")
Back to Journals » Clinical Ophthalmology » Volume 14
Prevalence of Myopia in Newly Enlisted Airmen at Joint Base San Antonio
Authors Reed DS , Ferris LM , Santamaria J , Mehta A, Musto M, Apsey D, Legault GL
Received 1 October 2019
Accepted for publication 18 December 2019
Published 17 January 2020 Volume 2020:14 Pages 133—137
DOI https://doi.org/10.2147/OPTH.S233048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Donovan S Reed, 1 Lyndsey M Ferris, 1 Joseph Santamaria, 1 Aditya Mehta, 2 Marc Musto, 1 Doug Apsey, 1 Gary L Legault 2
1Department of Ophthalmology, Wilford Hall Eye Center, Lackland AFB, San Antonio, TX, USA; 2Department of Ophthalmology, Brooke Army Medical Center, Fort Sam Houston, San Antonio, TX, USA
Correspondence: Donovan S Reed
Wilford Hall Ambulatory Surgical Center, Department of Ophthalmology, 1100 Wilford Hall LoopLackland AFB, San Antonio, TX 78236 Tel +1 615-943-3222
Email [email protected]
Purpose: Myopia is the most common type of refractive error and can lead to significant visual impairment. The frequency of myopia has risen considerably, and its worldwide prevalence is expected to continue to increase. Myopia is present in an increasing number of Basic Military Trainees upon entry into the United States Air Force. This study aims to demonstrate the prevalence of myopia in newly enlisted members of the United States Air Force.
Methods: This study is an institutional retrospective analysis of data collected from the United States Air Force candidates entering Basic Military Training from 1 January 2017 to 31 March 2017. A random selection of 767 Air Force Basic Military Trainees were included in the analysis, yielding 1534 total eyes. The primary outcome measure studied is the mean spherical equivalent (MSE) of participants at initial evaluation. A linear regression analysis was performed to identify any associations related to participant demographics.
Results: Of participants analyzed, 45% had myopia (<− 0.5 D) and 2% high myopia (<− 6.0 D) upon entry into the United States Air Force. Myopia was found to be associated with male gender (p = < 0.001).
Conclusion: Myopia is present in a significant proportion of Basic Military Trainees upon entry into the United States Air Force, regardless of age, gender, race, or ethnicity. The prevalence of myopia presented is higher than previous studies, reflecting a continued trend towards increased myopia prevalence worldwide.
Keywords: myopia, astigmatism, refractive error, refractive surgery
Introduction
Myopia is the most common type of refractive error and can lead to significant visual impairment. The etiology of myopia is related to both genetic and environmental factors.1 Modifiable risk factors such as the ratio of near-work to outdoor activities have been implicated.2–4 Other theories of myopia development and progression that are not fovea-centric include retinal hyperopic defocus and the persistence of a non-foveal visual environment.5 Higher levels of education and socioeconomic status have also been correlated to myopia.6
The frequency of myopic individuals has risen considerably over the past few decades and its worldwide prevalence and economic burden is expected to continue to increase.7,8 The increasing prevalence of myopia has been demonstrated across the globe, including Europe and North America, and recent studies in East Asia and Europe have demonstrated an astounding myopia prevalence, particularly amongst its young adult population.9–14 Studies performed in United States populations within the last 20 years demonstrate increased prevalence, but the increase is much less than the newest East Asian and European studies have demonstrated.15 Recent data from the United States National Health and Nutrition Examination Survey demonstrated an estimated prevalence of myopia to be 33.1% in persons aged 20 years or older from 1999 to 2004.16 However, this was collected before the prevalence of myopia began to surge in other regions of the world. In another study produced by the Armed Forces Medical Surveillance Center, which focused on the incidence of diagnoses of disorders of refraction and accommodation in US active duty military members from 2000 to 2014, myopia was diagnosed at a total rate of 8.9%, but a rate of 24% in individuals 19 years or younger and 11.3% of individuals aged 20–24 years.17 Another recent study examining refractive error amongst active duty service members of all United States Armed Forces branches from 2001 to 2018 demonstrated a crude annual lifetime prevalence of 38.5% for myopia (<−0.5D), with crude overall incidence rate of 7.8 diagnoses per 100 person-years.18
The aim of this study to determine the prevalence of myopia in newly enlisted Airmen and determine its association with demographics such as age, gender, race, and/or ethnicity. Additionally, the authors hope to determine if the prevalence within this population is comparable to recent data published concerning young adults in other world populations. By understanding the prevalence of myopia amongst the newest members of the United States Air Force, the Department of Defense may better allocate the ophthalmic resources necessary to ensure a future of mission-ready eye care. Furthermore, future studies identifying modifiable risk factors could lead to the development of cost-effective interventional strategies to help prevent myopic progression in the young adult population.9,17
Methods
This is a Lackland Air Force Base Institutional Review Board approved retrospective analysis. All data to be analyzed have been obtained de-identified as part of the standard evaluation upon entry into the United States Air Force and adhered to the guidelines of the Declaration of Helsinki; as such, a waiver of consent was approved by the Lackland Air Force Base Institutional Review Board. The data were collected from evaluations of United States Air Force candidates that entered Basic Military Training from 1 January 2017 to 31 March 2017. All participants were evaluated, treated and/or followed by the Reid Optometry Clinic at JBSA-Lackland, Texas.
Inclusion Criteria
All Air Force Basic Military Trainees who underwent optometric evaluations at the Reid Optometry Clinic at JBSA-Lackland from 1 January 2017 to 31 March 2017.
Exclusion Criteria
- Participants who do not meet the inclusion criteria listed above
- Participants who previously had refractive surgery
- Participants with anisometropia >1.5 diopters
- Participants with missing or incomplete data
A blinded de-identified sampling of 800 candidates entered into basic military training during the period of 1 January 2017 through 31 March 2017 was performed. Of note, the ratio of male to female candidates examined was kept in concordance with the average rate of entry into the USAF, being approximately 3:1. As such, of the pool of candidates who entered into the USAF during this period, 550 male participants and 250 female participants were otherwise randomly selected. Demographic data examined for each participant include age at time of evaluation, gender, race, and ethnicity. Additionally, uncorrected Snellen (converted to logMAR) distance visual acuity (dVA) was collected. These data were determined by examination at the individual’s specific Military Entrance Processing Station. If the candidate’s uncorrected Snellen dVA was worse than 20/20, then the refractive error was determined by auto-refraction at either the Military Entrance Processing Station or the Reid Optometry Clinic at Lackland Air Force Base upon arrival to JBSA-Lackland. Reid Optometry Clinic staff optometrists performed a cycloplegic refraction on those candidates with high refractive error requiring a waiver for enlistment or those for whom the initial auto-refraction was unable to yield a corrected Snellen dVA of 20/20 or better. If the participant’s refractive error was determined by cycloplegic refraction via phoropter, this data were utilized in determination of the participant’s mean spherical equivalent (sphere + ½ cylinder) as opposed to the auto-refraction data.
Instrumentation
A phoropter is a non-invasive ophthalmic diagnostic system, frequently utilized in routine clinical eye care for refractive error determination. Its accuracy and precision are based on objective and subjective findings and are clinician dependent. An automated refractor is an ophthalmic device that provides an objective-only measurement of a patient’s refractive error by measuring the amount of reflection from a cone of infrared light required to properly focus an image on the patient’s retina.19 The refractions utilized in this study were conducted either manually with a phoropter or with a Zeiss VISUREF 100 ARK Autorefractor Keratometer ©.
Analysis
The cumulative data were collected and the prevalence and means in terms of the above listed variables were determined. In this study, the primary outcome measure was the refractive error of participants in terms of mean spherical equivalent (MSE) at initial evaluation. This value was utilized to estimate the prevalence of myopia in this population. Myopia and high myopia were defined as a spherical equivalent of <−0.5 diopter (D) and <−6.0 D, respectively. In addition to a simple prevalence assessment, univariate analyses comparing myopia to participant demographics were performed utilizing the Statistical Package for the Social Sciences (SPSS) statistics processing software. P-values were calculated to determine statistical significance of the data, with a p-value of <0.05 being deemed statistically significant.
Results
A total of 767 Air Force Basic Military Trainees who underwent optometric evaluations at JBSA-Lackland from 1 January 2017 to 31 March 2017 and met the above inclusion/exclusion criteria were included in the analysis, yielding an aggregate of 1534 eyes examined. Thirty-three participants originally selected were excluded from the analysis, having met one of the exclusion criteria listed. Demographic data including age, gender, race, and ethnicity are included in Table 1. The mean MSE for participants’ right eye (OD) is −1.08 ± 1.78 and for the left eye (OS) is −1.04 ± 1.78. Three hundred sixty-nine (48%) total participants were not refracted due to an entering vision of 20/20 Snellen distance visual acuity or greater without visual aids. Of participants refracted, 345 (45%) had myopia, 14 (2%) high myopia, and one participant demonstrated <−8.00D myopia. Of participants refracted, 330 (43%) demonstrated astigmatism in the right eye with a mean cylinder of −0.86 ± 0.78 and 319 (42%) with a mean of −0.91 ± 0.83, for the left eye. A total of 15 participants required a formal waiver for entry into the USAF; three for amblyopia, one for refractive error (being <−8.00D myopia), and 11 for astigmatism greater than 3.00 diopters. The results of the univariate analyses are demonstrated in Table 2. Males were significantly more myopic than females (p-value of <0.001). Race, age, and ethnicity were not found to be associated with myopia.
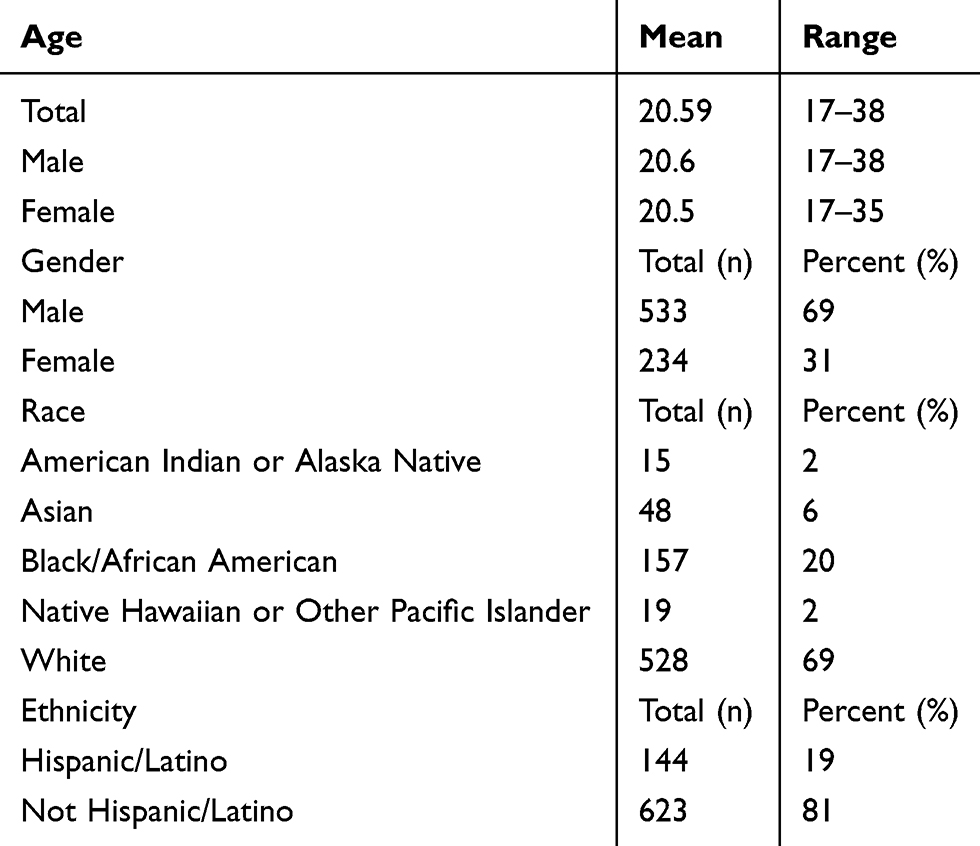 |
Table 1 Demographic Data of Participants |
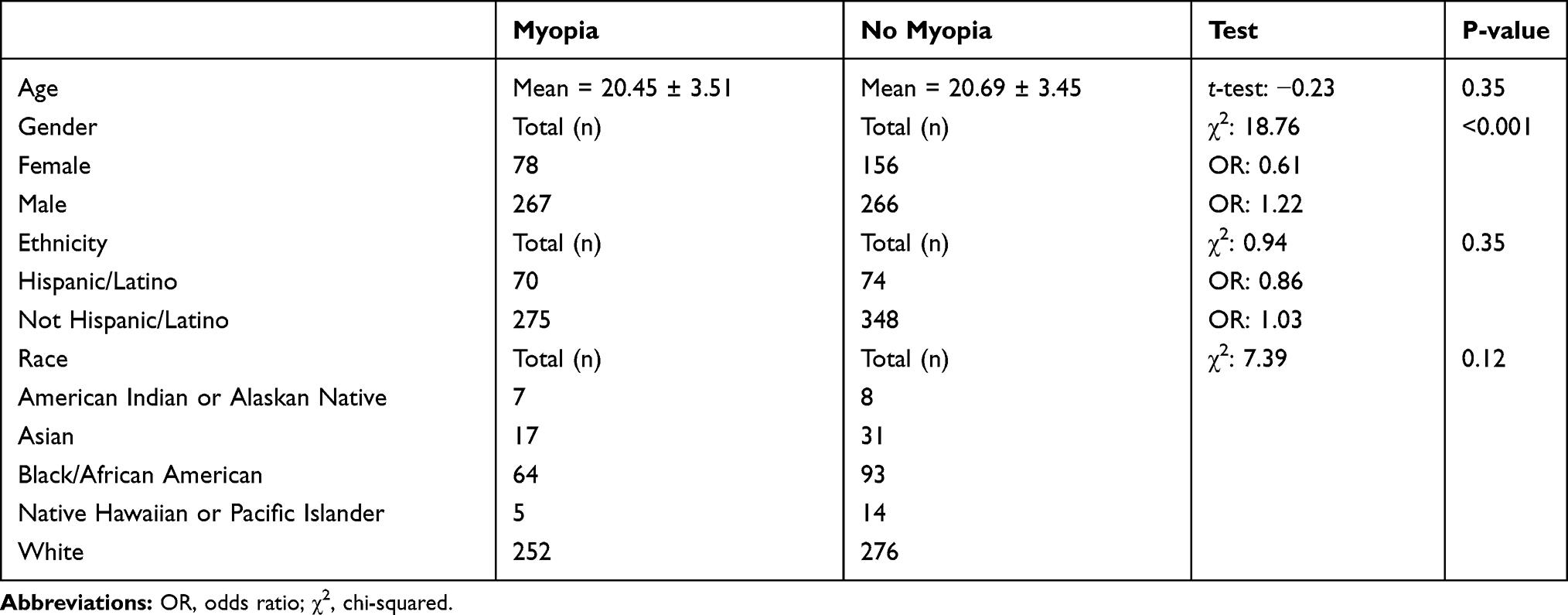 |
Table 2 Myopia versus Demographics, Univariate Analyses |
Discussion
This study reveals an increasing prevalence of myopia in newly enlisted Airmen. The myopia prevalence is comparable to a recent study performed by Wright and colleagues, which demonstrated that 41% of active duty USAF pilots utilize corrective lenses.20 Furthermore, it is similar to the analysis by Vitale and colleagues, who demonstrated an estimated prevalence of 41.6% in those aged 12–54 within the United States population.21 The results presented do, however, demonstrate higher values of myopia than another recent study examining refractive error amongst active duty service members of all United States Armed Forces branches from 2001 to 2018, which demonstrated a crude annual lifetime prevalence of 38.5% for myopia (<−0.5D).18
Interestingly, a statistically significant difference between gender and myopia was demonstrated, being more likely for male participants to have myopia. This is in direct contrast to recent studies that have reported higher rates of myopia in young adult women in comparison to men.22,23 Nevertheless, there may be an element of self-selection for young women with poor vision who assume they may be unable to pursue a career in the USAF, which could have contributed to the gender differences observed in this study. The proportion of white and American Indian participants with myopia trended to significance; however, the low numbers of underrepresented races likely limited the power to attain a statistically significant difference when comparing race to myopia. Other limitations of the study include its generalizability, as the young active duty enlisted population may differ from the young adult population of the United States at large. Furthermore, there may be an element of self-selection in terms of vision characteristics prior to enlistment into the USAF, as people with low vision, color blindness, or other visual compromises may decide not to enlist into the USAF due to assumptions of disqualification or may be disqualified prior to entry. The exclusion criteria for entry into the USAF is −8.00D of myopia without a waiver, which significantly limits the prevalence of high myopes and ultimately the total number of myopic participants present in this study population. Furthermore, auto-refractions, though demonstrated to be an accurate estimation of refractive error, still remain inferior to clinician-derived manifest refraction. Additionally, not all determinations of refractive error were performed on the same auto-refractor or phoropter. A diverse group of operators performed examinations from Military Entrance Processing Station sites across the country. This may limit the reliability of the results demonstrated. The biggest limitation of the study is the assumption that participants with uncorrected visual acuity >/= Snellen 20/20 are emmetropic, which was required to successfully perform the study.
Even considering the study’s limitations, the presented results demonstrate an increase in myopia in this young-adult population. As such, the need for increased ocular health care and vision correction via spectacles, contact lenses, and/or refractive surgery within the Department of Defense is likely to increase in the future. As there were a relatively low percentage of waivers required in this group, it is unlikely the USAF will need to modify current vision standards for entrance into the United States Air Force. Still, this concept may need to be revisited in the future for both entrance and retention standards in addition to recruitment practices.
Conclusion
Myopia is present in a significant proportion of enlistees upon entry into the USAF, regardless of age, gender, race, or ethnicity. The prevalence of myopia presented is higher than previous studies, reflecting a continued trend toward increased myopia prevalence. With nearly half of all candidates entering Basic Military Training having myopia, there are significant implications in terms of cost and resource allocation for the USAF. Establishment of early interventional strategies to reduce the burden of disease in a cost-effective manner will be key to counteracting the likely increased vision loss related to myopia in the future. Furthermore, the identification of modifiable risk factors could lead to the development of cost-effective interventional strategies to help prevent myopic progression in the young adult population.7
Disclaimer
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, Wilford Hall Ambulatory Surgical Center, The U.S. Army medical Department, the U.S. Army Office of the Surgeon General, The Department of the Air Force, The Department of the Army, Department of the Navy, or the Department of Defense or U.S. Government. The opinions expressed on this document are solely those of the author(s) and do not represent an endorsement by or the views of the United States Air Force, the Department of Defense, or the United States Government.
Acknowledgment
Jay Aiden, Ph.D. Statistician. Brooke Army Medical Center.
Funding
The authors received no external or grant funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiol Opt. 2005;25:381–391. doi:10.1111/j.1475-1313.2005.00298.x
2. French AN, Morgan IG, Mitchell P, Rose KA. Risk factors for incident myopia in Australian schoolchildren: the Syndey adolescent vascular and eye study. Ophthalmology. 2013;120(10):2100–2108. doi:10.1016/j.ophtha.2013.02.035
3. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–1285. doi:10.1016/j.ophtha.2007.12.019
4. Sherwin JC, Reacher MH, Keogh RH, Khawaja AP, Mackey DA, Foster PJ. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology. 2012;119(10):2141–2151. doi:10.1016/j.ophtha.2012.04.020
5. Berntsen DA, Barr CD, Mutti DO, Zadnik K. Peripheral defocus and myopia progression in myopic children randomly assigned to wear single vision and progressive addition lenses. Inv Ophth Vis Sci. 2013;54:5761–5770. doi:10.1167/iovs.13-11904
6. Foster PJ, Jiang Y. Epidemiology of myopia. Eye (Lond). 2014;28(2):202–208. doi:10.1038/eye.2013.280
7. Polling JR, Kok RGW, Tideman JWL, Meskat B, Klaver CCW. Effectiveness study of atropine for progressive myopia in Europeans. Eye. 2016;30:998–1004. doi:10.1038/eye.2016.78
8. Pan C-W, Ramamurthy D, Saw S-M. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32:2–16. doi:10.1111/opo.2011.32.issue-1
9. Vitale S, Sperduto RD, Ferris FL. Increased prevalence of myopia in the United States between 1971–1972 and 1999–2004. Arch Ophthalmol. 2009;127:1632–1639. doi:10.1001/archophthalmol.2009.303
10. Sun J, Zhou J, Zhao P, et al. High prevalence of myopia and high myopia in 5060 Chinese University students in Shanghai. Invest Ophthalmol Vis Sci. 2012;53(12):7504–7509. doi:10.1167/iovs.11-8343
11. Williams KM, Bertelsen G, Cumberland P, et al. Increasing prevalence of myopia in Europe and the impact of education. Ophthalmology. 2015;122(7):1489–1497. doi:10.1016/j.ophtha.2015.03.018
12. Shapira Y, Mimouni M, Machluf Y, Chaiter Y, Saab H, Mezer E. The increasing burden of myopia in Israel among young adults over a generation: analysis of predisposing factors. Ophthalmology. 2019;126(12):1617–1626. doi:10.1016/j.ophtha.2019.06.025
13. Alvarez-Peregrina CC, Sanchez-Tena MA, Martinez-Perez CC, Villa-Collar CC. Prevalence and risk factors of myopia in Spain. J Ophthalmol. 2019;2019:3419576. doi:10.1155/2019/2431481
14. Signes-Soler I, Pinero DP, Murillo MI, Tablada S. Prevalence of visual impairment and refractive errors in an urban area of Mexico. Int J Ophthalmol. 2019;12(10):1612–1617. doi:10.18240/ijo.2019.10.14
15. Saw SM, Goh PP, Cheng A, et al. Ethnicity-specific prevalences of refractive errors vary in Asian children in neighboring Malaysia and Singapore. Br J Ophthalmol. 2006;90:1230–1235. doi:10.1136/bjo.2006.093450
16. Vitale S, Ellwein L, Cotch MF, Ferris FL
17. O’Donnell F, Taubman S, Clark L. Incidence and prevalence of diagnoses of eye disorders of refraction and accommodation, active component service members, U.S. Armed Forces, 2000–2014. MSMR. 2015;22(3):11–16.
18. Reynolds ME, Taubman SB, Stahlman S. Incidence and prevalence of selected refractive errors, active component, U.S. Armed Forces, 2001–2018. MSMR. 2019;26(9):26–30.
19. Pesudovs K, Weisinger H. A comparison of autorefractor performance. Opt Vis Sci. 2004;8(7):554–558. doi:10.1097/00006324-200407000-00018
20. Wright ST, Ivan DJ, Clark LCPJ, Gooch JM, William T. Corrective lens use and refractive error among United States Air Force aircrew. Mil Med. 2010;175(3):197–201. doi:10.7205/MILMED-D-09-00047
21. Vitale S, Sperduto RD, Ferris FL. Increased prevalence of myopia in the United States between 1971–1972 and 1999–2004. Arch Ophthalmol. 2009;127(12):1632–1639. doi:10.1001/archophthalmol.2009.303
22. Dayan YB, Levin A, Morad Y et al. The changing prevalence of myopia in young adults: a 13-year series of population-based prevalence surveys. Inv Ophth Vis Sci. 2005;46:2760–2765. doi:10.1167/iovs.04-0260
23. Hyman L, Gwiazda J, Hussein M et al. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch Ophthalmol. 2005;123(7):977–987. doi:10.1001/archopht.123.7.977
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.