")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Prevalence of Raynaud’s Phenomenon in Saudi Arabia
Authors Mustafa M , Alsulaimani H , Alhaddad A, Almujil S, Albar Z, Bawazir Y , Alsolaimani R, Omair MA
Received 9 December 2021
Accepted for publication 1 March 2022
Published 9 March 2022 Volume 2022:14 Pages 17—24
DOI https://doi.org/10.2147/OARRR.S352655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Tamer Gheita
Mohammad Mustafa,1 Hadeel Alsulaimani,2 Abdulrahman Alhaddad,3 Sara Almujil,2 Zainab Albar,4 Yasser Bawazir,5 Roaa Alsolaimani,5 Mohammed A Omair6
1Department of Medicine, Rheumatology Unit, University of Jeddah, Jeddah, Saudi Arabia; 2Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 3Faculty of Medicine, King Saud Bin Abdulaziz University for Health and Science, Jeddah, Saudi Arabia; 4School of Medicine, Umm Al Qura University, Makkah, Saudi Arabia; 5Rheumatology Unit, Department of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 6Division of Rheumatology, Department of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Mohammad Mustafa, Department of Medicine, University of Jeddah, Jeddah, Saudi Arabia, Tel +966 541318900, Email [email protected]
Purpose: Raynaud’s phenomenon (RP) is defined as frequent ischaemic attacks in the fingers and toes due to vascular vasospasm. Studies have been conducted in many countries worldwide to determine the prevalence of RP. The aim of the current study was to assess the prevalence of RP in the Saudi Arabian population.
Patients and Methods: An online survey based on international consensus criteria used to diagnose RP was conducted to collect data from individuals from the Saudi population. Participants were considered positive if they had triphasic or biphasic colours of the extremities with cold-related sensitivity. Awareness of RP was also assessed.
Results: A total of 1025 responses were collected and included in the final analysis. The prevalence of RP was 4.29%, including 22% men and 77% women. The most common age group among women was 26– 40 years (36.3%). Familiarity with RP was low, with 56.82% of participants lacking adequate awareness regarding RP. Only 32% of patients with RP reported attending doctor visits regarding symptoms of the disease.
Conclusion: The RP prevalence in Saudi Arabia is comparable to that reported in the international literature. Public awareness activities should be conducted to increase knowledge about RP.
Trial Registration: Not applicable.
Keywords: Raynaud’s phenomenon, cold sensitivity, awareness
Introduction
Raynaud’s phenomenon (RP) is a relatively common vasospastic condition that carries a significant burden of pain and hand-related disability that is often neglected. The state induces episodic spasms of arteries resulting in reduced blood flow to the fingers and, less commonly, the toes, which produces a colour change characteristic of the disorder as a response to physical, emotional, or chemical stress.1 It presents with multiple attacks producing two or three colour changes, beginning with white, blue and then changing to red to indicate cyanosis and hyperaemia.1,2 Although the disease’s pathogenesis has yet to be elucidated, different intravascular, neural and vascular abnormalities play a role in the phenomenon.2,3
Recent studies have aided in clarifying the pathophysiology of RP. RP is highly localized and affects the arterial inflow of specific skin areas, such as the fingers, toes, ears and tip of the nose. These sites are distinct from other skin areas in that they have specialized structural and functional features for thermoregulation.4 They have a high density of arteriovenous anastomoses, which bypass the capillaries and provide direct connections between arterioles and venules. The arteriovenous anastomoses therefore do not contribute to capillary blood flow, which provides essential nutritional support to the skin, but instead function as thermoregulatory structures.4 During exposure to cold, the arteriovenous anastomoses remain predominantly closed, whereas they are fully dilated during the elimination of heat. Cold-induced cutaneous vasoconstriction is mediated by a reflex increase in sympathetic constrictor nerve activity and local cold-induced amplification of the sympathetic response.
RP can be classified into two types, primary (which is idiopathic) or secondary to a wide range of underlying medical conditions.1 Other causes for secondary RP are vascular trauma and the use of vibrating tools.5 In primary RP, patients have a younger age at onset (usually between 15 and 30 years) than those with the secondary subtype, the thumb is generally spared,6 and there is no evidence of an underlying cause, peripheral vascular disease, digital ischaemic injury, or abnormal nail fold capillaries. Although primary RP can be uncomfortable, it is a relatively benign condition. However, secondary RP can be the first presentation of many underlying diseases, such as autoimmune and systemic rheumatic conditions.6,7 Despite the community of RP worldwide, a consensus among physicians on an ideal diagnostic criterion has not yet been reached. However, a panel of physicians recently concurred via a Delphi exercise upon a new 3 step approach diagnostic system they deemed “appropriate and accurate”.8
The non-pharmacological management is fundamental in RP treatment. In some instances, avoiding precipitating factors can be challenging, and small doses of vasodilators such as calcium channel blockers, angiotensin receptor blockers, or angiotensin converting enzyme inhibitors can be started. Failure of first line treatment or development of complications such as ulcers or gangrene requires adding phosphodiesterase inhibitors or intravenous prostaglandins. Bosentan an endothelin receptor blocker has been shown to reduce digital ulcers but has no direct impact on RP.9
Previous studies estimated that the prevalence of RP is affected by sex and geographic location, resulting in a range from 20% in women to less than 1% in men according to the definition used and the study selection criteria.6 In 2015, the first meta-analysis to study the global epidemiology of RP showed that the prevalence among the general population was 4.85%, with an annual incidence of 0.25%.6 This meta-analysis also demonstrated that RP is more common in women and has a young onset age.6 SmoKing and family history were commonly identified risk factors. A study conducted in South Carolina in the United States estimated that 3.5% of the adult population had RP, with the rate being highest in white women and lowest in black men. The overall ratio of males to females also suggests that the condition is more common in women.10 A Spanish study indicated that 3.2% of men and 4.7% of women had RP, with 89% of all cases consisting of primary RP and 11% consisting of secondary RP. Additionally, there was a strong association between RP and perniosis, acrocyanosis, or migraines in women.11 Aljohani et al11,12 evaluated RP in 747 Saudi medical students and reported a prevalence of 5.3%, most of whom were women. There was no correlation between an RP diagnosis and smoking in this study, probably due to the selection bias of the study population.12
The incidence of RP dramatically exceeds the number of patients who seek medical attention.13 Furthermore, another study showed that among 63 patients diagnosed with RP, only 12 (19%) discussed the issue with a physician, reflecting their lack of knowledge about the phenomenon as a disease.13 However, insufficient information about RP was also found among healthcare practitioners, reflecting the lack of knowledge in the general population.11
In this manuscript, we will assess the prevalence of RP and determine the level of RP awareness associated with diagnosis of RP after controlling for common risk factors using the Saudi Arabian general population. This will help to improve awareness of RP among healthcare providers and the general population and to provide optimal patient care in Saudi Arabia.
Materials and Methods
Design and Setting
This cross-sectional study was conducted between May 2020 and February 2021 among the general Saudi Arabian population. Participants with a coexisting rheumatological disease such as systemic sclerosis (SSc), systemic lupus erythematosus (SLE), Sjögren’s syndrome (SS), vasculitis, and inflammatory myositis were included. Participants using medications that could induce RP, such as beta-blockers, selective serotonin reuptake inhibitors (SSRIs), ergotamine, and chemotherapy agents, were excluded. This study was consistent with the Declaration of Helsinki and it was approved by the Department of Biomedical Ethics Unit & Academic Affairs of King Abdulaziz University, Jeddah (reference number 263-20). All participants were informed about the purpose of the survey and consent was obtained from them by their voluntary completion of the survey. For the participant under 18 years of age, parental informed consent was taken before their participation.
Sampling
The sample size was determined using the Raosoft online sample size calculator.14 The sample size (N=385) was calculated using the size of the general population, a 5% type I error and a 95% confidence interval.
Data Collection
The survey used an online questionnaire platform and was distributed in a randomized manner that ensured its delivery to most Saudi Arabian citizens through social media (WhatsApp and Twitter). The survey was divided into 4 parts.
Part one included the respondent characteristics, such as age, sex, education level, income, occupation, and smoking history (6 items).
Part two consisted of a validated question for the diagnosis of RP based on international consensus criteria for RP diagnosis: 1) Are your fingers susceptible to cold? 2) Do your fingers change colour when they are exposed to cold temperatures? 3) Do they turn white, blue, red, or multiple colours? (3 items).8 Participants were considered to have self-reported RP if they had triphasic or biphasic colours with cold-related sensitivity.
Part three was a non-validated question that was designed by investigators based on previous studies to evaluate various elements that can be risk factors for RP and to differentiate between primary and secondary aetiologies.6,10,11,13,15
Part four was a question measuring the awareness level of RP and its requirements for seeking medical advice.
Statistical Analysis
Data quality was assessed by determining the distribution of relevant variables. All variables were categorically summarized as frequencies and percentages. The primary outcome measure was a binary variable indicating diagnosis of RP extracted from two questions in the survey, defined as the presence of finger colour changes to white and blue or red.
Univariate analyses were performed using logistic regression to assess the associations between the binary outcome variable diagnosis of RP and the independent variables knowledge about RP and its common risk factors. Significant variables associated with a diagnosis of RP with a p-value <0.05 in the univariate analyses were selected for inclusion in the multivariate logistic regression model depending on the variable selection criteria in Vittinghoff et al16 2012.
Model fitting was thoroughly performed by adding one relevant variable after another, and four variables were used in each multivariate model because only 44 participants were diagnosed with RP. The rule of thumb of including one variable for each of the ten outcome events was used to avoid model overfitting.17 The variables were assessed for multicollinearity and maintained or removed depending on the Akaike information criteria (AIC). Goodness of fit of the multivariate model was assessed using the Pearson chi square test until we developed our three best multivariate models. Stata 16 was used to perform all statistical analyses.18
Reporting
This study was conducted and the manuscript was reported according to the Strobe guidelines for observational studies.19
Results
Descriptive characteristics of the study participants are presented in Table 1. A total of 1500 participants were invited to complete the questionnaire. Of those, 1025 participants completed the questionnaire, generating a response rate of 68.3%, and were included in the final analysis. Forty-four respondents answered positively, suggesting a diagnosis of RP (4.29%), and 56.82% lacked adequate awareness regarding RP. As shown in Table 1, Fisher’s test was used to compare the RP groups because some cells had fewer than 5 responses. Significantly different variables with p-values less than 0.05 included age, female sex, family history, knowledge about RP, association with other rheumatological diseases, and repeated doctor office visits for RP symptom complaints.
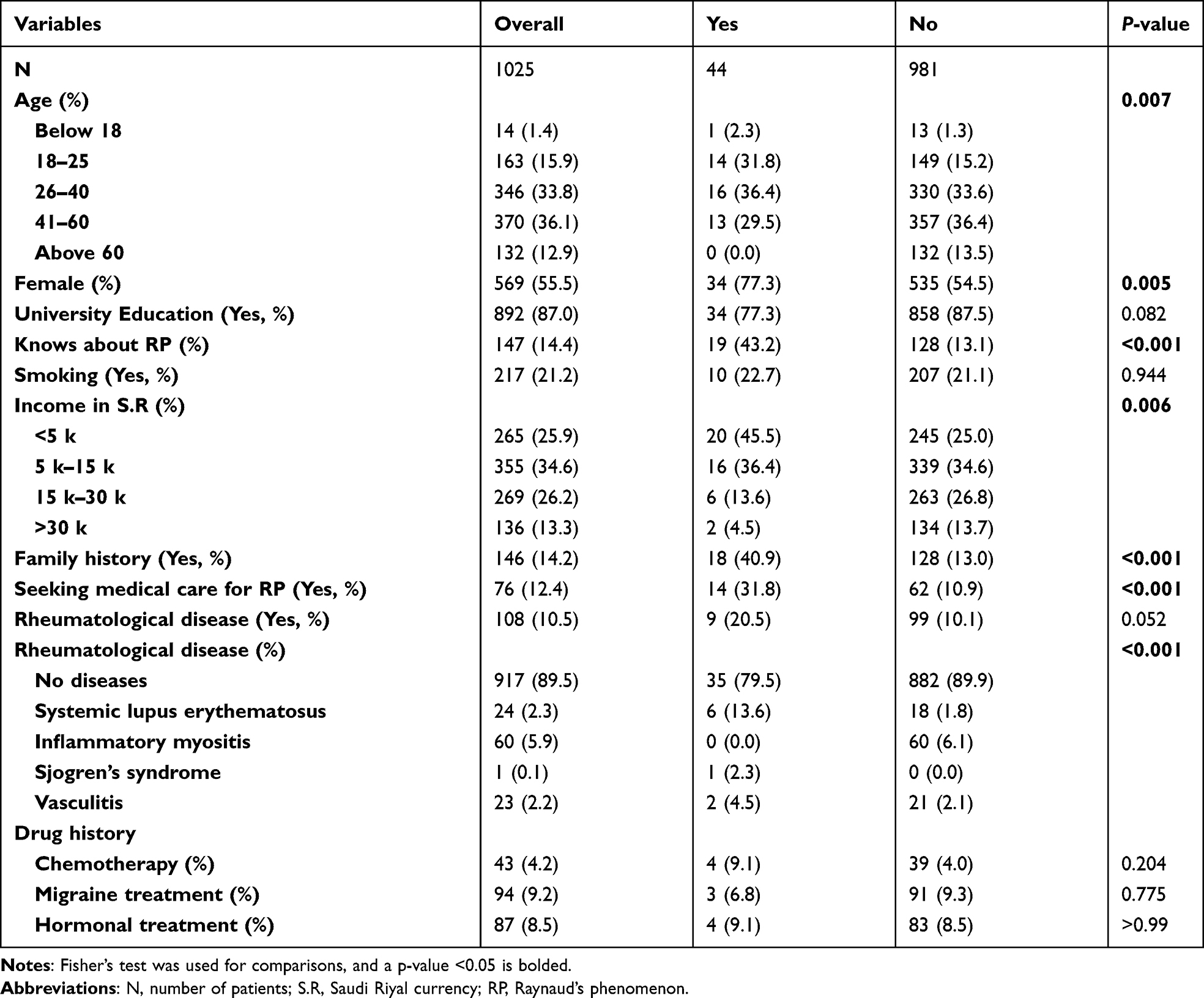 |
Table 1 Descriptive Characteristics of Respondents Across Raynaud’s Phenomenon Groups |
There was no significant difference between the RP and non-RP groups regarding income, smoking, reported chemotherapy drug history, migraine, or hormonal therapies. We evaluated the association between RP and common risk factors using univariate logistic regression models (Table 2). Variables selected for inclusion in the multivariate models with a p-value less than 0.05 were considered significant. The final multivariate models used to evaluate the association between RP and knowledge about RP, after controlling for age group and sex, are shown in Table 3.
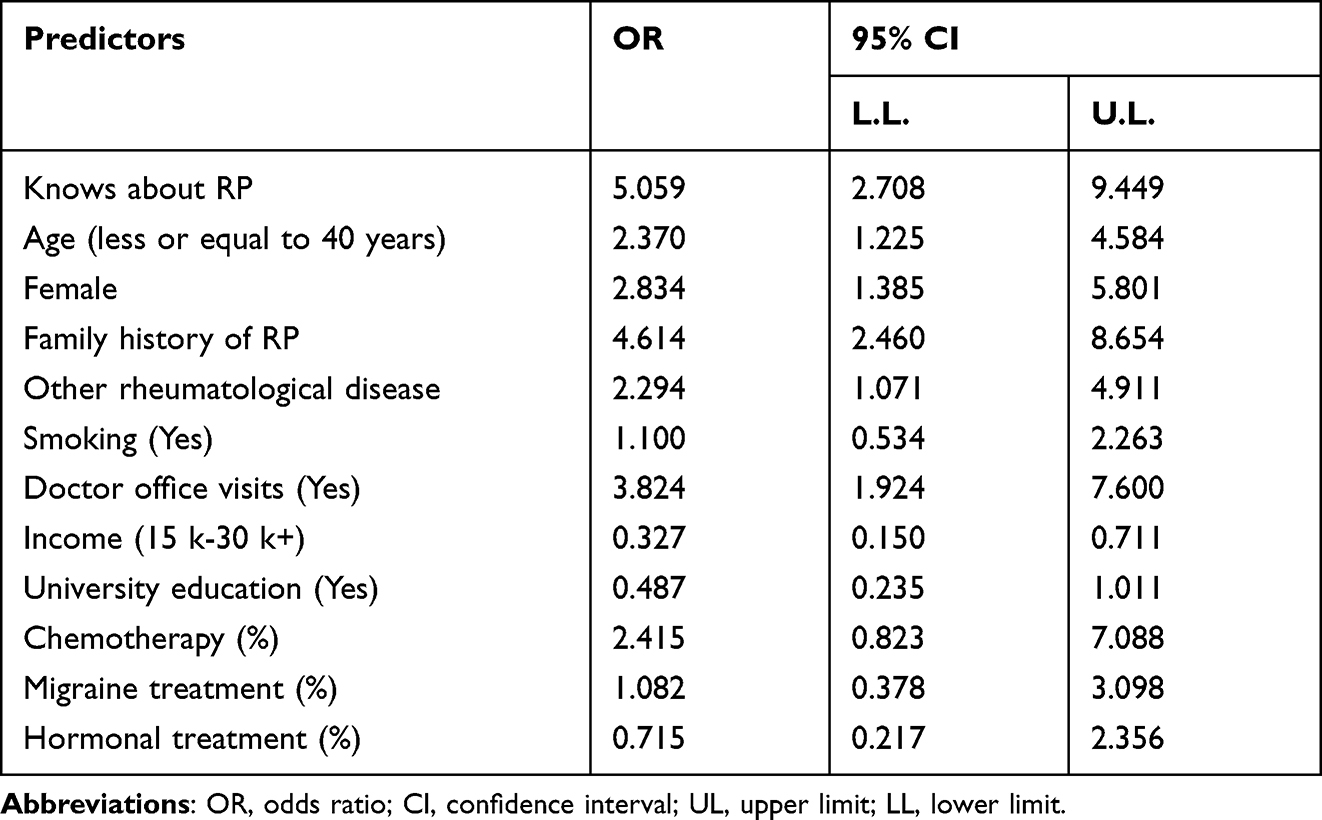 |
Table 2 Association Between Common Risk Factors and the Diagnosis of Raynaud’s Phenomenon Using Univariate Logistic Regression Analysis |
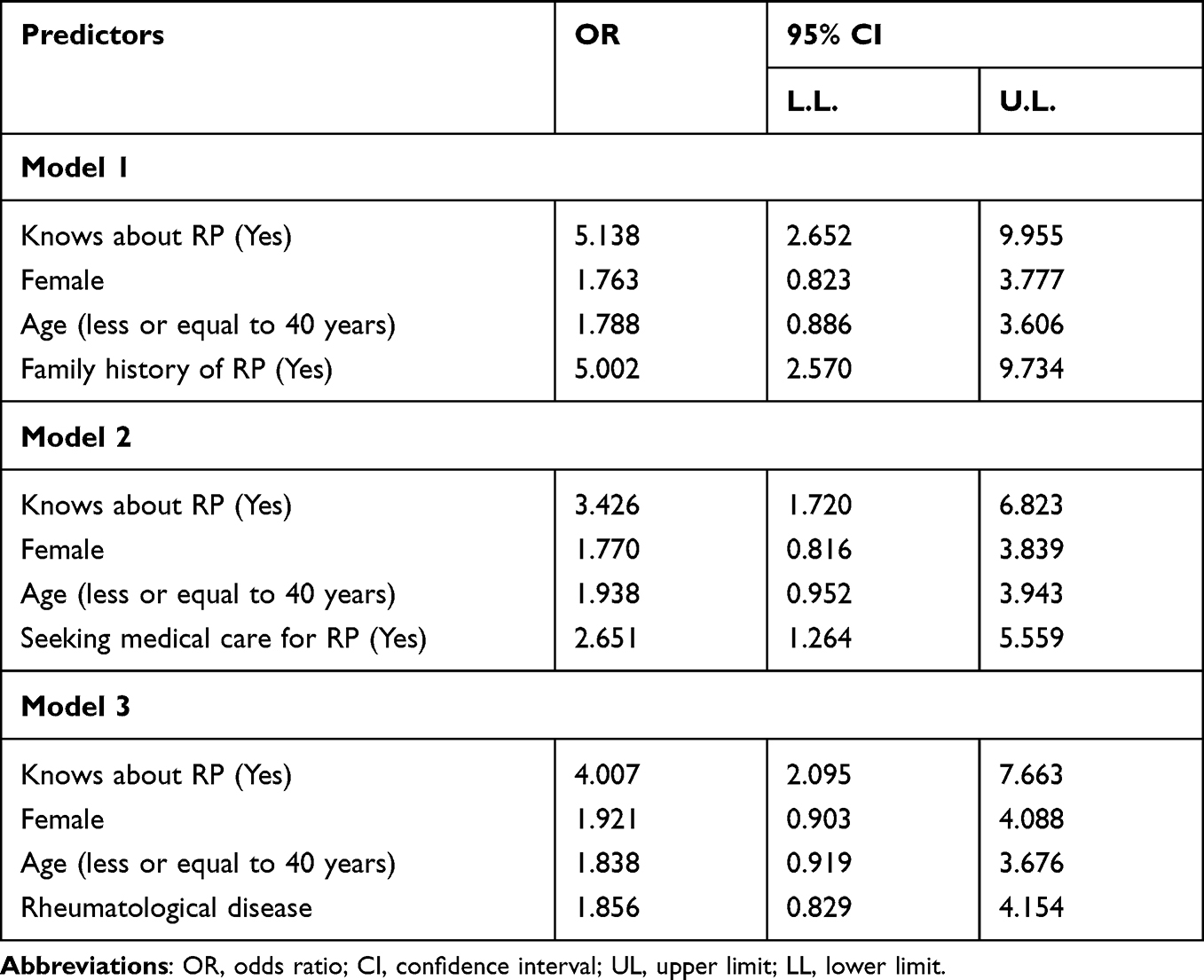 |
Table 3 Associations Between RP Diagnosis and Knowledge Using Multivariate Logistic Regression Models |
In model 1, participants who had knowledge about RP were 5 times more likely to have a diagnosis of RP after controlling for age, sex, and family history, with a 95% confidence interval of 2.65–9.95. After additionally controlling for repeated doctor visits (model 2) and association with other rheumatological diseases (model 3), participants with knowledge about RP were 3 and 4 times more likely to have a diagnosis of RP, resulting in a 95% confidence intervals of 1.72–6.82 and 2.09–7.66, respectively.
Discussion
This study aims to estimate the prevalence of RP and explore the level of awareness of RP in the general population in Saudi Arabia. The prevalence of RP was 4.29%, with a female predominance. Two-thirds of the study population lacked knowledge about RP. Only one-third of RP patients sought medical advice regarding their symptoms.
RP is underdiagnosed worldwide. There are no data about the disease in the Saudi Arabian general population. To our knowledge, our study is the first cross-sectional study to measure the prevalence and awareness of RP among the general Saudi Arabian population. Similarly, a local study performed on 747 medical students at Taibah University suggested that the prevalence of RP is 5.3%, with a higher incidence in women (81.2%).12 Another study in the region conducted on 1414 Turkish medical students revealed similar results (4.8%) and showed a positive correlation between smoking and RP, especially in women.20
The prevalence of RP in Saudi Arabia was consistent with that found in a meta-analysis and systematic review of 33 articles published in 2015 (4.85%).6 The majority of the articles (17 articles) in the meta-analysis used the same study design as our study. However, not all studies in the meta-analysis were conducted in regions with similar climates.6 This finding rejects the misconception that RP is not prevalent in regions with hot climates. Transitioning from very hot weather into an air-conditioned building is a common trigger among Saudi Arabian RP patients. As expected, women were more commonly affected.1,2,4,6–8,10–13,15,20 This finding is associated with the nature of the disease and might be attributed to high oestrogen levels.21
In our study, RP generally presented in the 3rd decade of life; hence, the analysis confirmed that 16 of the 44 patients (36.6%) with RP were between the ages of 21 and 40 years. A study in north western Greece found that the disease often presents in the 4th decade of life.22 This may be due to the difference in the average age of the population, which is older in Greece.23 Although some studies have found a positive correlation between RP and smoking, our data failed to show this association. This might be because only 21.2% in our collected sample were smokers. Finally, a study published in 1996 concluded that 14.3% of RP cases were due to secondary causes.24 However, our study demonstrated that different rheumatological diseases appeared to be responsible for approximately 20% of RP cases. This may be due to the development of new diagnostic methods, modalities, and improvements in diagnostic criteria over the past 20 years.
However, our study also showed that more than two-thirds of the participants who were classified as having RP had higher education levels. This might be explained by most of the study population (50%) being young or due to selection bias, as shown in Table 1, which indicates that 87% of the study population had a higher education level. We also found that more than half of the entire population does not clearly understand RP. This could indicate a lack of awareness of this disease. However, the results demonstrated that one-third of participants diagnosed with RP stated that they frequently visited doctors due to disturbing RP symptoms. The low percentage of doctor visits regarding RP symptoms can be attributed to the lack of awareness of the phenomenon as a disease or due to financial issues and barriers to accessing the health care system. This is supported by the fact that a large proportion of identified patients had an income of less than 5 K S.R. (Saudi Riyal), which is less than the average income of the Saudi Arabian population.25 Both factors, a higher education level and low personal income, can indirectly lead to a more stressful lifestyle that can exacerbate the disease. We have previously identified a lack of public awareness in other disease areas, such as SLE and rheumatoid arthritis (RA).26–28
This study has some notable limitations. It only gives an estimate of the prevalence of RP, as the gold standard of RP diagnosis is made clinically by a healthcare provider.29 Furthermore, our data collection phase of the research occurred during the COVID-19 pandemic; therefore, our methodology was designed within quarantine constraints. Consequently, our diagnosis findings were limited because they were self-reported based on the questionnaire, and clinical examinations and nail-fold capillary tests, which are the standard patient assessments, were not performed. In addition, due to the method used to complete the survey, most of those who answered the questionnaire were highly educated, which can be considered a selection bias. Despite the aforementioned limitations, our study identified a prevalence similar to the global data and identified characteristics of patients with self-reported RP. We also confirmed that awareness of the disease among the general population requires improvement through education. Future studies are required to confirm our findings through a second phase of confirmation and follow-up.
Conclusions
The prevalence of RP in Saudi Arabia was 4.29%, with most RP patients being women. More than half of the population does not have an adequate awareness of the disease. Only one-third of patients diagnosed with RP sought medical attention. This study demonstrates a lack of understanding of this disease. Further medical attention and awareness campaigns regarding RP are recommended.
Abbreviations
RP, Raynaud’s phenomenon; SSc, systemic sclerosis; SLE, systemic lupus erythematosus; SS, Sjögren’s syndrome; SSRIs, selective serotonin reuptake inhibitors; AIC, Akaike information criteria; K S.R, Kilo Saudi Riyal; RA, rheumatoid arthritis.
Ethics Approval and Informed Consent
This study was approved by the Department of Biomedical Ethics Unit & Academic Affairs of King Abdulaziz University, Jeddah (reference number 263-20). The participants’ consent was obtained by their voluntary completion of the survey.
Consent for Publication
Consent was obtained from participants by their voluntary completion of the survey.
Funding
All authors did not receive any financial support for this work. There is no financial relationship with any organization supporting this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Temprano KK. A review of Raynaud’s disease. Mo Med. 2016;113(2):123–126.
2. Prete M, Fatone MC, Favoino E, Perosa F. Raynaud’s phenomenon: from molecular pathogenesis to therapy. Autoimmun Rev. 2014;13(6):655–667. doi:10.1016/j.autrev.2013.12.001
3. Ho M, Belch JJ. Raynaud’s phenomenon: state of the art 1998. Scand J Rheumatol. 1998;27(5):319–322. doi:10.1080/03009749850154311
4. Flavahan NA. A vascular mechanistic approach to understanding Raynaud phenomenon. Nat Rev Rheumatol. 2015;11(3):146–158. doi:10.1038/nrrheum.2014.195
5. Nilsson T, Wahlström J, Burström L, de Souza RJ. Hand-arm vibration and the risk of vascular and neurological diseases-A systematic review and meta-analysis. PLoS One. 2017;12(7):e0180795. doi:10.1371/journal.pone.0180795
6. Garner R, Kumari R, Lanyon P, Doherty M, Zhang W. Prevalence, risk factors and associations of primary Raynaud’s phenomenon: systematic review and meta-analysis of observational studies. BMJ open. 2015;5(3):e006389–e006389. doi:10.1136/bmjopen-2014-006389
7. Chikura B, Moore T, Manning J, Vail A, Herrick AL. Thumb involvement in Raynaud’s phenomenon as an indicator of underlying connective tissue disease. J Rheumatol. 2010;37(4):783–786. doi:10.3899/jrheum.091117
8. Maverakis E, Patel F, Kronenberg DG, et al. International consensus criteria for the diagnosis of Raynaud’s phenomenon. J Autoimmun. 2014;48–49:60–65. doi:10.1016/j.jaut.2014.01.020
9. Lis-święty A. Recent advances in the workup and management of Raynaud phenomenon. Pol Arch Intern Med. 2019;129(11):798–808. doi:10.20452/pamw.15008
10. Weinrich MC, Maricq HR, Keil JE, McGregor AR, Diat F. Prevalence of Raynaud phenomenon in the adult population of south carolina. J Clin Epidemiol. 1990;43(12):1343–1349. doi:10.1016/0895-4356(90)90101-T
11. Riera G, Vilardell M, Vaque J, Fonollosa V, Bermejo B. Prevalence of Raynaud’s phenomenon in a healthy Spanish population. J Rheumatol. 1993;20(1):66–69.
12. Aljohani R, Abuzaid HI, Alhazmi RE, Sdaqir AA, Amer SM. Prevalence of primary Raynaud’s phenomena among healthy medical students in the western region of Saudi Arabia. Int J Med Develop Countries. 2020;706–710. doi:10.24911/IJMDC.51-1578239190
13. Palmer KT, Griffin MJ, Syddall H, Pannett B, Cooper C, Coggon D. Prevalence of Raynaud’s phenomenon in Great Britain and its relation to hand transmitted vibration: a national postal survey. Occup Environ Med. 2000;57(7):448–452. doi:10.1136/oem.57.7.448
14. Raosoft. The raosoft online sample size calculator. Available from: http://www.raosoft.com/samplesize.html.
15. Sanges S, Farhat M, Assaraf M, et al. Raising rare disease awareness using red flags, role play simulation and patient educators: results of a novel educational workshop on Raynaud phenomenon and systemic sclerosis. Orphanet J Rare Dis. 2020;15(1):1–10. doi:10.1186/s13023-020-01439-z
16. Vittinghoff E, Glidden DV, McCulloch CE, Shiboski SC. Regression Methods in Biostatistics.
17. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
18. StataCorp. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.
19. Elm EV, Altman DG, Egger M, Pocock SJ, Gotzche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335:806–808. doi:10.1136/bmj.39335.541782.AD
20. Çakır N, Pamuk ÖN, Dönmez S, et al. Prevalence of Raynaud’s phenomenon in healthy Turkish medical students and hospital personnel. Rheumatol Int. 2008;29(2):185–188. doi:10.1007/s00296-008-0666-9
21. Serizawa I, Iwasaki N, Ishida H, Saito S, Ishikawa T. G-protein coupled estrogen receptor-mediated non-genomic facilitatory effect of estrogen on cooling-induced reduction of skin blood flow in mice. Eur J Pharmacol. 2017;797:26–31. doi:10.1016/j.ejphar.2017.01.013
22. Voulgari PV, Alamanos Y, Papazisi D, Christou K, Papanikolaou C, Drosos AA. Prevalence of Raynaud’s phenomenon in a healthy Greek population. Ann Rheum Dis. 2000;59(3):206–210. doi:10.1136/ard.59.3.206
23. Plecher P. Greece - median age of the population 1950–2050. 2020:2020.
24. Hirschl M, Kundi M. Initial prevalence and incidence of secondary Raynaud’s phenomenon in patients with Raynaud’s symptomatology. J Rheumatol. 1996;23(2):302–309.
25. General Authority of Statistics. Household Income and Expenditure Survey. Riyadh: General Authority of Statistics; 2018.
26. Omair MA, Al Ohali SM, Abdulkarim FA, Madhi HA, Alghamdi LA. Awareness and misconceptions of female students in King Saud University on systemic lupus erythematosus. Rheumatology. 2015;5(3):165. doi:10.4172/2161-1149.1000165
27. Hazzazi AA, Ageeli MH, Muyidi AA, Abulgasim AM, Yateemi AA, Alhakami N. Population awareness about rheumatoid arthritis in Jazan region, Saudi Arabia. Int J Med Dev Countries. 2020;4(3):668–675. doi:10.24911/IJMDC.51-1576010943
28. Elhussein N, Ahmed RM, Elhussein N, et al. Awareness of rheumatoid arthritis among population in taif, Saudi Arabia awareness of rheumatoid arthritis among population in taif, Saudi Arabia. Indian J Appl Res. 2018;8(3):9–12.
29. Block JA, Sequeira W. Raynaud’s phenomenon. Lancet. 2001;357(9273):2042–2048. doi:10.1016/S0140-6736(00)05118-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.