")
Back to Journals » Infection and Drug Resistance » Volume 13
Prevention Strategies to Minimize the Infection Risk Associated with Biologic and Targeted Immunomodulators
Authors Kordzadeh-Kermani E, Khalili H , Karimzadeh I , Salehi M
Received 1 October 2019
Accepted for publication 29 January 2020
Published 18 February 2020 Volume 2020:13 Pages 513—532
DOI https://doi.org/10.2147/IDR.S233137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Elaheh Kordzadeh-Kermani,1 Hossein Khalili,1 Iman Karimzadeh,2 Mohammadreza Salehi3
1Department of Clinical Pharmacy, School of Pharmacy, Tehran University of Medical Sciences, Tehran, Iran; 2Department of Clinical Pharmacy, School of Pharmacy, Shiraz University of Medical Sciences, Shiraz, Iran; 3Department of Infectious Diseases, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Hossein Khalili
Department of Clinical Pharmacy, School of Pharmacy, Tehran University of Medical Sciences, P.o. Box 14155/6451, Tehran, Iran
Tel/Fax +98 216 695 4709
Email [email protected]
Abstract: The introduction of biologic and targeted immunomodulators is a significant breakthrough in the therapeutic area of various fields of medicine. The occurrence of serious infections, a complication of secondary immunosuppression associated with these agents, leads to increased morbidity and mortality. Implementing preventive strategies could minimize infection-related complications and improve therapeutic outcomes. The purpose of this review is to focus on current evident approaches regarding screening, monitoring, preventing (immunization and chemoprophylaxis), and management of infections in patients who are candidates for about 70 biologic and targeted immunomodulators. Recommendations are based on relevant guidelines, especially the ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document series published in 2018.
Keywords: biologic immunomodulators, targeted immunomodulators, immunization, chemoprophylaxis
Introduction
Biologic immunomodulators are biosimilar medications synthesized by living organisms structurally related to antibodies, interleukins, and receptors that specifically target oncogenic cells or immune system pathways.1 Targeted immunomodulators such as BCR-ABL tyrosine kinase inhibitors, phosphatidylinositol-3-kinase inhibitor, bruton tyrosine kinase inhibitors, and mammalian target of rapamycin (mTOR) inhibitors are small molecules which affect intracellular signaling cascades that eventually modulate protein expression.2
The availability of biologic and targeted immunomodulators has revolutionized pharmacotherapy of diseases in diverse aspects of medicine, including onco-hematology, rheumatology, nephrology, transplantation, neurology, pulmonology, and dermatology. Despite their therapeutic benefit, concerns regarding the potential risk of infections have been a challenge for using these agents in clinical practice.3 Severe infection is a significant cause of morbidity and mortality in patients treated with immunosuppressants. Most patients on immunomodulator drugs require long term therapies; however, a significant number of these patients do not receive appropriate preventive care regarding infections.4
Biologic and targeted immunomodulators are categorized into several pharmacologic classes. Unlike traditional immunosuppressants, immune suppression associated with these agents is specific to certain signals in the immune system, occasionally causing profound immune suppression mimicking primary immunodeficiency disorders.5–7 Depending on their mechanism of action and impact on the immune system, the infection risk associated with these therapies varies among pharmacologic classes; some affect intracellular signaling pathways, some bind to receptors of cellular immunity while some others inhibit the actions of cytokines (Table 1).
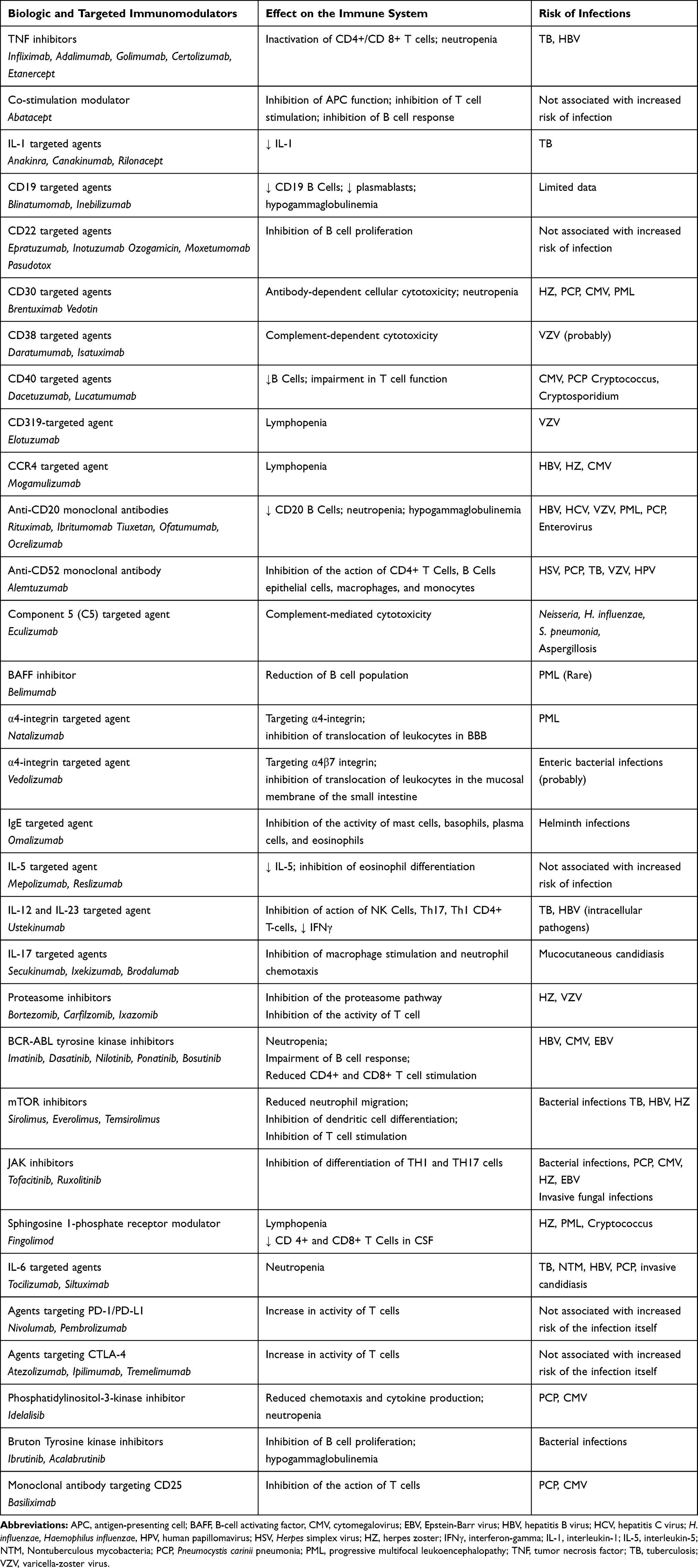 |
Table 1 Biologic and Targeted Immunomodulators Classification and Their Impacts on the Immune System |
The European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Infections in Compromised Hosts Consensus have reviewed articles and made recommendations to instruct clinicians on the strategies to prevent and manage infections associated with biologic and targeted immunomodulators.8–13 In this review, we aim to focus on evidence-based strategies according to the latest guidelines to provide practitioners guidance regarding screening, chemoprophylaxis, vaccination, and management of infections in patients on biologic and targeted immunomodulators.
Methods
We conducted a literature search in databases including Scopus, Medline, Embase, Cochrane Database Systematic Reviews and Google Scholar from January 2007 to August 2019 using the search terms related to each of the agents along with “infection”, “vaccination”, “screening”, “prophylaxis”, “monitoring”, “immunization”, “immune response”, “treatment”, and “management”. Polyclonal antibodies (e.g., anti-thymocyte globulin, rozrolimupab), and monoclonal antibodies that lack prominent immunosuppressive effects (e.g., trastuzumab) were beyond the scope of our review and are not considered here. We included articles and guidelines from the latest updates of ESCMID, The Infectious Diseases Society of America (IDSA), The European League Against Rheumatism (EULAR), National Comprehensive Cancer Network (NCCN), American College of Rheumatology (ACR), American College of Gastroenterology (ACG), The American Association for the Study of Liver Diseases (AASLD), The Canadian Dermatology Association (CDA), European Conference on Infections in Leukaemia (ECIL), The Advisory Committee on Immunization Practices (ACIP), The American Society of Transplantation (AST), European Conference on Infections in Leukaemia (ECIL), The German Society of Hematology and Medical Oncology and the International Consensus Guidelines on the Management of Cytomegalovirus.8–29 We also included recommendations from Uptodate online, the relevant review articles, expert opinions, and European Medicines Agency (EMA) drug labels, especially on subjects that the guidelines do not offer an opinion. The recommendations regarding screening for infections, immunization, prevention, and monitoring of infections in patients candidates for biologic and targeted immunomodulators were finally categorized by the class of immunosuppressive agents.
Results
Of the relevant articles we found, data were obtained from 31 guidelines as well as consensus recommendations and 17 review papers. Comprehensive recommendations were not found on subjects such as prophylactic measures for prevention of pneumocystis pneumonia in biologic therapy of rheumatologic diseases, screening of infections for patients undergoing basiliximab induction, preventive measures to prevent infections associated with abatacept, immunization in patients undergoing treatment with new generations of anti-CD20 monoclonal antibodies and late onset neutropenia associated with anti-CD20 monoclonal antibodies. Such data were obtained from expert opinions, review articles, the EMA drug labels and clinical trials. The recommendations regarding screening, prophylaxis, monitoring, and immunization of infections associated with biologic and targeted immunomodulators are summarized in Tables 2–5.
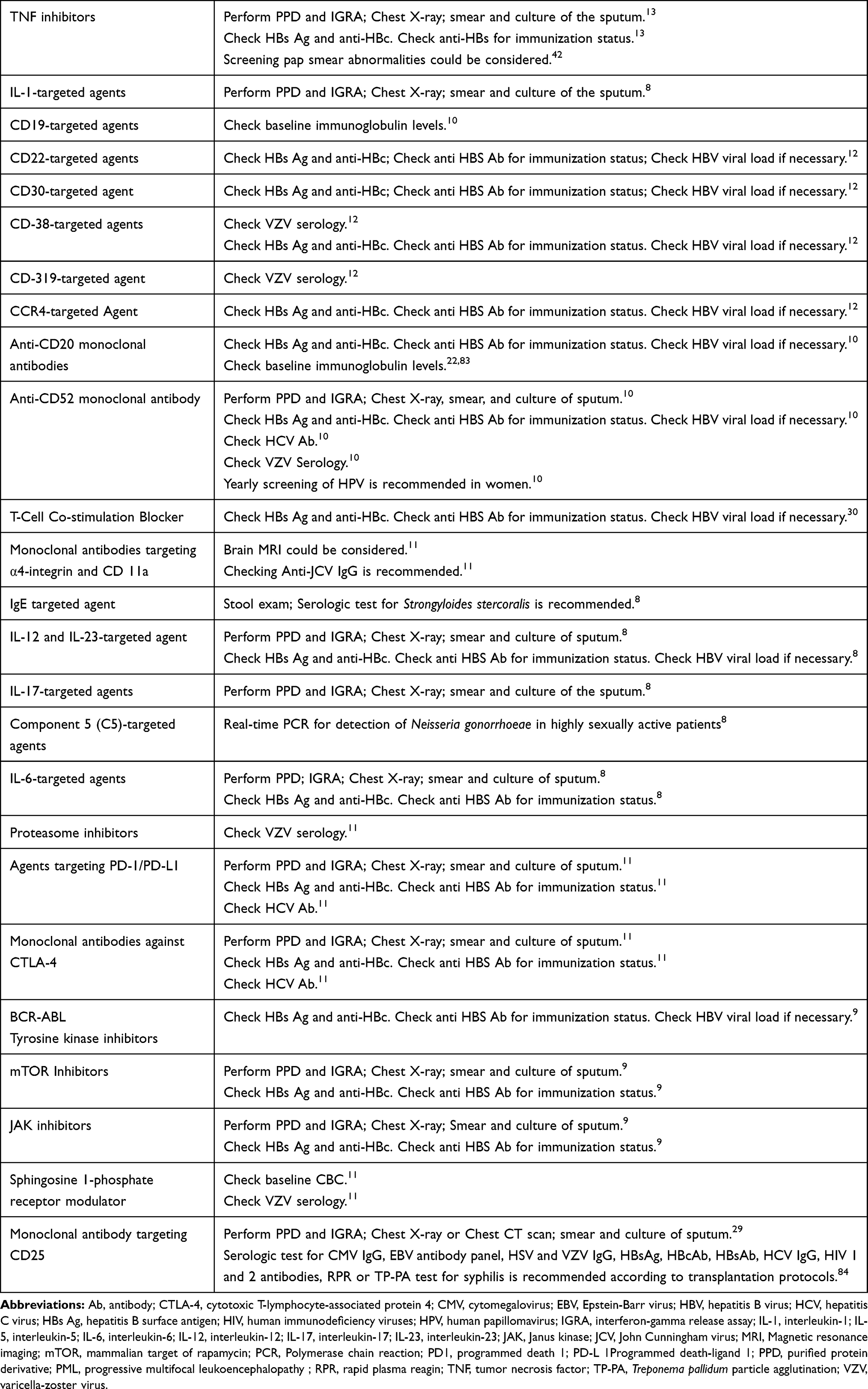 |
Table 2 Evidence and Recommendations on Screening of Infections in Patients Candidates for Biologic and Targeted Immunomodulatory Therapies |
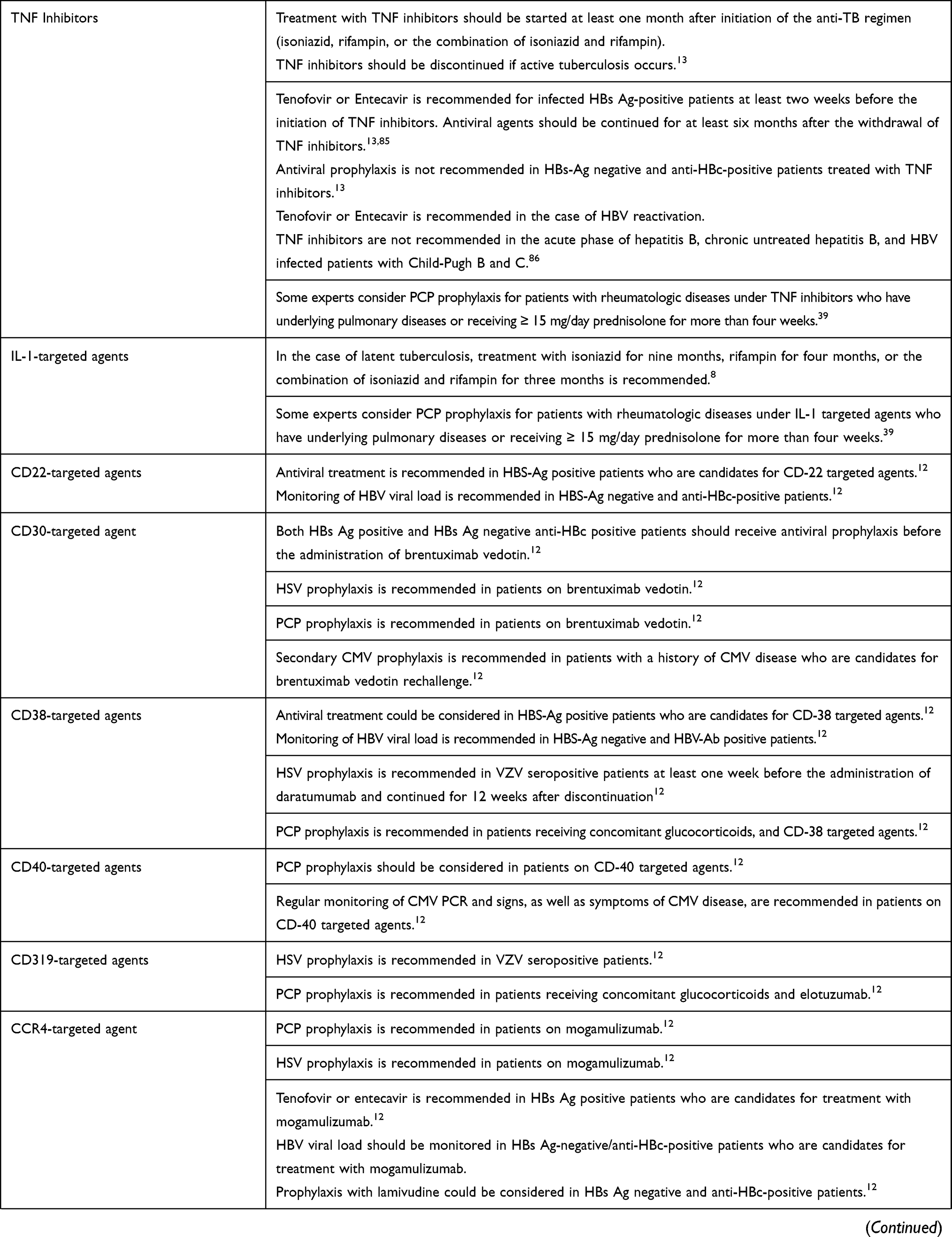 | 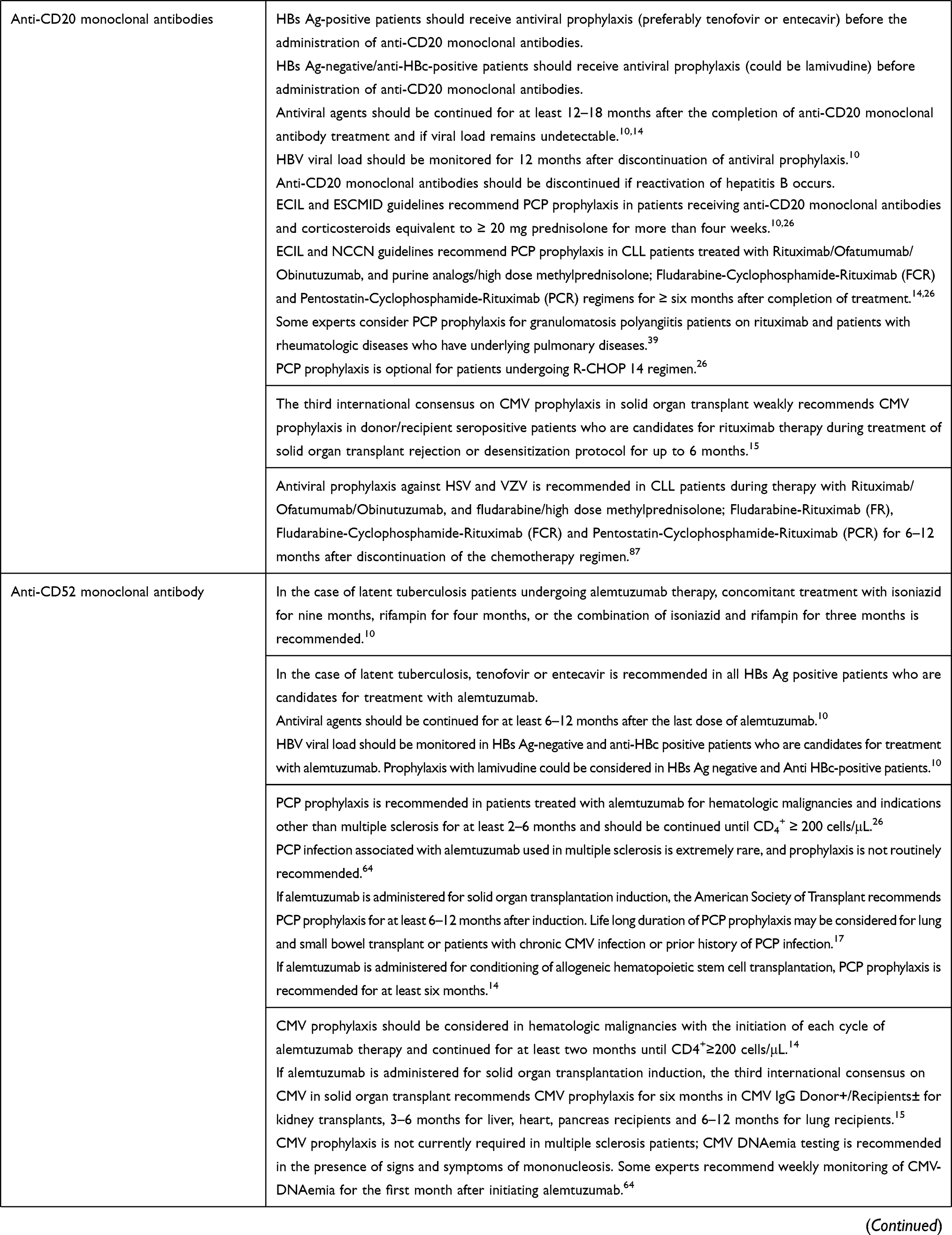 | 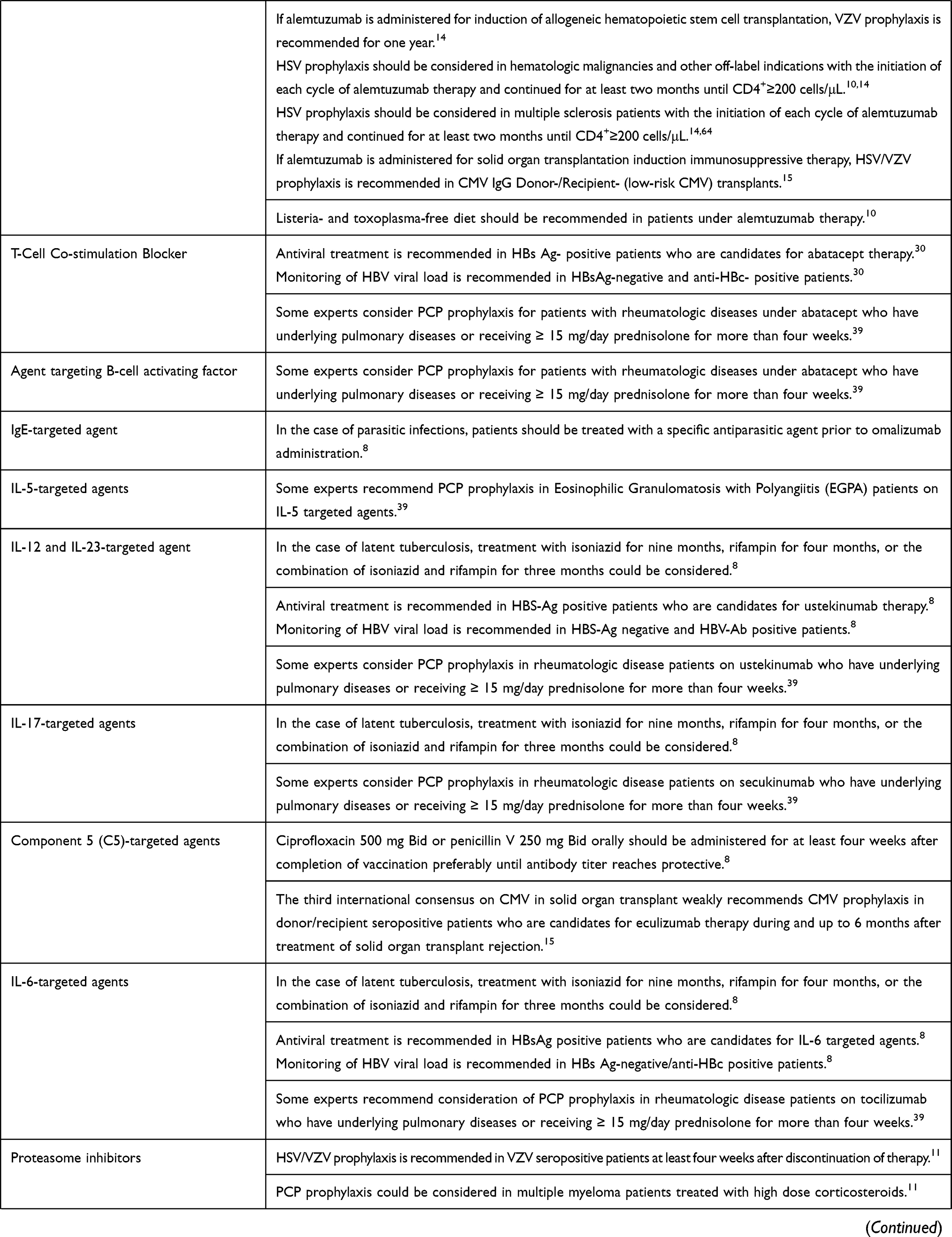 | 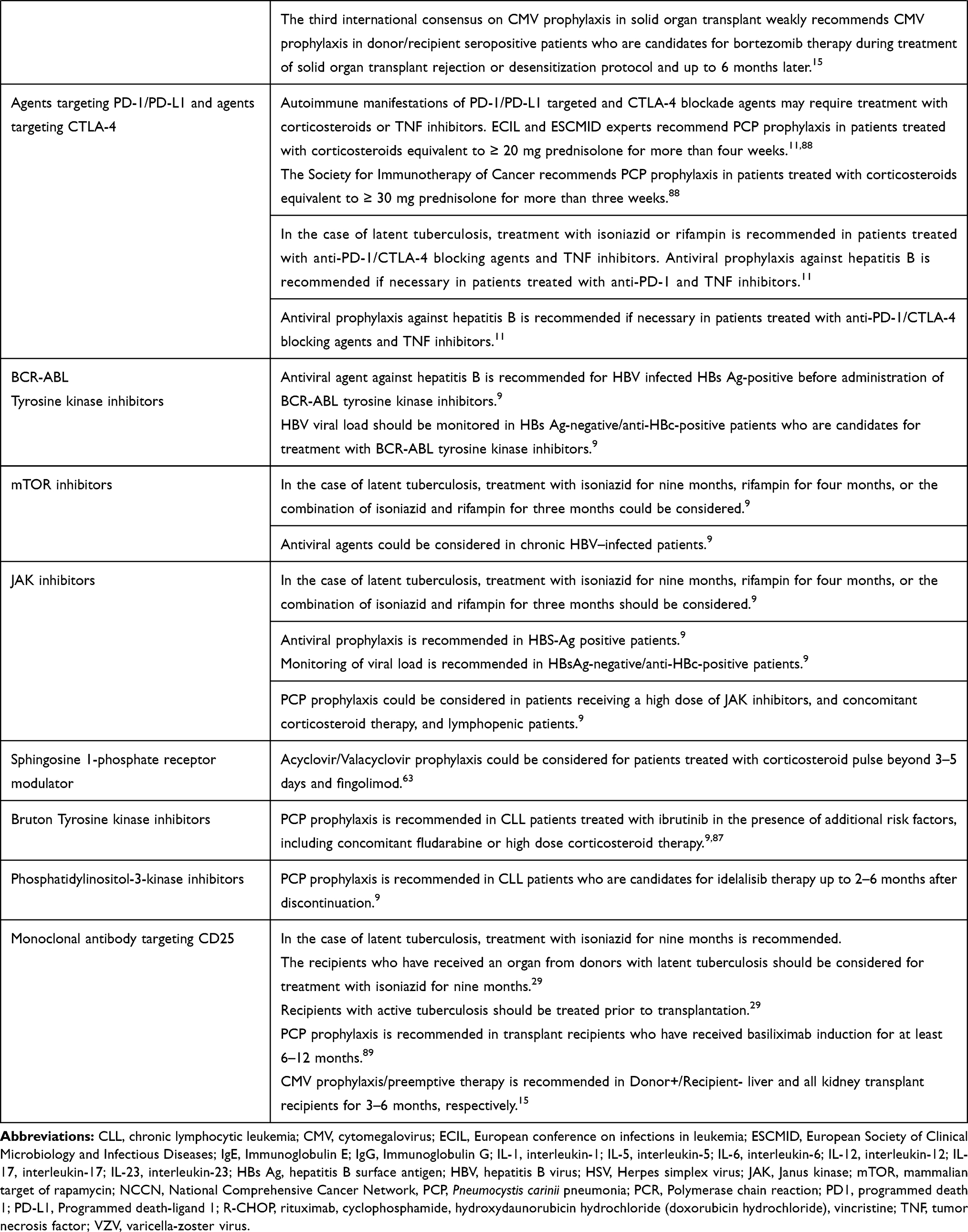 |
Table 3 Evidence and Recommendations on the Prevention and Management of Infections in Patients Candidates for Biologic and Targeted Immunomodulatory Therapies |
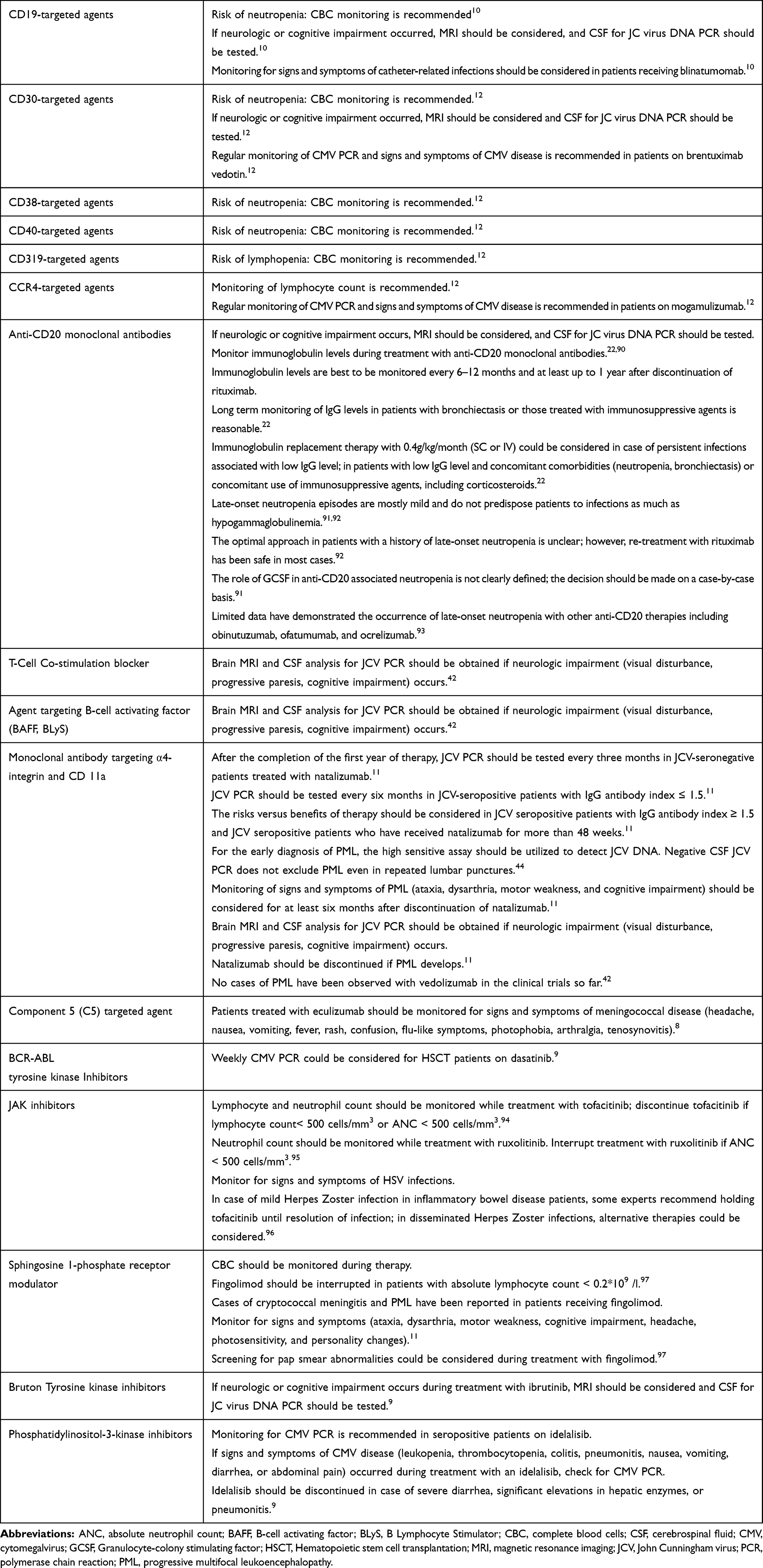 |
Table 4 Evidence and Recommendations on Monitoring of Patients on Biologic and Targeted Immunomodulatory Therapies |
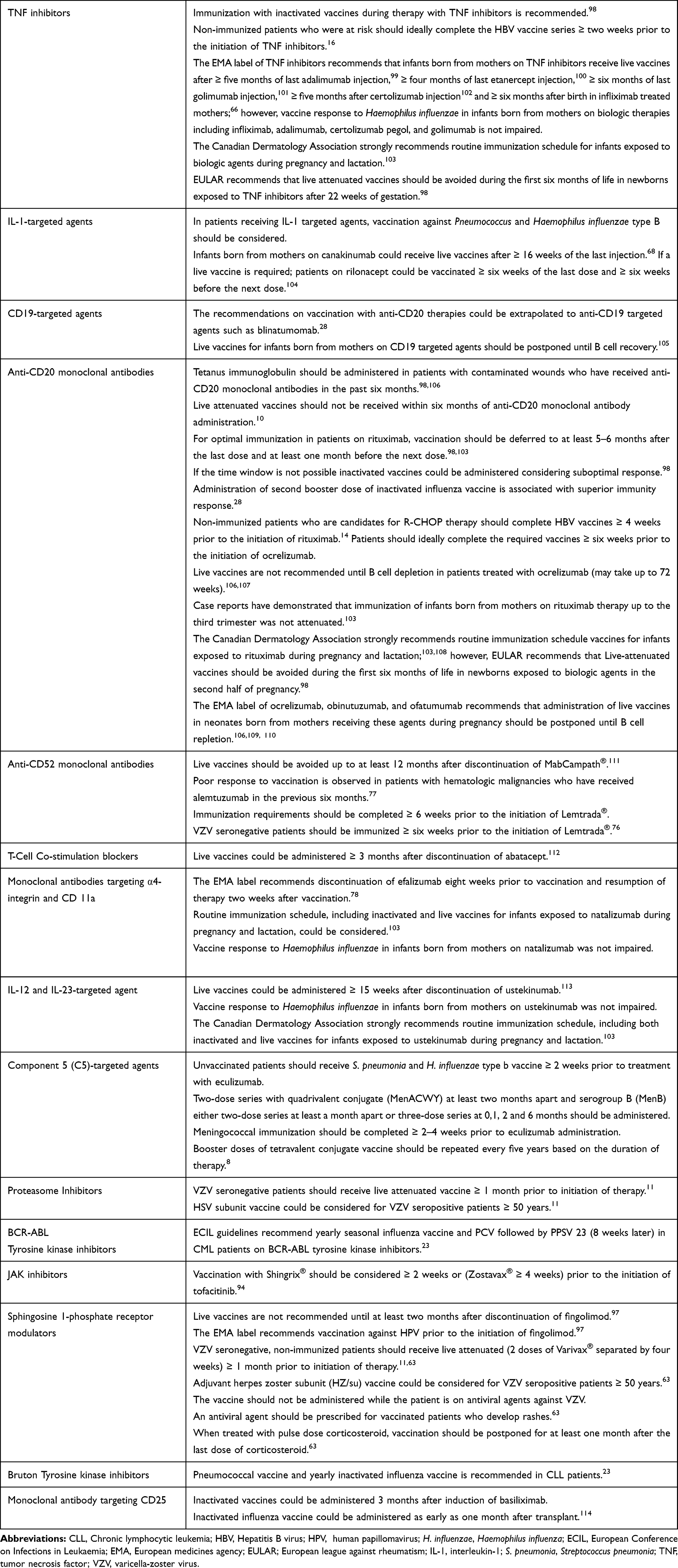 |
Table 5 Evidence and Recommendations on Immunization of Patients on Biologic and Targeted Immunomodulatory Therapies |
Discussion
The growing number of approved biologic and targeted immunomodulators on the market and their various approved and off-label indications explain the necessity to guide health care professionals in the prevention and management of infections and define the relative risk of particular infections associated with these agents. This study reviewed and summarized prevention strategies, including screening, monitoring, immunization, prophylaxis, and management of infections associated with about 70 biologic and targeted therapies based on relevant guidelines, especially ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus document series published in 2018.8–13
The Risk of Hepatitis B Virus (HBV) Reactivation
Extensive studies have shown that the risk of HBV reactivation is highest with anti-CD20 targeted agents including rituximab, ofatumumab, obinutuzumab,27,30 and probably ocrelizumab.31 These agents are associated with a significant risk of HBV reactivation in both HBs Ag-positive and HBs Ag-negative/anti-HBc-positive patients. Studies have shown that tenofovir and entecavir are significantly more effective than lamivudine in preventing HBV reactivation in patients on anti-CD20 monoclonal antibodies.32,33 Therefore, ESCMID recommends either tenofovir or entecavir-based regimens for antiviral therapy in both active and occult hepatitis B patients who are candidates for anti-CD20 targeted agents.10
HBs Ag-positive patients are at high risk of HBV reactivation with alemtuzumab. Also, HBs Ag-negative/anti-HBc-positive patients are moderate to high risk for reactivation of hepatitis B; Therefore, ESCMID recommends that all patients with active hepatitis B should receive antiviral prophylaxis. Individuals with occult infection could either receive prophylaxis or be monitored for reactivation of HBV based on the indication of alemtuzumab and concomitant use of corticosteroids in certain clinical conditions (e.g., transplantation, multiple sclerosis)10,30
Anti-TNF monoclonal antibodies are considered as moderate to high risk for reactivation of hepatitis B in active infection and moderate risk for occult infection. The risk of HBV reactivation in HBsAg-positive patients is moderate with etanercept, and HBsAg-negative/anti-HBc-positive patients are probably at low risk for seroconversion with etanercept. Accordingly, ESCMID recommends antiviral prophylaxis with either tenofovir or entecavir only for HBsAg-positive patients under TNF inhibitors.13
Tocilizumab, abatacept, ustekinumab, mogamulizumab, and BCR-ABL tyrosine kinase inhibitors are associated with a moderate risk of HBV reactivation.30 Data on the risk of HBV reactivation with tofacitinib is limited; In a study, reactivation of hepatitis B occurred in 2 of 4 HBs Ag positive patients.34 Reactivation of HBV did not occur in any of the HBs Ag-negative/anti-HBc-positive patients. Few case reports have demonstrated fatal HBV reactivation in HBs Ag-positive patients receiving 5–10 mg/day everolimus for renal cell carcinoma and breast cancer.35,36 Therefore, ESCMID recommends antiviral prophylaxis only in HBs Ag-positive patients treated with mTOR inhibitors, janus kinase (JAK) inhibitors, BCR-ABL tyrosine kinase inhibitors, IL-6 targeted immunomodulators, ustekinumab, and mogamulizumab. Pre-emptive antiviral prophylaxis is reasonable in occult HBV infections during treatment with these agents.8–13
The Risk of Pneumocystis Carinii Pneumonia (PCP)
The greatest risk of PCP infection is attributed to alemtuzumab, and universal prophylaxis is required in solid organ transplant recipients and patients with hematologic diseases who have received this agent. Limited data suggest the risk of PCP with bortezomib in multiple myeloma patients treated with high dose corticosteroids; however, the overall risk is low.37,38 The incidence of PCP with TNF inhibitors, tocilizumab, and rituximab is also low; however, several studies have demonstrated that the risk of infection is increased in particular conditions including age >65 years, concurrent long-term corticosteroid use (e.g., ≥ 15 mg/day prednisolone for more than four weeks), and co-existence of either pulmonary diseases or underlying granulomatosis with polyangiitis.38,39 Comparative studies have shown a greater risk with TNF inhibitors, particularly infliximab than tocilizumab.40 Eighteen cases of ibrutinib associated PCP have been published; in most of them, the patients were neutropenic.41 Currently, trimethoprim/sulfamethoxazole is the drug of choice for the primary prophylaxis of PCP in different clinical conditions such as hematological malignancies and stem cell transplantation. Second-line choices for PCP prophylaxis in the case of trimethoprim/sulfamethoxazole intolerance include pentamidine inhalation, oral dapsone, and oral atovaquone.26 These recommendations regarding PCP prophylaxis can be extrapolated to the setting of biologic and targeted immunomodulators.
The Risk of Progressive Multifocal Leukoencephalopathy (PML)
The incidence of PML appears to be greatest with monoclonal antibodies targeting α4-integrin. PML associated with efalizumab and natalizumab has been reported 1 in 300 patients and 1 in 1000 patients, respectively.42,43 In contrast, to date, no case of PML has been reported with vedolizumab.44 Fifteen case reports of PML have been reported in patients treated with fingolimod. Treatment duration, age, and JC virus (JCV) antibody titer could be associated with the occurrence of fingolimod-induced PML.45,46 Cases of PML have been reported with anti-CD20 monoclonal antibodies (15 cases with rituximab and 5 cases with ocrelizumab); however, most of these cases could be attributed to previous natalizumab or fingolimod therapy. Therefore, it is reasonable to monitor MRI for signs and symptoms of PML (e.g., visual disturbance, progressive paresis, cognitive impairment) when switching from either natalizumab or fingolimod to anti-CD20 therapies.47 Currently, there is no standard and specific therapy for PML. The offending agent should be discontinued permanently. Plasma exchange (e.g., 3–5 exchanges over 5 to 8 days) has been used for the reversal of natalizumab-associated PML. However, this modality often leads to immune reconstitution inflammatory syndrome (IRIS) phenomenon, which is a neurological deterioration associated with brain swelling and risk of herniation.48
The Risk of Latent Tuberculosis
Rheumatoid arthritis itself is associated with increased risk of tuberculosis reactivation up to 3.17 times. In patients with rheumatoid arthritis treated with TNF inhibitors, the risk is increased up to 17 fold than the general population.49 When compared with etanercept, other anti-TNF monoclonal antibodies are associated with a statistically significant higher risk of tuberculosis reactivation. Ai et al. demonstrated that the risk of tuberculosis reactivation with adalimumab and infliximab is 3.88 and 2.78 times more than etanercept, respectively. The effect of anti-TNF monoclonal antibodies on inducing T-cell apoptosis, complement-dependent cytotoxicity, and pharmacokinetic properties could explain the higher potential of adalimumab and infliximab over etanercept in reactivating latent tuberculosis.19,50 Statistical difference between infliximab and adalimumab has not been found; however, the risk of latent tuberculosis reactivation with infliximab was 1.28 times more than adalimumab.49 Another meta-analysis showed that the incidence rate of tuberculosis was highest with infliximab and certolizumab, followed by adalimumab, golimumab, tofacitinib, tocilizumab, etanercept, abatacept, and rituximab (44/9277; 13/4396; 30/12757; 4/3209; 11/6507; 9/12905; 3/7164; 2/7743; and 2/11962, respectively).51 The incidence of tuberculosis reactivation was similar in adalimumab- and golimumab-treated patients.51 It is noteworthy that the results could be affected by several confounding factors such as including patients from tuberculosis endemic areas in most of the certolizumab trials. The incidence rate of tuberculosis was 5–10 times more than the general population in North America and Western Europe (an incidence rate of 5–20 times were reported for anti-TNF therapies in these areas). A cohort study demonstrated that the risk of tuberculosis is higher with infliximab- and anakinra-treated groups versus etanercept recipients (adjusted risk ratio: 1.6, 1.3, and 1.2, respectively).52 Results of clinical trials have reported 10 cases of tuberculosis in 2588 ruxolitinib-treated patients.53 Limited reports of tuberculosis following ustekinumab therapy exist; however, no case of latent tuberculosis reactivation has been reported with secukinumab so far.54
The incidence of tuberculosis in kidney transplant recipients and multiple sclerosis patients treated with alemtuzumab was found to be 0.67% and 0.3%, respectively;55 however, in a small study conducted in a high endemic area, the incidence of tuberculosis in patients with hematologic malignancies and autoimmune cytopenias was 31–45%.56 Few cases of tuberculosis reactivation have been reported in metastatic renal cell carcinoma patients receiving mTOR inhibitors,57,58 and in one case report in lung transplantation, reactivation of latent tuberculosis has been attributed to mTOR inhibitors.59
In summary, available data indicate that the risk of tuberculosis is greatest with monoclonal antibodies against TNF and alemtuzumab (because of insufficient data and diversities in sample size, we could not compare the risk) followed by JAK inhibitors and IL-1 targeted agents. Limited cases of reactivation of tuberculosis exist on mTOR inhibitors used in chemotherapy. The risk of tuberculosis reactivation with rituximab and tocilizumab was not more than the general population and appeared to be negligible.54 Accordingly, ESCMID recommends anti-TB prophylaxis in patients who are candidates to receive TNF inhibitors, alemtuzumab, JAK inhibitors, and mTOR inhibitors (used in chemotherapy regimens). Isoniazid for nine months, rifampin for four months, or the combination of isoniazid and rifampin for three months could be considered for the treatment of latent tuberculosis in the setting of biologic and targeted immunomodulators.
The Risk of Herpes Simplex Virus (HSV) and Varicella-Zoster Virus (VZV) Infections
Compared to the bortezomib-free regimens, the incidence of herpes zoster infection increased up to two-fold when bortezomib was added to the chemotherapeutic regimen of multiple myeloma patients (11% and 22.3%, respectively).60 Tofacitinib-treated patients experienced HSV infection with an incidence rate of 4.4 per 100 patient-years and up to 7.7 per 100 patient-years in the Asian population versus 1.5 per 100 patient-years in rheumatoid arthritis patients receiving placebo.42,61 The incidence rates of HSV infection in patients with rheumatoid arthritis receiving TNF inhibitors and rituximab were 1.6 (golimumab) to 2.4 (certolizumab) and 2.2 per 100 patient-years, respectively. Incidence rates and hazard ratios were not statistically significant among TNF inhibitors and rituximab; glucocorticoids were associated with increased risk of infection.62
The graph represented by Arvin et al. in 2015 demonstrates comparative incidence of VZV infections associated with disease-modifying therapy of multiple sclerosis; the incidence of VZV infection is greatest with alemtuzumab 12 mg/day (7–45 per 1000 patient-year) followed by fingolimod 0.5 mg/day (6–17.5 per 1000 patient-year), natalizumab (8–16 per 1000 patient-year), and rituximab (8–13 per 1000 patient-year).63
ESCMID recommends HSV/VZV prophylaxis for proteasome inhibitors- and alemtuzumab-treated patients (for all their indications) and also considers HSV prophylaxis in fingolimod-treated patients that concurrently receive corticosteroid pulse therapy. Acyclovir/Valacyclovir could be taken into account as prophylaxis of HSV/VZV in susceptible patients discussed above.11
The Risk of Cytomegalovirus (CMV) Infection
Alemtuzumab is associated with a remarkable risk of CMV infection, particularly in hematologic malignancies and solid organ transplant recipients, and CMV prophylaxis is recommended in these populations. However, the risk of CMV infection in patients with multiple sclerosis treated with alemtuzumab is less than 1 per 100 patient-years.10 Therefore, ESCMID does not recommend CMV prophylaxis for multiple sclerosis patients on alemtuzumab.10,64 Dasatinib has been associated with CMV reactivation, particularly in post-HSCT patients (adjusted hazard ratio, 7.65; 95% confidence interval, 1.84–31.7);9,65 and ESCMID recommends monitoring of CMV infection in these individuals. Besides dasatinib, regular monitoring of CMV PCR and signs as well as symptoms of CMV disease is also recommended for patients receiving mogamulizumab.12 Finally, the third international consensus on CMV in solid organ transplant weakly recommends CMV prophylaxis for donor/recipient seropositive patients who were candidates for either bortezomib or eculizumab therapy as treatment of solid organ transplant rejection or a part of desensitization protocol.15 Antiviral options for CMV prophylaxis include intravenous ganciclovir, oral valganciclovir, and high doses of oral valacyclovir.15
Immunization in Patients on Biologic and Targeted Immunomodulators
According to IDSA guidelines published in 2013, live vaccines, including measles, mumps, and rubella (MMR), live-attenuated influenza vaccine (LAIV), Bacillus Calmette–Guérin (BCG) vaccine, oral polio vaccine (OPV), live-attenuated HSV, and yellow fever should be avoided ≤ 2–4 weeks before initiation and during treatment with immunosuppressants.16 The international guidelines recommend inactivated influenza, pneumococcal, toxoid tetanus, hepatitis A vaccine, hepatitis B, and human papillomavirus vaccines in patients with autoimmune rheumatologic diseases including those under biologic and targeted immunomodulators.18,20,21
The live-attenuated HSV vaccine should be preferably administered ≥ 4 weeks prior to the initiation of immunosuppressive agents for high risk individuals including those older than 50 years. ACIP does not make any recommendations on the administration of recombinant Zoster vaccine (Shingrix®) in highly-immunocompromised patients due to lack of data on efficacy and safety in this population;24,25 however, recombinant zoster vaccine, has demonstrated greater efficacy than live-attenuated HSV vaccine (Zostavax®), decreases the risk of HZ in patients older than 70 years and also appears an interesting alternative to live-attenuated HSV vaccine in immunocompromised patients.
Humoral response to vaccine is generally not impaired in patients on TNF alpha inhibitors (except infliximab),66 anakinra,67 canakinumab,68 abatacept,69 belimumab,70 natalizumab,71 ustekinumab,72 IL-17-targeted agents,73 tocilizumab,74 probably proteasome inhibitors75 and alemtuzumab (in doses approved for multiple sclerosis).76 Meanwhile, immune response to vaccines is significantly decreased in patients receiving rituximab66 and alemtuzumab (used in hematologic malignancies).77 No data exist for immunization in patients under CD19 and CD22 targeted therapies; based on their impact on humoral immunity vaccine response is probably diminished during treatment with these agents. Immune response to vaccine may be attenuated in patients on efalizumab,78 BCR-ABL tyrosine kinase inhibitors,79 tofacitinib80 and ibrutinib.81 Patients treated with vedolizumab have shown reduced response to oral vaccines but not injectable ones.42 Interestingly, mTOR inhibitors have been shown to enhance immune response to certain vaccines.82
Conclusions
Biologic and targeted immunomodulators are associated with increased risk of particular bacterial, fungal, and viral infections based on their impact on the immune system. In order to minimize the potential infection risk, screening, immunization, monitoring, and prophylactic protocols should be implemented. Limited information exists on the risk of infections associated with the recently developed biologic agents including CD19, CD22; CD30; CD38; CD319; CD40; CCR4–targeted agents; second and third generation anti-CD20 monoclonal antibodies, second and third generations of BCR-ABL tyrosine kinase inhibitors; and their impact on patient response to immunization. Consequently, consensus guidelines do not make comprehensive recommendations regarding these agents. Further clinical research will guide us regarding the necessary safety measures to minimize the infection risk of these agents.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morrow TH, Felcone LH. Defining the difference: what makes biologics unique. Biotechnol Healthc. 2004;1(4):24–29.
2. Ferguson FM, Gray NS. Kinase inhibitors: the road ahead. Nat Rev Drug Discov. 2018;17(5):353–377. doi:10.1038/nrd.2018.21
3. Bresnihan B, Cunnane G. Infection complications associated with the use of biologic immunomodulators. Rheum Dis Clin North Am. 2003;29(1):185–202. doi:10.1016/S0889-857X(02)00101-1
4. Meroni PL, Zavaglia D, Girmenia C. Vaccinations in adults with rheumatoid arthritis in an era of new disease-modifying anti-rheumatic drugs. Clin Exp Rheumatol. 2018;36(2):317–328.
5. Henrickson SE, Ruffner MA, Kwan M. Unintended immunological consequences of biologic therapy. Curr Allergy Asthma Rep. 2016;16(6):46. doi:10.1007/s11882-016-0624-7
6. Kaplan B, Bonagura VR. Secondary hypogammaglobulinemia: an increasingly recognized complication of treatment with immunomodulators and after solid organ transplantation. Immunol Allergy Clin North Am. 2019;39(1):31–47. doi:10.1016/j.iac.2018.08.005
7. Eisenberg R. Immune Compromise Associated with Biologics. Stiehm’s Immune Deficiencies Academic Press; 2014:889–906.
8. Winthrop KL, Mariette X, Silva JT, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: an infection diseases perspective (Soluble immune effector molecules [II]: agents targeting interleukins, immunoglobulins and complement factors). Clin Microbiol Infect. 2018;24:S21–S40. doi:10.1016/j.cmi.2018.02.002
9. Reinwald M, Silva JT, Mueller NJ, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: an infection diseases perspective (Intracellular signaling pathways: tyrosine kinase and mTOR inhibitors). Clin Microbiol Infect. 2018;24:S53–70. doi:10.1016/j.cmi.2018.02.009
10. Mikulska M, Lanini S, Gudiol C, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: an infection diseases perspective (Agents targeting lymphoid cells surface antigens [I]: CD19, CD20 and CD52). Clin Microbiol Infect. 2018;24:S71–S82.
11. Redelman-Sidi G, Michielin O, Cervera C, et al. ESCMID study group for infections in compromised hosts (ESGICH) consensus document on the safety of targeted and biological therapies: an infection diseases perspective (Immune checkpoint inhibitors, cell adhesion inhibitors, sphingosine-1-phosphate receptor modulators and proteasome inhibitors). Clin Microbiol Infect. 2018;24:S95–S107. doi:10.1016/j.cmi.2018.01.030
12. Drgona L, Gudiol C, Lanini S, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: an infection diseases perspective (Agents targeting lymphoid or myeloid cells surface antigens [II]: CD22, CD30, CD33, CD38, CD40, SLAMF-7 and CCR4). Clin Microbiol Infect. 2018;24:S83–S94. doi:10.1016/j.cmi.2018.03.022
13. Baddley JW, Cantini F, Goletti D, et al. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: an infectious diseases perspective (Soluble immune effector molecules [I]: anti-tumor necrosis factor-α agents). Clin Microbiol Infect. 2018;24:S10–S20. doi:10.1016/j.cmi.2017.12.025
14. Baden LR, Swaminathan S, Angarone M, et al. Prevention and treatment of cancer-related infections, Version 2.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2016;14(7):882–913. doi:10.6004/jnccn.2016.0093
15. Kotton CN, Kumar D, Caliendo AM, et al. The third international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. 2018;102(6):900–931. doi:10.1097/TP.0000000000002191
16. Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2013;58(3):e44–e100.
17. Martin SI, Fishman JA, AST Infection Diseases Community of Practice. Pneumocystis pneumonia in solid organ transplantation. Am J Transplant. 2013;13(s4):272–279. doi:10.1111/ajt.2013.13.issue-s4
18. Van Assen S, Elkayam O, Agmon-Levin N, et al. Vaccination in adult patients with auto-immune inflammatory rheumatic diseases: a systematic literature review for the European League Against Rheumatism evidence-based recommendations for vaccination in adult patients with auto-immune inflammatory rheumatic diseases. Autoimmun Rev. 2011;10(6):341–352. doi:10.1016/j.autrev.2010.12.003
19. Salinas GF, De Rycke L, Barendregt B, et al. Anti-TNF treatment blocks the induction of T cell-dependent humoral responses. Ann Rheum Dis. 2013;72(6):1037–1043. doi:10.1136/annrheumdis-2011-201270
20. Farraye FA, Melmed GY, Lichtenstein GR, et al. ACG clinical guideline: preventive care in inflammatory bowel disease. Am J Gastroenterol. 2017;112(2):241. doi:10.1038/ajg.2016.537
21. Singh JA, Saag KG, Bridges SL, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. doi:10.1002/art.39480
22. Wijetilleka S, Jayne DR, Mukhtyar C, et al. Recommendations for the management of secondary hypogammaglobulinaemia due to B cell targeted immunomodulators in autoimmune rheumatic diseases. Rheumatology. 2018;58(5):889–896. doi:10.1093/rheumatology/key394
23. Mikulska M, Cesaro S, de Lavallade H, et al. Vaccination of patients with haematological malignancies who did not have transplantations: guidelines from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis. 2019;19(6). doi:10.1016/S1473-3099(18)30601-7
24. Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2008;57(5):1–30.
25. Kroger AT, Duchin J, Vázquez M. General best practice guidelines for immunization. best practices guidance of the advisory committee on immunization practices (ACIP). Available from: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/index.html.
26. Maertens J, Cesaro S, Maschmeyer G, et al. ECIL guidelines for preventing Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J Antimicrob Chemother. 2016;71(9):2397–2404. doi:10.1093/jac/dkw157
27. Reddy KR, Beavers KL, Hammond SP, et al. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148(1):215–219. doi:10.1053/j.gastro.2014.10.039
28. Rieger CT, Liss B, Mellinghoff S, et al. Anti-infective vaccination strategies in patients with hematologic malignancies or solid tumors. Guideline of the Infectious Diseases Working Party (AGIHO) of the German Society for Hematology and Medical Oncology (DGHO). Ann Oncol. 2018;29(6):1354–1365. doi:10.1093/annonc/mdy117
29. Subramanian AK, Theodoropoulos NM. Mycobacterium tuberculosis infections in solid organ transplantation: Guidelines from the infectious diseases community of practice of the American Society of Transplantation . Clin Transplant. 2019 Sep;33(9):e13513. doi:10.1111/ctr.13513
30. Loomba R, Liang TJ. Hepatitis B reactivation associated with immune suppressive and biological modifier therapies: current concepts, management strategies, and future directions. Gastroenterology. 2017;152(6):1297–1309. doi:10.1053/j.gastro.2017.02.009
31. Ciardi MR, Iannetta M, Zingaropoli MA, et al. Reactivation of hepatitis B virus with immune-escape mutations after ocrelizumab treatment for multiple sclerosis. Open Forum Infect Dis. 2018;6(1):ofy356.
32. Li HR, Huang JJ, Guo HQ, et al. Comparison of entecavir and lamivudine in preventing hepatitis B reactivation in lymphoma patients during chemotherapy. J Viral Hepat. 2011;18(12):877–883. doi:10.1111/j.1365-2893.2010.01386.x
33. Picardi M, Della Pepa R, Giordano C, et al. Tenofovir vs lamivudine for the prevention of hepatitis B virus reactivation in advanced-stage DLBCL. Blood. 2019;133(5):498. doi:10.1182/blood-2018-10-878892
34. Chen YM, Huang WN, Wu YD, et al. Reactivation of hepatitis B virus infection in patients with rheumatoid arthritis receiving tofacitinib: a real-world study. Ann Rheum Dis. 2018;77(5):780–782. doi:10.1136/annrheumdis-2017-211322
35. Göksu SS, Bilal Ş, Coşkun HŞ. Hepatitis B reactivation related to everolimus. World J Hepatol. 2013;5(1):43. doi:10.4254/wjh.v5.i1.43
36. Mizuno S, Yamagishi Y, Ebinuma H, et al. Progressive liver failure induced by everolimus for renal cell carcinoma in a 58-year-old male hepatitis B virus carrier. Clin J Gastroenterol. 2013;6(2):188–192. doi:10.1007/s12328-013-0371-4
37. Swan CD, Reid AB. Three cases of presumed pneumocystis pneumonia in patients receiving bortezomib therapy for multiple myeloma. IDCases. 2014;1(3):32–35. doi:10.1016/j.idcr.2014.04.002
38. Wondergem MJ, Grünberg K, Wittgen BP, et al. Interstitial pneumonitis caused by Pneumocystis jirovecii pneumonia (PCP) during bortezomib treatment. Histopathology. 2009;54(5):631–633. doi:10.1111/j.1365-2559.2009.03263.x
39. Tabanor JA, Lakshminarayanan S. Do patients on biologic drugs for rheumatic disease need PCP prophylaxis? Cleve Clin J Med. 2019;86(7):449–453. doi:10.3949/ccjm.86a.18084
40. Mori S, Yoshitama T, Hidaka T, et al. Comparative risk of hospitalized infection between biological agents in rheumatoid arthritis patients: a multicenter retrospective cohort study in Japan. PLoS One. 2017;12(6):e0179179. doi:10.1371/journal.pone.0179179
41. Lee R, Nayernama A, Jones SC, et al. Ibrutinib‐associated Pneumocystis jirovecii pneumonia. Am J Hematol. 2017;92(11):E646–E648. doi:10.1002/ajh.24890
42. Noreña I, Fernández-Ruiz M, Aguado JM. Viral infections in the biologic therapy era. Expert. Rev Anti Infect Ther. 2018;16(10):781–791. doi:10.1080/14787210.2018.1521270
43. Carson KR, Focosi D, Major EO, et al. Monoclonal antibody-associated progressive multifocal leucoencephalopathy in patients treated with rituximab, natalizumab, and efalizumab: a Review from the Research on Adverse Drug Events and Reports (RADAR) Project. Lancet Oncol. 2009;10(8):816–824. doi:10.1016/S1470-2045(09)70161-5
44. Blankenbach K, Schwab N, Hofner B, et al. Natalizumab-associated progressive multifocal leukoencephalopathy in Germany. Neurology. 2019;92(19):e2232–e2233. doi:10.1212/WNL.0000000000007451
45. Siegler JE, Galetta S. Editors’ note: progressive multifocal leukoencephalopathy after fingolimod treatment. Neurology. 2019;92(3):150. doi:10.1212/WNL.0000000000006772
46. Lalive PH, Roth S, Du Pasquier R. Reader response: progressive multifocal leukoencephalopathy after fingolimod treatment. Neurology. 2019;92(3):151. doi:10.1212/WNL.0000000000006773
47. Bigaut K, De Seze J, Collongues N. Ocrelizumab for the treatment of multiple sclerosis. Expert Rev Neurother. 2019;19(2):97–108. doi:10.1080/14737175.2019.1561284
48. Williamson EM, Berger JR. Diagnosis and treatment of progressive multifocal leukoencephalopathy associated with multiple sclerosis therapies. Neurotherapeutics. 2017;14(4):961–973. doi:10.1007/s13311-017-0570-7
49. Ai JW, Zhang S, Ruan QL, et al. The risk of tuberculosis in patients with rheumatoid arthritis treated with tumor necrosis factor-α antagonist: a meta analysis of both randomized controlled trials and registry/cohort studies. J Rheumatol. 2015;42(12):2229–2237. doi:10.3899/jrheum.150057
50. Bongartz T, Sutton AJ, Sweeting MJ, et al. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295(19):2275–2285. doi:10.1001/jama.295.19.2275
51. Souto A, Maneiro JR, Salgado E, et al. Risk of tuberculosis in patients with chronic immune-mediated inflammatory diseases treated with biologics and tofacitinib: a systematic review and meta-analysis of randomized controlled trials and long-term extension studies. Rheumatology. 2014;53(10):1872–1885. doi:10.1093/rheumatology/keu172
52. Brassard P, Kezouh A, Suissa S. Antirheumatic drugs and the risk of tuberculosis. Clin Infect Dis. 2006;43(6):717–722.
53. Lussana F, Cattaneo M, Rambaldi A, et al. Ruxolitinib‐associated infections: a systematic review and meta‐analysis. Am J Hematol. 2018;93(3):339–347. doi:10.1002/ajh.24976
54. Cantini F, Nannini C, Niccoli L, et al. Risk of tuberculosis reactivation in patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis receiving non-anti-TNF-targeted biologics. Mediators Inflamm. 2017;2017:8909834. doi:10.1155/2017/8909834
55. Helfrich M, Ison MG. Opportunistic infections complicating solid organ transplantation with alemtuzumab induction. Transpl Infect Dis. 2015;17(5):627–636. doi:10.1111/tid.2015.17.issue-5
56. Au WY, Leung AY, Eric WC, et al. High incidence of tuberculosis after alemtuzumab treatment in Hong Kong Chinese patients. Leuk Res. 2008;32(4):547–551. doi:10.1016/j.leukres.2007.06.010
57. Jeon SY, Yhim HY, Lee NR, et al. Everolimus-induced activation of latent Mycobacterium tuberculosis infection in a patient with metastatic renal cell carcinoma. Korean J Intern Med. 2017;32(2):365–368. doi:10.3904/kjim.2015.121
58. Coriat R, Mir O, Ropert S, et al. Reactivation of tuberculosis during temsirolimus therapy. Invest New Drugs. 2011;29(6):1494–1496. doi:10.1007/s10637-010-9487-2
59. Guirao-Arrabal E, Santos F, Redel‐Montero J, et al. Risk of tuberculosis after lung transplantation: the value of pretransplant chest computed tomography and the impact of m TOR inhibitors and azathioprine use. Transpl Infect Dis. 2016;18(4):512–519. doi:10.1111/tid.12555
60. Nucci M, Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009;49(8):1211–1225. doi:10.1086/599191
61. Winthrop KL, Yamanaka H, Valdez H, et al. Herpes zoster and tofacitinib therapy in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014;66(10):2675–2684. doi:10.1002/art.v66.10
62. Yun H, Xie F, Delzell E, et al. Risks of herpes zoster in patients with rheumatoid arthritis according to biologic disease-modifying therapy. Arthritis Care Res (Hoboken). 2015;67(5):731–736. doi:10.1002/acr.22470
63. Arvin AM, Wolinsky JS, Kappos L, et al. Varicella-zoster virus infections in patients treated with fingolimod: risk assessment and consensus recommendations for management. JAMA Neurol. 2015;72(1):31–39. doi:10.1001/jamaneurol.2014.3065
64. Buonomo AR, Zappulo E, Viceconte G, et al. Risk of opportunistic infections in patients treated with alemtuzumab for multiple sclerosis. Expert Opin Drug Saf. 2018;17(7):709–717. doi:10.1080/14740338.2018.1483330
65. Prestes DP, Arbona E, Nevett-Fernandez A, et al. Dasatinib use and risk of cytomegalovirus reactivation after allogeneic hematopoietic-cell transplantation. Clin Infect Dis. 2017;65(3):510–513. doi:10.1093/cid/cix325
66. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: remicade. European Medicines Agency EMA/CHMP/47828/2019. Available from: https://www.ema.europa.eu/en/documents/product-information/remicade-epar-product-information_en.pdf.
67. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: kineret. Available from: https://www.ema.europa.eu/en/documents/product-information/kineret-epar-product-information_en.pdf.
68. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: ilaris EMEA/H/C/001109. Available from: https://www.ema.europa.eu/en/documents/product-information/ilaris-epar-product-information_en.pdf.
69. Alten R, Bingham CO, Cohen SB, et al. Antibody response to pneumococcal and influenza vaccination in patients with rheumatoid arthritis receiving abatacept. BMC Musculoskelet Disord. 2016;17(1):231. doi:10.1186/s12891-016-1082-z
70. Chatham W, Chadha A, Fettiplace J, et al. A randomized, open-label study to investigate the effect of belimumab on pneumococcal vaccination in patients with active, autoantibody-positive systemic lupus erythematosus. Lupus. 2017;26(14):1483–1490. doi:10.1177/0961203317703495
71. Kaufman M, Pardo G, Rossman H, Sweetser MT, Forrestal F, Duda P. Natalizumab treatment shows no clinically meaningful effects on immunization responses in patients with relapsing-remitting multiple sclerosis. J Neurol Sci. 2014;341(1–2):22–27. doi:10.1016/j.jns.2014.03.035
72. Brodmerkel C, Wadman E, Langley RG, et al. Immune response to pneumococcus and tetanus toxoid in patients with moderate-to-severe psoriasis following long-term ustekinumab use. J Drugs Dermatol. 2013;12(10):1122–1129.
73. Chioato A, Noseda E, Stevens M, et al. Treatment with the interleukin-17A-blocking antibody secukinumab does not interfere with the efficacy of influenza and meningococcal vaccinations in healthy subjects: results of an open-label, parallel-group, randomized single-center study. Clin Vaccine Immunol. 2012;19(10):1597–1602. doi:10.1128/CVI.00386-12
74. Mori S, Ueki Y, Hirakata N, et al. Impact of tocilizumab therapy on antibody response to influenza vaccine in patients with rheumatoid arthritis. Ann Rheum Dis. 2012;71(12):2006–2010. doi:10.1136/annrheumdis-2012-201950
75. Celotto K, Nair J, Lee K. The effect of bortezomib treatment on antibody titers against common viral and vaccine antigens. Clin Lymph Myelom Leuk. 2015;15:e179. doi:10.1016/j.clml.2015.07.402
76. Berger T, Elovaara I, Fredrikson S, et al. Alemtuzumab use in clinical practice: recommendations from European multiple sclerosis experts. CNS Drugs. 2017;31(1):33–50. doi:10.1007/s40263-016-0394-8
77. Issa NC, Baden LR. Current issues in vaccines for adult patients with hematologic malignancies. J Natl Compr Canc Netw. 2012;10(11):1447–1454. doi:10.6004/jnccn.2012.0147
78. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: raptiva EMEA/H/C/000542. Available from: https://www.ema.europa.eu/en/documents/product-information/raptiva-epar-product-information_en.pdf.
79. De Lavallade H, Khoder A, Hart M, et al. Tyrosine kinase inhibitors impair B-cell immune responses in CML through off-target inhibition of kinases important for cell signaling. Blood. 2013;122(2):227–238. doi:10.1182/blood-2012-11-465039
80. Winthrop KL, Silverfield J, Racewicz A, et al. The effect of tofacitinib on pneumococcal and influenza vaccine responses in rheumatoid arthritis. Ann Rheum Dis. 2016;75(4):687–695. doi:10.1136/annrheumdis-2014-207191
81. Douglas AP, Trubiano JA, Barr I, Leung V, Slavin MA, Tam CS. Ibrutinib may impair serological responses to influenza vaccination. Haematologica. 2017;102(10):e397. doi:10.3324/haematol.2017.164285
82. Struijk GH, Minnee RC, Koch SD, et al. Maintenance immunosuppressive therapy with everolimus preserves humoral immune responses. Kidney Int. 2010;78(9):934–940. doi:10.1038/ki.2010.269
83. Barmettler S, Ong MS, Farmer JR, et al. Association of immunoglobulin levels, infection risk, and mortality with rituximab and hypogammaglobulinemia. JAMA Netw Open. 2018;1(7):e184169. doi:10.1001/jamanetworkopen.2018.4169
84. Danovitch GM, editor. Handbook of Kidney Transplantation. Lippincott Williams & Wilkins; 2017 June, 13.
85. Terrault NA, Lok AS, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599. doi:10.1002/hep.29800
86. Winthrop KL. Tumor necrosis factor-alpha inhibitors: bacterial, viral, and fungal infections. Bow Blumberg EA, Bond Sh, editors. UpToDate Inc.2019. Available from: https://www.uptodate.com/contents/tumor-necrosis-factor-alpha-inhibitors-bacterial-viral-and-fungal-infections.
87. Morrison VA. Prevention of infections in patients with chronic lymphocytic leukemia. Bow E, Throner AR, editors. UpToDate Inc. 2019. Available from: https://www.uptodate.com/contents/prevention-of-infections-in-patients-with-chronic-lymphocytic-leukemia.
88. Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5(1):95. doi:10.1186/s40425-017-0300-z
89. Fishman JA, Gans H; AST Infectious Diseases Community of Practice. Pneumocystis jiroveci in solid organ transplantation: guidelines from the american society of transplantation infectious diseases community of practice. Clin Transplant. 2019;33:e13587.
90. Casulo C, Maragulia J, Zelenetz AD. Incidence of hypogammaglobulinemia in patients receiving rituximab and the use of intravenous immunoglobulin for recurrent infections. Clin Lymph Myelom Leuk. 2013;13(2):106–111. doi:10.1016/j.clml.2012.11.011
91. Yilmaz E, Mahani MG, Bilen MA, et al. Clinical characteristics of rituximab-induced late onset neutropenia. Am J Hematol. 2010;85(10):810–812. doi:10.1002/ajh.21818
92. Salmon JH, Cacoub P, Combe B, et al. Late-onset neutropenia after treatment with rituximab for rheumatoid arthritis and other autoimmune diseases: data from the autoimmunity and rituximab registry. RMD Open. 2015;1(1):e000034. doi:10.1136/rmdopen-2014-000034
93. Cohen BA. Late-onset neutropenia following ocrelizumab therapy for multiple sclerosis. Neurology. 2019;92(9):435–436. doi:10.1212/WNL.0000000000006924
94. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: xeljanz EMEA/H/C/004214. Available from: https://www.ema.europa.eu/en/documents/product-information/xeljanz-epar-product-information_en.pdf.
95. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: Jakavi - EMEA/H/C/002464. Available from: https://www.ema.europa.eu/en/documents/product-information/jakavi-epar-product-information_en.pdf. Accessed February 10, 2020.
96. Click B, Regueiro M. Managing Risks with Biologics. Curr Gastroenterol Rep. 2019;21(1):1. doi:10.1007/s11894-019-0669-6
97. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: gilenya EMEA/H/C/002202. Available from: https://www.ema.europa.eu/en/documents/product-information/gilenya-epar-product-information_en.pdf.
98. Furer V, Rondaan C, Heijstek MW, et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann Rheum Dis. 2020;79(1):39–52. doi:10.1136/annrheumdis-2019-215882
99. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: humira EMEA/H/C/000481. Available from: https://www.ema.europa.eu/en/documents/product-information/humira-epar-product-information_en.pdf.
100. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: enbrel. EMEA/H/C/000262l. Available from: https://www.ema.europa.eu/en/documents/product-information/enbrel-epar-product-information_en.pdf.
101. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: Simponi. European Medicines Agency. EMEA/H/C/000992. Available from: https://www.ema.europa.eu/en/documents/product-information/simponi-epar-product-information_en.pdf.
102. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: cimzia. EMEA/H/C/001037. Available from: https://www.ema.europa.eu/en/documents/product-information/cimzia-epar-product-information_en.pdf.
103. Papp KA, Haraoui B, Kumar D, et al. Vaccination guidelines for patients with immune-mediated disorders on immunosuppressive therapies. J Cutan Med Surg. 2019;23(1):50–74. doi:10.1177/1203475418811335
104. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: regeneron EMEA/H/C/001047. Available from: https://www.ema.europa.eu/en/documents/product-information/rilonacept-regeneron-epar-product-information_en.pdf.
105. Committee for Medicinal Products for Human Use (CHMP) International non- proprietary name: blincyto EMEA/H/C/003731 https://www.ema.europa.eu/en/documents/product-information/blincyto-epar-product-information_en.pdf.
106. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: ocrevus EMA/790835/2017. Available from: https://www.ema.europa.eu/en/documents/product-information/ocrevus-epar-product-information_en.pdf.
107. Stokmaier D, Winthrop K, Chognot C, et al. Effect of ocrelizumab on vaccine responses in patients with multiple sclerosis (S36. 002).
108. Beaulieu DB, Ananthakrishnan AN, Martin C, et al. Use of biologic therapy by pregnant women with inflammatory bowel disease does not affect infant response to vaccines. Clin Gastroenterol Hepatol. 2018;16(1):99–105. doi:10.1016/j.cgh.2017.08.041
109. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: arzerra EMEA/H/C/001131. Available from: https://www.ema.europa.eu/en/documents/product-information/arzerra-epar-product-information_en.pdf.
110. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: Gazyvaro - EMEA/H/C/002799. Available from:https://www.ema.europa.eu/en/documents/product-information/gazyvaro-epar-product-information_en.pdf. Accessed February 5, 2020.
111. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: mabcampath EMEA/H/C/000353. Available from: https://www.ema.europa.eu/en/documents/product-information/mabcampath-epar-product-information_en.pdf.
112. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: orenica EMEA/H/C/000701. Available from: https://www.ema.europa.eu/en/documents/product-information/orencia-epar-product-information_en.pdf.
113. Committee for Medicinal Products for Human Use (CHMP). International non- proprietary name: stelara EMEA/H/C/000958. Available from: https://www.ema.europa.eu/en/documents/product-information/stelara-epar-product-information_en.pdf.
114. Danziger Isakov L, Kumar D; AST ID Community of Practice. Vaccination of solid organ transplant candidates and recipients: guidelines from the American society of transplantation infectious diseases community of practice. Clin Transplant. 2019;33:e13563.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.