")
Back to Journals » Patient Preference and Adherence » Volume 14
Prevalence of Depressive Symptoms in Patients with Type 1 and 2 Diabetes Mellitus
Authors Bąk E , Marcisz-Dyla E, Młynarska A , Sternal D, Kadłubowska M, Marcisz C
Received 8 November 2019
Accepted for publication 11 February 2020
Published 3 March 2020 Volume 2020:14 Pages 443—454
DOI https://doi.org/10.2147/PPA.S237767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Ewelina Bąk,1 Ewa Marcisz-Dyla,2 Agnieszka Młynarska,3 Danuta Sternal,1 Monika Kadłubowska,1 Czesław Marcisz3
1Faculty of Health Sciences, University of Bielsko-Biala, Bielsko-Biala, Poland; 2Department of Anxiety Disorders, Hospital of Ministry of Internal Affairs, Katowice, Poland; 3Department of Gerontology and Geriatric Nursing, School of Health Sciences, Medical University of Silesia, Katowice, Poland
Correspondence: Ewelina Bąk
Faculty of Health Sciences, University of Bielsko-Biala, ul. Willowa 2, Bielsko-Biala 43-309, Poland
Tel +48 33 827 9198
Email [email protected]
Purpose: Patients with diabetes are at increased risk of developing depression. The aim of the study was to determine the occurrence of depressive symptoms in patients with type 1 (T1DM) and type 2 diabetes (T2DM), including the association with different independent sociodemographic and clinical variables.
Patients and Methods: The studies were carried out on 618 people, including 115 patients with T1DM and 215 patients with T2DM and 288 people without diabetes constituting two control groups. Subjects were characterized in terms of sociodemographic, clinical and biochemical aspects, and the occurrence of depressive symptoms using Beck Depression Inventory (BDI) was determined. In the logistic regression analysis, the correlations between BDI score and with independent variables such as sex, age, body mass index, duration of diabetes, HbA1c level, diabetic complications and mean arterial pressure were examined.
Results: The mean BDI score was significantly higher in women and men with T1DM and T2DM compared to controls. In diabetic patients, depressive symptoms occurred more often in women than in men. Among patients with T1DM, the incidence of depressive symptoms was 17.5% of the women and 8.6% of the men and in patients with T2DM, the incidence of depressive symptoms was revealed in 28.9% of the women and in 19.8% of the men. In patients with T1DM and T2DM, the occurrence of depressive symptoms increases with age, HbA1c level and complications, and the risk of depressive symptoms turned out to be almost three times higher in women than in men with T2DM.
Conclusion: The prevalence of depressive symptoms in diabetic patients is higher than in non-diabetics. Depressive symptoms account for 13% of the patients with T1DM and 24.7% of the patients with T2DM. The risk of depressive symptoms in T1DM and T2DM increases with age, HbA1c level and the presence of complications, and it is gender-related in T2DM only.
Keywords: type 1 diabetes, type 2 diabetes, depressive symptoms, Beck Depression Inventory
Introduction
Diabetes is one of the most common chronic diseases, especially in highly developed societies. It is estimated that in Poland diabetes is diagnosed in more than 2.33 million people, including 2.15 million people with type 2 diabetes (T2DM) and 180,000 persons with type 1 diabetes (T1DM).1
The literature shows that depression symptoms were more common in patients with diabetes than in the general population. In the published meta-analysis of Anderson et al2 it was shown that in patients with T1DM and T2DM, the incidence of depression was twice as high as that observed in persons without diabetes. The majority of studies in which the occurrence of depression associated with diabetes was proven, concerned patients with T2DM. The occurrence of depression in patients with T2DM turned out to be different depending on the country of the studied population. The incidence of depression in Spaniards comprised 32.7% of the patients with T2DM and increased with age, presence of disease complications and worse glycaemic control.3 Studies in China have shown that the incidence of depression affected every third patient with T2DM, it appeared more often in people with higher levels of glycated haemoglobin (HbA1c), longer duration of diabetes, more complications and higher body mass index (BMI), in those who were lonely, had low social support and low health insurance.4 The occurrence of symptoms of depression associated with diabetes was observed in 7.5% of the patients with T2DM in Finland. These symptoms intensified in connection with the occurrence of somatic diseases, low physical activity and a loneliness.5 In studies on the Brazilian population with T2DM, coexistence of depression was demonstrated in one-third of patients in one study6 and in almost every fifth patient, more often with higher HbA1c level, in another study.7 The incidence of depression in Koreans with T2DM was 29.4%.8 The particularly frequent occurrence of depression in patients with T2DM of 40.2% was observed in the population of Pakistan, which was noted in patients with low education, concomitant diseases and more often in women.9 In the study of the Nepalese patients with T2DM, depressive symptoms were also diagnosed in a high percentage of patients (40.3%), and they occurred more often in women and increased with elevated HbA1c level, arterial blood pressure and the presence of diabetic complications.10 In patients with T2DM from 2 centers in Turkey, it was shown that about 30% of them had depression.11,12 The occurrence of depression in these patients was associated with higher HbA1c level11 and correlated positively with the duration of the disease and negatively with the level of education.12 Among patients with T2DM in the USA, depression was revealed in every fourth subject.13 In a large study involving approximately 2800 patients with T2DM from 14 countries, 10.6% were diagnosed with current major depressive disorder and 17.0% reported moderate to severe levels of depressive symptomatology.14 Current major depressive disorder was significantly associated with female sex, a lower level of education, doing less exercise, higher levels of diabetes distress and a previous diagnosis of major depressive disorder. The proportion of those with either current major depressive disorder or moderate to severe levels of depressive symptomatology who had a diagnosis or any treatment for their depression recorded in their medical records was extremely low and non-existent in many countries (0–29.6%). This international study, the largest of this type ever undertaken, shows that people with diabetes frequently have depressive disorders and also significant levels of depressive symptoms.14 In patients with T1DM Gendelman et al15 showed that every fifth patient used antidepressants, and in the non-diabetic control group, these drugs were used twice less frequently. In another study of patients with T1DM, depression was demonstrated in 14% of the subjects.16
The variation in the frequency of depression revealed in diabetic patients seems to depend on the sex of the subjects, the type of diabetes, the study procedure, source of cases and methods of depression assessment.2 In a meta-analysis of cross-sectional studies of diagnosed depression and depressive symptoms, Anderson et al2 showed that, according to various studies, the incidence of depression included from 11% of the diabetic patients, where the diagnosis was based on diagnostic interviews, up to 31% of the diabetic patients in whom symptoms of depression were determined using self-report inventories.2 These authors have noted that the prevalence of comorbid depression was significantly higher in diabetic women than in diabetic men, and depressive symptoms were more frequent in patients with T2DM compared to patients with T1DM.2
The aim of the study was to determine the occurrence of depressive symptoms in patients with T1DM and T2DM, including the association with different independent variables, such as gender, age, BMI, duration of diabetes and diabetic complications, HbA1c level and mean arterial pressure.
Materials and Methods
Participants
The study was conducted in 618 adults aged 18 to 60 years, including 330 patients with T1DM and T2DM and 288 non-diabetic controls. There were 115 patients with T1DM, including 57 women and 58 men. The group with T2DM was comprised of 215 patients, including 114 women and 101 men. Considering the fact that about 6% of the population in Poland suffer from diagnosed diabetes1 with the assumption that the maximum error is 10% and the confidence level is 95%, the minimum sample sizes were estimated to be 96 persons for T1DM and 97 persons for T2DM. Thus the size of the investigated sample was sufficient for the analysis. Control groups for T1DM included 43 women and 62 men, and for T2DM – 94 women and 89 men. The selection of study participants was carried out randomly. The female patients were selected out of 87 randomly chosen patients with type 1 diabetes. The male patients were selected out of 78 randomly chosen patients with type 1 diabetes. The controls for T1DM were selected out of 73 randomly chosen healthy women and 82 randomly chosen healthy men. The female patients were selected out of 151 randomly chosen patients with type 2 diabetes. The male patients were selected out of 145 randomly chosen patients with type 2 diabetes. The controls were selected out of 126 randomly chosen healthy women and 124 randomly chosen healthy men. The reason for reducing the number of patients and the controls qualified for further studies were incompletely filled surveys. The inclusion criterion for the studied group of patients was the prevalence of diabetic patients included after 1 year of diagnosis. The study excluded persons who had an inflammation in the last 3 months, with gestational diabetes, were diagnosed with depression, cancer, diseases of the endocrine glands or alcoholism, person taking psychotropic drugs, immunosuppressive drugs, glucocorticoids or anti-inflammatory drugs, and those who did not consent to the study. Treatment with T1DM consisted basically on diet and insulin, and treatment with T2DM – on diet and sulfonylurea and biguanide, and insulin in some patients. Comorbidities and diabetes complications were diagnosed by specialist physicians, mainly internists, cardiologists, neurologists, nephrologists, diabetologists and ophthalmologist. All of the ill studied subjects were patients of the Regional Hospital in Bielsko-Biala (the Diabetic Unit), the Diabetic Unit of the Medi-Diab Non-Public Medical Center, and the Diabetic Unit in Katowice.
Persons assigned to control groups did not declare diagnosed chronic diseases and did not use drugs and fasting glucose was normal. Controls were recruited at the primary care clinics during routine periodic medical examinations.
The study was carried out from March 2016 to January 2017. To carry out the study, the approval of the Bioethics Committee of the Beskid Medical Chamber in Bielsko-Biała was obtained at the meeting on 11 February 2016 (no approval 2016/02/11/1).
All procedures performed in the study involving human participants were in accordance with the ethical standards of the committee and with the 1964 Declaration of Helsinki. Written informed consents were obtained from all individual participants included in the study.
Methods
In all subjects, fasting glycemia in blood was determined. In patients with diabetes HbA1c level was determined. The systolic and diastolic blood pressure was measured.
The sociodemographic and clinical characteristics of the subjects were analyzed, which included parameters such as age, sex, place of residence, education, marital status, occupational activity, body mass and height with the calculation of BMI, use of alcohol and cigarettes, co-morbidities, duration of diabetes, occurrence of diabetes complications and used medications.
The occurrence of depression symptoms was determined using Beck Depression Inventory (BDI).17 BDI is a screening tool for assessing the severity of depressive symptoms. The scale consists of 21 questions rated from 0 to 3 points, which correspond to the increasing intensity of symptoms. The results obtained in BDI range between 0 and 63. The threshold score used to identify a depression was ≥16.18 BDI is a standardized and validated questionnaire, repeatedly used in mood disorder assessments, with a high reliability index (Cronbach α coefficient was 0.92–0.93).17 Cronbach α value of BDI for our results was estimated in patients with T1DM at the level of 0.916 for women and 0.857 for men and in patients with T2DM at the level of 0.873 for women and 0.928 for men, showing high good internal consistency.
Statistical Analysis
The statistical calculations were carried out using the Statistica 10.0 StatSoft program. In the analysis of the quantitative variables, Student’s t-test was used, and when none of the variables met the assumptions of the parametric model (normality of distribution, homogeneity of variances) the Mann–Whitney U-test was used. In the analysis of qualitative variables, the following tests were used: Chi-square, Chi-square with Yates correction, Fisher test. Based on the logistic regression model, in the examined patients with diabetes, it was determined which of the analyzed variables (sex, age, BMI, duration of diabetes, HbA1c level, diabetic complications and mean arterial pressure) could have a significant impact on the occurrence of depression disorders. The value of p<0.05 was assumed to be the statistical significance level.
Results
The patients with T1DM, including women aged 31.5 ± 8.9 (mean ± SD) years and men aged 28.2 ± 7.1 years. The group with T2DM including women aged 51.1 ± 9.7 years and men aged 53.4 ± 6.8 years. Controls for T1DM included women and men aged 27.7 ± 6.8 and 29.5 ± 6.9 years, respectively, and for T2DM – women and men aged 50.2 ± 5.9 and 51.3 ± 5.7, respectively. Patients with T2DM, both men and women, were older than those in control groups (p<0.05–0.01) (Tables 1 and 2).
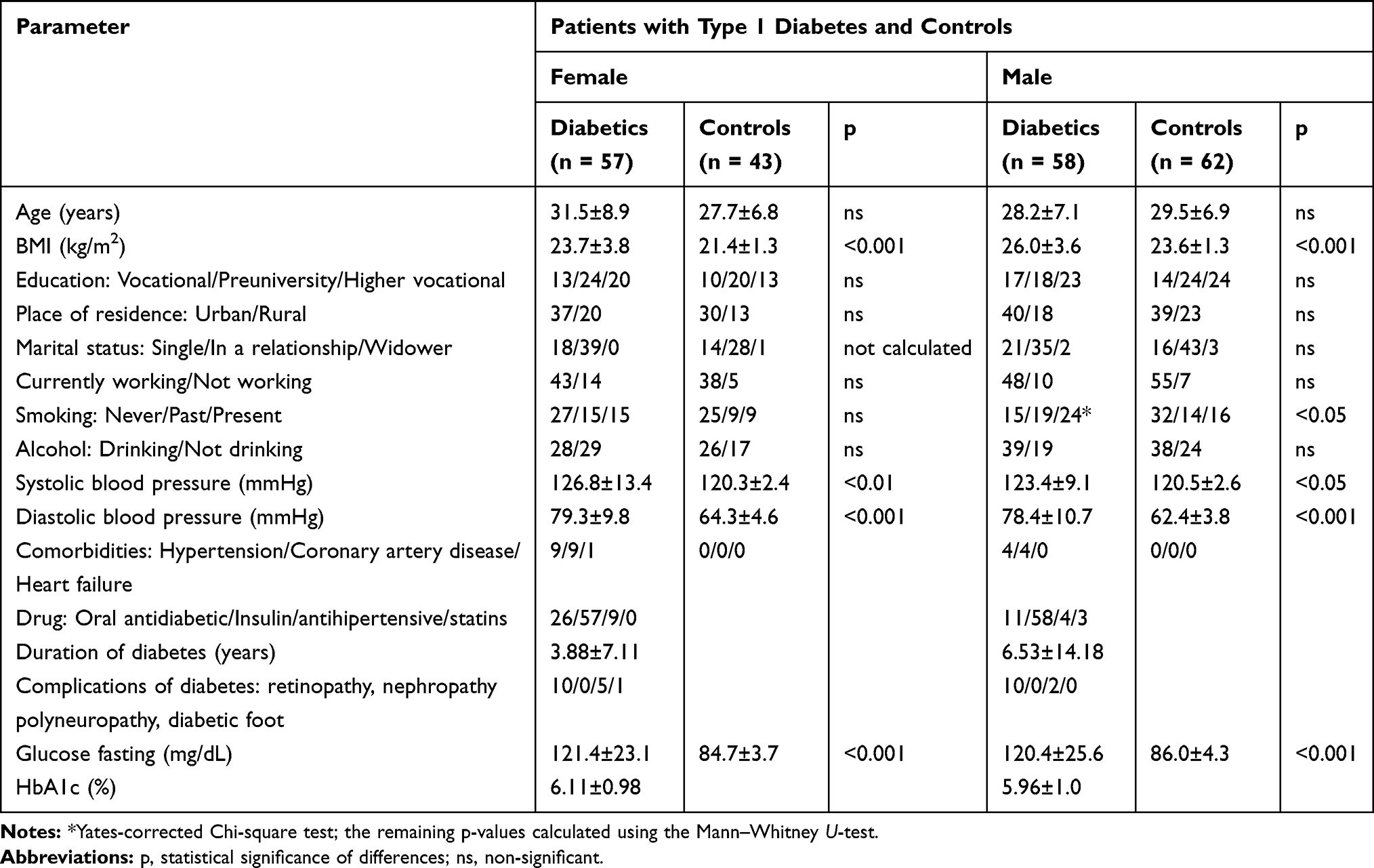 |
Table 1 Sociodemographic, Clinical, Biochemical Characteristics of Patients with Type 1 Diabetes and Controls |
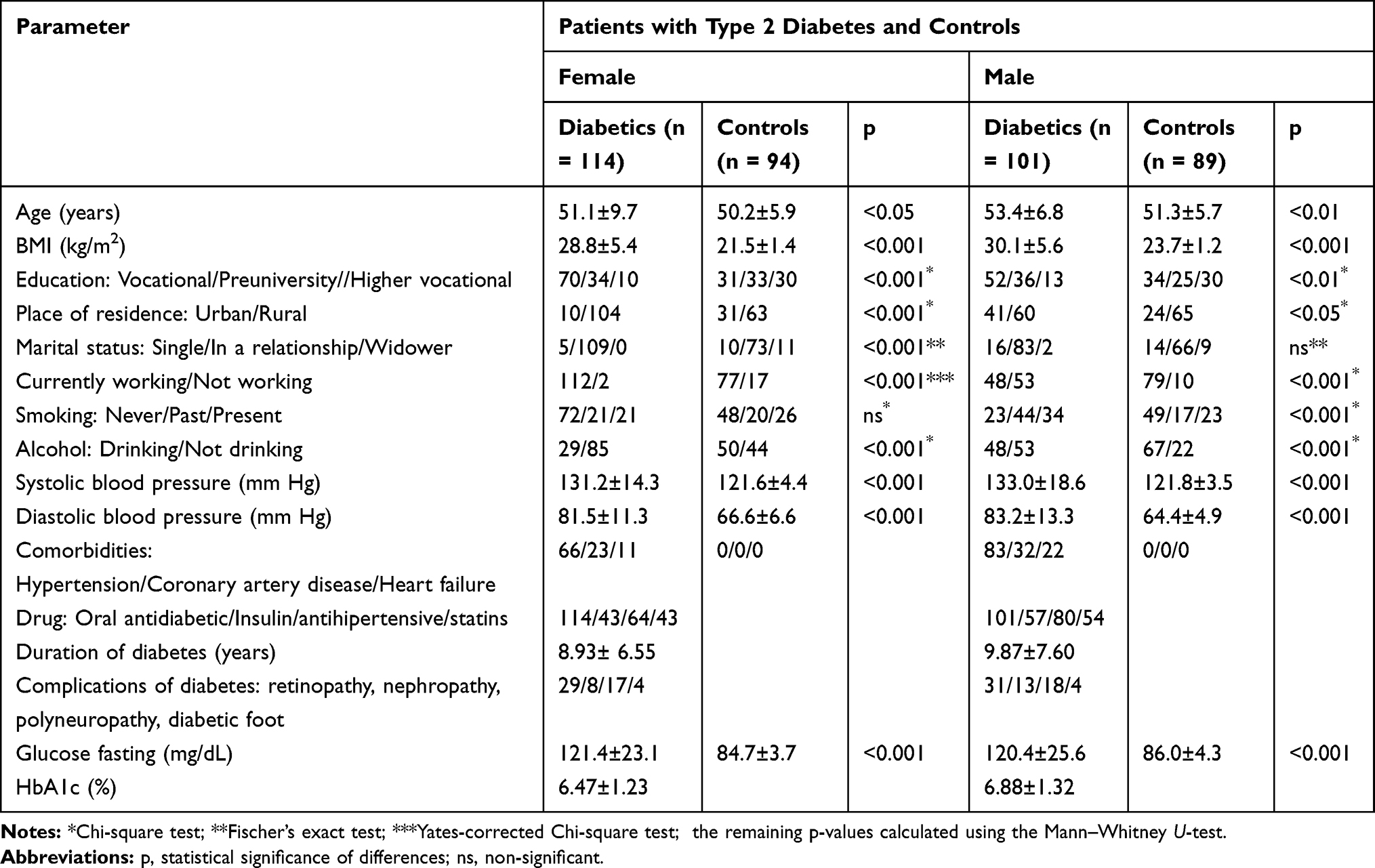 |
Table 2 Sociodemographic, Clinical, Biochemical Characteristics of Patients with Type 2 Diabetes and Controls |
The sociodemographic, clinical and biochemical characteristics of the subjects are presented in Tables 1 and 2. Patients with diabetes had a higher BMI than comparable controls (p<0.001). Compared with control subjects, patients with T2DM differed in their level of education (p<0.01–0.001), place of residence (p<0.05–0.001), marital status in women (p<0.001), work (p<0.001), smoking in the group of men (p<0.001) and drinking alcohol (p<0.001). In patients with T1DM and T2DM, higher systolic and diastolic blood pressure (p<0.05–0.001) were found than in controls (Tables 1 and 2). HbA1c levels <7% were in 81% of the women and 83% of the men with T1DM and in patients with T2DM – in 78% of the women and 67% of the men. HbA1c levels in other diabetic patients were ≥7%.
The mean BDI score was significantly higher in women and men with T1DM and T2DM than in corresponding control groups (p<0.001; Table 3). The mean BDI score in both women and men was 7 in T1DM and 11.5 in T2DM. The incidence of depressive symptoms determined with a BDI score ≥16 was significantly higher in diabetic patients than in control subjects (p<0.01–0.001). In diabetic patients, depressive symptoms occurred more often in women than in men (Table 3). Among patients with T1DM, the incidence of depressive symptoms was 17.5% of the women and 8.6% of the men, and in patients with T2DM, the incidence of depressive symptoms was revealed in 28.9% of women and in 19.8% of men.
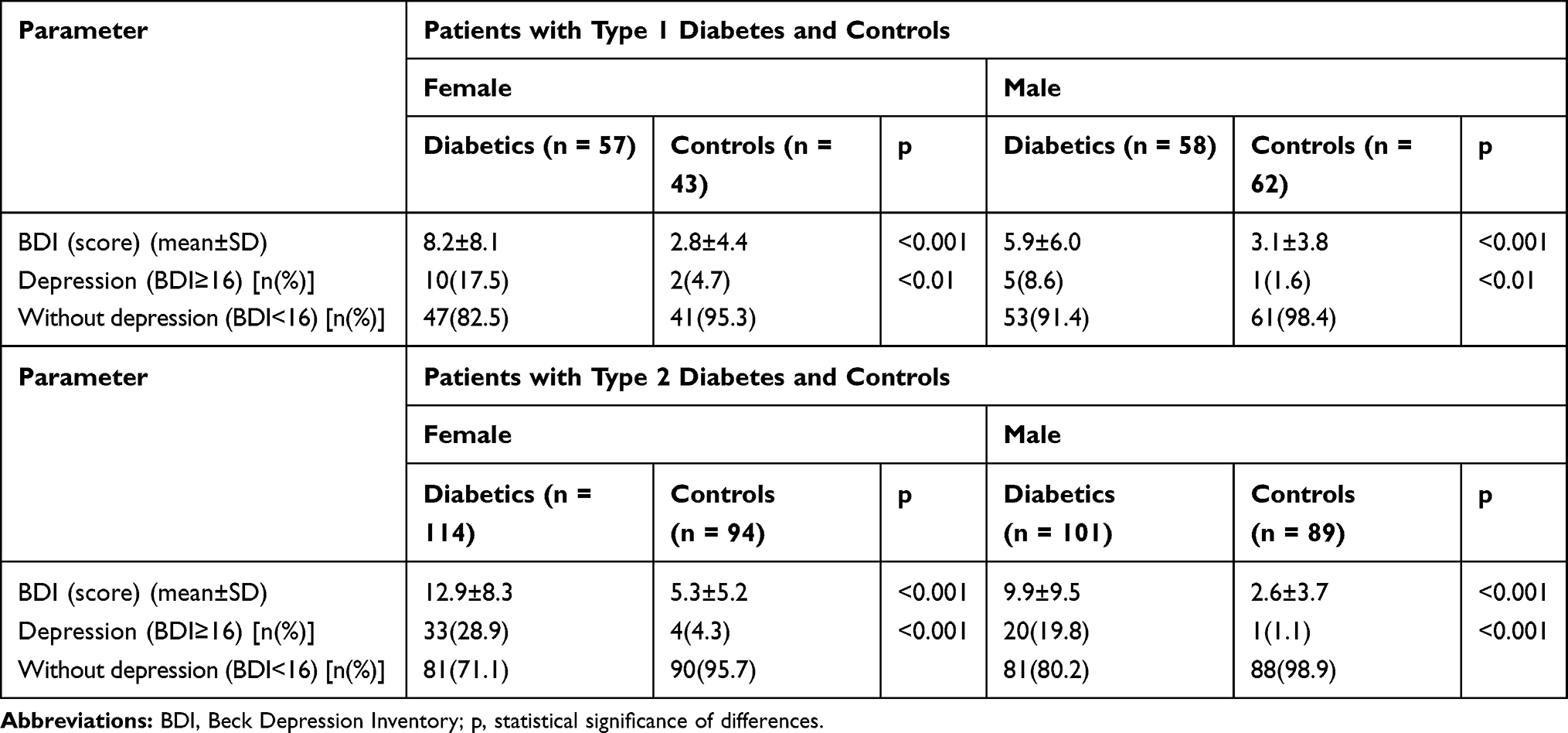 |
Table 3 Prevalence of Depression in Patients with Diabetes and Controls |
The next stage of the study was to take into account all the components of BDI and to show the variation in the frequency of their occurrence in diabetic patients in comparison with control subjects. In women with T1DM sadness, pessimism, agitation, loss of interest, indecisiveness, worthlessness, irritability, tiredness or fatigue and loss of interest in sex were significantly more common than in women in the control group (p<0.05–0.001; Table 4). In the analyzed men with T1DM, such BDI components as pessimism, loss of energy, irritability, changes in appetite and tiredness or fatigue were observed more frequently than in control men (p<0.05–0.001; Table 4). On the other hand, the frequency of depressive symptoms in patients with T2DM and control subjects turned out to be more varied than that of the control group compared with the patients with T1DM (Tables 4 and 5). Women with T2DM more often than control women reported symptoms, such as sadness, pessimism, past failures, loss of pleasure, self-criticalness, crying, agitation, loss of interest, indecisiveness, loss of energy, changes in sleeping pattern, irritability, changes in appetite, tiredness or fatigue, and loss of interest in sex (p<0.05–0.001) (Table 5). In men with T2DM, the incidence of sadness, pessimism, past failure, loss of pleasure, guilty feeling, punishment feeling, self-dislike, crying, agitation, loss of interest, indecisiveness, worthlessness, loss of energy, changes in sleeping pattern, irritability, changes in appetite, tiredness or fatigue, and loss of interest in sex was greater than in the control group (p<0.05–0.001) (Table 5).
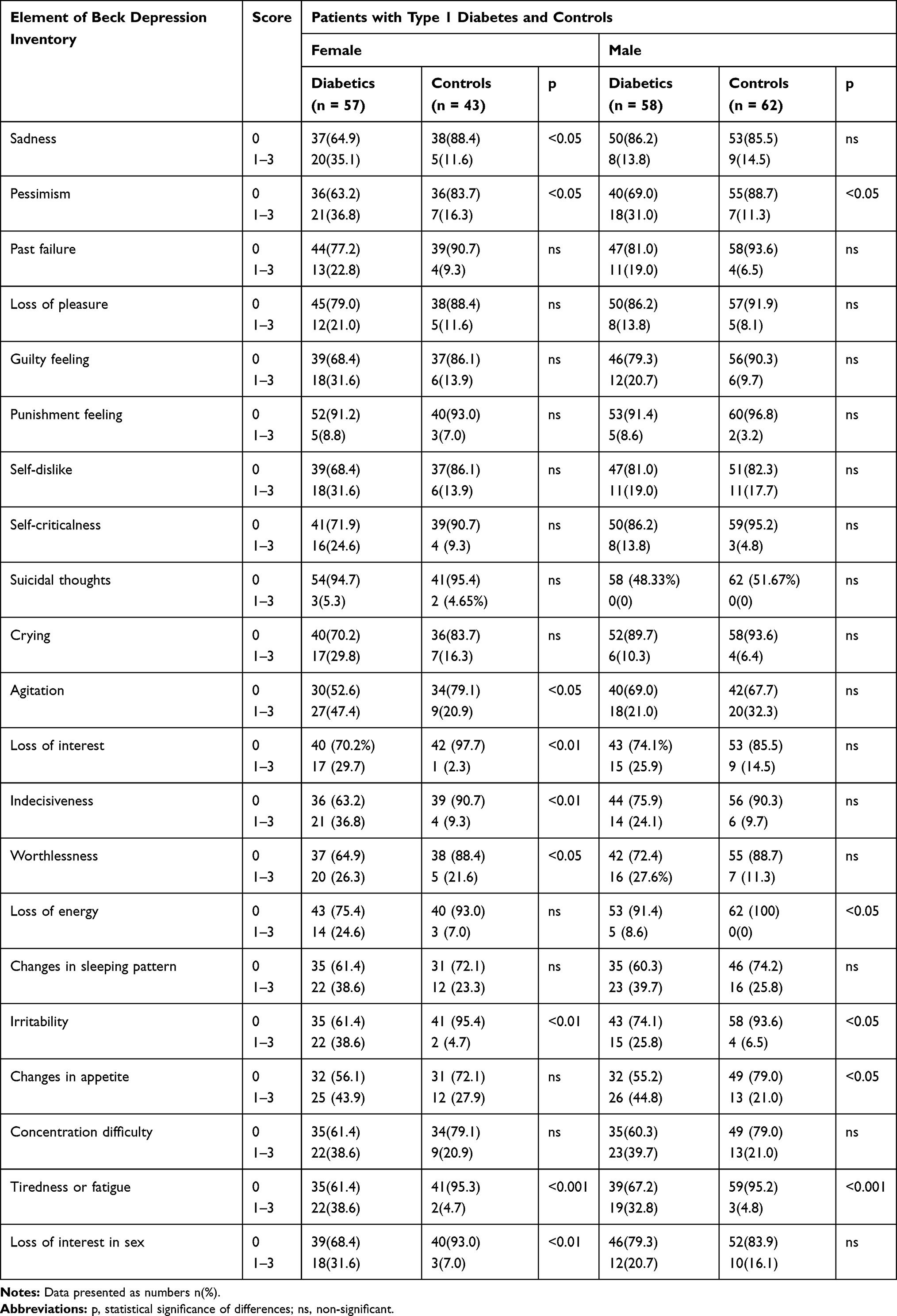 |
Table 4 Prevalence of Depressive Symptoms in Patients with Type 1 Diabetes and Controls |
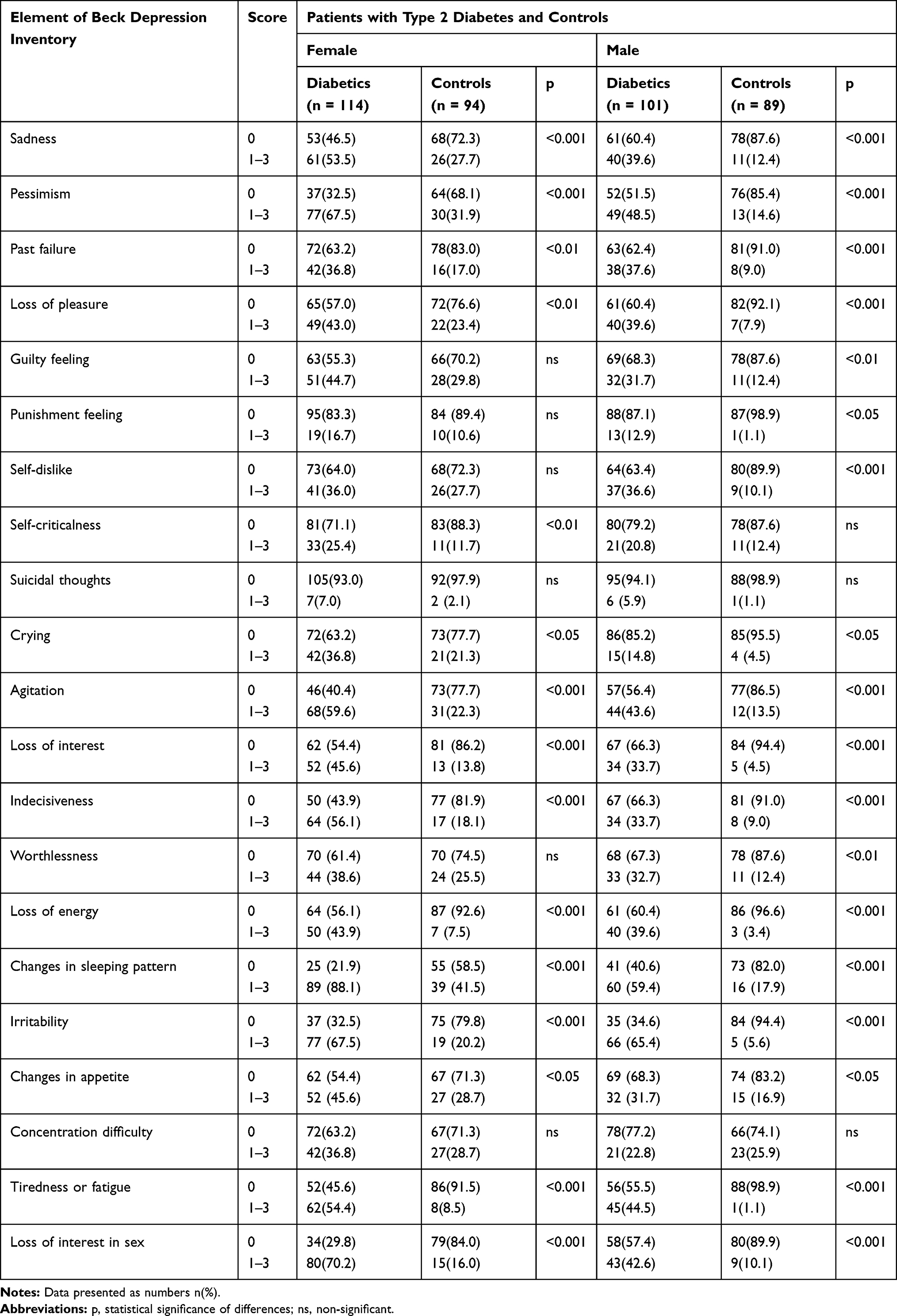 |
Table 5 Prevalence of Depressive Symptoms in Patients with Type 2 Diabetes and Controls |
The results of the logistic regression analysis of the obtained BDI values in diabetic patients in connection with independent variables, such as sex, age, BMI, duration of diabetes, HbA1c level, diabetic complications and mean arterial pressure, are presented in Table 6 and Figure 1.
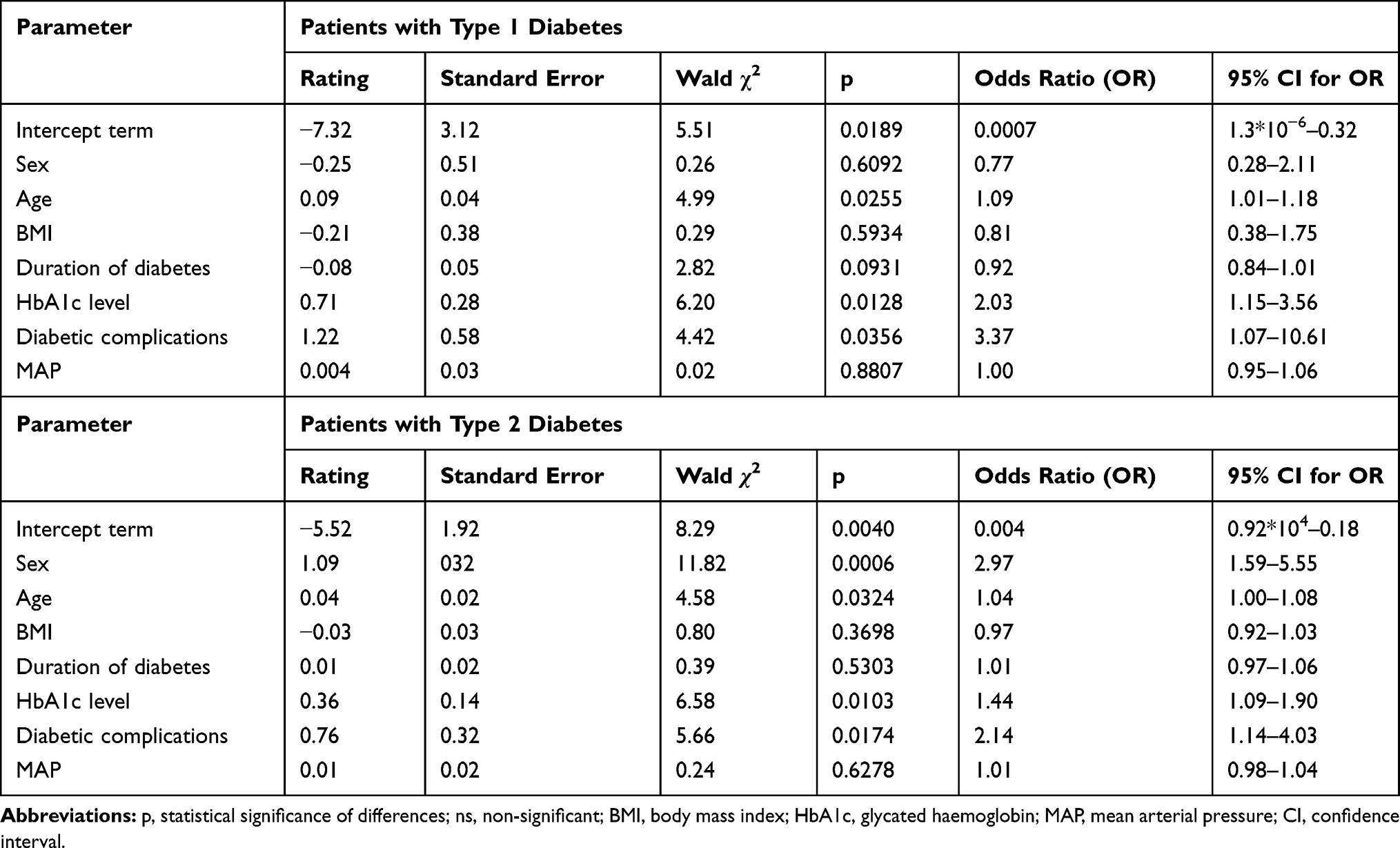 |
Table 6 Results from the Logistic Regression Analysis of Values of Beck Depression Inventory in Diabetics Depending on the Presence of Independent Variables |
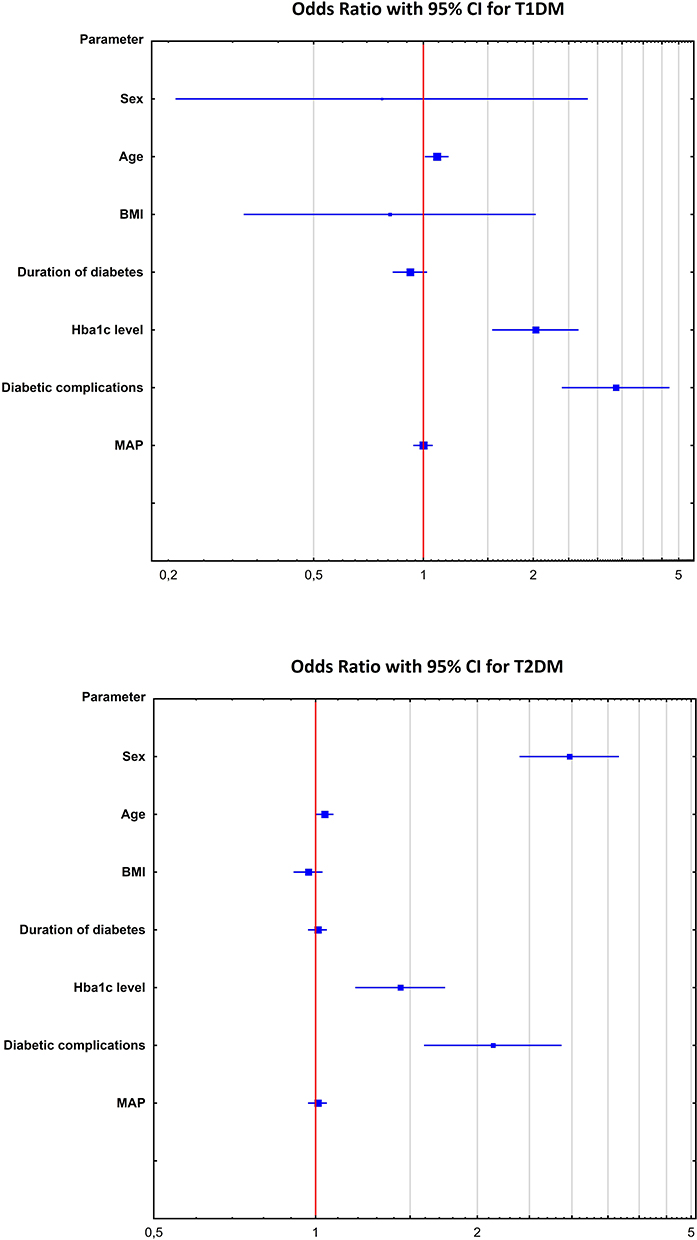 |
Figure 1 Risk analysis for prevalence of depressive symptoms in T1DM and T2DM (logarithmic scale). Abbreviations: BMI, body mass index; HbA1c, glycated haemoglobin; MAP, mean arterial pressure. |
It has been shown in Table 6 and Figure 1 that in patients with T1DM, the occurrence of depressive symptoms increases with age (p=0.0255, odds ratio=1.09), HbA1c level (p=0.0128, OR=2.03) and diabetic complications (p=0.0356, OR=3.37). The performed analysis allowed for concluding that the created model was statistically significant which was proven by the result of the likelihood ratio test (χ2 = 25.10; p<0.0007). The model’s goodness of fit R2 = 0.28 (Nagelkerke). The sufficient goodness of fit was confirmed by the result of the Hosmer–Lemeshow test (p=0.6437).
In turn, in patients with T2DM, the risk of depressive symptoms turned out to be almost three times higher in women than in men (p=0.0006, OR=2.97), increased with age (p=0.0324, OR=1.04), HbA1c level (p=0.0103, OR=1.44) and diabetic complications (p=0.0174, OR=2.14) (Table 6, Figure 1). It may be concluded that the created model was statistically significant which was proven by the result of the likelihood ratio test (χ2 = 34.28; p<0.0001). The model’s goodness of fit R2 = 0.20 (Nagelkerke). The sufficient goodness of fit was confirmed by the result of the Hosmer–Lemeshow test (p=0.2792).
Discussion
In our study, we showed that the incidence and severity of depressive symptoms in patients with T1DM and T2DM was significantly higher than in non-diabetic subjects. In both types of diabetes, the BDI score was found to be higher in women than in men and higher in patients with T2DM compared to patients with T1DM. Similar results were obtained by other authors in terms of differences in BDI values between diabetic patients and controls without diabetes. In patients with T1DM, of whom about 20% of people used antidepressants, mean BDI score was higher than in controls without diabetes; in this group, every 11th respondent used antidepressant.15 Higher BDI scores were also observed in patients with T2DM compared to non-diabetic controls.6,19 In patients, both women and men, with T2DM, the mean BDI score in the own study was 11.5, while in other studies, it ranged from 9.5,6 10.6,19 12.612 to even 19.8.10
In patients with T1DM, depression symptoms such as loss of interest, indecisiveness, irritability, tiredness or fatigue and loss of interest in sex in women and tiredness or fatigue in men were significantly more common than in the control group. On the other hand, in patients with T2DM in comparison with the control group, there were significantly more such symptoms of depression, as sadness, pessimism, past failure, loss of pleasure, self-criticalness, agitation, loss of interest, indecisiveness, loss of energy, changes in sleeping pattern, irritability, tiredness or fatigue and loss of interest in sex in a group of women, and sadness, pessimism, past failure, loss of pleasure, guilty feeling, self-dislike, agitation, loss of interest, indecisiveness, worthlessness, loss of energy, changes in sleeping pattern, irritability, tiredness or fatigue and loss of interest in sex in a group of men. The occurrence of some of the symptoms of depression, namely loss of energy, sleep pattern disturbance, tiredness or fatigue, loss of interest in sex and loss of pleasure, has also been found in another study in patients with T2DM with associated chronic kidney disease.20
When the threshold of BDI score ≥1618 was taken to diagnose depressive symptoms, it turned out that in our study, the diagnosis occurred in 17.5% of the women and 8.6% of the men with T1DM and in 28.9% of the women and 19.8% of the men with T2DM. In the studies of Lloyd et al16 depressive symptomatology defined by BDI score ≥16 was revealed in 14% of the patients with T1DM, with the disease more frequently affecting men (16%) than women (14%), which is the reverse of that in our own study and described in the meta-analysis by Anderson et al,2 where the incidence of depression in patients with T1DM was higher in women than in men regardless of the method used to assess depression and controlled and uncontrolled studies. In our study, depressive symptoms were diagnosed in every fourth person among the examined women and men with T2DM in total. In other studies including patients with T2DM with a BDI score ≥16 (as in this study), the incidence of depressive symptoms was 7.5%,5 17%,21 29.4%,8 32.7%,3 35.2%6 and even 40.2%.9 In T2DM, depression was more common in women.3,9-11,14,21
The differentiation of the incidence of depressive symptoms in T1DM and in T2DM in our study may be related mainly to the age of the examined patients (mean age of patients with T1DM was below 30 years and T2DM – over 50 years), duration of diabetes (it was longer in T2DM), occurrence of diabetic complications (in T2DM the incidence of diabetic complications was about 2 times higher than in T1DM) and the occurrence of concomitant somatic chronic diseases, which mainly included patients with T2DM. The association of depressive symptoms with T2DM accompanying chronic somatic diseases was suggested by Mäntyselkä et al5 and Sweileh et al.9
Based on the logistic regression analysis, we showed that the occurrence of depressive symptoms correlated with age, HbA1c level and co-morbid diabetic complications in patients with T1DM and additionally with the female gender in patients with T2DM. This means that the incidence of depressive symptoms was greater when diabetic patients were older, had poorly controlled glycemia and were affected by complications of the disease. Similar connections between the occurrence of depressive symptoms and many other variables in diabetic patients were observed by other authors. In patients with T1DM with accompanying complications of the disease, the BDI score was higher than in those without complications15 and the occurrence of depression was associated with poorly controlled glycemia.22 On the other hand, in patients with T2DM, it was found that the incidence of depression was increased in patients with diabetic complications,3,4,10 especially those with micro- and macroangiopathy.23 The increased risk of depression in patients with T2DM was also caused by poorly controlled glycemia with higher HbA1c level.3,4,10,11,24 As in our study, the prevalence of depression in T2DM was higher in women than in men and increased with age.21
This study is associated with some limitations. Firstly, the diagnosis of depression was based only on BDI, but it was not supported by psychiatric or psychological examination, ie no diagnostic interview was carried out, so the obtained results of depression using only the questionnaire method could be overestimated. Secondly, only the patients treated at specialist diabetologic units who were under constant medical supervision were selected for the study, which means that they were not representative of the whole population, because it also includes patients who do not use specialist care. Thirdly, it was not possible to compare the study results between the groups with T1DM and T2DM, because these groups differed in terms of, eg age, BMI, mode of treatment, HbA1c levels, and the occurrence of complications and the symptoms of depression.
Conclusion
The prevalence of depressive symptoms in diabetic patients is higher than in non-diabetics. Depressive symptoms account for one-eighth of patients with T1DM, including twice as many women as men, and quarter of patients with T2DM, including 1.5 times more women than men. The risk of depressive symptoms in T1DM increases with age, HbA1c level and the presence of diabetic complications. The risk of depressive symptoms in patients with T2DM is gender-related and increases with age, HbA1c level and the presence of diabetic complications.
Ethics Statement
The study was performed with the consent of the Bioethics Committee of the Beskidzka Regional Chamber of Physicians in Bielsko-Biala on 11 February 2016 (Consent No. 2016/02/11/1). The study does not report on or involve the use of any animals. All procedures performed in the study (involving human participants) were in accordance with the ethical standards of the committee and with the 1964 Declaration of Helsinki. Written informed consents were obtained from all individual participants included in the study. The study does not contain data from any individual person and data obtained from the questionnaires are available upon request.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Statistical Report: Diabetes statistics in Poland and in the world. [homepage in Polish] Available from: http://cukrzycapolska.pl/cukrzyca/statystyki.
2. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care. 2001;24(6):1069–1078. doi:10.2337/diacare.24.6.1069
3. Rodríguez Calvín JL, Zapatero Gaviria A, Martín Ríos MD. Prevalence of depression in type 2 diabetes mellitus. Rev Clin Esp. 2015;215(3):156–164. doi:10.1016/j.rce.2014.10.010
4. Zhang W, Xu H, Zhao S, et al. Prevalence and influencing factors of co-morbid depression in patients with type 2 diabetes mellitus: a General Hospital based study. Diabetol Metab Syndr. 2015;7:60. doi:10.1186/s13098-015-0053-0
5. Mäntyselkä P, Korniloff K, Saaristo T, et al. Association of depressive symptoms with impaired glucose regulation, screen-detected, and previously known type 2 diabetes: findings from the Finnish D2D survey. Diabetes Care. 2011;34(1):71–76. doi:10.2337/dc10-1044
6. Ferreira MC, Piaia C, Cadore AC, Antoniolli MA, Gamborgi GP, Oliveira PP. Clinical variables associated with depression in patients with type 2 diabetes. Rev Assoc Med Bras. 2015;61(4):336–340. doi:10.1590/1806-9282.61.04.336
7. Papelbaum M, Moreira RO, Coutinho W, et al. Depression, glycemic control and type 2 diabetes. Diabetol Metab Syndr. 2011;3(1):26. doi:10.1186/1758-5996-3-26
8. Chung JO, Cho DH, Chung DJ, Chung MY. Assessment of factors associated with the quality of life in Korean type 2 diabetic patients. Intern Med. 2013;52(2):179–185. doi:10.2169/internalmedicine.52.7513
9. Sweileh WM, Abu-Hadeed HM, Al-Jabi SW, Zyoud SH. Prevalence of depression among people with type 2 diabetes mellitus: a cross sectional study in Palestine. BMC Public Health. 2014;14:163. doi:10.1186/1471-2458-14-163
10. Niraula K, Kohrt BA, Flora MS, et al. Prevalence of depression and associated risk factors among persons with type-2 diabetes mellitus without a prior psychiatric history: a cross-sectional study in clinical settings in urban Nepal. BMC Psychiatry. 2013;13:309. doi:10.1186/1471-244X-13-309
11. Eker S. Prevalence of depression symptoms in diabetes mellitus. Open Access Maced J Med Sci. 2018;6(2):340–343. doi:10.3889/oamjms.2018.085
12. Parildar H, Cigerli O, Demirag NG. Depression, coping strategies, glycemic control and patient compliance in type 2 diabetic patients in an endocrine outpatient clinic. Pak J Med Sci. 2015;31(1):19–24. doi:10.12669/pjms.311.6011
13. de Groot M, Doyle T, Averyt J, Risaliti C, Shubroo J. Depressive symptoms and type 2 diabetes mellitus in rural appalachia: an 18-month follow-up study. Int J Psychiatry Med. 2015;48(4):263–277. doi:10.2190/PM.48.4.c
14. Lloyd CE, Nouwen A, Sartorius N, et al. Prevalence and correlates of depressive disorders in people with Type 2 diabetes: results from the International Prevalence and Treatment of Diabetes and Depression (INTERPRET-DD) study, a collaborative study carried out in 14 countries. Diabet Med. 2018;35(6):760–769. doi:10.1111/dme.2018.35.issue-6
15. Gendelman N, Snell-Bergeon JK, McFann K, et al. Prevalence and correlates of depression in individuals with and without type 1 diabetes. Diabetes Care. 2009;32(4):575–579. doi:10.2337/dc08-1835
16. Lloyd CE, Pambianco G, Orchard TJ. Does diabetes-related distress explain the presence of depressive symptoms and/or poor self-care in individuals with type 1 diabetes? Diabet Med. 2010;27(2):234–237. doi:10.1111/dme.2010.27.issue-2
17. Beck A, Steer R, Brown G. The Beck Depression Inventory – Second Edition. San Antonio, TX: Psychological Corporation; 1996.
18. Wing RR, Marcus MD, Blair EH, Epstein LH, Burton LR. Depressive symptomatology in obese adults with type II diabetes. Diabetes Care. 1990;13:170–172. doi:10.2337/diacare.13.2.170
19. Exebio JC, Zarini GG, Exebio C, Huffman FG. Healthy eating index scores associated with symptoms of depression in Cuban-Americans with and without type 2 diabetes: a cross sectional study. Nutr J. 2011;10:135. doi:10.1186/1475-2891-10-135
20. Sakraida TJ, Weber MT. The relationship between depressive symptoms and self-management behaviors in patients with T2DM and stage 3 CKD. Perspect Psychiatr Care. 2016;52(4):273–282. doi:10.1111/ppc.2016.52.issue-4
21. Alajmani DSA, Alkaabi AM, Alhosani MW, et al. Prevalence of undiagnosed depression in patients with type 2 diabetes. Front Endocrinol (Lausanne). 2019;3(10):259. doi:10.3389/fendo.2019.00259
22. Van Tilburg MA, McCaskill CC, Lane JD, et al. Depressed mood is a factor in glycemic control in type 1 diabetes. Psychosom Med. 2001;63(4):551–555. doi:10.1097/00006842-200107000-00005
23. Lin EH, Rutter CM, Katon W, et al. Depression and advanced complications of diabetes: a prospective cohort study. Diabetes Care. 2010;33(2):264–269. doi:10.2337/dc09-1068
24. Marrero DG, Ma Y, de Groot M, et al.; Diabetes Prevention Program Research Group. Depressive symptoms, antidepressant medication use, and new onset of diabetes in participants of the diabetes prevention program and the diabetes prevention program outcomes study. Psychosom Med. 2015;77(3):303–310. doi:10.1097/PSY.0000000000000156
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.