")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Prevalence of Overweight and Obesity, and Its Associated Factors Among Health-care Workers, Teachers, and Bankers in Arusha City, Tanzania
Authors Zubery D , Kimiywe J , Martin HD
Received 2 October 2020
Accepted for publication 16 December 2020
Published 2 February 2021 Volume 2021:14 Pages 455—465
DOI https://doi.org/10.2147/DMSO.S283595
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ming-Hui Zou
Dalahile Zubery,1 Judith Kimiywe,2 Haikael D Martin1
1Department of Food Biotechnology and Nutritional Sciences, School of Life Sciences and Bioengineering, Nelson Mandela African Institution of Science and Technology, Arusha, Tanzania; 2Department of Foods, Nutrition and Dietetics, Kenyatta University, Nairobi, Kenya
Correspondence: Dalahile Zubery Tel +255 759 945 149
Email [email protected]
Background: Tanzania is one of the developing countries experiencing an increasing trend of overweight and obesity among adults. Working adults have been identified as a high-risk group more exposed to the predictors of overweight and obesity than the general population. However, limited studies have been done in this group. This study aimed to identify the prevalence of overweight and obesity and its associated risk factors among health-care workers, teachers, and bankers in Arusha city council.
Subjects and Methods: A descriptive cross-sectional study was conducted among health-care workers, teachers, and bankers. A total of 305 working adults aged 18– 60 years participated in the study. A modified World Health Organization (WHO) STEPwise approach for chronic disease risk factor surveillance was used to collect data about socio-demographic characteristics, lifestyle behaviors, dietary practices and anthropometric measurement. The Global Physical Activity Questionnaire (GPAQ) was used to collect information about level of physical activities. The anthropometric measurement and level of physical activities were calculated and ranked according to WHO guidelines.
Results: Overall, 68.9% (31.1% overweight and 37.8% obese) of working adults were overweight or obese. Age (adjusted odds ratio [AOR=7.73; 95% CI: 1.93– 30.87]), gender (AOR=2.60; 95% CI: 1.30– 5.21), marital status (AOR=2.47; 95% CI: 1.11– 5.50), years spent with the current institution (AOR=4.59; 95% CI: 1.38– 17.80), using private car or public transport to and from work (AOR=2.43; 95% CI: 1.10– 5.39) and sedentary work (AOR=2.43; 95% CI: 1.04– 5.71), were significant factors associated with overweight or obesity.
Conclusion: The study identified a higher prevalence of overweight and obesity in Tanzania compared with previous studies. The results from this study are useful for the education sector, financial institutions and health sector on designing workplace wellness programs to reduce the burden of overweight and obesity among this working category.
Keywords: overweight, obesity, working adults, associated factors, Arusha
Introduction
Overweight and obesity are significant risk factors for various non-communicable diseases, including cardiovascular disease, cancer, diabetes, obstructive sleep apnea, osteoarthritis, and affect reproductive performance negatively.1 In 2016, more than 1.9 billion (39%) adults aged 18 years and above were overweight, while more than 650 million (13%) were obese worldwide.2 Projection shows that 2.16 billion (38%) of the world’s adult population will be overweight and 1.12 billion (20%) will be obese by 2030.3 The prevalence of overweight and obesity among adults in Africa is 27% and 8% respectively.2,4 In Tanzania, the prevalence of obesity has risen from 0.6% in 1980 to 3.6% in 1986 and the trend is doubling subsequently in every decade since 1990s.5–8
The consumption of high-energy food, physical inactivity, the sedentary nature of many forms of work and means of transportation contribute to the rise of overweight and obesity.9,10 Occupation relates with socio-economic and lifestyle factors such as physical inactivity and sedentary lifestyle, hence it is considered as a predicting factor for obesity.11 In addition, the economic transition has influenced the adaptation of low physical activity occupations that involve more sedentary activities than previously.12 Despite this, the WHO recognizes the workplace as an excellent setting for prevention and management of diet-related diseases as it can promote healthy lifestyle changes.13–15
Health-care workers, teachers, and bankers have been identified as high-risk occupation groups more exposed to the predictors of overweight and obesity than the general population.16–19 They spend long working hours on sedentary activities due to the nature of their work and socio-economic status may influence the adaptation of less physical activities. It is important to identify the predicting factors for overweight and obesity among these occupation groups for the following reasons: Firstly, protection of available workforce productivity. Secondly, teachers are role models to their students and can influence adaptation of healthy lifestyle habit to the children. Thirdly, health-care workers play a significant role in promoting a healthy lifestyle to their patients due to their prior knowledge on overweight and obesity. Lastly, bankers have an important role in the growing finance sector in Tanzania.
Unfortunately, there is limited information on the burden of overweight and obesity among working adults.2,20 Therefore, this study aimed to determine factors associated with overweight and obesity among health-care workers, teachers, and bankers for protection of available workforce productivity and design of workplace interventions for prevention and management of overweight and obesity in the workplace, and also indirect intervention to the community through students, patients, and customers.
Subjects and Methods
Study Design and Setting
This was a descriptive cross-sectional study that involved working adults aged between 18–60 years working in the Arusha City Council. The region has a higher proportion of urban population (31.3%) compared with the national proportional average (23.1%) and is the third highest urbanized region in the country.21 Arusha City Council has a total number of 160,091 employees as per the 2012 National Census.22 It is a district with a large number of employees compared with other districts in the region.
Sampling Procedure and Study Population
A multistage sampling with three different sampling techniques was used in this study. In the first stage 3 out of 25 wards were purposively selected due to having an adequate representative number of health centers, schools and banks. In the second stage, a random selection of health centers, schools, and banks from 3 wards was made as follows: 8 out of 21 health centers were selected, for schools 10 out of 22 were selected and for banks 8 out of 18 were selected using a ballot method. In the third stage, the eligible number of participants from each site was as follows: for health centers at least 8 health workers, for schools and banks at least 13 participants from each, and the participation at this stage was voluntary. The study included working adults from government and non-government offices in the selected wards of Levolosi, Sekei, and Themi, excluding pregnant women and part-time workers.
Data Collection
The enrollment of participants and data collection were done from August 2019 to February 2020. Data collection was done by well-trained research assistants using a pre-tested questionnaire. The questionnaire was translated from English to Swahili for easy administration. A modified WHO STEP-wise survey questionnaire including the Global Physical Activity Questionnaire was used to collect information about lifestyle factors which included socio-demographic data, level of physical activities, anthropometric measurement, and dietary practices of the study participants.23
Alcohol Consumption, Dietary Practices, and Physical Activities
Alcohol consumption was assessed by recall if the respondent was a lifetime alcohol abstainer, 12-months abstainer or past 30-days drinker. The frequency of consumption was also recorded except the quantity of alcohol intake. The assessment of dietary practices was based on frequency of consumption of fruits and vegetable in a week, estimated amount of serving, and type of meals eaten at work five days in a week.
The Global Physical Activity Questionnaire was used to estimate levels of physical activities based on intensity, duration, and frequency of physical activity at work, during transport and at recreational settings. The data collected included number of days, hours and minutes of physical activity performed at work, in transport and recreational settings for at least 10 minutes or more continuously each day.24 The duration, intensity, and frequency of physical activities performed in a typical week were used to determine the Metabolic Equivalent (MET) as the unit for measuring physical activity energy expenditure. Each individual was classified as having high, moderate, or low level of physical activity following a standard classification approach.24 Sedentary work was defined as a job that requires sitting for 6 hours out of 8 hours at work.
Anthropometric Measurements
Anthropometric measurements were taken by qualified nutritionists whereby height was measured to the nearest 0.5 cm using a portable SHORRTM stadiometer (Shorr Productions, Olney, MA, USA) and weight was measured to the nearest 0.1 kg using a SECATM digital weighing scale (Seca GmbH, Hamburg, Germany). Body Mass Index (BMI) was calculated by dividing the body weight by height in meters squared (kg/m2) and the results were ranked into four groups: ≤18.4 kg/m2 as underweight, 18.5–24.9 kg/m2 as normal weight, 25.0–29.9 kg/m2 as overweight, and ≥30 kg/m2 as obese.25 Waist circumference was taken to the nearest 0.5 cm around the waist, midway between the last rib bone and the iliac bone by using a waist circumference tape. The results were ranked as follows: >94 cm for male and >80 cm for female had increased risk of metabolic complications and >102 cm for male and >88 cm for female had substantially increased risk of metabolic complication. All measurements were taken by considering the standard methods of anthropometric measurement.26,27
Statistical Analysis
The collected data were entered in Microsoft Excel™ (2013) and analyzed using Statistical Package for Social Science Version 20.0 software (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to analyze socio-demographic characteristics. To summarize categorical data, frequency and percentage were used and for continuous data mean and standard deviation. The difference between groups was assessed using chi-squared test for categorical variables and ANOVA for continuous variables. Binary logistic regression analysis was performed to identify lifestyle factors that were associated with overweight or obesity. Independent variables that showed p < 0.25 in the bivariate logistic regression analysis were used in multivariable analysis, and p< 0.05 was considered statistically significant.
Results
Socio-Demographic Characteristics of the Health-care Workers, Teachers, and Bankers
A total of 305 respondents participated in this study. However, 19 had incomplete data, thus were removed from statistical analysis. The final sample size was 286 participants from three working populations: health-care workers (61; 21.3%), teachers(131; 45.8%), and bankers (94; 32.9%). The mean (±SD) height, weight, and BMI of respondents was162.7 (±7.7) cm, 75.1 (±16.2) kg, and 28.4 (±5.9) kg/m2 respectively. More than half of the respondents (204; 71.3%) were female, and 82 (28.7%) were male. The majority of the respondents (121; 42.3%) were aged 30–39 years, and 141 (49.3%) had attended college education. More than half of the respondents (182; 63.6%) were married or cohabiting, and 122 (42.7%) had been with the current institution for more than seven years. The majority of teachers were earning 250,000–500,000 Tsh (70.9%), health-care workers were earning 500,000–750,000 Tsh (31.3%), and most bankers earned more than 1,000,000 Tsh (81.6%) (Table 1).
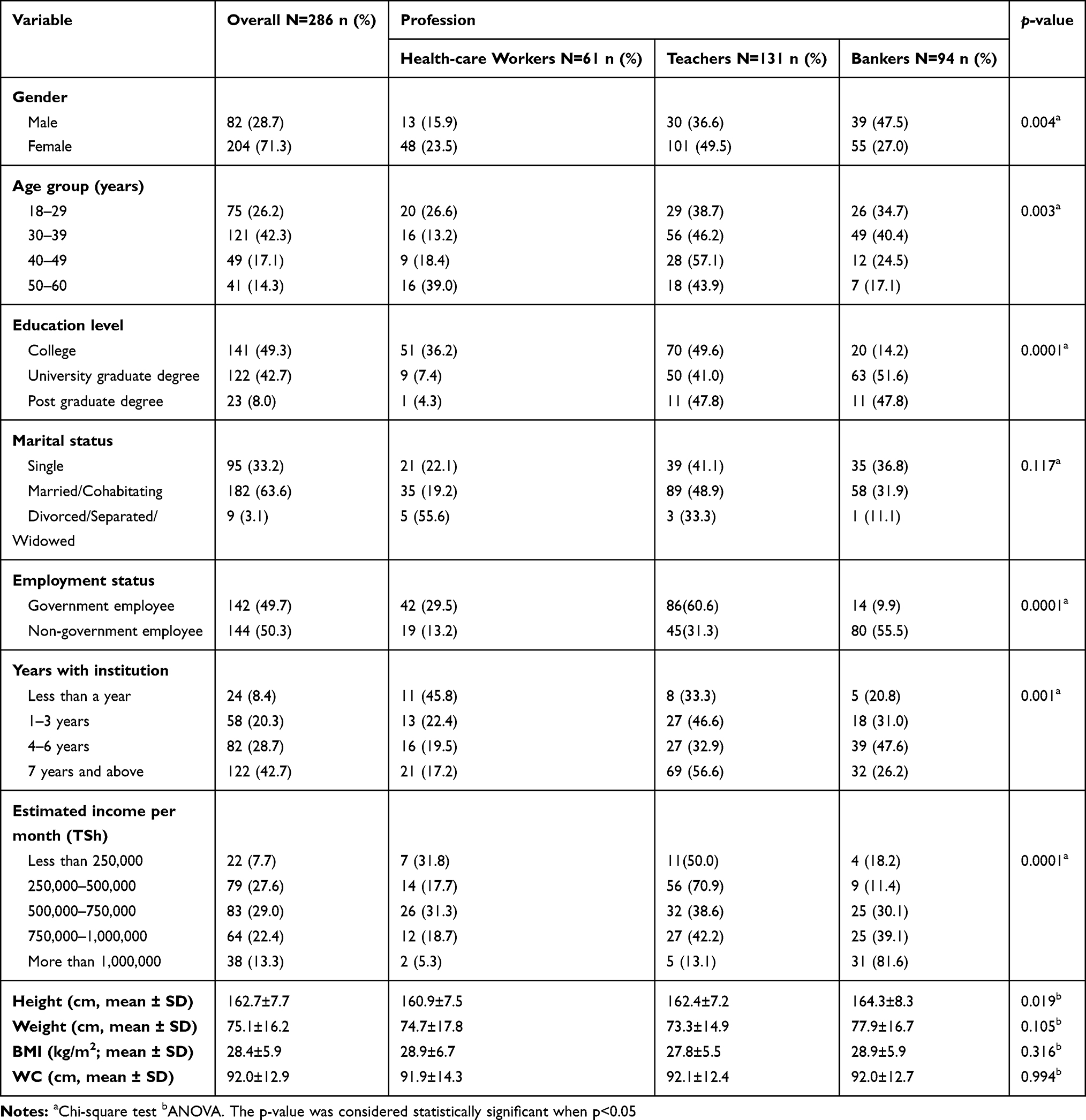 |
Table 1 Socio-Demographic Characteristics of the Health-care Workers, Teachers, and Bankers |
Lifestyle Factors of the Health-care Workers, Teachers, and Bankers
About 56 (19.6%) of the study participants consumed alcohol, and most of them (34; 60.7%) (p=0.0001), were bankers. The consumption of vegetables was higher among teachers (72; 50.0%) (p= 0.308) than other working adults, although the difference was not statistically significant. Of the meals eaten at work five days a week, nearly half of the respondents (132; 46.2%) (p= 0.063) were eating breakfast and lunch at work, and mostly were bankers. Moreover, use of car or public transport as means of transport to and from work was common to about 186 (65%) and a substantial proportion of them were bankers (78; 42.0%) (p= 0.0001). All bankers reported that the nature of their work is sedentary (94; 39.8%), which was different from their counterparts and they also spend more than six hours (65; 48.8%) doing sedentary work compared with health-care workers (14; 11.4%) and teachers (44; 35.8%). A low level of physical activity was more prevalent among bankers (62; 48%) than health-care workers (20; 15.75%) and teachers (45; 35.4%) (p= 0.0001 for each) as shown in Table 2.
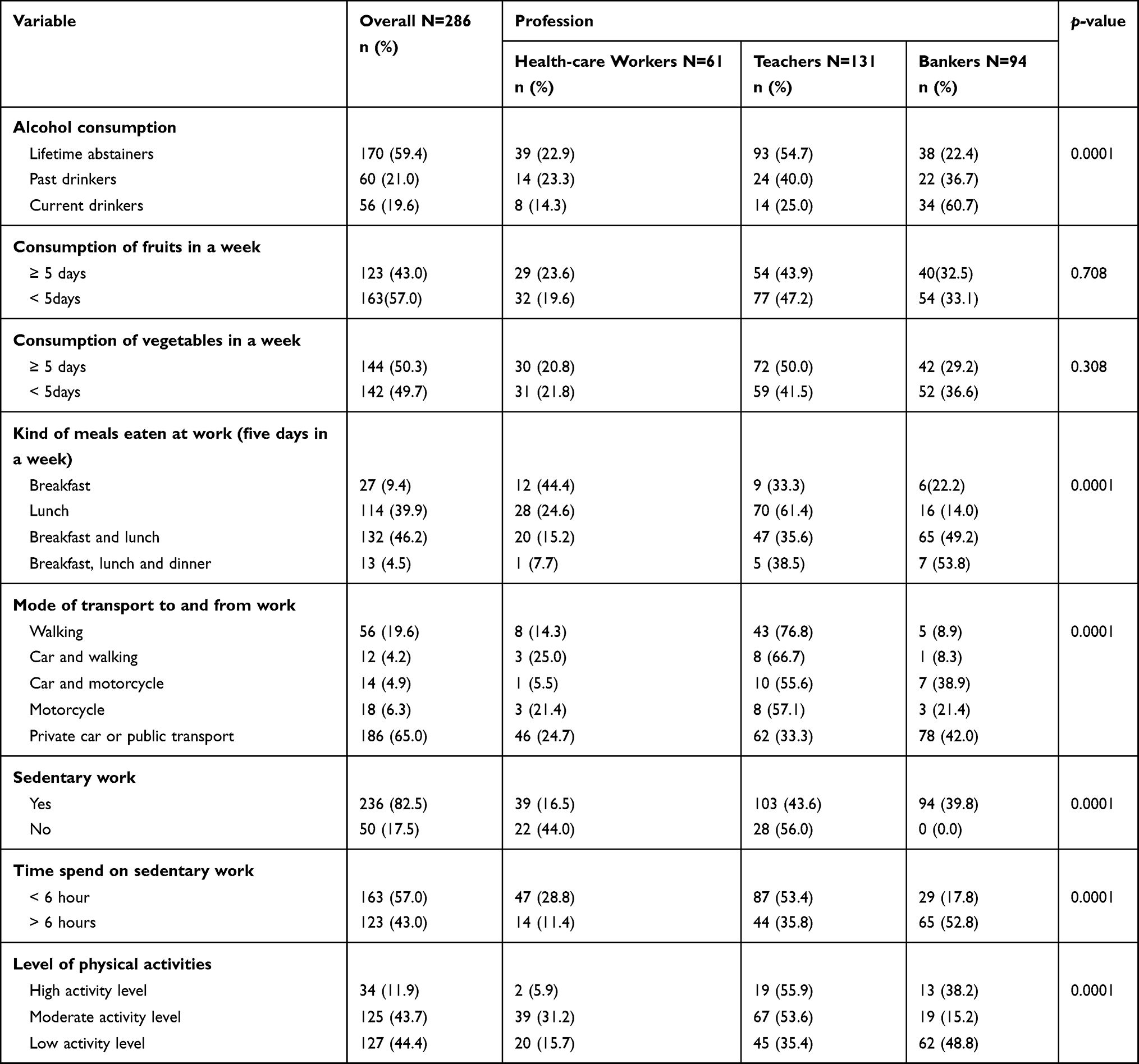 |
Table 2 Lifestyle Factors of the Health-care Workers, Teachers, and Bankers |
Prevalence of Overweight and Obesity Among Health-care Workers, Teachers, and Bankers
The overall prevalence of overweight and obesity among working adults was 68.9% (31.1% overweight and 37.8% obesity). By considering the profession, a higher prevalence of overweight or obesity was found among bankers (77.7%) compared with health-care workers (68.9%) and teachers (62.6%) (Figure 1A and B). A higher prevalence of overweight or obesity (74.5%) was found among women compared with men (54.9%) (Figure 2A). Furthermore, the prevalence of overweight or obesity was higher among respondents aged 40–49 years (91.8%), and a prevalence of 87.8% was found for those who were aged 50–60 years (Figure 2B).
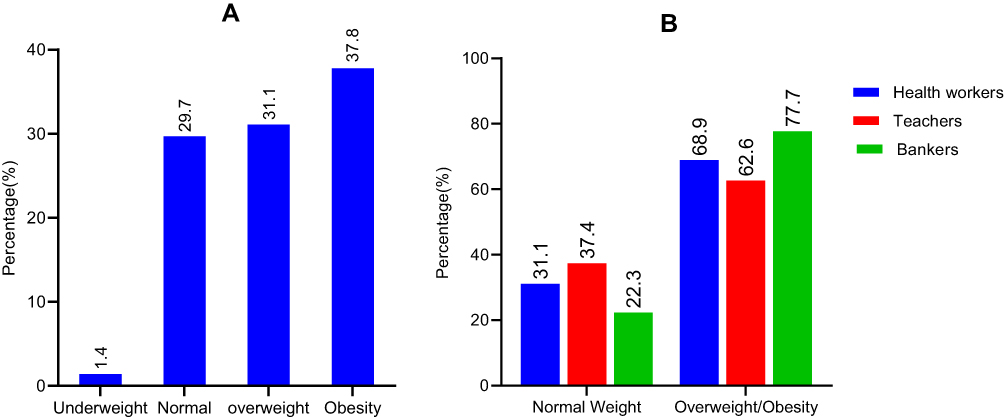 |
Figure 1 (A) Overall prevalence of overweight and obesity among working adults in Arusha city. (B) Prevalence of overweight or obesity among Health-care workers, Teachers, and Bankers. |
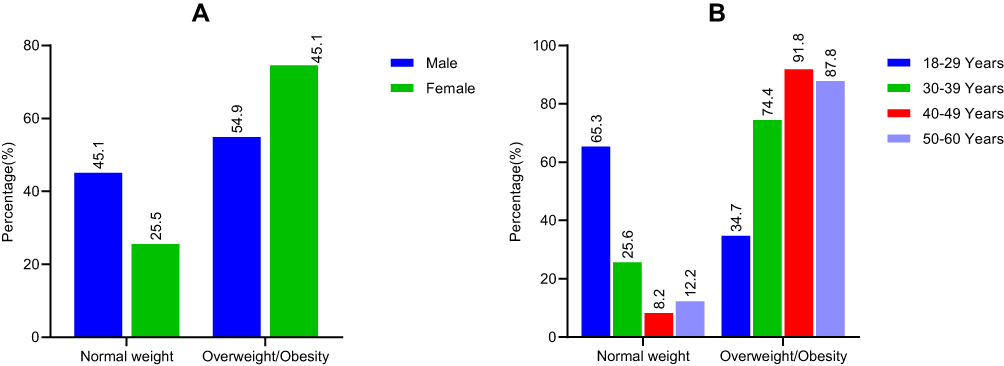 |
Figure 2 (A) Distribution of gender on body mass index (BMI): (B) Distribution of age categories on body mass index (BMI). |
Factors Associated with Overweight Or Obesity Among Health-care Workers, Teachers, and Bankers
The dependent variable of this study was grouped into two; normal weight and overweight/obesity. In multivariable logistic regression analysis gender, age, marital status, years spent with the current institution, means of transport to and from work, and sedentary work were significantly associated with overweight or obesity with p < 0.05. In the adjusted odds ratio, it was found that women had 2.59 (95% CI 1.297–5.207) times increased odds of being overweight or obese compared with men. The results also show that working adults aged 40–49 and 50–60 had a higher risk (AOR=7.73, 95% CI: 1.93–30.87; AOR=5.34, 95% CI 1.34–21.38, respectively) of being overweight or obese compared with those aged 18–29 years. Married or co-habiting participants showed increased odds of being overweight or obese compared with singles (AOR=2.47, 95% CI 1.113–5.500). The odds of being overweight or obese increased with the increase in number of years at work. Respondents who had worked for 7 years and above were 4.28 times more likely to be overweight or obese than those who had worked for less than a year (AOR=4.28, 95% CI 1.54–15.86). Similarly, the odds of overweight or obesity increased as income increased as follows: 500,000–750,000 Tsh (AOR=0.48, 95% CI 0.49–1.95), 750,000–1,000,000 (AOR=0.86, 95% CI 0.18–4.01) and more than 1,000,000 (AOR=1.25, 95% CI 0.22–7.15) (Table 3). The respondents who were using car or public transport as a means of transport to and from work showed an increased risk of overweight or obesity (AOR 2.430, 95% CI 1.096–5.390) compared with those who were walking. The sedentary workers had higher odds (2.43, 95% CI 1.037–5.706) of being overweight or obese than non-sedentary workers (Table 4).
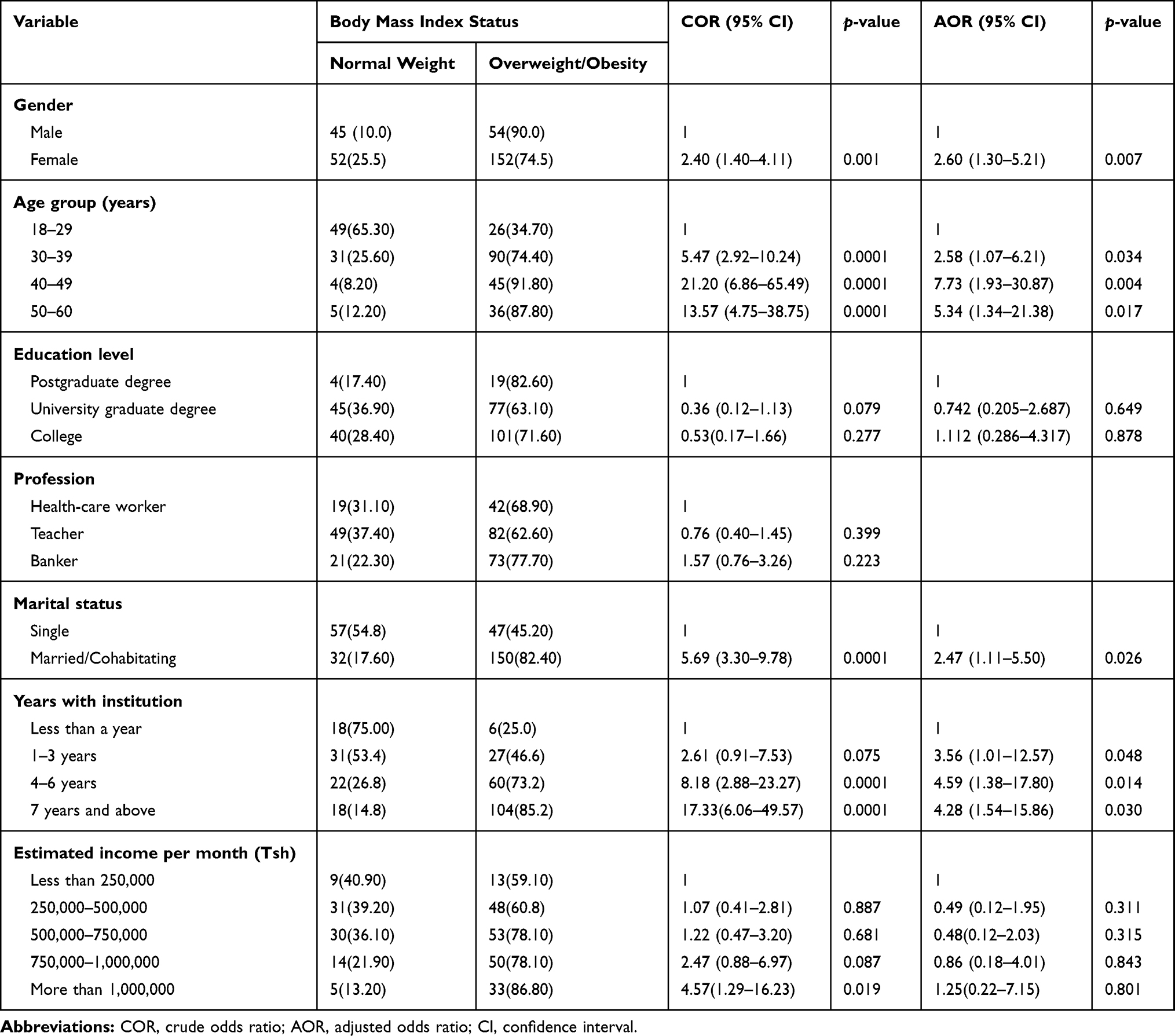 |
Table 3 Socio-Demographic Factors Associated with Overweight and Obesity Among Health-care Workers, Teachers, and Bankers |
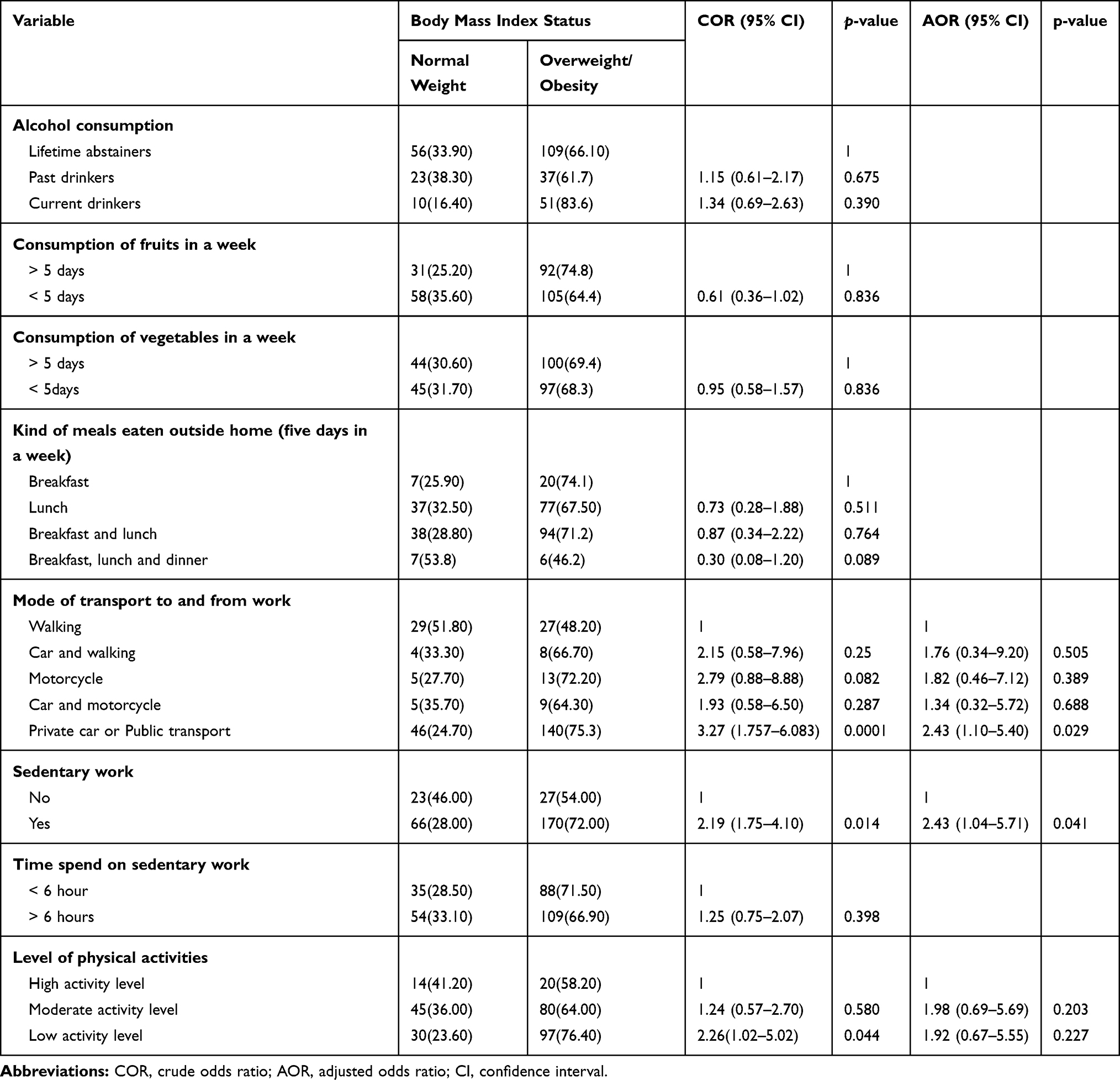 |
Table 4 Lifestyle Factors Associated with Overweight and Obesity Among Health-care Workers, Teachers, and Bankers |
Discussion
Overweight and obesity have been identified as a global health concern28,29 affecting both developed and developing countries.30 In Tanzania, a high prevalence of overweight and obesity has been reported among women, urban communities, and high socio-economic status populations.31 Unfortunately, limited studies have been done to assess overweight and obesity and their associated risk factors among working adults in Tanzania.2,20 Therefore this study was conducted to determine the prevalence of overweight and obesity and its associated factors among health-care workers, teachers, and bankers because they are considered to be neglected groups during research studies despite being recognized as high-risk groups.
The overall prevalence of overweight and obesity among working adults was 68.9% (31.1% overweight and 37.8% obesity). These findings are comparable with the multi-country large-scale longitudinal study done in four sub-Saharan countries in different sites of Nigeria, South Africa, Tanzania, and Uganda among nurses, teachers, and village residents, which reported the prevalence of overweight and obesity were 31% and 34%, respectively.2 The current study has found a higher prevalence of obesity (108; 37.8%) among working adults in Arusha City Council than the prevalence of obesity reported from previous studies. The prevalence of obesity in the studies conducted in 2003, 2012 and 2019 were 25%, 23.44%, and 25%, respectively.20,32,33 However, the prevalence of obesity was lower than those reported from other countries such as Nigeria (62.2%)9 and Libya (42.4%).34 The higher prevalence of overweight or obesity among working adults might be influenced by sedentary behaviors, which might be contributed to by the nature of their work, and the socio-economic status that may encourage the adaptation of less physical activities and consumption of unhealthy diets.35,36
The female working adults were two times more likely to be overweight or obese than males. The results agree with the findings reported by Addo et al. in 2015 and Darebo et al. in 2019, that the odds of overweight or obesity among females was two times higher compared with males.19,37 Gender variability in overweight or obesity might be ascribed by biological factors of having less lean mass and more fat mass. Also, during the childbearing period sex hormones have a significant impact on fat deposition, hence increasing the risk of excess weight gain in women.38,39 Furthermore, the prevalence of overweight or obesity increased with the increase in age. Similar findings have been reported by Low et al.40 and Addo et al.,19 that the prevalence of overweight and obesity increased as age increases. In addition, Low et al. found that the estimated peak increase in prevalence of obesity as age increases was 40–50 years in developing countries while it was 50–60 years in developed countries, which is in line with the current study. The increase in the prevalence of obesity with age could be due to the fact that 40–60 years is a peak age in career progression, so people tend to relax as they reach self-actualization, hence decrease physical activities, but hormonal changes may also be a factor.41,42
Besides, the findings from this study showed that married or co-habiting working adults had increased odds of being overweight or obese compared with those who were single. The results support the findings reported by Dagne et al.43 and Tzotzas et al.,44 that married adults had higher odds of being overweight or obese than unmarried adults. The exact association between marriage and obesity is not well understood. The study done by Averett et al.45 hypothesized that increase in BMI among married couples is due to the increased social support, along with regularly eating dense food that increases the risk of being overweight or obese.45 The results also showed that the odds of being overweight or obese increased with the increase in number of years spent at work. Likewise, the study done by Addo et al.19 in 2015 documented that the odds of being overweight or obese for people who had worked for three years and above was higher than those who had worked for less than a year. Means of transport to and from work was another significant finding observed in this study. The odds of being overweight or obese among those who were using car or public transport was two times higher compared with those who were walking. Similarly, a study done in Atlanta to assess the obesity relationships with community design, physical activity, and time spent in cars found an increased likelihood of being obese by 6% with each additional hour spent in a car per day.46 Results from this study also concur with a study done in China which reported that an increase in car use is associated with being obese.47
The odds of being overweight or obese was higher among sedentary working adults than non-sedentary working adults. This finding is supported by other similar studies done in the United States35 and Japan,48 which reported that sedentary work increases the risk of obesity among workers. In addition, sedentary work and physical inactivity are identified as risk factors for overweight and obesity.19,31,49 However, the current study did not find any significant association between a low level of physical activity and being overweight or obese. Furthermore, occupation sitting time has been associated with being overweight or obese.50–52 However, the current study did not find any significant association. Although the consumption of vegetables was not associated with being overweight or obese, higher consumption of vegetables was found among teachers than other working populations; this could be attributed to availability of vegetable gardens at schools and possibly the socio-economic class of teachers, since vegetables in Tanzania are low in cost compared with meat and fish. For fruits, low consumption of fruits was reported among working adults who were overweight or obese, however some of the respondents who were overweight or obese claimed that the consumption of some fruits contributed to the increase in excess weight gain so this area raises a question for further research.
Limitations of the Study
This was a descriptive cross-sectional study which is limited to explore the causal relationship between the risk factors and overweight or obesity due to the use of a questionnaire. Hence, further research on causality of overweight and obesity should be done to establish cause and effect relationships, especially on socio-economic factors, because estimated income among bankers was higher than other working populations and higher prevalence of overweight or obesity was found among bankers. In addition, more of the study participants were women in comparison with other studies. This could be the reason for a higher prevalence of overweight and obesity in this study since women tend to have a higher percentage of body fat compared with men.
Conclusion
The study found a high prevalence of overweight and obesity among working adults. These findings appear to show an emerging problem in working populations. The findings will inform the education sector, financial institutions and health sector on designing workplace wellness programs to reduce the burden of overweight and obesity among this working category. Workplace wellness programs may focus on providing information and education about the adaptation of healthy lifestyles specifically on healthy eating habits and physical activities to prevent and manage the modifiable risk factors for overweight or obesity.
Data Sharing Statement
The data set used for this study is available upon reasonable request.
Ethical Considerations
The study was conducted according to the Declaration of Helsinki. Ethical clearance certificate number KNCHREC 0014 was obtained from Northern Tanzania Health Research Ethics Committee (KNCHREC). Written permission to conduct research was also sought from Arusha City Council, administrators of the selected banks, schools and health facilities who participated in the study. Respondents signed written informed consent after being briefed on the study. To ensure confidentiality data collection was done individually in a special prepared room in their working area and codes known only by researchers were used instead of names in identifying participants to maintain anonymity.
Acknowledgments
We would like to thank all participants who accepted to take part in this study and the administrators of facilities who participated in the study for their generous support, also nurses, research assistants, and nutritionists who helped in data collection. Our sincere thanks go to the African Center for Research, Agriculture advancement Teaching Excellence and Sustainability (CREATES) at Nelson Mandela-African Institution of Science and Technology for financial support of this study.
Disclosure
The authors report no competing interests in this work.
References
1. Berrington de Gonzalez A, Hartge P, Cerhan JR, et al. Body-mass index and mortality among 1.46 million white adults. New England J Med. 2010;363(23):2211–2219. doi:10.1056/NEJMoa1000367
2. Ajayi IO, Adebamowo C, Adami H-O, et al. Urban–rural and geographic differences in overweight and obesity in four sub-Saharan African adult populations: a multi-country cross-sectional study. BMC Public Health. 2016;16(1):1126. doi:10.1186/s12889-016-3789-z
3. Kelly T, Yang W, Chen C-S, Reynolds K, He J. Global burden of obesity in 2005 and projections to 2030. Int J Obes. 2008;32(9):1431–1437. doi:10.1038/ijo.2008.102
4. Alwan A. Global Status Report on Noncommunicable Diseases 2010. World Health Organization; 2011.
5. Organization WH. Obesity: Preventing and Managing the Global Epidemic. World Health Organization; 2000.
6. Organization WH. Global Status Report on Noncommunicable Diseases 2014. World Health Organization; 2014.
7. Mpembeni RN, Muhihi AJ, Maghembe MJ, et al. Overweight, obesity and perceptions about body weight among primary schoolchildren in Dar es Salaam, Tanzania. Tanzan J Health Res. 2014;16:4. doi:10.4314/thrb.v16i4.7
8. Njelekela MA, Mpembeni R, Muhihi A, et al. Gender-related differences in the prevalence of cardiovascular disease risk factors and their correlates in urban Tanzania. BMC Cardiovasc Disord. 2009;9(1):30. doi:10.1186/1471-2261-9-30
9. Ogunjimi L, Ikorok MM, Olayinka Y. Prevalence of obesity among Nigeria nurses: the Akwa Ibom state experience. Int NGO J. 2010;5(2):45–49.
10. Amoh I, Appiah-Brempong E. Prevalence and risk factors of obesity among senior high school students in the Adansi North district of Ghana. Int J Community Med Public Health. 2017;4(10):3762. doi:10.18203/2394-6040.ijcmph20174247
11. Allman-Farinelli MA, Chey T, Merom D, Bauman AE. Occupational risk of overweight and obesity: an analysis of the Australian Health Survey. J Occupational Med Toxicol. 2010;5(1):1–9. doi:10.1186/1745-6673-5-14
12. Brownson RC, Boehmer TK, Luke DA. Declining rates of physical activity in the United States: what are the contributors? Annu Rev Public Health. 2005;26:421–443. doi:10.1146/annurev.publhealth.26.021304.144437
13. Bosu WK. Determinants of mean blood pressure and hypertension among workers in west africa. Int J Hypertens. 2016;2016:2016. doi:10.1155/2016/3192149
14. Anderson LM, Quinn TA, Glanz K, et al. The effectiveness of worksite nutrition and physical activity interventions for controlling employee overweight and obesity: a systematic review. Am J Prev Med. 2009;37(4):340–357. doi:10.1016/j.amepre.2009.07.003
15. Conn VS, Hafdahl AR, Cooper PS, Brown LM, Lusk SL. Meta-analysis of workplace physical activity interventions. Am J Prev Med. 2009;37(4):330–339. doi:10.1016/j.amepre.2009.06.008
16. Chou C-F, Johnson PJ. Health disparities among America’s health care providers: evidence from the integrated health interview series, 1982 to 2004. J Occupational Environmental Med. 2008;50(6):696. doi:10.1097/JOM.0b013e31816515b5
17. Skaal L, Pengpid S. Obesity and health problems among South African healthcare workers: do healthcare workers take care of themselves? South African Family Practice. 2011;53(6):563–567. doi:10.1080/20786204.2011.10874153
18. Pobee RA, Owusu W, Plahar W. The prevalence of obesity among female teachers of child-bearing age in Ghana. African j Food, Agriculture, Nutrition Development. 2013;13:3.
19. Addo PN, Nyarko KM, Sackey SO, Akweongo P, Sarfo B. Prevalence of obesity and overweight and associated factors among financial institution workers in Accra Metropolis, Ghana: a cross sectional study. BMC Res Notes. 2015;8(1):599. doi:10.1186/s13104-015-1590-1
20. Nyaruhucha C, Achen J, Msuya J, Shayo N, Kulwa K. Prevalence and awareness of obesity among people of different age groups in educational institutions in Morogoro, Tanzania. East Afr Med J. 2003;80(2):68–72. doi:10.4314/eamj.v80i2.8648
21. National bureau of statistics (Tanzania) and ICF Macro.Tanzania Population and Housing census.Government of Tanzania, Dodoma. 2006;Volume X.
22. URoT. Arusha region basic demographic and social-economic profile. National Breau Statistics, Ministry Finance. 2016;84(2):289–298.
23. Mayige M, Kagaruki G. Tanzania STEPS survey report. Dar Es Salaam. 2013.
24. Armstrong T, Bull F. Development of the world health organization global physical activity questionnaire (GPAQ). J Public Health. 2006;14(2):66–70. doi:10.1007/s10389-006-0024-x
25. Organization WH. Global Database on Body Mass Index. 2006. Global Database on Body Mass Index; 2016.
26. WHO. WHO STEPS Surveillance Manual: The WHO STEPwise Approach to Chronic Disease Risk Factor Surveillance. Geneva: World Health Organization; 2005.
27. WHO. Prevalence of Noncommunicable Disease Risk Factors in the Republic of Moldova STEPS 2013. Regional Office for Europe. Vol. 2014. Denmark;2014.
28. Goettler A, Grosse A, Sonntag D. Productivity loss due to overweight and obesity: a systematic review of indirect costs. BMJ Open. 2017;7:10. doi:10.1136/bmjopen-2016-014632
29. Raine KD, Nykiforuk CI, Vu‐Nguyen K, et al. Understanding key influencers’ attitudes and beliefs about healthy public policy change for obesity prevention. Obesity. 2014;22(11):2426–2433. doi:10.1002/oby.20860
30. Murtagh E, Collaboration NRF. Worldwide trends in children’s and adolescents’ body mass index, underweight, overweight and obesity, in comparison with adults, from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies with 128.9 million participants (Pre-published version). Lancent.2017.
31. Shayo GA, Mugusi FM. Prevalence of obesity and associated risk factors among adults in Kinondoni municipal district, Dar es Salaam Tanzania. BMC Public Health. 2011;11(1):365. doi:10.1186/1471-2458-11-365
32. Muhihi AJ, Njelekela MA, Mpembeni R, Mwiru RS, Mligiliche N, Mtabaji J. Obesity, overweight, and perceptions about body weight among middle-aged adults in Dar es Salaam, Tanzania. ISRN Obesity. 2012;2012:2012. doi:10.5402/2012/368520
33. Kamanga L. Colorectal Cancer Epidemiology in Tanzania: Patterns in Relation to Dietary and Lifestyle Factors. NM-AIST; 2019.
34. Lemamsha H, Randhawa G, Papadopoulos C. Prevalence of overweight and obesity among libyan men and women. Biomed Res Int. 2019;2019:2019. doi:10.1155/2019/8531360
35. Choi B, Schnall PL, Yang H, et al. Sedentary work, low physical job demand, and obesity in US workers. Am J Ind Med. 2010;53(11):1088–1101. doi:10.1002/ajim.20886
36. Ismail IM, Kulkarni AG, Kamble SV, Borker SA, Rekha R, Amruth M. Prevalence of hypertension and its risk factors among bank employees of Sullia Taluk, Karnataka. Sahel Medical J. 2013;16(4):139. doi:10.4103/1118-8561.125553
37. Darebo T, Mesfin A, Gebremedhin S. Prevalence and factors associated with overweight and obesity among adults in Hawassa city, southern Ethiopia: a community based cross-sectional study. BMC Obesity. 2019;6(1):8. doi:10.1186/s40608-019-0227-7
38. Siega-Riz AM, Evenson KR, Dole N. Pregnancy-related weight gain—a link to obesity? Nutr Rev. 2004;62(suppl_2):S105–S111. doi:10.1111/j.1753-4887.2004.tb00079.x
39. Fat OA. Storage depends on Gender. Medical News. 2011.
40. Low S, Chin MC, Deurenberg-Yap M. Review on epidemic of obesity. Annals Acad Med Singapore. 2009;38(1):57.
41. Erem C, Arslan C, Hacihasanoglu A, et al. Prevalence of obesity and associated risk factors in a Turkish population (Trabzon city, Turkey). Obes Res. 2004;12(7):1117–1127. doi:10.1038/oby.2004.140
42. Villareal D, Apovian C, Kushner R, Klein S. American Society for Nutrition; NAASO, The Obesity Society. Obesity in older adults: technical review and position statement of the American Society for Nutrition and NAASO, The obesity society. Am J Clin Nutr. 2005;82(5):923–934. doi:10.1093/ajcn/82.5.923
43. Dagne S, Gelaw YA, Abebe Z, Wassie MM. <p>Factors associated with overweight and obesity among adults in northeast Ethiopia: a cross-sectional study. Diabetes, Metabolic Syndrome Obesity. 2019;12:391. doi:10.2147/DMSO.S179699
44. Tzotzas T, Vlahavas G, Papadopoulou SK, Kapantais E, Kaklamanou D, Hassapidou M. Marital status and educational level associated to obesity in greek adults: data from the national epidemiological survey. BMC Public Health. 2010;10(1):732. doi:10.1186/1471-2458-10-732
45. Averett SL, Sikora A, Argys LM. For better or worse: relationship status and body mass index. Econ Hum Biol. 2008;3(6):330–349. doi:10.1016/j.ehb.2008.07.003
46. Frank LD, Andresen MA, Schmid TL. Obesity relationships with community design, physical activity, and time spent in cars. Am J Prev Med. 2004;27(2):87–96. doi:10.1016/j.amepre.2004.04.011
47. Bell AC, Ge K, Popkin BM. The road to obesity or the path to prevention: motorized transportation and obesity in China. Obes Res. 2002;10(4):277–283. doi:10.1038/oby.2002.38
48. Ishizaki M, Morikawa Y, Nakagawa H, et al. The influence of work characteristics on body mass index and waist to hip ratio in Japanese employees. Ind Health. 2004;42(1):41–49. doi:10.2486/indhealth.42.41
49. Alghamdi AS, Yahya MA, Alshammari GM, Osman MA. Prevalence of overweight and obesity among police officers in Riyadh City and risk factors for cardiovascular disease. Lipids Health Dis. 2017;16(1):79. doi:10.1186/s12944-017-0467-9
50. Mummery WK, Schofield GM, Steele R, Eakin EG, Brown WJ. Occupational sitting time and overweight and obesity in Australian workers. Am J Prev Med. 2005;29(2):91–97. doi:10.1016/j.amepre.2005.04.003
51. Yang L, Hipp JA, Marx CM, Brownson RC. Peer reviewed: occupational sitting and weight status in a diverse sample of employees in midwest metropolitan cities, 2012–2013. Prev Chronic Dis. 2014;11:11. doi:10.5888/pcd11.140286
52. Chau JY, van der Ploeg HP, Merom D, Chey T, Bauman AE. Cross-sectional associations between occupational and leisure-time sitting, physical activity and obesity in working adults. Prev Med. 2012;54(3–4):195–200. doi:10.1016/j.ypmed.2011.12.020
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.