")
Back to Journals » Cancer Management and Research » Volume 11
Prevalence and risk factors of anxiety and depression in Chinese patients with lung cancer: a cross-sectional study
Authors Yan X, Chen X, Li M , Zhang P
Received 18 January 2019
Accepted for publication 8 April 2019
Published 9 May 2019 Volume 2019:11 Pages 4347—4356
DOI https://doi.org/10.2147/CMAR.S202119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alexandra R. Fernandes
Xiaoru Yan,1,2,* Xun Chen,3,4,* Meng Li,1,3 Peitong Zhang1
1Department of Oncology, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 2Graduate School, Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 3Graduate School, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 4Department of Gastroenterology, Dongfang Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Background: Lung cancer is very common in China. The low cure rate, limited overall survival, and continuous therapies lead the patients to experience considerable psychological distress. Traditional Chinese medicine therapy is one unique treatment method in China. Nevertheless, most patients in the existing studies on anxiety and depression were treated in western medical hospitals. Therefore, it is necessary to identify the prevalence and risk factors of these emotional disorders in lung cancer patients treated in traditional Chinese medical hospitals. These findings may assist in clinical intervention.
Patients and methods: A total of 315 patients with lung cancer were enrolled. Individuals completed the Hospital Anxiety and Depression Scale to assess their levels of anxiety and depression. Demographic and clinical data were also collected. Binary logistic regression analysis was used to identify factors that significantly predicted anxiety and depression.
Results: The anxiety and depression prevalence rates of lung cancer patients were 43.5% and 57.1%, respectively. In the univariate analysis, patients without surgery, who were young, or who received radiotherapy were more likely to experience anxiety. Patients without surgery, who were young, or who had late-stage cancer, were more likely to experience depression. Binary logistic regression analysis showed that the risk factors of both anxiety and depression were lack of surgery and young and middle age (<65, especially 45–65 years).
Conclusion: Anxiety and depression were very common in lung cancer patients. Lack of surgery, young, and middle age, were independent risk factors for anxiety and depression. Therefore, medical workers should pay close attention to the emotional changes of young or middle-aged patients, or patients without the chance to undergo surgery.
Keywords: anxiety, depression, lung cancer, mental health
Introduction
Lung cancer is one of the most common cancer diagnoses, and one of the leading causes of cancer-related mortality in China. The 5-year prevalence of lung cancer in China was 130.2 per 100,000 according to the data released by the national cancer center in 2015.1 The lung cancer related mortality around the world is expected to grow to 3 million in 2035.2 Most patients with lung cancer often confront a limited life span and have to receive surgery, chemical radiotherapy, targeting, and other treatments. These treatments could lead to physical deformities, body dysfunction, and multiple side-effects. While receiving treatment, the high cost also greatly increases the pressure on patients.3 Because of the diagnosis and treatments, many lung cancer patients experience more considerable psychological distress than the general population, particularly anxious and depressive symptoms.4 Studies have shown that the incidence of depressive symptoms in patients with lung cancer was 12.4–65%,5–12 and anxious symptoms 20.9–65%.7–12
Cancer patients with depression and anxiety have a worse quality-of-life and longer hospital stay.9,13,14 Depressive symptoms are associated with poorer adherence to treatment,6 high death ideation,15 suicide,16 and short survival time. Moreover, they can also increase the mortality of non-small cell lung cancer17 and breast cancer.18 Given the harmful impacts of depression and anxiety on cancer patients, identifying the related risk factors is very meaningful.
Studies have revealed a variety of factors influencing the prevalence of depression or anxiety. For depression, the relevant factors were pain, gender, age, residence, education level, marital status, cancer type, pathological type, cancer stage, and personality characteristics.5,6,13,19,20 For anxiety, they were pain, gender, residence, smoking, cancer type, cancer stage, and family support.19–23 Considering that cancer type is an important influencing factor in the prevalence of depressive and anxious symptoms, it would be better if we enroll participants with one cancer type. In China, lung cancer is a very common cancer type. So we chose lung cancer patients as participants. As we all know, traditional Chinese medicine therapy is one unique treatment method in China. It is totally different from western medicine. However, current related studies have been mostly conducted in western medical hospitals. Therefore, the aim of our study was to assess the prevalence of depression and anxiety in lung cancer patients who were treated in a traditional Chinese medical hospital, and identify the risk factors related to them. Understanding the factors that influence the prevalence of depression and anxiety in lung cancer patients may enable early targeted interventions to high-risk survivors, which can attenuate these negative emotional reactions. The study was approved by the ethics committee.
Methods
Participants
A convenience sample of participants was recruited from the Oncology Department of Guanganmen Hospital, a traditional Chinese medical hospital in Beijing, between April 2017 and January 2018. Outpatient lung cancer patients with a confirmed pathological diagnosis were invited to participate in this study. All patients were informed and agreed to be investigated; 315 eligible patients completed the survey that we distributed, 37 of them were in stage I, 34 were in stage II, 113 patients were in stage III, and 131 in stage IV. As for cancer type, 151 of them had adenocarcinoma, 54 had squamous cell carcinoma, 109 were small cell lung cancer patients, and one had large cell carcinoma. Inclusion criteria were: (i) diagnosed with primary bronchial lung cancer by pathology and/or cytology; (ii) aware of having lung cancer; (iii) aged ≥18 years; (iv) Karnofsky Performance Status (KPS) score ≥60; (v) able to communicate with clinicians and cooperate with investigation; and (vi) able to read and understand the questions. Patients with schizophrenia or other psychiatric disorders, acute or unstable complications, poor compliance, or incomplete data were excluded from the study. Our study was approved by the Human Research Ethics Committees of Guanganmen Hospital, China Academy of Chinese Medical Sciences (reference number: 2017-136-KY). Our study was conducted in compliance with the Declaration of Helsinki, and all patients provided written informed consent.
Measures
Demographic and clinical data
Demographic data included: name, age, gender, education level, and healthcare type. Clinical data were obtained from patients’ medical records, which included pathological type, cancer clinical stage, KPS score, disease course, and cancer therapy (surgery, chemotherapy, radiotherapy, and targeted therapy). The eighth edition of the Tumor Node Metastasis (TNM) staging system of the American Joint Committee on Cancer (AJCC) was used to define clinical stages.
Depression and anxiety
Patients’ depression and anxiety was evaluated using the Hospital Anxiety and Depression Scale (HADS).24 HADS is a 14-item questionnaire that contains two 7-item sub-scales which can assess depressive and anxious symptoms during the past week. This scale is a self-report instrument and has been widely used among cancer patients.25 Scores on each sub-scale range from 0–21, if the total scores of each sub-scale are 8 or more, positive depressive symptoms or anxiety will be considered. In order to enable the eligible patients to understand the questionnaire, we used the Chinese vision of HADS. The participants completed HADS at the time of recruitment.
Statistical analysis
All data were analyzed using SPSS version 22.0 (IBM, Inc., Armonk, NY, USA). Patients’ demographic and clinical information as well as the levels of depression and anxiety were calculated by descriptive statistics. Comparisons between depression/anxiety and non-depression/non-anxiety groups were performed using the independent-sample t-test or Rank sum test for continuous variables and chi-square test for categorical variables. In order to identify significant factors associated with lung cancer patients’ depression and anxiety, a binary logistic regression model was used after univariate analysis.26 P<0.05 was regarded as being statistically significant.
Results
Characteristics of all participants
A total of 402 lung cancer patients met the inclusion criteria. Twenty-two participants were not interested in the research, and 41 had no time to complete the survey. Three hundred and thirty-nine patients agreed to participate in the study. After excluding 22 patients for unidentified TNM stage and two for uncompleted HADS, 315 patients completed the study (Figure 1); 211 (66.98%) were male. The average age of participants was 62.57 years (range=34–89). As for education background, 12.7% were primary school, 31.4% were middle school, 32.4% were high school, and 23.5% were college or higher. Ninety-one patients (28.9%) reported paying medical costs all by themselves, whereas 224 patients (71.1%) had medical insurance. Regarding pathological type, 47.9% of the participants had adenocarcinoma, 17.1% had squamous cell carcinoma, 34.6% had small cell lung cancer, and one patient had large cell carcinoma. As for cancer clinical stage, there were 37 patients (11.7%) in stage I, 34 (10.8%) in stage II, 113 (35.9%) in stage III, and 131 (41.6%) in stage IV. The mean KPS score of the study population was 87.9 (range=60–100), and the disease course was 12 months (range=1–205). Regarding cancer therapy, 31.7% had surgery, 72.1% had chemotherapy, 26.7% had radiotherapy, and 13% accepted targeted therapy (Table 1).
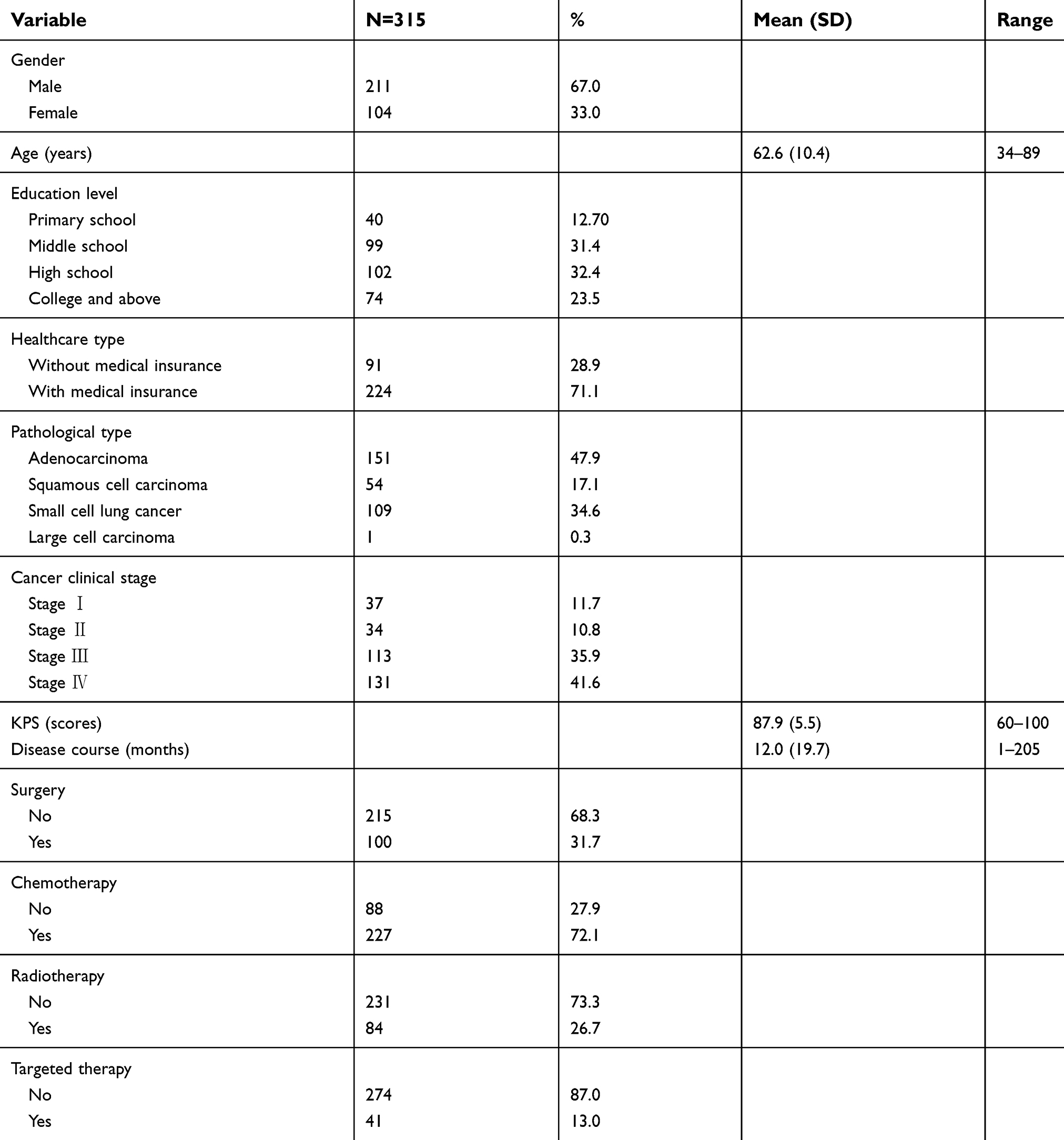 | Table 1 Characteristics of all participants |
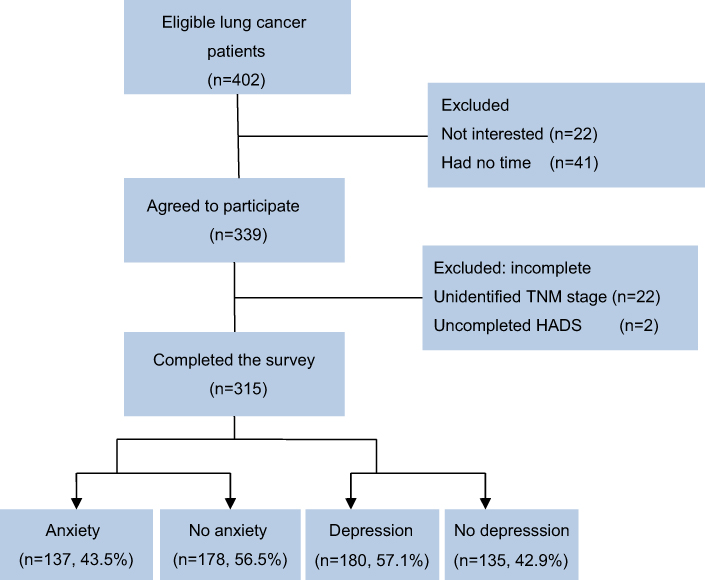 | Figure 1 Enrollment flow of patients. |
Patients’ anxiety and depression prevalence
Among the 315 lung cancer participants, 137 (43.5%) were identified with anxiety, and 180 (57.1%) were identified with depression. The prevalence of depression was higher than anxiety. The average score of the anxiety patients was 10 (range=8–21) and the depression patients was 11.9 (range=8–21).
Univariate analysis of factors in anxiety and depression
The anxiety group and non-anxiety group were significantly different in age (P<0.001), surgery (P=0.010), and radiotherapy (P=0.030). Table 3 shows that the anxiety patients were younger (59.9±10.4 years) than non-anxiety patients (64.6±10.0). Patients without surgery or who received radiotherapy had a higher prevalence of anxiety. No differences were observed in gender, education level, healthcare type, pathological type, cancer clinical stage, KPS, disease course, chemotherapy, or targeted therapy between the two groups (P>0.05) (Table 2).
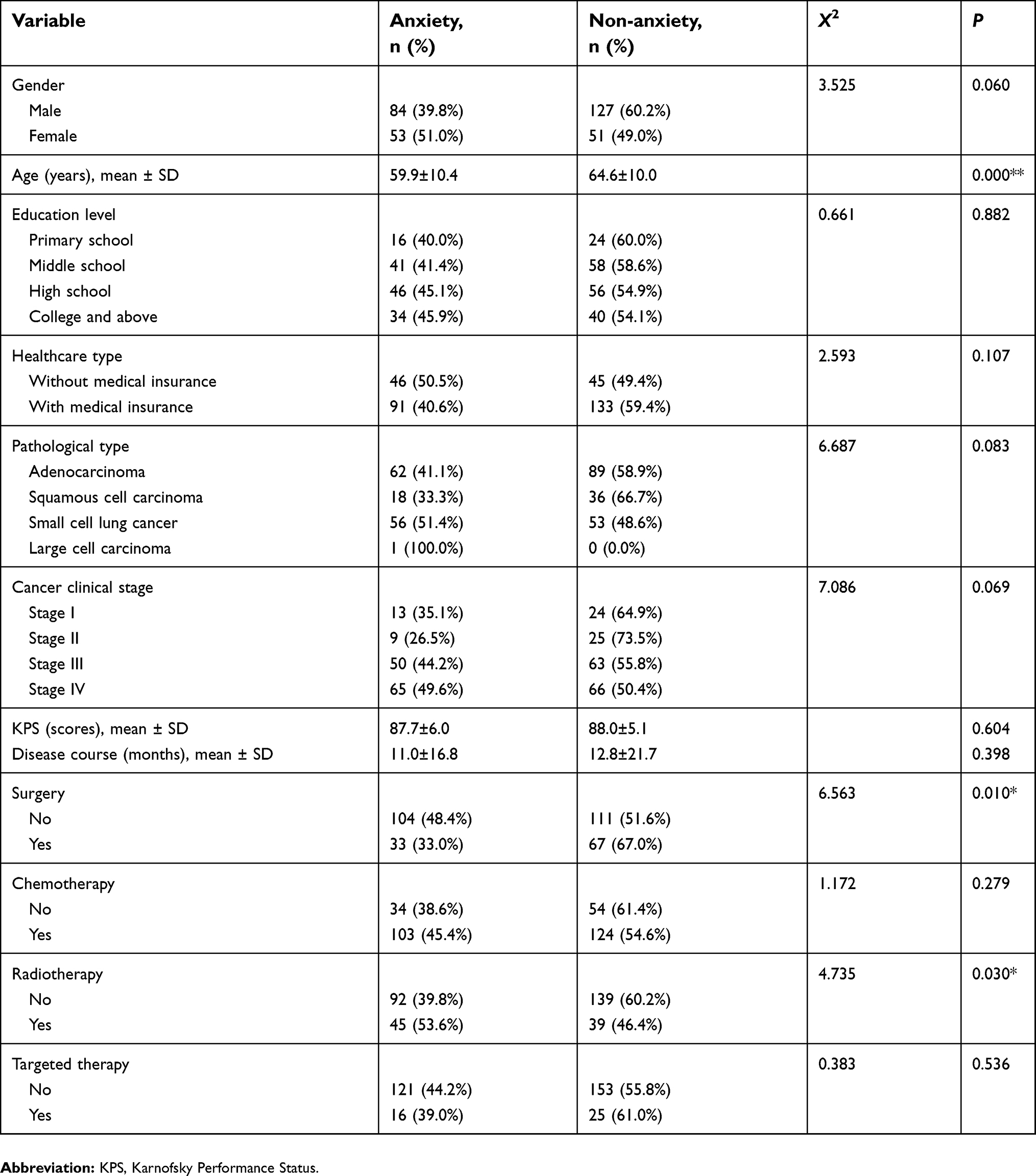 | Table 2 Univariate analysis of factors in anxiety |
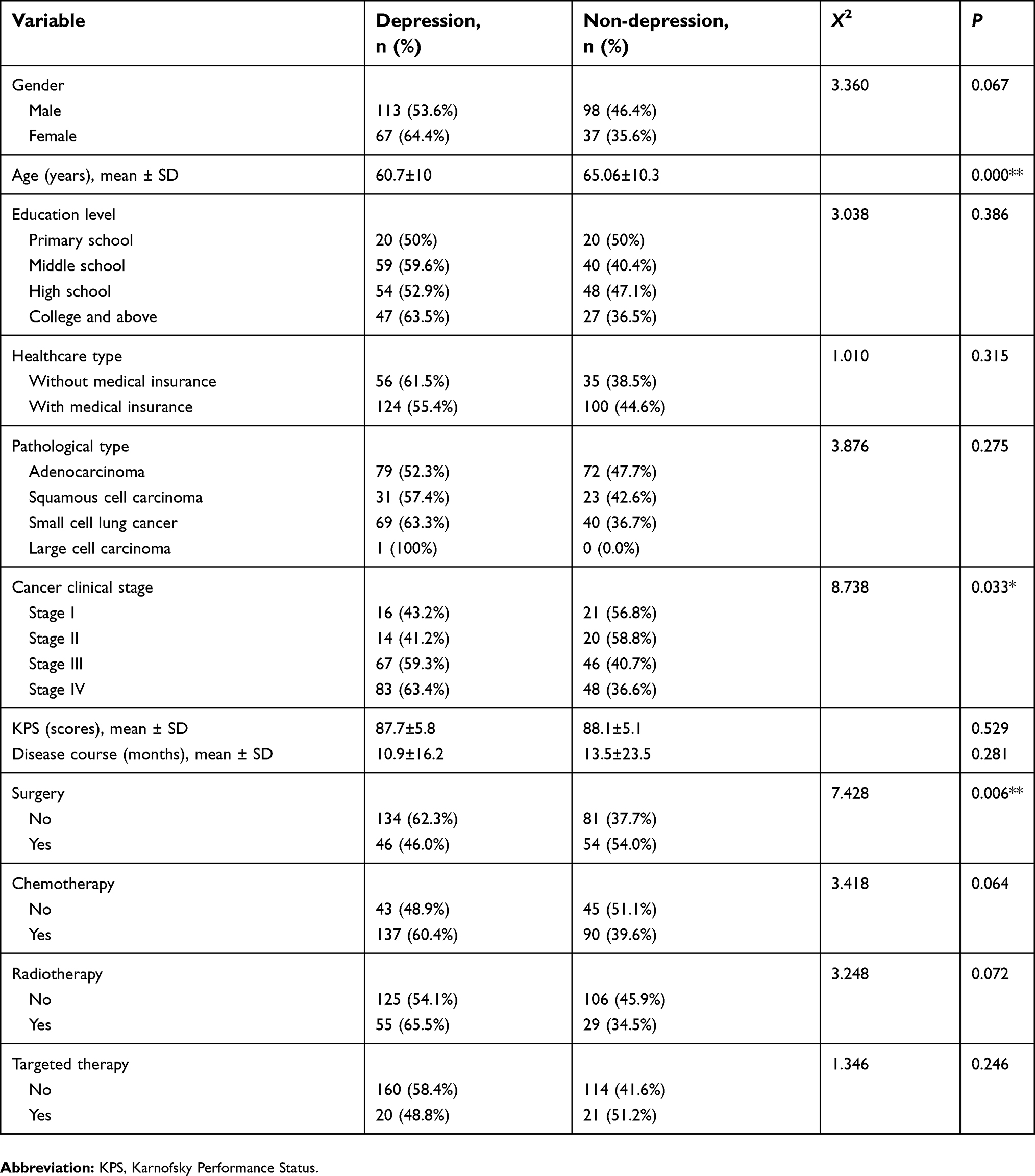 | Table 3 Univariate analysis of factors in depression |
In univariate analysis, the depression and non-depression groups were significantly different in age (P<0.001), cancer clinical stage (P=0.033), and surgery (P=0.006). The mean age of depressed patients was 60.7 years, while that of non-depression patients was 65.06 years. Patients with depression were younger than patients without. Compared with patients in other clinical stages, patients in stage III and stage IV had the higher prevalence of depression. Regarding surgery treatment, patients who received surgery had higher prevalence than those who did not. No differences were observed in gender, education level, healthcare type, pathological type, KPS, disease course, chemotherapy, radiotherapy, or targeted therapy (P>0.05) (Table 3).
Multivariate analysis of factors in anxiety and depression
After univariate analysis, we selected variables with P<0.1 for binary regression analysis. For anxiety, the variables were gender (P=0.060), age (P<0.001), pathological type (P=0.083), cancer clinical stage (P=0.069), surgery (P=0.010), and radiotherapy (P=0.030). For depression, the variables were gender (P=0.067), age (P<0.001), cancer clinical stage (P=0.033), surgery (P=0.006), chemotherapy (P=0.064), and radiotherapy (P=0.072). The significant risk factors of anxiety and depression are shown in Table 4. Patients without surgery had about twice the odds of anxiety and depression than patients received surgery. Age<65 years, especially in the range from 45–65, was a high risk factor of anxiety and depression. Compared with participants aged ≥65 years, participants aged 45–65 years had 8.535-times the odds of anxiety and 4.689-times the odds of depression. No other significant risk factors were identified.
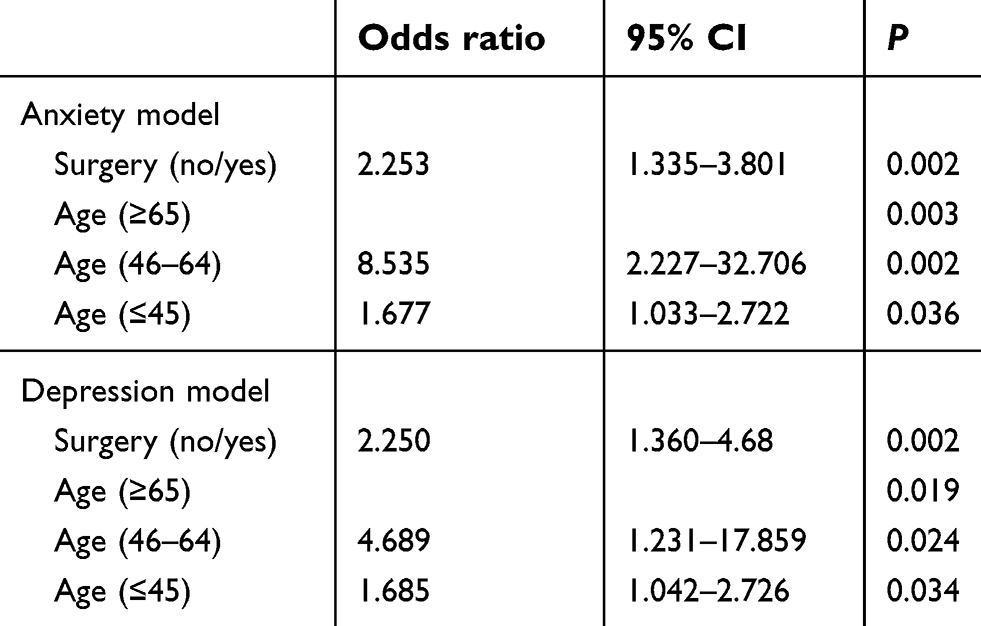 | Table 4 Multivariate analysis of factors in anxiety and depression |
Discussion
This study aimed to investigate the prevalence of anxiety and depression in Chinese patients with lung cancer, as well as the related risk factors. We found the prevalence of anxiety and depression for the 315 lung cancer patients were 43.5% and 57.1%, respectively. Binary regression analysis showed that lack of surgery and younger age (<65 years, especially 45–65 years) were strong independent predictors of both anxiety and depression.
Compared with some previous literature, the reported rates of anxiety in our study were slightly lower. Zang et al27 found that as high as 89.4% of Chinese patients with lung cancer had anxiety in a general hospital of Hebei province. Another study by Longfang et al28 showed that the prevalence was 51.4% in a general hospital of Chongqing province. Similarly, Zhou et al29 found the prevalence of anxiety among lung cancer patients in general hospitals was 50.71%. In China, cancer patients often go to western medical hospitals for treatments such as surgery, chemotherapy, and radiotherapy first. And then, if there are no other effective treatments, they will try traditional Chinese medicine therapy, such as decoction, acupuncture and moxibustion, hydropathic compress, Baduanjin, and Tai Chi. As a consequence, lung cancer patients in traditional Chinese medical hospitals often have a longer disease course so they may have learned to face the cancer after receiving many anti-cancer treatments. In other words, they may be less anxious. Patients in the above studies were all invited from western medical hospitals, while participants of our study were from traditional Chinese medical hospital, which may explain the differences in results. However, one study reported that 35.6% of patients had anxiety in two general hospitals in Shanxi province.30 One possible reason for the lower prevalence of anxiety was that they chose 9 as the cut-off score to identify cases of anxiety, yet we selected 8.
Regarding the prevalence of depression in Chinese patients with lung cancer, our finding is consistent with Pan et al's31 research (60%). However, two studies showed a significantly higher incidence of depression.32,33 This may be due to the different instruments. They all used the self-rating depression scale (SDS) to evaluate depression of participants, while we chose the HADS-D. Compared with two previous studies using the HADS-D, the prevalence of depression in our research is much higher.13,34 As we mentioned before, traditional Chinese medicine is generally considered the lung cancer patient's last hope. This means that patients in traditional Chinese medical hospitals had more serious symptoms and shorter survival time in most cases. Both of the two studies were conducted in western medical hospitals. Hence, it is not hard to understand that the prevalence of depression in our study was higher.
As for the normal population in China, some studies revealed that the incidence of anxiety was 0.46–1.91%35–37 and depression was 3–7.2%.38,39 Apparently, the prevalence of anxiety and depression among lung cancer was markedly higher than in the normal population. Thus, it is indispensable to explore the relation between psychological distress and lung cancer patients when facing such high prevalence.
Both anxiety and depression were obviously associated with two factors, which were lack of surgery and younger age (<65 years). During the investigation, we found that the vast majority of patients in our hospital, who did not undergo surgeries, had no chance to receive surgeries. In general, having a chance to receive surgery means a greater possibility of being cured. Based on this belief, patients with surgeries would be more optimistic and hopeful. Fortunately, hope and optimism are associated with less depression and less anxiety, respectively.40 Nevertheless, no literature results are similar to ours. In contrast, Park et al’s26 study revealed that thoracotomy was a risk factor for postoperative anxiety as well as postoperative depression. The participants of his study all underwent curative pulmonary resection. Furthermore, the time point of Park et al’s postoperative survey was the first clinic visit which is 2 weeks after discharge. The differences of inclusion criteria and length of time after surgery may result in the discrepancy of findings. The young and middle-aged are the main labor force and creators for society. Therefore, they need to bear considerable responsibilities and pressure from family and society. It would be a serious challenge to the family’s financial state once they were diagnosed as lung cancer, let alone treatment expense. Therefore, it’s not surprising that young and middle-aged people, especially middle-aged, were more likely to be depressed and anxious. Similar results were shown in two studies.20,34 Although some researchers have reported the independent risk factors associated with anxiety and depression in lung cancer patients were gender, education level, pathological type, cancer stage, and disease course,5,6,10,13,20,23,28,34 our findings did not detect this relationship.
Some limitations of our study should be mentioned. First, since this was a cross-sectional study, causal relations between the prevalence of anxiety and depression and variables cannot be determined. Second, the relatively small sample size and enrolling participants all from one traditional Chinese medicine hospital may limit the generalizability of the results. Third, we can not be sure if the participants had depressive or anxious symptoms prior to their diagnosis from the survey. Finally, due to the limited time of each investigation, we did not collect information about potential related variables, such as occupation, marital status, income, social support, alcohol status, smoking status, some somatization symptoms, recurrences, and so on.
In the future, cross-sectional studies with a large sample conducted in multiple centers will be needed. Furthermore, research should detect the associations of other variables, as mentioned above. In addition, one study showed that depression could reduce lung cancer patients’ survival time.6 Another research indicated that depression symptoms present at the time of cancer diagnosis were associated with increased mortality, and remission of depression symptoms at follow-up was associated with similar mortality as never having had depression symptoms.41 Further research is needed to elucidate the mechanisms of these findings. Maybe we can investigate whether anti-depression treatment can prolong survival time. Even though most patients with lung cancer can not be cured and die within a short period of time, there are still some traditional Chinese medicine treatments to alleviate their anxiety and depression. One of our previous reviews demonstrates that acupuncture and moxibustion, point application therapy, and five-element music treatment are good choices for treating depression in cancer patients.42
Conclusion
This study demonstrated that anxiety and depression were very common among lung cancer patients. Lack of surgery, young, and middle age were independently risk factors for anxiety and depression. Therefore, medical workers should pay close attention to the emotional changes of these high-risk patients through communication or recording changes in potentially related somatic symptoms like insomnia and poor appetite.
Acknowledgments
This research was supported by “National Natural Science Foundation of China”, No. 81673797; “Beijing Municipal Natural Science Foundation”, No. 7182142; and The Innovative Funding for PhD Students at China Academy of Chinese Medical Sciences, No. CX201802.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng R, Zeng H, Zhang S, Chen T, Chen W. National estimates of cancer prevalence in China, 2011. Cancer Lett. 2016;370:33–38. doi:10.1016/j.canlet.2015.10.003
2. Didkowska J, Wojciechowska U, Mańczuk M, et al. Lung cancer epidemiology: contemporary and future challenges worldwide. Ann Transl Med. 2016;4. doi:10.21037/atm.2016.04.05
3. Sharp L, Carsin AE, Timmons A. Associations between cancer‐related financial stress and strain and psychological well‐being among individuals living with cancer. Psycho-Oncol. 2013;22:745–755. doi:10.1002/pon.3055
4. Haun MW, Sklenarova H, Villalobos M, et al. Depression, anxiety and disease-related distress in couples affected by advanced lung cancer. Lung Cancer. 2014;86:274–280. doi:10.1016/j.lungcan.2014.09.009
5. Shimizu K, Nakaya N, Saito-Nakaya K, et al. Clinical biopsychosocial risk factors for depression in lung cancer patients: a comprehensive analysis using data from the lung cancer database project. Ann Oncol. 2012;23:1973–1979. doi:10.1093/annonc/mds061
6. Arrieta Ó, Angulo LP, Núñez-Valencia C, et al. Association of depression and anxiety on quality of life, treatment adherence, and prognosis in patients with advanced non-small cell lung cancer. Ann Surg Oncol. 2013;20:1941–1948. doi:10.1245/s10434-012-2793-5
7. Jung JY, Lee JM, Kim MS, Shim YM, Zo JI, Yun YH. Comparison of fatigue, depression, and anxiety as factors affecting posttreatment health‐related quality of life in lung cancer survivors. Psycho-Oncol. 2018;27:465–470. doi:10.1002/pon.4513
8. Chambers SK, Baade P, Youl P, et al. Psychological distress and quality of life in lung cancer: the role of health‐related stigma, illness appraisals and social constraints. Psycho-Oncol. 2015;24:1569–1577. doi:10.1002/pon.3829
9. Polański J, Chabowski M, Chudiak A, et al. Intensity of anxiety and depression in patients with lung cancer in relation to quality of life. Pulm Disord Ther. 2017;1023:29–36.
10. Erol Y, Çakan A, Ergönül AG, et al. Psychiatric assessments in patients operated on due to lung cancer. Asian Cardiovasc Thorac Ann. 2017;25:518–521. doi:10.1177/0218492317724044
11. Ye ZJ, Qiu HZ, Li PF, et al. Predicting changes in quality of life and emotional distress in Chinese patients with lung, gastric, and colon‐rectal cancer diagnoses: the role of psychological resilience. Psycho-Oncol. 2017;26:829–835. doi:10.1002/pon.4237
12. Chabowski M, Polański J, Jankowska-Polańska B, Janczak D, Rosińczuk J. Is nutritional status associated with the level of anxiety, depression and pain in patients with lung cancer? J Thorac Dis. 2018;10:2303. doi:10.21037/jtd
13. Gu W, Xu Y-M, Zhu J-H, Zhong B-L. Depression and its impact on health-related quality of life among Chinese inpatients with lung cancer. Oncotarget. 2017;8:104806. doi:10.18632/oncotarget.v8i62
14. Gu W, Xu Y-M, Zhong B-L. Health-related quality of life in Chinese inpatients with lung cancer treated in large general hospitals: across-sectional study. BMJ Open. 2018;8:e019873. doi:10.1136/bmjopen-2017-019873
15. Diaz-Frutos D, Baca-Garcia E, Mahillo-Fernandez I, Garcia-Foncillas J, Lopez-Castroman J. Suicide ideation among oncologic patients in a Spanish ward. Psychol Health Med. 2016;21:261–271. doi:10.1080/13548506.2015.1058960
16. Anguiano L, Mayer DK, Piven ML, Rosenstein D. A literature review of suicide in cancer patients. Cancer Nurs. 2012;35:E14–E26. doi:10.1097/NCC.0b013e31822fc76c
17. Pinquart M, Duberstein P. Depression and cancer mortality: a meta-analysis. Psychol Med. 2010;40:1797–1810. doi:10.1017/S0033291709992285
18. Vodermaier A, Linden W, Rnic K, et al. Prospective associations of depression with survival: a population-based cohort study in patients with newly diagnosed breast cancer. Breast Cancer Res Treat. 2014;143:373–384. doi:10.1007/s10549-013-2795-4
19. Andrykowski MA, Steffens RF, Bush HM, Tucker TC. Disparities in mental health outcomes among lung cancer survivors associated with ruralness of residence. Psycho-Oncol. 2014;23:428–436. doi:10.1002/pon.3440
20. Salvo N, Zeng L, Zhang L, et al. Frequency of reporting and predictive factors for anxiety and depression in patients with advanced cancer. Clin Oncol. 2012;24:139–148. doi:10.1016/j.clon.2011.05.003
21. Lekka D, Pachi A, Tselebis A, et al. Pain and anxiety versus sense of family support in lung cancer patients. Pain Res Treat. 2014;2014:312941. doi:10.1155/2014/312941
22. Choi SH, Chan RR, Lehto RH. Relationships between smoking status and psychological distress, optimism, and health environment perceptions at time of diagnosis of actual or suspected lung cancer. Cancer Nurs. 2019;42:156–163.
23. Hong JS, Tian J. Prevalence of anxiety and depression and their risk factors in Chinese cancer patients. Support Care Cancer. 2014;22:453–459. doi:10.1007/s00520-013-1997-y
24. Zigmond A, Snaith R. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370.
25. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale: an updated literature review. J Psychosom Res. 2002;52:69–77.
26. Park S, Kang CH, Hwang Y, et al. Risk factors for postoperative anxiety and depression after surgical treatment for lung cancer. Eur J Cardiothorac Surg. 2015;49:e16–e21. doi:10.1093/ejcts/ezv336
27. Zang Y, Junmin Z, Weijing Q. Symptom clusters of lung cancer patients and correlation between them and anxiety and depression. Chin Nurs Res. 2018;32(3):384–387.
28. Longfang P, Xiangmei Y, Yueling H. Study on related factors of anxiety of lung cancer patients. Chin Nurs Res. 2012;26(3):686–688.
29. Zhou YM, Liang ZN, Deng L. A survey on anxiety and depression of inpatients with lung cancer. Today Nurs. 2009;12:88–89.
30. Zhang S, Li X, Miao G, et al. Anxiety, depression and self-efficacy in lung cancer patients. J Mod Oncol. 2015;23(9):1221–1223.
31. Pan X, Liang Y, Liu Q. Analysis of the depression status and related factors in elderly patients with lung cancer chemotherapy. Oncol Prog. 2017;15(12):1488–1490.
32. Xiaohong Y, Yiping Z, Lan S, et al. Depression and related factors in inpatients with lung cancer. Chin Rural Health Serv Adm. 2012;32(6):652–654.
33. Jindong X. 319 Cases of Patients with Lung Cancer Merge Depression Analysis and Characteristics of Traditional Chinese Medicine Research. Xinjiang Medical University.2017.
34. Xiaoyan J, Qiaoxian Z. Prevalence of anxiety and depression in 100 lung cancer patients with chemotherapy. Fujian Med J. 2018;40(3):154–156.
35. Sun XL, Li KQ, Cui LJ, et al. Epidemiological survey on generalized anxiety disorder in 4 areas of Hebei province. J Clin Rehabil Tissue Eng Res. 2007;11(39):7842–7844.
36. Ning LI, Jiang C, Liu H, et al. Epidemiological survey of anxiety disorders in urban and rural residents of Liaoning Province. Chin J Prev Control Chronic Non-Commun Dis. 2008;16(2):179–181.
37. Zhong SM, Xiao YN, Chen MY, et al. Epidemiological survey of generalized anxiety disorder in Yunfu City. Hainan Med J. 2015;26(1):135–137.
38. Lin XQ, Zhong WL, Lin SG. The epidemiological investigation on the prevalence of depression among the permanent residents aged 18 and above in Fujian province. Chronic Pathematol J. 2014;15(7):523–525.
39. Yang X. An epidemiological investigation of depression among 3744 Freshmen. China J Health Psychol. 2007;15(6):499–501.
40. Fischer IC, Cripe LD, Rand KL. Predicting symptoms of anxiety and depression in patients living with advanced cancer: the differential roles of hope and optimism. Support Care Cancer. 2018;26(10):3471–3477. doi:10.1007/s00520-018-4215-0
41. Sullivan DR, Forsberg CW, Ganzini L, Au DH, Gould MK, Provenzale D, Slatore CG. Longitudinal changes in depression symptoms and survival among patients with lung cancer: a national cohort assessment. J Clin Oncol. 2016;34:3984. doi:10.1200/JCO.2016.66.8459
42. Xiaoru Y, Peitong Z. Research progress of clinical research on TCM for cancer-related depression. Glob Chin Med. 2016;9:1571–1574.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.