")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Prevalence of Asymptomatic Bacteriuria, Associated Factors and Antimicrobial Susceptibility Profile of Bacteria Among Pregnant Women Attending Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Authors Wabe YA, Reda DY, Abreham ET , Gobene DB, Ali MM
Received 23 July 2020
Accepted for publication 14 September 2020
Published 29 September 2020 Volume 2020:16 Pages 923—932
DOI https://doi.org/10.2147/TCRM.S267101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Yasin Awol Wabe,1 Dawit Yihdego Reda,2 Estifanos Tsige Abreham,3 Degeuf Beyene Gobene,3 Musa Mohammed Ali2
1Werabe Comprehensive Specialized Hospital, Worabe, Ethiopia; 2Hawassa University, School of Medical Laboratory Science, Hawassa, Ethiopia; 3Ethiopian Public Health Institute, Addis Ababa, Ethiopia
Correspondence: Yasin Awol Wabe Email [email protected]
Introduction: Asymptomatic bacteriuria (ASB) is the presence of bacteria in significant quantity in the absence of signs and symptoms of urinary tract infection (UTI). ASB, if it occurs during pregnancy, can cause serious complications both among fetus and pregnant women.
Objective: The aim of this study was to determine the prevalence of ASB, its associated factors, and antimicrobial susceptibility profile of bacterial isolates among pregnant women.
Methods: A cross-sectional study was conducted from July to September 2019 among 290 pregnant women at Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Clean-catch midstream urine specimens were collected using sterile containers and cultured on MacConkey agar and sheep blood agar to isolate bacteria. Socio-demographic and obstetric data were collected using a structured questionnaire. Data were analyzed by SPSS version 22. The association between ASB and risk factors was assessed using logistic regressions. A p-value ≤ 0.05 was considered as a cut point to determine the significant association.
Results: From 290 study participants, 16.9% with 95 CI [13.1, 21.5] were positive for ASB. The predominant bacteria were Escherichia coli (43%) and Staphylococcus aureus (20%). Majority of E. coli (91.0%) were susceptible to nitrofurantoin and gentamycin; most of them were resistant to amoxicillin (86.4%) and cotrimoxazole (77.7%). The proportion of multi-drug resistance (MDR) isolates was 57.1%. Previous infection with UTI, previous history of catheterization, and natural abortion were significantly associated with ASB.
Conclusion: In the study area, ASB is prevalent in the study area indicating the importance of screening of ASB and possible treatment to prevent its consequences.
Keywords: asymptomatic bacteriuria, antibiotic susceptibility, pregnant woman, Addis Ababa, Ethiopia
Introduction
Urinary tract infection (UTI) is an infection of the urinary tract system; it can occur both in the community and hospital environment.1,2 Even though all age groups are affected by UTI, pregnant women,3–5 and immuno-compromised individuals6 are more susceptible. Generally, women are at greater risk of UTI as compared to males because of anatomical position and short urethra.6,7 If UTI occurs among pregnant women; it can be with symptoms or without symptoms. Urinary tract infection without signs and symptoms is known as asymptomatic bacteriuria (ASB).
Asymptomatic bacteriuria is the presence of a significant quantity of bacteria (≥105) in a urine specimen in the absence of signs and symptoms of UTI.8 Asymptomatic bacteriuria may progress to symptomatic UTI during pregnancy because of the following reasons: altered hormones, physiological changes, and reduced immunity.9 Other factors that could predispose pregnant women to bacteriuria are age, lower socioeconomic status, multiparty, past history of UTI, history of catheterization, aminoaciduria, anemia, and diabetes mellitus.10–12
In most cases, the leading cause of UTI is E. coli,13 while other Gram-negative bacteria such as Pseudomonas aeruginosa, Klebsiella pneumoniae, Proteus species, and some Gram-positive bacteria are also responsible.14 Significant numbers of pregnant women with ASB may develop acute upper UTI.15 Upper UTI can have a direct and indirect impact on the fetus.16,17
There are scarce data on the prevalence of ASB in Addis Ababa. The aim of this study was to determine the prevalence of ASB, its associated factors, and antimicrobial susceptibility profile of bacterial isolates among pregnant women attending Saint Paul’s Hospital Millennium Medical College (SPHMMC) Addis Ababa, Ethiopia.
Methods
Study Area
This study was conducted at SPHMMC which is located in Addis Ababa, the capital city of Ethiopia. The hospital provides health care services for about two million patients per year. Every month, about 830 pregnant women visit antenatal care unit of the hospital for follow-up.
Study Design and Study Population
A hospital-based cross-sectional study was conducted from July to September 2019. Pregnant women of all gestational age without signs and symptoms of UTI (such as dysuria, haematuria, fever, suprapubic pain, flank pain, the urgency of urination) were included in the study. Pregnant women with a history of antibiotics in the last 15 days and those with known congenital anomalies of the urinary tract system were excluded from the study.
Variables of the Study
Dependent Variables
Prevalence of ASB.
Independent Variables
Socio-demographic factors and other related factors such as the history of UTI, hemoglobin level, history of catheterization, educational status, monthly income, gestational age, history of natural abortion, parity, history of stillbirth, etc.
Sample Size Determination
The sample size was determined using a single population proportion formula, by considering the prevalence of UTI (21.2%) reported from Tigray Regional State, Ethiopia,4 95% confidence interval and a 5% margin of error. The total sample size after considering risk factors and 10% contingency was equal to 290.
Sampling Technique
To recruit study participants systematic random sampling technique was used by considering the three months of study period. According to the hospital plan and the past three months’ performance report, about 1518 pregnant women were expected to visit the antenatal care unit during the study period. This estimate was divided into the sample size (n=290) to determine the sampling interval (K value) which was five. The first study participant was selected by lottery method; then onward, every 5th pregnant women were invited to participate in the study until the required sample size was obtained.
Data Collection
Socio-demographic and factors that could predispose to ASB (history of UTI, hemoglobin level, history of catheterization, educational status, monthly income, gestational age, history of natural abortion, parity, history of stillbirth, etc.) were captured by using a structured questionnaire. Participants were instructed on how to collect clean-catch midstream urine. They were informed to clean their hands with water and soap then cleanse their periurethral area with a sterile cotton swab soaked in normal saline to reduce contamination. About 10–15 milliliter of clean-catch midstream urine was collected from all study participants using a wide-mouthed sterile container. Specimens were transported to the microbiology laboratory of Ethiopian Public Health Institute (EPHI) within 1–2 hours after collection. Uncentrifuged, well mixed, urine of 0.001 mL was inoculated onto MacConkey agar and 5% sheep blood agar by a calibrated wire loop and then incubated aerobically at 37°C overnight. Colony count per mL of the sample was multiplied by 1000 to get the total colony-forming unit (CFU) per mL of urine. A plate with 105 CFU/mL colony count or greater was considered as significant growth.18 Bacteria were identified by colony characteristics, Gram reaction, catalase test, coagulase test, and biochemical tests.19
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed using disk diffusion method on Mueller-Hinton agar (Oxoid Ltd, Hampshire, UK) according to Clinical and Laboratory Standards Institute (CLSI) guideline.20 Antimicrobials tested were comprised of ampicillin (10μg), amoxicillin (20μg), amoxicillin-clavulanic acid (20/10μg), ciprofloxacin (5μg), ceftriaxone (30μg), azithromycin (15μg) cefuroxime (30μg), nitrofurantoin (300μg), erythromycin (15μg), cotrimoxazole (25μg), tetracycline (30μg), clindamycin (2μg), gentamicin (10μg), penicillin (30μg), and meropenem (10μg).
Quality Control
To maintain the quality of socio-demographic and obstetric data, the questionnaire was pretested among pregnant women that represent 5% of the total sample size at Tikur Anbesa Specialized Hospital. Originally the questionnaire was prepared in English then it was translated to Amharic and finally translated back to English by different translators to check its consistency. The sterility of all culture media was checked by incubating 5% of them without inoculation at 37 OC. The performance of culture media was checked by using control strains such as E. coli (ATCC-25,922), S. aureus (ATCC-25,923), and P. aeruginosa (ATCC-27,853) throughout the study.
Operational Definitions
Asymptomatic Bacteriuria (ASB)
Bacterial colony count greater than or equal to 105 cfu/mL from urine sample collected from a person with no signs and symptoms of UTIs (such as dysuria, haematuria, fever, suprapubic pain, flank pain, the urgency of urination).21
Multidrug-Resistance (MDR)
Bacteria that show resistance to two or more classes of antimicrobial agents.22
Data Processing and Analysis
Data were cleaned, coded and entered using Epi Info Version 7.2 and analyzed by SPSS software version 22. Descriptive statistics was used to determine the prevalence of ASB, the proportion of bacteria, and AST profiles of bacteria. To determine factors associated with ASB bivariate and multivariable logistic regression were used. Variables with a p-value less than 0.25 in bivariate analysis were selected for further analysis by multivariable logistic regression. A p-value of less than 0.05 was taken as a cut point to determine significant association.
Results
Socio-Demographic Characteristics of Study Participants
In this study, a total of 290 pregnant women were included with a response rate of 100%. The mean age of the participants was 27± 4.5 years. Two hundred-eighty (96.6%) participants were married. Twenty percent of participants attended the College or University level of education. More than half of the study participants resided in an urban area (Table 1).
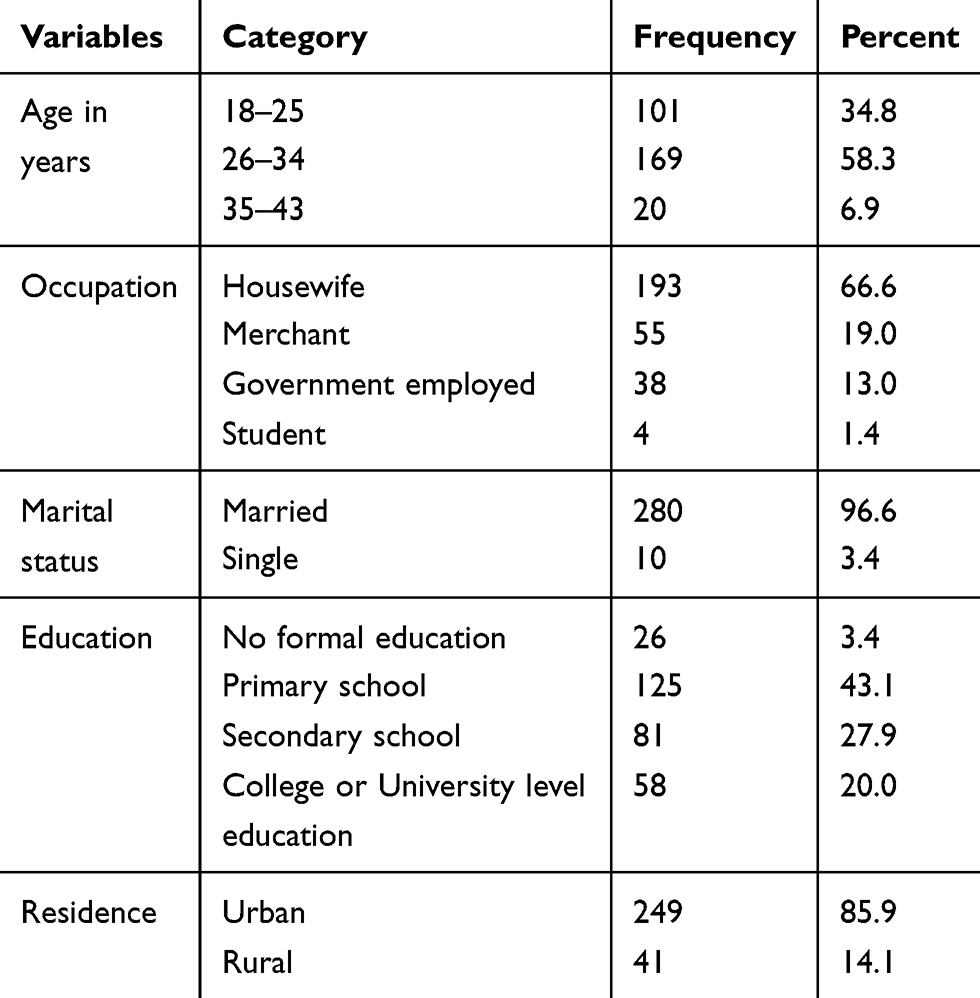 |
Table 1 Socio-Demographic Characteristics of Pregnant Women Attending the Antenatal Clinic of the Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2019 (N= 290) |
Prevalence of Asymptomatic Bacteriuria
Out of 290 pregnant women without signs and symptoms of UTI, 49 (16.9%) (95%, CI=13.1–21.5) had significant bacteriuria. Among participants with significant bacteriuria, 47 (95.9%) were positive for one bacteria while 2(4.1%) were positive for more than one organism. In this study, eight different types of bacteria were identified. Out of 49 bacteria isolated, 29 (59.2%) were Gram-negative bacteria and 20 (40.8%) were Gram-positive bacteria. The predominant bacteria were E. coli 21 (43%) and S. aureus 10 (20.4%) followed by S. saprophyticus 7(14.3%), K. Pneumoniae 3(6.1%), Enterobacter cloacae 2(4.1%), Enterococcus faecalis 2(4.1%), Klebsiella oxytoca 1(2.1%), and Enterobacter aerogens 1(2.1%). The two mixed cultures contained E. coli with Candida albicans and S. saprophyticus with C. albicans.
Factors Associated with Asymptomatic Bacteriuria
High prevalence of ASB was observed among participants within the age group of 26–34 years (17.8%), housewives (18.1%), urban residents (17.7%), married (17.1%), and with no formal education (23.1%). However, there was no significant association between ASB and socio-demographic characteristics (Table 2). In multivariable analysis, the prevalence of ASB was significantly associated with a history of UTI [AOR=3.11, 95% Cl: 1.42, 6.79], history catheterization [AOR=2.31, 95% Cl: 1.04, 5.73], anemia [AOR=10.49, 95% Cl: 4.54, 24.04], and history of natural abortion [AOR=2.36, 95% Cl: 1.13, 4.94] (Table 3).
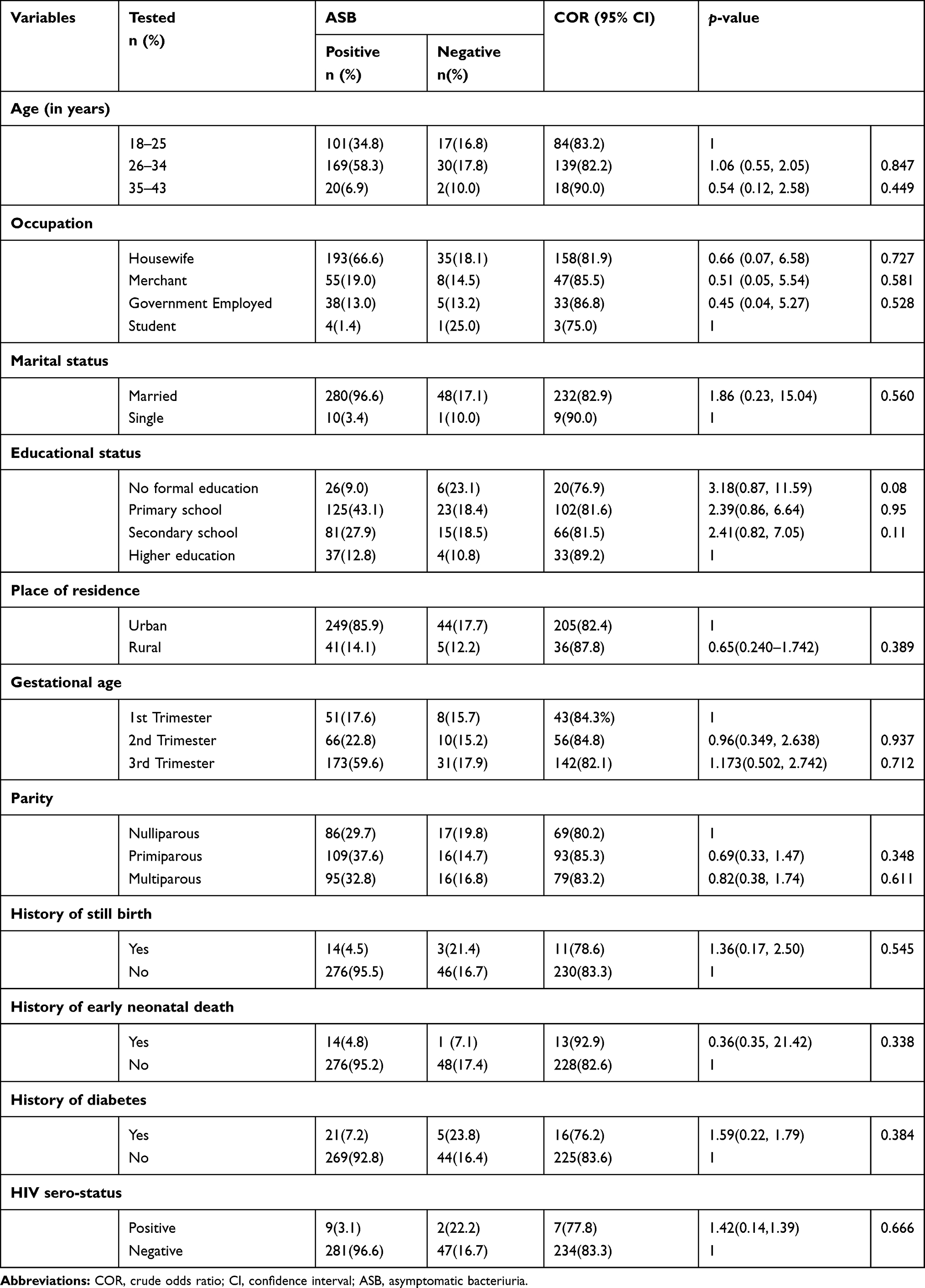 |
Table 2 ASB Across Different Socio-Demographic Characteristics Among Pregnant Women Attending Antenatal Clinic of the Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2019 (N=290) |
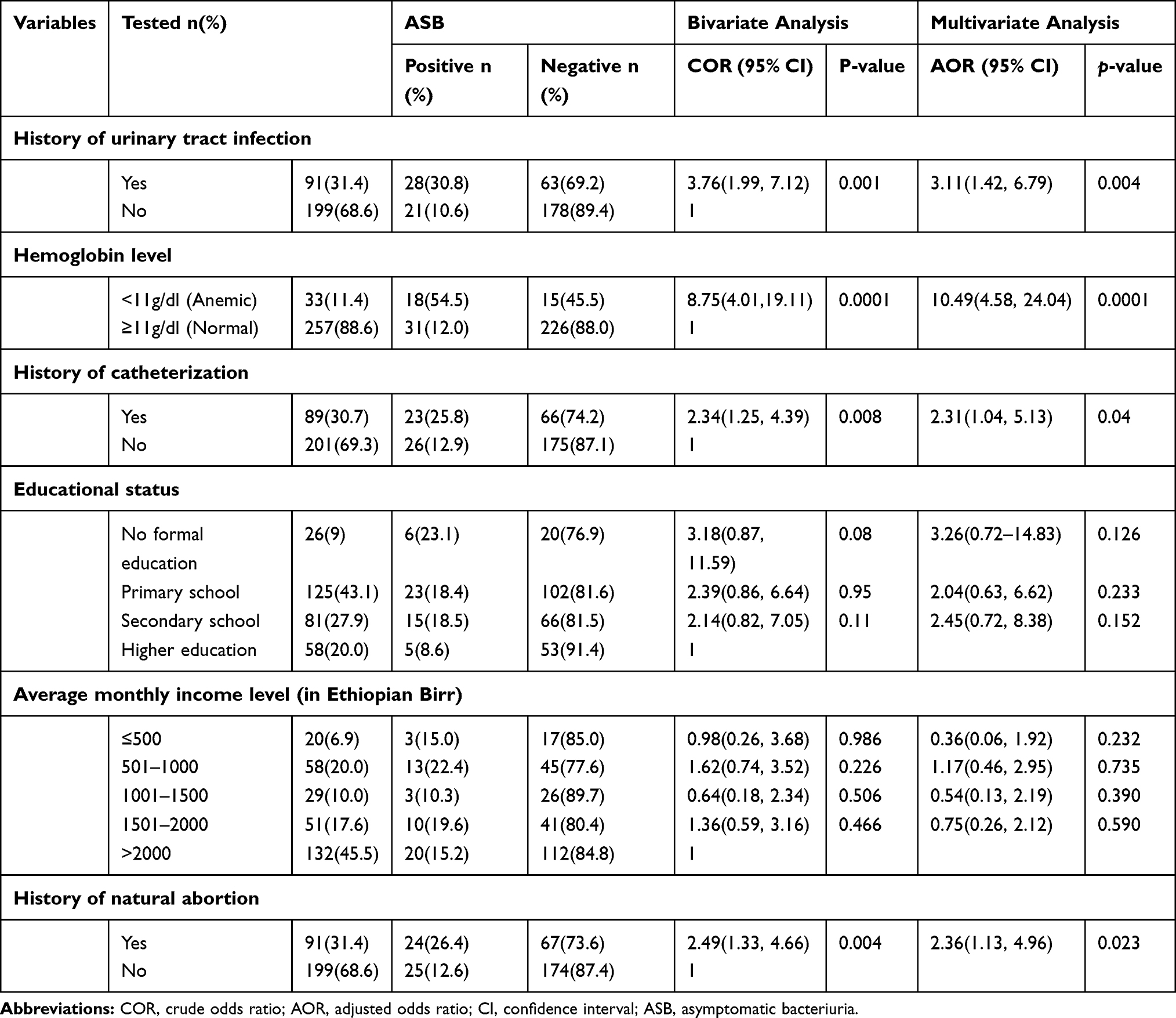 |
Table 3 Bivariate and Multivariable Analyses of Factors Associated with ASB Among Pregnant Women Attending the Antenatal Clinic of the Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2019 (N=290) |
Antimicrobial Susceptibility Profile of Bacteria
The antimicrobial susceptibility profile of Gram-negative bacteria (susceptible bacteria) falls within the range of 13.8%-93.1%. The majority of the Gram-negative bacteria were susceptible to nitrofurantoin (n=27; 93.1%), gentamycin (n=25; 86.2%), ceftriaxone (n=24; 82.8%), cefuroxime (n=23; 82.8%), and meropenem (n=22; 75.9%). Most Gram-negative bacteria were resistant to amoxicillin (n=23; 79.3%), cotrimoxazole (n=19; 65.5%), and amoxicillin-clavulanic acid (n=11; 37.9%). Most of E. coli (n=19; 86.4%) were resistant to amoxicillin (Table 4).
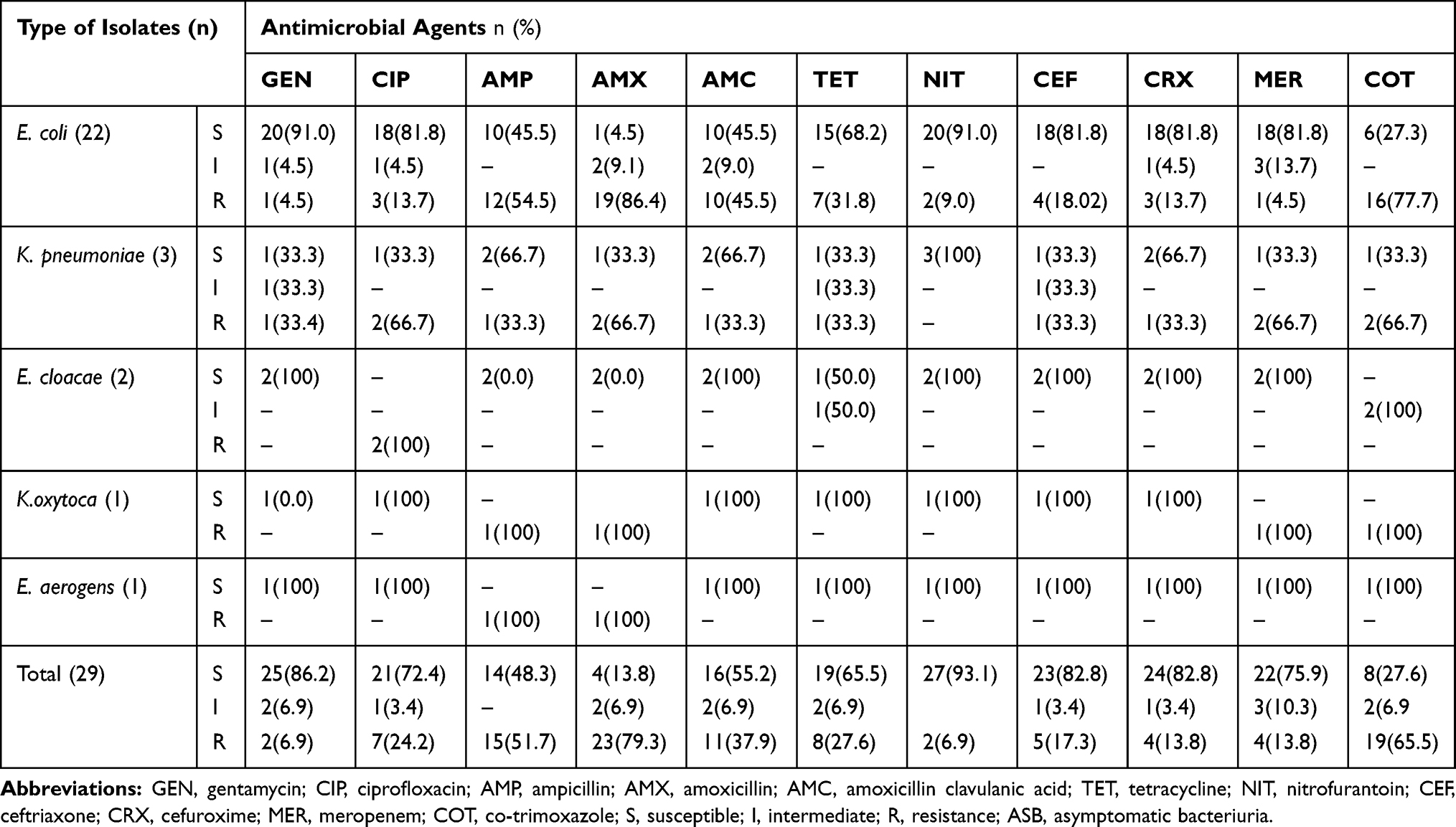 |
Table 4 Antimicrobial Susceptibility Profile of Gram-Negative Bacteria Isolated from Pregnant Women with ASB at Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2019 (n=29) |
All Gram-positive bacteria were susceptible to nitrofurantoin (n=20; 100%). Majority were susceptible to azithromycin (n=18; 90.0%), gentamicin, and ciprofloxacin (for each n=17; 85.0%) and clindamycin (n=16; 80.0%). Most of S. aureus were susceptible to gentamicin, ciprofloxacin, and azithromycin (n=9; 90.0%); however, 70% were resistant to penicillin. Seventy-five percent of S. saprophyticus were susceptible to gentamycin, ciprofloxacin, clindamycin, and azithromycin (Table 5). Out of 49 bacteria isolated in this study, 28 (57.1%) were MDR; 15 (51.7%) of this belongs to Gram-negative while 13 (65.0%) belongs to Gram-positive bacteria (Table 6).
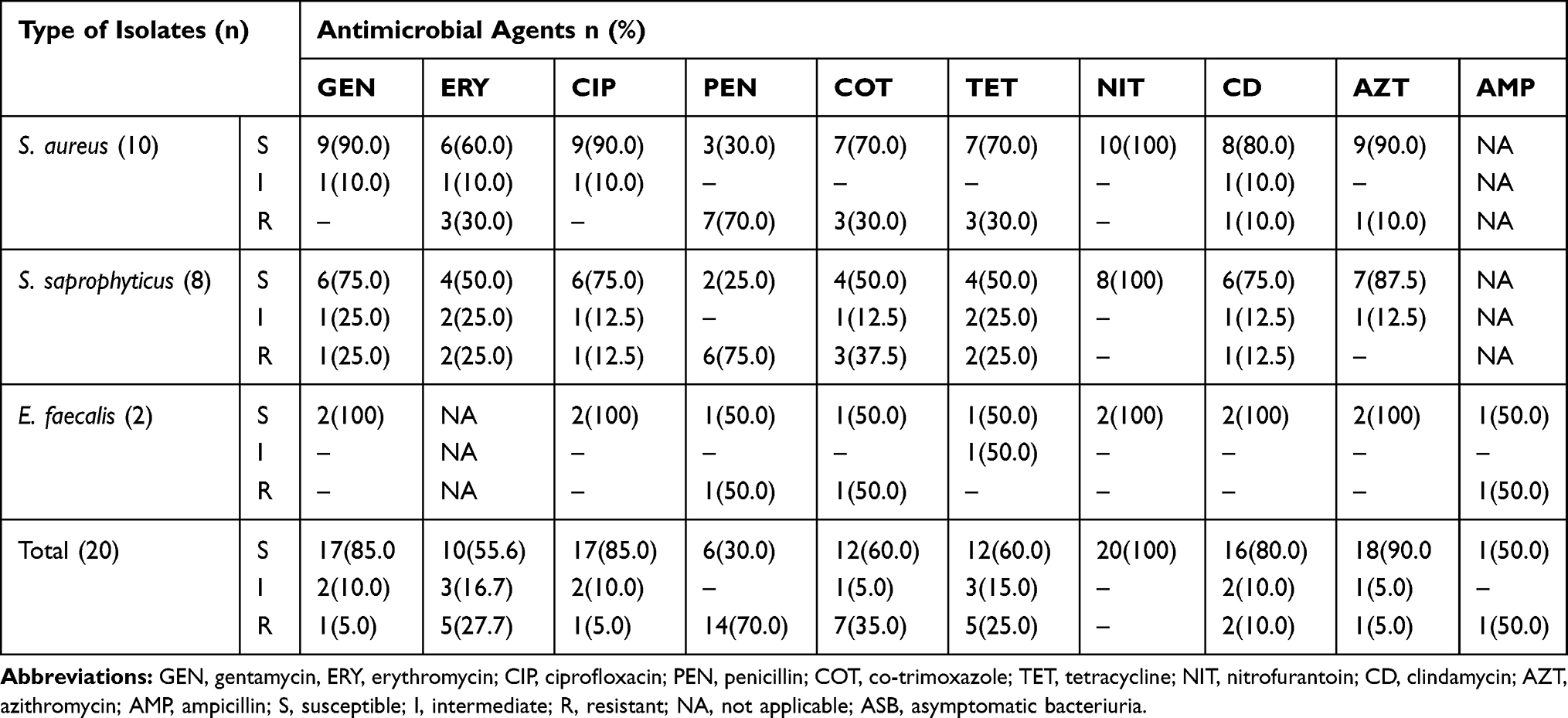 |
Table 5 Antimicrobial Susceptibility Profile of Gram-Positive Bacteria Isolated from Pregnant Women with ASB at Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2019 (n=20) |
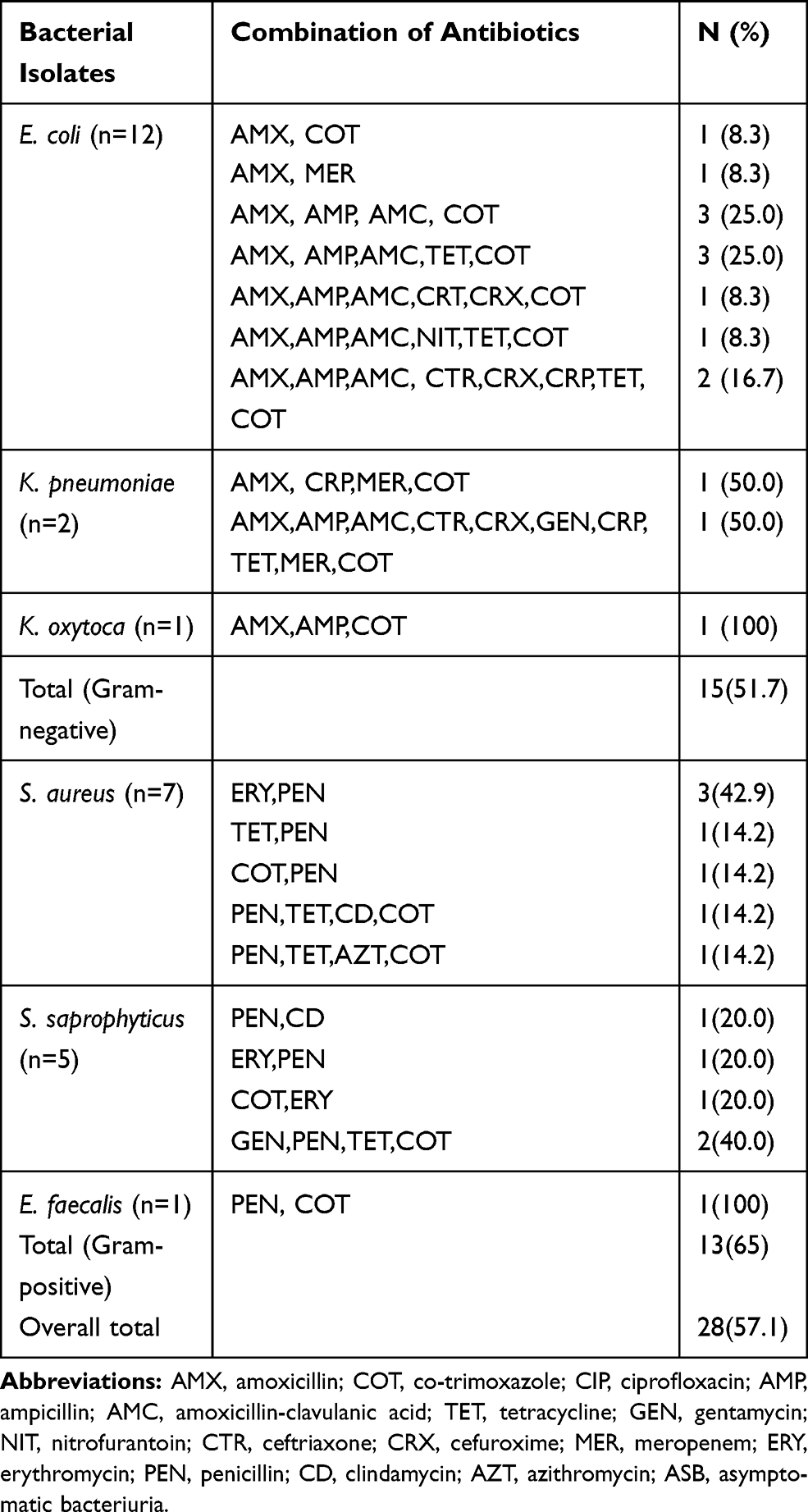 |
Table 6 Multi-Drug Resistance Profile of Bacteria Isolated from Pregnant Women with ASB at Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2019 (n=28) |
Discussion
The prevalence of ASB among pregnant women in the current study (16.9%) is in line with a study conducted in Bangladesh (16.5%)23 and Adama, Ethiopia (16.1%).24 However, it is low compared to the prevalence of ASB reported from Iraq (42.9%),25 Nigeria (37.1%),26 Saudi Arabia (32.1%),27 and Adigrat, Ethiopia (21.2%).4 In addition, the finding of the current study is higher than the prevalence of UTI reported from Nigeria (11%)28 and Bahir Dar, Ethiopia (11.5%).29 The variation could be attributed to social habits and education levels of the study participants.
The proportion of Gram-negative bacteria (59.2%) identified in the present study is higher than the proportion of Gram-positive bacteria (40.8%). This finding is in line with studies conducted in Gondar, Ethiopia,30 Tanzania,31 and Nigeria.26 E. coli was found to be the most prevalent (43%) bacteria isolated in this study. A similar finding was reported from Adama, Ethiopia (37.3%),24 Kenya (38.8%),32 and Tanzania (64.2%).33 This could be due to virulence factors harbored by the bacteria to colonize the urinary epithelium and difficultly of maintaining personal hygiene during pregnancy. The second predominant bacteria were S. aureus (20.4%) followed by S. saprophyticus (14.3%). This finding is comparable with the study conducted in Iraq (25.0%)25 and Kenya (29.7%).32 The proportion of S. saprophyticus (14.3%) in the current study is comparable with report from Adigrat, Ethiopia (12.7%).4 In contrast, a high proportion of S. saprophyticus was reported from Bahir Dar, Ethiopia (48.2%)29 and Nigeria (44.5%).3
In the current study, participants with the previous history of UTI had about 3 times chance of developing ASB (p=0.004). A similar finding was reported from Gondar, Ethiopia30 and Egypt.34 The possible explanation for this association could be due to the existence of antibiotic-resistant strains from the previous infection. The history of catheterization was also significantly associated with ASB (p=0.04). This is in line with a study conducted in Dessie, Ethiopia.5 The reason for this could be due to the introduction of bacteria to the sterile site during catheterization. Frequent and long-term catheterization could create a favorable environment for bacterial colonization and growth as a biofilm. Pregnant women with a history of natural abortion were 2.36 times more likely to develop ASB (p=0.023). The results of this study disagree with the finding reported from Cameron.35
Majority of Gram-negative bacteria isolated in the current study were susceptible to nitrofurantoin (93.1%), gentamicin (85.2%), ceftriaxone (82.2%), cefuroxime (79.3%), meropenem (75.2%), and ciprofloxacin (75.2%). This finding is comparable with a study conducted in Dessie, Ethiopia,5 Hawassa, Ethiopia,6 and Bale, Ethiopia.36 However, most Gram-negative bacteria were resistant to amoxicillin (79.3%), amoxicillin-clavulanic acid (37.9%). The easy accessibility, indiscriminate and frequent use of antibiotics might cause the emergence of bacteria which are resistant to amoxicillin and amoxicillin-clavulanic acid.
Most E. coli isolated in this study were susceptible to gentamicin, nitrofurantoin, ceftriaxone, ciprofloxacin, and cefuroxime. However, most E. coli were resistant to ampicillin, cotrimoxazole, and amoxicillin-clavulanic acid. The proportion of antibiotic-resistant E. coli found in this study is higher than the proportion antibiotic-resistant E. coli reported from other parts of Ethiopia29 but it is low compared to report from Kenya.32 Moreover, the finding of this study is not in line with a report from India, where 6170% of E. coli were susceptible to ampicillin and amoxicillin-clavulanic acid, respectively.37 These differences could be due to variations in antibiotic prescription patterns across various countries.
All K. pneumoniae isolated in this study were susceptible to nitrofurantoin and most of them were susceptible to ampicillin, amoxicillin-clavulanic acid, and cefuroxime. The finding is not comparable with finding reported from Tanzania.31 All K. oxytoca and E. aerogens were resistant to ampicillin and amoxicillin. The high resistance to ampicillin and amoxicillin observed in this study may be due to the easy availability of antibiotics in local pharmacies and frequent prescription of antibiotics by physicians without antimicrobial susceptibility testing.
In the current study, none of the Gram-positive bacteria were resistant to nitrofurantoin. This could be due to the infrequent use of the drug in the study area. Most S. aureus isolated in the current study were resistant to penicillin, erythromycin, and tetracycline. This finding is not in line with the report from Togo.38 In addition, all E. faecalis were susceptible to gentamicin and ciprofloxacin; however, half of them were resistant to ampicillin and penicillin. In contrast, according to a study conducted in Togo, all E. faecalis were resistant to ciprofloxacin.38 In our study, a significant number (57.1%) of bacteria were MDR which is lower than MDR reported from Jimma, Ethiopia (90%),39 Dire Dawa, Ethiopia (100%),30 and Nigeria (100%).40
Limitation of the Study
As participants may not remember all information asked during data collection, this study is prone to recall bias.
Conclusion
The prevalence of ASB among pregnant women in the present study was 16.9%. History of UTI, history of catheterization, and history of natural abortion were significantly associated with ASB. The most prevalent bacteria isolated in this study were E. coli (43.0%), S. aureus (20.4%), and S. saprophyticus (14.3%). The majority of bacteria isolated in the present study were susceptible to nitrofurantoin and gentamicin. The study also showed that most of the bacteria were MDR.
Abbreviations
ANC, antenatal care; ASB, asymptomatic bacteriuria; ATCC, American Type Culture Collection; CFU, colony-forming unit; MDR, multidrug-resistance; HIV, human immunodeficiency virus; SPHMMC, Saint Paul’s Hospital Millennium Medical College; UTI, urinary tract infection.
Data Sharing Statement
All relevant data generated and analyzed are available within the paper.
Ethical Approval and Consent to Participate
The study was approved by the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences (Ref No IRB/205/11) and Saint Paul’s Hospital Millennium Medical College (Ref No pm23/368). An official permission letter was obtained from the Saint Paul’s Hospital Millennium Medical College administration office. Participants enrolled in the study were informed about the study objectives, expected outcomes, benefits, and risks associated with it. Written informed consent was taken from all participants before the interview. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
We would like to thank Ethiopian Public Health Institutes Laboratory, Saint Paul’s Hospital Millennium Medical College for facilitating the study. We also acknowledge all study participants for their willingness to take part in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests.
References
1. Onanuga A, Maureen CO, Deboh ED. Carriage of multi-drug resistant urobacteria by asymptomatic pregnant women in yenagoa, bayelsa state, Nigeria. Afr J Infect Dis. 2018;12(2):14–20. doi:10.21010/ajid.v12i2.3
2. Radha S, Nambisan B, Prabhakaran NK, Jamal S. Prevalence and outcome of asymptomatic bacteriuria in early pregnancy. Int J Reproduction, Contraception, Obstet Gynecol. 2017;6(1):223–227. doi:10.18203/2320-1770.ijrcog20164663
3. Aminu KY, Aliyu UU Asymptomatic bacteriuria in pregnant women in the antenatal booking clinic at aminu kano teaching hospital, Kano, Nigeria. Open J Obstet Gynecol. 2015; 5:286–297. doi:10.4236/ojog.2015.55042
4. Tadesse S, Kahsay T, Adhanom G, et al. Prevalence, antimicrobial susceptibility profile and predictors of asymptomatic bacteriuria among pregnant women in Adigrat General Hospital, Northern Ethiopia. BMC Res Notes. 2018;11:740. doi:10.1186/s13104-018-3911-7
5. Ali IE, Gebrecherkos T, Gizachew M, Menberu MA. Asymptomatic bacteriuria and antimicrobial susceptibility pattern of the isolates among pregnant women attending Dessie referral hospital, Northeast Ethiopia. Turk J Urol. 2018;44(3):251–260. doi:10.5152/tud.2018.07741
6. Tessema NT, Ali MM, Zenebe MH. Bacterial associated urinary tract infection, risk factors, and drug susceptibility profile among adult people living with HIV at Hawassa University Comprehensive Specialized Hospital, Hawassa, Southern Ethiopia. Nature Scientific Rep. 2020;10:10790. doi:10.1038/s41598-020-67840-7
7. Al-Jendy AS, Al-Ofairi BA. Bacterial pathogens of patients with urinary tract infections and antibiotics susceptibility in Taiz Governorate–Yemen. Al-Mustansiriyah J Sci. 2019;30(1):43–51. doi:10.23851/mjs.v30i1.530
8. Labi AK, Yawson AE, Ganyaglo GY, Newman MJ. Prevalence and associated risk factors of asymptomatic bacteriuria in ante-natal clients in a large teaching hospital in ghana. Ghana Med J. 2015;49(3):154–158. doi:10.4314/gmj.v49i3.5
9. Tadesse E, Teshome M, Merid Y, Kibret B, Shimelis T. Asymptomatic urinary tract infection among pregnant women attending the antenatal clinic of hawassa referral hospital, Southern Ethiopia. BMC Res Notes. 2014;7(155):1–5.
10. Elzayat MA, Ashton BV, Dabour ME, Cheng F. Prevalence of undiagnosed asymptomatic bacteriuria and associated risk factors during pregnancy: a cross-sectional study at two tertiary centres in Cairo, Egypt. BMJ Open. 2017;17(3):e013198.
11. Manjula R, Kavya H, Kashinakunti SV, Solabannavar S, Dorle AS, Lalitha HD. Diagnostic accuracy of griess test for asymptomatic bacteriuria in pregnancy. Br J Med Med Res. 2016;11(8):1–7. doi:10.9734/BJMMR/2016/20754
12. Paari P, Sindhuja TP, Dhinakaran S, Paul CM P. A cross-sectional study on asymptomatic bacteriuria among antenatal women attending an urban tertiary health care center in Southern India. Int J Reprod Contracept Obstet Gynecol. 2017;6(10):4523. doi:10.18203/2320-1770.ijrcog20174435
13. Pantagada N, Kamala P, Asymptomatic bacteriuria among pregnant women attending a tertiary care Hospital. Int J Current Microbiol Applied Sci. 2017;6(3):523–529. doi:10.20546/ijcmas.2017.603.061
14. Ramalingam K, Surasani VM, Bollu M. Prevalence of asymptomatic bacteriuria in antenatal women coming to NRIMC&GH. Bangladesh J Obstet Gynaecol. 2015;30(1):30–36. doi:10.3329/bjog.v30i1.30505
15. Laily F, Lutan D, Amelia S, Tala MRZ, Nasution A T. Associated risk factors for urinary tract infection among pregnant women at Puskesmas Kenangan, Deli Serdang district. IOP Conf Series: Earth Environmental Sci. 2018;125:012035. doi:10.1088/1755-1315/125/1/012035
16. Negussie A, Worku G, Beyene E. Bacterial identification and drug susceptibility pattern of urinary tract infection in pregnant Women at Karamara Hospital Jigjiga, Eastern Ethiopia. Afr J Bacteriol Res. 2018;10(2):15–22. doi:10.5897/JBR2017.0255
17. Ankur G, Namita S, Sapna G, et al. Prevalence of asymptomatic urinary tract infections in the three trimesters of pregnancy. Int J Curr Microbiol App Sci. 2015;(1):110–117.
18. Onyenweaku FC, Amah HC, Obeagu EI, Nwandikor UU, Onwuasoanya UF. Prevalence of asymptomatic bacteriuria and its antibiotic susceptibility pattern in pregnant women attending private ante natal clinics in Umuahia Metropolitan. Int J Curr Res Biol Med. 2017;2(2):13–23. doi:10.22192/ijcrbm.2017.02.02.00
19. Cheesbrough M. District Laboratory Practice in Tropical Countries, Part 2. New York: Cambridge University Press; 2006.
20. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
21. Kamel HA, Hegab MH, Al-sehrawey AA, Hassan HM. Prevalence of asymptomatic bacteriuria in patients with preterm labor. Egyptian J Hospital Med. 2018;73(9):7444–7447. doi:10.12816/EJHM.2018.18699
22. Marami D, Balakrishnan S, Seyoum B. Prevalence, antimicrobial susceptibility pattern of bacterial isolates, and associated factors of urinary tract infections among HIV-positive patients at Hiwot Fana Specialized University Hospital, Eastern Ethiopia. Canadian J Infectious Diseases Med Microbiol. 2019;2019:1–8. doi:10.1155/2019/6780354
23. Khanum S, Ahmed JU, Khanam. Bacterial etiology, antibiotic sensitivity pattern and risk factors for asymptomatic bacteriuria during pregnancy: experience in a tertiary care Hospital. BIRDEM Med J. 2016;6(2):79–83. doi:10.3329/birdem.v6i2.31289
24. Nisha AK, Etana AE, Tesso H. Prevalence of asymptomatic bacteriuria during pregnancy in Adama city, Ethiopia. Int J Microbiol Immunol Res. 2015l;3(5):058–63.
25. Bayati AH, Ghaib AH, Nasraldeen N, Hamalaw SA, Zainab AH. Asymptomatic bacteriuria among pregnant women in sulaimani city. GJBB. 2016;5(3):327–330.
26. Tosin OA, Mathew AO, Bello FJ, Oludare IO, Dolapo AL, Abosede AF. Asymptomatic bacteriuria among antenatal women attending private hospital in lagos, Nigeria. Sch J App Med Sci. 2014;2(6D):3076–3080.
27. Abderrazzack AF, Aguid MN, Hig-Zounet BT, Tidjani A, Ameyapoh Y. Asymptomatic microbial urinary tract infection in HIV positive pregnant women in Ndjamena (Chad). Int J Innovations Biol Chem Sci. 2015;6:1–7.
28. Chukwu OS, Ezeonu IM, Victor MA, et al. Incidence, aetiology and antibiotic susceptibility profile of asymptomatic bacteriuria in pregnant women in Nsukka Urban, Enugu state, Nigeria. World J Life Sci Med Res. 2014;3(3):94.
29. Derbie A, Mekonnen D, Abate E, Tadesse S, Birku T, Biadglegne F. Bacterial isolates and their current drug susceptibility profile from urine among asymptomatic pregnant women attending at a referral hospital, northwest ethiopia. Ethiopian J Reproductive Health. 2018;10(2):1–10.
30. Alemu A, Moges F, Shiferaw Y, et al. Bacterial profile and drug susceptibility pattern of urinary tract infection in pregnant women at University of Gondar Teaching Hospital, Northwest Ethiopia. BMC Res Notes. 2012;5(197):1–7.
31. Mwei MK, Mchome B, John B, Maro B. Asymptomatic bacteriuria among pregnant women attending antenatal clinic at kilimanjaro christian medical centre in Northern Tanzania. Clin Pract. 2018;15(6):917–922.
32. Ayoyi AO, Kikuvi G, Bii C, Kariuki S. Prevalence, aetiology and antibiotic sensitivity profile of asymptomatic bacteriuria isolates from pregnant women in selected antenatal clinic from Nairobi, Kenya. Pan Afr Med J. 2017;26:1–12. doi:10.11604/pamj.2017.26.41.10975
33. Mwambete KD, Msigwa M. Prevalence of asymptomatic urinary tract infections among pregnant women residing in a rural and an urban area in Tanzania. East Central African J Pharm Sci. 2017;20(13):27–32.
34. Mohamed NR, Omar H, Abd-Allah IM. Prevalence and risk factors of urinary tract infection among pregnant women in Ismailia City, Egypt. IOSR J Nursing Health Sci. 2017;19592320. doi:10.9790/1959-0603076272
35. Nguefack CT, Ebongue CO, Chokotheu CN, Ewougo CE, Njamen TN. Clinical presentation, risk factors and pathogens involved in bacteriuria of pregnant women attending antenatal clinic of 3 hospitals in a developing country: a cross sectional analytic study. BMC Pregnancy Childbirth. 2019;19(143):1–6.
36. Taye S, Getachew M, Desalegn Z, Biratu A, Mubashir K, Bacterial profile, antibiotic susceptibility pattern and associated factors among pregnant women with urinary tract infection in Goba and Sinana Woredas, Bale Zone, Southeast Ethiopia. BMC Res Notes. 2018;11(799):799. doi:10.1186/s13104-018-3910-8
37. Sujatha R, Nawani M. Prevalence of asymptomatic bacteriuria and its antibacterial susceptibility pattern among pregnant women attending the antenatal clinic at Kanpur, India. J Clin Diagnostic Res. 2014;8(4):C01C03. doi:10.7860/JCDR/2014/6599.4205
38. Foudaa AA, Seglab TD, Mounerouc S, et al. Sensibility of uropathogens in pregnant women with asymptomatic bacteriuria in Lome, Togo. Scientific J Biol Sci. 2015;4(4):30–35. doi:10.14196/sjbs.v4i4.1866
39. Gizachew Z, Kassa T, Beyene G, Howe R, Yeshitila B. Multi-Drug resistant bacteria and associated factors among reproductive age women with significant bacteriuria. Ethiop Med J. 2019;1:31–43.
40. Akpan NG, Umoyen AJ, Luka TT, Onwuezobe IA, Antia UE, Okon AS. Asymptomatic uropathogenic bacteriuria among pregnant and non-pregnant women at St Luke’s Hospital Anua, Offot Ukwa District Uyo: A reassessment case-control approach. American J Lab Med. 2019;4(1):1–10. doi:10.11648/j.ajlm.20190401.11
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.