")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Prevalence of dementia in Egypt: a systematic review
Authors Elshahidi MH , Elhadidi MA, Sharaqi AA, Mostafa A, Elzhery MA
Received 14 November 2016
Accepted for publication 14 December 2016
Published 6 March 2017 Volume 2017:13 Pages 715—720
DOI https://doi.org/10.2147/NDT.S127605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Video abstract presented by Mohamed H Elshahidi.
Views: 131
Mohamed H Elshahidi,1 Muhammad A Elhadidi,2 Ahmed A Sharaqi,1 Ahmed Mostafa,3 Mohamed A Elzhery1
1Faculty of Medicine, Mansoura University, Mansoura, 2Faculty of Medicine, Zagazig University, Zagazig, 3Faculty of Medicine, Sohag University, Sohag, Egypt
Background: With the growing prevalence of dementia worldwide, two-third of the people with dementia are projected to be from the developing countries by 2050.
Aim: This study reviews the literature regarding dementia prevalence in Egypt.
Methods: Six databases were systematically searched from their dates of inception till July 2016. Studies published in English and reporting dementia prevalence among nonhospitalized individuals after clinical examinations were considered eligible. References were screened independently by two reviewers in two steps: 1) abstract screening and 2) full-text reviewing. In addition, quality of the included studies was assessed using the Newcastle–Ottawa scale.
Results: Of the 1,630 references retrieved, six studies (n=28,029 participants) met our inclusion criteria. In all studies, dementia was ascertained using a three-phase survey (Phase I: screening, Phase II: clinical diagnosis, Phase III: laboratory investigations). The dementia prevalence ranged from 2.01% to 5.07%. Dementia increased with age, with the rapid increase among those aging ≥80. Also, its prevalence was higher among illiterate groups than among educated groups. Included studies were of low risk of bias.
Conclusion: Dementia prevalence in Egypt demands including people with dementia in the health care system and promoting the awareness of dementia among the public. Also, more epidemiological studies in this field are needed.
Keywords: aging, epidemiology, Alzheimer’s disease, vascular dementia
Introduction
Rationale
Dementia is a neurological disease that causes cognitive and behavioral impairments that could ultimately interfere with the ability to function at work or to do the usual daily activities.1,2 It also negatively impacts the caregivers of persons with dementia.3,4 Dementia can be diagnosed by the neuropsychometric assessment method which has proven to be the best in the developing countries.5 There are several causes of dementia: Alzheimer’s disease on top of them followed by vascular dementia, Lewy body dementia, and frontotemporal dementia.6 Dementia does not only affect an individual’s quality of life but also has many adverse economic consequences. The cost per person is $ 868 in low-income countries and $ 3,109 in lower- to middle-income countries (such as Egypt).7 In 2010, 57.7% of dementia patients were from low- and middle-income countries. The increase in aging rates worldwide in tandem with the increasing rates of dementia incidences makes dementia a huge public health challenge for the developing countries.8,9
Objective
The aim of this review is to summarize current evidence regarding the prevalence of dementia in Egypt by analyzing systematically published epidemiological studies reporting dementia prevalence among the Egyptian population.
Methods
Protocol
Search strategy and inclusion criteria were developed according to the Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Statement guidelines for reporting systematic reviews and were documented in a protocol (PROSPERO registration number: CRD42016039695).10,11
Inclusion and exclusion criteria
Cross-sectional studies in which dementia was ascertained through clinical evaluation were considered eligible. Other studies or non-research articles that were not relevant to the topic were excluded. In addition, reviews and studies in which dementia was not confirmed through clinical evaluation were considered ineligible.
Information sources
An electronic search of English literature on PubMed, EBSCOhost, Web of Science, Scopus, Ovid (MEDLINE), and Google Scholar was conducted.
Search
All databases were searched from their date of inception till July 2016. The following search terms were used: “(prevalence OR epidemiology) AND (dementia OR alzheimer*) AND egypt*”.
Study selection
Two authors independently screened all the studies for eligibility in two steps: 1) abstract screening and 2) full-text reviewing. Any conflict was resolved through discussion.
Data extraction
Two authors extracted the data independently using Excel sheets prepared by the team.
Data items
The following data were extracted: first author’s name, year of publication, location and duration of the study, the number of participants, region (urban or rural), minimum age, and prevalence of dementia. Any disagreement was resolved through discussion.
Risk-of-bias assessment/quality assessment
Two authors independently assessed the risk of bias in the selected studies using the Newcastle–Ottawa scale (NOS) for non-randomized trials. Any conflict was resolved through discussion. A modified version of the NOS used by Douglas was implemented.12,13 Each study could attain a maximum score of 5. Studies with a score of ≥3 will be considered of low risk of bias, and those with a score of <3 will be considered of high risk of bias. The scale assessed the following domains: representativeness of the population, sample size, ascertainment of the condition, nonrespondents, and quality of statistical analyses.
Results
Study selection
Of the retrieved 1,630 references, six studies met our inclusion criteria (Figure 1).14–19 The six eligible studies were conducted in four governorates in Egypt between 1993 and 2013 (Table 1; Figure 2). Two studies were conducted in the New Valley governorate,15,16 and two were conducted in the Red Sea governorate.17,18 However, it is not stated whether the studies included the same individuals.
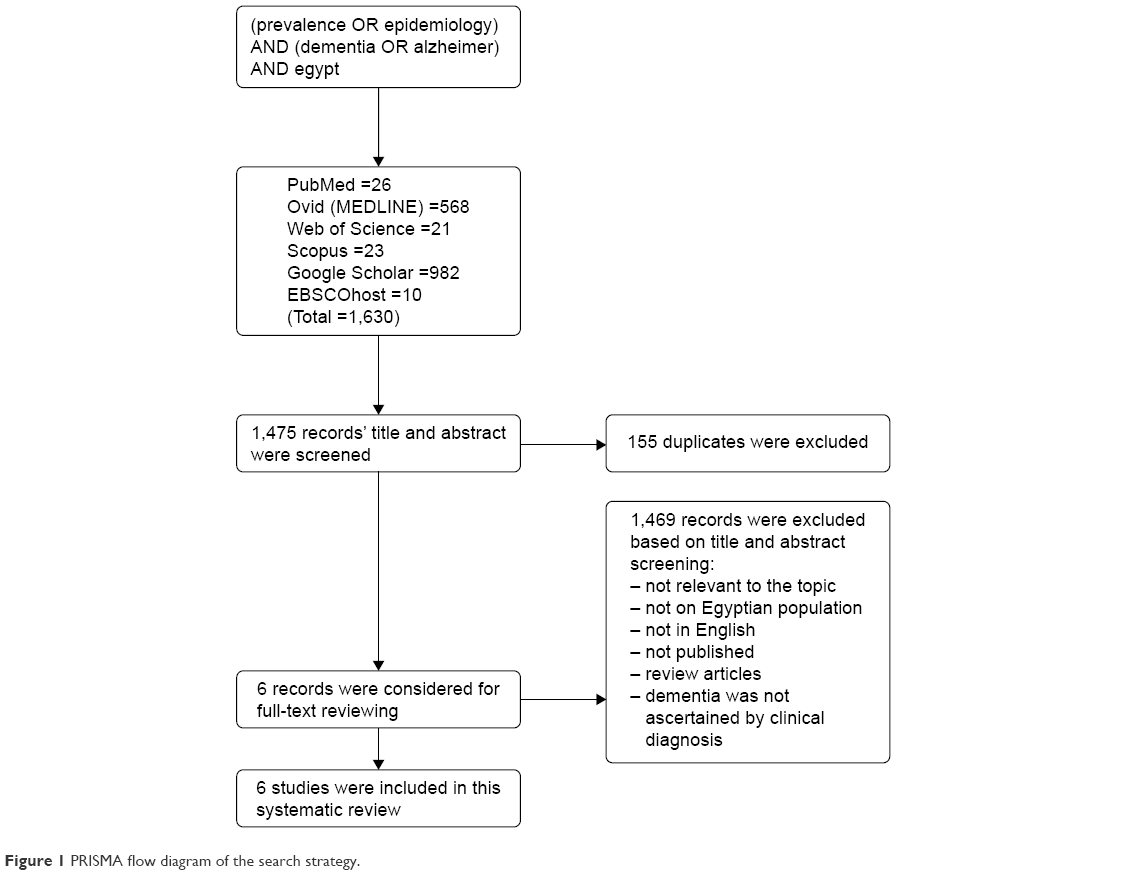 | Figure 1 PRISMA flow diagram of the search strategy. |
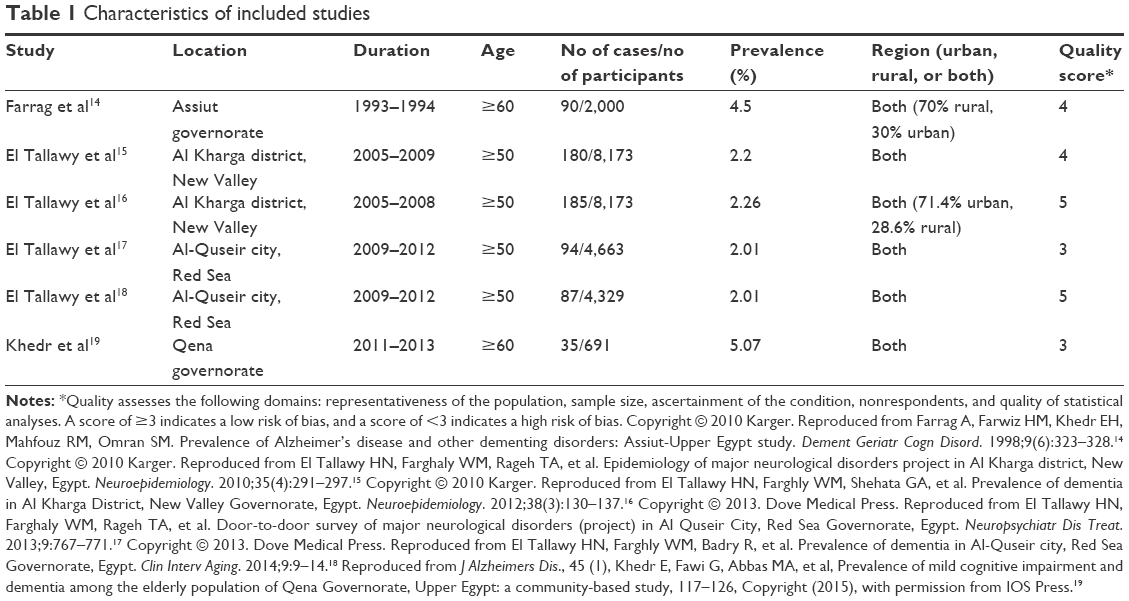 | Table 1 Characteristics of included studies |
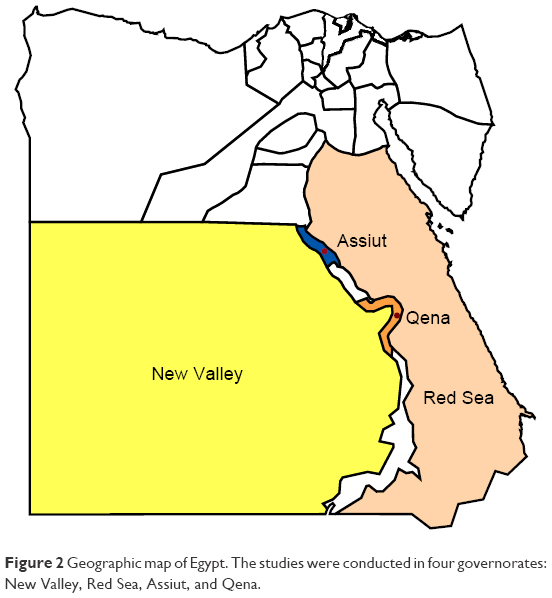 | Figure 2 Geographic map of Egypt. The studies were conducted in four governorates: New Valley, Red Sea, Assiut, and Qena. |
Subjects
A total of 28,029 elder individuals were investigated, and 671 were ascertained as affected with dementia. Four studies were performed on subjects aging ≥50,15–18 and the other two studies were conducted on people aging ≥60.14,19 Most studies did not report substance-induced dementia or dementia due to alcohol because of the sociocultural characteristics of the communities.14,16–18 In addition, two studies reported dementia in communities with high prevalence of Parkinson’s disease,12,19 one study reported high prevalence of cerebral palsy in the community,17 and one study reported dementia due to chronic renal diseases or hepatic disease because of schistosomiasis.14 In most of the studies, the percentage of nonrespondents ranged from 1% to 3.7%.14,16,17,19
Methods of assessment
All of the six included studies were carried out using a three-phase survey. In Phase I, four studies used the Mini Mental State Examination (MMSE) questionnaire for screening of dementia.14,15,18,19 The questionnaire was administered by trained neurologists, house officers, or neurology residents. For the illiterate people, the writing and reading parts of the MMSE were excluded, and the full score was calculated as 28 instead of 30 points.14,16,18,19 The other two studies used a questionnaire (sensitivity: 96%, specificity: 93.2%) prepared by the study team. Subjects who were suspected of having dementia proceeded to the next phase. In Phase II, clinical evaluation was made by trained neurologists using Diagnostic and Statistical Manual of Mental Disorders, Hachinski Ischemic Score, Wechsler Memory Scale-III, Clinical Dementia Rating scale, and Instrumental Activities of Daily Living scale. However, two studies used the diagnostic criteria recommended by the World Health Organization (WHO).16,17 In Phase III, laboratory investigations were carried out. Four studies used imaging methods to confirm dementia including magnetic resonance imaging/computed tomography.14,16,18,19
Prevalence of dementia
Dementia prevalence varied among studies. It was found to range from 2.01% to 5.07%. Four of the studies reported age-stratified prevalence of dementia (Table 2).14,16,18,19 The data showed that dementia increased with an increase in age. With the exception of one study,14 the other three studies reported a higher prevalence of dementia among females than males in the age group from 50 to 79. However, studies reporting dementia among those aging >80 showed a high prevalence among males than females.
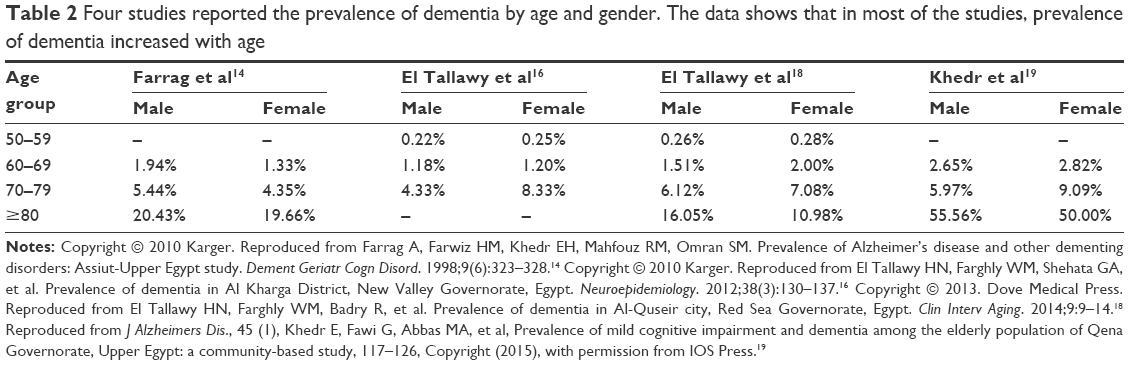 | Table 2 Four studies reported the prevalence of dementia by age and gender. The data shows that in most of the studies, prevalence of dementia increased with age |
Others
Only two studies reported the degree of dementia (Table 3). They reported that majority of people with dementia had mild or moderate dementia, and few percentage had severe dementia. Furthermore, three studies reported the dementia prevalence by education status (Table 3). They all reported a higher prevalence of dementia among illiterate people than among educated people. Moreover, two studies reported dementia with respect to residency (urban or rural). However, their results varied (Table 3).
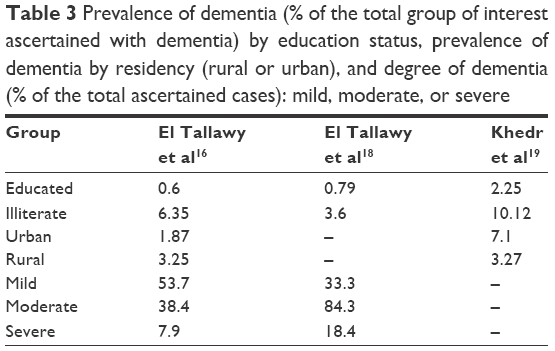 | Table 3 Prevalence of dementia (% of the total group of interest ascertained with dementia) by education status, prevalence of dementia by residency (rural or urban), and degree of dementia (% of the total ascertained cases): mild, moderate, or severe |
Quality assessment
Upon evaluation by the NOS, most of the studies were found to be of high quality (score ≥3) and low risk of bias (Table 1).
Discussion
This review aims to collect and summarize evidence regarding dementia prevalence in Egypt. It is found that the prevalence of dementia varied among studies. However, the epidemiological data on dementia rates in Egypt are deficient. It is suggested that dementia is not considered a health challenge due to the high proportion of youth in the population.20 In addition, the public belief of dementia as a sign of normal aging underestimates its priority.9,21 However, the current demographic transition makes dementia a future challenge to be taken into account. In 2013, nearly four million of the Egyptian population were above the age of 65.22 With an expected increase of this age group to 13.3% by 2050, consequences of dementia will also increase.23 The prevalence of dementia in Egypt compared with other countries in North Africa and Middle East region is quite different. In a study conducted in Wadi Ara, the prevalence rate was reported as 20.46% for those aging ≥65.24 This can be due to methodological issues, genetic factors, socioeconomic characteristics of the population, or mortality rate among elderly.20,29 Methodologically, it was possible that some patients who did not proceed to Phase II had dementia. This may cause the prevalence to be underestimated. Also, this may be due to failure during the interview (Phase I) to include individuals with dementia. Furthermore, the variation in the screening tool might account for the differences in the reported dementia prevalence rate.
Despite that the included governorates cover large areas of Egypt, most of them are deserts and are modestly inhabited. The four governorates are inhabited by 8.93% of the Egyptian population.25 Moreover, dementia prevalence increases greatly with an increase in age. This is in line with the result observed in other regions of the world.26 Also, the gender-related susceptibility of dementia is unclear, which is consistent with the study by Kiliaan et al.27 Besides, in all studies, education is found to have a protective role against dementia which is in line with the study by Sharp and Gatz.28
Conclusion
This study aims to provide recent evidence regarding dementia prevalence among the Egyptian population in order to inform policy makers to consider dementia on the health care agenda in order to help relieve the sufferings of people with dementia. This can be achieved through making dementia a public health priority nationally, promoting social awareness about dementia, improving professional attitude toward dementia, and developing dementia policies and plans for supporting caregivers.
Limitations
Some studies have not reported all the data regarding the population with dementia that they investigated; for example, only two studies reported data regarding residence-specific prevalence and the degree of dementia.
Recommendation
There is a gap regarding the prevalence of dementia that needs to be covered. More studies with large sample sizes in multiple regions are in need. Also, well-designed studies investigating the underlying genetic risk factors for dementia, the difference between rural and urban prevalence, and gender susceptibility of dementia among Egyptian population are needed.
Acknowledgments
The authors thank Ahmed Negida, Faculty of Medicine, Zagazig University, for his continuous help, guidance, and support. They also appreciate the help of Medical Research Group of Egypt (MRGE).
Disclosure
The authors declare no conflicts of interest in this work.
References
McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263–269. | ||
Pérès K, Helmer C, Amieva H, et al. Natural history of decline in instrumental activities of daily living performance over the 10 years preceding the clinical diagnosis of dementia: a prospective population-based study. J Am Geriatr Soc. 2008;56(1):37–44. | ||
Brodaty H, Donkin M. Family caregivers of people with dementia. Dialogues Clin Neurosci. 2009;11(2):217–228. | ||
Schulz R, Martire LM. Family caregiving of persons with dementia: prevalence, health effects, and support strategies. Am J Geriatr Psychiatry. 2004;12(3):240–249. | ||
Chaves ML, Ilha D, Maia AL, Motta E, Lehmen R, Oliveira LM. Diagnosing dementia and normal aging: clinical relevance of brain ratios and cognitive performance in a Brazilian sample. Braz J Med Biol Res. 1999;32(9):1133–1143. | ||
Whitehouse PJ. Classification of the dementias. Lancet. 2003;361(9364):1227. | ||
WHO. Thematic briefs for the First WHO Ministerial Conference on Global Action Against Dementia, 16–17 March 2015. Geneva: WHO. Available from: http://www.who.int/mental_health/neurology/dementia/thematic_briefs_dementia/en/. Accessed September 6, 2016. | ||
Kalaria RN, Maestre GE, Arizaga R, et al; World Federation of Neurology Dementia Research Group. Alzheimer’s disease and vascular dementia in developing countries: prevalence, management, and risk factors. Lancet Neurol. 2008;7(9):812–826. | ||
Shaji KS. Dementia care in developing countries: the road ahead. Indian J Psychiatry. 2009;51 (Suppl 1):S5–S7. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. Accessed September 6, 2016. | ||
Issam M, Mostafa A, Tariq M, Sharaqi A, Elwy M. Prevalence of dementia in Egypt: a systematic review. PROSPERO 2016: CRD42016039695. Available from: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016039695 | ||
Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa, ON: Ottawa Hospital Research Institute. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed September 6, 2016. | ||
Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015;314(22):2373–2383. | ||
Farrag A, Farwiz HM, Khedr EH, Mahfouz RM, Omran SM. Prevalence of Alzheimer’s disease and other dementing disorders: Assiut-Upper Egypt study. Dement Geriatr Cogn Disord. 1998;9(6):323–328. | ||
El Tallawy HN, Farghaly WM, Rageh TA, et al. Epidemiology of major neurological disorders project in Al Kharga district, New Valley, Egypt. Neuroepidemiology. 2010;35(4):291–297. | ||
El Tallawy HN, Farghly WM, Shehata GA, et al. Prevalence of dementia in Al Kharga District, New Valley Governorate, Egypt. Neuroepidemiology. 2012;38(3):130–137. | ||
El Tallawy HN, Farghaly WM, Rageh TA, et al. Door-to-door survey of major neurological disorders (project) in Al Quseir City, Red Sea Governorate, Egypt. Neuropsychiatr Dis Treat. 2013;9:767–771. | ||
El Tallawy HN, Farghly WM, Badry R, et al. Prevalence of dementia in Al-Quseir city, Red Sea Governorate, Egypt. Clin Interv Aging. 2014;9:9–14. | ||
Khedr E, Fawi G, Abbas MA, et al. Prevalence of mild cognitive impairment and dementia among the elderly population of Qena Governorate, Upper Egypt: a community-based study. J Alzheimers Dis. 2015;45(1):117–126. | ||
Benamer HTS. Dementia. In: Neurological Disorders in the Arab World. Springer International Publishing; 2014:167–179. | ||
WHO and Alzheimer’s Disease International. Dementia: a public health priority. WHO. Available from: http://www.who.int/mental_health/publications/dementia_report_2012/en/. Accessed September 6, 2016. | ||
Loza N, Fawzi W. Care for the elderly: the Egyptian experience. Neurobiol Aging. 2014;35(3):715. | ||
Awad A, Zohary A. The end of Egypt population growth in the 21st century: challenges and aspirations. In: The 35th Annual Conference on Population and Development Issues: Current Situation & Aspirations; December 20–22, 2005; Cairo. | ||
Bowirrat A, Treves TA, Friedland RP, Korczyn AD. Prevalence of Alzheimer’s type dementia in an elderly Arab population. Eur J Neurol. 2001;8(2):119–123. | ||
Central Agency for Public Mobilization and Statistics (CAPMAS). Egypt in figures 2015. Available from: http://www.msrintranet.capmas.gov.eg/pdf/EgyptinFigures2015/EgyptinFigures/Tables/PDF/1-%20 | ||
Prince M, Ali GC, Guerchet M, Prina AM, Albanese E, Wu YT. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimers Res Ther. 2016;8(1):23. | ||
Kiliaan AJ, Arnoldussen IA, Gustafson DR. Adipokines: a link between obesity and dementia? Lancet Neurol. 2014;13(9):913–923. | ||
Sharp ES, Gatz M. Relationship between education and dementia: an updated systematic review. Alzheimer Dis Assoc Disord. 2011;25(4):289–304. | ||
Loy CT, Schofield PR, Turner AM, Kwok JB. Genetics of dementia. Lancet. 2014;383(9919):828–840. |
 /pop.pdf
/pop.pdf
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.