")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Prevalence of Anemia and Associated Factors Among Term Newborns in Nekemte Specialized Hospital, Western Ethiopia
Authors Dereje I , Etefa T , Gebremariam T, Getaye A, Tunta A , Gerbi A
Received 28 June 2021
Accepted for publication 27 August 2021
Published 17 September 2021 Volume 2021:14 Pages 2607—2615
DOI https://doi.org/10.2147/JMDH.S326962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ifa Dereje,1 Tesema Etefa,2 Teka Gebremariam,2 Asfaw Getaye,3 Abayneh Tunta,4 Asfaw Gerbi2
1Department of Medicine, College of Health Sciences, Salale University, Fiche, Oromia, Ethiopia; 2Human Anatomy Unit, Department of Biomedical Sciences, Faculty of Medical Science, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia; 3Department of Nursing, College of Health Science, Salale University, Fitche, Oromia, Ethiopia; 4Department of Biomedical Sciences, Faculty of Health Sciences, Woldia University, Woldia, Amhara, Ethiopia
Correspondence: Ifa Dereje Tel +251-915697574
Email [email protected]
Background: Anemia is a global public health problem that affects approximately one-third of the global population. Infants and children are the ones to develop both short-term and long-term devastating complications from anemia. Although anemia is a very big public health concern, newborns, especially in developing countries, are usually overlooked and undiagnosed.
Purpose: The aim of this study was to assess the prevalence of anemia and associated factors among term newborns in Nekemte Specialized Hospital, Western Ethiopia.
Methods: A facility-based cross-sectional study involving 278 newborns was conducted from October to November, 2020 with an interview-based questionnaire that included maternal socio-demographic and obstetrics characteristics, newborn’s weight and sex. The data were analyzed with SPSS version 20. The prevalence of newborn anemia was shown in percentage and as a pie-chart. Bivariate analysis and binary logistic regression were used to identify the predictors of anemia in the term newborn.
Results: The overall prevalence of newborn anemia in the hospital was 29.1%. Maternal anemia (AOR: 3.95, 95% C.I.: 1.97– 7.92), delivery by cesarean section (AOR: 4.17, 95% C.I.: 1.89– 9.20), vaginal bleeding during pregnancy (AOR: 5.43, 95% C.I.: 1.60– 18.39), and maternal failure to take iron-folate supplements during pregnancy (AOR: 2.17, 95% C.I.:1.07– 4.41) were factors associated with newborn anemia.
Conclusion: Anemia among newborns in the hospital was a moderate public health problem. Policy makers should consider maternal health education and appropriate health interventions to reduce the problem. In addition, further longitudinal studies are needed to identify specific causes of newborn anemia in order to prevent the possible complications.
Keywords: iron deficiency, neonates, maternal anemia, mode of delivery
Introduction
Anemia can be defined based on a decrease in hemoglobin (Hgb) levels, red blood cells (RBCs), or hematocrit. Based on the concentration of Hgb, anemia is a concentration of Hgb that is less than two standard deviations below the mean for the age and sex for the normal population.1 Since there is no set Hgb limit for cord blood to define newborn anemia, this study used a Hgb value of less than 13.5 g/dL, adopted from lower limit of study conducted in Ethiopia.2
Anemia is a widespread health threat that affects people around the world. According to global data from 2013, 2 billion people are affected by anemia. Children under 5 years of age are the age group at highest risk for devastating long-term effects of anemia.3
Infants under six months of age are at high risk of anemia due to their rapid growth and limited iron intake, as breast milk is low in iron.4 For this reason, they rely mainly on iron from intrauterine life.5 It is even more devastating when the pregnant mother, who is the source of fetal iron, is anemic. Approximately 42% of pregnant women worldwide and 22% of pregnant women in Ethiopia are anemic.6,7
There are insufficient studies conducted on the prevalence of newborn anemia in several parts of the world. According to studies conducted in sub-Saharan Africa, the prevalence of newborn anemia was 35% in Nigeria, 57% in Ghana, 23% in Malawi, and 61% in Benin.8–12 In two studies conducted in Ethiopia, the prevalence of 9% and 25% were reported in Addis Ababa and Gondar, respectively.13,14
Anemia before the age of 6 months is more than 2-folds associated with an increased rate of diarrheal and respiratory disease.15 Furthermore, anemia in newborns can lead to complications such as hypotension, mental confusion, heart failure and ultimately multiple organ failure.16
If the anemia is not corrected on time, irreversible long-term complications such as bone diseases, liver and spleen enlargement, growth disorders, decreased motor activity, social inattention, and severe cognitive impairments will follow.15–18
Although knowledge of the status of anemia in newborns is very important, global data on the prevalence of anemia do not include this age group and there are very insufficient studies of anemia in newborns.19 Although newborn anemia can have severe effects on the health and wellbeing of newborns along their life course, it receives little attention from health-care providers and researchers in low-income countries. There are no policies or guidelines for screening of newborn anemia in Ethiopia. To the best of our knowledge, no other study has addressed this problem in our study hospital, which serves a large number of populations in the West of the country. Therefore, this study aimed to determine the prevalence of newborn anemia and associated factors in Nekemte Specialized Hospital.
Materials and Methods
Study Area and Study Period
The study was conducted in the maternity ward at Nekemte Specialized Hospital. The Hospital is located in the city of Nekemte, the capital of East Wollega Zone, Oromia region, 331 km from Addis Ababa to western Ethiopia. It serves more than 2 million people. It is also serving as a clinical attachment site for medical and other health science students. The study was carried out from October 10, to November 20, 2020.
Study Design and Populations
A facility-based cross-sectional study was conducted from October to November, 2020 at the maternity ward of Nekemte Specialized Hospital in Western Ethiopia. The source population was all mothers with their term newborns born in 2020 at Nekemte Specialized Hospital. Mothers and their term newborn babies who fulfilled eligibility criteria and were born at Nekemte Specialized Hospital during the study period were the study population. Inclusion and exclusion criteria were as follows: Newborn babies with 37–42 completed weeks (term) of gestation and delivered in the hospital during the study period were included in the study. Twins, newborns with inaccessible umbilical cord blood samples, newborns with structural congenital anomalies, newborns of mothers with known non-obstetric diseases were excluded from the study.
Sample Size Determination and Sampling Techniques
The sample size was determined using single population proportion formula, with a 95% confidence level, a 5% error rate, and a 25% (0.25) prevalence (p) of anemia in full-term newborns from a study conducted at University of Gondar comprehensive specialized hospital.14 Using the formula, an initial sample size of 288 participants was found. According to data from Nekemte Specialized Hospital, 3683 deliveries took place in the hospital in one year in 2018/19. The source population used is 3683 (roughly the number of deliveries per year). Since 3683 is less than 10,000, the required sample size was calculated using a finite population proportion formula that gave n=268. Adding 10% of the sample size as a contingency for non-response rate, the total sample size was 295. In this study, all mothers and their newborns who met the eligibility criteria were consecutively recruited until the sample size was complete.
Data Collection Methods
The mother’s socio-demographic and clinical data were collected using a structured questionnaire based on interviews that was created in English and translated to the local languages. Maternal Mid upper arm circumference (MUAC) was measured using the standard method during the interview. The weight and sex of the newborn baby were determined by midwives at birth. Maternal Hgb was determined with a portable hemoglobinometer, the HemoCue Hgb analyzer (HemoCueHb 201+, Sweden) according to standard guidelines prior to the birth of the newborn. Two milliliters (2mL) of umbilical cord blood sample was collected. During the sampling, the umbilical cord was clamped 1–3 minutes after birth as recommended by the WHO.20 The collected sample was immediately poured into a test tube with ethylenediaminetetraacetic acid (EDTA) and gently mixed to prevent blood clotting. The collected sample was then taken to the hospital’s medical laboratory unit for Complete Blood Count (CBC) analysis using automated whole blood hematological analyzer (Mindray BC-5150). Two experienced laboratory technicians carried out the CBC in strict compliance with the standard operating procedures. In this study, newborn anemia is defined as Hgb <13.5g/dL (Adopted from study conducted in Ethiopia) and maternal anemia as Hgb <11g/dL.2,21
Data Processing and Analysis
The data was manually cleaned, processed, checked for completeness and entered into Epi-data version 3.1. It was then exported into SPSS version 20 for analysis. After categorizing and defining the variables, a descriptive analysis was carried out for each of the independent variables and presented with numbers, frequencies and percentages. Binary logistic regression analysis was used to assess the relationship between the dependent variable and each independent variable. A multivariable logistic regression analysis was then performed to control the confounding effect of other variables and to determine predictors of anemia. Associations between dependent and independent variables that result in a p-value of <0.25 were identified as candidates for the multivariable logistic regression model. An adjusted odds ratio (AOR) with a confidence interval of 95% and a p-value <0.05 were declared as having a significant relationship with the outcome variable. Multicollinearity and fitness of the model were checked.
Data Quality Control
Initially, a pre-test was performed to assess the integrity of questionnaire with 5% of the sample size at the Wollega University Referral Hospital. After the pretest, some modifications were made to the questionnaire. To ensure the quality of the data collectors and supervisors were given a one-day orientation to the approach to study participants, the use of the questionnaire, the demonstration of collecting maternal capillary and newborn UCB samples, the measurement of maternal MUAC, and about ethical approaches to data collection. To maintain the quality of the laboratory test, Canada Mount Sinai Hospital Lunenfeld – Tanenbaum Research Institute’s standard operating procedures for collecting perinatal specimens for research was followed. These include clamping the umbilical cord immediately after birth, positioning the placenta with the fetal surface and umbilical cord facing up, drawing blood from the umbilical vein with a sterile 10mL syringe with a sterile 18G blunt end needle, carefully inserting of the needle into the umbilical vein at a suitable angle, gently withdrawing the plunger of the syringe for blood collection, clamping of the umbilical cord above the venipuncture site, pulling the needle out of the umbilical cord and inserting it into the upper end of the blood collection tube and transferring blood into the tube and finally, invert the collection tube properly a few times to mix the blood sample.22 The CBC analysis was performed according to the hospital protocol. After the blood sample was taken, the sample and request paper were labeled with the same identification number. The quality of the data was maintained through daily on-site monitoring during the data collection period.
Ethical Considerations
Ethical approval to conduct the study was obtained from the Institutional Review Board of the Jimma University Institute of Health with reference number of IHRPGJ/836/2020. A written permission letter for data collection has been submitted to the administration of the Nekemte Specialized Hospital, maternity ward and the hospital’s laboratory department. The mother’s written informed consent and assent was obtained. For newborns diagnosed with anemia, communication has been established with the appropriate midwife for further assessment and treatment. In order to protect the privacy and confidentiality of the participants, no personal identification such as name was collected. Prevention of COVID-19 was considered by wearing personal protective equipment and applying necessary infection prevention techniques during all steps of data collection. This study was carried out in accordance with the Helsinki Declaration.
Results
Maternal Socio Demographic Characteristics
Two hundred seventy-eight (278) mothers and their newborns were included in this study, yielding a response rate of 94.2%. Table 1 shows the socio-demographic characteristics of the mother of newborns born at Nekemte Specialized Hospital. Most of the mothers (85.6%; 238/278) who gave birth to the newborns were between 20 and 34 years old with a mean age of 26 ± 4.4 years. Besides, the majority (55%; 153/278) of the mothers were from urban areas. About 89.6% (249/278) of the mothers were married. Around half (47.8%; 133/278) of them have no formal education or have only attended elementary school. According to this study, only 67/278 (24.1%) mothers were employed. In addition, the monthly family income of nearly quarter (25.2%; 70/278) of the mothers was below the World Bank’s extreme poverty line of $57 per month ($1.90 per day) or 2143ETB (Table 1).
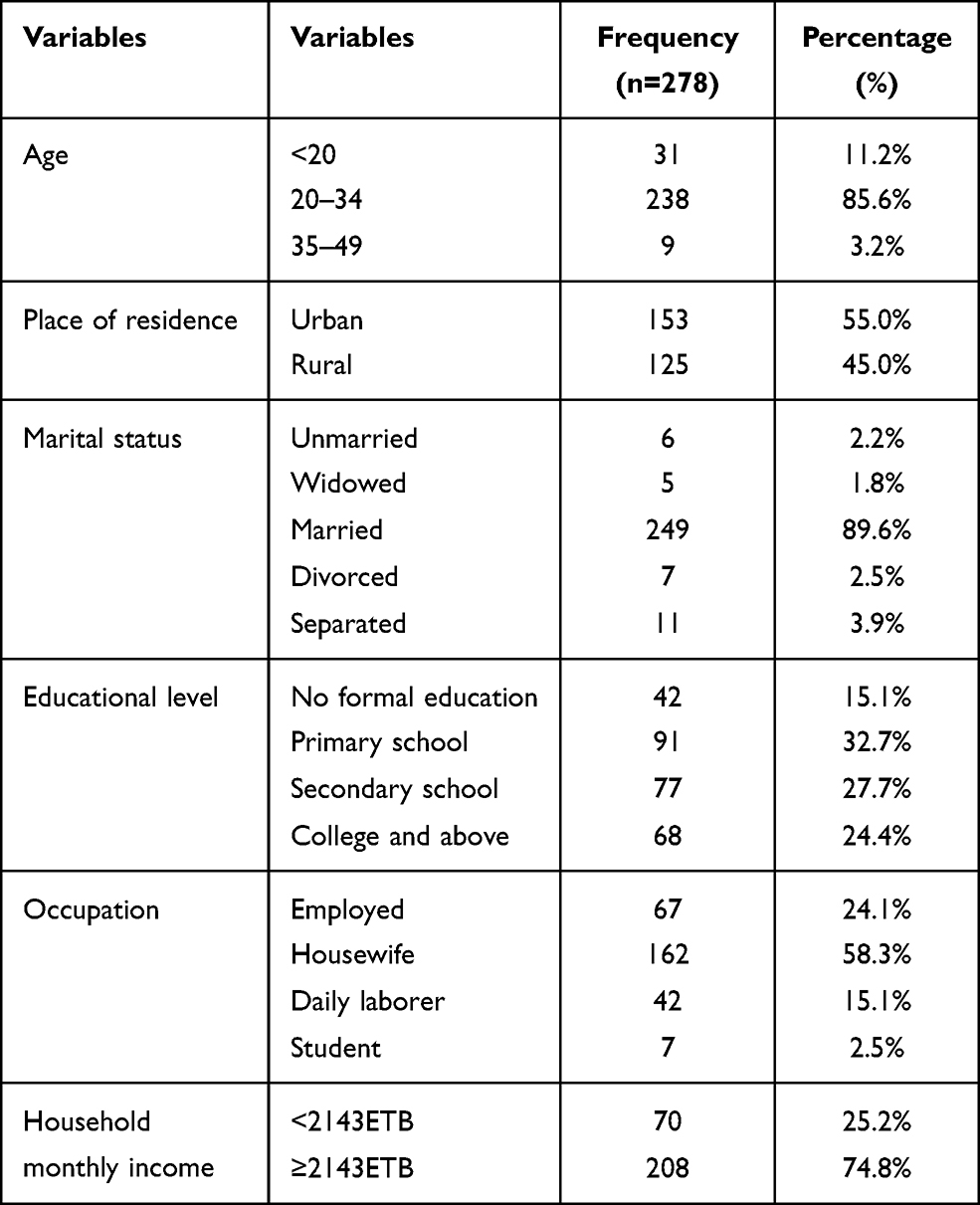 |
Table 1 Maternal Socio-Demographic Characteristics of Newborns Delivered at Nekemte Specialized Hospital, Western Ethiopia, October to November, 2020 (n=278) |
Maternal Obstetric Characteristics and Newborn Weight and Sex
Table 2 shows the maternal obstetric characteristics and the weight and sex of newborns at Nekemte Specialized Hospital. About eight in ten mothers (82%; 228/278) have had their ANC follow-up for the current pregnancy. But only just under a third (32.0%; 73/228) of the mothers finished their 4th visit. About a third (31.3%; 87/278) of the mothers were primiparous and more than two-thirds (72.3%; 201/278) stated that they had consumed iron-folate daily during their current pregnancy. Only twenty (7.2%; 20/278) mothers reported vaginal bleeding during pregnancy. Only about every sixth mother (17.3%; 48/278) gave birth to their baby by cesarean section. Regarding the maternal MUAC, 263/278 (94.6%) mothers had a MUAC of 23cm or more. Of the total of mothers participated in the study, 67/278 (24.1%) mothers had anemia with a Hgb concentration <11g/dl. Only 6 newborns had a weighed less than 2500g and the male-to-female ratio among the newborns was 0.97 to 1 (137/141) (Table 2).
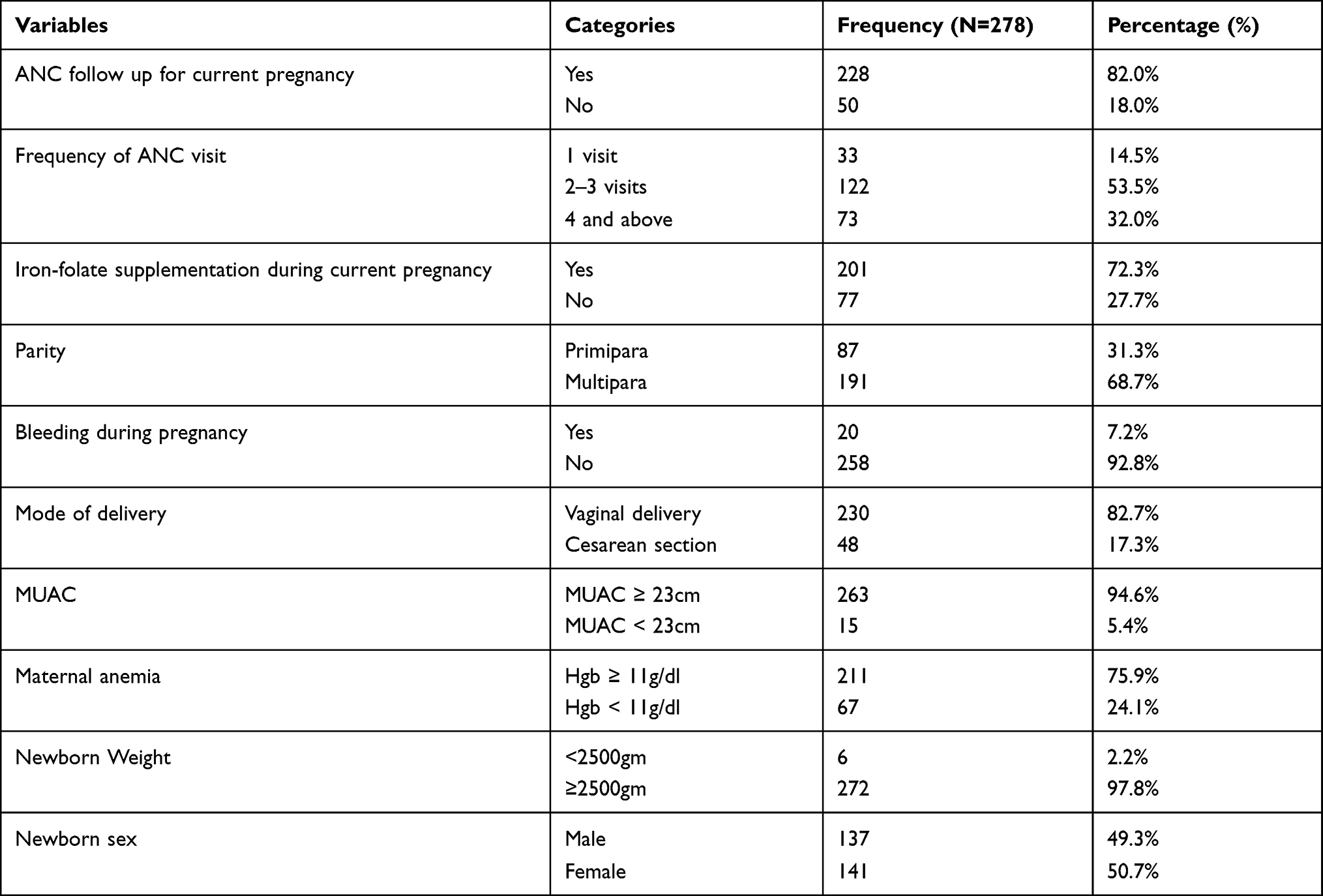 |
Table 2 Maternal Obstetric Characteristics and Newborns Weight and Sex at Nekemte Specialized Hospital, Western Ethiopia, October to November 2020 (n=278) |
Prevalence of Newborn Anemia
The prevalence of anemia (Hgb <13.5g/dl) among term newborns in Nekemte Specialized Hospital was 81/278 (29.1%) with a 95% Confidence Interval of 24.1% to 35.6%. The mean ± SD of Hgb concentration of the umbilical cord blood was 14.83 ± 2.22g/dl.
Predictors of Newborn’s Anemia
First, a bivariable logistic regression analysis was performed for all independent variables. Associations between dependent and independent variables resulted in a p-value of <0.25 in bivariable analysis were entered into SPSS version 20 using the backward LR method for multivariable logistic regression. Four variables showed a significant association with the prevalence of newborn anemia at a p-value <0.05.
Table 3 shows the multivariable logistic regression of factors associated with newborn’s anemia. Newborns delivered by cesarean section were 4.17 (95% C.I.: 1.89–9.20, P < 0.001) times more likely to be anemic compared to newborns delivered vaginally. Similarly, newborns from mothers with anemia during pregnancy were 3.95 (95% C.I.: 1.97–7.92, p < 0.001) times more likely to be anemic than newborns from non-anemic mothers.
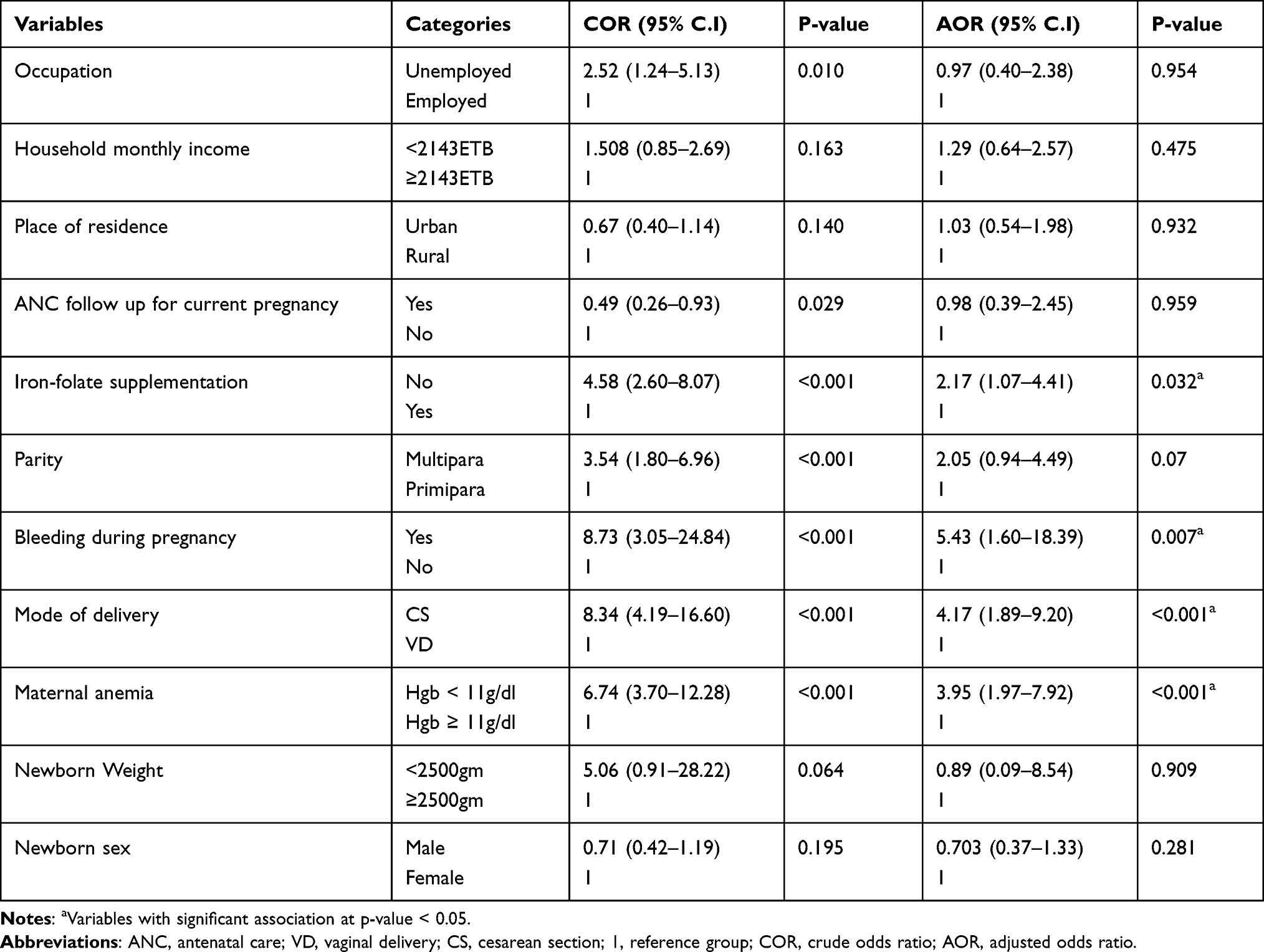 |
Table 3 Multivariable Logistic Regression Analysis Result Showing Factors Associated with Anemia Among Newborns at Nekemte Specialized Hospital, October to November, 2020 (n=278) |
The risk of developing anemia in newborns born to mothers without iron-folate supplementation during pregnancy was 2.17 (95% C.I.: 1.07–4.41, p=0.032) times higher than that of newborns born to mothers with iron-folate supplementation. Mothers who had vaginal bleeding during pregnancy were 5.43 (95% C.I.: 1.60–18.39, p=0.007) times more likely to give birth to anemic newborns (Table 3).
Discussion
This study attempted to determine the prevalence of anemia and associated factors in newborns born at Nekemte Specialized Hospital. Of a total of 278 newborns included in the study, 81 (29.1%) were anemic. The prevalence of anemia in this study compared to WHO public health limits indicates a moderate public health problem.19 Cesarean delivery, maternal anemia, maternal failure to take iron-folate supplements during pregnancy and vaginal bleeding during pregnancy were factors which have been associated with newborn anemia.
The prevalence of newborn anemia in this study is consistent with studies from Rio de Janeiro in Brazil (32.6%), Lagos Nigeria (35%), and Gondar in Ethiopia (25%).9,14,23
The observed prevalence of 29.1% in our finding is lower than that of studies in Ghana (57.3%), Benin (61.1%), and southern Nigeria (65.6%).8,10,11 The possible reason for the lower prevalence observed compared to the study in Ghana may be due to a difference in methodology, sample size, and study population. A study in Ghana was prospectively studied on a sample of 1154, including premature babies, about half of the mothers of whom had HIV or malaria infection. Besides, Hgb cut-off point used in the study conducted in Ghana was 12.5 g/dL. In addition, the study in Benin was prospectively studied for over one-year with 617 mothers and 656 newborns, including premature births and multiple pregnancies. A study from Nigeria was examined in malaria-endemic areas. These factors may have increased the prevalence of newborn anemia in these studies.
The results of the current study revealed a higher prevalence of newborn anemia than studies in New York, USA (21%), the Netherlands (21%), Romania (3.1%), Nepal (5.7%), southern Malawi (23.4%), and Addis Ababa (9%).12,13,24–27 The lower prevalence in New York, the Netherlands, and Romania could be due to the difference in the socio-demographics and economic status of the mothers in our study. The GDP (Gross Domestic Product) per capita in US dollars (USD) of the United States, the Netherlands and Romania in 2020 is 63,543, 52,304 and 12,896, respectively. However, in 2020, Ethiopia’s GDP per capita was $936.28.28 The literacy rate of the Romanian population aged 15 years and over was 98.88. But only 51.8% of Ethiopia’s 15-year-olds and older are literate.29 The deviation from the study conducted in Malawi may be due to the use of a lower Hgb limit (<12.5g/dl) in the Malawian study. The difference between our study and studies from Nepal and Addis Ababa could be due to the small sample size in both studies (Nepal: n=114, Addis Ababa: n=89) compared to our study.
Maternal anemia was one of the factors linked to newborn anemia in our study, which is in line with studies done in, Turkey, Ghana, Nigeria, Benin, Malawi, and Addis Ababa.8,9,11–13,30 The possible reasons for this association can be attributed to factors such as nutritional deficiencies, hemoglobin variants and hemolytic disorders. However, the present finding contradicts studies from Iran and Gondar.14,31 In addition, a Pakistani study reported no association between maternal and newborn Hgb scores.32 The discrepancy could be due to the small sample size in studies from Iran (n=170 newborns) and Gondar (n=192 newborns) and the exclusion of mothers with Hgb <10g/dL in the study from Pakistan, which is not excluded in the present study.
According to our study, cesarean delivery increases newborn anemia more than four-fold than that of vaginal delivery. This study is in line with several studies in Egypt, Pakistan, South Korea, the Netherlands, and Poland.25,33–37 The possible reason for increased anemia in newborns born by cesarean section may be attributed to the following causes: Cesarean section is associated with weak force and duration of placental transfusion, which can lead to anemia in newborns. The decrease in placental transfusion during cesarean section may be due to the lack of uterine or vaginal pressure, which pushes fluids out of the fetus’ lungs and supports breathing, the effect of anesthesia, uterine incision, and immediate clamping of the umbilical cord.38
In contrast to our study, studies in Turkey and Iraq found no significant association between cesarean section and newborn hemoglobin levels.39,40 A possible explanation could be the small number of newborns (n= 7) delivered by cesarean section in the study carried out in Turkey and the difference in study design compared to the study carried out in Iraq.
In the current study, newborns born to mothers who had vaginal bleeding during pregnancy had a higher prevalence of anemia than newborns born to mothers without vaginal bleeding. This finding is supported by a study conducted in Canada.41 In contrast, a study conducted in South Korea found no significant association between admission for vaginal bleeding and newborn anemia.36 The possible discrepancy between this study and our study could be due to the difference in study design, methodology and socio-demographic status of the mothers from those in our study. The study conducted in South Korea used a retrospective case-control design with singleton births after 26 gestational weeks that were complicated with placenta previa. The cut-off point used in the study was different from our study (14.5g/dL). According to the World Bank, South Korea’s GDP per capita in 2020 was $31,489. However, in 2020, Ethiopia’s GDP per capita was $936.28 According to the WHO Global Health Observatory report (2018), the neonatal mortality rate in South Korea’s and Ethiopia was 2.79/1000 live births versus 28.57/1000 live births. ANC coverage of at least 4 visits in South Korea was 98.1% and Ethiopia’s 4th ANC visit coverage was only 43.00%.42 Besides, mothers with vaginal bleeding in South Korea tend to seek medical help early and receive adequate treatment than mothers in our study due to better health-care systems.
In the present study, maternal iron-folate supplementation of the mother during pregnancy was associated with reduced newborn anemia. A study in Iraq, Italy, and Peru also supports our current results.43–45 The possible reason for the protective effect of maternal iron-folate supplementation during pregnancy is that iron supplementation during pregnancy increases maternal iron stores. This in turn increases the amount of placental iron transfer to the fetus.
Overall, this study yielded important insights into the prevalence of newborn anemia in Nekemte Specialized Hospital and the associated factors. The results of this study can be used by health professionals and policy makers to plan improvements at this age. However, there are some limitations in this study. Micronutrient deficiencies responsible for the anemia or specific causes of anemia in newborns have not been identified. In addition, red cell indices are not included in this study. A relatively small sample size was used in this study. Since the study design was cross-sectional, it is difficult to establish a causal relationship between newborn anemia and the factors involved.
Conclusion
According to this study, the prevalence of anemia in term newborns at Nekemte Specialized Hospital was 29.1%. Maternal anemia, cesarean delivery, vaginal bleeding during pregnancy, and lack of iron-folate supplementation during pregnancy were factors that have been linked to newborn anemia. Hence, health-care providers and the policy makers should pay attention to pregnant women with the risk factors. It is also recommended that women of childbearing potential be educated about newborn anemia. Large longitudinal studies with larger sample sizes are also required to identify the specific etiologies and causes of newborn anemia.
Acknowledgments
The authors would like to acknowledge Jimma University biomedical science department unit of anatomy and Nekemte Specialized Hospital for their support provided throughout the study period.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Lanzkowsky P. Classification and diagnosis of anemia in children. In: Lanzkowsky’s Manual of Pediatric Hematology and Oncology. Elsevier; 2016:32–41.
2. Tiruneh T, Kiros T, Getu S. Hematological reference intervals among full-term newborns in Ethiopia: a cross-sectional study. BMC Pediatr. 2020;20(1):1–6. doi:10.1186/s12887-020-02320-5
3. Kassebaum NJ. The global burden of anemia. Hematol Oncol Clin. 2016;30(2):247–308. doi:10.1016/j.hoc.2015.11.002
4. Lozoff B, Beard J, Connor J, Felt B, Georgieff M, Schallert T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr Rev. 2006;64(5):S34–S43. doi:10.1301/nr.2006.may.S34-S43
5. Chaparro CM. Setting the stage for child health and development: prevention of iron deficiency in early infancy. J Nutr. 2008;138(12):2529–2533. doi:10.1093/jn/138.12.2529
6. Bekele A, Tilahun M, Mekuria A. Prevalence of anemia and its associated factors among pregnant women attending antenatal care in health institutions of Arba Minch Town, Gamo Gofa Zone, Ethiopia: a cross-sectional study. Anemia. 2016;2016:1–9. doi:10.1155/2016/1073192
7. WHO. Worldwide Prevalence of Anaemia 1993–2005: WHO Global Database on Anaemia. WHO; 2008.
8. Laar AK, Grant FE, Addo Y, et al. Predictors of fetal anemia and cord blood malaria parasitemia among newborns of HIV-positive mothers. BMC Res Notes. 2013;6(1):350. doi:10.1186/1756-0500-6-350
9. Adediran A, Gbadegesin A, Adeyemo TA, et al. Cord blood haemoglobin and ferritin concentrations in newborns of anaemic and non-anaemic mothers in Lagos, Nigeria. Niger Med J. 2013;54(1):22. doi:10.4103/0300-1652.108889
10. Uneke C, Iyare F, Sunday-Adeoye I, Asiegu O, Nwosu K, Ajayi J. Effects of maternal plasmodium falciparum malaria, anemia and HIV infection on fetal hemoglobin levels in Nigeria. Internet J Gynecol Obstet. 2009;12. Available from: http://ispub.com/IJGO/12/1/12598.
11. Koura GK, Ouedraogo S, Le Port A, et al. Anaemia during pregnancy: impact on birth outcome and infant haemoglobin level during the first 18 months of life. Trop Med Int Health. 2012;17(3):283–291.
12. Brabin B, Kalanda BF, Verhoeff FH, Chimsuku L, Broadhead R. Risk factors for fetal anaemia in a malarious area of Malawi. Ann Trop Paediatr. 2004;24(4):311–321. doi:10.1179/027249304225019136
13. Terefe B, Birhanu A, Nigussie P, Tsegaye A. Effect of maternal iron deficiency anemia on the iron store of newborns in Ethiopia. Anemia. 2015;2015:1–6. doi:10.1155/2015/808204
14. Tiruneh T, Shiferaw E, Enawgaw B. Prevalence and associated factors of anemia among full-term newborn babies at University of Gondar comprehensive specialized hospital, Northwest Ethiopia: a cross-sectional study. Ital J Pediatr. 2020;46(1):1–7. doi:10.1186/s13052-019-0764-1
15. Levy A, Fraser D, Rosen SD, et al. Anemia as a risk factor for infectious diseases in infants and toddlers: results from a prospective study. Eur J Epidemiol. 2005;20(3):277–284. doi:10.1007/s10654-004-6515-6
16. Allali S, Brousse V, Sacri A-S, Chalumeau M, de Montalembert M. Anemia in children: prevalence, causes, diagnostic work-up, and long-term consequences. Expert Rev Hematol. 2017;10(11):1023–1028. doi:10.1080/17474086.2017.1354696
17. Abay A, Yalew HW, Tariku A, Gebeye E. Determinants of prenatal anemia in Ethiopia. Archiv Public Health. 2017;75(1):51. doi:10.1186/s13690-017-0215-7
18. Mosiño A, Villagómez-Estrada KP, Prieto-Patrón A. Association between school performance and anemia in adolescents in Mexico. Int J Environ Res Public Health. 2020;17(5):1466. doi:10.3390/ijerph17051466
19. WHO. The Global Prevalence of Anaemia in 2011. Geneva: WHO; 2015.
20. World Health Organization. Guideline: Delayed Umbilical Cord Clamping for Improved Maternal and Infant Health and Nutrition Outcomes. World Health Organization; 2014.
21. WHO. Iron deficiency anemia. assessment, prevention, and control. A Guide for Programme Managers. WHO; 2001:47–62.
22. Research center for women’s and Infants’s Health (2) BioBank. Standard Operating Procedures for the Collection of Perinatal Specimens for Research. Canada Mount Sinai Hospital Lunenfeld- Tanenbaum Research Institute; 2015.
23. de Sá SA, Willner E, Pereira TAD, de Souza VR, Boaventura GT, de Azeredo VB. Anemia in pregnancy: impact on weight and in the development of anemia in newborn. Nutr Hosp. 2015;32(5):2071–2079.
24. Lee S, Guillet R, Cooper EM, et al. Prevalence of anemia and associations between neonatal iron status, hepcidin, and maternal iron status among neonates born to pregnant adolescents. Pediatr Res. 2016;79(1):42–48. doi:10.1038/pr.2015.183
25. Kalteren WS, Ter Horst HJ, den Heijer AE, de Vetten L, Kooi EM, Bos AF. Perinatal anemia is associated with neonatal and neurodevelopmental outcomes in infants with moderate to severe perinatal asphyxia. Neonatology. 2018;114(4):315–322. doi:10.1159/000490369
26. Simion IN, Iacob D, Fratila A, Nyiredi A, Ilie C. Assessment of neonatal anemia and its impact in neonatal adaptation. Revista Societatii Române De Chirurgie Pediatrica. 2013;16:54.
27. Timilsina S, Karki S, Gautam A, Bhusal P, Paudel G, Sharma D. Correlation between maternal and umbilical cord blood in pregnant women of Pokhara Valley: a cross sectional study. BMC Pregnancy Childbirth. 2018;18(1):70. doi:10.1186/s12884-018-1697-1
28. World Bank. GDP per capita (Current US$)-1960 to 2020; 2021. Available from: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD.
29. UNESCO Institute of Statstics. Literacy rate, adult total (% of people ages 15 and above); 2021. Available from: https://data.worldbank.org/indicator/SE.ADT.LITR.ZS.
30. Dane B, Arslan N, Batmaz G, Dane C. Does maternal anemia affect the newborn. Özgün Arastirma. 2013;195–199. Available from: turkarchpediatr.org//en/does-maternal-anemia-affect-the-newborn-13536.
31. McArdle H, Andersen H, Jones H, Gambling L. Copper and iron transport across the placenta: regulation and interactions. J Neuroendocrinol. 2008;20(4):427–431. doi:10.1111/j.1365-2826.2008.01658.x
32. Qaiser DH, Sandila MP, Omair A, Ghori GM. Correlation of routine haematological parameters between normal maternal blood and the cord blood of healthy newborns in selected hospitals of Karachi. J Coll Physicians Surg Pak. 2013;23(2):128–131.
33. El Gendy FM, Allam AA, Allam MM, Allam RK. Haematological parameters of newborns delivered vaginally versus caesarean section. Menoufia Med J. 2016;29(2):259. doi:10.4103/1110-2098.192429
34. Abd El-Gaber AE-N, Mahmoud AM. Correlation between mode of delivery and newborn’s cord blood composition. Open J Obstetr Gynecol. 2019;9(3):395–403. doi:10.4236/ojog.2019.93040
35. Qaiser DH, Sandila MP, Kazmi T, Ahmed ST. Influence of maternal factors on hematological parameters of healthy newborns of Karachi. Pak J Physiol. 2009;5(2):34–37.
36. Jang DG, Jo YS, Lee SJ, Lee GSR. Risk factors of neonatal anemia in placenta previa. Int J Med Sci. 2011;8(7):554. doi:10.7150/ijms.8.554
37. Redźko S, Przepieść J, Żak J, Urban J, Wysocka J. Influence of perinatal factors on hematological variables in umbilical cord blood. J Perinat Med. 2005;33(1):42–45. doi:10.1515/JPM.2005.007
38. Zhou Y-B, Zhu L-P, Liu J-M, Liu J-M. Impact of cesarean section on placental transfusion and iron-related hematological indices in term neonates: a systematic review and meta-analysis. Placenta. 2014;35(1):1–8. doi:10.1016/j.placenta.2013.10.011
39. Beşkardeş A, Salihoğlu Ö, Can E, Atalay D, Akyol B, Hatipoğlu S. Oxygen saturation of healthy term neonates during the first 30 minutes of life. Pediatr Int. 2013;55(1):44–48. doi:10.1111/j.1442-200X.2012.03731.x
40. Al-Habbobi -MAA-M, Al-Mudallal SS. Evaluation of the effect of mode of delivery on hematological parameters of healthy full-term newborns. Iraqi J Med Sci. 2010;8(1):29–38.
41. Crane JM, Van den Hof MC, Dodds L, Armson BA, Liston R. Neonatal outcomes with placenta previa. Obstet Gynecol. 1999;93(4):541–544.
42. World Health Organization. Global health observatory, Ethiopia, Republic of Korea; 2021. Available from: https://www.who.int/data/gho/data/countries.
43. Al-bakka AA, Umran RM. Effect of maternal supplementation with iron on neonatal iron status and birth weight. Med J Babylon. 2013;10(4):827–833.
44. Parisi F, Berti C, Mandò C, Martinelli A, Mazzali C, Cetin I. Effects of different regimens of iron prophylaxis on maternal iron status and pregnancy outcome: a randomized control trial. J Mater Fetal Neonat Med. 2017;30(15):1787–1792. doi:10.1080/14767058.2016.1224841
45. O’Brien KO, Zavaleta N, Abrams SA, Caulfield LE. Maternal iron status influences iron transfer to the fetus during the third trimester of pregnancy. Am J Clin Nutr. 2003;77(4):924–930. doi:10.1093/ajcn/77.4.924
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.