")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Prevalence of Normal-Weight Obesity in Community-Dwelling Chinese Older Adults: Results from the Beijing Longitudinal Study of Aging
Authors Ji T, Zhang L, Tang Z, Sun F, Li Y, Ma L
Received 22 January 2020
Accepted for publication 25 April 2020
Published 12 May 2020 Volume 2020:13 Pages 1611—1617
DOI https://doi.org/10.2147/DMSO.S246884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Tong Ji,1,2,* Li Zhang,1,* Zhe Tang,2 Fei Sun,2 Yun Li,1 Lina Ma1
1Department of Geriatrics, Xuanwu Hospital, Capital Medical University, China National Clinical Research Center for Geriatric Medicine, Beijing 100053, People’s Republic of China; 2Beijing Geriatric Healthcare Center, Xuanwu Hospital, Capital Medical University, Beijing Institute of Geriatrics, Beijing 100053, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lina Ma; Zhe Tang Email [email protected]; [email protected]
Objective: Normal-weight obesity (NWO) is characterized by high body fat percentage (BFP) in individuals with normal body mass index (BMI). This condition may increase the risk of serious health problems, such as cardiovascular diseases, diabetes, insulin resistance, hypertension, and metabolic syndrome. However, the prevalence of NWO in older adults in Beijing remains unclear. This study aimed to investigate the prevalence of overweight and obesity among older adults in Beijing, using three obesity assessment indicators: BMI, waist circumference, and BFP.
Design: Cross-sectional study.
Setting and Participants: Data were obtained from the 2012 Beijing Longitudinal Study of Aging, which used a stratified, sectional, random, and cluster sampling method.
Methods: Questionnaires, physical examinations, and laboratory tests were completed. Obesity was divided into four categories based on combinations of BMI and BFP: non-obese, muscle-type obesity, NWO and fatty obesity.
Results: A total of 2393 community-dwelling older adults with an average age of 72.98± 8.09 years old were recruited. Of them, 1051 were male (43.92%) and 1245 were living in rural areas (52.03%). The prevalence of overweight and obesity among older people in Beijing was 35.5% and 16.1%, respectively. When the sample was divided according to obesity classification, the proportion of muscular obesity, NWO and adipose obesity was 14.7%, 10.7%, and 41.8%, respectively. The prevalence of central obesity was 62.3%. The prevalence of obesity decreased with age, but it was higher in females than in males as well as among individuals living in urban areas than in individuals living in rural areas.
Conclusion: The prevalence of NWO was 10.7% among older adults in Beijing and increased with age. Older adults who are female or living in urban areas should be instructed to take measures aimed at reducing body fat and increasing muscle strength.
Keywords: obesity, normal-weight obesity, body fat percentage, older adults
Introduction
Obesity is defined as abnormal or excessive fat accumulation that may damage health.1 Over the past 30 years, with economic development and the improvement of living standards, the prevalence of overweight and obesity has grown at an alarming rate, becoming a major public health problem globally. More than 1.9 billion people, equivalent to 39% of adults worldwide, were overweight in 2014, while about 13% were obese.2 In China, there were 43.2 million obese men and 46.4 million obese women in 2014, making the Chinese population top of the global obesity rankings in absolute terms.2 As the population ages, the prevalence of obesity among older adults also increases. According to the National Health and Nutrition Examination Survey (NHANES), the prevalence of obesity among adults aged 60 years and over has increased from 35.1% in 2007–2008 to 41% in 2015–2016.3 In 2013, the Chinese Center for Disease Control and Prevention launched the fourth chronic disease and risk factors monitoring program, which spans 31 provinces; the program showed that the overall obesity and central obesity rate among people aged 60 years and over were 13.2% and 55.4%, respectively.4 Obesity creates a serious strain on healthcare systems; in 2014 alone, the total cost of obesity in the United States was estimated at $149.4 billion, with obesity-related medical costs being highest among people over 65 years of age.5 However, obesity is associated with a range of chronic conditions, which further increases costs. For example, in 2010 in China, the total economic burden of major chronic diseases associated with overweight and obesity reached 90.768 billion yuan, accounting for 42.9% of the overall economic burden associated with major chronic diseases.6
Research on obesity has used the body mass index (BMI) and waist circumference (WC) as relevant indicators in older adults. However, these indicators are unable to quantitatively assess fat content. The characteristics of obesity in the elderly are related to the increase in fat mass and increase in fat infiltration to the muscles and a decrease in muscle mass. As body composition changes with age, the accuracy of the BMI and WC, as well as other crude indicators, decreases when applied to older adults.
Recently, using more direct measures, such as body fat percentage (BFP), has been proposed as a tool better able to predict the risk of development of metabolic disorders;7 nevertheless, the evidence is scarce and its usefulness remains controversial. A previous study has reported positive correlations between BFP and hypertension, dyslipidemia, diabetes, as well as other obesity-associated risk factors for chronic disease among older adults in rural China.8 Furthermore, the type of obesity where weight remains within normal range but the body fat content is significantly increased has been called “normal-weight obesity” (NWO).9 Several previous studies have reported the prevalence of NWO among older adults. One study, which defined NWO with a BF cutoff value ≥25% for men and ≥35% for women, has reported a prevalence of 21.4% and 31.3% among American men and women, respectively.10 According to a nationwide study of the Chinese population, the prevalence of NWO was 4.76%, 6.81%, and 3.34%, among the general population, men, and women, respectively.11 Moreover, a Korean study, including 2167 middle-aged and older adults showed that the overall prevalence of NWO was 8.3%.12 However, the prevalence of NWO among older adults in Beijing is unclear. We hypothesized the prevalence of NWO increased with age in older adults in Beijing.
Methods
Participants
Data were from the Beijing Longitudinal Study of Aging (BLSA). Based on the sample data of Beijing in 2012, we used stratified, cluster and random sampling methods to select the elderly aged 60 and above in Xicheng District, Daxing District and Huairou District in Beijing. This study was expected to investigate 2778 people, the actual survey of 2411 people (86.8%). Among them, 2393 people were subjected to BMI measurement, 2382 people were subjected to waist circumference measurement, and 1223 persons were measured for BFP. The Ethics Committee of Xuanwu Hospital, Capital Medical University approved this study. This study was conducted in accordance with the Declaration of Helsinki. All participants signed an informed consent form.
Sociodemographic Variables
Sociodemographic information was collected by trained investigators: basic information (age, sex, living area, education level, etc.), family status (marital status, family relationship, etc.), lifestyle (smoking, drinking, eating habits, sleep, exercise, etc.), and chronic medical history.
Anthropometric Measurements
Anthropometric measurements included height, weight, waist circumference and BFP, all of which were collected by trained investigators qualified at using standard methods, as relevant. All instruments used were first calibrated according to recognized standards.
Shoes were taken off for weight and height measurement. Weight was measured in kilograms on a calibrated digital scale, and standing height was measured in centimeters with the participant’s back to a stadiometer’s backboard. The WC was measured with the participants standing with feet 25–30 cm apart, and the measurement position is at the midpoint of the line connecting the front upper edge of the horizontal position and the lower edge of the 12th rib.
Using the OMRON HBF-306 Bio-Resistance Body Composition Analyzer (Yangzhou City, Jiangsu Province, China), bioelectrical impedance values were obtained. Subjects were asked to avoid eating or drinking anything during the fasting period. Participants had a single bipolar measurement of resistance and reactance taken at 50 kHz between their hands while in standing position and keep their arms at 90 degrees from the body. According to the resistance between two palms to calculate the total body fat, it was necessary to put the resistance value, height, weight, age, sex into the equation. This equation was provided by the OMRON company. The quotient of total body fat and weight multiplied by 100 was termed percent body fat.
Obesity Criteria
NWO is defined as a state whereby the BMI remains within the normal range, but overfat, which is excessive body fat, is present; this is also known as “invisible” obesity.9 The classification criteria are recommended by the Guidelines for Prevention and Control of Overweight and Obesity in Chinese Adults.13 Based on the BMI, obesity is defined as follows: BMI <18.5 kg/m2 is underweight, BMI between 18.5 and 23.9 kg/m2 is normal weight, BMI 24–27.9 kg/m2 is overweight, and BMI >28 kg/m2 is obesity. Obesity based on the WC was defined as: male WC≥80 cm, female WC≥85 cm. Obesity based on the BFP, according to the classification criteria recommended in 2012 for the use with Chinese adults, was defined as: male ≥25% body fat over the standard, female ≥35% as body fat over the standard.14
Obesity was divided into four categories based on combinations of BMI and BFP: non-obese (BMI<24 kg/m2 and BFP: male<25% and female<35%), muscle-type obesity (BMI≥24 kg/m2, BFP: male <25% and female <35%), NWO (BMI<24 kg/m2 and BFP: male ≥25% and female ≥35%), and fatty obesity (BMI ≥24 kg/m2 and BFP: male ≥25% and female ≥35%).15
Statistical Methods
Epidata software was used for data input, and secondary input and automatic verification were performed to ensure the accuracy of data entry. All data were processed using SPSS 11.5. The count data were expressed as a percentage, and the inter-group rates were compared using the χ2 test or Fisher’s exact probability method. The prevalence rate was normalized based on the national standard population composition rate (%) of the sixth population census in 2010. P-value <0.05 was considered statistically significant.
Results
The average age of the 2393 community-dwelling older adults was 72.98±8.09 years old. Of them, 1051 were male (43.92%) and 1245 were living in rural areas (52.03%). The prevalence rate of overweight based on BMI among older adults was 33.9%; it was slightly higher among males than among females, and it was higher among residents of urban than among those of rural areas. The overall prevalence of obesity based on BMI was 15.5%, and it decreased with age and was higher in female and urban residents (Tables 1 and 2). The overall prevalence of central obesity based on WC was 62.3% and higher in urban areas (Table 3).
 |
Table 1 The Characteristics of Obesity Based on Body Mass Index |
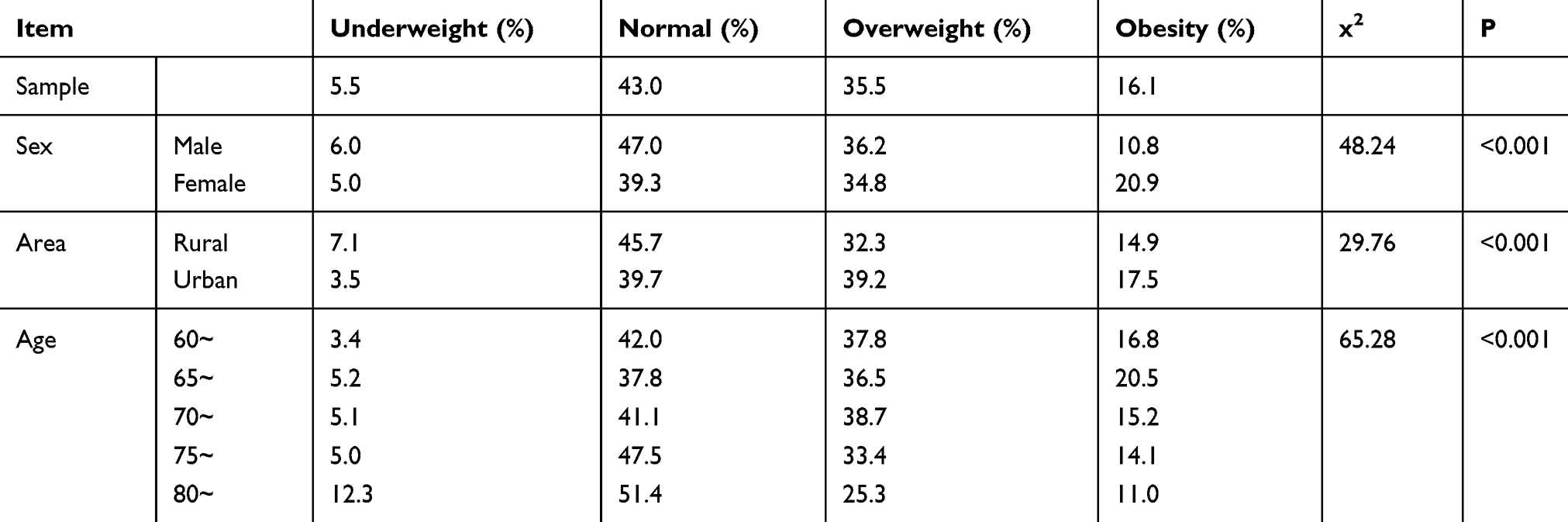 |
Table 2 The Assessment Standardized Rate of Beijing Elderly Based on Body Mass Index |
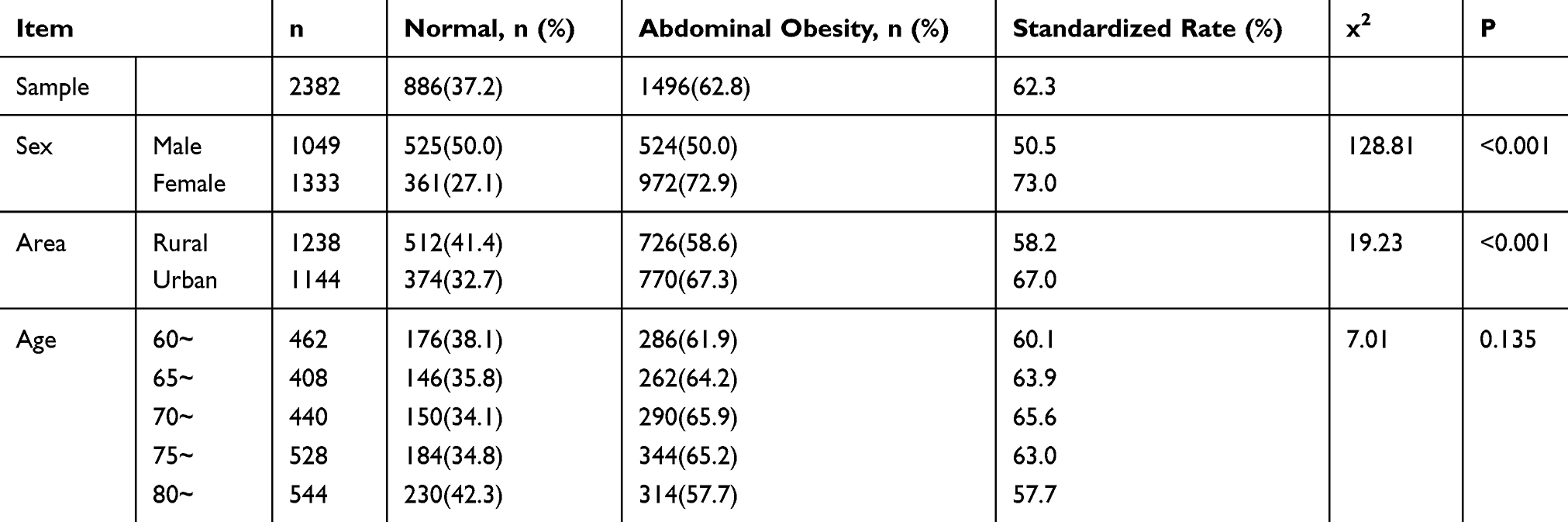 |
Table 3 The Characteristics of Obesity Based on Waist Circumference |
The prevalence of overfat based on BFP was 52.4%. Among overfat participants, there were more men than women, and more city residents than rural residents. There was a statistically significant difference in the prevalence of obesity between all age groups. The rate of overfat among adults aged 60–80 years increased with age (Table 4).
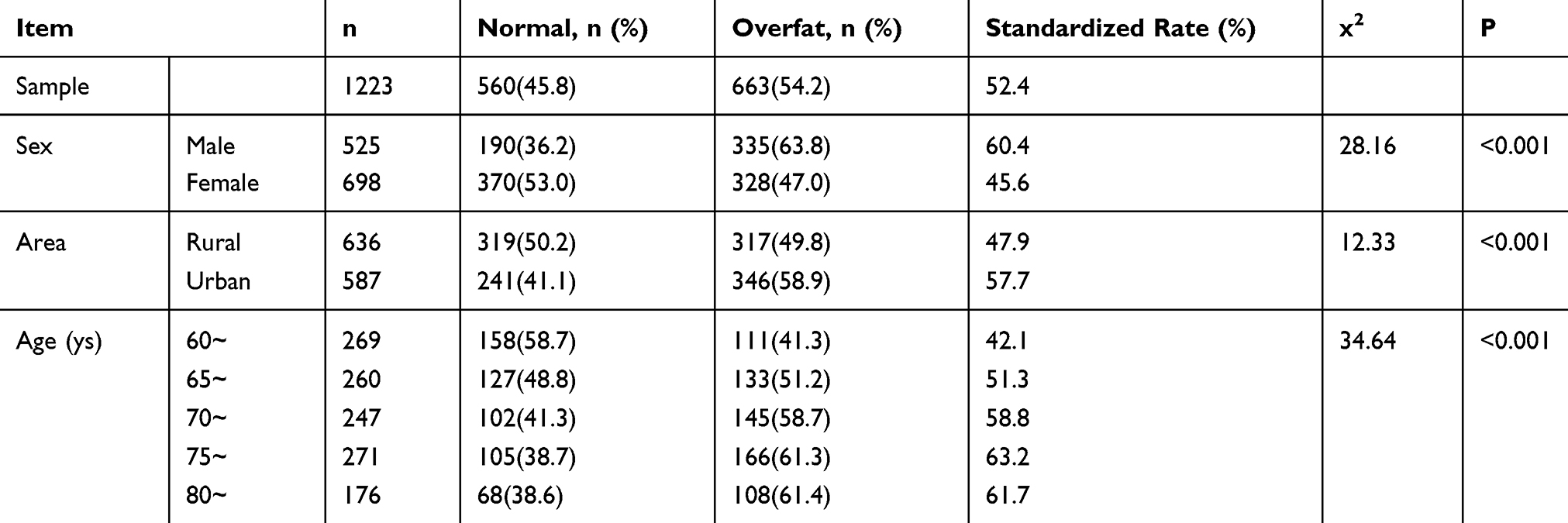 |
Table 4 The Characteristics of Obesity Based on Body Fat Percentage |
Among urban and rural residents aged 60 years and over in Beijing, the proportion of muscle type, NWO, and fatty obesity was 14.7%, 10.7%, and 41.8% separately. The proportion of participants without any type of obesity was 32.9%. Compared to female participants, male participants reported a higher prevalence of non-obese and lower prevalence of fatty obesity. The prevalence of NWO and fatty obesity among older adults living in urban areas was higher than among adults living in rural areas. The prevalence of NWO increased with age, and the prevalence of fatty obesity was highest among adults aged 70–75 years (Tables 5 and 6).
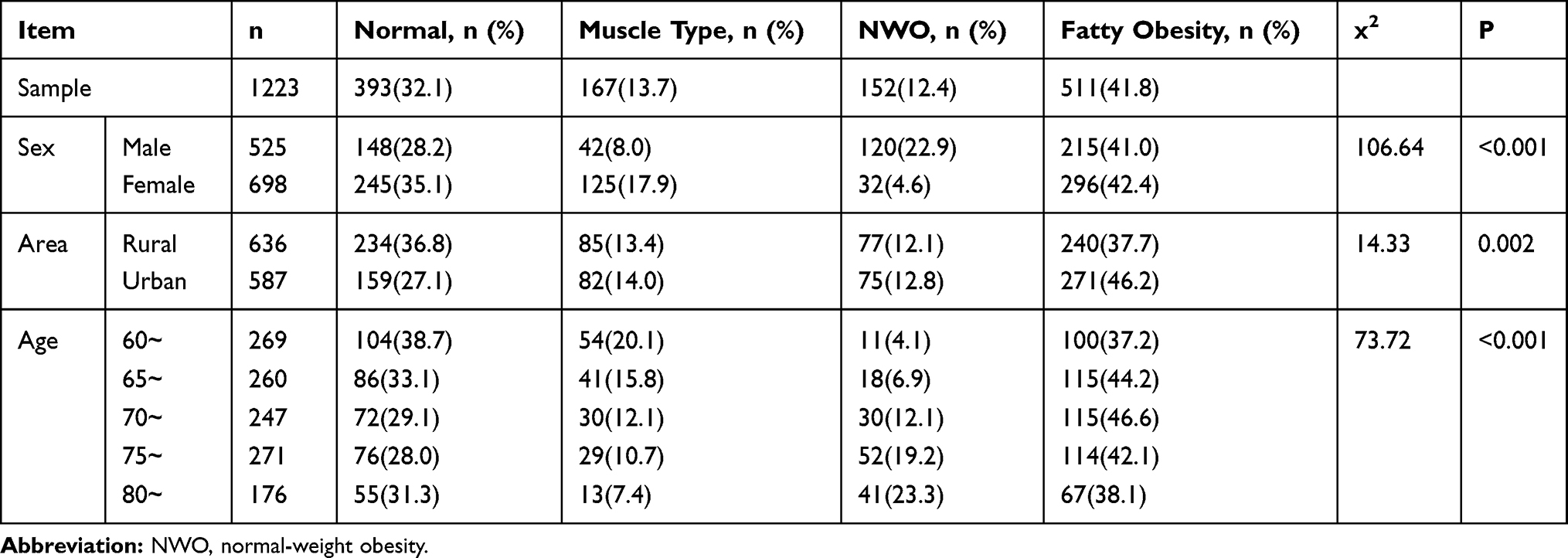 |
Table 5 The Characteristics of Obesity Based on Different Obesity Types |
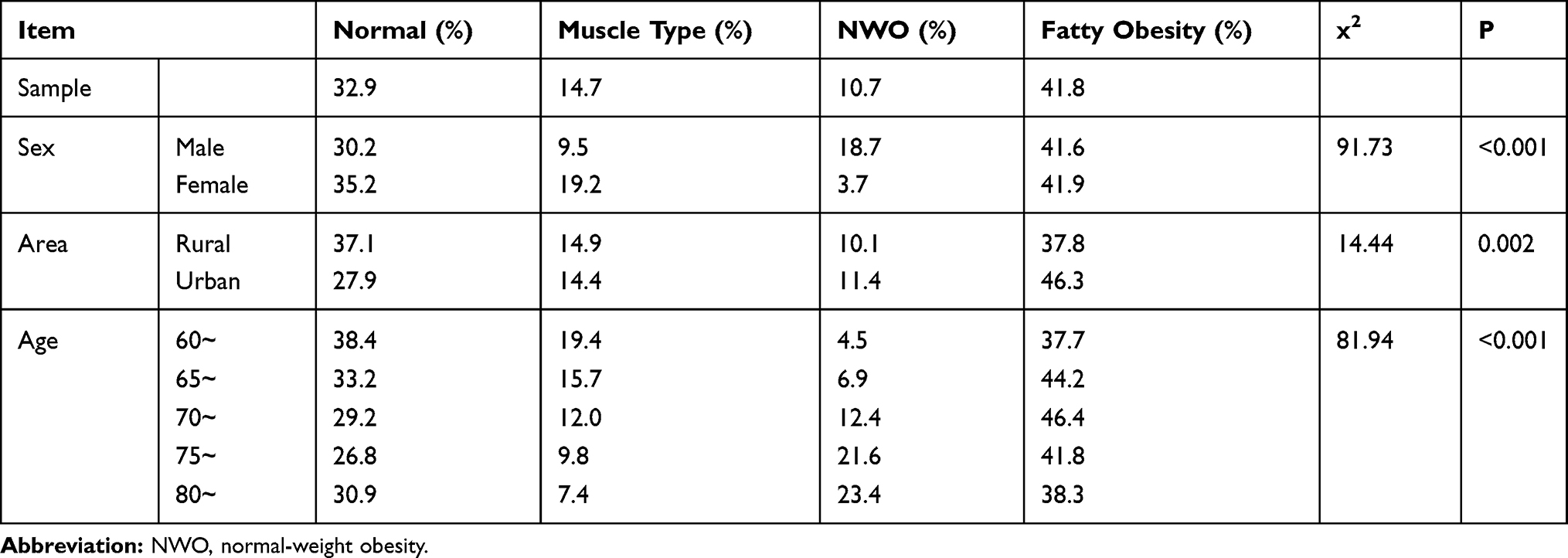 |
Table 6 The Assessment Standardized Rate of Beijing Elderly Based on Different Obesity Types |
Discussion
This study showed that more than 50% of older adults in Beijing were overweight or overfat, and reached the indices of central obesity. There were differences in the rates of obesity, central obesity, and overfat between genders as well as between urban and rural residents. Compared with the 2010 China Chronic Disease Survey,16 the overweight (33.9%) and obesity (15.5%) rates among adults over 60 years old in Beijing have increased; however, they remain lower than overweight and obesity rates for older adults in the United States (obese: 41.0%, n=4322)3 and Europe (overweight: 42.2%, obese: 20.9%, n=11,906)17 over the same period.
This study has shown that central obesity rate among adults over 60 years old in Beijing was 62.3%, which was higher than the rate reported in the NHANES study in the United States in 2011 (54.2%),18 which can be partially explained by the fact that Asian populations are more prone to accumulating abdominal fat. The incidence of abdominal obesity among the elderly in Beijing was significantly higher than that in the 2010 China Chronic Disease Survey (48.6%).16 Our results showed that the prevalence of NWO among older adults in Beijing was 10.7%, 18.7%, and 3.7% among the general population, males, and females, respectively, which was lower than comparable populations in the United States (male: 21.4%, female: 31.3%, n=4489)10 and higher than Korea (overall: 8.3%, n=3546).12
The prevalence of obesity and central obesity was significantly higher among females than among males. The rate of overfat and NWO was higher among males than among females, which was consistent with other studies of Chinese populations.11 There are several possible reasons for these findings. First, females have different social roles, and household activities traditionally assigned to females have been replaced by automated equipment, which has reduced the amount and intensity of activity. Second, postmenopausal estrogen levels decline, increasing the risk of obesity. Third, skeletal muscle, fat, bone minerals, and other body components’ composition changes with age. Studies have shown that the prevalence of sarcopenia is greater among males than among females,19 which suggests that the muscle decay rate is higher among males than among females.
The prevalence of obesity, central obesity, and overfat among adults who live within urban areas was higher than among adults living in rural areas, which was consistent with previous studies.16,20,21 Our findings show that the NWO follows a similar pattern. There are several possible explanations for these findings. First, urban residents have relatively high work pressure, irregular eating and sleeping habits, while work- and leisure-related physical activities have been overtaken by mechanical equipment, leading to an increase in time spent sitting, resulting, in turn, in a high prevalence of obesity among older adults living within urban areas. Second, the intensity of physical activity among older adults living in rural areas is higher than that of adults living in urban areas, resulting in the rural residents having higher muscle content. However, compared with rural residents, the average cultural level of the urban population is high. Therefore, it is easier to find the disease hazards, and it is easier to actively reduce the risk factors of obesity.
Our results have shown that the prevalence of obesity, central obesity, and overfat decreased with age, while the prevalence of NWO increased with age. There are several possible explanations for these findings. First, the body fat content gradually increases, while the muscle mass decreases with age; the prevalence of sarcopenia and sarcopenic-obesity increases with age.22 Second, the risk of teeth loss increases with age, resulting in reduced chewing ability, which might restrict optimum nutrition. Adults over the age of 80 years might suffer from insufficient intake of protein-based energy, leading to muscle and fat decomposition resulting in a decrease in body fat. This shows that BMI is limited in its ability to evaluate body composition, which implies that it may misrepresent true adiposity.
This study has several limitations. First, we used hand-to-hand bioelectrical impedance to measure BFP; however, its accuracy is not as good as dual-energy X-ray absorptiometry. Using the BIA is inexpensive, radiation-free, and it is a feasible method of measuring BFP, especially as part of a large-scale epidemiological investigation. Second, this study only investigated the prevalence of different types of obesity among older adults. A cohort study of the relationship between obesity and atherosclerosis among older adults is currently being developed. Third, some factors such as room temperature, hydration state, medications and time of menopause might affect the BFP, thus should be considered in further research. However, this study has a strength that the sampling method of class stratification, segmentation, randomization and cluster was adopted, which could avoid the selection bias in cross-sectional observational studies; therefore, the sample was representative of the elderly population in Beijing.
Conclusions and Implications
This study shows a high prevalence of fatty obesity, abdominal obesity, and NWO among older adults in Beijing. However, as the diagnostic criteria for NWO are not clear, a global consensus is needed before we can better understand the relationship between NWO and asthenia, disability, arteriosclerosis, and mortality. Obesity among older adults in Beijing is a significant public health concern. Older adults should be instructed to take measures aimed at reducing body fat and increasing muscle strength.
Acknowledgment
Tong Ji and Li Zhang are co-first authors for this study.
Funding
This work was supported by the National Key R&D Program of China (2018YFC2002101, 2017YFBl401202), Beijing Natural Science Foundation (7202059), and Beijing Municipal Administration of Hospitals Incubating Program (PX2020036).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Report of a WHO consultation. Obesity: preventing and managing the global epidemic. World Health Organ Tech Rep Ser. 2000;894:
2. Collaboration NCDRF. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387(10026):1377–1396. doi:10.1016/S0140-6736(16)30054-X
3. Hales CM, Fryar CD, Carroll MD, Freedman DS, Ogden CL. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007–2008 to 2015–2016. JAMA. 2018;319(16):1723–1725. doi:10.1001/jama.2018.3060
4. Shige Q, Zhihui W, Zhixin L, Limin W, Mei Z, Xinying Z. The epidemiological characteristics of obesity among the Chinese elderly population and its attributable fractions for chronic diseases. Chin J Geriatr. 2018;37(8):919–923.
5. Kim DD, Basu A. Estimating the medical care costs of obesity in the United States: systematic review, meta-analysis, and empirical analysis. Value Health. 2016;19(5):602–613. doi:10.1016/j.jval.2016.02.008
6. Juan Z, Xiaoming S, Xiaofeng L. Economic costs of both overweight and obesity among Chinese urban and rural residents, in 2010. Chin J Epidemiol. 2013;43(6):598–600.
7. Zegarra-Lizana PA, Ramos-Orosco EJ, Guarnizo-Poma M, et al. Relationship between body fat percentage and insulin resistance in adults with BMI values below 25 Kg/M2 in a private clinic. Diabetes Metab Syndr. 2019;13(5):2855–2859. doi:10.1016/j.dsx.2019.07.038
8. Yu X. Correlation between body fat percentage, visceral fat index and other cardiovascular risk factors and their aggregation in rural population of Jilin Province. Chin Circ J. 2016;31(zl):6.
9. Franco LP, Morais CC, Cominetti C. Normal-weight obesity syndrome: diagnosis, prevalence, and clinical implications. Nutr Rev. 2016;74(9):558–570. doi:10.1093/nutrit/nuw019
10. Batsis JA, Sahakyan KR, Rodriguez-Escudero JP, Bartels SJ, Somers VK, Lopez-Jimenez F. Normal weight obesity and mortality in United States subjects >/=60 years of age (from the Third National Health and Nutrition Examination Survey). Am J Cardiol. 2013;112(10):1592–1598. doi:10.1016/j.amjcard.2013.07.014
11. Jia A, Xu S, Xing Y, et al. Prevalence and cardiometabolic risks of normal weight obesity in Chinese population: a nationwide study. Nutr Metab Cardiovasc Dis. 2018;28(10):1045–1053. doi:10.1016/j.numecd.2018.06.015
12. Kim S, Kyung C, Park JS, et al. Normal-weight obesity is associated with increased risk of subclinical atherosclerosis. Cardiovasc Diabetol. 2015;14:58. doi:10.1186/s12933-015-0220-5
13. China WGoOi. Guidelines for prevention and control of overweight and obesity in adults in China (excerpt). Acta Nutr Sin. 2004;26(1):1–4.
14. Li L, Wang C, Bao Y, Peng L, Gu H, Jia W. Optimal body fat percentage cut-offs for obesity in Chinese adults. Clin Exp Pharmacol Physiol. 2012;39(4):393–398. doi:10.1111/j.1440-1681.2012.05684.x
15. Oliveros E, Somers VK, Sochor O, Goel K, Lopez-Jimenez F. The concept of normal weight obesity. Prog Cardiovasc Dis. 2014;56(4):426–433. doi:10.1016/j.pcad.2013.10.003
16. Jiang Y, Zhang M, Li Y, Li X, Wang L, Zhao W. Relationship between prevalent features of central obesity and clustering of cardiometabolic diseases among Chinese elder people. Chin Prev Med. 2013;47(9):816–820.
17. Marques A, Peralta M, Naia A, Loureiro N, de Matos MG. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur J Public Health. 2018;28(2):295–300. doi:10.1093/eurpub/ckx143
18. Ford ES, Maynard LM, Li C. Trends in mean waist circumference and abdominal obesity among US adults, 1999–2012. JAMA. 2014;312(11):1151–1152. doi:10.1001/jama.2014.8362
19. Cheng Q, Zhu X, Zhang X, et al. A cross-sectional study of loss of muscle mass corresponding to sarcopenia in healthy Chinese men and women: reference values, prevalence, and association with bone mass. J Bone Miner Metab. 2014;32(1):78–88. doi:10.1007/s00774-013-0468-3
20. Tian GB. Centre for the study of obesity gathered the elderly cardiovascular metabolism and the influence of risk factors for popular characteristics. Chin J Front Med Sci. 2014.
21. Li XY, Jiang Y, Hu N, et al. Prevalence and characteristic of overweight and obesity among adults in China, 2010. Chin Prev Med. 2012;46(8):683.
22. Zamboni M, Mazzali G, Fantin F, Rossi A, Di Francesco V. Sarcopenic obesity: a new category of obesity in the elderly. Nutr Metab Cardiovasc Dis. 2008;18(5):388–395. doi:10.1016/j.numecd.2007.10.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.