")
Back to Journals » Journal of Pain Research » Volume 15
Prevalence of Pain and Its Risk Factors Among ICU Personnel in Tertiary Hospital in China: A Cross-Sectional Study
Authors Wang M , Ding Q, Sang L , Song L
Received 15 March 2022
Accepted for publication 13 June 2022
Published 20 June 2022 Volume 2022:15 Pages 1749—1758
DOI https://doi.org/10.2147/JPR.S366536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Maoying Wang,1,* Qianrong Ding,2,* Ling Sang,1 Li Song1
1Department of Pain Management, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 2Department of Intensive Care Unit Management, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Song, Department of Pain Management, West China Hospital, Sichuan University, West China Hospital, Sichuan University, #37, Guo Xue Xiang, Chengdu, Sichuan Province, 610041, People’s Republic of China, Tel +8618980601501, Fax +8602885423593, Email [email protected]
Background: Although pain is commonly observed among medical staff, studies on pain among intensive care unit personnel are uncommon, especially intensive care unit (ICU) doctors and workers. Moreover, few studies have focused on the prevalence of pain and the associated factors.
Purpose: The aim of this study was to estimate the prevalence of pain among ICU personnel (including doctors, nurses and workers) and explore the risk factors for their pain.
Methods: We conducted an online survey that included sociodemographic and work-related items and questions about pain, ergonomics, and psychological factors. We used the short version of the validated Depression–Anxiety–Stress Scale (DASS-21) to assess the relationship between pain and mental disorders. All ICU personnel at West China Hospital of Sichuan University participated in this study.
Results: A total of 356 ICU personnel were included in the final analysis. The prevalence of pain was 72.2% among ICU nurses, 64.4% among ICU doctors and 52.9% among ICU workers. The most frequent location of pain was the lower back among nurses (65.9%) and workers (47.1%) and the neck among doctors (49.1%). The factors contributing to pain among ICU personnel were bending or twisting the neck, high levels of psychological fatigue, low self-perceived health status, female sex and high body mass index (BMI). Moreover, participants with pain indicated significantly higher depression (p ≤ 0.001), anxiety (p ≤ 0.001), and stress levels (p = 0.002) than those without pain.
Conclusion: This study indicates that ICU personnel exhibit a high prevalence of pain. Many factors, especially psychosocial and ergonomic factors, contribute to pain levels among ICU personnel and the poorer mental health levels observed in those experiencing pain. Therefore, disease prevention and health promotion measures are needed to protect the health of ICU personnel.
Keywords: occupational health, intensive care unit, cross-sectional studies, mental health
Introduction
An intensive care unit (ICU) provides rescue and treatment for critically ill patients, and the workers in this environment are exposed to the highest occupational risk in terms of ergonomic injuries.1 According to previous reports, ICU personnel experience more work-related musculoskeletal disorders (WRMDs) than do the medical staff of other wards.2 WRMDs are common among health care workers and defined as musculoskeletal disorders caused by work-related events.3 WRMDs rarely lead to life-threatening conditions, but they can significantly impact one’s quality of life,4 cause losses of labor time or increases in absenteeism, increase work restrictions,5 and increase the financial burden on the individual, organization and society.6
For ICU personnel, especially nurses, WRMDs are a major occupational health problem associated with physical and psychosocial factors, such as long periods of standing, heavy workloads, shift work, caring for patients with comorbidities, frequent emergency conditions and deaths,7 which increase ICU personnel susceptibility to WRMDs.8 In China, approximately 97% of ICU nurses experienced at least one WRMD within the previous year.9 In Turkey, data from 51 ICUs showed that a considerably high proportion (95.9%) of 323 ICU nurses reported experiencing WRMDs and revealed that the areas with the highest prevalence of musculoskeletal symptoms were the legs, lower back and back.8 In contrast, few studies have reported on the prevalence of head and abdomen pain in ICU personnel. In East Asia (China, Japan, and South Korea), a high prevalence of migraines is observed, with 11–20% of women and 6.0% of men in the general population,10 and although this issue is worthy of further study, it has received limited attention. In the ICU, nurses are frequently required to push, pull, elevate and bend their patients, sometimes with the help of workers, while doctors are primarily responsible for the management of patients. Although these features of working in an ICU might contribute to variations in the experience of pain among ICU personnel, the prevalence of pain among doctors and workers is poorly understood.
In addition to musculoskeletal diseases, medical staff are frequently diagnosed with mental health issues.11–13 Fangqiong Tian’s research suggested that the incidence of fatigue among Chinese physicians was 83.70%.11 In a study of 558 Poland registered nurses, as many as 77.1% described their perceived overall level of stress caused by work as very high.12 A study in 2007 demonstrated that 46.5% of critical care physicians and 30% of critical care nurses were at risk for burnout.13 The intense environment of the ICU leads to higher demands for physical strength and mental stability among medical staff.9 However, ICU personnel may also suffer from pain resulting from mental issues, and this effect is not well known.
The objective of this study was to investigate the prevalence of pain in different work positions and identify factors related to pain, including individual, physical and psychosocial factors, among ICU personnel at West China Hospital of Sichuan University.
Materials and Methods
Methods
The cross-sectional survey period lasted for 4 weeks from January to February 2022. The Research Ethics Committee of West China Hospital of Sichuan University approved the research procedures before the study commenced. The online survey was anonymous, and informed consent was obtained when participants accessed the online link. The study was conducted in accordance with the Declaration of Helsinki.
Participants
According to the prevalence of musculoskeletal disease, the quantity of independent variables in the logistic regression and the response rate, we included all ICU personnel from West China Hospital (including doctors, nurses and workers); we only excluded those workers who refused to participate in the study. West China Hospital of Sichuan University is the largest tertiary hospital in Western China, and 356 valid questionnaires were ultimately included in the analysis.
Questionnaire
The survey was conducted in the form of an online questionnaire that was developed using Chinese-based questionnaire software powered by www.wjx.cn (a platform providing functions equivalent to those provided by Amazon Mechanical Turk). The software generated an online link and a quick-response 2D image code, which was scanned by the WeChat app on a mobile device by participants to access and complete the questionnaire. The questionnaires contained required fields to prevent incomplete responses, and each WeChat account was only allowed to fill in the questionnaire once.
The research questionnaire consisted of three sections. Section 1 addressed demographic information, as well as job-related questions, including age, gender, height, weight, marital status, smoking, shift work, work profession (doctors, nurses or workers), and work experience in the ICU. In addition, ergonomic factors mainly derived from the Chinese version of the Dutch Musculoskeletal Questionnaire were also introduced in the questionnaire.14 Section 2 contained questions about pain level according to previously described methods.15 All research participants needed to answer the following question: “Do you have any pain?” The answer options were as follows: “No”, “Yes, acute pain”, and “Yes, chronic pain (defined as pain for 3 months or longer)”. Only participants who claimed to have pain were then asked to identify the location and severity of their pain. We used a numeric rating scale (NRS) ranging from 1 to 10 to assess the severity of pain (≥1 and <4 equal to mild pain, ≥4 and <7 equal to moderate pain, and ≥7 and ≤10 equal to severe pain). In addition, research participants with pain were also asked if they took any analgesic measures. In the third and last section, all research participants were asked to address psychosocial factors based on the short version of the Depression–Anxiety–Stress–Survey (DASS-21), which consists of 21 items and has shown good reliability and validity. Depending on the scores, the responses were divided into normal, mild, moderate, severe, very severe depression, anxiety and stress levels.16–18 We used the validated Chinese version of the DASS-21 for this study, and we collected information related to the participants’ job satisfaction (low, medium, high), psychological fatigue (low, medium, and high) and self-perceived health status (very good, generally good, generally bad, and very bad).
Statistical Analysis
Data analysis was performed with SPSS 25.0. The mean, standard deviation and percentages were used to describe the data. Differences between participant groups were tested using independent samples t-tests, chi-square tests, or rank-sum tests. The relationship between individual, physical, and psychological factors and pain was first validated by univariate logistic regression analysis. According to the number of independent variables and the number of samples with pain, we included those with values of p≤0.2 in the univariate analysis in the multivariate logistic regression analysis. ORs and 95% CIs were calculated to evaluate the effect of risk factors on pain. The statistical significance was set at a level of P<0.05.
Results
A total of 361 ICU personnel (257 nurses, 87 doctors and 17 workers) completed our questionnaire, and the response rate was 90.7%. Five nurses were excluded from the sample because they provided inconsistent or nonlogical answers. Therefore, the final number of valid questionnaires included in the analysis was 356, including 252 nurses, 87 doctors and 17 workers. The mean age of ICU nurses was 25.9±5.1 years, which was younger than that of ICU doctors (33.8±5.9; p<0.001) and ICU workers (44.3±6.0; p<0.001). The proportion of females was higher among nurses (80.2%) than doctors (55.2%; p<0.001). Fewer nurses were married (57.5%) than were doctors (75.9%; p=0.002) and workers (100%; p=0.001). Regarding ergonomic factors, nurses were exposed to a higher percentage of these factors than were doctors, such as walking for long periods of time and the frequency of bending at the trunk, heavy or awkward lifting, and bending or twisting of the neck (p<0.001 in all the factors above). Significant differences were not observed among the three groups in terms of their smoking status, ICU personnel work experience, or shift work experience (Table 1).
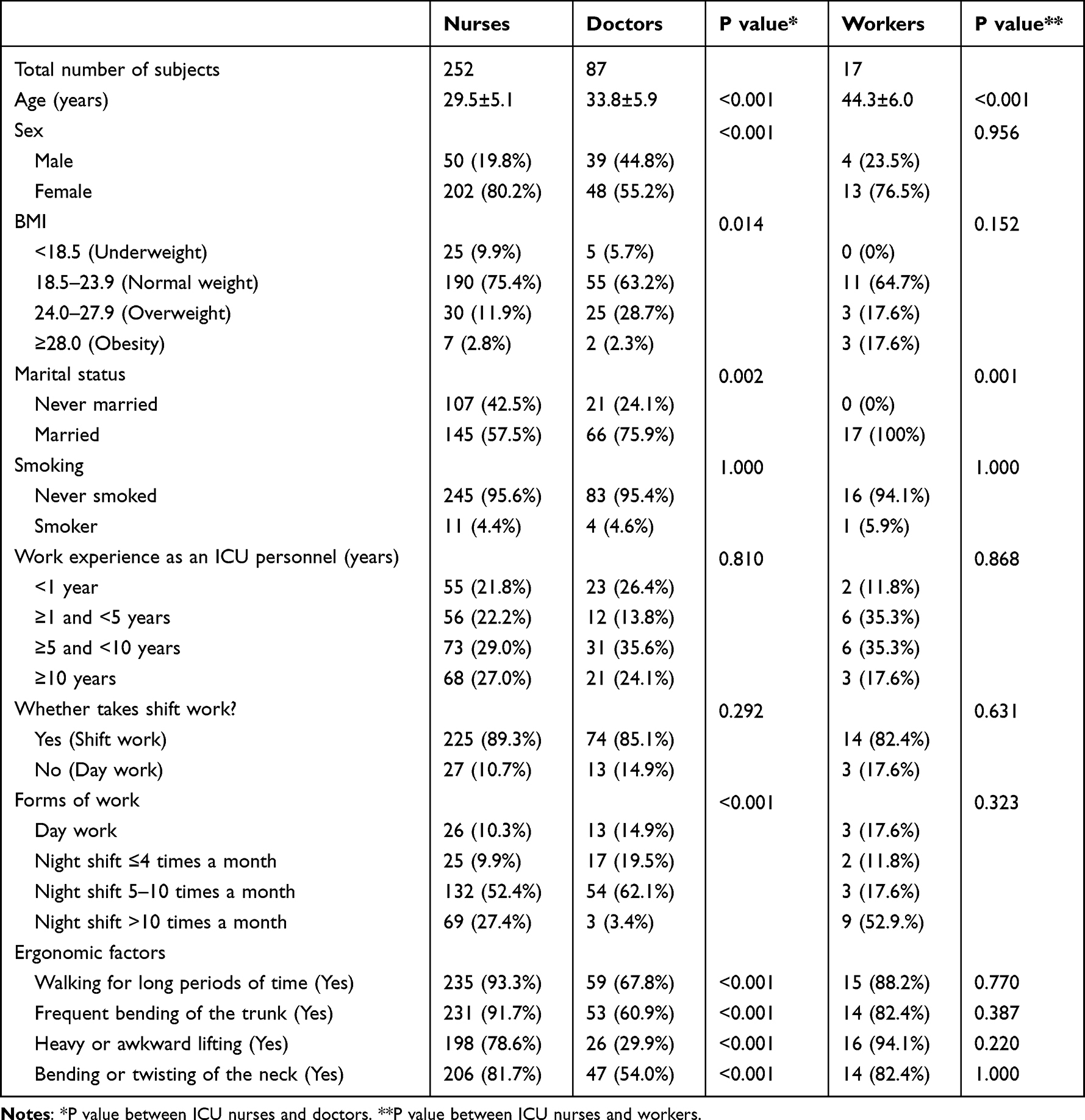 |
Table 1 Characteristics of Medical Staff in the Intensive Care Unit |
The prevalence of pain was 72.2% among nurses, 64.4% among doctors and 52.9% among workers, and there were no significant differences found among the groups. Among ICU personnel who had pain, the prevalence of chronic pain was 78.6% among nurses, 85.7% among doctors and 100% among workers; however, significant differences were not observed among the nurse, doctor and worker groups. The most frequent locations of pain were the lower back among nurses (65.9%) and workers (47.1%) and the neck among doctors (49.1%). Significant differences in the frequency of pain in the low back (65.9% vs 43.7%; p=0.001), shoulder (37.7% vs 24.1%; p=0.022) and lower limbs (40.5% vs 17.2%; p<0.001) were observed between ICU nurses and doctors. Similarly, significant differences in the frequency of pain in the upper back (25.0% vs 0.00%; p=0.039) were observed between ICU nurses and workers. Most of the ICU nurses (46.4%) indicated that their pain severity was mild, while most of the ICU doctors (33.3%; P=0.004) and workers (29.4%; P=0.02) indicated that their pain severity was moderate. The rates of analgesic treatment measures used by nurses, doctors and workers were 44.0%, 41.1% and 66.7%, respectively, and the pain control satisfaction rates of nurses, doctors and workers were 36.8%, 35.7% and 22.2%, respectively (Table 2). In terms of the DASS-21, the rank-sum test revealed significant differences among all three subscales (depression, anxiety and stress scale) when the pain and nonpain groups were compared (Table 3).
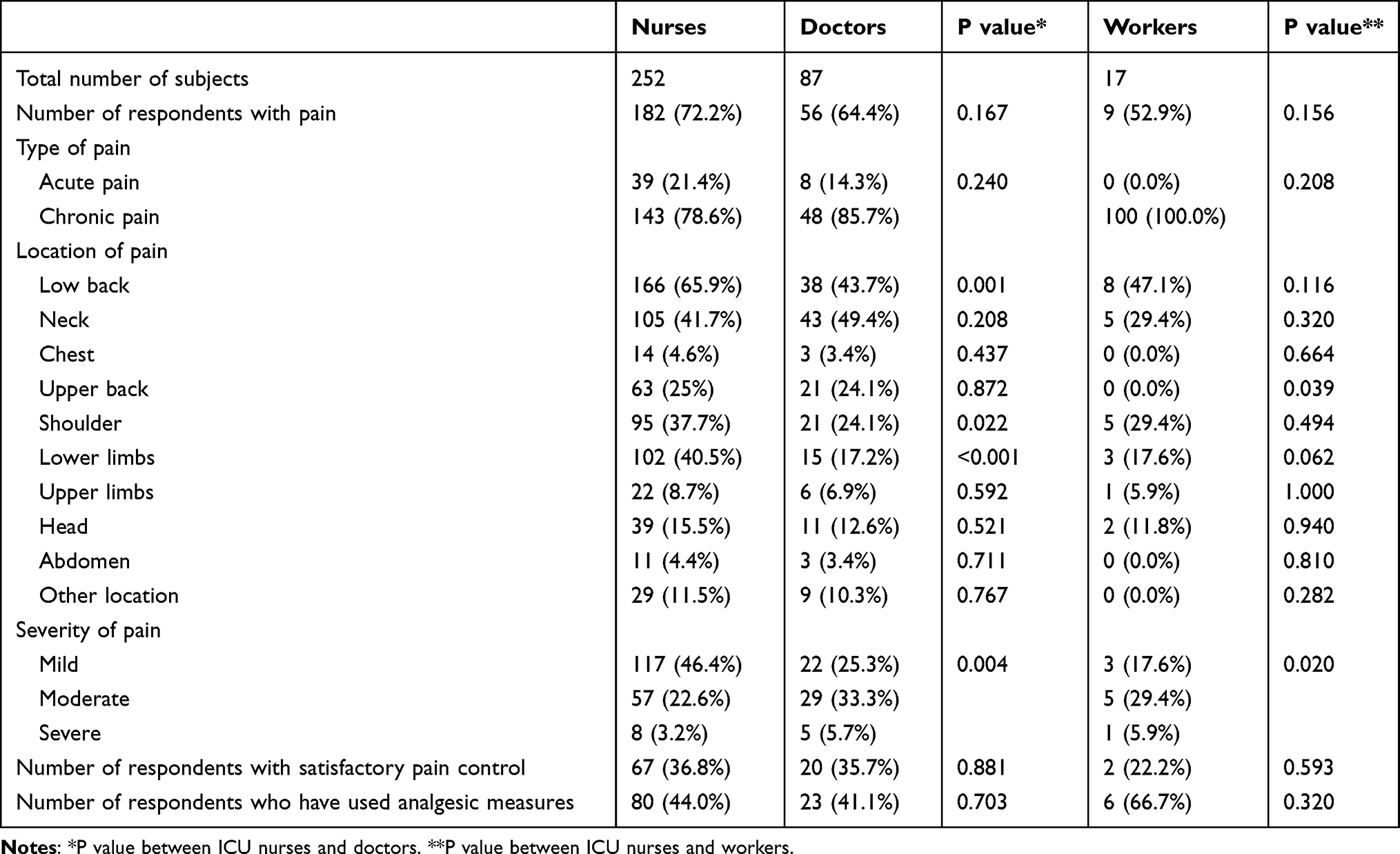 |
Table 2 Pain Characteristics of Medical Staff in the Intensive Care Unit |
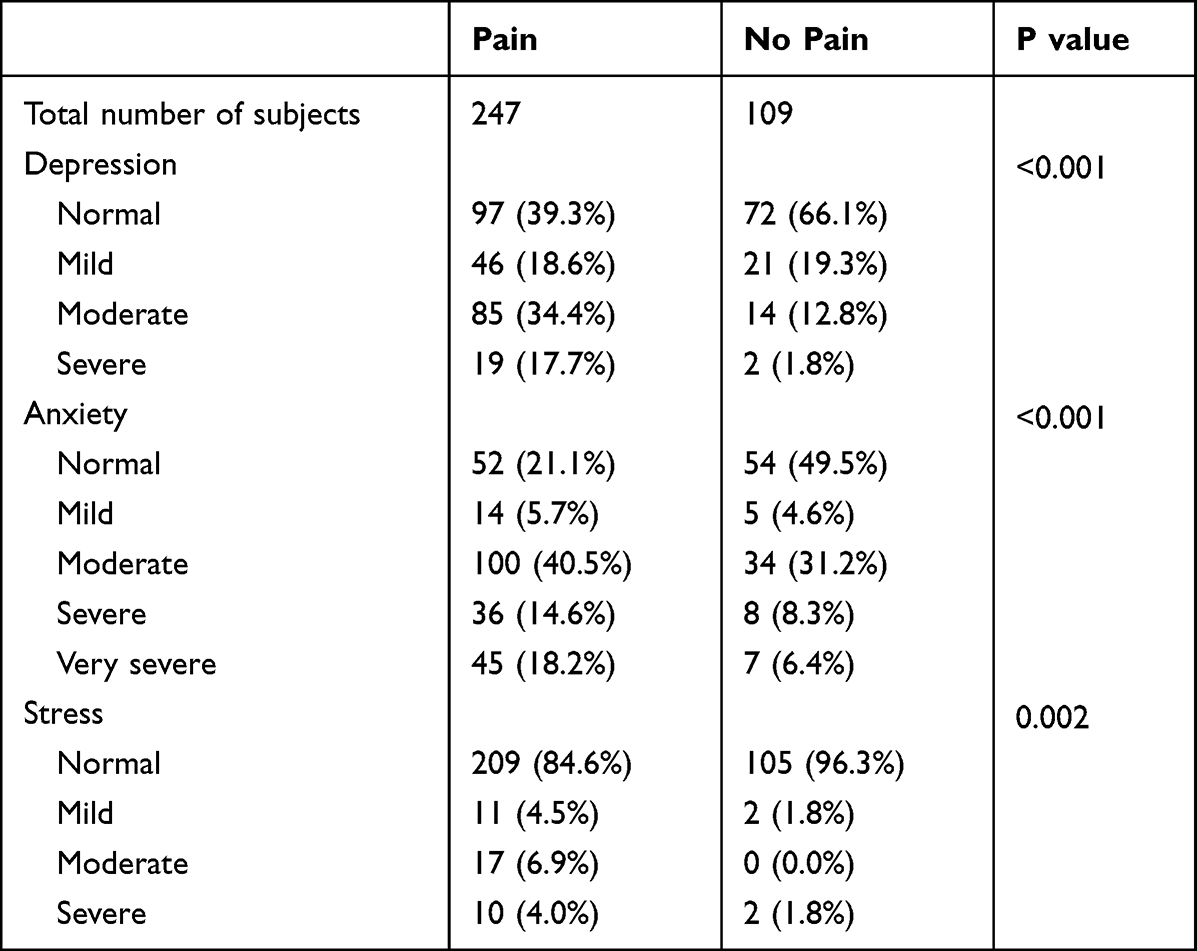 |
Table 3 DASS-21 Subscale Scores of Medical Staff in the Intensive Care Unit |
In the univariate regression analysis, sex, BMI, marital status, and ICU work experience were associated with pain level among ICU personnel. Regarding ergonomic factors, the frequent bending of the trunk, heavy or awkward lifting and bending or twisting of the neck were all statistically associated with pain. The univariate analysis also showed that job satisfaction, psychological fatigue and self-perceived health status were all associated with pain, while the multivariate logistic regression analysis revealed that sex, BMI, bending or twisting of the neck, psychological fatigue and self-perceived health status were independently associated with pain among ICU personnel (Table 4).
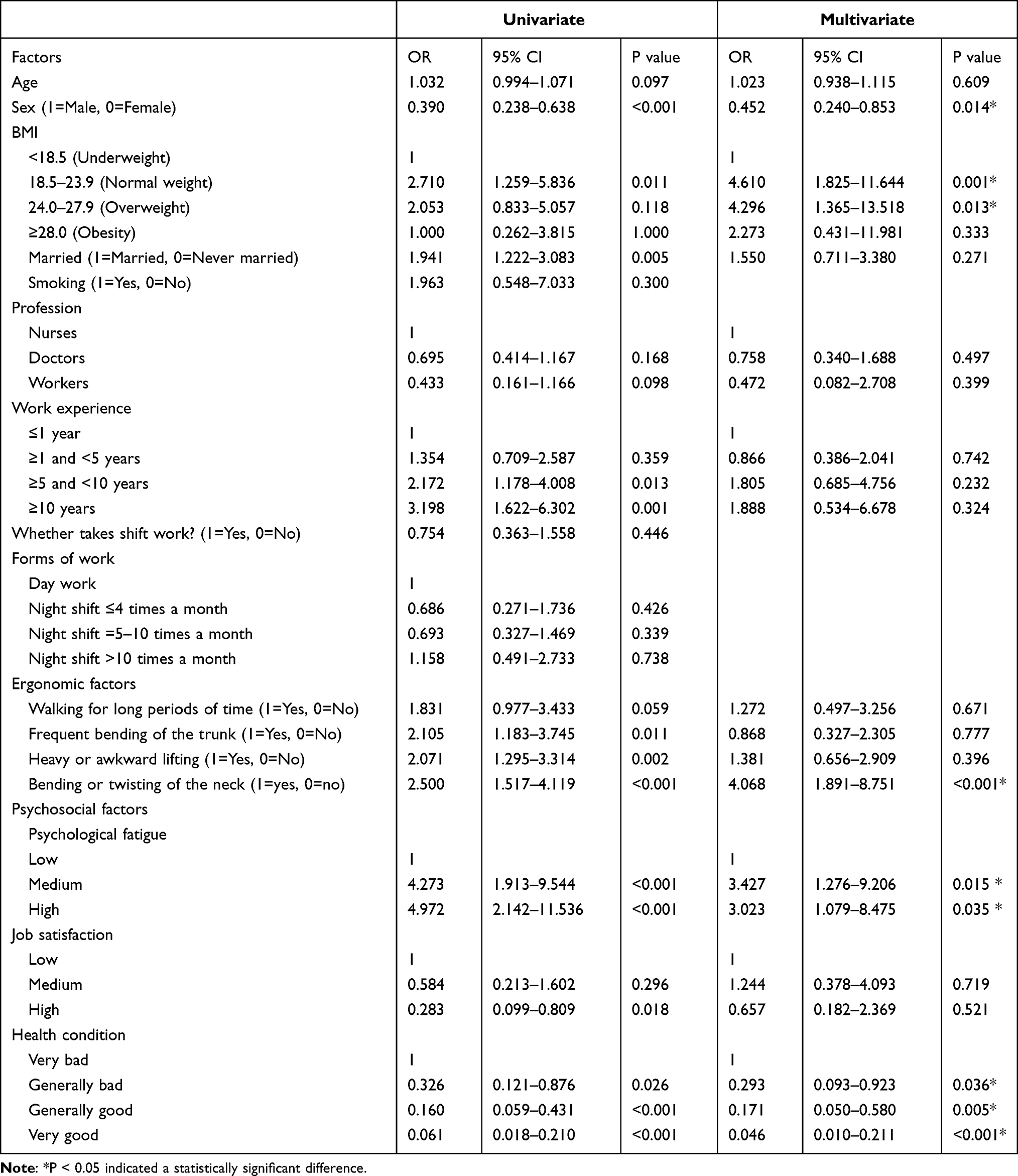 |
Table 4 Univariate and Multivariate Logistic Regression Analyses of Pain Risk Factors Among ICU Personnel |
Discussion
This study indicates that ICU personnel have a high prevalence of pain, with 72.7%, 64.4%, and 52.9% of ICU nurses, ICU doctors, and ICU workers reporting pain, respectively. The lower back and neck were frequently affected regions, which is consistent with reports from Hunan9 and Xinjiang19 (China), Malaysia,20 Nigeria21 and Iran.22 The salient point is that although almost half of the affected individuals reported using analgesic measures for treatment (44.0%, 41.1% and 66.7% of nurses, doctors and workers, respectively), the level of pain control satisfaction was low (36.8%, 35.7% and 22.2% of nurses, doctors and workers, respectively). We also found that those with pain had higher depression, anxiety, and stress levels. The risk factors for ICU personnel pain were individual factors (female sex and high BMI), ergonomic factors (bending or twisting of the neck) and psychosocial factors (high levels of psychological fatigue and low levels of self-perceived health status).
Reports indicate that the prevalence of lower back pain among ICU nurses worldwide over the last year ranged from 34.5%22 to 100%,21,23 with nursing positions in critical care units requiring considerably higher levels of physical exertion, such as long periods of standing for hours, heavy workloads, shift work, patients with complex health problems, and frequent emergency conditions and death; thus, the risk level of ICU nurses is much higher than that of nurses who work in other units.8 Moreover, limited data are available on the pain levels experienced by ICU doctors and workers worldwide. In our study, the prevalence of lower back pain was 65.9% among ICU nurses, 43.7% among doctors, and 47.1% among workers, thus indicating a high prevalence level among nurses, as well as doctors and workers. Consequently, ICU doctors and workers should receive greater attention in terms of pain. Previous studies have generally focused on musculoskeletal pain; however, our study also included the presence of head and abdomen pain. The prevalence of head pain among ICU personnel was 15.5% among ICU nurses, 12.6% among ICU doctors and 11.8% among ICU workers; these values are comparable to those found among the general East Asian population10 and undergraduate nursing students in Hong Kong;24 Thus, this issue warrants further attention.
We found that bending or twisting of the neck was associated with pain and that the neck was the main body location where ICU doctors reported feeling pain. As doctors and nurses use computers more widely in hospitals, ergonomic factors such as computer use posture, the suitability of computer tables and chairs, and mouse features have had increasingly serious effects on neck and shoulder pain.25 ICU nurses also frequently twist their necks to pay attention to monitors. Similarly, doctors and nurses in critical care units hold their neck and shoulders in a fixed position for a long time, which can lead to fatigue and pain.26 In our study, the frequent bending of the trunk and heavy or awkward lifting was significantly associated with pain in the univariate analysis, although this association was not found in the multivariate logistic regression analysis. This change in outcome is probably because the ICU personnel as a group work together to turn over and transport patients, especially nurses and workers, and this cooperation attenuates the effect of frequently bending one’s trunk and heavy or awkward lifting on pain level among ICU personnel. In addition, suitable personal protection methods are not currently available for neck and shoulder pain among ICU personnel.
Psychosocial factors (high levels of psychological fatigue and low levels of self-perceived health status) have also been shown to be associated with pain in ICU personnel. This finding indicates that ICU personnel who were dissatisfied with their health status were more prone to complain about pain. High levels of psychological fatigue could negatively impact a person’s physical and mental health at work and increase the possibility of injury among medical staff.27–30 Regarding pain level among a special occupational group, the same result has been observed. A study of 4500 Iranian industrial workers showed that psychosocial factors at work, such as fatigue and stress, largely contributed to the development of lower back pain.31 The health of medical staff may affect the safety of patients through medical errors, thereby increasing the risk of hospital-associated infection transmission.32–35
In addition, our study also showed that ICU personnel with pain had significantly higher levels of depression, anxiety and stress than did participants who reported having no pain. Previous reports have indicated that pain and depression are related in terms of brain regions and neurological function systems and that pain relief may relieve depression and vice versa.36,37 These findings illustrate a potential link between mental health and pain. However, we must take into account that other factors in addition to pain also affect mental health. Since December 2019, coronavirus disease 2019 (COVID-19) has become a global pandemic,38 which has introduced additional psychological burdens for ICU personnel, including fear of being infected, inability to rest, inability to care for one’s family, struggling with difficult emotions, witnessing more frequent end-of-life decisions, and making difficult ethical decisions.39 A previous study revealed that a high percentage (94.4%) of frontline medical workers working in COVID-19 treatment centers had negative emotional reactions.40 Both the COVID-19 pandemic and the critical care setting are situations that present high levels of psychological risks for health care providers.39 Our findings encourage clinicians and occupational health staff to identify these mental health issues early to reduce the level of pain-related problems for ICU personnel.
We also found that sex and BMI are associated with pain. Regarding BMI, this finding is consistent with a previous study showing that BMI is positively associated with musculoskeletal pain.41 Epidemiological studies have linked high BMI to pain; however, these studies have not provided any factors to explain this association. Moreover, our study showed that female sex is a risk factor for pain, which is consistent with previous findings indicating the important role of sex in pain reporting.42,43 The influence of sex is expected because women are smaller in stature and have less muscle strength than men, and more physically demanding occupations correspond to a higher risk of pain.44 To reduce pain among ICU personnel, a multifactorial approach that includes ergonomic and psychosocial interventions should be considered in the future.
As with every study, our work had some limitations. First, we used self-reported measures and retrospective questionnaires. To obtain accurate results, honest responses from the participants were necessary. Second, our study sample was small (n=356), mainly due to the low number of workers. Our study is not necessarily representative of all ICU personnel in China, and more research is needed to determine a more accurate prevalence of pain and its risk factors. Third, participants completing the DASS-21 scale may have been currently suffering from or suffered pain in the past; however, this test can only reflect the mental health situation of the participants at the time they completed the scale questions. We could not determine the causal relationship between pain and anxiety, depression, and stress, and we only included the DASS-21 responses in the difference analysis but not the regression analysis; all of which are further limitations of our research. Last, it is necessary to conduct a prospective cohort study design with a larger sample size in the future to provide more reliable research evidence for pain among medical staff in China.
Conclusion
This study reveals the high prevalence of pain among ICU personnel. Psychosocial factors, such as psychological fatigue, and ergonomic factors, such as bending or twisting the neck, play important roles in the development of pain. In addition, ICU personnel with pain have significantly higher rates of positivity for mental disorders. However, whether their pain is the main cause of their increased levels of depression, anxiety or stress has not been clarified. Thus, measures are needed to prevent musculoskeletal and psychiatric disorders and to ensure the health of ICU personnel.
Ethics Approval
The study was approved by the ethics committees at West China Hospital (approval number: 1017/2021).
Acknowledgments
The authors thank all the ICU personnel who participated in the study at West China Hospital of Sichuan University. All their help is truly appreciated.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Sichuan Science and Technology program, grant number: 2020YFS0188. The funding sources were involved in the conduct of the study and development of the submission.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Freimann T, Merisalu E, Pääsuke M. Effects of a home-exercise therapy programme on cervical and lumbar range of motion among nurses with neck and lower back pain: a quasi-experimental study. BMC Sports Sci Med Rehabil. 2015;7:31. doi:10.1186/s13102-015-0025-6
2. Black TR, Shah SM, Busch AJ, et al. Effect of transfer, lifting, and repositioning (TLR) injury prevention program on musculoskeletal injury among direct care workers. J Occup Environ Hyg. 2011;8(4):226–235. doi:10.1080/15459624.2011.564110
3. Salik Y, Ozcan A. Work-related musculoskeletal disorders: a survey of physical therapists in Izmir-Turkey. BMC Musculoskelet Disord. 2004;5:27. doi:10.1186/1471-2474-5-27
4. Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol. 2004;14(1):13–23. doi:10.1016/j.jelekin.2003.09.015
5. Bernardelli G, Vigna L, Nava C, et al. Physical activity in healthcare workers with low back pain: effects of the Back-FIT randomized trial. J Occup Environ Med. 2020;62(6):e245–e249. doi:10.1097/JOM.0000000000001844
6. Kemmlert K. Prevention of occupational musculo-skeletal injuries. labour inspectorate investigation. Scand J Rehabil Med Suppl. 1996;35(35):1–34. doi:10.1016/S0891-4222(96)90015-3
7. AACN. Scope and standards for progressive and critical care nursing practice. Available from: https://www.aacn.org/~/media/aacn-website/nursing-excellence/standards/aacn-scope-and-standards-for-progressive-and-critical-care-nursing-practice.pdf.
8. Sezgin D, Esin MN. Predisposing factors for musculoskeletal symptoms in intensive care unit nurses. Int Nurs Rev. 2015;62(1):92–101. doi:10.1111/inr.12157
9. Yang S, Lu J, Zeng J, et al. Prevalence and risk factors of work-related musculoskeletal disorders among intensive care unit nurses in China. Workplace Health Saf. 2019;67(6):275–287. doi:10.1177/2165079918809107
10. Takeshima T, Wan Q, Zhang Y, et al. Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J Headache Pain. 2019;20(1):111. doi:10.1186/s10194-019-1062-4
11. Tian F, Shu Q, Cui Q, et al. The mediating role of psychological capital in the relationship between occupational stress and fatigue: a cross-sectional study among 1104 Chinese physicians. Front Public Health. 2020;8:12. doi:10.3389/fpubh.2020.00012
12. Kowalczuk K, Krajewska-Kułak E, Sobolewski M. The effect of subjective perception of work in relation to occupational and demographic factors on the mental health of Polish nurses. Front Psychiatry. 2020;11:591957. doi:10.3389/fpsyt.2020.591957
13. Malaquin S, Mahjoub Y, Musi A, et al. Burnout syndrome in critical care team members: a monocentric cross sectional survey. Anaesth Crit Care Pain Med. 2017;36(4):223–228. doi:10.1016/j.accpm.2016.06.011
14. Hildebrandt VH, Bongers PM, van Dijk FJ, et al. Dutch musculoskeletal questionnaire: description and basic qualities. Ergonomics. 2001;44(12):1038–1055. doi:10.1080/00140130110087437
15. Möckel L, Gerhard A, Mohr M, et al. Prevalence of pain, analgesic self-medication and mental health in German pre-hospital emergency medical service personnel: a nationwide survey pilot-study. Int Arch Occup Environ Health. 2021;94(8):1975–1982. doi:10.1007/s00420-021-01730-x
16. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-u
17. Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(Pt 2):227–239. doi:10.1348/014466505X29657
18. Nilges P, Essau C. Depression, anxiety and stress scales: DASS–A screening procedure not only for pain patients. Schmerz. 2015;29(6):649–657. doi:10.1007/s00482-015-0019-z
19. Yan P, Yang Y, Zhang L, et al. Correlation analysis between work-related musculoskeletal disorders and the nursing practice environment, quality of life, and social support in the nursing professionals. Medicine. 2018;97(9):e0026. doi:10.1097/MD.0000000000010026
20. Krishnan KS, Raju G, Shawkataly O. Prevalence of work-related musculoskeletal disorders: psychological and physical risk factors. Int J Environ Res Public Health. 2021;18:17. doi:10.3390/ijerph18179361
21. Bolarinde SO, Oyewole I, Abobarin AF. Work-related musculoskeletal disorders among nurses in various specialty areas in a Nigerian tertiary health institution. J Emerg Pract Trauma. 2019;5(2):41–46. doi:10.15171/JEPT.2019.04
22. Arsalani N, Fallahi-Khoshknab M, Josephson M, et al. Musculoskeletal disorders and working conditions among Iranian nursing personnel. Int J Occup Saf Ergon. 2014;20(4):671–680. doi:10.1080/10803548.2014.11077073
23. Akodu AK, Ashalejo ZO. Work-related musculoskeletal disorders and work ability among hospital nurses. J Taibah Univ Med Sci. 2019;14(3):252–261. doi:10.1016/j.jtumed.2019.02.009
24. Xie YJ, Lin M, Wong YT, Yan L, Zhang D, Gao Y. Migraine attacks and relevant trigger factors in undergraduate nursing students in Hong Kong: a cross-sectional study. J Pain Res. 2022;15:701–713. doi:10.2147/JPR.S337465
25. Lin SC, Lin LL, Liu CJ, et al. Exploring the factors affecting musculoskeletal disorders risk among hospital nurses. PLoS One. 2020;15(4):e0231319. doi:10.1371/journal.pone.0231319
26. Halim I, Omar AR. Development of prolonged standing strain index to quantify risk levels of standing jobs. Int J Occup Saf Ergon. 2012;18(1):85–96. doi:10.1080/10803548.2012.110769172
27. Gander P, O’Keeffe K, Santos-Fernandez E, et al. Fatigue and nurses’ work patterns: an online questionnaire survey. Int J Nurs Stud. 2019;98:67–74. doi:10.1016/j.ijnurstu.2019.06.011
28. Hatch DJ, Freude G, Martus P, et al. Age, burnout and physical and psychological work ability among nurses. Occup Med. 2018;68(4):246–254. doi:10.1093/occmed/kqy033
29. Barker LM, Nussbaum MA. The effects of fatigue on performance in simulated nursing work. Ergonomics. 2011;54(9):815–829. doi:10.1080/00140139.2011.597878
30. Silva T, Araújo WN, Stival MM, et al. Musculoskeletal discomfort, work ability and fatigue in nursing professionals working in a hospital environment. Rev Esc Enferm USP. 2018;52:e03332. doi:10.1590/S1980-220X2017022903332
31. Ghaffari M, Alipour A, Farshad AA, et al. Effect of psychosocial factors on low back pain in industrial workers. Occup Med. 2008;58(5):341–347. doi:10.1093/occmed/kqn006
32. Hugonnet S, Harbarth S, Sax H, et al. Nursing resources: a major determinant of nosocomial infection? Curr Opin Infect Dis. 2004;17(4):329–333. doi:10.1097/01.qco.0000136931.83167.d2
33. Hugonnet S, Villaveces A, Pittet D. Nurse staffing level and nosocomial infections: empirical evaluation of the case-crossover and case-time-control designs. Am J Epidemiol. 2007;165(11):1321–1327. doi:10.1093/aje/kwm041
34. Rogers AE, Hwang WT, Scott LD, et al. The working hours of hospital staff nurses and patient safety. Health Aff. 2004;23(4):202–212. doi:10.1377/hlthaff.23.4.202
35. Virtanen M, Kurvinen T, Terho K, et al. Work hours, work stress, and collaboration among ward staff in relation to risk of hospital-associated infection among patients. Med Care. 2009;47(3):310–318. doi:10.1097/MLR.0b013e3181893c64
36. Sheng J, Liu S, Wang Y, et al. The link between depression and chronic pain: neural mechanisms in the brain. Neural Plast. 2017;2017:9724371. doi:10.1155/2017/9724371
37. Angst F, Benz T, Lehmann S, et al. Extended overview of the longitudinal pain-depression association: a comparison of six cohorts treated for specific chronic pain conditions. J Affect Disord. 2020;273:508–516. doi:10.1016/j.jad.2020.05.044
38. Johns Hopkins University and Medicine: Coronavirus Resource Center. COVID-19 data in motion. Available from: https://coronavirus.jhu.edu/.
39. Azoulay E, Cariou A, Bruneel F, et al. Symptoms of anxiety, depression, and peritraumatic dissociation in critical care clinicians managing patients with COVID-19. A cross-sectional study. Am J Respir Crit Care Med. 2020;202(10):1388–1398. doi:10.1164/rccm.202006-2568OC
40. Kebede MA, Demissie DB, Bitew ZW, et al. Emotional responses and perceived stressors of frontline medical staffs in case of COVID-19 treatment centers and obstetrics emergency in Ethiopia. BMC Psychiatry. 2021;21(1):308. doi:10.1186/s12888-021-03311-1
41. Viester L, Verhagen EA, Oude Hengel KM, et al. The relation between body mass index and musculoskeletal symptoms in the working population. BMC Musculoskelet Disord. 2013;14:238. doi:10.1186/1471-2474-14-238
42. Sugano A, Nomura T. Influence of water exercise and land stretching on salivary cortisol concentrations and anxiety in chronic low back pain patients. J Physiol Anthropol Appl Human Sci. 2000;19(4):175–180. doi:10.2114/jpa.19.175
43. Smith DR, Leggat PA. Musculoskeletal disorders among rural Australian nursing students. Aust J Rural Health. 2004;12(6):241–245. doi:10.1111/j.1440-1854.2004.00620.x
44. Munabi IG, Buwembo W, Kitara DL, et al. Musculoskeletal disorder risk factors among nursing professionals in low resource settings: a cross-sectional study in Uganda. BMC Nurs. 2014;13(1):7. doi:10.1186/1472-6955-13-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.