")
Back to Journals » Infection and Drug Resistance » Volume 13
Prevalence of Common Nosocomial Infections and Evaluation of Antibiotic Resistance Patterns in Patients with Secondary Infections in Hamadan, Iran
Authors Nouri F , Karami P, Zarei O , Kosari F, Alikhani MY , Zandkarimi E , Rezazadeh Zarandi E, Taheri M
Received 21 April 2020
Accepted for publication 25 June 2020
Published 15 July 2020 Volume 2020:13 Pages 2365—2374
DOI https://doi.org/10.2147/IDR.S259252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Fatemeh Nouri,1 Pezhman Karami,2 Omid Zarei,3 Faezeh Kosari,3 Mohammad Yousef Alikhani,2 Eghbal Zandkarimi,4 Ebrahim Rezazadeh Zarandi,5 Mohammad Taheri2
1Department of Pharmaceutical Biotechnology, School of Pharmacy, Hamadan University of Medical Sciences, Hamadan, Iran; 2Department of Medical Microbiology, Faculty of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 3Student Research Committee, Hamadan University of Medical Sciences, Hamadan, Iran; 4Department of Epidemiology and Biostatistics, Faculty of Medicine, Kurdistan University of Medical Sciences, Sanandaj, Iran; 5Immunology of Infectious Diseases Research Center, Research Institute of Basic Medical Sciences, Rafsanjan University of Medical Sciences, Rafsanjan, Iran
Correspondence: Mohammad Taheri
Department of Medical Microbiology, Hamadan University of Medical Sciences, Hamadan, Iran
Tel +98-9124061190
Fax +98-8134237100
Email [email protected]
Introduction: The prevalence of nosocomial infections in patients hospitalized to three hospitals of Shahid Beheshti, Farshchian, and Be’ saat in Hamadan was investigated for 2 years (2018 to 2020).
Materials and Methods: The samples were cultured and characterized using morphological and diagnostic biochemical tests. The analysis of the frequency of the isolates and their antibiotic resistance were calculated using SPSS (version 22) at a significant level of P-value < 0.05.
Results: Bacterial isolates were collected from the 1194 clinical specimens, of which 1394 were isolated from urine, 16 from CSF, and 588 from tracheal aspiration. Also, 654 (54.8%) isolates were obtained from females and 540 (45.2%) from males with the age range 15– 73 years (P> 0.05). The results showed that 22.1% were gram-positive and 77.9% were gram-negative. In our study, the frequency of Klebsiella pneumoniae bacteria was higher than in some studies, and this indicates the genetic changes and resistance of this bacterium to many antibiotics.
Conclusion: To prevent further spread of resistance, increase the effectiveness of antibiotics and prevent multidrug resistance, it is essential to establish a precise schedule for the use of antibiotics and assess the resistance pattern periodically in each region based on the antibiotic resistance pattern.
Keywords: nosocomial infections, UTI, trachea, CSF, antimicrobial resistance pattern
Introduction
Nosocomial infections (NI) include infections that are acquired from a hospital or other health care centers, which appear for the first time within 48 hours of hospital admission, 3 days of discharge or 30 days of operation.1,2 However, in some cases, the NIs occur within 30 days after discharge, such as surgical site infections.2 Over recent decades, NIs have become a major health concern worldwide. Due to the increasing number of health centers and hospitals, emerging new infectious diseases or the re-emergence of old infectious diseases, increasing antibiotic resistance and prolonging the length of stay for hospitalized patients receiving specialist care, NIs are rapidly increasing, especially in developing countries.3 There are no accurate statistics on the prevalence of NIs, their adverse health effects, and financial complications in Iran. Based on the previous studies on the prevalence and antimicrobial resistance, it can be concluded that there is a different prevalence of NIs in Iranian hospitals.4 Many factors can cause NIs, including patient age (children and elderly individuals are more susceptible to contracting NIs), underlying diseases (eg failure in various organs, impaired mucosal defense in burn wound, trauma, surgery and immunodeficiency disorder), receiving immunosuppressive drugs, malnutrition and catheter-related infections.5–7 The most common causes of NIs include Escherichia coli (the main cause of urinary tract infections), Staphylococcus aureus (the main cause of surgical site and respiratory tract infections),8,9 Pseudomonas aeruginosa (the cause of respiratory tract infections),9 and Gram-positive bacteria (most common microorganisms in the development of primary bacteremia).10,11 The three major sites for NIs include urinary tract system (31%), respiratory system (24%), and the bloodstream (16%). The NIs can also occur in the skin and other organs. Pneumonia, urinary tract infection, and septicemia are the most commonly diagnosed NIs on the three major sites. It has been reported that Ventilator-associated Pneumonia (VAP) is the most common nosocomial infection in the intensive care unit (ICU) and responsible for approximately fifty percent of all hospital-acquired pneumonia cases12 and UTI is the most common NIs in the developed countries.13 Catheterization leads to about 80% of hospital-acquired UTIs due to the formation of microbial biofilms and especially biofilms composed of Klebsiella spp. and Candida.14 Since the formation of biofilm is an important factor in increasing antibiotic resistance and decreasing drug sensitivity, it is essential to pay particular attention to the catheters used in hospitalized patients and urinary catheter users.9,15,16
Due to the importance of hospitals in providing health services, emerging new infectious diseases, increasing antibiotic resistance, prolonging the length of stay for hospitalized patients and lack of accurate information and statistics on NIs in Iran, this study aimed to provide the prevalence of NIs in Hamadan, west of Iran in comparison with the international statistics. Moreover, this article also aimed to determine the antimicrobial resistance patterns and prevalence of the resistant isolates in NIs in hospitalized patients.
Materials and Methods
In this study, the prevalence of nosocomial infections in hospitalized patients to three hospitals of Shahid Beheshti, Farshchian, and Besaat in Hamadan was evaluated for 2 last years (2018 to 2020).
The prevalence of pulmonary infection (VAP), UTI, cerebrospinal fluid (CSF) infection were investigated in terms of causing agent and its frequency as well as the pattern of antibiotic resistance to commonly used antibiotics. The samples were taken from patients at the time of 48 hours after hospital admission. The samples were cultured and characterized using morphological and biochemical tests according to microbiological guidelines. Briefly, for urine samples, midstream urine samples were collected and then cultured on blood agar and MacConkey agar media. Finally, the cultured samples were incubated at 37 °C for 24–48 h. Tracheal samples were taken from the lower respiratory tract under sterile conditions and cultured on blood or chocolate and MacConkey agar. The cultured samples were incubated at 37 °C for 24 h. Diagnostic biochemical tests were performed to identify the agents isolated from the infections depending on the isolate type, sampling site, and gram-positive or negative bacteria. Also, catalase, coagulase, optochin, and novobiocin disks, CAMP, and esculin agar tests were utilized for the identification of the isolated gram-positive bacteria. Moreover, the indole diagnostic, Triple Sugar Iron Agar (TSI), citrate, lysine decarboxylase, oxidase, and motility tests were used for the identification of the isolated gram-negative bacteria. Then, the antibiotic resistance of the isolates was analyzed using Modified Disk Diffusion Method (MDDM) by Mueller-Hinton agar medium according to the Clinical & Laboratory Standards Institute (CLSI) instructions. For this purpose, a suspension of pure bacteria with a concentration of 0.5 McFarland (1.5 × 108 CFU.mL−1) was prepared in sterile saline and the antibiotic resistance of the isolates was evaluated against different antibiotic groups.
In the present study, E. coli strain (ATCC 25922) was used as the control strain for antibiotic susceptibility testing. Various groups of antibiotic including aminoglycosides (amikacin and gentamicin), carbapenem (imipenem), first-generation cephalosporins (cephasoline), second-generation cephalosporins (cefotaxime), third-generation cephalosporins (ceftazidime, ceftriaxone), nitrophores (nitrofurantoin), quinolones (ciprofloxacin and nalidixic acid), sulfonamides (co-trimoxazole), glycopeptides (vancomycin), macrolides (azithromycin) were investigated. After 24 h of incubation at 37 °C, the diameter of the growth zone was measured and the sensitivity of the isolates was estimated according to the CLSI instructions. The frequency of the isolates and their antibiotic resistance were analyzed by using SPSS (version 22) with a 0.05 significant level.
Results
In this research, bacterial isolates were obtained from 1194 clinical specimens, of which 1394 were isolated from urine, 16 from CSF, and 588 from tracheal aspiration. Also, 654 (54.8%) isolates were collected from females and 540 (45.2%) from males with the age range 15–73 years (P> 0.05). The results showed that 22.1% were gram-positive and 77.9% were gram-negative.
The most frequent in gram-negative samples were in the order of E. coli with 832 (59.6%), K. pneumoniae with 139 (9.9%), P. aeruginosa 71 (5.09%), Enterobacter spp. 31 (2.2%), Acinetobacter baumannii 30 (2.15%), Klebsiella oxytoca 18 (1.2%) which isolated from UTI specimens; K. pneumoniae 3 (18.7%), P. aeruginosa 1 (6.25%) which isolated via CSF and K. pneumoniae 164 (27.8%), A. baumannii 118 (20.06%), P. aeruginosa 97 (16.4%), E. coli 57 (9.6%) which were isolated from tracheal aspiration. In gram-positive isolates, the most abundance samples were S. aureus 70 (5.02%) and coagulase-negative staphylococci species including, S. epidermidis 52 (3.7%), S. saprophyticus 13 (0.09%), Micrococcus 35 (2.5%), S. pyogenes 9 (0.06%) and Enterococcus 9 (0.06%) in UTI samples. The most frequent gram-positive isolates in the tracheal sample including S. aureus 52 (8.8%), S. epidermidis 27 (4.5%); and S. viridans 11 (68.7%) and S. aureus 1 (6.25%) were isolated from CSF samples (Table 1).
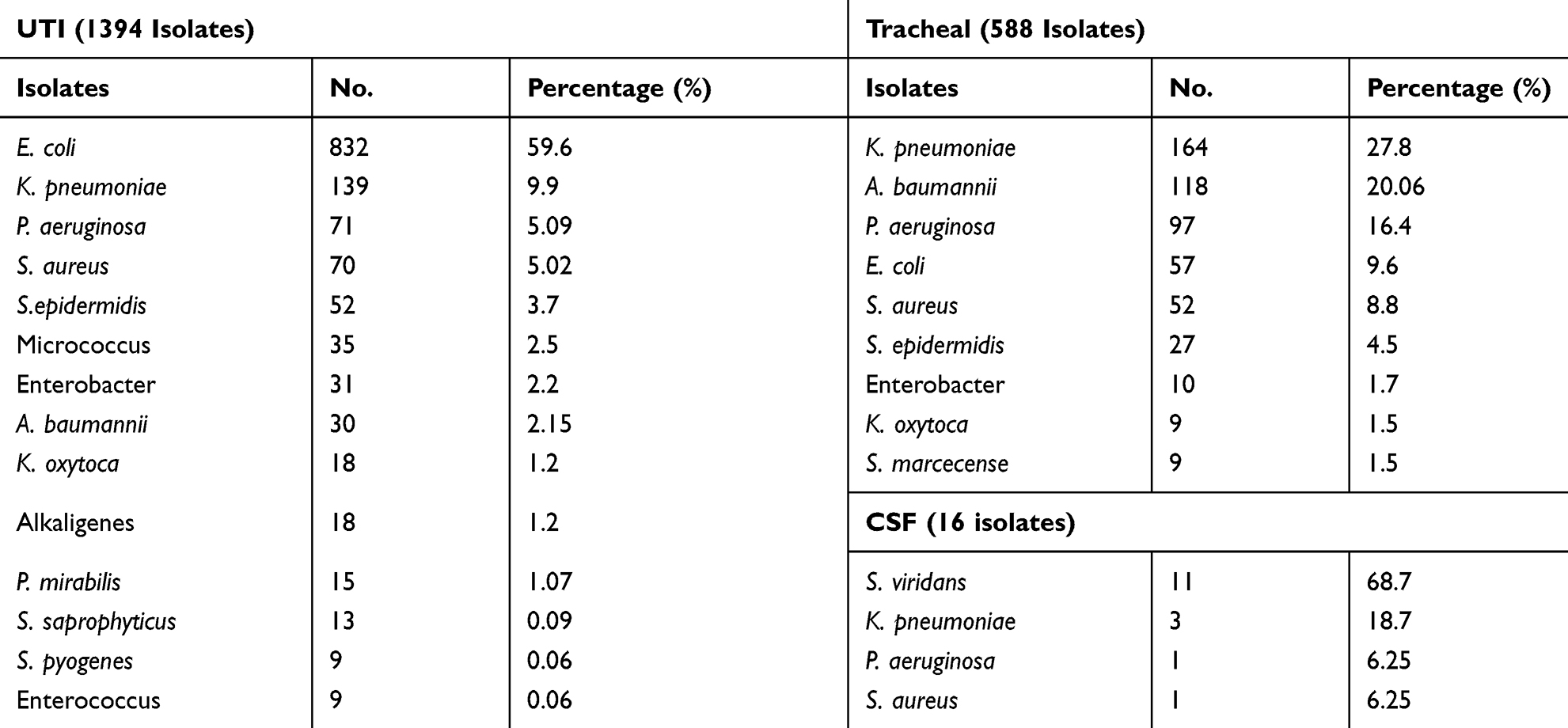 |
Table 1 The Most Prevalent Bacterial Isolates According to Their Sampling Sites |
Moreover, 123 antibiotic-resistant S. aureus isolates were detected. S. aureus 70 (5.02%), 52 (8.8%), and 1 (6.25%) which were isolated from UTI, tracheal, and CSF respectively. The rest of the resistant isolates were collected from other parts of the patient’s body. The maximum antibiotic resistance in K. pneumoniae was observed against cefotetan 81 (58.2%), in UTI (Table 2), and the tracheal (Table 3) and CSF samples (Table 4) ceftazidime 120 (73.1%) and 3 (100%) were observed respectively.
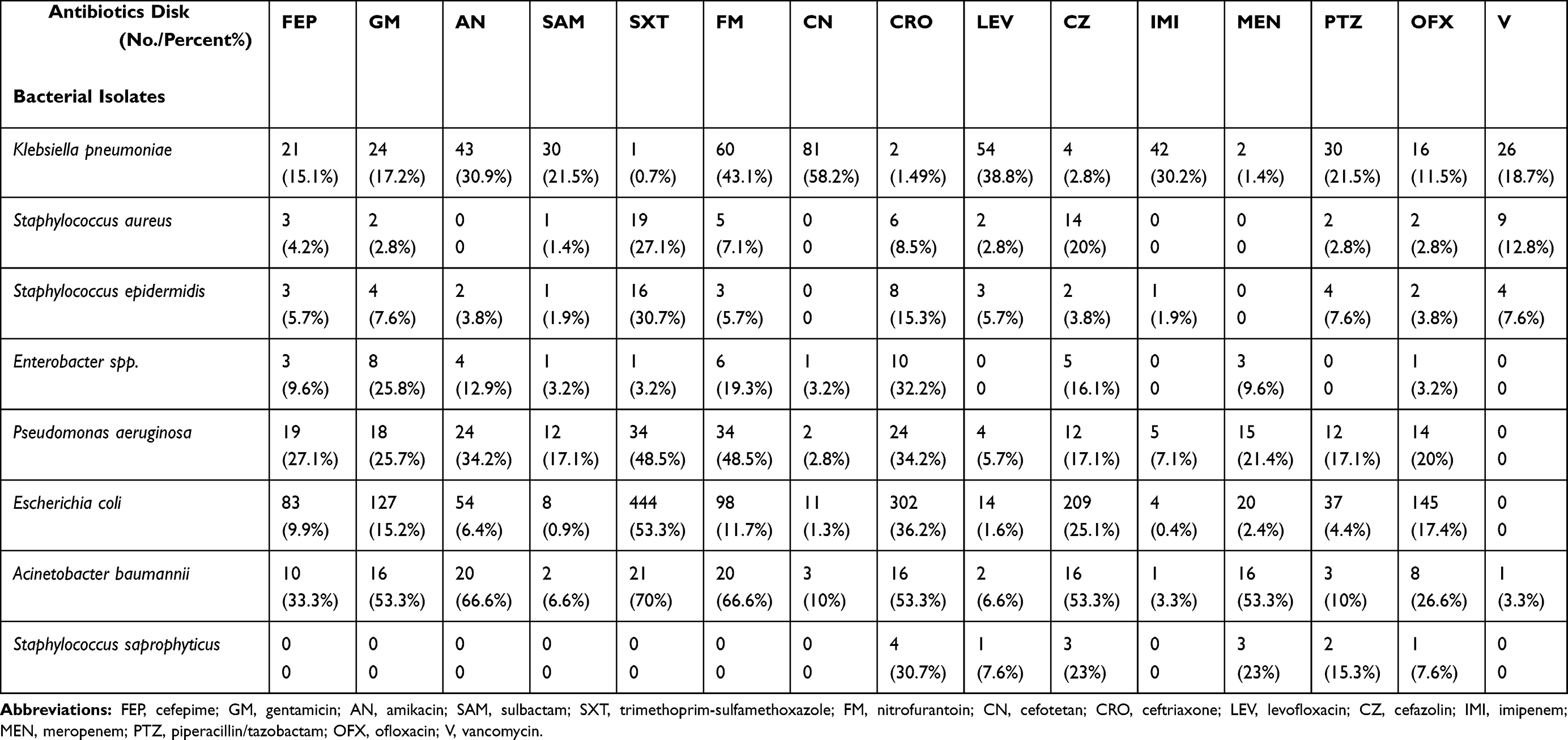 |
Table 2 Antibiotic Resistance Profile of Organisms Isolated from UTI Infections |
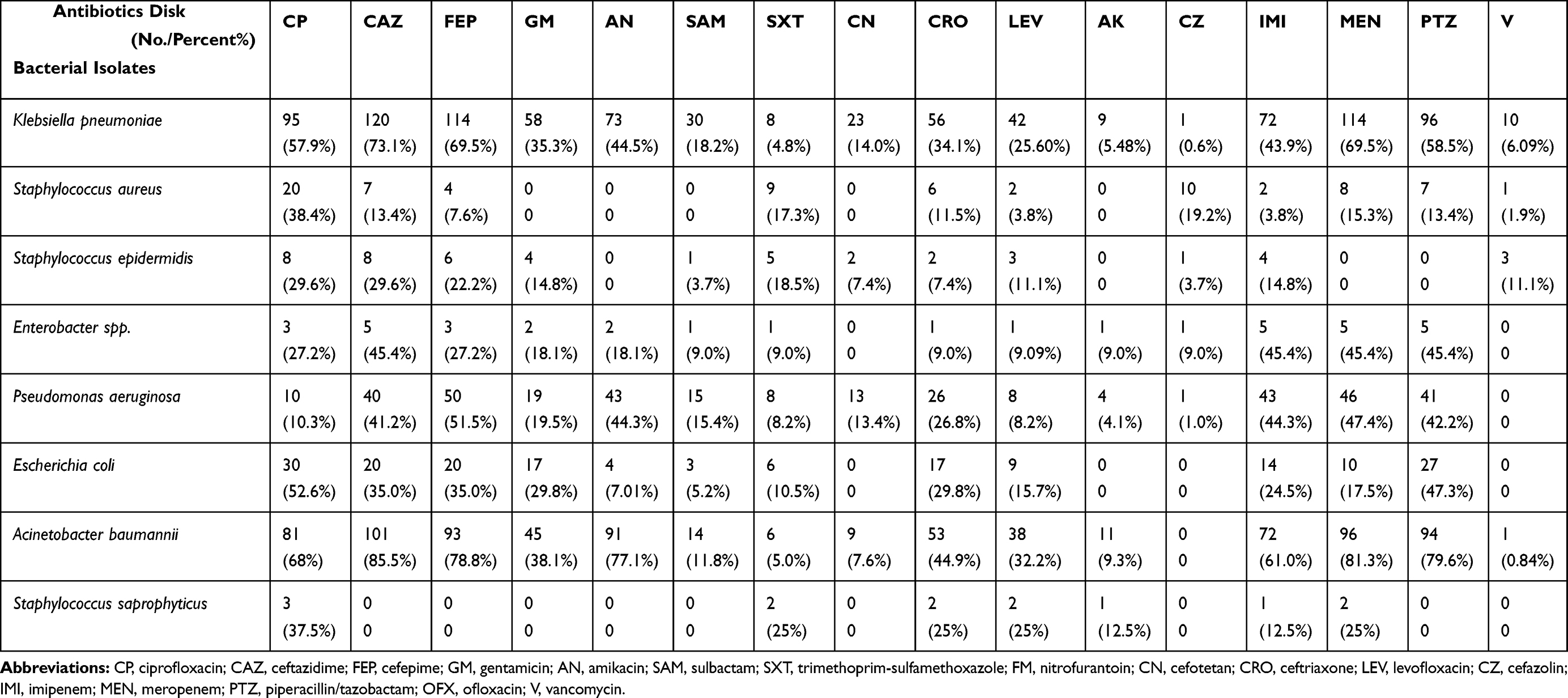 |
Table 3 Antibiotic Resistance Profile of Organisms Isolated from Tracheal Infections |
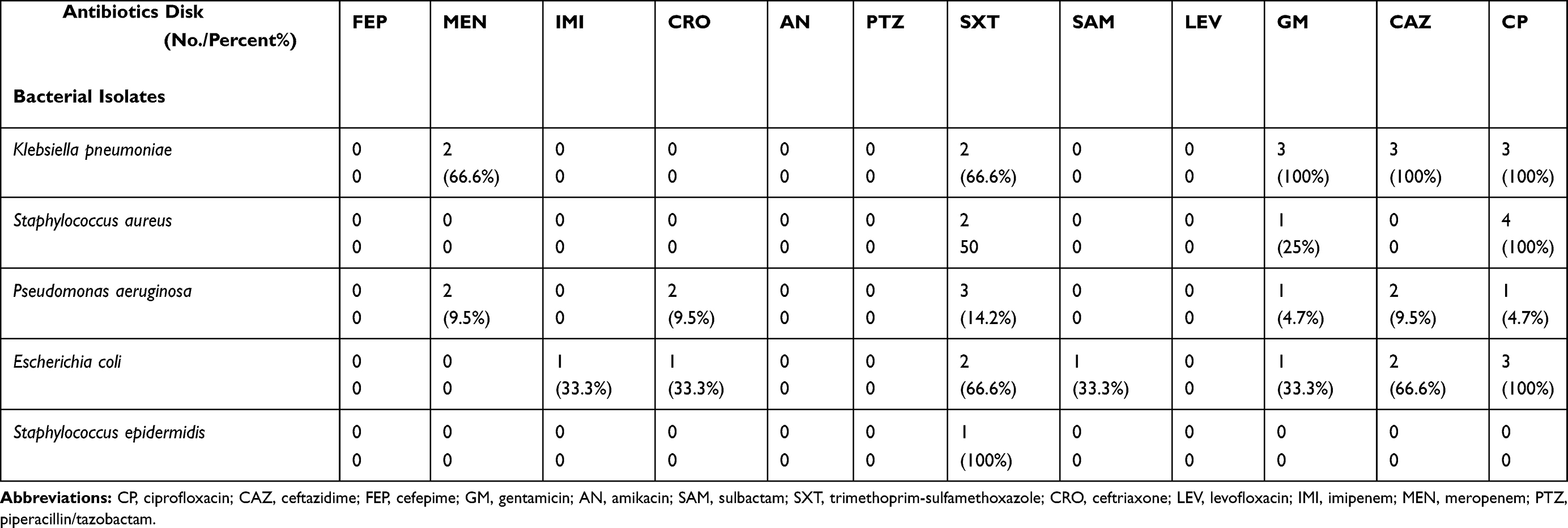 |
Table 4 Antibiotic Resistance Profile of Organisms Isolated from CSF Infections |
For S. epidermidis isolates, as observed, 80 isolates of S. epidermidis were resistant to the studied antibiotics including 52 (3.7%), 27 (4.5%), and 1 (6.25%) resistance isolates were obtained from the urine, trachea, and CSF samples, respectively. According to the results, there were 41 resistance samples among the Enterobacter isolates. Of them, 31 (2.2%) and 10 (1.7%) were isolated from the urine and trachea of the patients, and no resistance was observed in the Enterobacter samples isolated from CSF. Of all Pseudomonas isolates, 169 specimens showed antibiotic resistance. Among them, 71 (5.09%), 97 (16.4%), 1 (6.25%) specimens were isolated from urine, tracheal tube, and CSF respectively. Also, there were 892 resistance samples in E. coli isolates, of which 832 (59.6%), 57 (9.6%), and 3 (15.7%) specimens were isolated from urine, trachea, and CSF, respectively.
Based on the results, there were 148 antibiotic-resistant isolates were detected among the Acinetobacter isolates. Of them, 30 (2.1%), 118 (20.06%) resistantisolates were isolated from urine and trachea, respectively. There were 26 antibiotic-resistant isolates among Proteus spp. isolates. Of them, 15 (1.07%) Proteus mirabilis were isolated via UTI. Proteus vulgaris 7 (1.1%) and Proteus mirabilis 4 (0.6%) were isolated from tracheal samples. In total, 27 antibiotic-resistant isolates were identified in K. oxycoca bacteria, of which 18 (1.2%) and 9 (1.5%) were isolated from urine and tracheal samples, respectively. In S. saprophyticus isolates, 125 resistant isolates were detected, which 13 (0.09%) isolates obtained from UTI samples.
20 antibiotic-resistant isolates were detected in Group A 9 (0.6%) and B 9 (0.6%) streptococci, of which 18 (1.2%) were isolated from the UTI samples, and 2 (0.2%) others isolated from the trachea samples (Table 1). In the Enterococci (Group D streptococci) bacteria isolated from patients, 12 antibiotic-resistant isolates were identified, of which 3 (0.5%) and 9 (0.6%) samples were isolated from tracheal and urine samples, respectively. Listeria isolates were not isolated from the studied sites, including trachea, urine, CSF. Morganella Morgani 2 (0.1%) and Moraxella catarrhalis 2 (0.1%) showed antibiotic resistance and all of them (100%) were isolated in urine samples. Besides, in the tracheal samples 1 (0.1%) Moraxella catarrhalis was isolated.
In Hafnia alvei isolates, 3 resistant were identified, which 1 (0.07%) and 2 (0.3%) from the urine and tracheal samples were isolated. Also, 1 resistant isolate was detected among Edwardsia isolates, which all of them were isolated from urine samples (100%).
In Alcaligenes spp isolates, there were 19 resistant specimens, 18 (1.2%) and 1 (0.1%) samples were isolated from urine and trachea, respectively. In S. marcescens isolates, 11 antibiotic resistance specimens were detected. Of the 9 (1.5%) and 2 (0.1%), isolates were obtained from the trachea and urine samples, respectively. Also, 5 resistant isolates were identified in diphtheroid isolates, 2 (0.1%) and 3 (0.5%) of which were isolated from urine and trachea samples.
Discussion
The spread of antibiotic-resistant NIs or healthcare-associated infections has become a public health concern worldwide.17,18 The rate of NI in developed and developing countries is 7% and 10% respectively. This difference in antimicrobial susceptibility depends on several factors including endemic resistant pathogens, misuse or overuse of antibiotics in the treatment of patients, the severity of the disease, longer hospitalization are the most important factors.19 Because these infections occur during hospitalization along with disability, prolong hospitalization, and economic burden.10 Increasing antibiotic resistance among the microorganisms causing NIs is associated with a high mortality rate in hospitalized patients.20,21 Investigating the prevalence of these resistant bacteria can be useful to control NIs.22,23
In this study, the prevalence of gram-negative bacteria (77.9%) in NIs was much higher than that of gram-positive bacteria (22.1%). Hence, the main cause of NIs is gram-negative bacteria, which is consistent with the findings of the Sikka et al.24 Moreover, our findings implied that UTI is the main nosocomial infection caused by bacteria. According to the results, the most prevalent gram-negative bacteria causing NIs were in the order of E. coli>Klebsiella>P. aeruginosa, which is consistent with the findings of Tolera et al, and Sikka et al.21,24 Also, the most common bacterium causing NIs among gram-positive bacteria was S. aureus, which is in agreement with Wang et al.25
The prevalence of antibiotic resistance in the studied bacteria was in the order of E. coli> Klebsiella>Acinetobacter>S. aureus that is in contrast with Amini et al in 2017 study26 in that reported Klebsiella with the low prevalence and our study antibiotic resistance to Klebsiella was increased and placed in the second prevalent bacteria. Generally, the most prevalent and antibiotic resistance in the studied bacteria were observed in the samples isolated from tracheal aspiration and UTIs. Agaba et al, also reported that Klebsiella, Acinetobacter, and S. aureus were the most cause of NIs. In the mentioned study, the most resistant isolates were isolated from tracheal aspiration and UTIs, which is in agreement with our findings.27 The resistance to A. baumannii as one of the most important pathogens acquired from hospitals is increasing and the evaluation of its antimicrobial patterns is so necessary.28,29
In the present study, antibiotic resistance was observed to different antibiotics. The most resistant to cefotetan, nitrofurantoin, levofloxacin, amikacin, imipenem, piperacillin-tazobactam, co-trimoxazole, were found in E. coli isolates from urine samples. In Maechler study in 2015, Klebsiella isolates 13%30 was reported compared with the present research with 27.8% in the trachea. This difference may be attributed to the sampling site of the specimens because, in the mentioned study, all samples were only isolated from the ICU ward, where patients had a weakened immune system. In the current study, the highest prevalence of antibiotic resistance in Klebsiella strains was observed in trachea and urine specimens. Also, the antibiotic resistance to ciprofloxacin, ceftazidime, cefepime, amikacin, imipenem, meropenem, and piperacillin discs was higher than other studied antibiotics (Table 2).
The prevalence of antibiotic resistance in gram-positive S. aureus and S. epidermidis was lower than in gram-negative bacteria. The results of Carlsen et al,31 study on the susceptibility of urinary pathogens causing NIs showed that the highest antibiotic susceptibility to ciprofloxacin and nitrofurantoin was observed in E. coli and K. pneumoniae isolates, respectively and these results are consistent with our findings. In the present study, the more number of antibiotics were investigated, and there was a higher antibiotic susceptibility in some studied antibiotics such as nitrofurantoin, ampicillin, clindamycin, linezolid, penicillin G, oxacillin, piperacillin, and tobramycin. In our research Klebsiella and E. coli isolates susceptibility to co-trimoxazole are in contrast in UTI samples so that the resistance rate for Klebsiella and E.coli was 1 (0.7%) and 444 (53%) against co-trimoxazole are the minimum and maximum resistance to co-trimoxazole respectively.31 This finding of Klebsiella is in contrast with the Sakkas H study in 201932 that reported the prevalence of co-trimoxazole resistant bacteria 95%. This difference may be due to the different geographical region and so in our region, the pattern of antibacterial resistance of klebsiella to co-trimoxazole is different from other areas significantly. It can be interpreted that co-trimoxazole prescription for UTI infection is a low rate. In addition, the resistance rate of K. pneumoniae to fluoroquinolones including levofloxacin and ciprofloxacin is approximately 50% in the urine and trachea sources and is in agreement with our previous study.33
Khanal et al,34 is in agreement with this research that reported the most gram-negative bacteria were isolated from the aspirate samples of Acinetobacter spp. Then, K. pneumoniae and subsequently Pseudomonas strains with multi-drug resistance to combined cefotaxime and cefotaxime-clavulanate were also identified. In the current work, the rate of resistant Acinetobacter baumannii to ceftazidime and meropenem was 85.1% and 81.3% in the urine and trachea samples, respectively.
Moreover, in Malik et al,35 K. pneumoniae was identified as the most common bacteria. The highest sensitivity was also observed among the combined drugs of cefoperazone-sulbactam and piperacillin-tazobactam, in which over 60% sensitivity was observed among gram-negative bacteria and 100% sensitivity to vancomycin and linezolid was observed among gram-positive bacteria. These results are consistent with our findings in terms of the sequence of the strains. One S. aureus isolated from the trachea was resistant to vancomycin although the confidential test to confirm or reject this finding is necessary. Also, resistance to vancomycin in S. aureus was reported previously.32 In terms of Acinetobacter, a study in Pakistan in 201636 that reported the high prevalence of resistance to 3rd generation of cephalosporins approximately 100%, is in contrast to the present work in which Acinetobacter isolates resistance rate was lower than 50% that may be due to the overuse of aforementioned antibiotics in that country that is in neighboring of Iran.
Conclusion
In this study, the prevalence of antibiotic resistance was high in most common pathogenic strains. Therefore, the results of this study demonstrated that antibiotics with a high resistance level must be less used for the treatment of infections. Moreover, to prevent the spread of resistance among various strains and improve the effectiveness of antibiotics, it is suggested to establish a precise schedule for antibiotic use in each region based on their antibiotic resistance pattern. Due to the increase in the number of tracheal infections as well as the emergence of antibiotic-resistant strains, it is necessary to take the necessary guidelines to minimize these cases including directional airflow in the room and the use of positive pressure to prevent the placement of infectious particles in the isolated room.
Abbreviations
NIs, nosocomial infections; UTI, urinary tract infection; ICU, intensive care unit; VAP, ventilator-associated pneumonia.
Data Sharing Statement
All data used are available. Please contact the corresponding authors for data requests.
Ethics Approval
This study was approved by the ethics committee of Hamadan University of Medical Sciences.
Consent to Participate
In this study, we weren’t in touch with the children directly, although all sample urines were collected from the laboratory of the Be’ sat, Beheshti, and Sina hospitals.
Acknowledgment
We are thankful for the cooperation of the laboratory of the Be’ sat, Beheshti, and Sina hospitals and we are grateful for Hamadan University of Medical Sciences for their financial supports of this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicting interests related to this manuscript.
References
1. Revelas A. Healthcare–associated infections: a public health problem. Nigerian Med J. 2012;53(2):59. doi:10.4103/0300-1652.103543
2. Cassini A, Högberg LD, Plachouras D, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66. doi:10.1016/S1473-3099(18)30605-4
3. Rezai MS, Bagheri-Nesami M, Nikkhah A. Catheter-related urinary nosocomial infections in intensive care units: an epidemiologic study in North of Iran. Caspian J Inter Med. 2017;8(2):76.
4. Darvishpoor K, Rezaei Manesh MR. Prevalence of nosocomial infections and microbial causes in Torbat heydariyeh 9dey educational and clinical hospital in 2012 and 2013. Iran J Med Microbiol. 2016;10(1):93–96.
5. Madani SH, Khazaei S, Kanani M, Shahi M. Antibiotic resistance pattern of E. coli isolated from urine culture in Imam Reza Hospital Kermanshah-2006. 2008.
6. Organization WH. Report on the burden of endemic health care-associated infection worldwide. 2011.
7. Zhou X, García-Cobos S, Ruijs GJ, et al. Epidemiology of extended-spectrum β-lactamase-producing E. coli and vancomycin-resistant enterococci in the Northern Dutch–German cross-border region. Front Microbiol. 2017;8:1914. doi:10.3389/fmicb.2017.01914
8. Anderson DJ. Surgical site infections. Infect Dis Clin North Am. 2011;25(1):135–153. doi:10.1016/j.idc.2010.11.004
9. Khademi F, Yousefi AA, Karami P, Ghazvini K, Ghanbari F. Prevalence and antimicrobial susceptibility patterns of bacteria isolated from different clinical infections in Hamadan, Iran. Infection, Epidemiology and Medicine. 2016;2(3):8–13. doi:10.18869/modares.iem.2.3.8
10. Khan HA, Baig FK, Mehboob R. Nosocomial infections: epidemiology, prevention, control and surveillance. Asian Pac J Trop Biomed. 2017;7(5):478–482. doi:10.1016/j.apjtb.2017.01.019
11. Khan HA, Ahmad A, Mehboob R. Nosocomial infections and their control strategies. Asian Pac J Trop Biomed. 2015;5(7):509–514. doi:10.1016/j.apjtb.2015.05.001
12. Kalanuria AA, Zai W, Mirski M. Ventilator-associated pneumonia in the ICU. Critical Care. 2014;18(2):208. doi:10.1186/cc13775
13. Rao R, Khan AA, Mathai D, et al. Prevalence and risk factors for hospital-acquired infections “clean care is safer care. 2020.
14. Majumder MMI, Ahmed T, Ahmed S, Khan AR. Microbiology of Catheter Associated Urinary Tract Infection. Microbiology of Urinary Tract Infections-Microbial Agents and Predisposing Factors. IntechOpen; 2018.
15. Aminiahidashti H, Bozorgi F. Current knowledge about nosocomial infections. Advan Biores. 2016;7:4.
16. Challacombe SJ. Immunologic aspects of oral candidiasis. Oral Surg Oral Med Oral Pathol. 1994;78(2):202–210. doi:10.1016/0030-4220(94)90148-1
17. O’neill J. Antimicrobial resistance. Tackling a crisis for the health and wealth of nations. 2014.
18. Bereket W, Hemalatha K, Getenet B, et al. Update on bacterial nosocomial infections. Eur Rev Med Pharmacol Sci. 2012;16(8):1039–1044.
19. Bonnet V, Dupont H, Glorion S, et al. Influence of bacterial resistance on mortality in intensive care units: a registry study from 2000 to 2013 (IICU Study). J Hosp Infect. 2019;102(3):317–324. doi:10.1016/j.jhin.2019.01.011
20. Oliphant CM, Eroschenko K. Antibiotic resistance, part 2: gram-negative pathogens. J Nurs Pract. 2015;11(1):79–86. doi:10.1016/j.nurpra.2014.10.008
21. Tolera M, Abate D, Dheresa M, Marami D. Bacterial nosocomial infections and antimicrobial susceptibility pattern among patients admitted at Hiwot Fana Specialized University Hospital, Eastern Ethiopia. Advan Med. 2018;2018.
22. Denning DW, Perlin DS, Muldoon EG, et al. Delivering on antimicrobial resistance agenda not possible without improving fungal diagnostic capabilities. Emerg Infect Dis. 2017;23(2):177. doi:10.3201/eid2302.152042
23. Reacher MH, Shah A, Livermore DM, et al. Bacteraemia and antibiotic resistance of its pathogens reported in England and Wales between 1990 and 1998: trend analysis. BMJ. 2000;320(7229):213–216. doi:10.1136/bmj.320.7229.213
24. Sikka R, Mann J, Vashist M, Chaudhary U, Deep A. Prevalence and antibiotic sensitivity pattern of bacteria isolated from nosocomial infections in a Surgical Ward. 2012.
25. Wang A, Daneman N, Tan C, Brownstein JS, MacFadden DR. Evaluating the relationship between hospital antibiotic use and antibiotic resistance in common nosocomial pathogens. Infect Control Hosp Epidemiol. 2017;38(12):1457–1463. doi:10.1017/ice.2017.222
26. Amini M, Vaseie M, Ansari I. The evaluation of nosocomial urinary tract infections and antimicrobial resistance in ICU patients, Tehran, Iran, 2012-2016. Acta Medica Mediterranea. 2017;33:945–952.
27. Agaba P, Tumukunde J, Tindimwebwa J, Kwizera A. Nosocomial bacterial infections and their antimicrobial susceptibility patterns among patients in Ugandan intensive care units: a cross sectional study. BMC Res Notes. 2017;10(1):349. doi:10.1186/s13104-017-2695-5
28. Bahador A, Bazargani A, Taheri M, et al. Clonal lineages and virulence factors among Acinetobacter baumannii isolated from Southwest of Iran. J Pure Appl Micribiol. 2013;7:1559–1566.
29. Khaledi A, Elahifar O, Vazini H, et al. Increasing trend of imipenem-resistance among acinetobacter baumannii isolated from Hospital Acquired Pneumonia in Northeast of Iran. Avicenna J Clin Microbiol Infect. 2017;4(3):e45454. doi:10.5812/ajcmi.45454
30. Maechler F, Diaz LP, Schröder C, Geffers C, Behnke M, Gastmeier P. Prevalence of carbapenem-resistant organisms and other Gram-negative MDRO in German ICUs: first results from the national nosocomial infection surveillance system (KISS). Infection. 2015;43(2):163–168. doi:10.1007/s15010-014-0701-6
31. Carlsen S, Krall SP, Xu KT, Tomanec A, Farias D, Richman P. Sensitivity of urinary pathogens for patients discharged from the emergency department compared with the hospital antibiogram. BMC Emerg Med. 2019;19(1):1–4. doi:10.1186/s12873-019-0264-z
32. Sakkas H, Bozidis P, Ilia A, Mpekoulis G, Papadopoulou C. Antimicrobial resistance in bacterial pathogens and detection of carbapenemases in Klebsiella pneumoniae isolates from Hospital Wastewater. Antibiotics. 2019;8(3):85. doi:10.3390/antibiotics8030085
33. Shokoohizadeh L, Saniee M, Mirzaee M, Taheri M. Mutations in gyrA and parC genes in quinolone-resistant klebsiella pneumoniae isolates from borujerd hospitals. J Adv Med Biomed Res. 2019;27(120):1–7.
34. Khanal S, Joshi DR, Bhatta DR, Devkota U, Pokhrel BM. β-lactamase-producing multidrug-resistant bacterial pathogens from tracheal aspirates of intensive care unit patients at National Institute of Neurological and Allied Sciences, Nepal. ISRN Microbiol. 2013;2013.
35. Malik MI, Malik M, Chaudhary A. Antimicrobial susceptibility pattern of bacteria isolated from tracheal secretions in intensive care units admitted patients of Lahore General Hospital. Pak J Chest Med. 2018;24(2):72–77.
36. Sohail M, Rashid A, Aslam B, et al. Antimicrobial susceptibility of Acinetobacter clinical isolates and emerging antibiogram trends for nosocomial infection management. Rev Soc Bras Med Trop. 2016;49(3):300–304. doi:10.1590/0037-8682-0111-2016
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.