")
Back to Journals » Journal of Pain Research » Volume 13
Prevalence and Severity of Dermatological Condition-Associated Skin Pain in the Chinese
Authors Wang X, Lai Q, Zheng B, Ye L, Wen S, Yan Y, Yang B , Man MQ
Received 28 January 2020
Accepted for publication 7 May 2020
Published 26 May 2020 Volume 2020:13 Pages 1201—1207
DOI https://doi.org/10.2147/JPR.S245514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Xiaohua Wang,1,* Qingsong Lai,2,* Baoqing Zheng,1 Li Ye,1 Si Wen,1 Yunling Yan,1 Bin Yang,1 Mao-Qiang Man1
1Dermatology Hospital, Southern Medical University, Guangdong 510095, People’s Republic of China; 2Puning City Chronic Disease Prevention and Control Center, Guangdong 515300, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mao-Qiang Man; Bin Yang Email [email protected]; [email protected]
Background/Aim: Although the characteristics of cutaneous sensory symptoms in the general population have been documented, dermatological condition-associated skin pain has not been characterized yet. In the present study, we aimed to characterize dermatological condition-associated skin pain in the Chinese.
Subjects and Methods: A questionnaire was given to outpatients to identify self-proclaimed skin pain at our dermatology clinic. The severity of skin pain was assessed using pain scale 0– 10. Prevalence and pain severity were compared between males and females.
Results: A total of 2144 patients, including 1254 females and 890 males aged 13– 94 years, were included in this study. The overall prevalence of skin pain was 9.93% in this cohort. The prevalence of skin pain varied greatly with dermatological conditions (p< 0.0001). Moreover, a higher prevalence of skin pain was observed in males than in females (p< 0.05). Among the dermatological conditions reported, higher skin pain scales were found in subjects with either glucocorticoid-induced dermatitis (4.20 ± 0.73) or herpes zoster (4.00 ± 0.29). While the overall pain scales were comparable between males and females (2.38 ± 0.13 versus 2.68 ± 0.13), pain scales in patients with eczematous dermatitis were higher in females than in males (p< 0.05). Furthermore, pain scales correlated positively with age. However, pain scales did not differ between subjects with versus without a family history of cutaneous sensory symptoms. These results demonstrate that the prevalence and severity of dermatological condition-associated skin pain vary with dermatological conditions and gender in the Chinese.
Conclusion: Patients with some dermatological conditions may experience skin pain. Although the pain is moderate, it can negatively impact the quality of patients’ lives. Alleviation of skin pain should be considered when treating patients with certain dermatological conditions.
Keywords: skin disorders, skin pain, gender, prevalence
Introduction
Subjects with dermatological conditions can experience skin pain. Prior studies have shown that 20% of patients with skin sensory symptoms display characteristics of neuropathic pain1 and that over 40% of psoriatic patients also suffer from skin pain.2–4 Likewise, a substantial number of patients with atopic dermatitis experience skin pain with a pain intensity score as high as >7, evaluated using a pain scale 0 to 10.5,6 Vakharia et al7 reported that 14% of patients with atopic dermatitis had severe or very severe skin pain. Patients with rosacea displayed an overall reduction in heat pain sensitivity by 10% in comparison to those without rosacea or under normal healthy skin conditions.8 Moreover, involved area of rosacea displayed an over 10% reduction in heat pain threshold in comparison to either uninvolved areas or normal healthy controls.8 These patients can experience skin pain upon exposure to heat. Furthermore, over 30% of patients with hidradenitis suppurativa proclaimed skin pain.9 Although evidence indicates that the prevalence of some dermatological condition-associated skin pain is high, reports are sporadic. In addition, characteristics of dermatological condition-associated skin pain in most dermatological conditions are still poorly understood. In the present study, we characterize skin pain in a large cohort of Chinese patients with a variety of dermatological conditions.
Materials and Methods
Study Subjects
All participants were diagnosed with skin disorder(s) at an outpatient clinic at the Dermatology Hospital, a tertiary hospital located in Guangzhou city, Guangdong province, China. A questionnaire (Supplemental Table 1) was given to participants who visited the clinic to self-report skin pain. Participants also scored the severity of skin pain scale 0 to 10. A designated nurse collected the questionnaire upon its completion onsite. This work was approved by the institutional review board of the Dermatology Hospital of Southern Medical University, and carried out in accordance with the Declaration of Helsinki. Written informed consent was obtained from either participants or participants’ parent if participants were under age of 18 years. This study was conducted between March and May.
Data Analysis
Common skin disorders were individually analyzed. Subjects with either multiple skin disorders or a skin disorder which was found in <10 patients were pooled together as “others”. GraphPad Prism 5 software was used for all statistical analyses. Chi-square test or unpaired t-test was used to determine significance. Data are expressed as either mean ± SEM or %.
Results
A total of 2144 subjects, including 890 males and 1254 females aged 13–94 years, were included in the analyses. The ages of males and females were comparable. Only 8% of subjects considered their skin to be dry skin, while a larger portion (69%) of subjects considered their skin to be normal. More males than females reported oily skin (28% vs 20%, p<0.0001), whereas more females than males exhibited normal skin type (71% vs 65%, p=0.0007). The majority of these subjects (93%) declared no family history of cutaneous sensory symptoms. The demographic characteristics of the participants are detailed in Table 1.
 |
Table 1 Demographic Characteristics of Subjects |
Prevalence of Skin Pain Varies with Skin Disorders and Gender
We first analyzed whether the prevalence of self-reported skin pain varies with dermatological disorders. As seen in Table 2, prevalence of skin pain varied greatly with skin disorders in both males and females (Chi-square=63.40 for males and Chi-square=94.06 for females, p<0.0001 for both males and females). The overall prevalence of skin pain in this cohort was 9.93%. A higher prevalence was observed in males than in females (11.69% versus 8.69%, p<0.05). Moreover, the prevalence of skin pain did not differ significantly among dry, oily, and normal skin (Chi-square=5.448, p=0.0656). Taken together, these results indicate that the prevalence of skin pain varies with dermatological condition and gender.
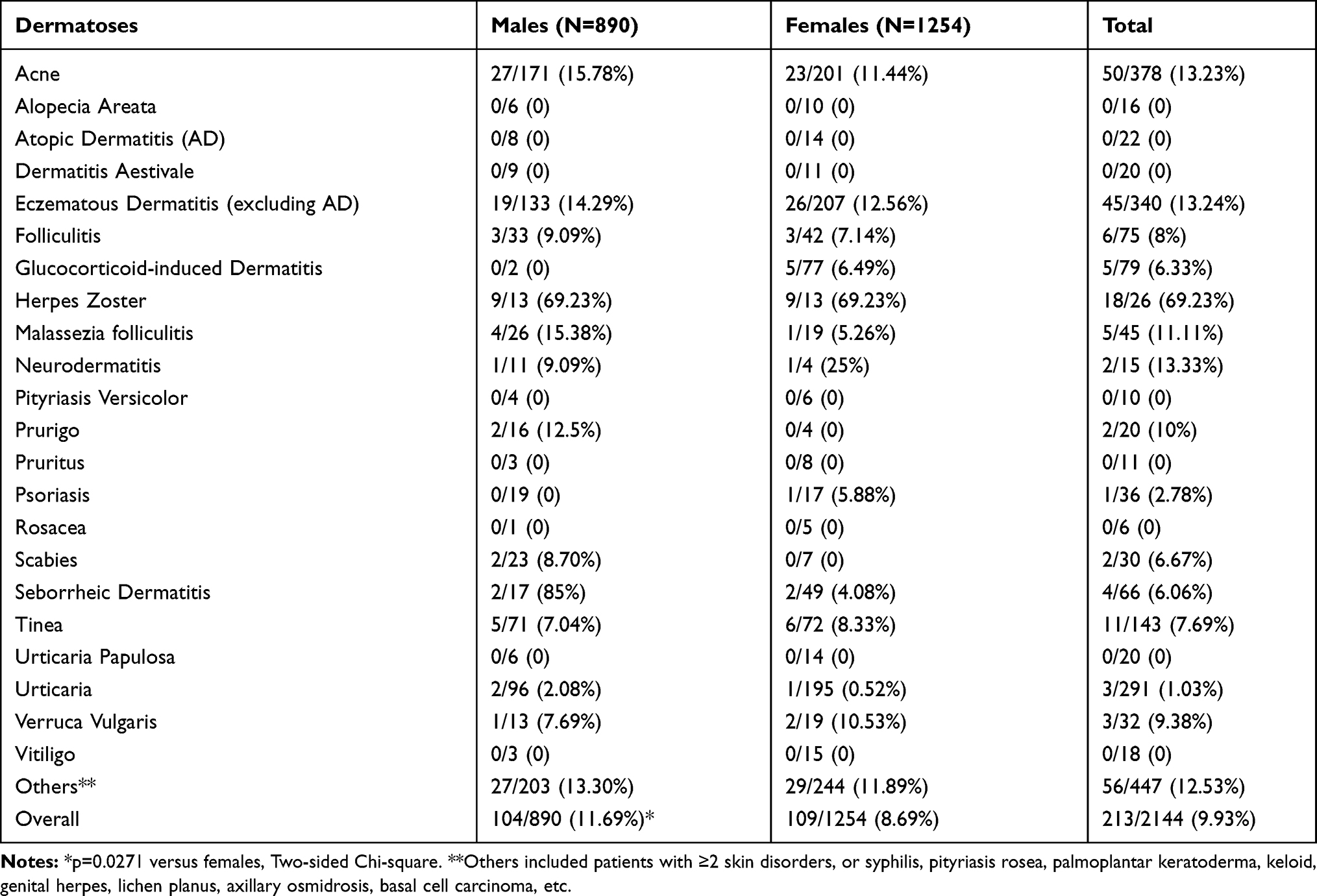 |
Table 2 Prevalence of Skin Pain in Males and Females (Mean ± SEM) |
Association of the Severity of Skin Pain with Skin Disorders
We next analyzed the severity of skin pain in skin disorders. The overall pain scales in the entire cohort were 2.53 ± 0.09 (95% CI 2.349–2.712). Males and females displayed comparable overall pain scales (2.38 ± 0.13, 95% CI 2.119–2.631 versus 2.68 ± 0.13, 95% CI 2.421–2.937). However, pain scales in patients with eczematous dermatitis were higher in females than in males (p<0.05) (Table 3). A higher pain scale was found in subjects with either Glucocorticoid-induced Dermatitis (pain scale=4.20 ± 0.73, 95% CI 2.160–6.240) or herpes zoster (pain scale=4.00 ± 0.29, 95% CI 3.385–4.615). However, pain scales were no differences between subjects with and without a family history of cutaneous sensory symptoms (2.74 ± 0.32 versus 2.51 ± 0.10, 95% CI −0.4567 to 0.9244). Interestingly, pain scales positively correlated with age (Pearson r=0.1714, p=0.0122). Collectively, these results demonstrate that severity of skin pain varies with dermatological condition and age.
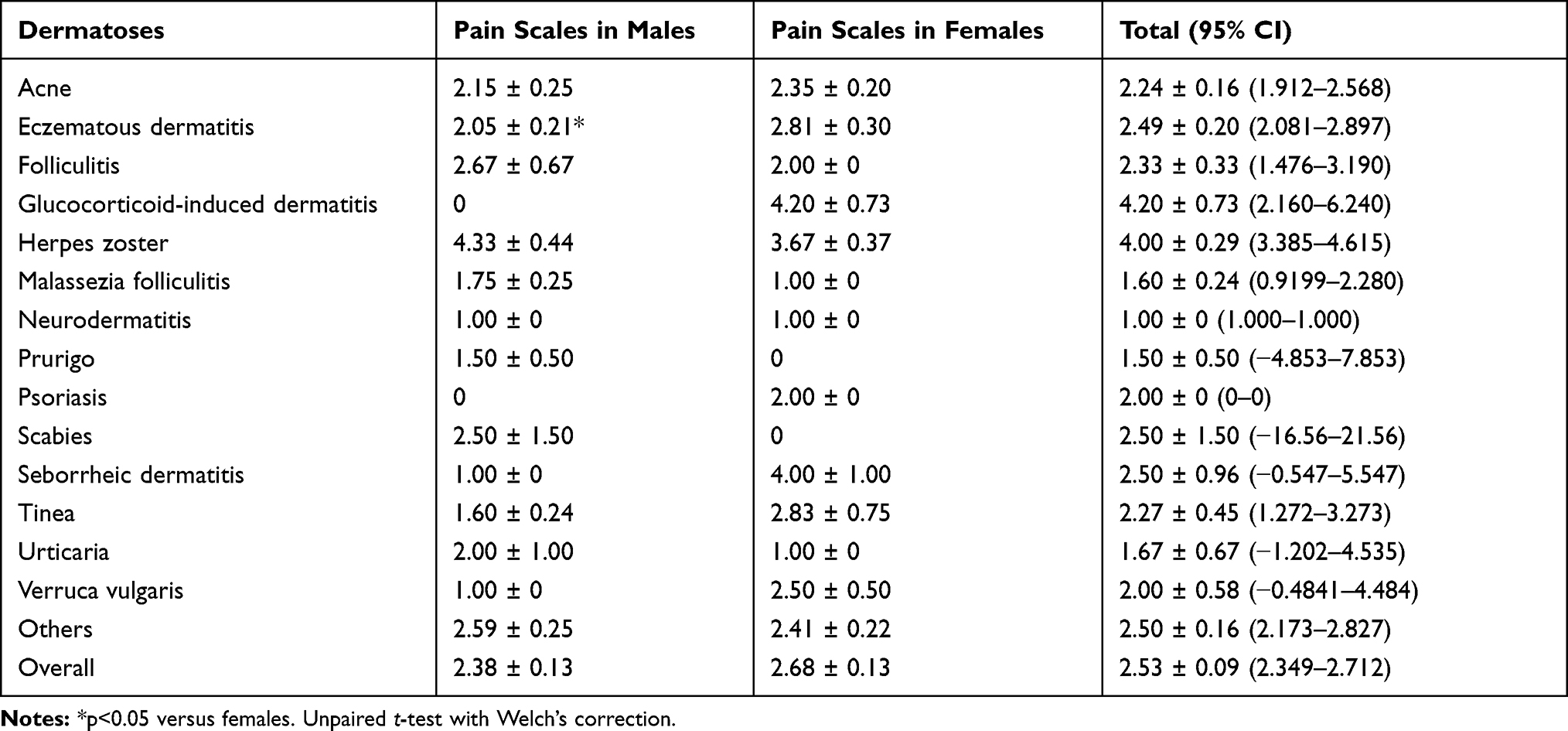 |
Table 3 Pain Scales in Males and Females (Mean ± SEM) |
Discussion
Previous studies have shown that subjects with certain dermatological conditions, including psoriasis, atopic dermatitis and sensitive skin, experience skin pain.1–8 The present study shows that a variety of other dermatological conditions are associated with skin pain, with an overall prevalence of 10%. Besides herpes zoster, which exhibits neuralgia because of damage to the nerve, a higher prevalence of skin pain was found in subjects with inflammatory dermatoses, such as acne and eczematous dermatitis. The underlying mechanism that causes skin pain in dermatological conditions can be attributed to increased cytokines in the skin, primarily in the upper dermis.10 Both eczematous dermatitis and acne display elevated levels of pro-inflammatory cytokines in the skin.11,12 It is well known that the activation of the receptors in the primary afferent fibers is required for the sensation of pain. There are two types of afferent fibers in the skin, ie, unmyelinated C-fiber and myelinated Aσ-fiber, which nociceptors can be activated by noxious stimuli.13 Previous studies have demonstrated that TNFα can activate cAMP-dependent protein kinase and nociceptive neurons, resulting in a sensation of pain.14,15 Moreover, TNFα can reduce the threshold of C fibers, resulting in an increased sensitivity to stimuli.16 Other cytokines, such IL-1β, IL-6 and IL-13, also play an important pathogenic role in the development of pain.16 Furthermore, inflammatory skin disorders, such as acne, eczema, and psoriasis, are often accompanied by an increase in mast cells.17–19 Mast cells can release algogenic substances, such as substance P and histamine, which can activate pruriceptors and nociceptors, leading to the transmission of nerve impulses by both unmyelinated C-fiber and myelinated Aσ-fiber to the brain, where itch and pain sensation are generated.18 Additionally, tryptase and SP released by mast cells can activate nociceptors on the nerve endings, resulting in the release of neuropeptides, and consequently leading to neurogenic inflammation and neurogenic pain.20 Hence, subjects with inflammatory dermatoses display higher prevalence of skin pain.
In contrast to previous studies, it is worth noting that in the present study, a high prevalence of skin pain was not found in patients with either psoriasis or atopic dermatitis.2–6 These discrepant results may be due to the differences in ethnicities and the environment, both of which can influence skin sensitivity.21–23 Our study was carried out between March and May, during which the average atmospheric humidity and temperature were 83% and 21°C, respectively. Generally, psoriasis remits under environmental conditions of high humidity and/or exposure to high dose of UV irradiation.24,25 Thus, the prevalence of skin pain associated with psoriasis and atopic dermatitis was lower in the present study. Moreover, the limited number of subjects (N=36 for psoriasis and N=22 for atopic dermatitis) in the present study can also render difficult to draw a solid conclusion of the prevalence of skin pain in these dermatological conditions. Further study in a larger cohort is required to determine the prevalence of skin pain in these dermatological conditions.
Interestingly, in contrast to inflammatory skin disorders, which exhibit both inflammatory pain and itch primarily mediated by cytokines, some dermatological conditions with neural itch, such as cholestatic pruritus, display itch and analgesia via activation of G-protein-coupled bile acid receptor (TGR5). These proteins are expressed on the small diameter neurons of the dorsal root ganglia that transmit both itch and pain signals from the skin.26 Activation of TGR5 with its ligand can induce itch and analgesia in mice.27 In addition to the stimuli and mediators at the skin site, the neurons in the spinal cord also determine the sensation of itch and pain. In the laminae I and II of the spinal cord, there are excitatory interneurons expressing gastrin releasing peptide receptor (GRPR neurons), which can receive inputs from both Aδ and C fibers.28 These GRPR neurons only transmit itch signals, but not pain signals.29 For example, mice with GRPR deficiency display less itching in comparison to the wild type mice.30 By contrast, pain can inhibit GRPR neurons, resulting in a reduction in itch sensation.28 Collectively, the pathogenesis of skin pain is complex, and varies with dermatological conditions.
In addition to well-known skin pain in herpes zoster, the present study also revealed various degrees of skin pain in other dermatoses, with an overall pain scale of 2.5. Although the pain is moderate, it can negatively impact the quality of patients’ lives.31 Because skin pain is associated with disease severity, alleviation of skin disorders could relieve pain,32 leading to the improvement in the quality of patients’ lives. Thus, appropriate treatments of these skin disorders can alleviate skin pain. Among the different types of medication, glucocorticoids are the most commonly used in the treatments of inflammatory skin disorders, but it should be aware that glucocorticoids can cause skin pain, too. Studies have shown that either topical or systemic administrations of glucocorticoids can cause severe damage to epidermal function, including reductions in antimicrobial peptides and defective permeability barrier homeostasis, although glucocorticoids can also effectively inhibit cutaneous inflammation.33,34 Compromised epidermal function predisposes to the development of infections and penetrations of substances into the skin. Hence, glucocorticoids should not be used for the long term. In contrast, safe emollients can benefit dermatological condition-associated skin pain because emollients can inhibit and prevent cutaneous inflammation, possibly via improvements in stratum corneum hydration and permeability barrier.35–37 Moreover, some dermatological conditions, such as eczematous dermatitis and acne, display defective permeability barrier while compromised permeability barrier is linked to skin pain,38 further suggesting the potential benefit of topical emollients for skin pain associated with, at least some, dermatological conditions. Finally, topical emollients can improve skin sensitivity. A considerable number of subjects with some dermatological conditions, including acne, psoriasis, and eczematous dermatitis, display sensitive skin,39,40 which is possibly caused by small nerve fiber neuropathy.41 Therefore, topical emollient could be a valuable regimen in the management of skin pain associated with some dermatological conditions. However, emollients can also induce adverse cutaneous reactions, including irritant and allergic reactions,42,43 which is possibly attributable to some of the ingredients in emollients, especially at a high concentration. For example, Jojoba oil, which contains eicosadienoic acid, can increase the production of prostaglandin E2 and tumor necrotic factor-α, which both are pro-inflammatory mediators.44 Similarly, stearic acid, ceteareth 20, PEG-40 castor oil, and PEG-100 stearate can also induce inflammation.45,46 Inflammation is linked to skin pain associated with some dermatological conditions. Thus, product safety should be considered when choosing emollients.
Conclusions
Although the present study did not compare the skin pain between dermatosis-free normal subjects and subjects with skin disorders, it clearly demonstrates that both the prevalence and severity of skin pain vary with gender and dermatological conditions in the Chinese. Though dermatosis-associated skin pain is moderate, it can negatively impact the quality of patients’ lives. Management of skin pain should be considered in the treatments of subjects with skin disorders.
Data Sharing Statement
Data are available upon request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Saint-Martory C, Sibaud V, Theunis J, et al. Arguments for neuropathic pain in sensitive skin. Br J Dermatol. 2015;172(4):1120–1121. doi:10.1111/bjd.13466
2. Patruno C, Napolitano M, Balato N, et al. Psoriasis and skin pain: instrumental and biological evaluations. Acta Derm Venereol. 2015;95(4):432–438. doi:10.2340/00015555-1965
3. Ljosaa TM, Rustoen T, Mörk C, et al. Skin pain and discomfort in psoriasis: an exploratory study of symptom prevalence and characteristics. Acta Derm Venereol. 2010;90(1):39–45. doi:10.2340/00015555-0764
4. Sampogna F, Gisondi P, Melchi CF, et al. Prevalence of symptoms experienced by patients with different clinical types of psoriasis. Br J Dermatol. 2004;151(3):594–599. doi:10.1111/j.1365-2133.2004.06093.x
5. Silverberg JI, Gelfand JM, Margolis DJ, et al. Pain is a common and burdensome symptom of atopic dermatitis in United States adults. J Allergy Clin Immunol Pract. 2019;7(8):2699–2706.e7. doi:10.1016/j.jaip.2019.05.055
6. Newton L, DeLozier AM, Griffiths PC, et al. Exploring content and psychometric validity of newly developed assessment tools for itch and skin pain in atopic dermatitis. J Patient Rep Outcomes. 2019;3(1):42. doi:10.1186/s41687-019-0128-z
7. Vakharia PP, Chopra R, Sacotte R, et al. Burden of skin pain in atopic dermatitis. Ann Allergy Asthma Immunol. 2017;119(6):548–552.e3. doi:10.1016/j.anai.2017.09.076
8. Guzman-Sanchez DA, Ishiuji Y, Patel T, Fountain J, Chan YH, Yosipovitch G. Enhanced skin blood flow and sensitivity to noxious heat stimuli in papulopustular rosacea. J Am Acad Dermatol. 2007;57(5):800–805. doi:10.1016/j.jaad.2007.06.009
9. Huilaja L, Hirvonen MJ, Lipitsä T, et al. Patients with hidradenitis suppurativa may suffer from neuropathic pain: a Finnish multicenter study. J Am Acad Dermatol. 2019;pii(Nov 12):
10. Misery L, Brenaut E, Le Garrec R, et al. Neuropathic pruritus. Nat Rev Neurol. 2014;10(7):408–416. doi:10.1038/nrneurol.2014.99
11. Tanghetti EA. The role of inflammation in the pathology of acne. J Clin Aesthet Dermatol. 2013;6(9):27–35.
12. Kerstan A, Leverkus M, Trautmann A. Effector pathways during eczematous dermatitis: where inflammation meets cell death. Exp Dermatol. 2009;18(10):893–899. doi:10.1111/j.1600-0625.2009.00919.x
13. Yam MF, Loh YC, Tan CS, Khadijah Adam S, Abdul Manan N, Basir R. General pathways of pain sensation and the major neurotransmitters involved in pain regulation. Int J Mol Sci. 2018;19(8):2164. doi:10.3390/ijms19082164
14. Zhang J-M, Li HQ, Liu B, Brull SJ. Acute topical application of tumor necrosis factor alpha evokes protein kinase A-dependent responses in rat sensory neurons. J Neurophysiol. 2002;88(3):1387–1392. doi:10.1152/jn.2002.88.3.1387
15. Sorkin LS, Xiao WH, Wagner R, Myers RR. Tumour necrosis factor-alpha induces ectopic activity in nociceptive primary afferent fibres. Neuroscience. 1997;81(1):255–262. doi:10.1016/S0306-4522(97)00147-4
16. de Oliveira CM, Sakata RK, Issy AM, Gerola LR, Salomão R. Cytokines and pain. Rev Bras Anestesiol. 2011;61(2):260–265. doi:10.1016/S0034-7094(11)70029-0
17. Toyoda M, Morohashi M. New aspects in acne inflammation. Dermatology. 2003;206(1):17–23. doi:10.1159/000067818
18. Kawakami T, Ando T, Kimura M, Wilson BS, Kawakami Y. Mast cells in atopic dermatitis. Curr Opin Immunol. 2009;21(6):666–678. doi:10.1016/j.coi.2009.09.006
19. Harvima IT, Nilsson G, Suttle MM, Naukkarinen A. Is there a role for mast cells in psoriasis? Arch Dermatol Res. 2008;300(9):461–478. doi:10.1007/s00403-008-0874-x
20. Gupta K, Harvima IT. Mast cell-neural interactions contribute to pain and itch. Immunol Rev. 2018;282(1):168–187. doi:10.1111/imr.12622
21. Lee E, Kim S, Lee J, Cho SA, Shin K. Ethnic differences in objective and subjective skin irritation response: an international study. Skin Res Technol. 2014;20(3):265–269. doi:10.1111/srt.12111
22. Jourdain R, de Lacharrière O, Bastien P, Maibach HI. Ethnic variations in self-perceived sensitive skin: epidemiological survey. Contact Dermatitis. 2002;46(3):162–169. doi:10.1034/j.1600-0536.2002.460307.x
23. Misery L, Sibaud V, Merial-Kieny C, Taieb C. Sensitive skin in the American population: prevalence, clinical data, and role of the dermatologist. Int J Dermatol. 2011;50(8):961–967. doi:10.1111/j.1365-4632.2011.04884.x
24. Søyland E, Heier I, Rodríguez-Gallego C, et al. Sun exposure induces rapid immunological changes in skin and peripheral blood in patients with psoriasis. Br J Dermatol. 2011;164(2):344–355. doi:10.1111/j.1365-2133.2010.10149.x
25. Balato N, Di Costanzo L, Patruno C, Patrì A, Ayala F. Effect of weather and environmental factors on the clinical course of psoriasis. Occup Environ Med. 2013;70(8):600. doi:10.1136/oemed-2013-101505
26. Alemi F, Kwon E, Poole DP, et al. The TGR5 receptor mediates bile acid-induced itch and analgesia. J Clin Invest. 2013;123(4):1513–1530. doi:10.1172/JCI64551
27. Dawson PA, Karpen SJ. Bile acids reach out to the spinal cord: new insights to the pathogenesis of itch and analgesia in cholestatic liver disease. Hepatology. 2014;59(4):1638–1641. doi:10.1002/hep.26786
28. Bardoni R, Shen KF, Li H, et al. Pain Inhibits GRPR Neurons via GABAergic Signaling in the Spinal Cord. Sci Rep. 2019;9(1):15804. doi:10.1038/s41598-019-52316-0
29. Albisetti GW, Pagani M, Platonova E, et al. Dorsal horn gastrin-releasing peptide expressing neurons transmit spinal itch but not pain signals. J Neurosci. 2019;39(12):2238–2250. doi:10.1523/JNEUROSCI.2559-18.2019
30. Swain MG. Gastrin-releasing peptide and pruritus: more than just scratching the surface. J Hepatol. 2008;48(4):681–683. doi:10.1016/j.jhep.2008.01.007
31. Ljosaa TM, Mork C, Stubhaug A, Moum T, Wahl AK. Skin pain and skin discomfort is associated with quality of life in patients with psoriasis. J Eur Acad Dermatol Venereol. 2012;26(1):29–35. doi:10.1111/j.1468-3083.2011.04000.x
32. Ljosaa TM, Stubhaug A, Mork C, Moum T, Wahl AK. Improvement in psoriasis area and severity index score predicts improvement in skin pain over time in patients with psoriasis. Acta Derm Venereol. 2013;93(3):330–334. doi:10.2340/00015555-1456
33. Man G, Mauro TM, Kim PL, et al. Topical hesperidin prevents glucocorticoid-induced abnormalities in epidermal barrier function in murine skin. Exp Dermatol. 2014;23(9):645–651. doi:10.1111/exd.12480
34. Kao JS, Fluhr JW, Man MQ, et al. Short-term glucocorticoid treatment compromises both permeability barrier homeostasis and stratum corneum integrity: inhibition of epidermal lipid synthesis accounts for functional abnormalities. J Invest Dermatol. 2003;120(3):456–464. doi:10.1046/j.1523-1747.2003.12053.x
35. Kikuchi K, Kobayashi H, Hirao T, Ito A, Takahashi H, Tagami H. Improvement of mild inflammatory changes of the facial skin induced by winter environment with daily applications of a moisturizing cream. A half-side test of biophysical skin parameters, cytokine expression pattern and the formation of cornified envelope. Dermatology. 2003;207(3):269–275. doi:10.1159/000073089
36. Man MQ, Ye L, Hu L, Jeong S, Elias PM, Lv C. Improvements in epidermal function prevent relapse of psoriasis: a self-controlled study. Clin Exp Dermatol. 2019;44(6):654–657. doi:10.1111/ced.13888
37. Hon KL, Kung JSC, Ng WGG, Leung TF. Emollient treatment of atopic dermatitis: latest evidence and clinical considerations. Drugs Context. 2018;7:212530. doi:10.7573/dic.212530
38. Seo SR, Lee SG, Lee HJ, Yoon MS, Kim DH. Disrupted skin barrier is associated with burning sensation after topical tacrolimus application in atopic dermatitis. Acta Derm Venereol. 2017;97(8):957–958. doi:10.2340/00015555-2699
39. Misery L, Weisshaar E, Brenaut E, et al. Pathophysiology and management of sensitive skin: position paper from the special interest group on sensitive skin of the International Forum for the Study of Itch (IFSI). J Eur Acad Dermatol Venereol. 2020;34(2):222–229. doi:10.1111/jdv.16000
40. Jeong S, Lee SH, Park BD, Wu Y, Man G, Man MQ. Comparison of the efficacy of Atopalm(®) multi-lamellar emulsion cream and Physiogel(®) intensive cream in improving epidermal permeability barrier in sensitive skin. Dermatol Ther. 2016;6(1):47–56. doi: 10.1007/s13555-016-0097-6.
41. Huet F, Dion A, Batardière A, et al. Sensitive skin can be small fibre neuropathy: results from a case-control quantitative sensory testing study. Br J Dermatol. 2018;179(5):1157–1162. doi:10.1111/bjd.17082
42. Liu D, Wen S, Huang LN, et al. Comparison of transepidermal water loss rates in subjects with skin patch test positive vs negative to skin care products. J Cosmet Dermatol. 2019. doi:10.1111/jocd.13264.
43. Huang LN, Zhong YP, Liu D, et al. Adverse cutaneous reactions to skin care products on the face vary with age, but not with sex. Contact Dermatitis. 2018;79(6):365–369. doi:10.1111/cod.13102
44. Huang YS, Huang WC, Li CW, Chuang LT. Eicosadienoic acid differentially modulates production of pro-inflammatory modulators in murine macrophages. Mol Cell Biochem. 2011;358(1–2):85–94. doi:10.1007/s11010-011-0924-0
45. Miao H, Chen L, Hao L, et al. Stearic acid induces proinflammatory cytokine production partly through activation of lactate-HIF1α pathway in chondrocytes. Sci Rep. 2015;5(1):13092. doi:10.1038/srep13092
46. Anderson EK, Hill AA, Hasty AH. Stearic acid accumulation in macrophages induces toll-like receptor 4/2-independent inflammation leading to endoplasmic reticulum stress-mediated apoptosis. Arterioscler Thromb Vasc Biol. 2012;32(7):1687–1695. doi:10.1161/ATVBAHA.112.250142
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.