")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Prevalence of Depression and the Quality-of-Life of Breast Cancer Patients in Jordan
Authors Alquraan L, Alzoubi KH , Rababa’h S, Karasneh R , Al-azzam S, Al-Azayzih A
Received 16 August 2020
Accepted for publication 13 October 2020
Published 3 November 2020 Volume 2020:13 Pages 1455—1462
DOI https://doi.org/10.2147/JMDH.S277243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Laiali Alquraan,1 Karem H Alzoubi,2 Suzie Rababa’h,3 Reema Karasneh,4 Sayer Al-azzam,2 Ahmad Al-Azayzih2,5
1Department of Biology, Yarmouk University, Irbid, Jordan; 2Department of Clinical Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Medical Science, Irbid Faculty, Al-Balqa Applied University (BAU), Irbid, Jordan; 4Department of Basic Medical Sciences, Yarmouk University, Irbid, Jordan; 5Department of Pharmacology and Therapeutics, United Arab Emirates University, Al Ain, United Arab Emirates
Correspondence: Laiali Alquraan
Department of Biology, Faculty of Science, Yarmouk University, P.O. Box 566, Irbid 21163, Jordan
Tel +962 2 7211111/ext. 2831
Fax +962 2 7211117
Email [email protected]
Objective: The objectives of the current study are to evaluate the prevalence of depression symptoms among breast cancer patients in Jordan and impact of the disease on patient’s quality-of-life.
Methods: A cross-sectional survey-based study was conducted over a 6-month period among breast cancer patients attending two major hospitals in Jordan. A validated questionnaire was used to evaluate the prevalence of depression symptoms and quality-of-life aspects among those patients utilizing Beck’s Depression Inventory-II score and 36-Item Survey Form (SF-36) score, respectively.
Results: The mean age±SD of patients (n=169) was 49.12± 6.48 years. Depression symptoms were reported in 30.2% of patients. As for quality-of-life, the physical functioning (PF) subscale was significantly associated with the patient’s age (P=0.03). The role-physical (RP) subscale was associated with number of sleeping hours (P=0.038). Marital status of breast cancer patients was significantly associated with role-emotional (RE) (P=0.015) and mental health (MH) (P=0.009) subscales. The number of patient’s siblings was significantly associated with daily habits such as PF (P=0.031) and RP (P=0.005) subscales. Moreover, the occupation of patients was associated with the PF (P=0.041) and MH (P=0.049).
Conclusion: About one-third of breast cancer patients reported depression symptoms. Quality-of-life subscales among those patients were associated with multiple social and health determinants, such as age, marital status, number of siblings, occupation, and number of sleeping hours. There is urgent need to support this group of patients to help them to cope with depression symptoms and to improve their quality-of-life.
Keywords: breast cancer, depression, quality-of-life, Beck’s Depression Inventory, SF-36
Introduction
Cancer is one of the most common health problems and the second, after cardiovascular diseases, in death cases among Jordanians.1 According to the Jordan Cancer Registry (JCR), the number of new cancer cases diagnosed among Jordanians has increased by 60.5% in the past years, from 3,370 cases in 2000 to 5,409 in 2013.2 In Jordan, cancer mortality information shows that breast cancer is the most common cause of cancer deaths in females, accounting for 22.4%, followed by colorectal (8.9%), and lung (7.0%).1 Cancer and symptoms associated with treatment are significant stressors for breast cancer patients receiving disease care.3 Receiving a cancer diagnosis is related with secondary psychological symptoms of severe distress such as pain, hopelessness, fear, anxiety, depression and fatigue.4 Depression is a common psychological symptom perceived by patients with breast cancer and affects the quality-of-life (QoL) in these patients. The prevalence of depression in breast cancer patients ranges from 1.5–50%, depending on factors including the basis of diagnostic and sample type.5,6 The rates for depression among breast cancer patients are high.7 This is due to the particular psychosocial, clinical, and hormonal factors that may affect mood in patients with breast cancer.7 The prevalence of depression among advanced stage cancer patients in Jordan was previously shown to be 51.9%.8 Another quantitative study showed that 53% of breast cancer survivors in Jordan were classified as abnormal on an anxiety scale, and 45% on the depression scale.9
Quality-of-life is a complex multi-dimensional evaluation of individuals' physical, psychological, and social well-being. Quality-of-life is an important datum reflecting the results of treatment applied to cancer patients. Several cancer-specific health-related quality-of-life (QoL) measures were developed to assess the short- and long-term effects of cancer on quality-of-life.10 In breast cancer patients, treatment consequences represent a great source of anxiety and depression that is accompanied with a decrease in the quality-of-life during cancer therapy.11 In the present study, we aim to assess the prevalence of depression symptoms and the QoL among patients with breast cancer diagnosis and how they associate with demographic and disease- related factors.
Methods and Settings
A cross-sectional survey study was conducted among breast cancer patients diagnosed between March 2018 and August 2018 at two major hospitals in Jordan (King Abdulla University Hospital, and the Royal Medical Services). The sample for the present study was based on convenient sampling, where all patients admitted to the oncology wards during the presence of the researcher were approached by the researcher to participate in the study. Included in the study were patients who were 18 years and above admitted with breast cancer diagnosis. Excluded were breast cancer patients with other secondary tumors or other major comorbidities such as.
A total of 189 patients were approached. The final number of patients who agreed to enroll in the study was 169. Thus, the response rate was 89.4%. As for sample size, the number of new breast cancer diagnoses in 2018 was 2,143.12 With the assumption of even distribution of new diagnosed cases across the year, the enrolled patients in the current study represent about 15% of these cases. Participants were not paid for participation in the study and none of them dropped out after enrollment in the study.
Two questionnaires were employed during the study: the first one included sociodemographic and health variables including age, nationality, marital status, education, occupation, monthly income, living place, average sleep hours, family history of depression, smoking status, physical activity, history of chronic diseases, and duration of breast cancer treatment. The second part of the questionnaire was concerned with evaluating the quality-of-life using the SF-36 scale,13 and depression status using the Beck depression inventory II (BDI-II).14 The SF-36 is a standardized tool for measuring quality-of-life. It includes the following subscales: physical functioning (PF), role-physical (RP), role-emotional (RE), vitality (VT), mental health (MH), social functioning (SF), bodily pain (BP), and general health (GH). The SF-36 is available as a validated tool in Arabic language.15 The Beck depression inventory II (BDI-II) is also a standardized tool to evaluate depression status, and available as a validated tool in Arabic language.16 Thus, the survey tool of the current study was done in Arabic language.
The protocol of this study was reviewed and approved by the Institutional Review Board of Jordan University of Science and Technology (Approval number 13/113/2018). The protocol of this is in accordance with the Declaration of Helsinki. Patients were approached during their hospital stay and requested to participate in the study, and given a brief explanation about the study purpose. If they agreed to participate, an interview time was scheduled. At interview, a detailed explanation of the study protocol was provided. Then, written informed consent was taken before the questionnaire administration from each participant. The interview was semi-structured, and all items of the study questionnaire were presented to the patient participants.
All the data collected were evaluated by SPSS 21.0 statistics package program (SPSS Inc., Chicago, IL, USA). Numbers and percentages were used to express categorical variables, whereas means and standard deviation were used for continuous variables. P<0.05 was considered significant. One-way ANOVA or unpaired t‑test were conducted to compare differences in SF-36 and Beck scales as per sociodemographic and health variable of the study subjects.
Results
Breast cancer patient (n=169 females) with a mean age±Standard Deviation (SD) of 49.12±6.48 years participated in this study. The majority of patients were married (71%), with three-to-four children, and housewives (62.7%). Moreover, a high percentage of patients completed secondary school education (46.2%), while only 4.1% of patients completed their graduate education. Demographic characteristics of breast cancer patients are shown in Table 1. The prevalence of depression symptoms was 30.2% among patients, distributed as 26% with mild depression, 19.5% as moderate depression, and 1.8% as severe depression, as shown in Table 2.
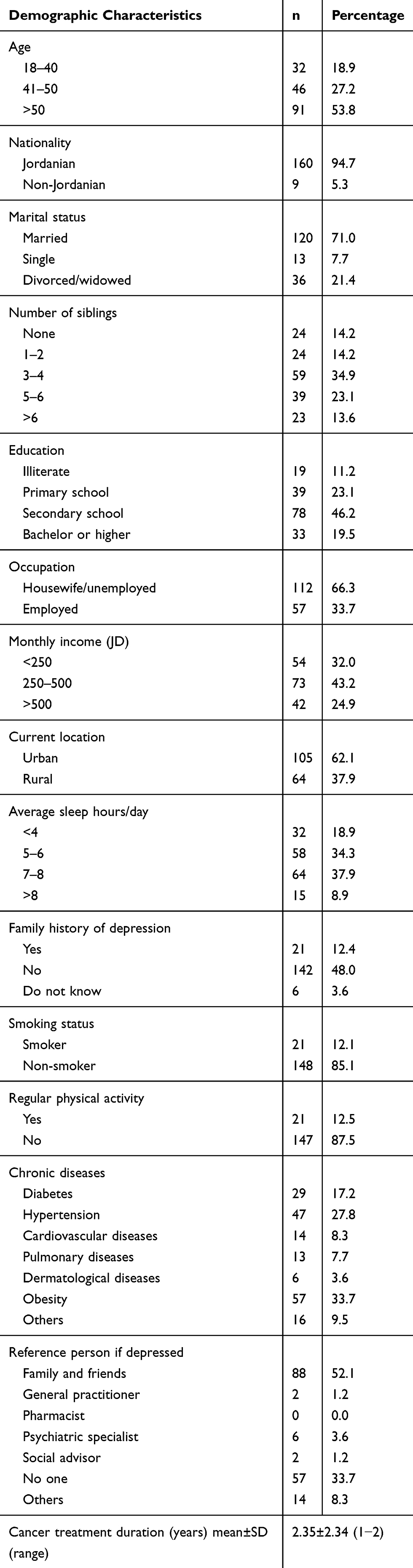 |
Table 1 Demographic Characteristics of Breast Cancer Patients (N=169) |
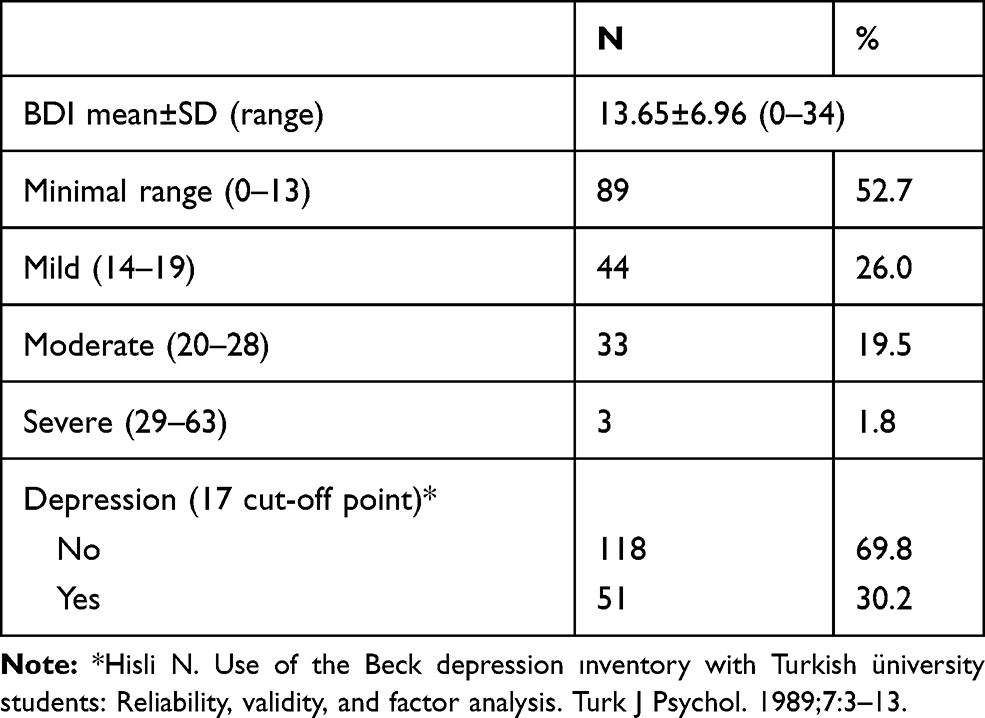 |
Table 2 The Average of Beck Depression Inventory-Categories and Subscales (Cronbach Alpha=0.772; N=169) |
Reliability, central tendency, and variability of scales of the SF-36 quality-of-life questionnaire among breast cancer patients are shown in Table 3. Table 4 show associations of SF-36 subscales with sociodemographic and health variables of study participants. The PF subscale was significantly associated with the patient’s age (P=0.03). The RP subscale was associated with number of sleeping hours (P=0.038). The marital status of breast cancer patients was significantly associated with RE (P=0.015) and MH (P=0.009) subscales. The number of patient’s siblings was significantly associated with daily habits such as PF (P=0.031) and RP (P=0.005) subscales. Moreover, the occupation of patients was associated with the PF (P=0.041) and MH (P=0.049). Patients’ nationality, education level, income, and living place were not associated with any of the SF-36 subscales.
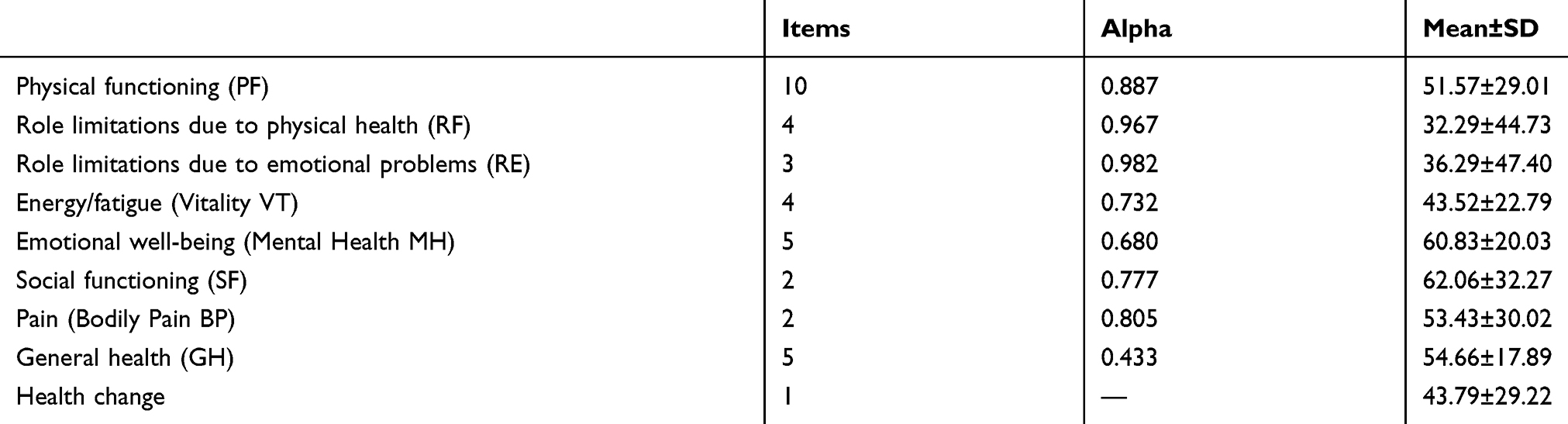 |
Table 3 Reliability, Central Tendency, and Variability of Scales of SF-36 Quality-of-Life Questionnaire of Breast Cancer Patients (Cronbach’s Alpha=0.84; N=169) |
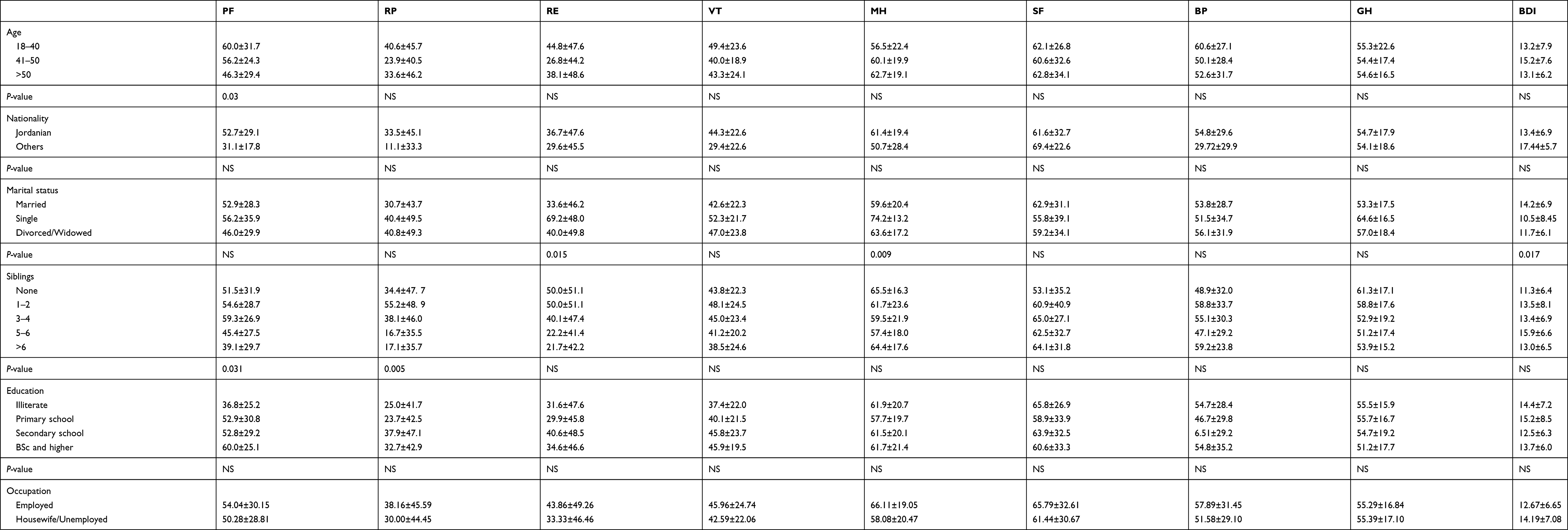 |
Table 4 The Comparison of the Sociodemographic Characteristics of Breast Cancer Patients with the Short Form 36 and Beck Depression Inventory Parameters (N=169) |
As for depression status, there is an association between family history of depression with both SF (P=0.026) and BP (P=0.047). Finally, the Beck depression inventory-II index showed a significant association with marital status (P=0.049) and sleeping hours (P=0.003) (Table 4).
Discussion
In this study, we examined the quality-of-life and prevalence of depression symptoms among breast cancer patients in Jordan. According to the BDI-II rating scale that was used to determine the depression symptoms and their severity, 30.2% of breast cancer patients displayed the cut-off point of the depression scale. Patients were distributed as 26.0% with mild depression symptoms, 19.5% with moderate symptoms, and 1.8% with severe symptoms. Marital status and average number of sleep hours during the day were significantly associated with development of depression symptoms among breast cancer patients.
It was previously shown that the prevalence of depression among breast cancer patients was 24.75% in Levant region.11 Another study at the outpatient clinics of a university hospital in Egypt showed a prevalence of depression of 38.8%.17 In a meta‑analysis study that evaluated the global prevalence of depression among breast cancer patients, 32.2% of patients were shown to have depression symptoms.18 Yet, a higher prevalence of depression symptoms (49.6%) was recorded in women with breast cancer in Saudi Arabia.19 Results of the different studies showed that depression was common among breast cancer patients. This variability in results in different studies might be explained by different disease stages, treatment strategies, and physical debilitation of patients’ caregivers. Moreover, psychological complications of breast cancer patients and the impaired body image of women might also be a factor. For example, fatigue and pain are among the symptoms that resulted from disease treatment and their consequences in interruption of daily activities may cause feelings of distress among these women. Woman appearance and concerns about her whole body.3 Moreover, mastectomy and hair loss due to chemotherapy or early menopause may be a serious threat to the self-image of a woman.20
In the current study, patients were compared according to their age with the SF‑36 sub‑scales; physical functioning scores of elderly patients were significantly lower than younger patients. Previous studies have reported age to have an effect on the quality-of-life and reported a strong decline in physical activity immediately after diagnosis with breast cancer.21,22 The current results showed that divorced patients had lower scores than other patients in emotional well-being, whereas their mean BDI-II scores were significantly higher. A previous study about the relation between marital status and optimism score among breast cancer survivors revealed that married women had significantly higher optimism compared to unmarried women.23 Another study from China showed that divorced women had a 30% lower score of social and family well-being compared with married women with breast cancer.24 A study about quality-of-life after adjuvant chemotherapy for breast cancer revealed that unmarried breast cancer survivors experienced lower mental well-being than married breast cancer survivors.25,26 The current study reported that a higher number of siblings was associated with a lower level of limitation role due to physical health and limitations role due to emotional problems in breast cancer patients. Such findings strongly imply that, in dealing with breast cancer patients, social support from family members and friends as well as other social connections plays an important role.
Both mental health and general health of employed patients were significantly better than those of the unemployed. The current results are similar to other studies which showed that general wellbeing of women who worked at least some hours per week was higher than those who did not work.27 Other findings revealed that physical wellbeing and other quality-of-life domains were positively related to the number of hours worked per week.28 General wellbeing may be higher in women working at the time of diagnosis because of good support received from coworkers and friends in the workplace. Feelings of life normalcy and the ability of work were shown to distract patients from their illness and to provide patients with a good sense of self-efficacy to cope with disease, which could be another explanation for the good impact of work on quality-of-life among cancer patients.27
Patients with an average sleep of less than 6 hours per day had been significantly correlated to limitations due to physical heath. A previous study has shown that breast cancer patients who were sleep deprived reported problems due to physical weaknesses in their ability to perform work and daily tasks.29 Other studies indicate poor sleep quality has been associated to lower life quality including physical activity.30,31 In fact, high level of physical activity was correlated with an increase in self-efficacy which, in turn, were correlated with enhancement in general health status parameters and quality-of-life.32,33
The current study has some limitations as it only included two medical centers in Jordan. It covered only a period of 6 months, and it only collected limited information about treatment and intervention given to patients. Future more comprehensive studies are needed to cover more clinical aspects of the disease and relate those to the status of depression of patients and their quality-of-life.
In conclusion, the current results showed the prevalence rate of depression among breast cancer patients to be 30.2%. The majority of the reported depression cases were minimal to mild in severity. Quality-of-life measurements domains were impacted by different factors including patient’s age, marital status, number of siblings, patient’s occupation, and average number of sleep hours per day. Current results showed a necessity to pay attention and provide more social and psychological support to breast cancer patients and to tailor the measurements taken to reduce the symptoms of depression and improve their quality-of-life.
Funding
This study was supported by Deanship of Research at Jordan University of Science and Technology.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdel-Razeq H, Attiga F, Mansour A. Cancer care in Jordan. Hematol Oncol Stem Cell Ther. 2015;8(2):64–70. doi:10.1016/j.hemonc.2015.02.001
2. Khader YS, Sharkas GF, Arkoub KH, Alfaqih MA, Nimri OF, Khader AM. The epidemiology and trend of cancer in Jordan, 2000-2013. J Cancer Epidemiol. 2018;2018:2937067. doi:10.1155/2018/2937067
3. Purkayastha D, Venkateswaran C, Nayar K, Unnikrishnan UG. Prevalence of depression in breast cancer patients and its association with their quality of life: a cross-sectional observational study. Indian J Palliat Care. 2017;23(3):268–273. doi:10.4103/IJPC.IJPC_6_17
4. Almigbal TH, Almutairi KM, Fu JB, et al. Assessment of psychological distress among cancer patients undergoing radiotherapy in Saudi Arabia. Psychol Res Behav Manag. 2019;12:691–700. doi:10.2147/PRBM.S209896
5. Massie MJ. Prevalence of depression in patients with cancer. J Natl Cancer Inst Monogr. 2004;2004(32):57–71. doi:10.1093/jncimonographs/lgh014
6. Zainal NZ, Nik-Jaafar NR, Baharudin A, Sabki ZA, Ng CG. Prevalence of depression in breast cancer survivors: a systematic review of observational studies. Asian Pac j Cancer Prev. 2013;14(4):2649–2656. doi:10.7314/APJCP.2013.14.4.2649
7. Tsaras K, Papathanasiou IV, Mitsi D, et al. Assessment of depression and anxiety in breast cancer patients: prevalence and associated factors. Asian Pac J Cancer Prev. 2018;19(6):1661–1669.
8. Mhaidat NM, Alzoubi KH, Al-Sweedan S, Alhusein BA. Prevalence of depression among cancer patients in Jordan: a national survey. Supportive Care Cancer. 2009;17(11):1403–1407. doi:10.1007/s00520-009-0600-z
9. Abu-Helalah M, Al-Hanaqta M, Alshraideh H, Abdulbaqi N, Hijazeen J. Quality of life and psychological well-being of breast cancer survivors in Jordan. Asian Pac j Cancer Prev. 2014;15(14):5927–5936. doi:10.7314/APJCP.2014.15.14.5927
10. van Roij J, Fransen H, van de Poll-franse L, Zijlstra M, Raijmakers N. Measuring health-related quality of life in patients with advanced cancer: a systematic review of self-administered measurement instruments. Qual Life Res. 2018;27(8):1937–1955. doi:10.1007/s11136-018-1809-4
11. Akel R, El Darsa H, Anouti B, et al. Anxiety, depression and quality of life in breast cancer patients in the levant. Asian Pac j Cancer Prev. 2017;18(10):2809–2816.
12. WHO. Global Breast Cancer Observatory 2018. Jordan; 2019.
13. Ware JE
14. Beck AT, Steer RA, Ball R, Ranieri W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J Pers Assess. 1996;67(3):588–597. doi:10.1207/s15327752jpa6703_13
15. Cech DJ, Martin ST. Chapter 5 - evaluation of function, activity, and participation. In: Cech DJ, Martin ST, editors. Functional Movement Development Across the Life Span.
16. Wang YP, Gorenstein C. Psychometric properties of the Beck Depression Inventory-II: a comprehensive review. Revista Brasileira de Psiquiatria (Sao Paulo, Brazil: 1999). 2013;35(4):416–431. doi:10.1590/1516-4446-2012-1048
17. El-Hadidy MA, Elnahas W, Hegazy MA, Hafez MT, Refky B, Wahab KM. Psychiatric morbidity among Egyptian breast cancer patients and their partners and its impact on surgical decision-making. Breast Cancer (Dove Med Press). 2012;4:25–32.
18. Pilevarzadeh M, Amirshahi M, Afsargharehbagh R, Rafiemanesh H, Hashemi SM, Balouchi A. Global prevalence of depression among breast cancer patients: a systematic review and meta-analysis. Breast Cancer Res Treat. 2019;176(3):519–533.
19. Ahmed AE, Albalawi AN, Qureshey ET, et al. Psychological symptoms in adult Saudi Arabian cancer patients: prevalence and association with self-rated oral health. Breast Cancer. 2018;10:153–159.
20. Couzi RJ, Helzlsouer KJ, Fetting JH. Prevalence of menopausal symptoms among women with a history of breast cancer and attitudes toward estrogen replacement therapy. J clin oncol. 1995;13(11):2737–2744. doi:10.1200/JCO.1995.13.11.2737
21. Ganz PA, Guadagnoli E, Landrum MB, Lash TL, Rakowski W, Silliman RA. Breast cancer in older women: quality of life and psychosocial adjustment in the 15 months after diagnosis. J clin oncol. 2003;21(21):4027–4033. doi:10.1200/JCO.2003.08.097
22. Derks MG, de Glas NA, Bastiaannet E, et al. Physical functioning in older patients with breast cancer: a prospective cohort study in the TEAM trial. The Oncologist. 2016;21(8):946–953. doi:10.1634/theoncologist.2016-0033
23. Croft L, Sorkin J, Gallicchio L. Marital status and optimism score among breast cancer survivors. Supportive Care Cancer. 2014;22(11):3027–3034. doi:10.1007/s00520-014-2308-y
24. Yan B, Yang LM, Hao LP, et al. Determinants of quality of life for breast cancer patients in Shanghai, China. PLoS One. 2016;11(4):e0153714. doi:10.1371/journal.pone.0153714
25. Broeckel JA, Jacobsen PB, Balducci L, Horton J, Lyman GH. Quality of life after adjuvant chemotherapy for breast cancer. Breast Cancer Res Treat. 2000;62(2):141–150. doi:10.1023/A:1006401914682
26. Tran TH, Trinh NL, Hoang Y, Nguyen TL, Vu TT. Health-related quality of life among vietnamese breast cancer women. Cancer Control. 2019;26(1):1073274819862787. doi:10.1177/1073274819862787
27. Timperi AW, Ergas IJ, Rehkopf DH, Roh JM, Kwan ML, Kushi LH. Employment status and quality of life in recently diagnosed breast cancer survivors. Psycho-Oncology. 2013;22(6):1411–1420.
28. Kennedy F, Haslam C, Munir F, Pryce J. Returning to work following cancer: a qualitative exploratory study into the experience of returning to work following cancer. Eur J Cancer Care (Engl). 2007;16(1):17–25. doi:10.1111/j.1365-2354.2007.00729.x
29. Fortner BV, Stepanski EJ, Wang SC, Kasprowicz S, Durrence HH. Sleep and quality of life in breast cancer patients. J Pain Symptom Manage. 2002;24(5):471–480.
30. Blair CK, Robien K, Inoue-Choi M, Rahn W, Lazovich D. Physical inactivity and risk of poor quality of life among elderly cancer survivors compared to women without cancer: the Iowa Women’s Health Study. J Cancer Survivorship. 2016;10(1):103–112. doi:10.1007/s11764-015-0456-9
31. Rafie C, Ning Y, Wang A, Gao X, Houlihan R. Impact of physical activity and sleep quality on quality of life of rural residents with and without a history of cancer: findings of the Day and Night Study. Cancer Manag Res. 2018;10:5525–5535.
32. McAuley E, Konopack JF, Motl RW, Morris KS, Doerksen SE, Rosengren KR. Physical activity and quality of life in older adults: influence of health status and self-efficacy. Ann Behav Med. 2006;31(1):99–103. doi:10.1207/s15324796abm3101_14
33. Phillips SM, McAuley E. Physical activity and quality of life in breast cancer survivors: the role of self-efficacy and health status. Psycho-Oncology. 2014;23(1):27–34. doi:10.1002/pon.3366
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.