")
Back to Journals » Clinical Interventions in Aging » Volume 16
Prevalence, Characteristics, and Associated Risk Factors of the Elderly with Hip Fractures: A Cross-Sectional Analysis of NHANES 2005–2010
Authors Zhang YW, Lu PP , Li YJ, Dai GC, Chen MH, Zhao YK, Cao MM, Rui YF
Received 8 November 2020
Accepted for publication 22 December 2020
Published 27 January 2021 Volume 2021:16 Pages 177—185
DOI https://doi.org/10.2147/CIA.S291071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yuan-Wei Zhang,1– 5,* Pan-Pan Lu,1– 5,* Ying-Juan Li,2,6 Guang-Chun Dai,1– 5 Min-Hao Chen,1– 5 Ya-Kuan Zhao,1– 5 Mu-Min Cao,1– 5 Yun-Feng Rui1– 5
1Department of Orthopedics, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, Jiangsu, People’s Republic of China; 2Multidisciplinary Team (MDT) for Geriatric Hip Fracture Management, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, Jiangsu, People’s Republic of China; 3School of Medicine, Southeast University, Nanjing, Jiangsu, People’s Republic of China; 4Orthopaedic Trauma Institute (OTI), Southeast University, Nanjing, Jiangsu, People’s Republic of China; 5Trauma Center, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, Jiangsu, People’s Republic of China; 6Department of Geriatrics, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun-Feng Rui
Department of Orthopedics, Zhongda Hospital, School of Medicine, Southeast University, No. 87 Ding Jia Qiao, Nanjing, Jiangsu 210009, People’s Republic of China
Email [email protected]
Objective: This cross-sectional study was aimed to update the assessment of prevalence, characteristics, and risk factors of the elderly with hip fractures in a non-institutionalized American population.
Methods: This current study included a total of 31,034 participants from the existing National Health and Nutritional Examination Survey (NHANES) database from 2005 to 2010, and 4,265 participants aged 65 years and older were ultimately identified. Their condition of hip fractures was determined by method of questionnaires according to the orthopedic surgeons’ diagnosis, and related epidemiological and demographic data were further collected. The univariate analysis was used to screen the risk factors of hip fractures in the elderly, and the logistic regression model was established to conduct the multivariate analysis.
Results: Of the total 4,265 participants with clear information of hip fractures in elderly, 127 individuals with hip fractures were identified according to results of questionnaires, exhibiting a prevalence of 28.49 per 1,000 (95% confidence interval [CI]=21.38– 35.60) for males and 31.03 per 1,000 (95% CI=23.72– 38.35) for females. The mean age of the elderly with hip fractures was 77.12± 5.88 years and tumble (48.0%) was the primary factor. In univariate analysis, age, race, smoking, drinking alcohol, and combined with osteoporosis were regarded as risk factors. Multivariate analysis showed that age (80 years and older), living alone, smoking, combined with diabetes and osteoporosis were the independent risk factors.
Conclusion: Our nationwide data indicate the prevalence of hip fractures in the elderly is generally on the rise, and the female occupies a higher proportion. Age (especially aged 80 years and older), race (mainly Non-Hispanic white), smoking, drinking alcohol, living alone, combined with diabetes and osteoporosis may be closely linked to the occurrence of hip fractures in the elderly, although these variables still need to be verified in further prospective investigations.
Keywords: hip fracture, the elderly, prevalence, risk factor, NHANES
Introduction
Recently, the elderly with hip fractures have become an increasingly serious public health problem worldwide. As the global society continues to age, the number of elderly patients with hip fractures has increased dramatically. It is estimated that by the middle of this century, more than 6 million individuals will suffer from hip fractures each year around the world, and most of them are elderly.1–3 Meanwhile, the disease conditions of elderly patients with hip fractures tend to be complicated, and the pressures that the medical and health service system must face is becoming more and more severe. Thus, due to the poor prognosis, various kinds of complications and high mortality, the elderly with hip fractures are often regarded as “the last fracture of whole life”.4–6 With regard to this, common risk factors of hip fractures in the elderly have also been reported in previous literature, which mainly includes advanced age, gender, smoking, drinking alcohol, hypertension, diabetes, and osteoporosis, and so on.5,6
However, the health management of elderly patients with hip fractures still has a long way to go. In this process, it is necessary to emphasize the prevention work before fractures, so as to avoid the domino effect caused by fracture as much as possible, such as the continued disability or even lethal effect, and the severe burden and consumption of financial, material and human resources.7–9 Regarding this, effective recognition of the associated risk factors of the elderly with hip fractures can provide a theoretical basis for the effective prevention of hip fractures. Therefore, this study is aimed to comprehensively investigate the prevalence, characteristics, and associated risk factors of the elderly with hip fractures based on a population from the NHANES 2005–2010. To the best of our knowledge, this is the first time to extract and analyze the relevant data of hip fractures in the elderly through the NHANES database, so as to provide a certain reference value for the related research in the future.
Methods
Data Source and Study Participants
The overall data in this study was obtained from the NHANES database during 2005–2010. In order to address the emerging public health issues and provide objective data on health conditions for American civilians, the NHANES database was set up and constantly updated and improved by American Centers for Disease Control and Prevention (CDC). Moreover, the representative sample of the non-institutionalized American civilians in each 2-year data collection cycle, such as health information and laboratory data, were selected by CDC via a multistage and complicated clustered probability design, which are all accessible for the researchers on the internet.10
In this study, we included a total of 31,034 participants from NHANES 2005–2010, and 4,265 participants aged 65 years and older remained after exclusion of three subjects with unclear memory of self-experienced hip fractures. Moreover, Figure 1 reveals the flow chart of the sample selection. During the process of extracting data from the NHANES database, the sequence of fracture history and risk factors were matched to each other by collection circles, which was also a fixed circle with continued information updated. In addition, it is worth noting that this is an exempt study due to the fact that the current study only involved secondary data analysis of the existing NHANES database, which is publicly available and have been de-identified, thus there is no need to apply an IRB approval from our own institution.
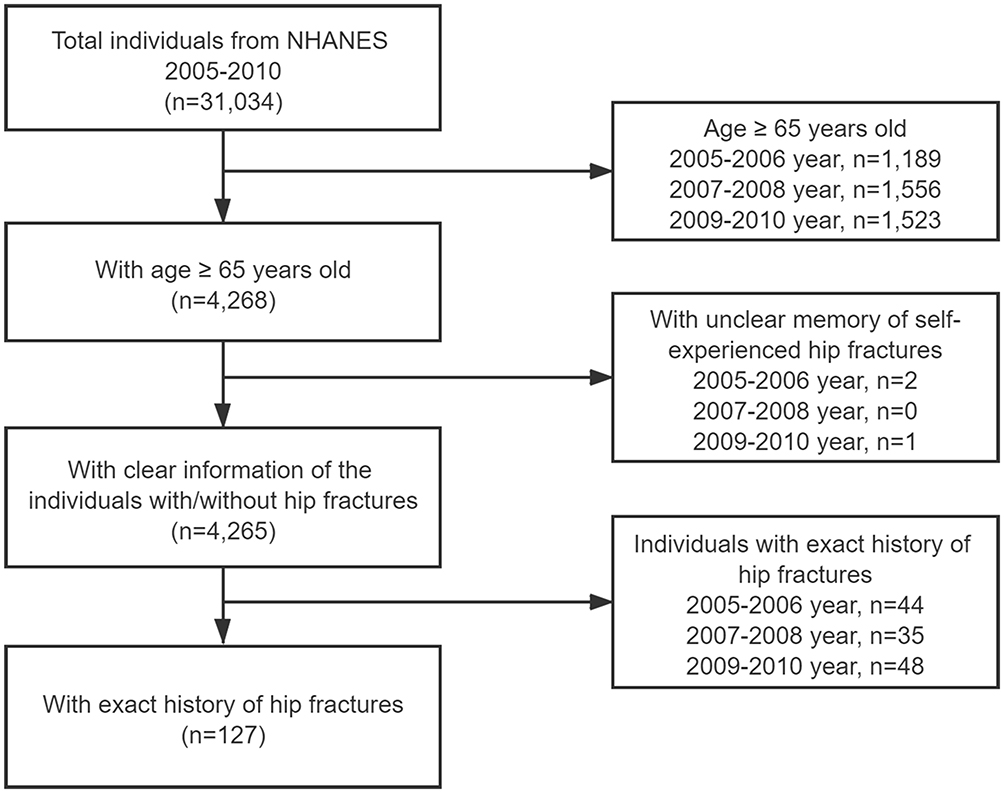 |
Figure 1 Flow chart of the sample selection from the NHANES 2005–2010. |
Related Epidemiological and Demographic Characteristics
According to the timeline defined by the NHANES database, the elderly with hip fractures were divided into the year groups of 2005–2006, 2007–2008, and 2009–2010. Moreover, the epidemiological characteristics of the elderly with hip fractures in this study were mainly described by 2-year as a cycle in the following variables: age, gender, total number of the elderly, prevalence of the elderly with hip fractures, times of hip fractures, and the specific age and factors of hip fracture in each time. In addition, it is also worth noting that, although this study included the information of the elderly (aged 65 years and older) with hip fractures, the first time they had a hip fracture might have been in childhood or adolescence.
Study Variables and Covariates
Furthermore, the overall individuals included in this study were naturally divided into the hip fracture group and non-hip fracture group according to the exact history of hip fractures. In the NHANES 2005–2010, the self-reported conditions of individuals in this study were collected through the method of questionnaires, including age, gender, race (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, and Other Race), marital status (married, living with partner, widowed, divorced, separated, and never married), smoking, drinking alcohol, combined with diseases (hypertension, diabetes, and osteoporosis), the medication history of the prednisone or cortisone, and the parents’ history of hip fractures. Moreover, it is essential to note that the condition of hip fractures was determined according to the professional orthopedic surgeons’ diagnosis. The details of study variables and covariates in this current study are all able to be wholly searched at the webpage of www.cdc.gov/nchs/nhanes.
Statistical Analysis
The overall data in this current study were extracted and statistically analyzed by the R version 4.0.3 software (R Foundation, Vienna, Austria) and SPSS 26.0 software (SPSS, Inc, Chicago, IL, USA), and manifested as mean±standard deviation (SD) or count (percentage). Moreover, accounting for the complicated sample survey designs, the related epidemiological and demographic characteristics between the participants with and without hip fractures were evaluated by Student’s t-test for continuous variables and Chi-square test for categorical variables. Moreover, for the variables of age, gender, race, marital status, smoking, drinking alcohol, combined with diseases, the medication history of prednisone or cortisone and the parents’ history of hip fractures were all assessed by the univariate analysis to screen the risk factors of hip fractures in the elderly. Then the logistic regression model was applied to conduct the multivariate analysis of associated risk factors in the elderly with hip fractures. In the logistic regression models, the link between the hip fractures and associated risk factors was exhibited as an odds ratio (OR) with a 95% CI. A P-value<0.05 was regarded as statistically significant.
Results
In a total of 4,265 participants with clear information of hip fractures in elderly, 127 individuals with hip fracture were identified according to the results of questionnaires, exhibiting a prevalence of 28.49 per 1,000 (95% CI=21.38–35.60) for males and 31.03 per 1,000 (95% CI=23.72–38.35) for females. In addition, the mean age of elderly with hip fractures included in this study was 77.12±5.88 years, and the females occupied a higher proportion (67/127, 52.8%). As for the frequency of hip fractures in elderly, it mainly only occurred once (116/127, 91.3%), and the occurrence of five times was the peak among the included individuals. Moreover, excluding the missing data in the NHANES database, from the factors of hip fracture that all included individuals suffered in the first time, tumble was the first (61/127, 48.0%), and fall from height ranked the second (26/127, 20.5%). Compared with the young and middle-aged individuals with hip fractures, traffic accidents were much lower in elderly with hip fractures (6/127, 4.7%).11 Besides, the proportion of individuals with multiple occurrences of fractures was 41/127 (32.3%). Related epidemiological and demographic characteristics of the elderly with hip fractures included in NHANES from 2005 to 2010 are summarized in Table 1, and the age and factors of the second to fifth times hip fracture of partial elderly are presented in the Supplementary Table 1.
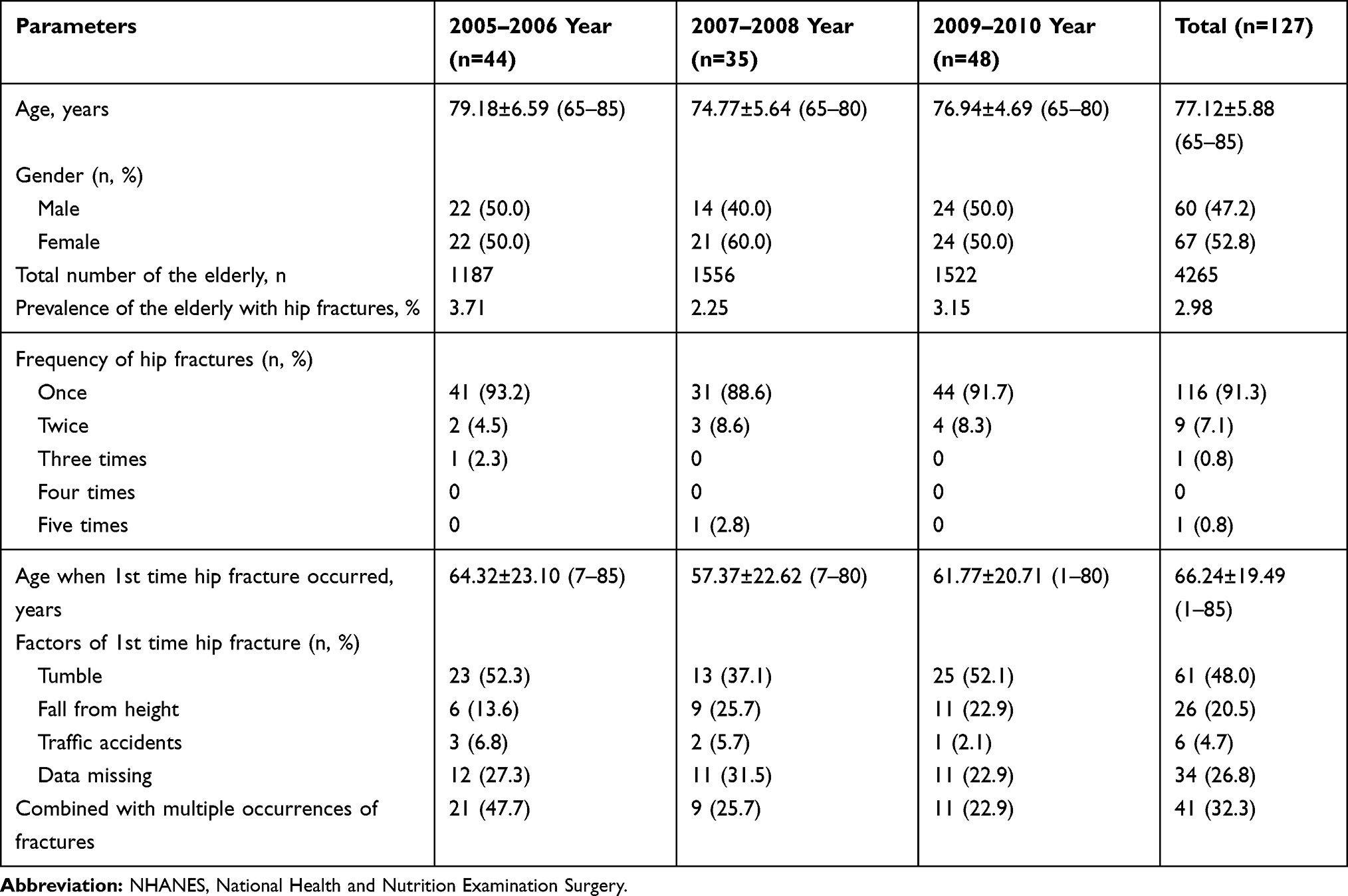 |
Table 1 Related Epidemiological and Demographic Characteristics of the Elderly with Hip Fractures Included in NHANES from 2005 to 2010 |
Table 2 reveals the univariate analysis of associated risk factors in the elderly with hip fractures. Therein, the mean age was significantly older in the hip fracture group (77.12±5.88 years) than in the non-hip fracture group (74.14±5.69 years), (t=5.813, P<0.001). Furthermore, by further dividing the included individuals into the groups of 65–80 years and ≥80 years, it can be discovered that the hip fracture group has the higher age characteristics (χ2=36.487, P<0.001). In terms of the factor of race, Non-Hispanic White exhibited a higher incidence of the elderly with the hip fractures than other ethnic groups (χ2=20.212, P<0.001). Moreover, similar to the several previous reports,12–15 the factors of smoking and drinking alcohol were also regarded as the risk factors for the elderly with hip fractures (χ2=36.914, P<0.001; χ2=8.292, P=0.004). Additionally, individuals combined with osteoporosis in hip fractures group also showed a significant difference with the non-hip fractures group (χ2=19.832, P<0.001), and no significant difference between the two groups were identified in terms of other factors.
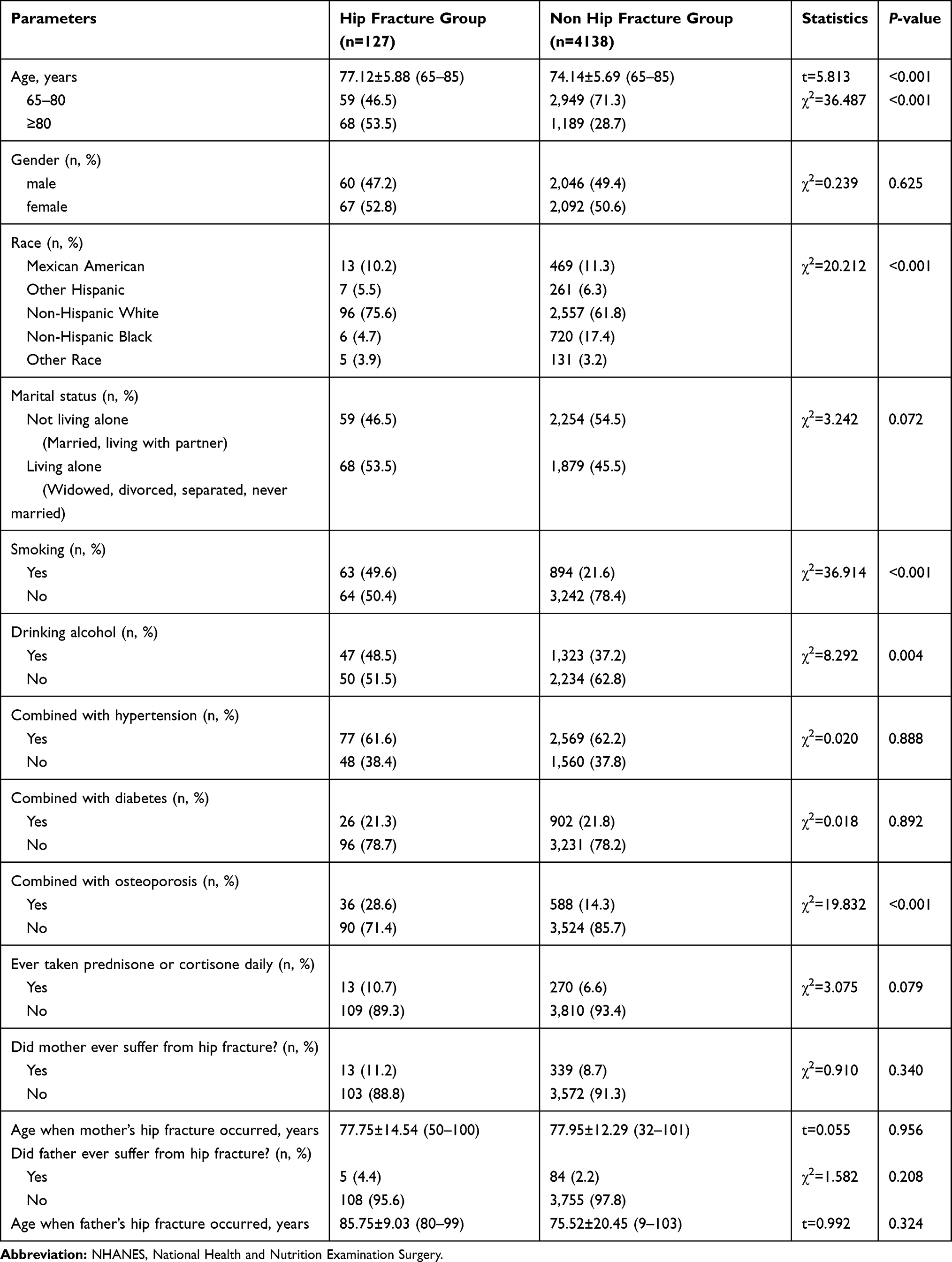 |
Table 2 Univariate Analysis of Associated Risk Factors in the Elderly with Hip Fractures Included in NHANES from 2005 to 2010 |
The multivariate analysis of associated risk factors in the elderly with hip fractures are summarized in Table 3, which indicates that individuals aged 80 years and older (OR=1.142, 95% CI=1.101–1185, P<0.001), living alone (OR=0.458, 95% CI=0.300–0.700, P<0.001), smoking (OR=0.035, 95% CI=0.022–0.055, P<0.001), combined with diabetes (OR=1.636, 95% CI=1.081–2.475, P=0.020), and combined with osteoporosis (OR=1.895, 95% CI=1.260–2.850, P=0.002) were the apparent independent risk factors of the elderly with hip fractures.
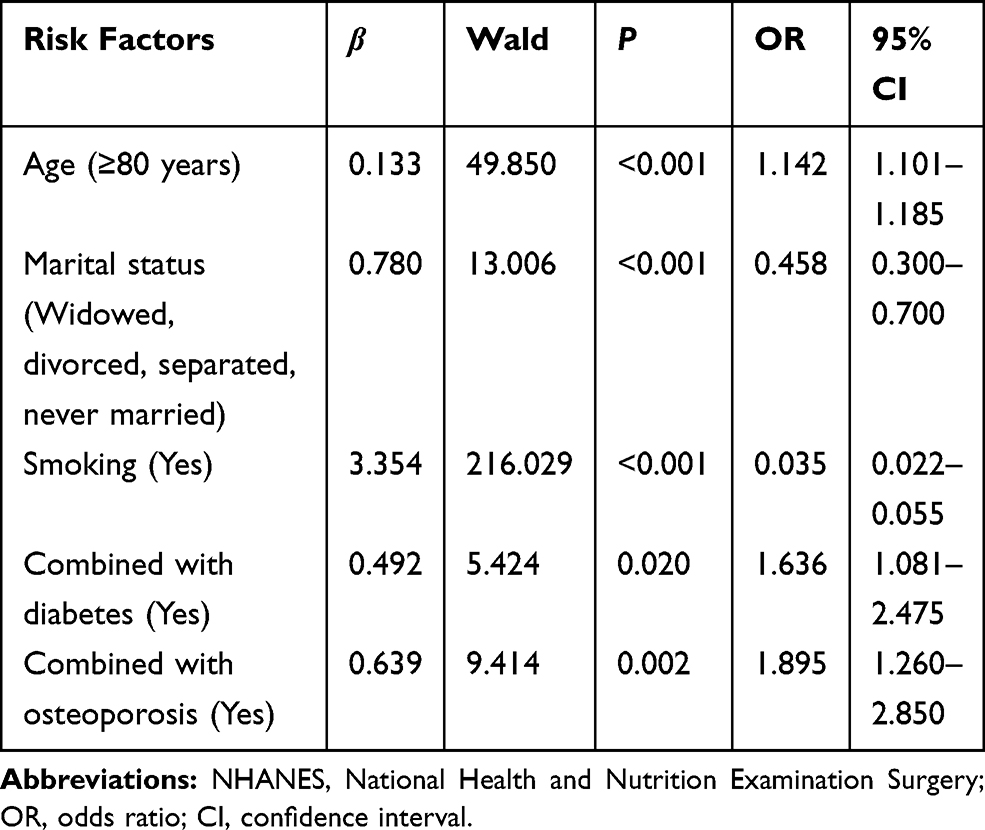 |
Table 3 Multivariate Analysis of Associated Risk Factors in the Elderly with Hip Fractures Included in NHANES from 2005 to 2010 |
Discussion
With the increase of age, the functions of various organs and tissues of the elderly gradually degenerate, and the physical function and physiological reserve capacity also decline. Moreover, the elderly usually have a combination of osteoporosis and a variety of comorbidities, which easily results in the occurrence of hip fractures.16,17 The result of this study reveals that the mean age of the hip fracture group is 77.12±5.88 years, and the female occupies a higher proportion (52.8%). This result may be related to the significantly higher incidence of postmenopausal osteoporosis in females than males. Osteoporosis in the elderly can bring about the increased fragility of bone, and only a slight trauma will cause the fractures.18 Additionally, the prevalence of hip fractures in the elderly is generally on the rise. Based on the information collected in NHANES 2005–2010, the prevalence of the elderly with hip fractures is 28.49 per 1,000 (95% CI=21.38–35.60) for males and 31.03 per 1,000 (95% CI=23.72–38.35) for females, which is generally higher than the previous reports between 1986 and 2005, with the annual mean number of hip fractures was 4.14 per 1,000 (95% CI=4.02–4.27) for males and 9.57 per 1,000 (95% CI=9.22–9.93) for females.19 Meanwhile, this result also vividly interprets the severe test and heavy pressure brought by the geriatric hip fractures to the health service system, which emphasizes the significance of the prevention and control of it.
Furthermore, this study also indicates that tumble (48.0%) is the primary factor of the elderly with hip fractures, which is consistent with the report by Dontas and Yiannakopoulos.20 Regarding this, in addition to the common factor of osteoporosis, the coordination and reaction abilities of the elderly also continue to decline with the increase of age. In this process, the muscle strength and the response of muscles around the hip joint are reduced, which is unable to effectively offset the harmful stress. This phenomenon also explains that when the hip joint is subjected to the external stress, fractures can be caused without obvious trauma. Thus, active anti-osteoporosis treatment and several kinds of effective measures to prevent the tumble, such as wearing anti-skid shoes, strengthening physical exercise and avoiding water on the ground, are the key to prevent the hip fractures in the elderly.
In addition to the factors of age and osteoporosis, race (mainly non-Hispanic white), smoking, drinking alcohol, living alone, and combined with diabetes are also vital risk factors of the elderly with hip fractures. Therein, common risk factors, such as age, gender, smoking, drinking alcohol, and osteoporosis, are basically consistent with the current international hip fracture assessment tools (such as the FRAX, Garvan Fracture Risk Calculator, and Qfracture) or the factors contained.21,22 However, this current study has observed that the risk factors of race and living alone are also the significant risk factors for the geriatric hip fractures. Compared with other races included in the NHANES database, the non-Hispanic white exhibits a higher incidence of hip fractures in the elderly (75.6%, P<0.001), which may be associated with the factors such as the specific race genes, dietary characteristics, and lifestyle habits. Furthermore, similar to the previous reports by Shen et al23 and Ward and Klesges,24 smoking (χ2=36.914, P<0.001) is another significant risk factor for elderly with hip fractures. According to a previous study performed by Marques et al,25 smoking can promote the occurrence of fractures by affecting the bone mineral density, and the influence of smoking on the risk of fractures is dose-dependent. When the smoking index reaches more than 200 cigarettes per year, the incidence of fractures is significantly increased.26 Meanwhile, in a large-scale cohort study, Gerdhem and Obrant27 also found that the risk of hip fractures in the elderly can be significantly reduced after 10-years of smoking cessation. Similarly, drinking alcohol (χ2=8.292, P=0.004) can also trigger the elderly towards hip fractures by affecting the bone mineral density. A previous study performed by Kim et al28 revealed that the bone mineral density of the femur and lumbar vertebrae will decrease in varying degrees in individuals who drink 40–100 g per day and have a history of drinking alcohol for more than 3 years. Hence, this study further reveals the significance of standardized smoking and alcohol cessation for the prevention of hip fractures in the elderly.
Interestingly, we have also unexpectedly observed that living alone is a vital risk factor of the elderly with hip fractures in this current study. In multivariate analysis, the factor of living alone (including the widowed, divorced, separated, and never married) showed asignificant statistical difference (OR=0.458, 95% CI=0.300–0.700, P<0.001), which may be related to the fact that this type of individual is mostly living alone. Due to the lack of care from their spouse and children, hip fractures are frequent in these individuals, which needs more attention from the medical and healthcare personnel, so as to strengthen the regular prevention and education of this group of individuals.
As a common concomitant disease in the elderly with hip fractures, diabetes has also been reported as a common risk factor in previous studies.29,30 However, in this study, the elderly with diabetes in the hip fracture group (21.3%) were similar to the non-hip fracture group (21.8%) and showed no significant difference in the univariate analysis (P=0.892). However, after the inclusion of multivariate analysis, there was a significant statistical difference (OR=1.636, 95% CI=1.081–2.475, P=0.020). This result may be related to the data loss of partial individuals in the NHANES database, which needs to be further included, analyzed, and verified in the future. However, it is certain that previous studies have indicated that glucose metabolites can affect the activity and function of the osteoblasts and osteoclasts,31,32 and the degradation and reconstruction of the bone matrix will also increase the bone fragility. Moreover, diabetes-related complications will also affect the activity and balance ability of individuals, thereby increasing the risk of tumble.33 Hence, it is still essential to pay attention to the risk factors of diabetes and its related complications in the elderly.
Currently, the research conclusions regarding the relationship between hip fracture and cardiovascular disease in the elderly are not consistent. Bagger et al34 suggested that elderly females with cardiovascular diseases have an increased risk of hip fracture. However, Sinnott et al35 pointed out that osteoporosis and atherosclerosis were two independent processes in postmenopausal females. In addition to cardiovascular diseases, the elderly individuals were often accompanied with various kinds of chronic diseases, which jointly affect the physical and mental health and result in the decreased motor function and increased risk of tumble. In this current study, the result shows that the hip fracture group with hypertension (61.6%) is similar to the non-hip fracture group (62.2%), and there is no significant statistical significance in the univariate or multivariate analysis. However, it is still necessary for us to recognize that the incidence of hip fractures in the elderly may be related to dizziness caused by hypertension and increased risk of tumble due to cardiovascular and cerebrovascular diseases.36,37
Ultimately, it is still essential to recognize and point out certain shortcomings in this current study. On one hand, this study is restricted by the self-reported nature of partial variables, such as history and factors of hip fractures and medication history of the prednisone or cortisone, and the inevitable report bias and recall bias might exist in this process. Despite this restriction, the overall data collection procedures in the NHANES database are reliable, and have been well validated for capturing accurate individuals sampling on which to ascertain the prevalence estimates. On the other hand, the sample size with reported hip fractures was relatively small, and only 127 individuals aged 65 years and older were ultimately included in the final analysis, which needs to include more years and a larger sample size for further analysis and validation in the future. In addition, limited by the updating mode of population information in NHANES database, the next cycle of geriatric hip fracture cases/controls will be planned to be conducted after the data in the NHANES database is completely updated in the future.
Conclusions
To sum up, based on the data extracted from the existing NHANES database from 2005 to 2010, the prevalence of hip fractures in the elderly is generally on the rise, and females occupy a higher proportion. Moreover, tumbling is the primary factor of hip fractures in elderly, and five is the highest number of occurrences among the included individuals. Compared with the non-hip fracture group, the hip fracture group in the elderly revealed a higher age characteristic, especially for the individuals aged 80 years and older. In addition to the common risk factors related to hip fractures in elderly (age, smoking, drinking alcohol, combined with diabetes and osteoporosis), race (mainly the Non-Hispanic white) and living alone are also significant risk factors for hip fractures in elderly, although these variables still need to be verified in further prospective investigations.
Ethical Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. The NHANES database used in this study did not contain identifiable nor protected the health information and is publicly available for download. Moreover, this is an exempt study due to the fact that the current study only involved secondary data analysis of the existing NHANES database, which is publicly available and has been de-identified, thus there is no need to apply an IRB approval from our own institution.
Funding
This work was supported by the “Summit of the Six Top Talents” Program of Jiangsu Province (2013-WSW-054); Jiangsu Provincial Medical Talent, The Project of Invigorating Health Care through Science, Technology and Education (ZDRCA2016083); The Six Projects Sponsoring Talent Summits of Jiangsu Province (LGY2017099).
Disclosure
The authors have no conflict of interest to disclose in relation to this article.
References
1. González-Quevedo D, Bautista-Enrique D, Pérez-Del-Río V, et al. Fracture liaison service and mortality in elderly hip fracture patients: a prospective cohort study. Osteoporos Int. 2020;31(1):77–84. doi:10.1007/s00198-019-05153-w
2. Loggers SAI, Van Lieshout EMM, Joosse P, et al. Prognosis of nonoperative treatment in elderly patients with a hip fracture: a systematic review and meta-analysis. Injury. 2020;51:2407–2413. doi:10.1016/j.injury.2020.08.027
3. Shimodan S, Sato D, Takahashi K, et al. Ten years change in post-fracture care for hip fracture patients. J Bone Miner Metab. 2020;38:222–229. doi:10.1007/s00774-019-01047-3
4. Barzilay JI, Buzkova P, Cauley JA, et al. The associations of subclinical atherosclerotic cardiovascular disease with hip fracture risk and bone mineral density in elderly adults. Osteoporos Int. 2018;29:2219–2230. doi:10.1007/s00198-018-4611-9
5. Tamaki J, Fujimori K, Ikehara S, et al. Estimates of hip fracture incidence in Japan using the National Health Insurance Claim Database in 2012-2015. Osteoporos Int. 2019;30:975–983. doi:10.1007/s00198-019-04844-8
6. Wei J, Zeng L, Li S, et al. Relationship between comorbidities and treatment decision-making in elderly hip fracture patients. Aging Clin Exp Res. 2019;31:1735–1741. doi:10.1007/s40520-019-01134-5
7. Chehade MJ, Carbone T, Awwad D, et al. Influence of fracture stability on early patient mortality and reoperation after pertrochanteric and intertrochanteric hip fractures. J Orthop Trauma. 2015;29:538–543. doi:10.1097/bot.0000000000000359
8. Pitto RP. The mortality and social prognosis of hip fractures. A prospective multifactorial study. Int Orthop. 1994;18:109–113. doi:10.1007/bf02484420
9. Buecking B, Struewer J, Waldermann A, et al. What determines health-related quality of life in hip fracture patients at the end of acute care?–a prospective observational study. Osteoporos Int. 2014;25:475–484. doi:10.1007/s00198-013-2415-5
10. Feskanich D, Meyer HE, Fung TT, et al. Milk and other dairy foods and risk of hip fracture in men and women. Osteoporos Int. 2018;29(2):385–396. doi:10.1007/s00198-017-4285-8
11. Yan L, Zhou B, Prentice A, Wang, X, Golden, M.H.N., et al. Epidemiological study of hip fracture in Shenyang, People’s Republic of China. Bone. 1999;24(2):151–155. doi:10.1016/s8756-3282(98)00168-9
12. Law MR, Hackshaw AK. A meta-analysis of cigarette smoking, bone mineral density and risk of hip fracture: recognition of a major effect. BMJ. 1997;315(7112):841–846. doi:10.1136/bmj.315.7112.841
13. Grisso JA, Kelsey JL, O’Brien LA, et al. Risk factors for hip fracture in men. Hip Fracture Study Group. Am J Epidemiol. 1997;145:786–793. doi:10.1093/oxfordjournals.aje.a009171
14. Cauley JA, Cawthon PM, Peters KE, et al. Risk factors for hip fracture in older men: the osteoporotic fractures in Men Study (MrOS). J Bone Miner Res. 2016;31:1810–1819. doi:10.1002/jbmr.2836
15. Høidrup S, Prescott E, Sørensen TI, et al. Tobacco smoking and risk of hip fracture in men and women. Int J Epidemiol. 2000;29:253–259. doi:10.1093/ije/29.2.253
16. Roy A, Heckman MG, O’Connor MI. Optimizing screening for osteoporosis in patients with fragility hip fracture. Clin Orthop Relat Res. 2011;469:1925–1930. doi:10.1007/s11999-011-1839-5
17. Tran T, Bliuc D, Pham HM, et al. A risk assessment tool for predicting fragility fractures and mortality in the elderly. J Bone Miner Res. 2020. doi:10.1002/jbmr.4100
18. Balasubramanian A, Zhang J, Chen L, et al. Risk of subsequent fracture after prior fracture among older women. Osteoporos Int. 2019;30:79–92. doi:10.1007/s00198-018-4732-1
19. Brauer CA, Coca-Perraillon M, Cutler DM, et al. Incidence and mortality of hip fractures in the United States. JAMA. 2009;302:1573–1579. doi:10.1001/jama.2009.1462
20. Dontas IA, Yiannakopoulos CK. Risk factors and prevention of osteoporosis-related fractures. J Musculoskelet Neuronal Interact. 2007;7:268–272.
21. Inderjeeth CA, Raymond WD. Case finding with GARVAN fracture risk calculator in primary prevention of fragility fractures in older people. Arch Gerontol Geriatr. 2020;86:103940. doi:10.1016/j.archger.2019.103940
22. Kanis JA, Harvey NC, Johansson H, et al. A decade of FRAX: how has it changed the management of osteoporosis? Aging Clin Exp Res. 2020;32:187–196. doi:10.1007/s40520-019-01432-y
23. Shen GS, Li Y, Zhao G, et al. Cigarette smoking and risk of hip fracture in women: a meta-analysis of prospective cohort studies. Injury. 2015;46:1333–1340. doi:10.1016/j.injury.2015.04.008
24. Ward KD, Klesges RC. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif Tissue Int. 2001;68:259–270. doi:10.1007/bf02390832
25. Marques EA, Elbejjani M, Gudnason V, et al. Cigarette smoking and hip volumetric bone mineral density and cortical volume loss in older adults: the AGES-Reykjavik study. Bone. 2018;108:186–192. doi:10.1016/j.bone.2018.01.014
26. Thorin MH, Wihlborg A, Åkesson K, et al. Smoking, smoking cessation, and fracture risk in elderly women followed for 10 years. Osteoporos Int. 2016;27:249–255. doi:10.1007/s00198-015-3290-z
27. Gerdhem P, Obrant KJ. Effects of cigarette-smoking on bone mass as assessed by dual-energy X-ray absorptiometry and ultrasound. Osteoporos Int. 2002;13:932–936. doi:10.1007/s001980200130
28. Kim MJ, Shim MS, Kim MK, et al. Effect of chronic alcohol ingestion on bone mineral density in males without liver cirrhosis. Korean J Intern Med. 2003;18:174–180. doi:10.3904/kjim.2003.18.3.174
29. Tebé C, Martínez-Laguna D, Carbonell-Abella C, et al. The association between type 2 diabetes mellitus, hip fracture, and post-hip fracture mortality: a multi-state cohort analysis. Osteoporos Int. 2019;30:2407–2415. doi:10.1007/s00198-019-05122-3
30. Huang HL, Pan CC, Hsiao YF, et al. Associations of body mass index and diabetes with hip fracture risk: a nationwide cohort study. BMC Public Health. 2018;18:1325. doi:10.1186/s12889-018-6230-y
31. Miazgowski T, Pynka S, Noworyta-Zietara M, et al. Bone mineral density and hip structural analysis in type 1 diabetic men. Eur J Endocrinol. 2007;156:123–127. doi:10.1530/eje.1.02309
32. Strotmeyer ES, Cauley JA, Orchard TJ, et al. Middle-aged premenopausal women with type 1 diabetes have lower bone mineral density and calcaneal quantitative ultrasound than nondiabetic women. Diabetes Care. 2006;29:306–311. doi:10.2337/diacare.29.02.06.dc05-1353
33. Kim SH, Kim YM, Yoo JS, et al. Increased risk of hip fractures in Korean patients with type 2 diabetes: a 6-year nationwide population-based study. J Bone Miner Metab. 2017;35:623–629. doi:10.1007/s00774-016-0798-z
34. Bagger YZ, Tankó LB, Alexandersen P, et al. Radiographic measure of aorta calcification is a site-specific predictor of bone loss and fracture risk at the hip. J Intern Med. 2006;259:598–605. doi:10.1111/j.1365-2796.2006.01640.x
35. Sinnott B, Syed I, Sevrukov A, et al. Coronary calcification and osteoporosis in men and postmenopausal women are independent processes associated with aging. Calcif Tissue Int. 2006;78:195–202. doi:10.1007/s00223-005-0244-z
36. Lee KH, Kim JY, Yim SJ, et al. Incidence and risk factors of subsequent hip fractures in Korea: multicenter study. J Korean Med Sci. 2014;29:992–994. doi:10.3346/jkms.2014.29.7.992
37. Liu S, Zhu Y, Chen W, et al. Risk factors for the second contralateral hip fracture in elderly patients: a systematic review and meta-analysis. Clin Rehabil. 2015;29:285–294. doi:10.1177/0269215514542358
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.