memo and posters are recommended to mitigate the spread of infection in an ophthalmic setting. Awareness can be created through lectures and brochures. Posters about the seriousness of COVID-19 should be displayed at appropriate places in the hospital. Infection control personnel should monitor the compliance of healthcare staff with recommended preventive measures as well as disinfection of the equipment and surroundings. Gloves and hand sanitizers need to be made freely available in healthcare settings.
Conclusion
Our study results suggest that certain preventive measures, such as the wearing of gloves, regular disinfection of the slit lamp, and the availability of slit lamp barriers, need to be improved, so that both the ophthalmologists and their patients are protected. We recommend creating awareness about preventive measures against COVID-19 and strict monitoring of infection control measures in healthcare settings.
Acknowledgments
We would like to thank Aliba Omar Syed, an MPH student at the University of California, Irvine (UCI), for reviewing and making valuable suggestions to the manuscript. The authors are grateful to all respondent ophthalmologists for their valuable time and effort in completing the survey.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee KJ. Coronavirus kills Chinese whistleblower ophthalmologist. American Academy of Ophthalmology; February 10, 2020. Available from: https://www.aao.org/headline/coronavirus-kills-chinese-whistleblower-ophthalmol.
2. Parrish RK, Stewart MW, Duncan Powers SL. Ophthalmologists are more than eye doctors—in memoriam Li Wenliang. Am J Ophthalmol. 2020;213:A1–A2. doi:10.1016/j.ajo.2020.02.014
3. Jørstad ØK, Moe MC, Eriksen K, Petrovski G, Bragadóttir R. Coronavirus disease 2019 (COVID-19) outbreak at the department of ophthalmology, Oslo University Hospital, Norway. Acta Ophthalmol. 2020;98(3):e388–e389. doi:10.1111/aos.14426
4. Minocha A, Sim SY, Than J, Vakros G. Survey of ophthalmology practitioners in A&E on current COVID-19 guidance at three Major UK Eye Hospitals. Eye. 2020;1–3. doi:10.1038/s41433-020-0857-5
5. Lim LW, Yip LW, Tay HW, et al. Sustainable practice of ophthalmology during COVID-19: challenges and solutions. Graefes Arch Clin Exp Ophthalmol. 2020;258(7):1427–1436. doi:10.1007/s00417-020-04682-z
6. Amesty MA, Alió Del Barrio JL, Alió JL. COVID-19 disease and ophthalmology: an update. Ophthalmol Ther. 2020;9(3):1–12. doi:10.1007/s40123-020-00260-y
7. Xia J, Tong J, Liu M, Shen Y, Guo D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J Med Virol. 2020;92(6):589–594. doi:10.1002/jmv.25725
8. Lu C-W, Liu X-F, Jia Z-F. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet. 2020;395(10224):e39. doi:10.1016/S0140-6736(20)30313-5
9. Chan W-M, Liu DTL, Chan PKS, et al. Precautions in ophthalmic practice in a hospital with a major acute SARS outbreak: an experience from Hong Kong. Eye (Lond). 2006;20(3):283–289. doi:10.1038/sj.eye.6701885
10. Nishiura H, Linton NM, Akhmetzhanov AR. Serial interval of novel coronavirus (COVID-19) infections. Int J Infect Dis. 2020;93:284–286. doi:10.1016/j.ijid.2020.02.060
11. Veritti D, Sarao V, Bandello F, Lanzetta P. Infection control measures in ophthalmology during the COVID-19 outbreak: a narrative review from an early experience in Italy. Eur J Ophthalmol. 2020;30(4):621–628. doi:10.1177/1120672120927865
12. Li J-PO, Lam DSC, Chen Y, Ting DSW. Novel Coronavirus disease 2019 (COVID-19): the importance of recognising possible early ocular manifestation and using protective eyewear. Br J Ophthalmol. 2020;104(3):297–298. doi:10.1136/bjophthalmol-2020-315994
13. World Health Organziation (WHO). The COVID-19 risk communication package for healthcare facilities; February 21, 2020. Available from: http://iris.wpro.who.int/handle/10665.1/14482.
14. Centers for Disease Control and Prevention (CDC). Coronavirus Disease 2019 (COVID-19); February 11, 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html.
15. American Academy of Ophthalmology (AAO). Important coronavirus updates for ophthalmologists; September 5, 2020. Available from: https://www.aao.org/headline/alert-important-coronavirus-context.
16. Kelley K, Clark B, Brown V, Sitzia J. Good practice in the conduct and reporting of survey research. Int J Qual Health Care. 2003;15(3):261–266. doi:10.1093/intqhc/mzg031
17. Tran EM, Tran MM, Clark MA, et al. Assessing the quality of published surveys in ophthalmology. Ophthalmic Epidemiol. 2020;27(5):339–343. doi:10.1080/09286586.2020.1746359
18. Google LLC. Google forms [web application]. Available from: https://google.com/forms/about/.
19. Statistical package for social sciences (SPSS) for windows. Version 21.0. Armonk, NY: IBM Corp; 2012.
20. CDC. MMWR. Characteristics of health care personnel with COVID-19 — United States, February 12–April 9, 2020. MMWR Morb Mortal Wkly Rep. 69;2020. doi:10.15585/mmwr.mm6915e6
21. Gharebaghi R, Desuatels J, Moshirfar M, Parvizi M, Daryabari S-H, Heidary F. COVID-19: preliminary clinical guidelines for ophthalmology practices. Med Hypothesis Discov Innov Ophthalmol. 2020;9(2):149–158.
22. Kuo IC, O’Brien TP. COVID-19 and ophthalmology: an underappreciated occupational hazard. Infect Control Hosp Epidemiol. 2020;1–2. doi:10.1017/ice.2020.238
23. The Royal College of Ophthalmologists (RCophth). COVID-19 clinical guidance for ophthalmologists. The Royal College of Ophthalmologists; May 2, 2020. Available from: https://www.rcophth.ac.uk/2020/05/covid-19-update-and-resources-for-ophthalmologists/.
24. EuroTimes. COVID-19 guidelines from Italy. Available from: https://www.eurotimes.org/guidelines-for-italian-ophthalmologists-on-covid-19/.
25. Romano MR, Montericcio A, Montalbano C, et al. Facing COVID-19 in ophthalmology department. Curr Eye Res. 2020;45(6):653–658. doi:10.1080/02713683.2020.1752737
26. Jammal HM, Alqudah NM, Khader Y. Awareness, perceptions, and attitude regarding coronavirus disease 2019 (COVID-19) among ophthalmologists in Jordan: cross-sectional online survey. Clin Ophthalmol. 2020;14:2195–2202. doi:10.2147/OPTH.S260460
27. Safadi K, Kruger JM, Chowers I, et al. Ophthalmology practice during the COVID-19 pandemic. BMJ Open Ophthalmol. 2020;5(1):e000487. doi:10.1136/bmjophth-2020-000487
28. Lacorzana J, Ortiz-Perez S, Rubio Prats M. Incidence of COVID-19 among ophthalmology professionals. Med Clin. 2020;155(5). doi:10.1016/j.medcle.2020.05.014
29. Qiao C, Zhang H, He M, et al. Symptomatic COVID-19 in eye professionals in Wuhan, China. Ophthalmology. 2020;127(9):1268–1270. doi:10.1016/j.ophtha.2020.04.026
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.