")
Back to Journals » International Journal of Women's Health » Volume 14
Prevalence of Sexual Dysfunction in Women with Type 1, 2 Diabetes and Thyroid Disorder: A Cross-Sectional Study in Taif City, Saudi Arabia
Authors Alshehri KM, Althobaiti RA, Alqurashi AI, Algethami NE , Alswat KA
Received 6 October 2021
Accepted for publication 22 December 2021
Published 17 March 2022 Volume 2022:14 Pages 385—394
DOI https://doi.org/10.2147/IJWH.S343065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Khalid M Alshehri,1 Raghad A Althobaiti,2 Athar I Alqurashi,3 Nada E Algethami,4 Khaled A Alswat5
1Medicine and Endocrinology, AlHada Armed Forced Hospital, Taif, Saudi Arabia; 2Obstetrics and Gynecology Department, Prince Sultan Military Medical City, Riyadh, Saudi Arabia; 3Internal Medicine Department, King Abdulaziz Specialist Hospital, Taif, Saudi Arabia; 4Medical College, Taif University, Taif, Saudi Arabia; 5Department of Medicine, School of Medicine, Taif University, Taif, 21944, Saudi Arabia
Correspondence: Raghad A Althobaiti, Obstetrics and Gynecology Department, Prince Sultan Military Medical City, Al Sulaimaniah, Riyadh, Saudi Arabia, Tel +966 505388455, Email [email protected]
Background: Women with diabetes mellitus or thyroid disorders are at risk of sexual dysfunction. This study aimed to estimate the prevalence of female sexual dysfunction (FSD) in women with diabetes and/or thyroid disorders and the impact of disease control on the ASEX score.
Methods: A cross-sectional study for female patients who had a routine clinic visits was included. The Arizona Sexual Experience Scale (ASEX) was used to evaluate for FSD. Those with a total score of ≥ 19 or scored ≥ 5 on any item or ≥ 4 on three items were considered to have FSD.
Results: A total of 253 female patients with a mean age of 39.1 ± 7.3 years were included. Two-thirds of the participants have no FSD. More than half (57.7%) of the participants had a strong desire for sex, and about 20% of the participants were unsatisfied with their orgasm. Compared to those with no FSD, those with FSD had lower BMI (P = 0.375), more likely to have a master’s degree or higher (P = 0.117), diabetes (P = 0.879), hypothyroidism (P = 0.625), diabetes-related microvascular and macrovascular complications (P = 0.049), higher HbA1c, fasting glucose, and TSH (P = 0.731, P = 0.161, and P = 0.561, respectively), lower total cholesterol and LDL (P = 0.368 and P = 0.339, respectively), and exercise more regularly (P = 0.929).
Conclusion: FSD was highly prevalent in our study population. Those with type 1 diabetes had the highest ASEX scores. We showed non-significant negative correlations between total ASEX score and both BMI and TSH, as well as a non-significant positive correlation between total ASEX score and both HbA1c and fasting glucose value.
Keywords: diabetes mellitus, thyroid disorders, female sexual dysfunction, prevalence
Introduction
Sexual functions are an important aspect of human life. Along with sleeping and eating, sexual functioning is one of the basic human drives. As such, sexual satisfaction and normal sexual functioning are significant factors in determining quality of life.1
Many definitions of sexual dysfunctions have been described in the literature. However, all refer to either a sexual life not meeting the person’s expectations or a disturbance in their normal sexual response during any part of intercourse that leads to less or no satisfaction. According to the Diagnostic and Statistical Manual of Mental Disorders (5th edition), there are three main categories of female sexual dysfunction (FSD): female sexual interest/arousal disorder, female orgasmic disorder, and genitopelvic pain/penetration disorder. 2,3
Depression was found to be the most common cause for FSD in several published studies, not to mention that sexual dysfunction itself could lead to depression as well.4 Also, antidepressant medications, such as serotonin reuptake inhibitors, affect sexual desire and function.5
Women with diabetes are at increased risk of developing depression which is the most well-established risk factor for female sexual dysfunction.6,7 Moreover, diabetes negatively impacts sexual function in different psychological ways including low self-image, tiredness, and reduced in pleasure from sex. 8,9
On the medical aspect, diabetes increases the risk of vaginal infection, dyspareunia, and general orgasmic problem.10
Furthermore, chronic diseases, such as systemic hypertension, can contribute to sexual dysfunction due to vascularity impairment of many structures, including the genital area.11 Also, DM and thyroid can potentially affect the quality of sexual life.12
Diabetes will affect more than 70 million in the Middle East and North African region by 2040. 13 Saudi Arabia also has one of the highest diabetes prevalence, estimated at 17.6%. 13 The consequences of diabetes result from its complications, including retinopathy, peripheral neuropathy, renal complications, stroke, and heart complications. 14 Diabetes has also been considered a risk factor for impaired sexual function in males and females. 15
The relation between diabetes and erectile dysfunction among men is well established.16 However, few studies focus on FSD among diabetic women with a poor understanding of factors leading to FSD among diabetic women. 17,18 FSD is more commonly surrounded by social barriers, preventing the patient from discussing sexual problems with the physician and taking appropriate medical advice.19
This study was motivated by the scarcity of studies on FSD in Saudi Arabia. Our study aims to add more information about FSD in the population of women from the Arab culture. We assess the prevalence of sexual dysfunction among women with diabetes mellitus and thyroid disorders and the relationships between DM complications, treatment modalities, and disease control.
Ethics Approval and Consent to Participate
The study was approved by the Ethical Committee (IRB) of AlHada Armed Forces Hospital, Taif, Saudi Arabia (reference number: 2020–444). All procedures were in accordance with the ethical standards of the regional research committee and with the Declaration of Helsinki 1964 and its later amendments. After explaining the study’s purposes, both written and verbal consent were obtained from all participants and women were informed that their participation was voluntary, confidential, and anonymous.
Methods
This was a cross-sectional study of female patients who had routine clinic visits to Prince Mansour Diabetes Center or AlHada Armed Forces Hospital, from January to November 2020 in Taif, Saudi Arabia. We included 18- to 50-year-old female patients with DM and/or thyroid patients, who are married and had recent (within 1 year) laboratory tests. We excluded those with end-stage renal disease, active psychiatric illness, and divorced/single. The questionnaire included the following items: personal data, physical activities, type of diabetes and thyroid disorder, DM complications, and medications. We also collected data about the height and weight of each patient, and their body mass index (BMI) was calculated. Laboratory data for our participants collected from the electronic medical record. We divided our participants according to high (>15,000 Saudi Riyals), moderate (15,000–5000), and low monthly (<5000 Saudi Riyals) income.
Three female physicians communicated with the female patients during the data collection. Also, we used a separate room in the clinic to obtain the data to ensure privacy. We briefly explained to patients about the data and scoring system before starting. Both verbal and written consent taken from participants before starting the interview, and their responses were completely confidential. Data collected through a questionnaire administered to each participant by one of the researchers through face-to-face interviews than by phone interview (due to COVID-19 lockdown).
The researchers used an Arabic validated version of the ASEX to screen FSD. 20 The ASEX consists of five questions to evaluate each of the following: the ability to reach orgasm, arousal, sex drive, satisfaction with orgasm, and vaginal lubrication for females. The scores ranged from 5 to 30, participants with high scores representing higher levels of sexual dysfunction. Participants classified into sexual dysfunction if they have one of the following: total score of 19 or more, if the patient scored five or more on any of the five items, and if the patient scored four or more on three items.
Data coded and entered in a Microsoft Excel spreadsheet, and then imported to Statistical Package for Social Sciences (SPSS) version 23. The qualitative data presented as numbers and percentages. The quantitative data are given as means and standard deviation (mean ± SD). The Chi-square test was used to study the relationship between variables, and the t-test was used to compare means. A P-value less than 0.05 (typically ≤0.05) is statistically significant.
Result
A total of 253 female participants were included in the study, with a mean age of 39.1 ± 7.3 years, with a mean BMI in the obesity range (Table 1). Two-thirds of the participants had a bachelor’s degree or higher, and one-fifth of the patients was earning a low income. The most common comorbidities were hypothyroidism, followed by type 2 diabetes, while the least prevalent were cardiac disease and stroke. Half of the patients are taking thyroxine, while one-fifth were taking cholecalciferol. The most prescribed medication was oral hypoglycemic agents for those with type 2 diabetes with optimal glycemic control based on the mean HbA1c and fasting glucose. Majorities of the participants report ≥150 min of exercise per week.
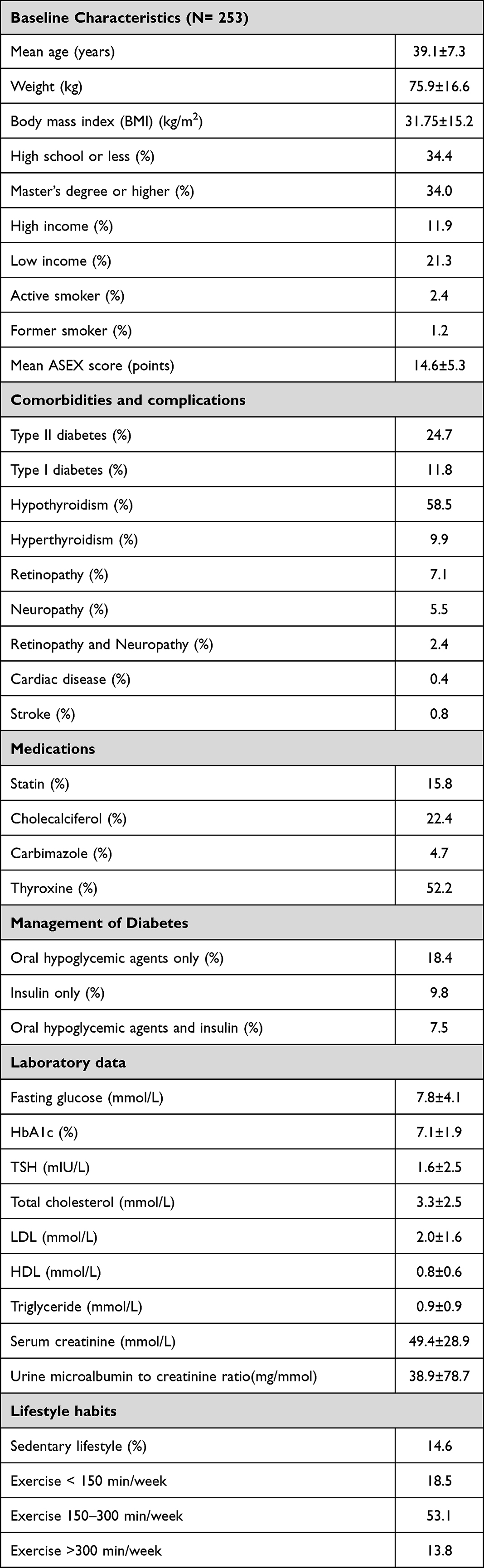 |
Table 1 Baseline Characteristics of the Whole Cohort |
Regarding the participant’s response to the Arizona Sexual Experiences Scale (ASEX), sex drive was strong in 57.7% (Table 2). Also, two-thirds of the participants were easily aroused, had no problem with vaginal dryness during sexual intercourse, and achieved orgasm. Around 20% of the participants were unsatisfied with their orgasm.
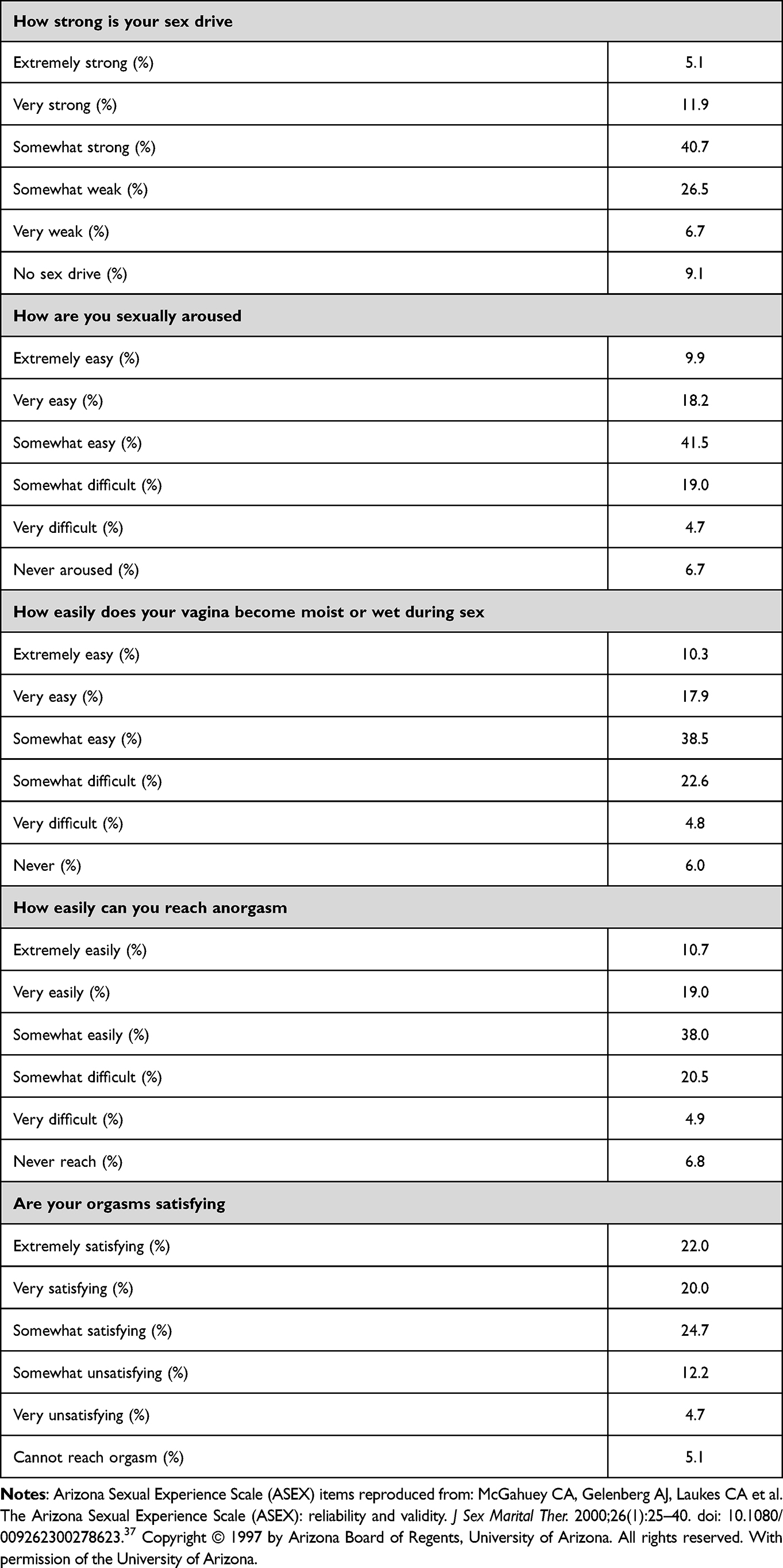 |
Table 2 Arizona Sexual Experiences Scale (ASEX) Response |
Based on the ASEX questionnaire, two-thirds of the participants have no FSD (Table 3). Compared to those with no FSD, those with FSD had lower BMI (P = 0.375), were more likely to have a master’s degree or higher (P = 0.117), diabetes (P = 0.879), hypothyroidism (P = 0.625), diabetes-related microvascular complications and stroke (P = 0.049), taking cholecalciferol (P = 0.222), higher HbA1c (P = 0.731), higher fasting glucose (P = 0.161), higher TSH level (P = 0.561), lower total cholesterol (P = 0.368), lower LDL level (P = 0.339), higher urinary microalbuminuria (P = 0.343), and exercise more regularly (P = 0.929).
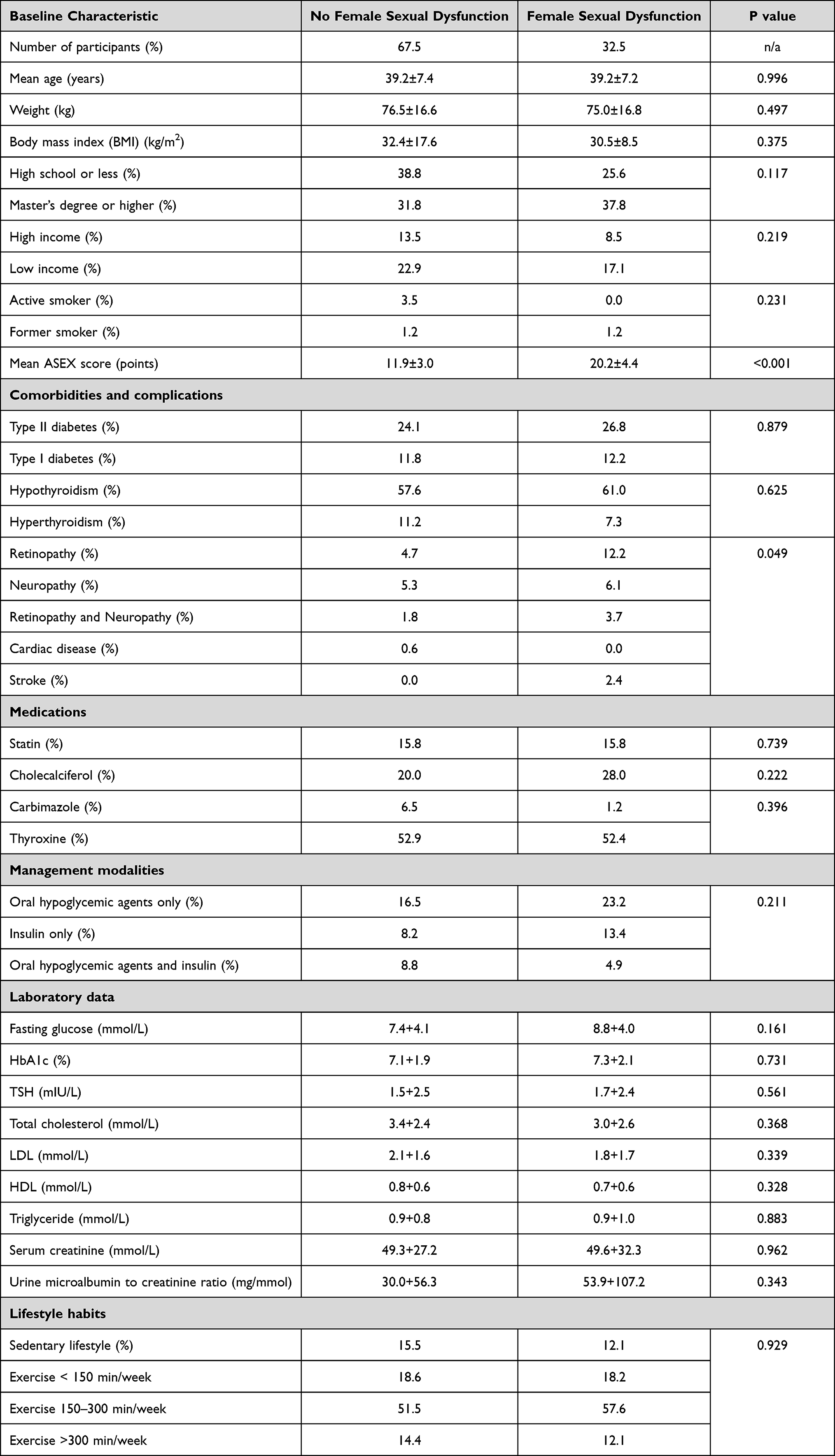 |
Table 3 Baseline Characteristics Based on the ASEX Score |
Patients with diabetes and coexisting thyroid disorders were found to have high ASEX score (Figure 1).
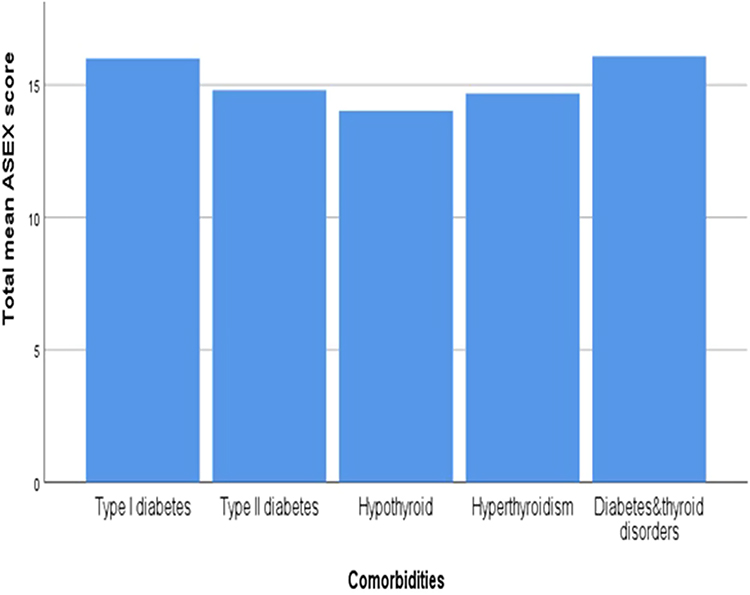 |
Figure 1 Total mean ASEX score according to the comorbidities. |
Partial correlation adjusting for age, education, income, smoking, comorbidities, and exercise showed a non-significant negative correlation between total FSD score and both BMI (r −0.275, P 0.363) and TSH (r = −0.070, P = 0.820) and a non-significant positive correlation between total FSD score and both HbA1c (r = 0.309, P = 0.304) and the fasting blood glucose (r = 0.460, P = 0.114).
Discussion
Our study shows that around one-third of the patients have FSD based on the ASEX tool. Similar findings were reported in a recent study in Turkey.21 Also, our study showed that patients with diabetes and thyroid dysfunction have the highest ASEX score. Previous studies nationally and regionally in patients with type 2 diabetes showed a higher prevalence of FSD.22,23 The observed difference is likely related to the younger age, optimal glycemic control, and the FSD screening tool in our study. Also, we showed that both fasting glucose and HbA1c positively correlated with the ASEX score. Similar findings were reported in previous studies.24,25 Patients with type 1 diabetes also had a higher ASEX score in our study. Similar findings were observed in the previously published case-control study.26
Hypothyroid patients in our study had the lowest ASEX score. A previous study showed that patients with subclinical hypothyroidism had an increased risk of FSD.27 The observed difference is likely related to the hypothyroidism control as we showed this in the mean TSH level and the negative correlation between ASEX and TSH in our study. The observed increased ASEX score in our patients with hyperthyroidism was demonstrated in a previous study and likely explained by hormonal changes other than TSH and depression.28
We showed that FSD patients have a lower BMI. This is opposite to what has been reported in a previous study, where BMI was negatively correlated with sexual dysfunction.29,30 This might be explained by our study population, where the low mean BMI might indicate poorly controlled underlying disease among the participants.
Our study included few patients who are actively smoking, but we did not identify a relationship with the score. Similar findings were observed between smoking and FSD in previous studies.31,32 LDL and total cholesterol in our patients with FSD were lower than those without FSD. This was also observed in a recently published study where hyperlipidemia increased FSD risk.33,34 Also, our patients with positive urinary microalbuminuria were more likely to have FSD. Similar findings were reported in previous studies in patients with chronic kidney disease.35,36
The strengths of our study include its novelty and the collection of comprehensive clinical and biochemical data. Limitations include the small patient size and that only a single center was included.
Conclusion
FSD is highly prevalent in our study population with a one-third (32.5%) of the patients have FSD based on the ASEX score. Type 1 diabetes has the highest ASEX score. Non-significant negative correlation between total ASEX score and both BMI and TSH and a non-significant positive correlation between total ASEX score and both HbA1c and fasting blood glucose. It seems that FSD is commonly prevalent among patients with thyroid disease and diabetes and increasing awareness among health-care provider is highly recommended to address this issue.
Abbreviations
DM, Diabetes mellitus; FSD, Female sexual dysfunctions; ASEX, Arizona Sexual Experience Scale; BMI, Body Mass Index; TSH, Thyroid stimulating hormone; HbA1C, Hemoglobin A1C; LDL, Low-density lipoprotein.
Data Sharing Statement
The datasets used in this study are available from the corresponding author upon request.
Acknowledgments
The authors would like to acknowledge Taif university for their support of the study. We also thank the patients who participated in the study. As well as AlHada and prince Mansour Military hospital for their facilitation of the data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was supported by the Taif University Research Support Project Number (TURSP-2020/37), Taif University, Taif, Saudi Arabia.
Disclosure
The authors have no conflicts of interest for this work to declare.
References
1. Flynn K, Lin L, Bruner D, et al. Sexual satisfaction and the importance of sexual health to quality of life throughout the life course of U.S. adults. J Sex Med. 2016;13(11):1642–1650. doi:10.1016/j.jsxm.2016.08.011
2. Chen C, Lin Y, Chiu L, et al. Female sexual dysfunction: definition, classification, and debates. Taiwan J Obstet Gynecol. 2013;52(1):3–7. doi:10.1016/j.tjog.2013.01.002
3. Gabriel Tobia W. DSM-5 changes in diagnostic criteria of sexual dysfunctions. Reprod Syst Sexual Disord. 2013;02:02. doi:10.4172/2161-038X.1000122
4. Schram MT, Baan C, Pouwer F, et al. Depression and quality of life in patients with diabetes: a systematic review from the European Depression in Diabetes (EDID) research consortium. Curr Diabetes Rev. 2009;5(2):112–119. doi:10.2174/157339909788166828
5. DCCT/EDIC Research Group, Enzlin P, Rosen R, Wiegel M, et al. Sexual dysfunction in women with type 1 diabetes: long- term findings from the DCCT/EDIC study cohort. Diabetes Care. 2009;32(5):780–785. doi:10.2337/dc08-1164.
6. Rockliffe-Fidler C, Kiemle G. Sexual function in diabetic women: a psychological perspective. Sexual Relationship Ther. 2003;18(2):143–159. doi:10.1080/1468199031000099415
7. Enzlin P, Mathieu C, Van den Bruel A, et al. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes Care. 2003;26(2):409–414. doi:10.2337/diacare.26.2.409
8. Kennedy SH, Rizvi S. Sexual dysfunction, depression, and the impact of antidepressants. J Clin Psychopharmacol. 2009;29(2):157–164. doi:10.1097/JCP.0b013e31819c76e9.
9. Basson R. Human sex-response cycles. J Sex Marital Ther. 2001;27(1):33–43. doi:10.1080/00926230152035831
10. Barnard KD, Naranjo D, Johnson N, et al. Diabetes and female sexual health: an ongoing challenge. Pract Diabetes. 2019;36(5):165–169. doi:10.1002/pdi.2238
11. Manolis AJ, Doumas M, Viigimaa M, Narkiewicz K. Hypertension, and sexual dysfunction. European Society of Hypertension. Sci Newslett. 2007;8:32.
12. Stechova K, Mastikova L, Urbaniec K, et al. Sexual dysfunction in women treated for type 1 diabetes and the impact of coexisting thyroid disease. Sexual Med. 2019;7(2):217–226. doi:10.1016/j.esxm.2019.03.001
13. Ogurtsova K, da Rocha Fernandes J, Huang Y, et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024
14. Mao W, Yip CW, Chen W. Complications of diabetes in China: health system and economic implications. BMC Public Health. 2019;19(1):269. doi:10.1186/s12889-019-6569-8
15. Giraldi A, Kristensen E. Sexual dysfunction in women with diabetes mellitus. J Sex Res. 2010;47(2–3):199–211. doi:10.1080/00224491003632834
16. Malavige L, Levy J. Erectile dysfunction in diabetes mellitus. J Sex Med. 2009;6(5):1232–1247. doi:10.1111/j.1743-6109.2008.01168.x
17. Monga M, Alexandrescu B, Katz S, Stein M, Ganiats T. Impact of infertility on quality of life, marital adjustment, and sexual function. Urology. 2004;63(1):126–130. doi:10.1016/j.urology.2003.09.015
18. Pontiroli A, Cortelazzi D, Morabito A. Female sexual dysfunction and diabetes: a systematic review and meta‐analysis. J Sex Med. 2013;10(4):1044–1051. doi:10.1111/jsm.12065
19. Mohsenpour B, Alizadeh N, Alizadeh N, Arasteh M, Karimian F. Comparison of sexual dysfunction between diabetic and non-diabetic women. J Midlife Health. 2013;4(3):167. doi:10.4103/0976-7800.119001
20. Nakhli J, El Kissi Y, Bouhlel S, et al. Reliability and validity of the Arizona Sexual Experiences Scale-Arabic version in Tunisian patients with schizophrenia. Compr Psychiatry. 2014;55(6):1473–1477. doi:10.1016/j.comppsych.2014.04.006
21. KarakaşUğurlu G, Uğurlu M, Çayköylü A. Prevalence of female sexual dysfunction and associated demographic factors in Turkey: a meta-analysis and meta-regression study. Int J Sexual Health. 2020;3:1–8.
22. Elyasi F, Kashi Z, Tasfieh B, Bahar A, Khademloo M. Sexual dysfunction in women with type 2 diabetes mellitus. Iran J Med Sci. 2015;40(3):206.
23. AlMogbel TA, Amin HS, AlSaad SM, AlMigbal TH. Prevalence of sexual dysfunction in Saudi women with Type 2 diabetes: is it affected by age, glycemic control, or obesity? Pak J Med Sci. 2017;33(3):732. doi:10.12669/pjms.333.12166
24. Maiorino MI, Bellastella G, Esposito K. Diabetes, and sexual dysfunction: current perspectives. Diabetes Metabol Syndr Obesity. 2014;7:95.
25. Afshari P, Yazdizadeh S, Abedi P, Rashidi H. The relation of diabetes type 2 with sexual function among reproductive age women in Iran, a case-control study. Advan Med. 2017:2017.
26. Enzlin P, Mathieu C, Van den Bruel A, Bosteels J, Vanderschueren D, Demyttenaere K. Sexual dysfunction in women with type 1 diabetes: a controlled study. Diabetes Care. 2002;25(4):672–677. doi:10.2337/diacare.25.4.672
27. Zhang Y, Tang Z, Ruan Y, et al. Prolactin and thyroid stimulating hormone (TSH) levels and sexual dysfunction in patients with schizophrenia treated with conventional antipsychotic medication: a cross-sectional study. Med Sci Monitor. 2018;24:9136. doi:10.12659/MSM.913759
28. Atis G, Dalkilinc A, Altuntas Y, et al. Hyperthyroidism: a risk factor for female sexual dysfunction. J Sex Med. 2011;8(8):2327–2333. doi:10.1111/j.1743-6109.2011.02354.x
29. Jamali S, Zarei H, Jahromi AR. The relationship between body mass index and sexual function in infertile women: a cross-sectional survey. Iranian J reprod med. 2014;12(3):189.
30. Mozafari M, Khajavikhan J, Jaafarpour M, Khani A, Direkvand-Moghadam A, Najafi F. Association of body weight and female sexual dysfunction: a case control study. Iran Red Crescent Med J. 2015;17(1):Jan. doi:10.5812/ircmj.24685
31. Costa RM, Peres L. Smoking is unrelated to female sexual function. Subst Use Misuse. 2015;50(2):189–194. doi:10.3109/10826084.2014.962054
32. Wallwiener C, Wallwiener L, Seeger H, Mück A, Bitzer J, Wallwiener M. Prevalence of sexual dysfunction, and impact of contraception in female German medical students. J Sex Med. 2010;7:6. doi:10.1111/j.1743-6109.2010.01742.x
33. Baldassarre M, Alvisi S, Mancini I, et al. Impaired lipid profile is a risk factor for the development of sexual dysfunction in women. J Sex Med. 2016;13(1):46–54. doi:10.1016/j.jsxm.2015.11.005
34. Xiang Y, Tang Y, Li J, How LD. Is the sexual function of premenopausal Chinese women without hyperlipidemia? Sexual Med. 2020;8(1):65–75. doi:10.1016/j.esxm.2019.10.004
35. Satta E, Magno C, Galì A, et al. Sexual dysfunction in women with diabetic kidney. Int J Endocrinol. 2014;2014:1–6. doi:10.1155/2014/346834
36. Palmer BF. Sexual dysfunction in men and women with chronic kidney disease and end-stage kidney disease. Adv Ren Replace Ther. 2003;10(1):48–60. doi:10.1053/jarr.2003.50003
37. McGahuey CA, Gelenberg AJ, Laukes CA, et al. The Arizona Sexual Experience Scale (ASEX): reliability and validity. J Sex Marital Ther. 2000;26(1):25–40. doi:10.1080/009262300278623
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.