")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Prevalence of Asymptomatic Venous Thromboembolism in Depressive Inpatients
Authors Takeshima M , Ishikawa H, Umeta Y , Kudoh M, Umakoshi A, Yoshizawa K , Ito Y , Hosoya T, Tsutsui K, Ohta H, Mishima K
Received 21 December 2019
Accepted for publication 20 February 2020
Published 26 February 2020 Volume 2020:16 Pages 579—587
DOI https://doi.org/10.2147/NDT.S243308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Taro Kishi
Masahiro Takeshima,1 Hiroyasu Ishikawa,1 Yoshiaki Umeta,2 Mizuki Kudoh,3 Akise Umakoshi,1 Kazuhisa Yoshizawa,4 Yu Ito,1 Tomoko Hosoya,1 Ko Tsutsui,1 Hidenobu Ohta,1 Kazuo Mishima1
1Department of Neuropsychiatry, Akita University Graduate School of Medicine, Akita 010-8543, Japan; 2Department of Psychiatry, Omagari City Hospital, Akita 014-0067, Japan; 3Department of Neuropsychiatry, Nakadori Rehabilitation Hospital, Akita 010-0001, Japan; 4Department of Psychiatry, Akita City Hospital, Akita 010-0933, Japan
Correspondence: Masahiro Takeshima
Department of Neuropsychiatry, Akita University Graduate School of Medicine, 1-1-1, Hondo, Akita 010-8543, Japan
Tel +81-18-884-6122
Fax +81-18-884-6445
Email [email protected]
Purpose: While depression has been recognized as a risk factor for venous thromboembolism (VTE), the prevalence of VTE in depressed inpatients has never been investigated. The aim of this study was thus to examine VTE prevalence and factors associated with VTE in depressed inpatients.
Patients and Methods: We conducted a retrospective cross-sectional study of consecutive depressed inpatients (n = 94) from January 1, 2018, to June 30, 2019, at the psychiatry department of Akita University Hospital. As part of our clinical routine, depressed inpatients were screened for VTE using D-dimer, and patients who screened positive underwent enhanced CT to examine VTE. A variety of data was extracted from medical records, including, amongst others, age, sex, body mass index, diagnoses of psychiatric disorders, total scores on the 17-item Hamilton Depression Rating Scale, duration of current depressive episode, daily dosages of antidepressants and antipsychotics, catatonia, and physical restraint.
Results: VTE was detected in 8.5% of depressed inpatients. There were no significant differences between VTE-positive and VTE-negative inpatients regarding any of the considered factors.
Conclusion: Our analysis shows a VTE prevalence of 8.5% in depressed inpatients, higher than that of 2.3% reported in a previous study in hospitalized patients with psychiatric disorders including depression. This emphasizes the importance of VTE screening for depressive inpatients.
Keywords: antidepressant, bipolar disorder, depression, sudden death, venous thrombosis
Introduction
Venous thromboembolism (VTE), comprising pulmonary embolism (PE) and deep-vein thrombosis (DVT), is an important cause of sudden death in patients with mental disorders.1 Catatonia and restraint have been pointed out as risk factors for VTE in the psychiatric field.2–4 Recently, depression also has been recognized as a risk factor for VTE. Since the 2000s, a series of large-scale observational studies were performed to investigate the relationships between depression, antidepressant use, and VTE.5–9 In 2018, Kunutsor et al meta-analyzed previous studies and reported that individuals with depression had a 1.31-fold and those using antidepressants a 1.27-fold increased risk of VTE.10 Parkin et al reported in a large prospective cohort study of women that the group taking antidepressants had a 1.22-fold increased risk of VTE compared to the group who showed depression or anxiety symptoms but did not take psychotropic drugs.9 The authors stated, however, that it was unclear whether the increased risk of VTE in the antidepressant group was due to the pharmacological effects of the antidepressants or to the effects of other factors related to depression and anxiety. Depressed patients may experience reduced mobility and dehydration, which may affect the onset of VTE. However, the relationship between depression severity and episode duration and thrombotic risk has not been investigated. Inpatients generally have more severe depressive symptoms than outpatients and may thus have a higher risk of VTE than outpatients. The prevalence of VTE in akinetic/hypokinetic patients has been shown to be relatively high compared to other patients with psychiatric disorders: 25.3% for catatonic inpatients,3 11.6% for restrained inpatients,4 and 2.3% for psychiatric inpatients.2 However, the prevalence of VTE in depressive inpatients has not been examined.
A VTE prevalence of 2.3–25.3% in hospitalized patients with psychiatric disorders does not seem high compared to the VTE prevalence in hospitalized patients with nonpsychiatric disorders.2–4 The prevalence of VTE has been reported at 0.5–58% in hospitalized non postsurgical patients with nonpsychiatric disorders,11–26 and at 4.8–24.4% in those without VTE symptoms.14,17,19,24 Given the recent increase in the number of people requiring hospitalization for VTE, clarifying the prevalence of VTE in hospitalized patients with psychiatric disorders such as depression is of academic as well as of clinical value.27
We, therefore, performed a retrospective cross-sectional study of depressed inpatients to examine the prevalence of VTE and factors associated with VTE in this specific patient subgroup.
Materials and Methods
Study Design
This retrospective study was approved by the Ethical Committee for Human Research of Akita University (no. 2243) and exempt from the requirement of informed consent, as it involved de-identified data acquired during routine care of patients.
This study aimed to determine VTE prevalence in depressed inpatients and to examine whether depression severity affects VTE prevalence.
Study Population and Setting
Consecutive inpatients diagnosed with major depressive disorder (MDD), bipolar I disorder, or bipolar II disorder manifesting in the depressive state were included, over a 1.5-year period between January 1, 2018, and June 30, 2019, at the psychiatric department of Akita University Hospital. Patients were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5). The psychiatric department of Akita University Hospital is an acute psychiatric unit with 36 beds. In 2018, the average length of stay at the department was 31 days. Our hospital recommends diagnosing VTE with contrast-enhanced CT, based on the clinician’s judgment of harm and benefit, if there are no contra-indications for contrast agents, because very few doctors and technicians are in charge of ultrasonography.
Interventions
From January 1, 2018, in line with current clinical practice at our hospital, depressed inpatients were initially screened for VTE using NANOPIA® D-dimer, instead of risk assessment scores, within days of hospitalization. In cases of abnormal NANOPIA® D-dimer values (1 µg/mL or more), enhanced CT was performed to reach a diagnosis within 12 hrs after measuring D-dimer concentrations, if the patient did not meet the exclusion criteria for contrast CT described below.
Diagnosing System
D-Dimer
D-dimer plasma concentrations were measured with the commercially available NANOPIA® latex agglutination assay kit (Sekisui Medical Company Limited, Tokyo, Japan), based on the same method commonly used for D-dimer assays such as the STA-Liatest D-dimer (Diagnostica Stago, Asnières, France) that contains latex microparticles coated with a monoclonal antibody specific for fragment DD, in combination with an automated coagulation analyzer, the COAPRESTA 2000 (Sekisui Medical Co., Ltd., Tokyo, Japan).28,29 Concentrations were expressed in micrograms per milliliter (μg/mL), with a D-dimer level ≥1.0 μg/mL representing a positive result. With a cut-off value of 1 μg/mL, the sensitivity of NANOPIA D-dimer in diagnosing VTE was 99.6%.28
Computed Tomography
VTE (PE or DVT) was detected using multidetector-row helical CT scanning on two different devices (Discovery CT750HD and Discovery CT750HD-A; GE Healthcare Japan, Tokyo, Japan), with a slice thickness of 1.25 mm, at 20 s (early phase) for detecting pulmonary arterial embolization and at 210 s (delayed phase) for detecting DVT. Low-osmolar iodinated contrast medium (Omnipaque 300; Daiichi Sankyo Company Limited, Tokyo, Japan) was intravenously injected at a rate of 4.0 mL/s using a power injector, up to a total amount of body weight (kg) × 2 + 30 (mL) or a maximum of 150 mL. This contrast agent is contraindicated for patients with (1) iodine or iodine contrast agent sensitivity; (2) severe thyroid disease; (3) bronchial asthma; (4) severe renal dysfunction; (5) severe liver dysfunction; (6) severe heart failure; (7) macroglobulinemia; (8) multiple myeloma; (9) tetany; (10) or pheochromocytoma. Written informed consent was obtained before the patient underwent contrast CT. Diagnostic radiology specialists of the Japan Radiological Society or doctors with more than a decade’s experience in radiological diagnosis analyzed the CT scans. The physicians assessing the CT scans were not blinded to the D-dimer results.
Additional Characteristics Gathered
The following data were extracted from the patients’ medical records: age, sex, body mass index (BMI) (kg/m2), and diagnoses of psychiatric disorders (based on the DSM-5). The following psychiatric risk factors for VTE were also extracted: daily dosage of antidepressants, daily dosage of antipsychotics, catatonia (according to the DSM-5), occurrence of physical restraint, and the daily dosage of antidepressants/antipsychotics on the day when D-dimer concentrations were measured for the VTE screening. The daily dosage of antidepressants was converted to imipramine equivalents (IMPE),30 and the daily dosage of antipsychotics was converted to chlorpromazine equivalents (CPZE).30 Factors suspected by us to increase the risk of VTE in depressive inpatients were also extracted: severity of depression (total score on the 17-item Hamilton Depression Rating Scale [HAM-D17]) and duration of current depressive episode.
The following parameters known as nonpsychiatric risk factors for VTE were assessed according to previous studies: trauma within 4 weeks,31 surgery within 4 weeks,32 malignancy,31 hypertension,33 hyperlipidemia (HL),33 diabetes mellitus (DM),33 pregnancy,34 oral contraceptive use,35 and hormone replacement therapy.36 Last, the following data associated with VTE were extracted: past history of VTE, D-dimer value (µg/mL), type of VTE (DVT without PE, PE without DVT, DVT with PE), type of DVT (proximal or distal type), and symptomatic or asymptomatic VTE. Proximal/distal DVT was defined as a thrombus in the iliac, femoral, or popliteal veins that was at the distal aspect of the popliteal vein. Medications for VTE comprised the following: anticoagulants, graduated compression stockings (GCS), and intermittent pneumatic compression devices (IPC).
Data Analysis
The data were expressed as medians (25–75% percentile) for age, BMI, HAM-D17 scores, duration of current depressive episode, D-dimer, IMPE, and CPZE. To examine the differences between the VTE and non-VTE patient groups for binary variables, Fisher’s exact test was performed for sex, diagnosis of psychiatric disorder (major depressive disorder or bipolar disorder), past history of VTE, catatonia, physical restraint, anticoagulant, GCS, IPC, hypertension, HL, DM, infection, disseminated intravascular coagulation (DIC), trauma within 4 weeks, surgery within 4 weeks, and malignancy. To examine the differences between the VTE and non-VTE patient groups for continuous variables, the Mann–Whitney U-test was used for comparing age, BMI, total HAM-D17 scores, duration of current depressive episode (weeks), antidepressant dosage (IMPE) (mg/day), and antipsychotics dosage (CPZE) (mg/day). All explanatory variables with a two-sided p-value less than 0.05 were considered to indicate statistical significance; p-values were not adjusted for multiple testing. All statistical analyses were performed with IBM SPSS Statistics version 25.0 (IBM Corp., Chicago, IL, USA).
Results
The participant selection for this study is shown in Figure 1. Throughout the study period, 94 adult Japanese patients (female 65, age mean±SD: 62.4 ± 16.3) were hospitalized to undergo treatment for depression at Akita University Hospital. Of the 94 subjects, 89 were hospitalized from the community, three were transferred from other psychiatric hospitals, and two were transferred from other wards at the same hospital. No patient was assessed for VTE risk before D-dimer measurements. Almost all patients (n=92) underwent VTE screening, but two patients did not undergo the screening within 7 days of hospitalization. Twenty-six patients screened positive for VTE. No patient had any contraindications for iodinated contrast medium, and none was pregnant during the study period. Twenty-four patients then underwent enhanced CT, but two patients did not agree to the procedure. No patient wore GCS or IPC. Nine patients were using anticoagulants (two: prevention of VTE because of a history of VTE; seven: atrial fibrillation). Patients using oral contraceptives or undergoing hormone replacement therapy were not included. No patient had DIC or surgery within 4 weeks.
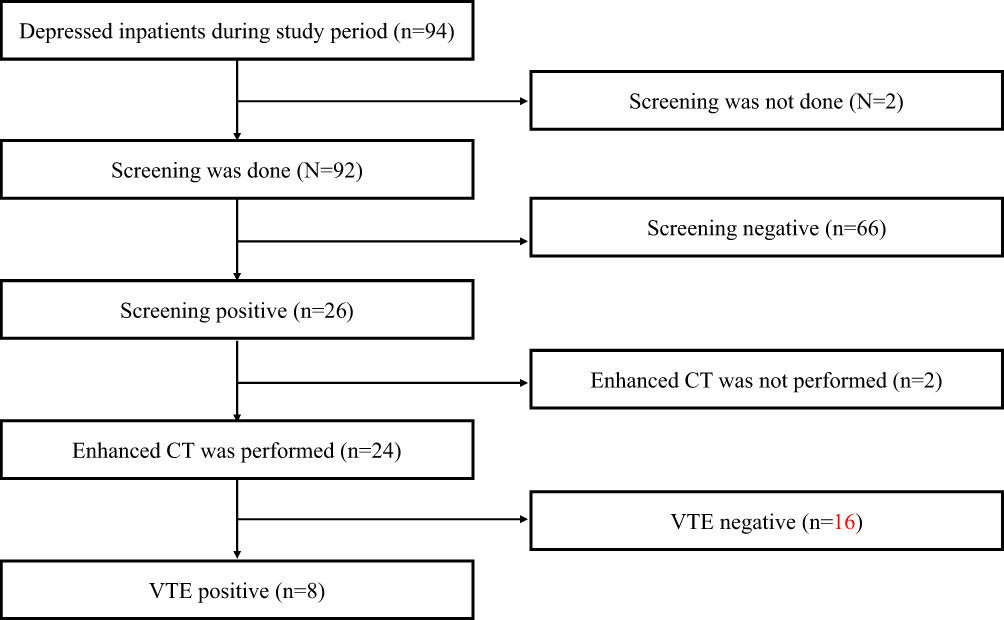 |
Figure 1 Participant selection. Notes: Throughout the study period, 94 Japanese patients were hospitalized to undergo treatment for depression at Akita University Hospital. Ninety-two patients underwent VTE screening, but two patients did not undergo the screening within 7 days of hospitalization. Twenty-six patients screened positive for VTE. Twenty-four patients then underwent enhanced CT, but two patients did not agree to the procedure. Eight patients were eventually diagnosed with VTE. Abbreviation: VTE, venous thromboembolism. |
Of all depressed inpatients, 8.5% (8/94) were diagnosed with VTE on enhanced CT (DVT only=3, PE only=4, co-occurrence of PE and DVT=1). All patients with DVT had distal DVT. The clinical characteristics of VTE-positive and VTE-negative patients are shown in Table 1. All patients were unrestrained. All patients diagnosed with VTE were asymptomatic. All patients with VTE improved on anticoagulant therapy without showing any side effects. In the patients who screened positive for VTE but refused to undergo contrast-enhanced CT, attention was paid to VTE risk factors such as dehydration, and they were discharged without developing symptomatic VTE.
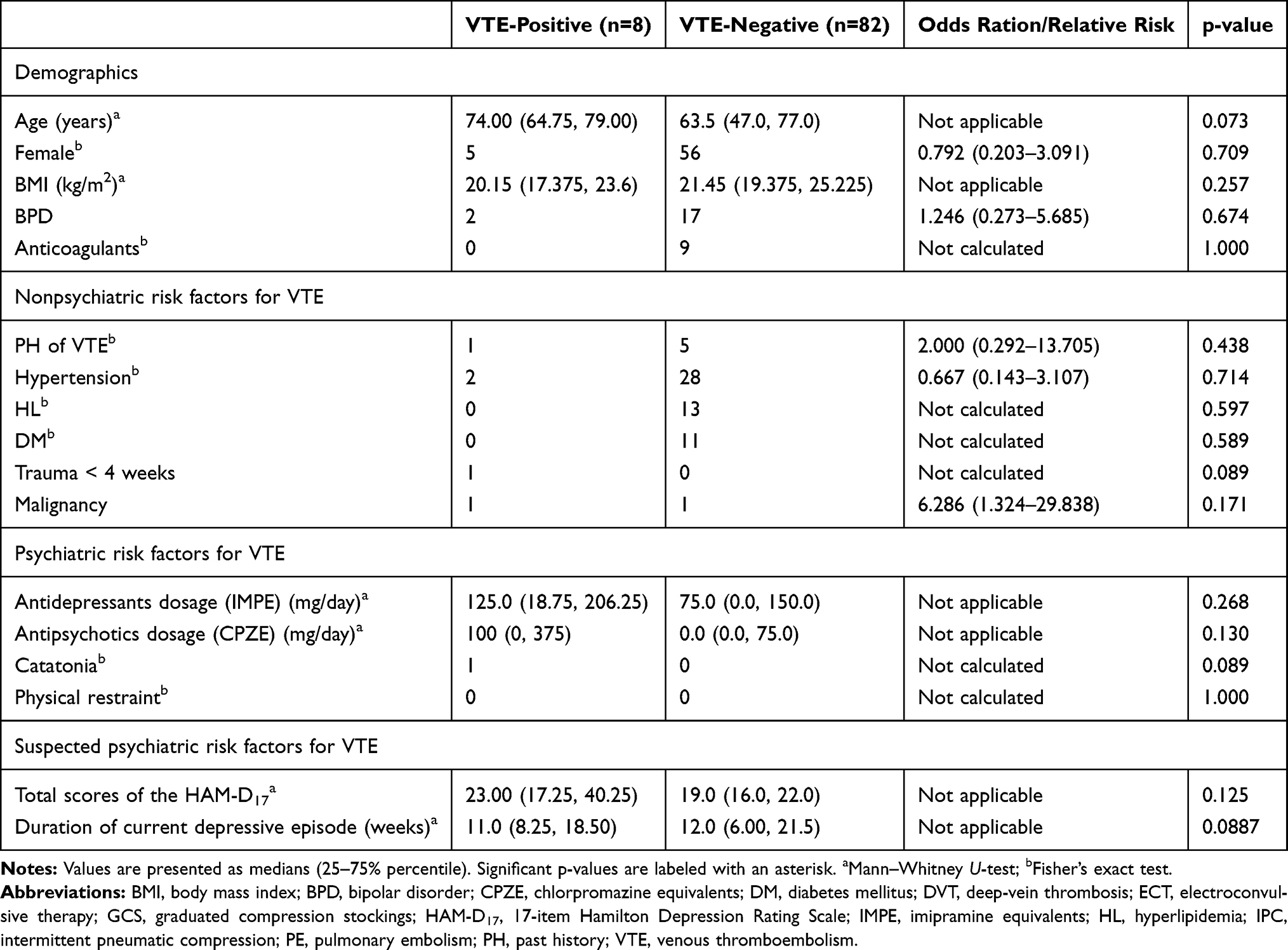 |
Table 1 Clinical and Demographic Characteristics of VTE-Positive and VTE-Negative Depressed Inpatients in This Study |
The univariate analysis showed no significant differences between VTE-positive and VTE-negative patients regarding any of the considered factors, that is, age, sex, BMI, diagnoses of psychiatric disorders (MDD or bipolar disorder), HAM-D17 scores, duration of current depressive episode, daily dosages of antidepressants and antipsychotics, catatonia, physical restraint, PH of VTE, anticoagulants, infection, hypertension, HL, DM, trauma, and malignancy.
Discussion
Our data show that 8.5% of depressed inpatients had VTE, less than the 11.6–25.3% observed in patients under restraint or with catatonia3,4 the but higher than the 2.3% reported in earlier studies in hospitalized patients with mental disorders.2 The study cannot definitely conclude that depressive inpatients have a generally higher risk of VTE than patients hospitalized with other mental disorders, because our study lacked a control group. However, depressed inpatients may have other risk factors for VTE such as dehydration, immobility, and the use of antidepressants, which may lead to a higher risk of VTE in this group compared to patients hospitalized for other psychiatric disorders. When patients are hospitalized in a depressed state, more attention should thus be paid to the potential occurrence and prevention of VTE. The prevalence of asymptomatic VTE was 8.5% in our study, about the same as that in inpatients with inflammatory bowel disease, which has been reported at 5.3%,22 and low compared to that in in-patients with advanced cancer or acute ischemic stroke, reported at 33.7% and 40.2%, respectively.13,16 Inpatients with depression may thus have a lower prevalence of asymptomatic VTE than patients hospitalized for physical illness.
This exploratory study did not reveal differences in the severity of depression or duration of the current depressive episode between VTE-positive and VTE-negative inpatients with depression. These results, although based on a small limited data set, thus suggest that it may be better to pay attention to the occurrence of VTE in all depressive inpatients, independently of these factors. Further large prospective studies are warranted to clarify unrevealed risk factors for VTE in depressive inpatients.
Previous studies pointed out the risk factors for VTE that are shown in Table 1. This study investigated differences in known risk factors for VTE between VTE-positive and VTE-negative inpatients with depression, but no significant differences were observed between the two groups. The previous studies were large-scale epidemiological studies and a meta-analysis, and the relatively low statistical power of our study may have led to these conflicting results.
All cases of VTE were asymptomatic in the current study, which is consistent with previous studies. In a previous study that examined VTE in patients hospitalized with psychiatric disorders using enhanced CT, similar to the current study, 97.4% of VTE cases were asymptomatic,2 while in earlier studies that examined DVT using ultrasonography, all DVT cases were asymptomatic.3,4 Studies that examined VTE in patients hospitalized at other departments reported 71.4–100% of cases to be asymptomatic.14,15,17,19-22,24,25 Asymptomatic VTE thus seems to be common in psychiatric as well as nonpsychiatric inpatients.
In this study, 62.5% of all patients with VTE had PE, which is similar to the 76.9% that a previous study reported.2 As PE cannot be detected by lower limb venous ultrasonography, enhanced CT must be conducted for a diagnosis. However, it is controversial whether enhanced CT should be performed in all cases that screen positive for VTE, because the prognosis of asymptomatic PE is unknown,37 and enhanced CT has potential risks such as anaphylaxis and renal failure.38 Therefore, clinicians must decide whether to perform enhanced CT to diagnose VTE, depending on the background and history of the individual patient.
Of all patients with VTE in the current study, 50% had DVT, which is similar to the 51.3% that a previous study reported.2 On the other hand, all of our patients with DVT had distal DVT, while only 55% of patients with DVT had distal DVT in the same previous study, which used contrast-enhanced CT for the diagnosis of VTE.2 It is unclear why the rates of distal DVT differ between these two studies, but we assume that the patients in the previous study may have had a higher risk of VTE than those in the current study. In our study, almost all depressive inpatients underwent VTE screening and enhanced CT, whereas in the earlier study, VTE screening was performed only in 25.6% of patients hospitalized for mental disorders, and contrast-enhanced CT was performed in 41.6% of patients who had screened positive for VTE. A selection bias in the earlier study may thus be the cause of the difference in distal DVT proportions.
As in a previous study, all VTE cases in this study improved on anticoagulant therapy without showing any side effects.2 VTE guidelines recommend anticoagulant therapy for PE and proximal DVT in principal, but not for distal DVT,39 because distal DVT has about half the risk of PE compared to proximal DVT, and because there is no further proximal extension if it does not occur within 2 weeks.40–42 The American College of Chest Physicians Evidence-Based Clinical Practice Guidelines recommend that distal DVT without severe symptoms or risk factors of proximal extension should not be treated with anticoagulant therapy immediately after diagnosis, but that the proximal extension should be monitored with ultrasound over 1–2 weeks.39 However, in hospitals where ultrasound cannot be performed in all necessary cases, there is no evidence for an advantage of either treating distal DVT immediately after the diagnosis or monitoring with enhanced CT to confirm the proximal extension.
To our knowledge, no study has examined the optimal D-dimer cutoff value for VTE screening in patients with psychiatric disorders. D-dimer is widely used for VTE screening, but is less useful for asymptomatic patients or hospitalized patients because of its low positive predictive value.43 Factors that may reduce the positive predictive value of D-dimer are advanced age, interfering comorbidities, or anticoagulant medication.44,45 Therefore, in order to enhance the usefulness of D-dimer in VTE screening, optimal and age-adjusted cutoff values for each medical department have been investigated.11,46-48 Since factors that affect D-dimer values are generally less likely in patients hospitalized for psychiatric disorders than in patients hospitalized for nonpsychiatric disorders, optimal cutoff values may be lower in the psychiatric field than in other fields; future studies are however warranted to address this question.
This study has some limitations. First, we included only 90 patients, and a lack of statistical power may have affected the results. Our analysis of risk factors for VTE was not adjusted, because of concerns about the reliability of a multivariable regression model due to the relatively small patient cohort and the limited number of VTE events in our population. Second, risk factors for VTE such as dehydration, immobility, drinking, and smoking could not be evaluated, due to the retrospective nature of the study. Third, physicians assessing the CT scans were not blinded to the D-dimer results, which may have led to a potential bias towards a diagnosis of VTE. Forth, as no study has so far examined the diagnostic accuracy of enhanced CT for DVT,49 asymptomatic DVT may have been underestimated in this study. Fifth, while the D-dimer cutoff value was set to 1.0 µg/mL in this study regardless of age, an age-adjusted cutoff may have been more optimal for older patients.46 Sixth, the clinical utility of D-dimer has primarily been validated in patients with symptoms of DVT and has a lower positive predictive value in asymptomatic or hospitalized patients. Seventh, Patients with a NANOPIA® D-dimer of less than 1 μg/mL may have VTE,28 and the prevalence of VTE in this study may, therefore, have been underestimated. Well-designed prospective studies including large samples are warranted to further investigate the prevalence of VTE in depressive inpatients and the potentially inter-correlated factors that might predict VTE.
Conclusion
We found a VTE prevalence in depressed inpatients of 8.5%, higher than the usually reported percentage for hospitalized patients with mental disorders, and our findings thus emphasize the importance of VTE screening for depressive inpatients.
Abbreviations
VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep-vein thrombosis; MDD, major depressive disorder; DSM-5, Statistical Manual of Mental Disorders-Fifth Edition; BMI, body mass index; IMPE, imipramine equivalents; CPZE, chlorpromazine equivalents; HAM-D17, 17-item Hamilton Depression Rating Scale; HL, hyperlipidemia; DM, diabetes mellitus; GCS, graduated compression stockings; IPC, intermittent pneumatic compression devices; DIC, disseminated intravascular coagulation.
Ethics Approval and Informed Consent
This study was approved by the Ethical Committee for Human Research of Akita University (no. 2243) and exempt from the requirement of informed consent, as it involved de-identified data acquired during routine care of patients.
Acknowledgments
We would like to thank Editage (www.editage.jp) for English language editing.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Akita University Support for Young Scientists program.
Disclosure
Masahiro Takeshima has received lecture fees from Daiichi Sankyo Company. The authors report no other conflicts of interest.
References
1. Manu P, Kane JM, Correll CU. Sudden deaths in psychiatric patients. J Clin Psychiatry. 2011;72(7):936–941. doi:10.4088/JCP.10m06244gry
2. Takeshima M, Ishikawa H, Shimizu K, Kanbayashi T, Shimizu T. Incidence of venous thromboembolism in psychiatric inpatients: a chart review. Neuropsychiatr Dis Treat. 2018;14:1363–1370. doi:10.2147/NDT
3. Ishida T, Sakurai H, Watanabe K, Iwashita S, Mimura M, Uchida H. Incidence of deep vein thrombosis in catatonic patients: a chart review. Psychiatry Res. 2016;241:61–65. doi:10.1016/j.psychres.2016.04.105
4. Ishida T, Katagiri T, Uchida H, et al. Incidence of deep vein thrombosis in restrained psychiatric patients. Psychosomatics. 2014;55(1):69–75. doi:10.1016/j.psym.2013.04.001
5. Wu CS, Chang CM, Chen CY, et al. Association between antidepressants and venous thromboembolism in Taiwan. J Clin Psychopharmacol. 2013;33(1):31–37. doi:10.1097/JCP.0b013e3182777425
6. Lee CW, Liao CH, Lin CL, Liang JA, Sung FC, Kao CH. Depression and risk of venous thromboembolism: a population-based retrospective cohort study. Psychosom Med. 2015;77(5):591–598. doi:10.1097/PSY.0000000000000193
7. Adelborg K, Sundbøll J, Videbech P, Grove EL. The risk of thromboembolism in users of antidepressants and antipsychotics. Adv Exp Med Biol. 2017;906:351–361.
8. Branchford BR. Venous thromboembolism risk with antidepressants: driven by disease or drugs? J Am Heart Assoc. 2017;6(5):e006293. doi:10.1161/JAHA.117.006293
9. Parkin L, Balkwill A, Sweetland S, et al. Antidepressants, depression, and venous thromboembolism risk: large prospective study of UK women. J Am Heart Assoc. 2017;6(5):e005316. doi:10.1161/JAHA.116.005316
10. Kunutsor SK, Seidu S, Khunti K. Depression, antidepressant use, and risk of venous thromboembolism: systematic review and meta-analysis of published observational evidence. Ann Med. 2018;50(6):529–537. doi:10.1080/07853890.2018.1500703
11. Kuwashiro T, Toyoda K, Oyama N, et al. High plasma D-dimer is a marker of deep vein thrombosis in acute stroke. J Stroke Cerebrovasc Dis. 2012;21(3):205–209. doi:10.1016/j.jstrokecerebrovasdis.2010.06.009
12. Pang H, Wang L, Liu J, et al. The prevalence and risk factors of venous thromboembolism in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. Clin Respir J. 2018;12(11):2573–2580. doi:10.1111/crj.2018.12.issue-11
13. White C, Noble SIR, Watson M, et al. Prevalence, symptom burden, and natural history of deep vein thrombosis in people with advanced cancer in specialist palliative care units (HIDDen): a prospective longitudinal observational study. Lancet Haematol. 2019;6(2):e79–e88. doi:10.1016/S2352-3026(18)30215-1
14. Inoue H, Watanabe H, Okami H, Kimura A, Takeshita K. The rate of venous thromboembolism before and after spine surgery as determined with indirect multidetector CT. JB JS Open Access. 2018;3(3):e0015. doi:10.2106/JBJS.OA.18.00015
15. Chua K, Kong KH, Chan SP. Prevalence and risk factors of asymptomatic lower extremity deep venous thrombosis in Asian neurorehabilitation admissions in Singapore. Arch Phys Med Rehabil. 2008;89(12):2316–2323. doi:10.1016/j.apmr.2008.05.025
16. Kelly J, Rudd A, Lewis RR, Coshall C, Moody A, Hunt BJ. Venous thromboembolism after acute ischemic stroke: a prospective study using magnetic resonance direct thrombus imaging. Stroke. 2004;35(10):2320–2325. doi:10.1161/01.STR.0000140741.13279.4f
17. Cronin CG, Lohan DG, Keane M, Roche C, Murphy JM. Prevalence and significance of asymptomatic venous thromboembolic disease found on oncologic staging CT. AJR Am J Roentgenol. 2007;189(1):162–170. doi:10.2214/AJR.07.2067
18. Ota S, Yamada N, Tsuji A, Ishikura K, Nakamura M, Ito M. Incidence and clinical predictors of deep vein thrombosis in patients hospitalized with heart failure in Japan. Circ J. 2009;73(8):1513–1517. doi:10.1253/circj.CJ-08-0990
19. Kawase K, Okazaki S, Toyoda K, et al. Sex difference in the prevalence of deep-vein thrombosis in Japanese patients with acute intracerebral hemorrhage. Cerebrovasc Dis. 2009;27(4):313–319. doi:10.1159/000202006
20. Sonoda K, Ikeda S, Mizuta Y, Miyahara Y, Kohno S. Evaluation of venous thromboembolism and coagulation-fibrinolysis markers in Japanese patients with inflammatory bowel disease. J Gastroenterol. 2004;39(10):948–954. doi:10.1007/s00535-004-1426-6
21. Ando K, Fujiya M, Nomura Y, et al. The incidence and risk factors of venous thromboembolism in patients with inflammatory bowel disease: a prospective multicenter cohort study. Digestion. 2019;100(4):229–237. doi:10.1159/000495289
22. Ando K, Fujiya M, Nomura Y, et al. The incidence and risk factors of venous thromboembolism in Japanese inpatients with inflammatory bowel disease: a retrospective cohort study. Intest Res. 2018;16(3):416–425. doi:10.5217/ir.2018.16.3.416
23. Gregory PC, Kuhlemeier KV. Prevalence of venous thromboembolism in acute hemorrhagic and thromboembolic stroke. Am J Phys Med Rehabil. 2003;82(5):364–369. doi:10.1097/01.PHM.0000064725.62897.A5
24. Schultz DJ, Brasel KJ, Washington L, et al. Incidence of asymptomatic pulmonary embolism in moderately to severely injured trauma patients. J Trauma. 2004;56(4):
25. Geerts WH, Code KI, Jay RM, Chen E, Szalai JP. A prospective study of venous thromboembolism after major trauma. N Engl J Med. 1994;331(24):1601–1606. doi:10.1056/NEJM199412153312401
26. Weng MT, Park SH, Matsuoka K, et al. Incidence and risk factor analysis of thromboembolic events in East Asian patients with inflammatory bowel disease, a multinational collaborative study. Inflamm Bowel Dis. 2018;24(8):1791–1800. doi:10.1093/ibd/izy058
27. Münster AM, Rasmussen TB, Falstie-Jensen AM, et al. A changing landscape: temporal trends in incidence and characteristics of patients hospitalized with venous thromboembolism 2006–2015. Thromb Res. 2019;176:46–53. doi:10.1016/j.thromres.2019.02.009
28. Yamaki T, Nozaki M, Sakurai H, et al. Combined use of pretest clinical probability score and latex agglutination D-dimer testing for excluding acute deep vein thrombosis. J Vasc Surg. 2009;50(5):1099–1105. doi:10.1016/j.jvs.2009.06.059
29. Waser G, Kathriner S, Wuillemin WA. Performance of the automated and rapid STA Liatest D-dimer on the STA-R analyzer. Thromb Res. 2005;116(2):165–170. doi:10.1016/j.thromres.2004.12.003
30. Inada T, Inagaki A. Psychotropic dose equivalence in Japan. Psychiatry Clin Neurosci. 2015;69(8):440–447. doi:10.1111/pcn.2015.69.issue-8
31. Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162(11):1245–1248. doi:10.1001/archinte.162.11.1245
32. Sugimura K, Sakuma M, Shirato K. Potential risk factors and incidence of pulmonary thromboembolism in Japan: results from an overview of mailed questionnaires and matched case-control study. Circ J. 2006;70(5):542–547. doi:10.1253/circj.70.542
33. Mahmoodi BK, Cushman M, Anne Næss I, et al. Association of traditional cardiovascular risk factors with venous thromboembolism: an individual participant data meta-analysis of prospective studies. Circulation. 2017;135(1):7–16. doi:10.1161/CIRCULATIONAHA.116.024507
34. Greer IA. Thrombosis in pregnancy: maternal and fetal issues. Lancet. 1999;353(9160):1258–1265. doi:10.1016/S0140-6736(98)10265-9
35. Baratloo A, Safari S, Rouhipour A, et al. The risk of venous thromboembolism with different generation of oral contraceptives; a systematic review and meta-analysis. Emerg (Tehran). 2014;2(1):1–11.
36. Rovinski D, Ramos RB, Fighera TM, Casanova GK, Spritzer PM. Risk of venous thromboembolism events in postmenopausal women using oral versus non-oral hormone therapy: a systematic review and meta-analysis. Thromb Res. 2018;168:83–95. doi:10.1016/j.thromres.2018.06.014
37. Sun JM, Kim TS, Lee J, et al. Unsuspected pulmonary emboli in lung cancer patients: the impact on survival and the significance of anticoagulation therapy. Lung Cancer. 2010;69(3):330–336. doi:10.1016/j.lungcan.2009.11.015
38. Maurer M, Heine O, Wolf M, Freyhardt P, Schnapauff D, Hamm B. Safety and tolerability of iobitridol in general and in patients with risk factors: results in more than 160000 patients. Eur J Radiol. 2011;80(2):357–362. doi:10.1016/j.ejrad.2010.03.018
39. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e419S–e496S. doi:10.1378/chest.11-2301
40. Lagerstedt CI, Olsson CG, Fagher BO, Oqvist BW, Albrechtsson U. Need for long-term anticoagulant treatment in symptomatic calf-vein thrombosis. Lancet. 1985;2(8454):515–518. doi:10.1016/S0140-6736(85)90459-3
41. Kakkar VV, Howe CT, Flanc C, Clarke MB. Natural history of postoperative deep-vein thrombosis. Lancet. 1969;2(7614):230–232. doi:10.1016/S0140-6736(69)90002-6
42. Huisman MV, Buller HR, Ten Cate JW, Vreeken J. Serial impedance plethysmography for suspected deep venous thrombosis in outpatients. The Amsterdam General Practitioner Study. N Engl J Med. 1986;314(13):823–828. doi:10.1056/NEJM198603273141305
43. Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006;295(2):199–207. doi:10.1001/jama.295.2.199
44. Hunt BJ. Plasma D-dimer assays in the diagnosis of venous thromboembolism in cancer patients. J Thromb Haemost. 2006;4(1):50–51. doi:10.1111/jth.2006.4.issue-1
45. Fuji T, Fujita S, Tachibana S, Kawai Y. A dose-ranging study evaluating the oral factor Xa inhibitor edoxaban for the prevention of venous thromboembolism in patients undergoing total knee arthroplasty. J Thromb Haemost. 2010;8(11):2458–2468. doi:10.1111/j.1538-7836.2010.04021.x
46. Konstantinides SV, Meyer G. The 2019 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2019;40(42):3453–3455. doi:10.1093/eurheartj/ehz726
47. Watanabe H, Madoiwa S, Sekiya H, et al. Predictive blood coagulation markers for early diagnosis of venous thromboembolism after total knee joint replacement. Thromb Res. 2011;128(6):e137–e143. doi:10.1016/j.thromres.2011.07.030
48. Kim JY, Kim KH, Cho JY, et al. D-dimer/troponin ratio in the differential diagnosis of acute pulmonary embolism from non-ST elevation myocardial infarction. Korean J Intern Med. 2019;34(6):1263–1271. doi:10.3904/kjim.2018.153
49. Katz DS, Loud PA, Bruce D, et al. Combined CT venography and pulmonary angiography: a comprehensive review. Radiographics. 2002;22(suppl_1):
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.