")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Prevalence of distorted body image in young Koreans and its association with age, sex, body weight status, and disordered eating behaviors
Authors Hong S, Jung Y, Kim M, Lee C, Hyun M, Bahk W, Yoon B, Lee KH
Received 9 February 2015
Accepted for publication 4 March 2015
Published 9 April 2015 Volume 2015:11 Pages 1043—1049
DOI https://doi.org/10.2147/NDT.S82504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wai Kwong Tang
Seong-Chul Hong,1 Young-Eun Jung,2 Moon-Doo Kim,2 Chang-In Lee,2 Mi-Yeul Hyun,3 Won-Myong Bahk,4 Bo-Hyun Yoon,5 Kwang Heun Lee6
1Department of Preventive Medicine, 2Department of Psychiatry, School of Medicine, 3College of Nursing, Jeju National University, Jeju, Republic of Korea; 4Department of Psychiatry, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 5Department of Psychiatry, Naju National Hospital, Naju, Republic of Korea; 6Department of Psychiatry, College of Medicine, Dongguk University, Gyeongju, Republic of Korea
Purpose: To define the prevalence of distorted body image in 10–24-year-old Koreans and determine its relationship with sex, age, body weight status, and disordered eating behaviors.
Methods: A total of 3,227 young Koreans were recruited from elementary, middle, and high schools, as well as from universities. The participants completed a self-reported questionnaire on body image, eating behaviors (Eating Attitude Test-26), and body weight status.
Results: The prevalence of a distorted body image in males was 49.7% and that in females was 51.2%. Distorted body image was more frequent in adolescents (age, 10–17 years) than in young adults (age, 18–24 years). The highest prevalence (55.3%) was reported in female elementary school students (age, 10–12 years). Distorted body image was associated with disordered eating behaviors and abnormal body weight status.
Conclusion: These results suggest that distorted body image is a public health problem, given its high frequency in young Koreans, and that it is associated with abnormal body weight status and disordered eating behaviors.
Keywords: distorted body image, weight status, disordered eating behaviors, young Koreans, Eating Attitude Test, BMI
Introduction
Distorted body image includes several psychopathological dimensions relating to one’s own body experience, including cognitive (disturbed perceptual and visuospatial abilities to evaluate body weight and shape), affective (concerns and unhappy feelings about the body), and behavioral components (body weight control and checking behaviors, denial of weight change consequences).1 As confirmed by DSM-5 (the Diagnostic and Statistical Manual of Mental Disorders, 5th ed) criteria, distorted body image is a core and often persistent symptom in eating disorders.2 It may play a crucial role in the development of disordered eating behaviors (excess dieting, purging, and binge eating) and lead to serious psychological and medical conditions. Distorted body image has particularly detrimental impacts on the physical, psychological, and social maturation of adolescents and young adults.3,4
Although a wide range of estimates of the prevalence of distorted body image (24%–62%) has been reported based on studies using different methods in different settings,5–8 it is clear that body image distortion is a common problem among adolescents. The development of distorted body image may differ according to age, sex, and cognitive developmental status, and these differences may reflect age- and sex-related developmental processes.3 According to our knowledge, few studies have examined the difference in the prevalence of body image distortion at the population level among any age group. This cross-sectional study focused on distorted body image among young Koreans, who are just beginning to be aware of their body image, as well as disordered eating attitudes and behaviors. This study was designed to assess the prevalence of distorted body image in adolescents and young adults aged 10–24 years and its association with sex and age. We also examined associations among body weight status, disordered eating behaviors, and distorted body image by age group (10–12, 13–14, 15–17, and 18–24 years).
Materials and methods
Participants and assessment
Of 2,550 eligible adolescents, 2,342 (91.8%) were recruited from three elementary schools (grades 5–6; age, 10–12 years), three middle schools (grade 8; age, 13–14 years), and three high schools (grade 10; age, 15–17 years) located in Jeju, Korea. The target schools, selected to represent typical Korean urban public schools, volunteered to participate in the study. After gaining approval for this study, researchers visited the schools, explained the purpose of the study to the students and teachers, and obtained their consent. No incentives were provided for participation. The researchers also sent letters to the parents, introducing the study’s purpose. The letter included a statement that the parents could freely refuse to respond if they did not agree with the study’s purpose. A convenience sample of 942 college students (age, 18–24 years) drawn from two universities located in Jeju, Korea, also participated in this study. Students were enrolled in a variety of settings: university residence halls, classrooms, private residence halls, and athletic team meetings. The research assistants screened participants for eligibility, explained the purpose of the study to the subjects, and obtained informed consent. And they were available to answer questions of clarification. This study was approved by the Jeju National University Hospital Review Board. Fifty-seven subjects were excluded because their responses were incomplete, leaving 3,227 subjects for analyses.
Distorted body image was assessed using somatotype drawings, which typically consist of a set of discrete schematic figures (nine men and nine women) that range from emaciated (1) to obese (9). The validity of somatotype drawing is well established (current effect size =0.87, concurrent validity =0.61–0.75).9 The participants were asked to select the body shape that represented their current body size based on a series of nine somatotype drawings. Numbers (1–9) were assigned to subjects based on their self-reported body mass index (BMI) values. Distorted body image was defined as a difference of ≥2 between the subject’s choice and his or her actual classification.10,11
Eating attitudes and behaviors were assessed using the Eating Attitudes Test-26 (EAT-26). The EAT-26 is a widely used measure to screen subjects for disordered attitudes and behaviors related to eating.12,13 It is a self-reported measure, and scores are ranked on a 6-point Likert scale. It includes three subscales: dieting, bulimia, and food preoccupation and oral control. The reliability and validity of the Korean form of the EAT-26 have been found to be acceptable (Cronbach’s α =0.83).14 The EAT-26 cutoff point to identify the presence of disordered eating attitudes and behaviors was a score ≥20, following a previous validation study conducted in Korean adolescents.14
The study participants completed a questionnaire regarding sociodemographic and clinical characteristics, including age, sex, school grade, parental marital status, parental education level, and subjective socioeconomic status. BMI (weight [kg]/height [m]2) was calculated based on self-reported weight and height. Adolescents were classified based on BMI data from the 2007 Korean National Growth Charts by age and sex as underweight (BMI <15th percentile), normal weight (15th percentile ≤ BMI <85th percentile), overweight (85th percentile ≤ BMI <95th percentile), or obese (BMI ≥95th percentile).15 For participants who were 18 years of age or older, the following categories were created: underweight (BMI <18.5), average (BMI ≥18.5 and <25), overweight (BMI ≥25 and <30), and obese (BMI ≥30).
Data analysis
Pearson’s chi-square test was used to compare categorical data for the independent variables vs the dependent variables. Correlations between independent variables and distorted body image were investigated. Factors potentially associated with a distorted body image identified in univariate analyses were entered into a logistic regression model to assess independence. Odds ratios (ORs) and 95% confidence intervals (CIs) were derived from a series of logistic regression analyses. All statistical analyses were performed using the SPSS version 18.0 software (SPSS, Inc., Chicago, IL, USA), and a two-tailed P-value <0.05 was considered significant.
Results
The 3,227 participants included 536 (16.6%) elementary school students (grades 5–6; age, 10–12 years), 1,098 (34.0%) middle school students (grade 8; age, 13–14 years), 666 (20.6%) high school students (grade 10; age, 15–17 years), and 927 (28.7%) college students (age, 18–24 years). A total of 1,691 males (52.4%) and 1,536 females (47.6%) were included. The self-reported BMI values were 19.54±3.21 (age, 10–12 years), 20.52±3.17 (age, 13–14 years), 21.16±3.03 (age, 15–17 years), and 21.42±2.99 (age, 18–24 years).
Distorted body image was found in 50.4% of all participants, with no difference observed between males (51.7%) and females (48.3%). The prevalence of distorted body image by age group, shown in Figure 1, was as follows: 10–12 years, 52.1%; 13–14 years, 52.4%; 15–17 years, 52.6%; and 18–24 years, 45.7%. Overall, the prevalence was significantly higher in adolescents and decreased in young adults. These patterns were similar for both sexes; however, the prevalence of distorted body image increased slightly but steadily in males until the age of 15–17 years, whereas it decreased slightly but steadily in females until the age of 15–17 years. The highest prevalence (55.3%) was observed in female elementary school students, and the lowest prevalence (43.1%) was found in male college students (Figure 1). The prevalence of distorted body image in females (48.3%) aged 18–24 years was higher than that in males (43.1%) of the same age range.
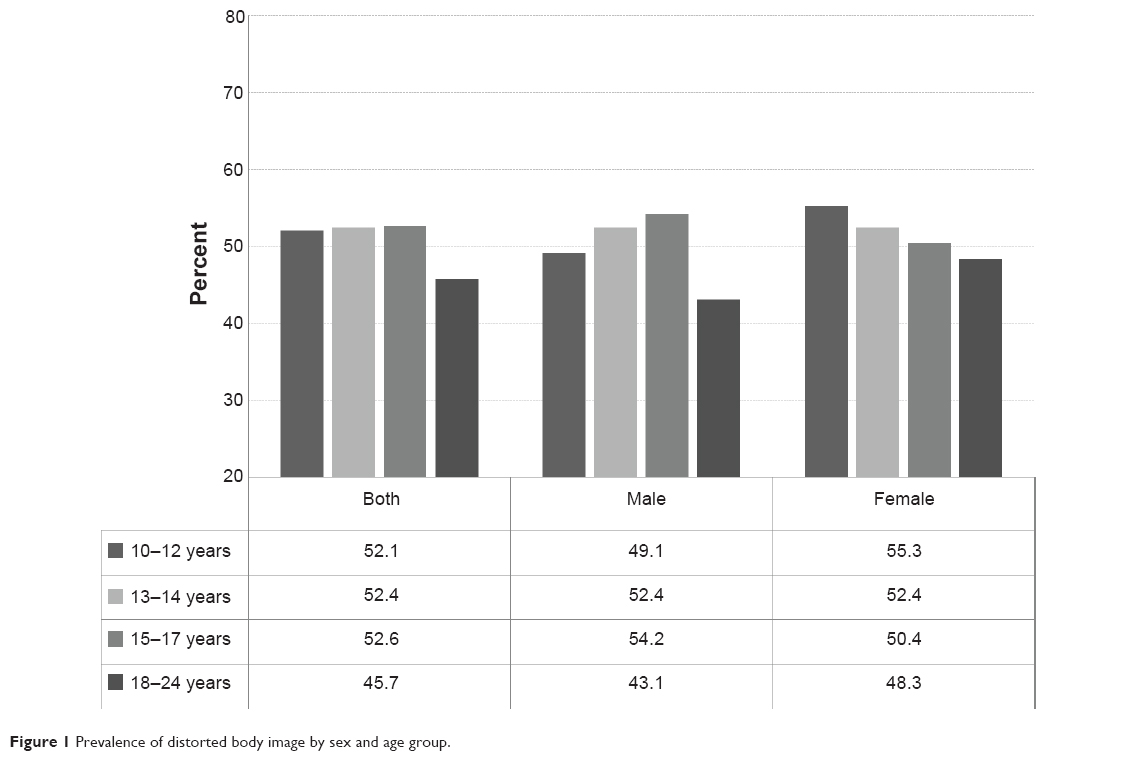 | Figure 1 Prevalence of distorted body image by sex and age group. |
Significant associations were detected between distorted body image and age group, maternal educational level, disordered eating behaviors, and body weight status (Table 1). The prevalence of distorted body image by body weight status was as follows: normal weight, 42.8% (n=1,041, underestimation: 50.2%, overestimation: 49.8%); underweight, 72.9% (n=161, underestimation: 6.2%, overestimation: 93.8%); overweight, 67.4% (n=254, underestimation: 44.1%, overestimation: 55.9%); and obesity, 88.7% (n=172, underestimation: 89.5%, overestimation: 10.5%). The prevalence of distorted body image was higher in the group with abnormal body weight than in the normal weight group (Figure 2).
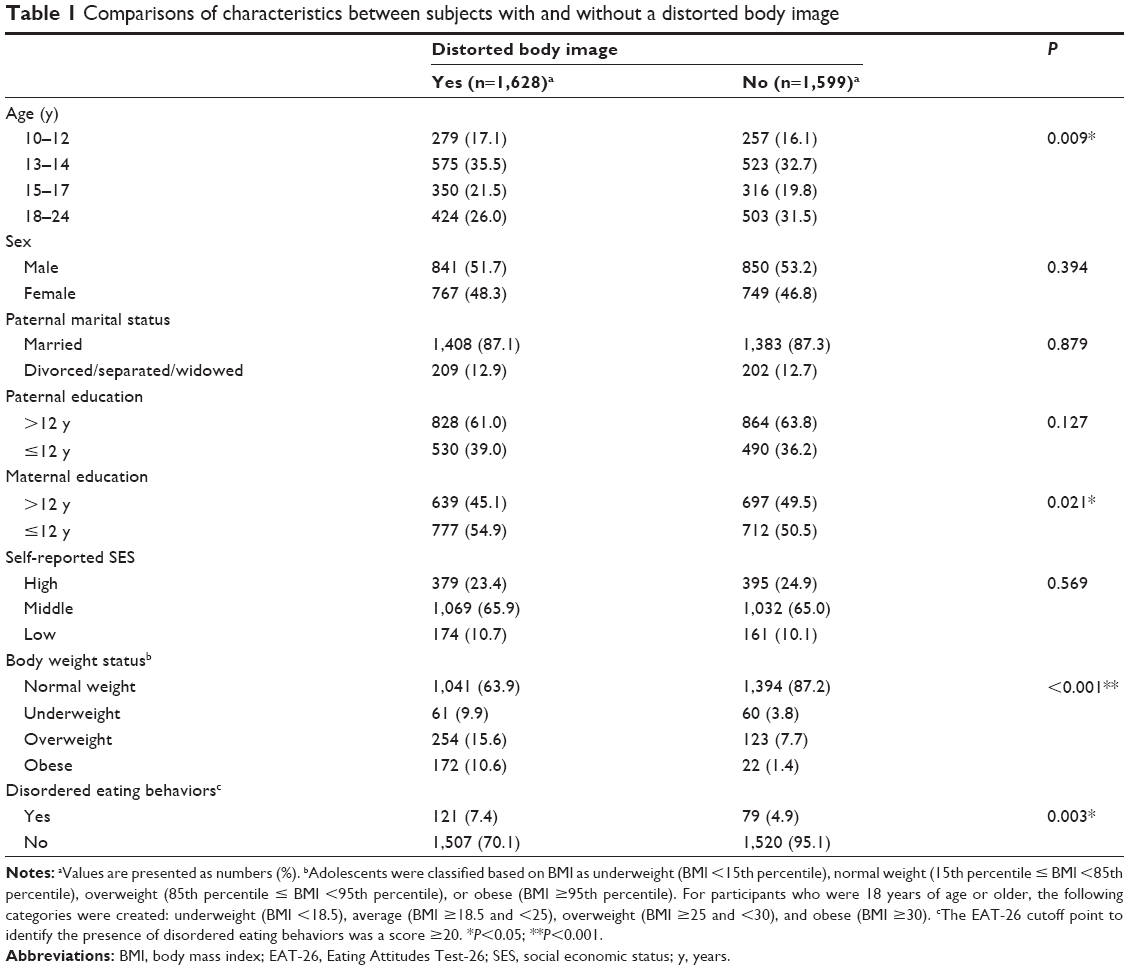 | Table 1 Comparisons of characteristics between subjects with and without a distorted body image |
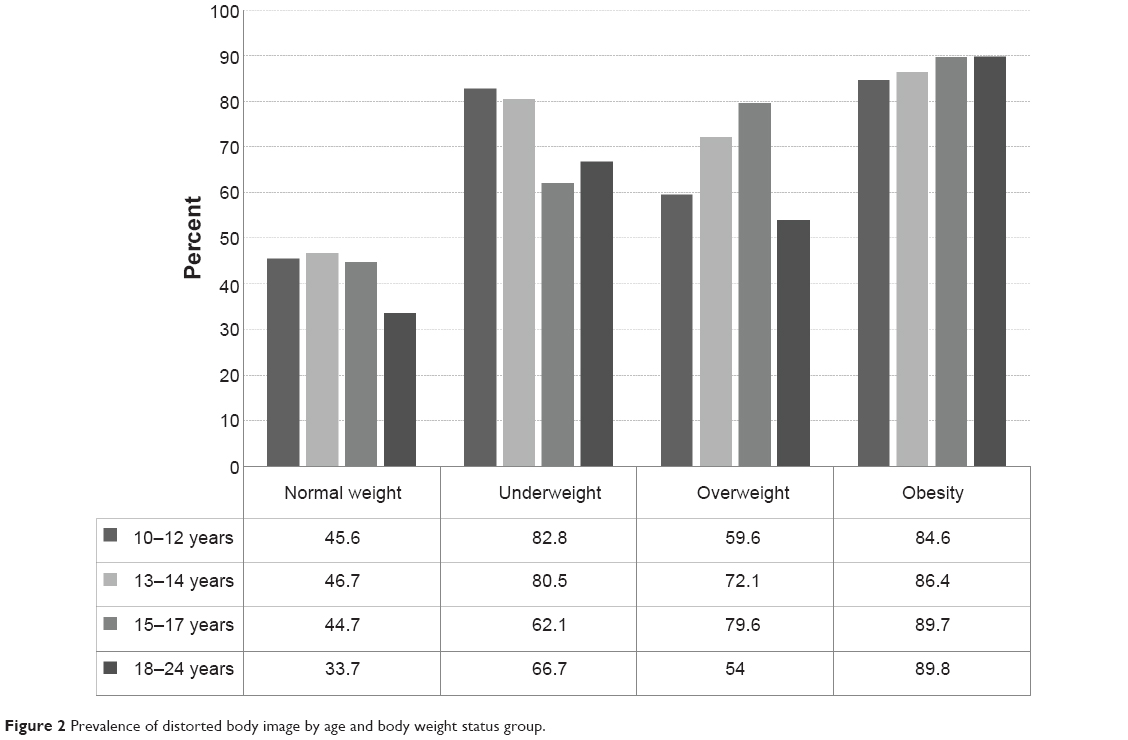 | Figure 2 Prevalence of distorted body image by age and body weight status group. |
Disordered eating behaviors were found in 6.2% of all participants. The EAT-26 scores were 6.72±6.09 (age, 10–12 years), 7.19±7.10 (age, 13–14 years), 7.18±7.53 (age, 15–17 years), and 6.86±6.13 (age, 18–24 years). There were no differences in the prevalence of disordered eating behaviors by sex (male: 5.8%, female: 6.6%) or age (10–12 years, 6.2%; 13–14 years, 6.3%; 15–17 years, 7.5%; and 18–24 years, 5.2%).
The presence of abnormal body weight was compared between the controls and subjects with a distorted body image by calculating ORs and significance levels (Table 2). The results indicated that underweight (OR, 3.87; 95% CI, 2.83–5.29; P<0.001), overweight (OR, 3.03; 95% CI, 2.40–3.84; P<0.001), and obese (OR, 13.77; 95% CI, 8.68–21.87; P<0.001) statuses were significantly related to distorted body image in all participants after adjusting for sex and age. The patterns were similar for all age groups, and were stronger in early adulthoods than in adolescents. Especially, the highest prevalence of body image distortion was observed in early adulthood with obesity (OR, 13.77). These patterns were similar for all age groups and were stronger in young adults than in adolescents. The highest prevalence of distorted body image was observed in obese young adults (OR, 13.77). Distorted body image was significantly associated with disordered eating behaviors (OR, 1.52; 95% CI, 1.14–2.04; P=0.005) after adjusting for age and sex (Table 2).
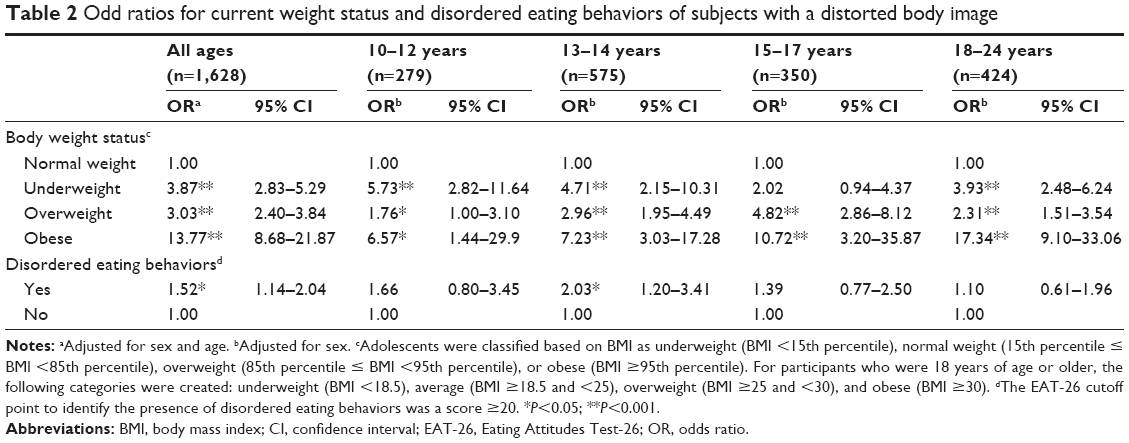 | Table 2 Odd ratios for current weight status and disordered eating behaviors of subjects with a distorted body image |
Discussion
In this study, distorted body image was common (50.4% in all age groups) in young Koreans (age, 10–24 years). The prevalence of body image distortion in our sample was higher than or similar to that (24%–62%) previously reported for adolescents.5–8 We found significant differences in the prevalence of distorted body image by age (10–12 years, 52.1%; 13–14 years, 52.4%; 15–17 years, 52.6%; and 18–24 years, 45.7%). Overall, the prevalence was noticeably higher in adolescents, and it decreased in young adults. The highest prevalence (55.3%) was observed in female elementary school students. We discovered that distorted body image peaked during adolescence and that the onset occurred at a younger age among females, specifically, in childhood or early adolescence. Distorted body image may be affected by individual differences in physical and cognitive development during childhood and adolescence.3 Several studies have shown that early puberty is associated with more body image dissatisfaction, particularly among children and adolescent girls.16–18 They may consider that changes in physical appearance and body shape (eg, body fat accumulation) during puberty deviate from the thin “ideal” body. Messages about a thin body type in the media play a key role in the development of a distorted body image and dissatisfaction. The media influence the concept of an ideal body shape, which may lead to a distorted body image in children and adolescents regardless of age or sex.19–21 Adolescence is the peak age for distorted body image; however, age differences in distorted body image are not well understood. Thus, larger-scale surveys that include more subjects from a wide age range are needed to clarify age patterns in body image distortion.
Distorted body image is clearly associated with abnormal body weight, regardless of age. Young Koreans with abnormal body weight status tended to over- or underestimate their body size; this pattern was much stronger in young adults aged 18–24 years than in adolescents. These findings suggest that actual abnormal body weight is significantly associated with body image distortion during adolescence and may be a risk factor affecting the persistence of such distortion beyond adolescence. We also found a significant association between distorted body image and disordered eating behaviors, particularly among middle school students aged 13–14 years. Previous studies have reported that adolescents with body image distortion are more likely to develop disordered eating attitudes and behaviors.22,23 Additionally, body weight status is independently associated with disordered eating behaviors.24,25 Young people with abnormal body weight may focus on the discrepancy between what is considered to be the “ideal” body shape and their perception of their own “actual” body shape. This thinking may lead to increased vulnerability to social pressure about their body and increased risk for disordered eating attitudes and behaviors. These factors, in turn, may be connected to the high prevalence of distorted body image in this group. Other factors may be involved, and interactions among multiple factors may exist. Further studies are needed to examine the causal relationships between distorted body image and related factors such as age, abnormal body weight status, and disordered eating attitudes and behaviors.
This study had several limitations. The participants comprised a convenience sample selected from several schools in a specific location; therefore, the findings may not represent all young Koreans. Distorted body image was assessed via self-reporting without corroboration by structured clinical measures. Additional studies are needed to develop good assessment measures, given the difficulties of assessing distorted body image in young people. We used self-reported data to assess disordered eating attitudes and behaviors, and it may be associated with underreporting or underestimation of symptoms of eating disorders. The absence of structural clinical interviews precluded the diagnosis of eating disorders and evaluation of comorbid psychiatric conditions. Furthermore, BMI values were also determined from self-reported data. Therefore, considerable self-report bias may have influenced our results. Finally, the cross-sectional nature of the study limited the interpretation of the results and was not optimal for investigating causal inference. These findings should be considered preliminary, and longitudinal research would be valuable to elaborate our findings and examine causality.
Conclusion
Our results indicate that body image distortion was present in approximately 50% of a sample of young Koreans aged 10–24 years. The prevalence was noticeably higher during adolescence than during early adulthood, and the highest value (55.3%) was reported in female elementary school students. Additionally, more than 40% of young adults aged 18–24 years demonstrated body image distortion; it was particularly common among those with abnormal body weight. Distorted body image was significantly associated with an abnormal body weight status and disordered eating behaviors. These findings emphasize the importance of early intervention to manage and prevent a distorted body image in young people.
Acknowledgment
This work was supported by the research grant of Jeju National University in 2011.
Disclosure
The authors report no conflicts of interest in this work.
References
Gaudio S, Quattrocchi CC. Neural basis of a multidimensional model of body image distortion in anorexia nervosa. Neurosci Biobehav Rev. 2012;36:1839–1847. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013. | ||
Littleton HL, Ollendick T. Negative body image and disordered eating behavior in children and adolescents: what places youth at risk and how can these problems be prevented? Clin Child Fam Psychol Rev. 2003;6:51–66. | ||
Thompson JK, Coovert MD, Richards KJ, et al. Development of body image, eating disturbance, and general psychological functioning in female adolescents: covariance structure modeling and longitudinal investigations. Int J Eat Disord. 1995;18:221–236. | ||
Schiefelbein EL, Mirchandani GG, George GC, et al. Association between depressed mood and perceived weight in middle and high school age students: Texas 2004–2005. Matern Child Health J. 2012;16:169–176. | ||
Park E. Overestimation and underestimation: adolescents’ weight perception in comparison to BMI-based weight status and how it varies across socio-demographic factors. J Sch Health. 2011;81:57–64. | ||
ter Bogt TF, van Dorsselaer SA, Monshouwer K, et al. Body mass index and body weight perception as risk factors for internalizing and externalizing problem behavior among adolescents. J Adolesc Health. 2006;39:27–34. | ||
Forman-Hoffman V. High prevalence of abnormal eating and weight control practices among U.S. high-school students. Eat Behav. 2004;5(4):325–336. | ||
Stunkard AJ, Sorensen T, Schulsinger T. Use of the Danish adoption register for the study of obesity and thinness. In: Kety SS, Rowland LP, Sidman RL, Matthysse SW, editors. The Genetics of Neurological and Psychiatric Disorders. New York, NY: Raven Press; 1983. | ||
Won JW, Bae JM. Quick measurement of an obesity level with somatotype drawings in outpatient clinic setting in Korea. J Korean Acad Fam Med. 1996;17:332–338. | ||
Grigg M, Bowman J, Redman S. Disordered eating and unhealthy weight reduction practices among adolescent females. Prev Med. 1996;25:748–756. | ||
Garner DM, Garfinkel PE. The eating attitudes test: an index of the symptoms of anorexia nervosa. Psychol Med. 1979;9:273–279. | ||
Garner DM, Olmstead BY, Garfinkel PE. The eating attitudes test: psychometric feature and clinical correlates. Psychol Med. 1982;12:871–878. | ||
Choi JH, Ahn DH, Nam JH, et al. Reliability and validity of eating attitude test-26 for Korean adolescents. Korean J Child Adolesc Psychiatry. 1998;9:91–97. | ||
Moon JS, Lee SY, Nam CM, et al. 2007 Korean national growth charts: review of developmental process and an outlook. Korean J Pediatr. 2008;51:1–25. | ||
Bucchianeri MM, Arikian AJ, Hannan PJ, et al. Body dissatisfaction from adolescence to young adulthood: findings from a 10-year longitudinal study. Body Image. 2013;10:1–7. | ||
Carlson Jones D. Body image among adolescent girls and boys: a longitudinal study. Dev Psychol. 2004;40:823–835. | ||
Berger U, Weitkamp K, Strauss B. Weight limits, estimations of future BMI, subjective pubertal timing and physical appearance comparisons among adolescent girls as precursors of disturbed eating behaviour in a community sample. Eur Eat Disord Rev. 2009;17:128–136. | ||
Groesz LM, Levine MP, Murnen SK. The effect of experimental presentation of thin media images on body satisfaction: a meta-analytic review. Int J Eat Disord. 2002;31:1–16. | ||
Veldhuis J, Konijn EA, Seidell JC. Negotiated media effects. Peer feedback modifies effects of media’s thin-body ideal on adolescent girls. Appetite. 2014;73:172–182. | ||
Jackson T, Chen H. Sociocultural influences on body image concerns of young Chinese males. J Adolesc Res. 2008;23:154–171. | ||
Stice E, Ng J, Shaw H. Risk factors and prodromal eating pathology. J Child Psychol Psychiatry. 2010;51:518–525. | ||
Neumark-Sztainer D, Paxton SJ, Hannan PJ, et al. Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. J Adolesc Health. 2006;39:244–251. | ||
Neumark-Sztainer D, Hannan PJ. Weight-related behaviors among adolescent girls and boys: results from a national survey. Arch Pediatr Adolesc Med. 2000;154:569–577. | ||
Goldschmidt AB, Aspen VP, Sinton MM, et al. Disordered eating attitudes and behaviors in overweight youth. Obesity. 2008;16:257–264. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.