")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Prevalence of diabetes and determinants: evidence from a minority region in People’s Republic of China
Authors Chen Q, Yi Y , Xia N , Li C, Luo Z, Huang G, Chen Y, Li S, Lai L, Wang M, Tan J, Zhang J, Shen H, Li B, Su F, Wei H, Dai X, Lu F, Li S
Received 9 June 2015
Accepted for publication 7 January 2016
Published 14 March 2016 Volume 2016:12 Pages 427—433
DOI https://doi.org/10.2147/TCRM.S90220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Qingyun Chen,1 Yanhua Yi,2 Ning Xia,1 Chunling Li,3 Zuojie Luo,1 Gaoming Huang,3 Ying Chen,1 Shumin Li,4 Luhua Lai,1 Mingdeng Wang,5 Jing Tan,6 Jie Zhang,1 Hanlei Shen,1 Bixun Li,7 Feiqun Su,8 Hua Wei,5 Xia Dai,1 Fengji Lu,9 Shuilian Li8
1Department of Endocrinology, First Affiliated Hospital of Guangxi Medical University, 2School for International Education, Guangxi Medical University, Nanning, 3Department of Public Health, Guangxi Medical University, Nanning, 4The Second People’s Hospital of Qinzhou, Qinzhou, 5Affiliated Hospital of Youjiang Medical University for Nationalities, Baise, 6Nandan County People’s Hospital, Nandan, 7Tumor Hospital of Guangxi Zhuang Autonomous Region, Nanning, 8Hezhou City People’s Hospital, Hezhou, 9Long’an County People’s Hospital, Nanning, Guangxi, People’s Republic of China
Background: This study aimed to examine the prevalence of diabetes mellitus and other categories of glucose intolerance (impaired glucose tolerance and impaired fasting glucose) and explore the risk factors in an ethnic minority region, Guangxi Zhuang Autonomous Region, People’s Republic of China.
Methods: A population-based study enrolled 53,270 residents older than 5 years in Guangxi, People’s Republic of China. The prevalence of diabetes was calculated using the 1999 World Health Organization (WHO) oral glucose tolerance test diagnostic criteria.
Results: Among 53,270 individuals, the prevalence of diabetes, impaired glucose tolerance, and impaired fasting glucose was 5.96%, 7.36%, and 2.62%, respectively. Of the 3,173 individuals with diabetes mellitus, 696 (21.94%) were found to have a history of diabetes and 2,477 (78.06%) were newly diagnosed. A lower prevalence was found in Zhuang ethnic minority people compared with the majority of Han people. The prevalence was significantly associated with age, body mass index, waist-to-hip ratio, dyslipidemia, medical history of hypertension, and family history of diabetes.
Conclusion: Guangxi shows a rapidly rising prevalence of diabetes. Weight control and blood lipid control are important to decrease the rapidly increasing prevalence of diabetes in Guangxi, an ethnic minority region.
Keywords: diabetes mellitus, ethnic minority, OGTT, diagnosis, factors, prevalence
Background
Diabetes is the major cause of morbidity and mortality in developed and developing countries. Based on the past survey conducted in 2010, 346 million people worldwide have diabetes, and an estimated 6 million are newly diagnosed annually.1,2
A previous study suggested that risk factors such as overeating, lack of physical activity, and obesity have led to a dramatic increase in the prevalence of diabetes, with very high rates in the Chinese population in the recent 30 years.3 However, it has been ~20 years since the first and second surveys of diabetes, 1980 and 1996, respectively, were conducted in Guangxi. Since China is a populous country with different ethnic groups and economic levels, the prevalence of diabetes varies widely between populations, reflecting differences in both regions and ethnicities.
Located in the south of People’s Republic of China, Guangxi Zhuang Autonomous Region (hereafter referred to as Guangxi) is a multiethnic area.4 Bordering Vietnam to the south, Guangxi has eleven ethnic minority groups, including Zhuang, Yao, Miao, Dong, Mulao, and other ethnic groups, accounting for 38% of its population, or 19.57 million people.5 The Zhuang is People’s Republic of China’s largest ethnic minority group living mainly in Guangxi. Under such context, the objectives of this study were to examine the prevalence of diabetes, impaired glucose tolerance (IGT), and impaired fasting glucose (IFG), and explore the determinants in an ethnic minority region.
Methods
Study site and study population
This survey was conducted during the period from July 2003 to December 2005 in Guangxi, and included a representative sample of the Guangxi population. Survey areas included cities (city districts) and rural areas (townships) of Nanning, Baise, Hezhou, Qinzhou, Nandan, Fengshan, Luzhai, and Longan, which are geographically distributed in the east, south, west, north, and middle parts of Guangxi. People living in their current residence for at least 5 years were included in the study.
Data collection and measurement
Trained staff collected data pertaining to demographic characteristics, personal and family medical history, and lifestyle risk factors through a questionnaire survey. The interview included questions for the diagnosis and treatment of diabetes, hypertension, dyslipidemia, and cardiovascular disease, and on the duration and amount of cigarette smoking and alcohol consumption. Blood pressure, body weight, height, waist circumference, and hip circumference were measured using standard diagnostic criteria.6 The Ethics Committee of the Guangxi Medical University approved the study protocol and written informed consent was obtained from the participants.
All the participants were required to fast overnight for more than 10 hours (if their reported fasting time was less than 10 hours, they were asked to return on another day), and were tested for fasting plasma glucose (FPG), blood serum lipid, uric acid, and fasting insulin. Plasma glucose and uric acid levels were measured using glucose oxidase method, and serum cholesterol and triglyceride levels were measured using commercially available reagents. Radioimmunoassay was used to measure blood serum insulin at the central laboratory of Guangxi Medical University. All the study laboratories were standardized and certified by the government.
Oral glucose tolerance test
After more than 3 days of dietary control, an oral glucose tolerance test (OGTT) was performed in all the participants. Participants without a medical history of diabetes were given a standard 75 g glucose solution. After 120±5 minutes, venous blood samples were collected to measure 2-hour postprandial plasma glucose level, and 2-hour postprandial capillary blood glucose level was measured using capillary fingertip blood sample. Immediate venous blood samples were collected if the capillary blood glucose was equal to or above 6.70 mmol/L. For safety reasons, participants with a medical history of diabetes were tested for FPG and/or 2-hour free-diet PPG, but OGTT was not performed in these patients. Furthermore, glucose oxidase method was used to measure plasma glucose levels.
Diagnostic criteria
The following diagnostic criteria were used to diagnose diabetes mellitus (DM), IFG, and IGT:
- The 1999 World Health Organization (WHO) diagnostic criteria were used to diagnose DM, IFG, and IGT.7 Results of plasma glucose testing were categorized as follows: normal glucose tolerance: FPG <6.1 mmol/L and 2-hour plasma glucose (2 h PG) <7.8 mmol/L; DM: FPG ≥7.0 mmol/L, 2 h PG ≥11.1 mmol/L, and with DM medical history; IFG: FPG ≥6.1 and <7.0 mmol/L with the exclusion of cases with DM history or 2 h PG ≥11.1 mmol/L; IGT: FPG <7.0 mmol/L and 2 h PG ≥7.8 and <11.1 mmol/L with the exclusion of cases with DM history.
- The Chinese obesity diagnostic criteria was used as the following: body mass index (BMI) <18.5 kg/m2 is regarded as emaciation, 18.5 kg/m2 ≤ BMI <24.0 kg/m2 as normal body weight, 24.0 kg/m2 ≤ BMI <28.0 kg/m2 as overweight, and BMI ≥28.0 kg/m2, as obese. Central obesity is defined according to the WHO standards. Males with waist-to-hip ratio (WHR) <0.90 and females with WHR <0.85 are regarded as normal, while males with WHR ≥0.90 and females with WHR ≥0.85 are regarded as having central obesity.
Statistical analysis
Age and sex-standardized prevalence were calculated by the direct method.7 Descriptive data were presented in frequency and percentage, followed by chi-square test or Fisher’s test as appropriate. Logistic regression was used to examine demographic, lifestyle, and metabolic factors accounting for diabetes and prediabetes. Data analyses were performed using R language and environment (version 3.1.0)8 and Epicalc package.9
Results
General population distribution
A total of 54,098 persons were eligible to participate in the survey. Eight hundred and twenty-eight individuals were excluded from the analysis according to inclusion criteria. The remaining 53,270 individuals were included in the data analysis. Of these individuals, 28,979 (54.4%) were men, while 24,291 (45.6%) were women. The age and sex of all individuals are summarized in Table 1. Among the 53,270 individuals, ethnical identity of 50,150 subjects was known: 15,226 (30.36%) belonged to Zhuang ethnicity, 33,347 (66.49%) to Han ethnicity, and 1,577 (3.14%) to other ethnic minorities.
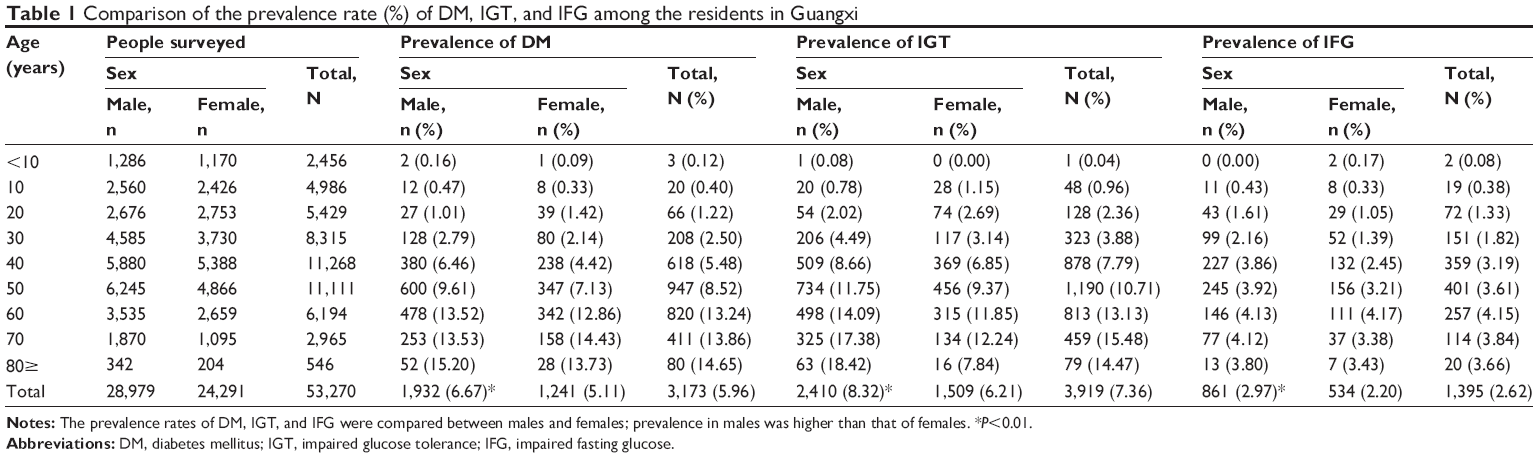 | Table 1 Comparison of the prevalence rate (%) of DM, IGT, and IFG among the residents in Guangxi |
Prevalence of DM, IGT, and IFG
The 53,270 individuals were divided into nine groups at a 10-year interval. The prevalence rates of DM, IGT, and IFG were 5.96% (standardized rate: 3.70%), 7.36% (standardized rate: 4.86%), and 2.62% (standardized rate: 1.88%), respectively. The prevalence rates were higher in men than in women (P<0.01) (Table 1). Among the 3,173 individuals with DM, 696 (21.94%) had a medical history of diabetes and 2,477 (78.06%) were newly diagnosed with diabetes.
Comparisons of prevalence in different ages
The study showed that the prevalence of DM, IGT, and IFG increased with age (Figure 1), but the prevalence of IFG was far less than that of DM and IGT. The difference in the prevalence of DM, IGT, and IFG among people with different age groups was statistically significant (P<0.01) (Table 1).
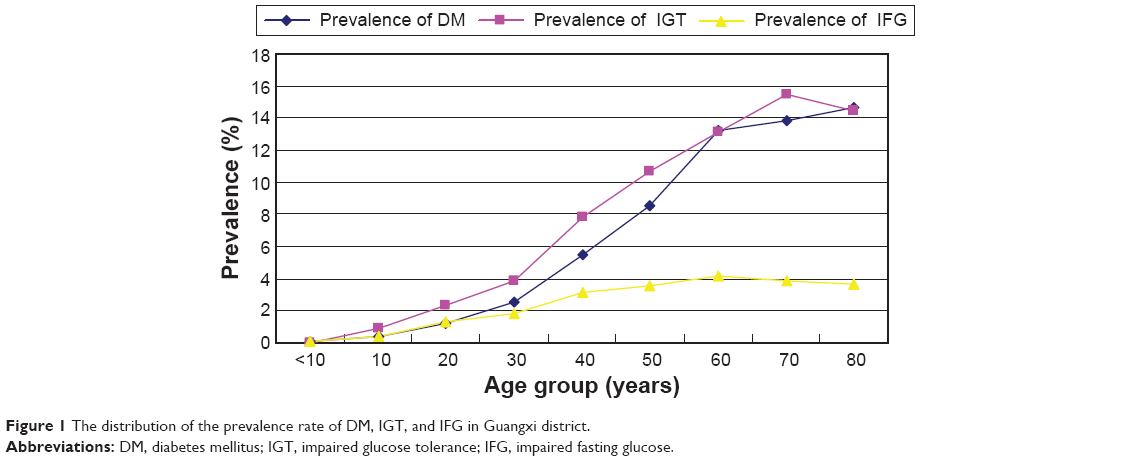 | Figure 1 The distribution of the prevalence rate of DM, IGT, and IFG in Guangxi district. |
Comparisons of prevalence in different ethnic groups
There were obvious differences in the prevalence of DM, IGT, and IFG among Han, Zhuang, and other ethnicities. The prevalence of DM, IGT, and IFG in Han ethnicity was 6.45%, 7.39%, and 2.69%, respectively, while in Zhuang ethnicity was 4.48%, 5.16%, and 2.09%, respectively. The related data showed the prevalence was higher in Han ethnicity than in Zhuang ethnicity (P<0.01). Furthermore, the prevalence was significantly higher in men than in women in Han and Zhuang ethnic groups (Table 2).
 | Table 2 Comparison of the prevalence rate (%) of DM, IGT, and IFG between different ethnic nationalities in Guangxi |
Risk factors of diabetic prevalence
Table 3 summarizes the association between risk factors and DM using a multivariable nonconditional logistic regression analysis. There was an evident age-dependent relationship between age groups and the prevalence of DM. The risks increased remarkably with old age. The association between risk factors such as hyperlipidemia history, hypertension history, and diabetes mellitus was also strong, which increased the risk by 1.85, 1.39, times compared those without the history. In addition, factors such as high BMI and abnormal WHR were also independent factors. Abnormal total cholesterol and triglyceride as well as high low-density lipoprotein levels were associated with increased risk of diabetes. People with a family history of diabetes were 3.2 times more likely to have diabetes compared with those without a family history. After adjusting for all the factors, this study showed that sex and ethnic groups were not significant risk factors for diabetes.
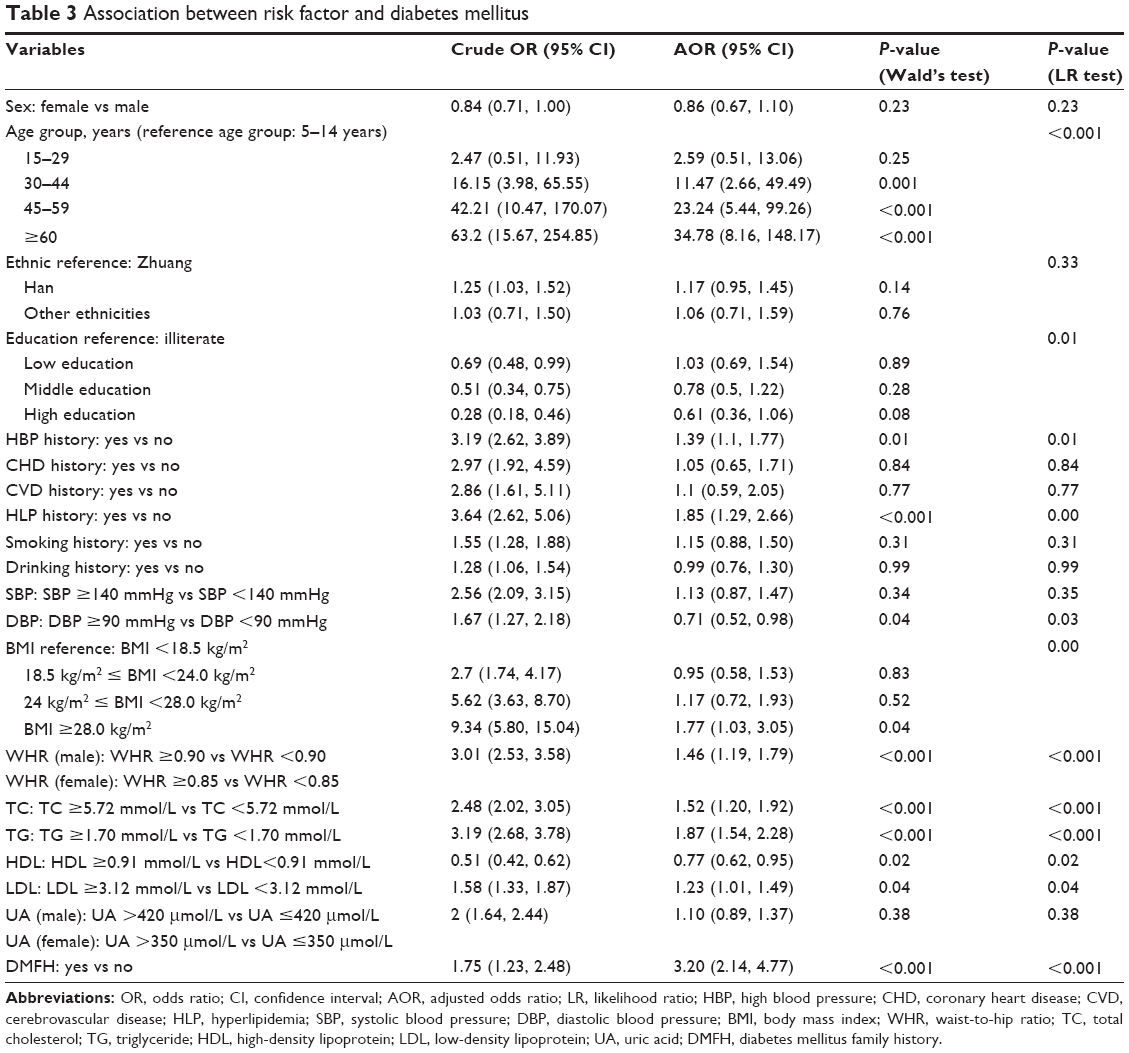 | Table 3 Association between risk factor and diabetes mellitus |
Discussion
Tendency of DM prevalence in Guangxi in 20 years
This was a large-scale epidemiological survey on DM in Guangxi, People’s Republic of China. Our survey found that the general prevalence of DM was 5.96% (taking the Chinese population in 2000 as reference) among people older than 5 years in Guangxi. For comparison, if the Chinese population in 1990 is taken as reference, the general prevalence was 0.98% in the first survey, 2.11% in the second survey, and 3.25% in the current (third) survey.6 The data presented from these surveys showed a substantial increase in the prevalence of total diabetes over these years. Increase in the prevalence of DM in Guangxi was related to the changes in lifestyle and other factors. Of the 3,173 individuals, 696 (21.94%) were found with a medical history of DM and 2,477 (78.06%) were newly diagnosed.
The general prevalence of IGT was 7.36% in this study. Compared with the past two surveys, the prevalence tendency of IGT was consistent with that of DM over the past 30 years. The general prevalence of IFG was 2.62% (the standardized prevalence was 1.88% in 2000), which was statistically significantly lower than that of IGT, indicating that the prevalence of islet function impairment was lower than that of insulin resistance.
Among people older than 15 years, the general prevalence of DM, IGT, and IFG was 6.46% (standardized rate: 4.72%), 8.00% (standardized rate: 6.08%), and 2.83% (standardized rate: 2.27%), respectively. Compared to the survey in 2002,10 the prevalence of DM and IGT was 2.52% (standardized rate: 1.43%) and 1.21% (standardized rate: 0.89%), respectively. The present standardized prevalence of DM and IGT in Guangxi is 3.3 and 6.8 times, respectively, higher than that observed in 2002. FBG testing was mainly performed in the previous study, while OGTT was performed on most participants in the present study, which improved the accuracy of diagnosis. The results of this study clearly showed that the prevalence of IGT was significantly much higher than that of IFG. The prevalence of IFG in Korea in 2001 was 23.9%.11 The difference of prevalence indicated that the increase in FPG and 2-hour postprandial blood glucose values varies across nations and districts.
The relationship between the prevalence of DM and demographic characteristics
The prevalence of DM, IGT, and IFG substantially increases with age.12–14 Söderberg et al14 reported that the peak onset time of DM was ~45–54 years, which was consistent with the findings of this study.
The body weight index including BMI and WHR had a close relationship with increase in the prevalence of DM, hypertension, and cardiovascular disease.15,16 The fact that participants with higher education level was less likely to have DM in this research was different to other studies.17
The DM prevalence was associated with ethnicity in a univariate analysis. Of 50,150 individuals in our study, 30.4% belonged to Zhuang ethnicity, 66.5% to Han ethnicity, and 3.1% to other ethnic minorities. However, after adjusting for other factors, the differences among the ethnic groups and sexes were not significant, which would merit further studies.
Risk factors of diabetic prevalence
The data showed that age, family history of diabetes, medical history of hypertension and hyperlipidemia, BMI, WHR, total cholesterol, triglyceride, and low-density lipoprotein were contributing factors to DM. High-density lipoprotein cholesterol was the protective variable of DM prevalence. Previous study also showed that excessive abdominal fat had more impact on cardiovascular disease than that in buttocks.18 WHR was the strongest independent obesity indicator associated with self-reported hypertension and diabetes.19
This study found that, despite genetic factors, the prevalence of DM in people with DM family history was 3.2 times higher than in those without DM family history. Similar results were reported in another research, which showed that the DM prevalence in immediate family relatives was 3.94%, while in the control group was 1.09%, and the relative risk was 3.62.20
Although evidence demonstrated that smokers are more likely to be diagnosed with DM than nonsmokers,21 our study showed that smoking was not a significant factor, after adjusting for other factors.
The rapid increase in the prevalence of DM, IGT, and IFG in Guangxi suggests that measures to control body weight and blood lipids would help prevent further deterioration in DM epidemiology.
Strengths and limitations
As a large-scale population-based study recently conducted in Guangxi, this study provided a strong evidence for governments and public health planners to adapt strategies for the prevention of diabetes in countries or communities with similar conditions, especially ethnic minority regions. Further studies should be conducted to learn the context factors in different ethnic groups in such an ethnic minority autonomous region with multilevel analysis.
Conclusion
This study showed an increasing prevalence of DM, IGT, and IFG in Guangxi. Weight control and blood lipid control are important to decrease the rapidly increasing prevalence of diabetes in an ethnic minority region.
Acknowledgment
This study was supported by National Natural Science Foundation of China (No. 30260042).
Disclosure
The authors report no conflicts of interest in this work.
References
King H, Aubert RE, Herman WH. Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes Care. 1998;21(9):1414–1431. | ||
WHO [homepage on the Internet]. Diabetes Fact Sheet. World Health Organization; 2012 [updated January, 2015] Available from: http://www.who.int/mediacentre/factsheets/fs312/en/. Accessed January, 2015. | ||
National Diabetes Research Group. Diabetes mellitus survey of 300,000 in fourteen provinces and cities of China. Chin Med J. 1981;20: 678–681. | ||
Huang L, Yang D, Yao L, et al. Guangxi’s rural health insurance scheme: evidence from an ethnic minority region in China. Rural Remote Health. 2013;13(2454). | ||
Ruixing Y, Yuming C, Shangling P, et al. Effects of demographic, dietary and other lifestyle factors on the prevalence of hyperlipidemia in Guangxi Hei Yi Zhuang and Han populations. Eur J Cardiovasc Prev Rehabil. 2006;13(6):977–984. | ||
Pan X-R, Yang W-Y, Li G-W, Liu J. Prevalence of diabetes and its risk factors in China, 1994. Diabetes Care. 1997;20(11):1664–1669. | ||
Zuo H, Shi Z, Hu X, Wu M, Guo Z, Hussain A. Prevalence of metabolic syndrome and factors associated with its components in Chinese adults. Metabolism. 2009;58(8):1102–1108. | ||
R Development Core Team (2015). R: a language and environment for statistical computing. Available from: http://www.R-project.org/. Accessed April, 2014. | ||
Virasakdi Chongsuvivatwong (2012). Epicalc: epidemiological calculator. R package version 2.15.1.0. Available from: http://CRAN.R-project.org/package=epicalc. Accessed September, 2012. | ||
Li LM, Rao KQ, Kong LZ, et al. [A description on the Chinese national nutrition and health survey in 2002]. Zhonghua Liu Xing Bing Xue Za Zhi. 2005;26(7):478–484. | ||
Kim S, Lee J, Lee J, et al. Prevalence of diabetes and impaired fasting glucose in Korea: Korean National Health and Nutrition Survey 2001. Diabetes Care. 2006;29(2):226–231. | ||
Yang W, Lu J, Weng J, et al. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362(12):1090–1101. | ||
Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. | ||
Söderberg S, Zimmet P, Tuomilehto J, et al. High incidence of type 2 diabetes and increasing conversion rates from impaired fasting glucose and impaired glucose tolerance to diabetes in Mauritius. J Intern Med. 2004;256(1):37–47. | ||
Wang Y, Mi J, Shan X, Wang QJ, Ge K. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes. 2007;31(1):177–188. | ||
Robbins JM, Vaccarino V, Zhang H, Kasl SV. Socioeconomic status and type 2 diabetes in African American and non-Hispanic white women and men: evidence from the Third National Health and Nutrition Examination Survey. Am J Public Health. 2001;91(1):76. | ||
Sayeed MA, Mahtab H, Khanam PA, et al. Diabetes and impaired fasting glycemia in the tribes of Khagrachari hill tracts of Bangladesh. Diabetes Care. 2004;27(5):1054–1059. | ||
Vague J. The degree of masculine differentiation of obesities a factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am J Clin Nutr. 1956;4(1):20–34. | ||
Grievink L, Alberts J, O’niel J, Gerstenbluth I. Waist circumference as a measurement of obesity in the Netherlands Antilles; associations with hypertension and diabetes mellitus. Eur J Clin Nutr. 2004;58(8):1159–1165. | ||
Wagener DK, Sacks JM, LaPorte RE, MaCgregor JM. The Pittsburgh study of insulin-dependent diabetes mellitus: risk for diabetes among relatives of IDDM. Diabetes. 1982;31(2):136–144. | ||
Foy CG, Bell RA, Farmer DF, Goff DC, Wagenknecht LE. Smoking and incidence of diabetes among US adults: findings from the Insulin Resistance Atherosclerosis Study. Diabetes Care. 2005;28(10):2501–2507. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.