")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Prevalence of multiple sclerosis in Al Quseir city, Red Sea Governorate, Egypt
Authors El Tallawy H, Farghaly W , Badry R, Metwally N, Shehata G, Rageh T, Ibrahim MAAEH, Kandil M
Received 25 April 2015
Accepted for publication 27 October 2015
Published 13 January 2016 Volume 2016:12 Pages 155—158
DOI https://doi.org/10.2147/NDT.S87348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Hamdy N El-Tallawy,1 Wafaa M A Farghaly,1 Reda Badry,1 Nabil A Metwally,2 Ghaydaa A Shehata,1 Tarek A Rageh,1 Mohamed Abd El Hamed,1 Mahmoud R Kandil1
1Department of Neurology and Psychiatry, Assiut University Hospital, Assiut, Egypt; 2Department of Neurology and Psychiatry, Al Azhar University Hospital, Assiut Branch, Assiut, Egypt
Background: Multiple sclerosis (MS) is a chronic and disabling disorder with considerable social effects and economic sequelae. It is one of the major causes of disability in young adults.
Objectives: This study aimed at detecting the prevalence of MS among the population of Al Quseir city.
Methods: This study is a part of door-to-door survey of major neurological disorders that was conducted in Al Quseir city, Red Sea Governorate, Egypt. The sample size was 33,285 persons. The youngest patient was 17 years old. The number of people at and above 17 years of age was 21,827. They were screened by three neurologists. Then, the positive cases were subjected to meticulous clinical evaluation by three staff members of Department of Neurology, Assiut University Hospital, Egypt. Essential investigations were done.
Results: A total of three cases of MS were diagnosed with an age-specific prevalence ≥17 years of 13.7/100,000.
Keywords: prevalence, multiple sclerosis, Al Quseir, door-to-door survey
Introduction
Multiple sclerosis (MS) is a chronic progressive disabling disorder with marked social and economic consequences in spite of its relatively low prevalence rates. The burden of MS is higher than that for stroke and Alzheimer’s disease because of its long duration, the higher prevalence among productive young adults, and the subsequent early losses because of physical disability, fatigue, and comorbidity. Moreover, there is a major need for assisting of patients in their activities of daily living. The costs of all treatment modalities and health care are very high.1 The etiology of MS is unknown. It is a complex multifactorial disorder, in which environmental factors interact with genetically susceptible individuals.2 Diagnostic criteria require evidence of dissemination of neurologic signs and symptoms in space and time. The McDonald criteria are the diagnostic criteria, most commonly used in 66% of the countries, followed by the Poser criteria used in 31% and the Schumacher criteria used in 3% of the countries.3 The use of McDonald criteria has enabled the earlier diagnosis of MS, with increased specificity and sensitivity.4 Magnetic resonance imaging (MRI) findings must themselves meet specific criteria to be considered attributable to MS.5,6 Several scales are used to measure disability in MS. In MS epidemiological descriptive researches, the burden of disability is frequently presented as Expanded Disability Status Scale (EDSS).7
In spite of the long history of epidemiological studies of MS, the geographical distribution and the true prevalence and incidence of MS remain uncertain. Recently, a clearer understanding of the distribution of MS appeared, although the debate continues. Variations in prevalence have been associated with latitude, which is the cornerstone in this aspect.8 In a previous Egyptian retrospective meta-analysis study in different referral centers, including five centers in Cairo metropolitan, and five other centers in different governorates, the prevalence of MS in Egypt was found to be 14.1/100,000.9 This study aimed at assessing the prevalence rate of MS among the population in Al Quseir city, Red Sea Governorate, Egypt.
Materials and methods
The current study was a part of a big Egyptian project designed to study epidemiology of major neurological disorders, including MS, dementia of different types, ataxias, epilepsy, trigeminal neuralgia, migraine headache, cerebral palsy, and different types of extrapyramidal diseases in Al Quseir city, Red Sea Governorate, Egypt. It was conducted as a door-to-door survey, including every door, through three stages from July 1, 2009 to June 31, 2011.
Study area
Al Quseir city is one of the cities of Red Sea Governorate. Its surface area is 7,636 km2. It is located on the equator at 27°15″.10 Most of the people have been residents of this city since birth, yet some people are immigrants from different areas of Egypt and have settled in this city for work (the population involved in the study should have stayed for 6 months at least in the study area).11
All households (n=33,285; 7,497 families) and both sexes (49.4% [n=16,428] males and 50.6% [n=16,857] females) were screened by three neurologists, in addition to 15 female social workers (for sociodemographic data collection) via a door-to-door survey. A standardized questionnaire (with sensitivity and specificity of 96% and 93.2%, respectively) was applied by three neurologists to every member of each family (children and elderly were screened through their caregivers). A total of 31,754 (95.4%) people were free from any neurological disorder, while 1,531 (4.6%) people of both sexes (3.9% [n=647] males and 5.2% [n=884] females) had different neurological disorders.11,12
Stages of the study
Stage 1
All households of Al Quseir city were screened by three neurologists at their homes to pick up any suspected case of neurological disorders including MS. To avoid missing any person during screening, capture–recapture method was used for those who were out of their home at the time of screening. They were screened by a standardized Arabic questionnaire designed specifically for the study.13 The youngest patient with MS was 17 years old. The number of inhabitants of Al Quseir city at or above 17 years of age was 21,827, with 49.98% males and 50.02% females.
Stage 2
All suspected patients visited Al Quseir general hospital for detailed history taking, full neurological and physical evaluation by three senior staff members of Neurology Department, Assiut University Hospital, Egypt. MRI study of the brain and spinal cord was obtained according to the symptomatic presentation of each patient. Neurophysiological studies (visual evoked potential, auditory brainstem evoked potential, and somatosensory evoked potential) were also done in Assiut University Hospital, Egypt.
Revised McDonald criteria4 for diagnosis of MS cases (including clinical and neuroimaging data) were used in this study.
Stage 3
Tabulation and analysis of data, in addition to manuscript writing, were done in the Department of Neurology and Psychiatry, Assiut University Hospital, Egypt.
Data analysis
Data analysis was performed using SPSS software package version 13 (IBM Corporation, Armonk, NY, USA).
Ethics
All participating subjects gave written consent to participate in the study. This study was approved by the Ethics Committee of the Faculty of Medicine, Assiut University, Egypt.
Results
In this study, the degree of case ascertainment is of high importance. A total of three MS patients were identified from the total population with a lifetime prevalence of 9.01/100,000. As the age of the youngest patient was 17 years old, the age-specific prevalence ≥17 years is 13.7/100,000. Age- and sex-specific prevalence of MS was 27.5/100,000 (for females in the population at or above 17 years old). Table 1 shows demographic data of patients with MS. By using EDSS for each patient, we could identify the course of illness for each patient (Figure 1).
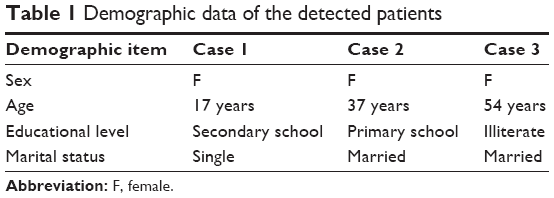 | Table 1 Demographic data of the detected patients |
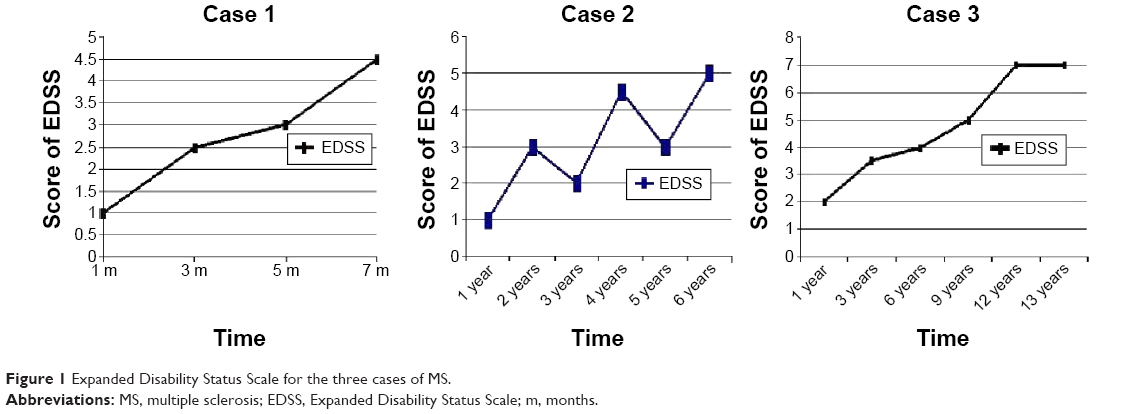 | Figure 1 Expanded Disability Status Scale for the three cases of MS. |
Case 1
A female patient, 17 years old, presented with diminution of vision, unsteadiness of gait (left cerebellar ataxia), bilateral pyramidal tract lesion, more prominent on the right side, precipitancy of micturition, internuclear ophthalmoplagia, and right upper motor neuron facial lesion since 7 months. MRI studies and evoked potentials done at the time of assessment proved the diagnosis according to the Revised McDonald criteria.
Case 2
A female patient, 37 years old, presented with diminution of vision of both eyes up to complete loss of vision on the left side (getting improved partially on steroid therapy), painful right eye movement, left hemihypethesia, including face, left-sided hemiplegia, and lost vibration sense bilaterally since 6 years. MRI studies done at the time of assessment proved the diagnosis according to the Revised McDonald criteria. The patient refused to do evoked potential studies.
Case 3
A female patient, 54 years old, presented 13 years ago with left cerebellar hemiataxia, precipitancy of micturation, throbbing headache, paresthesia on the right side of the body, bilaterally pale optic discs on the temporal side, and right pyramidal tract lesion. MRI studies and evoked potentials done at the time of assessment proved the diagnosis according to the Revised McDonald criteria.
Note: Dissemination of neurological signs and symptoms in time and place was clear in the three cases.
Discussion
In developing countries, reliable epidemiological studies of MS are lacking in spite of the previous trials in this field, thus severity, age-specific prevalence, and distribution of MS cases are unclear. In this study, the attempt to assess the prevalence of MS in Al Quseir city faced some obstacles: 1) limited number of neurologists in study area; 2) lack of availability of reliable investigation procedures in the study area; 3) lack of public awareness about MS; and 4) lack of MS comparison rates all over Egypt.
Age-specific prevalence of MS (above 17 years) in this study is 13.7/100,000, which is consistent with other studies,14,15 in which the authors stated that the prevalence of MS ranges between three and 39/100,000. The World Health Organization report about MS prevalence worldwide indicates that prevalence in Africa is 0.3; in Americas, it is 8.3; in Europe, it is 80; in South Asia, it is 2.8; and in Western Pacific, it is five.3 The probable effect of latitude may be the main factor causing the difference in prevalence between different studies.16 Mean rates tend to be higher in developed countries where the quality of disease investigations is also higher, a better accuracy in survey methodology is used, and assessments have been repeatedly conducted over time. The results of the current study are in accordance with those of a previous Egyptian retrospective meta-analysis study in different referral centers including five centers in the Cairo metropolitan area and five other centers: one center in each city of Alexandria in north Mediterranean coast, Mansoura, Tanta, and Zagazig in Delta, and Assiut in Upper Egypt which revealed that the prevalence of MS to be 14.1/100,000.9 The three detected cases, in the current study, were females and this is consistent with other studies,17,18 in which the authors assured that female-to-male ratio is 3:1. The mean exacerbation number over the last 48 weeks was 0.73, which is less than that recorded by Frohman16 who reported it to be 1.4 and this could be explained by the difference in climate between Al Quseir city and the other temperate zones. Differences in environmental exposures, and/or different genetic susceptibility underlying such differences cannot be ruled out. The positive correlation between MS prevalence and the country’s socioeconomic status can be confounded by the quality and number of epidemiological assessments conducted. Recently, a clearer understanding of the distribution of MS appeared, although the debate continues.19
Disclosure
The authors report no conflicts of interest in this work.
References
SM AIcd. Associazione author Italiana Sclerosi Multiplax. Available from: http://www.aism.it/home.aspx. 2003. Accessed September 6, 2004. | ||
Noseworthy J, Lucchinetti C, Rodriguez M, Weinshenker B. Multiple sclerosis. N Engl J Med. 2000;343:938–952. | ||
Organization WH. Atlas multiple sclerosis resources in the world. WHO Library Cataloguing-in-Publication Data. Organization WH. 2008:15–16. | ||
Chris H, Stephen C, Brenda B, et al. Diagnostic criteria for multiple sclerosis: 2010 Revision to the Mcdonald criteria. Ann Neurol. 2011;69:292–302. | ||
Barkhof F, Filippi M, Miller D, et al. Comparison of MR imaging criteria at first presentation to predict conversion to clinically definite multiple sclerosis. Brain. 1997;120:2059–2069. | ||
Tintore M, Rovira A, Martinez M, et al. Isolated demyelinating syndromes: comparison of different MR imaging criteria to predict conversion to clinically definite multiple sclerosis. Am J Neuroradiol. 2000;21:702–706. | ||
Kurtzke J. Rating neurological impairment in multiple sclerosis and expanded disability status scale (EDSS). Neurology. 1983;33:1444–1452. | ||
Pugliatti M, Rosati G, Carton H, et al. The epidemiology of multiple sclerosis in Europe. Eur J Neurol. 2006;13:720–722. | ||
Hashem S, El-Tamawy M, Hamdy S, Elmasry T. Epidemiology of multiple sclerosis in Egypt. Egypt J Neurol Psychiat Neurosurg. 2010;47(4):625–632. | ||
Saed M, Samia M, Karim A. [Center of information and decision on making, Red Sea Governorate achievement index.] 2010. Arabic. | ||
El-Tallawy H, Farghaly W, Metwally N, et al. Prevalence of neurological disorders in Al Quseir, Egypt: methodological aspects. Neuropsychiatr Dis Treat. 2013;9:1295–1300. doi:10.2147/NDT.S42392. | ||
Tallawy HN, Farghaly WM, Rageh TA, et al. Door-to-door survey of major neurological disorders (project) in Al Quseir City, Red Sea Governorate, Egypt. Neuropsychiatr Dis Treat. 2013;9:767–771. | ||
El-Tallawy H, Wafa M, Rageh T, et al. Epidemiology of major neurological disorders project in Al Kharga district, New Valley, Egypt. Neuroepidemiology. 2010;35(4):291–297. | ||
Compston A, Coles A. Multiple sclerosis. Lancet. 2002;359(9313):1221–1231. | ||
Kobelt G, Berg J, Atherly D, Hadjimichael O. Costs and quality of life in multiple sclerosis: a cross-sectional study in the United States. Neurology. 2006;66:1696–1702. | ||
Frohman E. Multiple sclerosis. Med Clin N Am. 2003;87(4):867–897. | ||
Ulku T, Mustafa T, Nese G, et al. Prevalence of multiple sclerosis: door to door survey in three rural areas of coastal black sea regions of Turkey. Neuroepidemiology. 2011;37:231–235. | ||
Trojano M, Paolicelli D, Lepore V, et al. Italian multiple sclerosis fata base network. Neurol Sci. 2006;27(5):358–361. | ||
Calabrese M, Reynolds R, Magliozzi R, et al. Regional distribution and evolution of gray matter damage in different populations of multiple sclerosis patients. PLoS One. 2015;10(8):e0135428. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.